 Arwa Althumairi
Arwa Althumairi Noot Mishal Ayed AlOtaibi
Noot Mishal Ayed AlOtaibi Arwa Alumran
Arwa Alumran Saja Alrayes
Saja Alrayes Amani Owaidah2
Amani Owaidah2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 09 September 2022
Sec. Occupational Health and Safety
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.917619
Background: A clinical professional has a challenging role during the coronavirus disease (COVID-19) pandemic in providing timely and accurate results with limited resources and a rapid increase in the number of samples to be tested. However, during the ongoing pandemic, the anxiety level of Medical Laboratory Professionals (MLT) has not been studied in Saudi Arabia within the hospital environment.
Aim: To determine the associated factors related with anxiety level of MLT at King Fahd Hospital of the University (KFHU) during the COVID-19 pandemic.
Methods: The study design was a cross-sectional quantitative study. Data were collected by administering a paper-based questionnaire that was distributed among MLT at KFHU. The questionnaire consisted of three sections. The first two sections were prepared by the researchers and included participant demographics and questions related to COVID-19. The third section used the Hamilton Anxiety Scale to assess anxiety levels.
Result: The study revealed that 70.4% of MLT showed no signs of anxiety, while 19.2% showed mild/moderate anxiety levels, and approximately 10.4% showed severe to extreme anxiety levels. In addition, a significant association between the anxiety level and difficulty breathing among MLT wearing personal protective equipment was observed. Moreover, a significant association between sex and anxiety level was identified. Females MLT had higher percentages of severe anxiety (12.8% vs. 5.1%) and mild/moderate anxiety (24.4 vs. 7.7%) than males.
Conclusions: Protecting the mental health status of MLT is an essential part of public health measures to fight the COVID-19 pandemic.
The coronavirus disease 2019 (COVID-19) emerged from Wuhan, China, in December 2019 and has spread across the globe rapidly (1). In March 2020, the World Health Organization (WHO) announced COVID-19 as a global pandemic (1). The first confirmed case of COVID-19 in Saudi Arabia was reported on March 3, 2020 (2). Since then, health care providers have been under considerable pressure due to direct and indirect contact with patients with COVID-19 (3). The occurrence of mistakes is expected due to the unpredicted occurrence of the pandemic and its treatment (4). The pressure might be explained by the mental, psychological and physical pressure in terms of getting infected or spreading the virus to their loved ones. Social isolation increases the demand for health care services and work burnout (5–7). Health care providers (HCPs) in pandemic outbreak conditions fight at the frontline either directly (e.g., physicians, nurses) or indirectly (e.g., laboratory technologists) to deliver patient care. Therefore, the HCP workforce plays a critical role in successfully responding to pandemic situations (8, 9).
A cross-sectional study using online questionnaires was performed in China to assess the mental health status of HCPs and administrative staff in hospitals. A total of 2,299 participants were enrolled in the study, 2,042 of which were HCPs, and the remaining 257 were administrative staff. Findings revealed that both groups showed different levels of severity of fear, anxiety, and depression (10). Moreover, comparing administrative staff, HCPs, and frontline HCPs, the results showed that frontline HCPs in close contact with infected patients recorded higher scores for fear, anxiety, and depression (10). However, it was found that the infectious disease was spread through co-worker rather than direct contact with patient (11).
Frontline HCPs were more susceptible to developing mental health disorders (10). This increased susceptibility may be due to long work hours, the need to wear personal protective equipment (PPE), and the routine donning and doffing of full PPE, which results in physical fatigue, mental stress and difficulty breathing (12, 13). Additionally, many HCPs felt unprepared to deal with the new pandemic due to their lack of knowledge. The fear of spreading the virus to families, friends, or colleagues contributed to the overall anxiety (14), prompting HCPs to isolate themselves from their families and change their daily routines. All of these factors affect mental health status through feelings of loneliness, physical and mental fatigue, insomnia and anxiety (14, 15).
