 Soo Young Kim1,2
Soo Young Kim1,2 Sung Hoon Jeong1,2
Sung Hoon Jeong1,2 Hye Jin Joo1,2
Hye Jin Joo1,2 Minah Park1,2
Minah Park1,2 Eun-Cheol Park2,3
Eun-Cheol Park2,3 Jung Hyun Kim3Junbok Lee4
Jung Hyun Kim3Junbok Lee4 Jaeyong Shin2,3*
Jaeyong Shin2,3*- 1Department of Public Health, Yonsei University, Seoul, South Korea
- 2Institute of Health Services Research, Yonsei University, Seoul, South Korea
- 3Department of Preventive Medicine, Yonsei University College of Medicine, Seoul, South Korea
- 4Health IT Center, Yonsei University Health System, Seoul, South Korea
This study aimed to clarify the association between hypertension and conventional cigarette and electronic cigarette (e-cigarette) use, together or individually. A total of 275,762 participants were included, of which 120,766 were men and 154,996 were women. The data were drawn from the Korea Community Health Survey conducted in 2019. A multiple logistic regression model was used to examine the association between hypertension and types of smoking. Hypertension was defined as systolic blood pressure higher than 140 mmHg or diastolic blood pressure higher than 90 mmHg. Based on the types of smoking, participants were grouped as dual smokers of conventional and e-cigarettes, e-cigarette only smokers, conventional cigarette only smokers, past-smokers, and non-smokers. Compared to non-smokers, dual smokers presented the highest odds ratio for hypertension in the male [odds ratio (OR): 1.24, confidence interval (CI): 1.10 to 1.39] and female groups (OR: 1.44 CI: 0.96 to 2.15). According to the Cochran-Mantel-Haenszel test, the two-sided p-value of <0.001 indicated an overall statistically significant association between types of smoking and hypertension. Use of both cigarette types was statistically significant in the male group, but only the use of conventional cigarettes and past smoking were statistically significant in the female group. Among smokers of the two cigarette types, those who were dual smokers of e-cigarettes and conventional cigarettes were the most likely to have the highest prevalence of hypertension.
Introduction
Electronic cigarette (e-cigarette) use has been spreading worldwide in recent years. An e-cigarette is a reusable cigarette, charging nicotine and other cigarette components in the form of a liquid. Since e-cigarettes do not contain the scent of conventional cigarettes, they are commonly favored by adolescents, resulting in an increased prevalence of smoking among the youth. Therefore, e-cigarettes should be thoroughly examined before being recommended as an alternative when helping people to quit smoking safely.
Compared to conventional cigarettes, there are fewer studies about e-cigarettes that assess a large enough sample size to ensure generalizability. E-cigarette devices create aerosols, which many people call “vaper.” This usually contains glycerin, propylene glycol, flavorings, and nicotine (1). The liquid components can vary; for instance, one of the flavoring components contains diacetyl, which is known to cause bronchiolitis obliterans, an irreversible respiratory disease (2, 3). Additionally, e-cigarettes can be harmful mentally as well as physically. A study showed that those who only used e-cigarettes were more likely to have suicidal ideation and planning than dual smokers (4). In another study, e-cigarette use was associated with adverse mental health status, particularly in women (5). As seen in previous studies, there are plural research showing the harmful effects of e-cigarettes. Therefore, further investigation on the safety of e-cigarettes is needed.
In this paper, association between cigarette use and hypertension will be investigated. Hypertension is one of the most well-known chronic disease. Burden of chronic disease has many layers of problems. Firstly, as one of the previous studies indicate, advances in research and health care have reduced mortality from acute diseases and extended life expectancy. Nevertheless, the layers of emotional stress that chronic disease give became a type of problem to cope with for the patients (6). Secondly, the rising cost of medical care is highly dependent on chronic disease patients. The indirect cost is to rise because, as the proportion of patients with chronic health conditions result in limited economic activity, eventually holding back the economic prosperity (7). On this account, we could conclude that there is great harm of cigarettes, and especially in e-cigarettes that could promote one to suffer from hypertension and other chronic diseases.
Smoking and hypertension have a well-known causal relationship (8–10). However, there are two contrary claims regarding e-cigarette smoking (11, 12). One study showed that blood pressure (BP) was controlled in smokers with arterial hypertension who switched to electronic cigarettes (11). In this study, e-cigarettes were used as a way to quit conventional smoking. This showed a considerable reduction in conventional cigarette use in e-cigarette users. Compared to regular conventional cigarette smokers, e-cigarette smokers experienced a reduction in median systolic BP (SBP) from 140 to 130 mmHg (p < 0.001) and diastolic BP (DBP) from 86 to 80 mmHg (p = 0.006). The study concluded that the decline in cigarette consumption was associated with a significant reduction in systolic and diastolic BP compared to the baseline at 12 months (11). However, another cross sectional study concluded that current users of e-cigarettes had higher odds for the prevalence of hypertension [odds ratio (OR) = 1.31 95% confidence interval (CI) (1.05–1.63)] than current conventional cigarette users [OR = 1.27 95% CI (1.10–1.47)]. Respondents who were concurrently smoking both conventional cigarettes and e-cigarettes had the highest odds of having hypertension [OR = 1.77 95% CI (1.32–2.39)], compared to non-smokers (12).
Using the data of a substantial sample size from the Korean Community Health Service (KCHS), which could represent the whole Korean population, we studied the association between e-cigarette use and hypertension according to different smoking practices.
Materials and methods
Data
Data used in the study were accessed from the KCHS implemented in 2019 by the Korea Center for Disease Control and Prevention Agency (KDCA) (13). The KCHS is a nationwide survey acquired annually to evaluate health behavior and health status since 2008 (14). The data from these surveys are used to monitor and estimate the prevalence of chronic diseases in the South Korean population (15, 16).
Participants
In total, 275,840 individuals over the age of 19 years were included in this study. Those aged below 18 years were excluded since this study aimed to investigate the prevalence of hypertension in adults. Moreover, only the participants who did not take hypertension-related medication were included. The KCHS received the Korea Centers for Disease Control and Prevention (KCDC) IRB approval (2016-10-01-P-A) in 2016. From 2017, the ethics approval for the KCHS was waived by the KCDC IRB as it does not fall under human subject research based on the enforcement rule of the bioethics and safety act.
Variables
The dependent variable was the prevalence of hypertension, determined by the SBP cutoff point of 140 mmHg or DBP of 90 mmHg (17). BP was acquired through the measurement section of data collection. The SBP and DBP were each measured three times, and the average was then calculated.
The main independent variable of interest was the type of cigarette used. We divided the variable of interest into five groups: current dual smokers of conventional and e-cigarettes were included in group 1; e-cigarette only smokers, group 2; current conventional cigarette only smokers, group 3; past smokers of either conventional or e-cigarette, group 4; and non-smokers, group 5.
To define the smokers and past smokers smoking, we used the questions asked in the KCHS. Those who answered yes to “Have you ever smoked certain type of cigarette?” and yes to “Are you currently smoking certain type of cigarette?” were defined as current smokers. If the respondent answered yes to the prior question and no to latter question, they were defined as past smokers. Lastly, those who responded no to either of the questions were set as those who never smoked. For past smokers, abstinence time requirement for past smokers was not recorded in the survey.
We controlled for covariates such as demographic and socioeconomic factors, health behaviors, and health conditions of the participants. The demographic factors were age (19–60, at 10-year intervals) and sex. The socioeconomic factors included education level (below middle school, high school, and university or higher), region (urban and rural areas), marital status (living with or without a spouse), occupation (white, pink, blue-collar, and unemployed), and household income in quartiles. Health behaviors included drinking habits (yes or no) and performing physical activity. Health conditions included the perceived amount of stress (a lot or less) and body mass index (underweight/normal and overweight/obese). Since this study examined smoking, we also included the age of onset of conventional smoking and calculated the pack-year of conventional smokers.