Studies supported that wearing masks might have the potential to reduce the risks of COVID-19 and other respiratory diseases; however, proper handling of masks is not known in society (16). Furthermore, previous studies found that using masks as precautionary measures might have mental and physical side effects, such as headache, fever, and difficulty breathing (13, 17). An understanding of the intensity, chronological, social influence, and timing of the pandemic will help in planning for services and help in future research to understand the geographical distribution of such a pandemic (18).
Several factors might affect mental health among health care providers and general populations during COVID-19, including sex differences, age, exposure to social media, news concerning COVID-19, and fake news, which were highly associated with increasing anxiety levels (19). Moreover, fewer years of work experience indicates a greater likelihood of developing mental health challenges as anxiety levels increase (20). One study reported that marital status affected the mental health status, and married individuals had higher anxiety levels than unmarried individuals (21). Conversely, another study found that widows/divorced individuals experienced more anxiety symptoms than married and single individuals (22). Long quarantine periods and contact with patients with COVID-19 or contaminated objects also led to a higher risk of anxiety (23). More studies on mental health during pandemics should be performed to cover different populations at an international level and ensure that appropriate measures are taken to optimize health care worker mental health and thus achieve optimal health care delivery (20).
During the pandemic, medical laboratory technicians (MLT) experienced an increasing demand to collect and analyze specimens in a timely manner with limited resources (24, 25). To the best of our knowledge, studies assessing the mental health status of HCPs during pandemics are limited, and of those studies agreed that MLT are experiencing high stress, anxiety and depression during the pandanis (26–28). The phycological distress could also related with work burn out. There could be several factors influencing psychological status, namely anxiety these could be, age, gender, marital status, educational level and work experience (26, 27). In addition, MLT were not included in most of the previous studies conducted in Saudi Arabia or Middle East despite their critical roles in collecting, handling, and analyzing patient samples, as well as reporting test results. The aim of this study was to determine the anxiety level of MLT at King Fahd Hospital of the University during the COVID-19 pandemic and to determine the factors that influenced their mental health status.
A quantitative cross-sectional study was conducted to determine the factors related with anxiety level among MLT at King Fahd Hospital of the University (KFUH) in Khobar, Saudi Arabia.
All MLT from KFUH participated in the study. The sample size was estimated using g power, with 95% confidence interval and level of error is 0.05 was 134 (29). One hundred fifty paper-based questionnaires were distributed to all MLT working in the studied hospital between October 29 and November 15, 2020. All MLT staff (150) at the study hospital were all included in the study and only completed questionnaires (125) were included in the study.
The questionnaire was designed in English and consisted of three sections, and the first two sections were designed and reviewed by the research team. The first section focused on collecting demographic data, which included five sets of close-ended questions on sex, age, marital status, years of experience, and working hours per day. The second section contained the COVID-19-related questions, including three sets of polar questions adapted from a previous study (3). The third section was the Hamilton Anxiety Scale (HAMA), a short scale developed in 1,959 by Dr. M. Hamilton, specified for assessing anxiety level. This tool was firstly design for clinical/diagnostic purposes for patient with anxiety neurosis, then it been commonly used as self-rated anxiety level (30). HAMA was previously assessed for its validity internationally including Arab country the internal validity considered as sufficient were between Cronbach alpha = 0.90–0.92 (31, 32). The third section contained 14 questions. The scoring was graded from 0 to 5 points as follows: 0 (not present), 1 (mild), 2 (moderate), 3 (severe), and 4 (very severe). Then, the total HAMA score was categorized as severe anxiety (score ≥ 14 points), mild and moderate anxiety (score of 7–13 points), and no anxiety (score of 0–6 points) following the guideline of study with similar geographical area (10, 33). The questionnaire survey was distributed in English as participant where fluent in English as shown in Appendix 1.
Ethical approval was obtained from the Institutional Review Board of Imam Abdulrahman Bin Faisal University, IRB Number: IRB-PGS-2020-03-350 (Appendix II). Additionally, this paper follows the principles of the Declaration of Helsinki and STROBE guidelines.