Statistical analysis
The frequency of use of the two cigarette types and hypertension stratified by covariates was compared using the chi-squared test. Multiple logistic regression analysis was carried out to examine the association between the type of smoking practice and hypertension.
The data were analyzed and further stratified by sex. The sex difference in smoking was considerable. Therefore, we believed that it would be more precise to divide participants into two groups based on sex (18). The predisposition to smoking was not only seen in Asian countries but also in European countries (19, 20).
The results are reported using ORs and CIs. A p-value < 0.05 was considered statistically significant. The SAS 9.4 (SAS Institute Inc; Cary, North Caroline) software was used for each part of the statistical analysis.
Results
According to the results of our study, 18.3% of the participants were smokers. However, when comparing this rate to other national statistics [20.2% in the Korea National Health and Nutrition Examination Survey (KNHANES) and 21.5% in the national statistics webpage managed by the government], our study results are slightly lower (21). Moreover, the proportion who smoked was 16.3% men and 2% in women. The rate from official national sources was two-fold higher than that of our study [KNHANES: men, 34.7%; women, 5.9%; Korea Statistics (KOSTAT): men, 35.7%; women, 6.7%].
Table 1 shows the general characteristics of the study participants. From the total of 275,762 participants, 120,766 were men and 154,996 were women. The proportion of participants with hypertension was 13.6% for men and 9.4% for women.
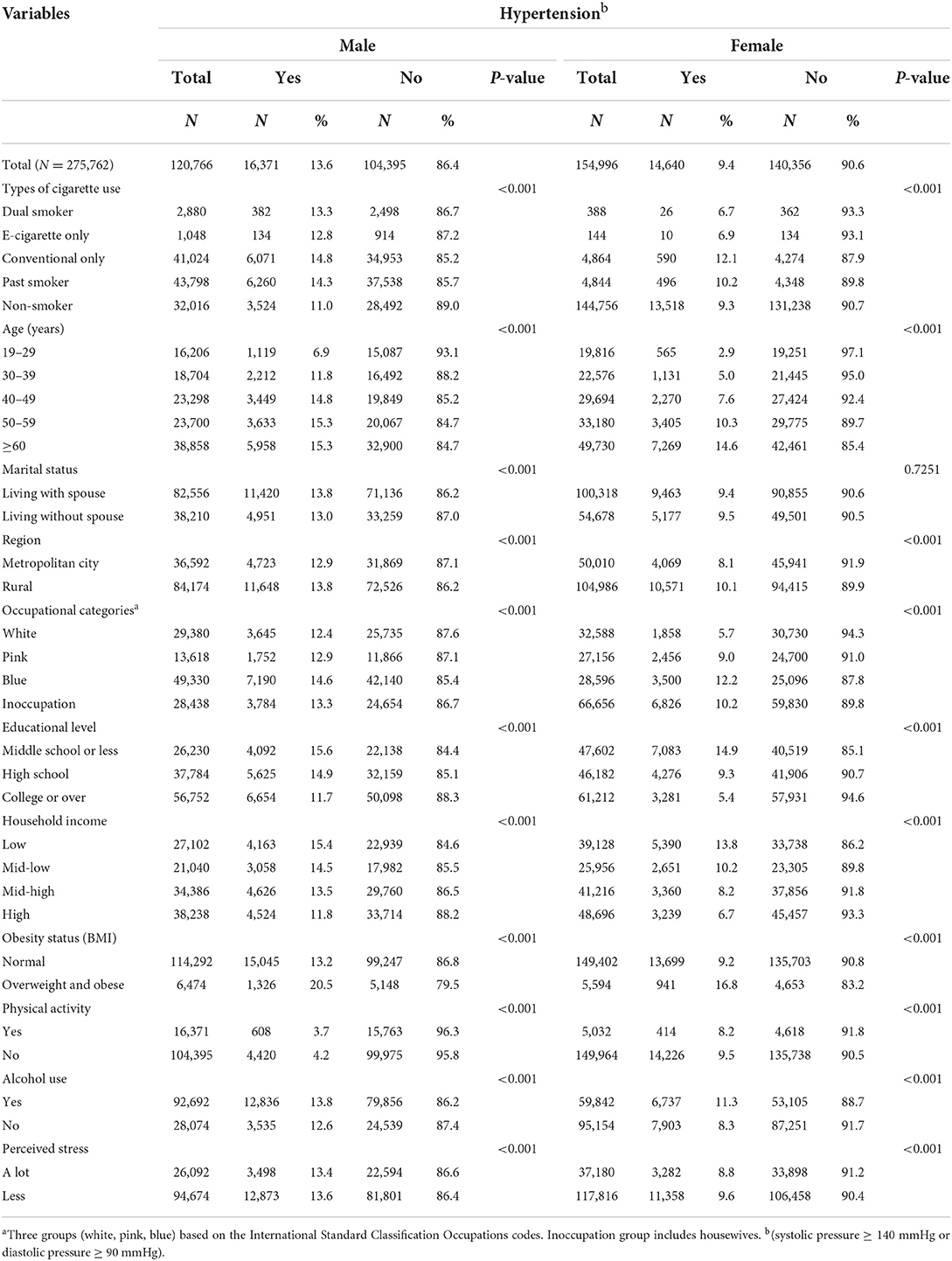
Table 1. General characteristics of the study population.
Table 2 presents the results of logistic regression. Men who smoked e- and conventional cigarettes simultaneously (group 1) and those who smoked only e-cigarettes (group 2) had the highest ORs associated with hypertension [group 1 OR = 1.24, 95% CI (1.11–1.39), group 2 OR = 1.22, 95% CI (1.02–1.48)]. Women with dual smoking (group 1) had the highest OR [OR = 1.44, 95% CI (0.96–2.16)], followed by women who were only e-cigarette smokers [group 2; OR = 1.41, 95% CI (0.74–2.70)]. Although the OR was the maximum, women with dual smoking and e-cigarette only smokers were statistically insignificant. The conventional cigarette only group (group 3) and former smoking group (group 4) were the next to follow in the sex-stratified statistics. These were the only statistically significant groups [group 3 OR = 1.35, 95% CI (1.24–1.48), group 4 OR = 1.11, 95% CI (1.11–1.35)].
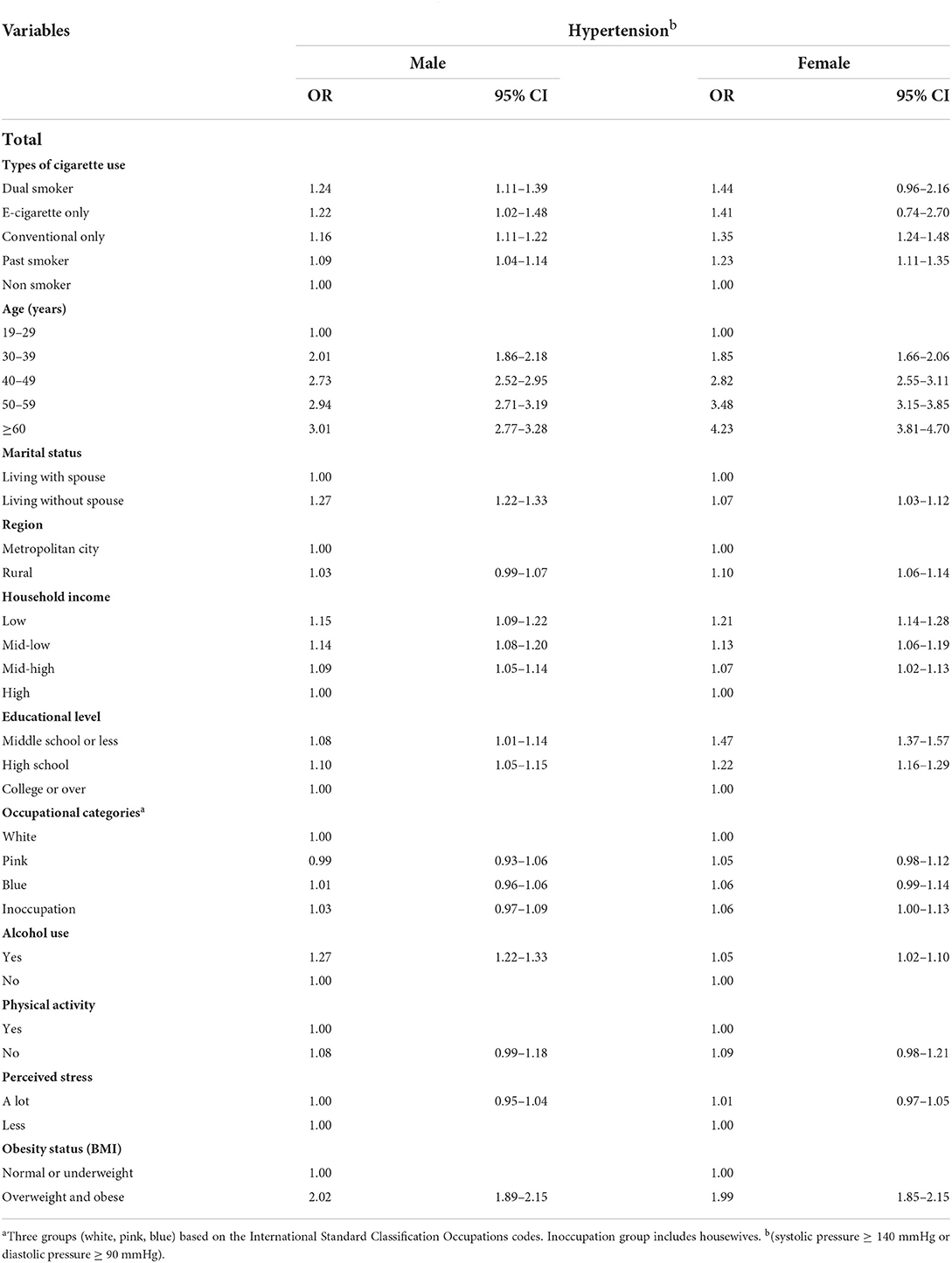
Table 2. Results of factors associated with hypertension by smoking type.
Table 3 shows the results of subgroup analysis stratified by independent variables. Among all the covariates that were modified, only the sociodemographic variables are presented in the table. Overall, the highest odds were found in dual or e-cigarette only smoking groups (group 1 and 2) in each variable for men. Women showed the same tendency as men. However, a few variables such as age group (30 and 40s) showed the highest odds in the conventional only cigarette smokers (group 3) and those who lived with a spouse or were unemployed. In both men and women, those who had educational level of college or over were more likely to have hypertension in those who smoke e-cigarette only [men OR: 1.32, 95% CI (1.05–1.65); female OR: 3.34, 95% CI (1.58–7.06)]. Moreover, among all the other covariates, all household income level particularly had dispersed tendency of having the highest OR across all types of cigarette use in both men and women.
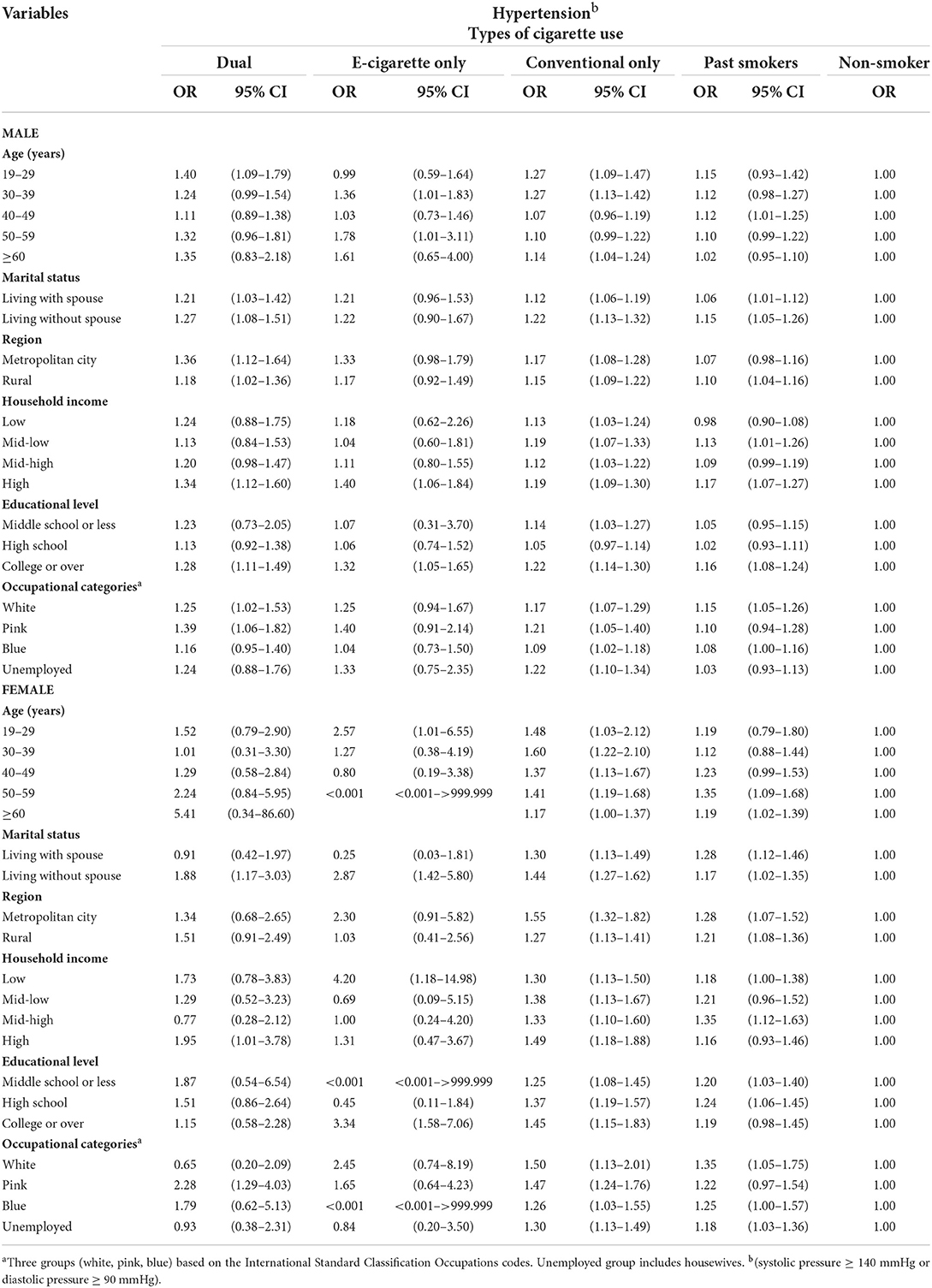
Table 3. The results of subgroup analysis stratified by independent variables.