All statistical analyses were performed using Statistical Package for Social Sciences (SPSS), Version 27.0. Armonk, NY. A chi-square test (X2) was performed in this study to assess the significance of associations between exposure factors (sex, age, marital status, years of experience, and working hours per day) and the outcome (anxiety scale). The results were considered statistically significant at a p < 0.05.
Eighty-three percent of MLT responded to the survey and were eligible, for a total of 125 participants; their characteristics are described in Table 1. Approximately 68.8% of the participants were females, while the males represented 31.2% of the participants. The majority of the participants were married (72.8%). Approximately 78.40% of the participants were aged <40 years. The majority of the participants had 6–11 and 11–15 years of experience at 33.60 and 30.40%, respectively. Moreover, 72.8% of the total participants worked an 8 h shift (Table 1).
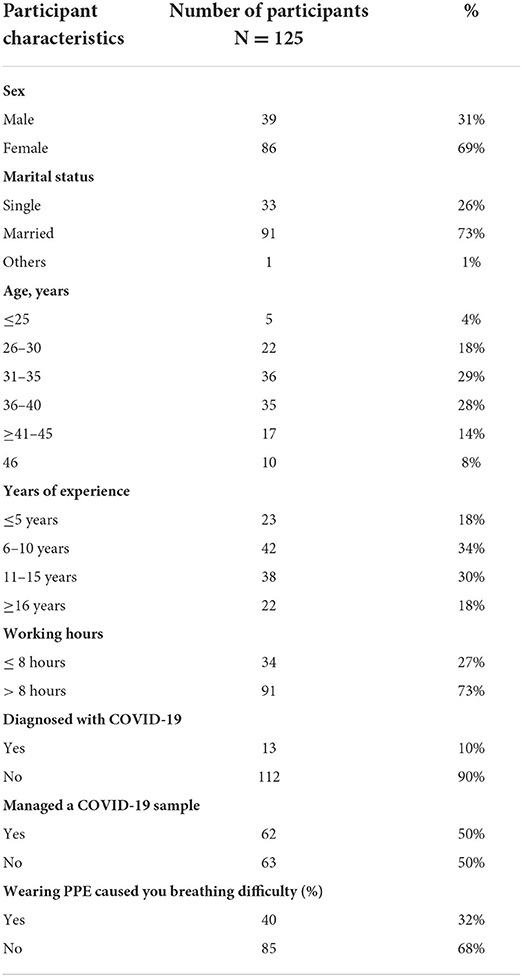
Table 1. Participant characteristics.
As shown in Table 2 most of the MLT were not diagnosed with COVID-19 (89.60%). Additionally, ~50.40% of the MLT managed or processed a COVID-19 sample. Additionally, ~32% of the MLT reported difficulty breathing while wearing PPE.

Table 2. Comparison of anxiety levels among participants with different demographic characteristics.
The anxiety level of MLT during COVID-19 was explored, as shown in; 70.4% were classified as not having anxiety, 19.2% were classified as having mild/moderate anxiety levels, and approximately 10.4% were classified as having severe to extreme anxiety levels.
As shown in Table 2, a statistically significant association between the anxiety level and sex was observed [X2 (DF) = 7.692 (2), p < 0.05]. Females had a higher percentage of severe anxiety (12.8%) than males (5.1%), and 24.4% of females had mild/moderate anxiety was compared with only 7.7% of male. MLT who considered wearing PPE to cause difficulty breathing had higher anxiety levels (22.80%) and ~(27.5%) were classified as having mild and moderate anxiety levels.
A statistically significant association was observed between the anxiety level and difficulty of breathing while wearing PPE [X2 (DF) = 13.869 (2), p < 0.05], (Table 2). No associations were observed between marital status, age, years of experience, working hours, COVID-19 diagnosis, and managing COVID-19 samples (all P > 0.05).
HCPs are often imperiled due to exposure to different types of professional hazards within their workplaces, especially infectious diseases (34). Studying the anxieties of HCPs during the current ongoing COVID-19 pandemic may provide important lessons for managing future pandemics (35, 36).