The logistic regression method indicated that the types of smoking and hypertension were related. Consistent with this, the Cochran-Mantel-Haenszel test for trend analysis also revealed that there is potential trend between types of smoking and hypertension. The two-sided p-value of < 0.001 showed there is an overall statistically significant association between the variable of interest (smoking) and the dependent variable (hypertension).
Table 4 presents the analysis of variables of interest stratified by pack-year and age of onset. In the male group, each group was statistically significant and more likely to experience hypertension than those who had not smoked, except for the e-cigarette only group (group 2). In group 2, the statistics were as follows: [pack-year < 20, OR = 1.16, 95% CI (0.92–1.45); 20 ≤ pack-year < 30, OR = 1.40, 95% CI (0.88–2.23); and pack-year > 30, OR = 1.72, 95% CI (0.99–3.00)]. Pack-year was calculated for group 2 and other groups, as past conventional cigarette smokers were included in the group.
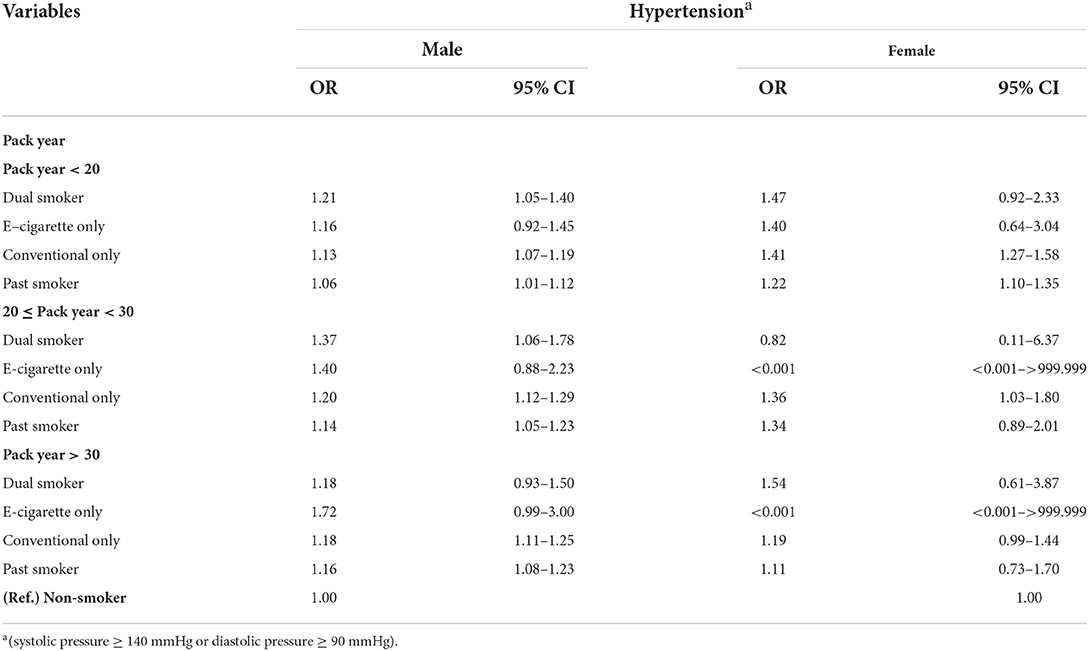
Table 4. Subgroup analysis by pack year.
Figure 1 is a forest plot stratified by the age at onset of smoking differentiated by the cigarette type used. A younger age at onset was associated with the tendency of developing hypertension compared to that in non-smokers, especially men [group 1; starting age < 16, OR = 1.45, 95% CI (1.08–1.94); starting age 16–18, OR = 1.25, 95% CI (1.02–1.53); starting age 19–23, OR = 1.20, 95% CI (1.02–1.40); starting age ≥ 24, OR = 1.12, 95% CI (0.70–1.80)]. Similarly, pack-year and age at onset showed a statistically insignificant association in group 2 due to the small sample size because e-cigarettes are relatively novel.
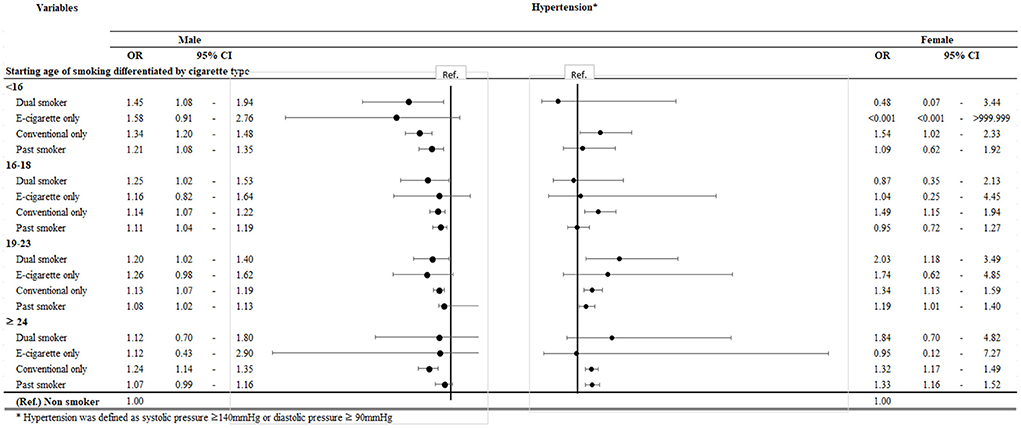
Figure 1. Subgroup analysis by initiation age.