To the best of our knowledge, this study is the first to focus on the anxiety levels of MLT during the COVID-19 pandemic and related factors. The majority of participants experienced no or mild anxiety. The current study focused on a group that was not studied before and required further intervention to maintain their psychological health.
In the present study, a statistically significant association was observed between anxiety levels and the number of MLT who experienced difficulty breathing while wearing PPE. This finding might be explained by changes in the laboratory guidelines to wear masks to abide by COVID-19 protective and social distancing protocols, while masks are often not necessary in routine practice. Many studies have found that due to the extensive increase in demand for HCPs, they experience long work hours and routinely don and doff full PPE, including face masks, gowns, and gloves, which increase physical fatigue, mental stress, social isolation and difficulty breathing (12, 37, 38).
Moreover, this study also revealed a correlation between the anxiety status and sex, and a statistically significant correlation between sex and the anxiety level was identified. A higher percentage of female MLT had mild to moderate anxiety levels than males. This finding was similar to previous studies conducted during the severe acute respiratory syndrome (SARS) epidemic. Females had higher stress levels and higher levels of depression and anxiety, and they also experienced more severe posttraumatic stress symptoms (39). Likewise, systematic research on the prevalence of symptoms and factors associated with mental health in the general population during the COVID-19 pandemic revealed an association in females exposed to the news concerning COVID-19. The sex differences and mental health have been explained in an earlier study, in which females had a lower ability to cope with trauma than males due to their biological and psychological nature (40). Sex is an important variable that should be considered in biological and social science studies, and more in-depth research must be conducted to understand the causes of these differences (41).
Fake news was strongly associated with increased anxiety levels. Exposure to news via different media sources, such as TV, Twitter and other channels, was significantly related to increased stress and anxiety among populations that reflected the health care provider's mental wellbeing (21, 23). Additionally, anxiety levels have increased not only by exposure to fake news but also by misunderstandings of the reported incidence and fatality rate of COVID-19 by the public (42). Saudi Arabia limited the channels that reveal the number of COVID-19 incidences only through authorized parties such as the Ministry of Health (MOH) websites, official social media accounts and MOH press conferences to ensure accuracy and transparency and to control what information is presented in the media.
A study conducted by Lai et al. (20) revealed that fewer years of work experience rendered individuals more likely to develop mental health illnesses due to increased anxiety levels (20). Exposing to a change in workforce or uncertainty in work, longer work hours usually occurred to joiner staff in which might increase anxiety (20, 43). Additionally, marital status affects mental health status, and married individuals have higher anxiety levels than unmarried individuals (21), and that could be justified as the fear of spread the disease to their beloved once (44). Due to the limited number of participants in our study, the association between age, marital status, years of experience, working hours and anxiety level have no significant finding.
Despite the limited number of participants in the study, only one group of health care providers was analyzed. This information provides insights into the anxiety status of an important group of health care practitioners that were not included in previous studies. This study should be generalized to include all groups of HCPs from the different regions of Saudi Arabia to accurately assess the mental health status of health care practitioners. A study of the factors that might affect the mental health status of laboratory technicians, such as the type of hospital, namely, public or private hospitals, or laboratory unit section, would be very helpful for implementing changes in a health care setting in Saudi Arabia. Nevertheless, Saudi Arabia made a remarkable effort to contain the pandemic by providing the hospital with well-equipped materials and, more importantly, a quick risk management plan to cope with the pandemic, which had a major effect on reducing the stress among HCP and the general population (45, 46). Although the use of masks helped reduce the spread of the disease, some guidelines were recommended to follow during and beyond the COVID-19 pandemic (47). Another limitation of the study was that patient were not asked about previous history of anxiety, this could be correlated with anxiety level in the baseline level before COVID-19. However, other studied showed that there is no relation of previous exposing to infectious diseases and level of anxiety (48).