Discussion
In this cross-sectional study on the types of cigarette use and their association with hypertension, dual smokers (group 1) had the highest odds of developing hypertension [OR = 1.24 95% CI (1.11–1.3.9)] among both men and women [OR = 1.44 95% CI (0.96–2.16)]. This was followed by the e-cigarette only smoking group (group 2); the association was not statistically significant in the conventional only group (group 3) and the past smoker group (group 4).
Previous epidemiological studies have described the effects of dual electronic and conventional cigarette use (22–24). Most people begin using electronic cigarettes after having experienced conventional smoking. Therefore, according to a study about the dual use of cigarettes, approximately 85% of e-cigarette users were dual users, and they had greater nicotine dependence and higher urinary cotinine levels than those of conventional cigarette only smokers (22). It is theorized that the nicotine in tobacco products activates the sympathoadrenal system, thereby increasing the heart rate, BP, and glucose levels (23). This result means that dual smokers tend to have a stronger dependency on nicotine than single use smokers of any type. Moreover, in a study regarding the “high-sensitivity C-reactive protein (hs-CRP),” a marker of inflammation which could act as a predictor of cardiovascular disease, researchers found that dual users had the highest risk of having elevated CRP levels. CRP increase is related to smoking intensity; thus, dual use is not recommended as reported by the study (24). Another study indicated that the reason why e-cigarette only smokers tend to have a decreased risk of disease compared to dual smokers is due to their relatively younger age, lower health risk, and higher socioeconomic status (25). Table 3 supports the proportional relationship between dual and e-cigarette only smokers and a higher possibility of hypertension prevalence as explained above. The highest OR among the types of cigarettes used is congregated in the dual or e-cigarette only group in men. Nevertheless, in women, since their proportion was markedly low in the dual or e-cigarette only smoker group, the highest ORs are dispersed throughout the different types of cigarettes used.
According to previous studies, there are results of the more educated respondents more likely to be aware of e-cigarettes, meaning that they perceive the harmfulness of e-cigarette (26, 27). However, in other studies, those with the higher education level were more likely to be current e-cigarette users (28, 29). In Table 3, our study findings showed that those who have educational level of college or higher and smoke e-cigarette only were most likely to have hypertension in both men and women [men OR: 1.32, 95% CI (1.05–1.65); women OR: 3.34, 95% CI (1.58–7.06)]. Our findings regarding income did not show the relation with e-cigarette smoker, but other studies assume that higher educational level and higher income level is associated with e-cigarette smoking. Moreover, further studies subdividing college or above degrees should be explored.
The biological mechanism underlying the harmful effects of electronic cigarette use on the development of various diseases including hypertension has been previously researched (9, 30–35). Hypertension can lead to various heart diseases, including myocardial infarction (MI) (30–34) and stroke (9, 35). According to a previous study, e-cigarette use is related to endothelial dysfunction (30, 31), oxidative stress (30–32), inflammation (30, 32, 33), and activation of platelet (30, 32) and the sympathetic nervous system (30, 32). This suggests that e-cigarettes could be an independent risk for MI in addition to the baseline risk of smoking (30–33). Another study indicated that nicotine and e-cigarette vaping incite a glucose-deprived environment in the neurovascular unit, resulting in a greater danger from stroke (9, 35). Similar to the previous research results regarding the cardiovascular complications stated above, a recent study reported on the “splenocardiac axis” that functions as an inflammatory signaling network, as the basis of ischemic heart disease. This increase in inflammation could lead to future cardiovascular events among e-cigarette users (34).
In addition to the fact that this is one of the first studies to identify the association between cigarette type practices, specifically e-cigarettes, and hypertension, there are also a few other strengths about the study. There was a recent epidemiologic study on vaping and hypertension (12). Similarly to our study, the previous study by Miller et al. researched different types of cigarettes used, including dual use of conventional and e-cigarettes, or the single use of each. Nevertheless, our study differs from this prior study since our data include only the Korean population. Moreover, to examine the association more clearly, we excluded those who took medication for hypertension. Lastly, we adjusted the association with pack-year or age at onset of smoking (Table 4; Figure 1), given that the amount and duration of smoking are important factors in a study regarding smoking.
This study has certain limitations. Firstly, the proportion of participants who only smoke e-cigarettes was lesser than that of conventional smokers. This caused the CI to be insignificant, even though the ORs were relevant. Since e-cigarette use is novel and people smoking them tend to also smoke conventional cigarettes, the numbers were uneven. On account of e-cigarette use being novel, young people tend to use it more, and single smokers in smoking studies are mostly conventional smokers; this group is usually compared with dual smokers (10, 36, 37). Second, although variables of pack-year and age at onset of conventional smoking were adjusted, some level of residual confounding was likely to exist among current exclusive e-cigarette smokers due to varying levels of lifetime exposure to e-cigarette smoking. The data from KDCA does not include information on the amount and duration of e-cigarette smoking. Moreover, family history related to hypertension or other chronic diseases should be adjusted for further studies when key variable is a type of chronic disease, which is highly affected by genetic factors. Third, since this was a survey on the use of cigarettes, it is possible that the female group did not answer the questions honestly. In Korea, due to cultural awareness, women tend to hide their smoking behavior (38). Therefore, the female group values may be less reliable. Lastly, further studies regarding e-cigarette only smokers using panel study designs other than cross-sectional studies, such as longitudinal analysis, are needed.
In conclusion, we found that among smokers of the two cigarette types, people who only smoke e-cigarettes and dual smokers of e- and conventional cigarettes are most likely to have a high prevalence of hypertension (SBP ≥ 140 mmHg or DBP ≥ 90 mmHg). Further research on the adverse effects of e-cigarette use is warranted. Moreover, e-cigarettes should be used after careful verification of the liquid components.