Protecting the mental health status of MLT is an essential part of public health measures to fight the COVID-19 pandemic due to their critical role in handling COVID-19 samples. Furthermore, anxiety level and other mental health status of health care providers during COVID-19 deserves attention, perhaps through online mental therapy clinics or through developing mental health consultation programs to be provided by hospitals in Saudi Arabia.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval was obtained from the Institutional Review Board of Imam Abdulrahman Bin Faisal University, IRB Number: IRB-PGS-2020-03-350 (Appendix II). The patients/participants provided their written informed consent to participate in this study.
AAlt, NA, AAlu, SA, and AO contributed to the design and implementation of the research, to the analysis of the results, and to the writing of the manuscript.
We thank our colleagues in the laboratory department at King Fahad Hospital of the University for their assistance in facilitating data collection. Additionally, I would like to appreciate American Journal Experts for their English editing of this paper.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.917619/full#supplementary-material
1. Anand KB, Karade S, Sen S, Gupta RM. SARS-CoV-2: Camazotz's curse. Med J Armed Forces India. (2020) 76:136–41. doi: 10.1016/j.mjafi.2020.04.008
2. Hassounah M, Raheel H, Alhefzi M. Digital response during COVID-19 Pandemic in Saudi Arabia (Preprint). J Med Internet Res. (2020) 22:1–14. doi: 10.2196/19338
3. Kang L, Ma S, Chen M, Yang J, Wang Y, Li R, et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav. Immun. (2020) 87:11–7. doi: 10.1016/j.bbi.2020.03.028
4. Simandan D. Being surprised and surprising ourselves: A geography of personal and social change. Prog Hum Geogr. (2020) 44:99–118. doi: 10.1177/0309132518810431
5. Gong Y, Han T, Chen W, Dib HH, Yang G, Zhuang R, et al. Prevalence of anxiety and depressive symptoms and related risk factors among physicians in china: a cross-sectional study. PLoS ONE. (2014) 9:e103242. doi: 10.1371/journal.pone.0103242
6. Shreffler J, Petrey J, Huecker M. The impact of COVID-19 on healthcare worker wellness: a scoping review. West J Emerg Med. (2020) 21:1059–66. doi: 10.5811/westjem.2020.7.48684
7. Yan Z, Cui Y, Chen W, Yu M, Long Q, Yuan Y, et al. The attitude and psychological status of medical staff in China during the COVID-19 outbreak: a cross-sectional survey. The Lancet. (2020) 396:S2. doi: 10.1016/S0140-6736(20)32422-3
8. Preti E, Di Mattei V, Perego G, Ferrari F, Mazzetti M, Taranto P, et al. The psychological impact of epidemic and pandemic outbreaks on healthcare workers: rapid review of the evidence. Curr Psychiatry Rep. (2020) 22:43. doi: 10.1007/s11920-020-01166-z
9. World Health Organization. The Impact of COVID-19 on Health and Care Workers: A Closer Look at Deaths. World Health Organization. (2021). Available online at: https://apps.who.int/iris/handle/10665/345300
10. Lu W, Wang H, Lin Y, Li L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. (2020) 288:1–5. doi: 10.1016/j.psychres.2020.112936
11. Mendonça-Galaio L, Sacadura-Leite E, Raposo J, França D, Correia A, Lobo R, et al. The COVID-19 impact in hospital healthcare workers: development of an occupational health risk management program. PJP. (2020) 38:26–31. doi: 10.1159/000515327
12. Gan WH, Lim JW, Koh D. Preventing intra-hospital infection and transmission of coronavirus disease 2019 in health-care workers. Saf Health Work. (2020) 11:241–3. doi: 10.1016/j.shaw.2020.03.001
13. Kisielinski K, Giboni P, Prescher A, Klosterhalfen B, Graessel D, Funken S, et al. Is a mask that covers the mouth and nose free from undesirable side effects in everyday use and free of potential hazards? Int J Environ Res Public Health. (2021) 18:4344. doi: 10.3390/ijerph18084344
14. Ornell F, Halpern SC, Paim Kessler FH, de Magalhães Narvaez JC. The impact of the COVID-19 pandemic on the mental health of healthcare professionals. Cadernos de Saude Publica. (2020) 36:e00063520. doi: 10.1590/0102-311x00063520