Data availability statement
Data used in the study were accessed from the KCHS implemented in 2019 by the Korea Center for Disease Control and Prevention Agency (KDCA), and further inquiries can be directed to the website (https://chs.kdca.go.kr/chs/rdr/rdrInfoPledgeMain.do).
Ethics statement
The KCHS received the Korea Centers for Disease Control and Prevention(KCDC) IRB approval (2016-10-01-P-A) in 2016. From 2017, the ethics approval for the KCHS was waived by the KCDC IRB as it does not fall under human subject research based on the enforcement rule of the bioethics and safety act. The patients/participants provided their written informed consent to participate in this study.
Author contributions
SK and JS contributed to the conception, design, acquisition, analysis and interpretation of the data, and drafted the manuscript. SK and SJ contributed to the conception and design of the study. HJ and JK worked on analyzing the data as designed. HJ and MP participated in the interpretation of the data. SK and JL wrote the manuscript. E-CP and JS critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Acknowledgments
The authors would like to express deep gratitude to the KCHS and KDCA for the foundation of the study data and allowed to use the data for research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Farsalinos KE, Polosa R. Safety evaluation and risk assessment of electronic cigarettes as tobacco cigarette substitutes: a systematic review. Ther Adv Drug Saf. (2014) 5:67–86. doi: 10.1177/2042098614524430
2. Dinakar C, O'Connor GT. The health effects of electronic cigarettes. N Engl J Med. (2016) 375:1372–81. doi: 10.1056/NEJMra1502466
3. Basáñez T, Majmundar A, Cruz TB, Allem J-P, Unger JB. E-cigarettes are being marketed as “vitamin delivery” devices. Am J Public Health. (2019) 109:194–6. doi: 10.2105/AJPH.2018.304804
4. Lee Y, Lee K-S. Association of depression and suicidality with electronic and conventional cigarette use in South Korean adolescents. Subst Use Misuse. (2019) 54:934–43. doi: 10.1080/10826084.2018.1552301
5. Pham T, Williams JV, Bhattarai A, Dores AK, Isherwood LJ, Patten SB. Electronic cigarette use and mental health: a Canadian population-based study. J Affect Disord. (2020) 260:646–52. doi: 10.1016/j.jad.2019.09.026
6. Turner J, Kelly B. Emotional dimensions of chronic disease. West J Med. (2000) 172:124. doi: 10.1136/ewjm.172.2.124
7. Lubeck DP, Yelin EH. A question of value: measuring the impact of chronic disease. Milbank Quart. (1988) 66:444–64. doi: 10.2307/3349964
8. Virdis A, Giannarelli C, Fritsch Neves M, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Curr Pharm Des. (2010) 16:2518–25. doi: 10.2174/138161210792062920
9. Kaisar MA, Villalba H, Prasad S, Liles T, Sifat AE, Sajja RK, et al. Offsetting the impact of smoking and e-cigarette vaping on the cerebrovascular system and stroke injury: is metformin a viable countermeasure? Redox Biol. (2017) 13:353–62. doi: 10.1016/j.redox.2017.06.006
10. Jeong SH, Jang BN, Kim SH, Jang S-I, Park E-C. Investigation of the association between smoking behavior and metabolic syndrome using lipid accumulation product index among South Korean adults. Int J Environ Res Public Health. (2021) 18:4151. doi: 10.3390/ijerph18084151
11. Polosa R, Morjaria JB, Caponnetto P, Battaglia E, Russo C, Ciampi C, et al. Blood pressure control in smokers with arterial hypertension who switched to electronic cigarettes. Int J Environ Res Public Health. (2016) 13:1123. doi: 10.3390/ijerph13111123
12. Miller CR, Shi H, Li D, Goniewicz ML. Cross-sectional associations of smoking and E-cigarette use with self-reported diagnosed hypertension: findings from wave 3 of the population assessment of tobacco and health study. Toxics. (2021) 9:52. doi: 10.3390/toxics9030052
13. Kim SH, Lee DW, Kwon J, Yang J, Park E-C, Jang S-I. Suicide related indicators and trends in Korea in 2019. Health Policy Manage. (2021) 31:232–9. doi: 10.4332/KJHPA.2021.31.2.232
14. Lee HJ, Jang J, Lee SA, Oh SS, Park E-C. Association between the type of diabetes treatment and depressive symptoms among patients with diabetes: a cross-sectional study of Korea community health surveys data, 2011–2016. Int J Environ Res Public Health. (2019) 16:4441. doi: 10.3390/ijerph16224441
15. Kim JL, Kim JM, Choi Y, Lee TH, Park EC. Effect of socioeconomic status on the linkage between suicidal ideation and suicide attempts. Suicide Life Threat Behav. (2016) 46:588–97. doi: 10.1111/sltb.12242
16. Lee JE, Ju YJ, Park E-C, Lee SY. Effect of poor sleep quality on subjective cognitive decline (SCD) or SCD-related functional difficulties: results from 220,000 nationwide general populations without dementia. J Affect Disord. (2020) 260:32–7. doi: 10.1016/j.jad.2019.08.082
17. Staessen JA, Wang J, Bianchi G, Birkenhäger WH. Essential hypertension. Lancet. (2003) 361:1629–41. doi: 10.1016/S0140-6736(03)13302-8
18. Cai H. Sex difference and smoking predisposition in patients with COVID-19. Lancet Respir Med. (2020) 8:e20. doi: 10.1016/S2213-2600(20)30117-X
19. Bobak M, Gilmore A, McKee M, Rose R, Marmot M. Changes in smoking prevalence in Russia, 1996–2004. Tob Control. (2006) 15:131–5. doi: 10.1136/tc.2005.014274
20. Waldron I. Patterns and causes of gender differences in smoking. Soc Sci Med. (1991) 32:989–1005. doi: 10.1016/0277-9536(91)90157-8
21. Agency(KDCA) KDCaP. National Health Statistics Report. National Health Statistics and Korea DIsease Control and Prevention Agency (2019).
22. Kim C-Y, Paek Y-J, Seo HG, Cheong YS, Lee CM, Park SM, et al. Dual use of electronic and conventional cigarettes is associated with higher cardiovascular risk factors in Korean men. Sci Rep. (2020) 10:1–10. doi: 10.1038/s41598-020-62545-3
23. Tweed JO, Hsia SH, Lutfy K, Friedman TC. The endocrine effects of nicotine and cigarette smoke. Trend Endocrinol Metab. (2012) 23:334–42. doi: 10.1016/j.tem.2012.03.006
24. Mainous III AG, Yadav S, Hong Y-R, Huo J. e-Cigarette and conventional tobacco cigarette use, dual use, and C-reactive protein. J Am Coll Cardiol. (2020) 75:2271–3. doi: 10.1016/j.jacc.2020.02.061
25. Parekh T, Pemmasani S, Desai R. Risk of stroke with e-cigarette and combustible cigarette use in young adults. Am J Prev Med. (2020) 58:446–52. doi: 10.1016/j.amepre.2019.10.008
26. Tan AS, Bigman CA. E-cigarette awareness and perceived harmfulness: prevalence and associations with smoking-cessation outcomes. Am J Prev Med. (2014) 47:141–9. doi: 10.1016/j.amepre.2014.02.011
27. Chapman SLC, Wu L-T. E-cigarette prevalence and correlates of use among adolescents versus adults: a review and comparison. J Psychiatr Res. (2014) 54:43–54. doi: 10.1016/j.jpsychires.2014.03.005
28. Wilson FA, Wang Y. Recent findings on the prevalence of e-cigarette use among adults in the US. Am J Prev Med. (2017) 52:385–90. doi: 10.1016/j.amepre.2016.10.029
29. Ab Rahman J, Mohd Yusoff MF, Nik Mohamed MH, Mahadir Naidu B, Lim KH, Tee GH, et al. The prevalence of E-cigarette use among adults in Malaysia. Asia Pac J Public Health. (2019) 31:9S−21. doi: 10.1177/1010539519834735
30. Alzahrani T, Pena I, Temesgen N, Glantz SA. Association between electronic cigarette use and myocardial infarction. Am J Prev Med. (2018) 55:455–61. doi: 10.1016/j.amepre.2018.05.004
31. Carnevale R, Sciarretta S, Violi F, Nocella C, Loffredo L, Perri L, et al. Acute impact of tobacco vs electronic cigarette smoking on oxidative stress and vascular function. Chest. (2016) 150:606–12. doi: 10.1016/j.chest.2016.04.012
32. Moheimani RS, Bhetraratana M, Yin F, Peters KM, Gornbein J, Araujo JA, et al. Increased cardiac sympathetic activity and oxidative stress in habitual electronic cigarette users: implications for cardiovascular risk. JAMA Cardiol. (2017) 2:278–84. doi: 10.1001/jamacardio.2016.5303
33. Higham A, Rattray NJ, Dewhurst JA, Trivedi DK, Fowler SJ, Goodacre R, et al. Electronic cigarette exposure triggers neutrophil inflammatory responses. Respir Res. (2016) 17:1–11. doi: 10.1186/s12931-016-0368-x
34. Boas Z, Gupta P, Moheimani RS, Bhetraratana M, Yin F, Peters KM, et al. Activation of the “Splenocardiac Axis” by electronic and tobacco cigarettes in otherwise healthy young adults. Physiol Rep. (2017) 5:e13393. doi: 10.14814/phy2.13393
35. Sifat AE, Vaidya B, Kaisar MA, Cucullo L, Abbruscato TJ. Nicotine and electronic cigarette (E-Cig) exposure decreases brain glucose utilization in ischemic stroke. J Neurochem. (2018) 147:204–21. doi: 10.1111/jnc.14561
36. Kim SH, Jeong SH, Park E-C, Jang S-I. Association of cigarette type initially smoked with suicidal behaviors among adolescents in Korea from 2015 to 2018. JAMA Netw Open. (2021) 4:e218803. doi: 10.1001/jamanetworkopen.2021.8803
37. Choi D-W, Jeon J, Lee SA, Han K-T, Park E-C, Jang S-I. Association between smoking behavior patterns and glycated hemoglobin levels in a general population. Int J Environ Res Public Health. (2018) 15:2260. doi: 10.3390/ijerph15102260
Keywords: exclusive e-cigarette use, hypertension, dual smoking, cigarette type, e-cigarette
Citation: Kim SY, Jeong SH, Joo HJ, Park M, Park E-C, Kim JH, Lee J and Shin J (2022) High prevalence of hypertension among smokers of conventional and e-cigarette: Using the nationally representative community dwelling survey. Front. Public Health 10:919585. doi: 10.3389/fpubh.2022.919585
Received: 04 May 2022; Accepted: 12 September 2022;
Published: 17 October 2022.
Edited by:
Dongming Wang, Huazhong University of Science and Technology, ChinaReviewed by:
Chichen Zhang, Southern Medical University, ChinaZhenxing Mao, Zhengzhou University, China
Copyright © 2022 Kim, Jeong, Joo, Park, Park, Kim, Lee and Shin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jaeyong Shin, ZHJzaGluQHl1aHMuYWM=