15. Baka Ł. Coronavirus anxiety and exhaustion among Polish front-line healthcare workers–the mediation effect of insomnia. Int J Occup Med Environ Health. (2021) 34:263–73. doi: 10.13075/ijomeh.1896.01745
16. Martin GP, Hanna E, McCartney M, Dingwall R. Science, society, and policy in the face of uncertainty: reflections on the debate around face coverings for the public during COVID-19. Crit Public Health. (2020) 30:501–8. doi: 10.1080/09581596.2020.1797997
17. Ong JJY, Bharatendu C, Goh Y, Tang JZY, Sooi KWX, Tan YL, et al. Headaches associated with personal protective equipment – a cross-sectional study among frontline healthcare workers during COVID-19. Headache. (2020) 60:864–77. doi: 10.1111/head.13811
18. Simandan D. On how much one can take: relocating exploitation and exclusion within the broader framework of allostatic load theory. Health Place. (2010) 16:1291–3. doi: 10.1016/j.healthplace.2010.08.009
19. Xiong J, Lipsitz O, Nasri F, Lui LMW, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J Affect Disord. (2020) 277:55–64. doi: 10.1016/j.jad.2020.08.001
20. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease (2019). JAMA network open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
21. Gao J, Zheng P, Jia Y, Chen H, Mao Y, Chen S, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE. (2020) 15:1–10. doi: 10.1371/journal.pone.0231924
22. Lei L, Huang X, Zhang S, Yang J, Yang L, Xu M. Comparison of prevalence and associated factors of anxiety and depression among people affected by versus people unaffected by quarantine during the COVID-19 epidemic in Southwestern China. Medical Science Monitor. (2020) 26:1–12. doi: 10.12659/MSM.924609
23. Moghanibashi-Mansourieh A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J Psychiatr. (2020) 51:102076. doi: 10.1016/j.ajp.2020.102076
24. Moore J. Laboratory professionals play important role in fight against COVID-19. Military Health System. (2021). Available online at: http://health.mil/News/Articles/2021/04/21/Laboratory-professionals-play-important-role-in-fight-against-COVID19
25. Simundic AM, Lippi G. Preanalytical phase–a continuous challenge for laboratory professionals. Biochemia medica. (2012) 22:145–9. doi: 10.11613/BM.2012.017
26. Zhang Y, Tian L, Li W, Wen X, Wu H, Gong R, et al. Mental health status among Chinese healthcare-associated infection control professionals during the outbreak of coronavirus disease 2019. Medicine (Baltimore). (2021) 100:e24503. doi: 10.1097/MD.0000000000024503
27. Nowrouzi-Kia B, Dong J, Gohar B, Hoad M. Factors associated with burnout among medical laboratory professionals in Ontario, Canada: an exploratory study during the second wave of the COVID-19 pandemic. Int J Health Plann Manage. (2022) 37:2183–97. doi: 10.1002/hpm.3460
28. Swaray SM, Tetteh J, Ekem-Ferguson G, Awinibuno IAN, Adu-Gyasi D, Acheampong F, et al. Psychological distress amongst medical laboratory professionals involved in covid-19-related duties: a nationally stratified cross-sectional survey, Ghana. Inquiry. (2021) 58:00469580211067479. doi: 10.1177/00469580211067479
29. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav Res Methods. (2009) 41:1149–60. doi: 10.3758/BRM.41.4.1149
30. Maier W, Buller R, Philipp M, Heuser I. The hamilton anxiety scale: reliability, validity and sensitivity to change in anxiety and depressive disorders. J Affect Disord. (1988) Ja14:61–8. doi: 10.1016/0165-0327(88)90072-9
31. Hallit S, Haddad C, Hallit R, Akel M, Obeid S, Haddad G, et al. Validation of the Hamilton anxiety rating scale and state trait anxiety inventory a and b in arabic among the lebanese population. Clin Epidemiology Glob Health. (2020) 8:1104–9. doi: 10.1016/j.cegh.2020.03.028
32. Zimmerman M, Kiefer R, Kerr S, Balling C. Reliability and validity of a self-report scale for daily assessments of the severity of anxiety symptoms. Compr Psychiatry. (2019) 90:37–42. doi: 10.1016/j.comppsych.2018.12.014
33. Abbas MAF, Zaid LZA, Hussaein M, Bakheet KH, Alhamdan NA, et al. Anxiety and depression among nursing staff at King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia. In: The 2013 WEI International Academic Conference Proceedings. Istanbul (2013).
34. Chen P, Lei J, Chen F, Zhou B. Experiences and perceptions risk of health-care workers from coronavirus: A protocol for systematic review. Medicine. (2020) 99:e20308. doi: 10.1097/MD.0000000000020308
35. WHO. Novel Coronavirus-China. (2020). Available online at: www.who.int/csr/don/25-january-2020-novel-coronavirus-china/en/.
36. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (London, England). (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
37. WHO. Channel News Asia. Global shortage of masks, protective equipment against coronavirus. (2020). Available online at: https://www.channelnewsasia.com/news/world/wuhan-coronavirus-world-masks-~shortage-who-12406572.
38. Saint SA, Moscovitch DA. Effects of mask-wearing on social anxiety: an exploratory review. Anxiety, Stress, Coping. (2021) 34:487–502. doi: 10.1080/10615806.2021.1929936
39. Lee AM, Wong JGWS, McAlonan GM, Cheung V, Cheung C, Sham PC, et al. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can J Psychiat. (2007) 52:233–40. doi: 10.1177/070674370705200405
40. Liu S, Yang L, Zhang C, Xu Y, Cai L, Ma S, et al. Gender differences in mental health problems of healthcare workers during the coronavirus disease 2019 outbreak. J Psychiatr Res. (2021) 137:393–400. doi: 10.1016/j.jpsychires.2021.03.014
41. Simandan D. Social capital, population health, and the gendered statistics of cardiovascular and all-cause mortality. SSM - Population Health. (2021) 16:100971. doi: 10.1016/j.ssmph.2021.100971
42. Simandan D, Rinner C, Capurri V. Confronting the Rise of Authoritarianism During the COVID-19 Pandemic should be a Priority for Critical Geographers and Social Scientists Canada. ACME: An International Journal for Critical Geographies (2022). p. 226–42.
43. Heidarijamebozorgi M, Jafari H, Sadeghi R, Sheikhbardsiri H, Kargar M, Gharaghani MA. The prevalence of depression, anxiety, and stress among nurses during the coronavirus disease 2019: A comparison between nurses in the frontline and the second line of care delivery. Nurs Res. (2021) 10:188.
44. Omri N, Mlouki I, Sfar H, Ben Youssef F, El Mhamdi S. The fear of Covid-19 and its predictive factors among health care workers in Mahdia Tunisia. Eur J Public Health. (2021). 31:ckab165.107. doi: 10.1093/eurpub/ckab165.107
45. Al-Tawfiq JA, Memish ZA. COVID-19 in the Eastern Mediterranean Region and Saudi Arabia: prevention and therapeutic strategies. Int J Antimicrob Agents. (2020) 55:105968. doi: 10.1016/j.ijantimicag.2020.105968
46. Alumran A. Role of Precautionary Measures in Containing the Natural Course of Novel Coronavirus Disease. JMDH. (2020) 13:615–20. doi: 10.2147/JMDH.S261643
47. Shapiro M, Bouder F. The risks of the mask. J Risk Res. (2021) 24:492–505. doi: 10.1080/13669877.2021.1907611
Keywords: anxiety level, laboratory, COVID-19, mental status, pandemic, PPE
Citation: Althumairi A, Ayed AlOtaibi NM, Alumran A, Alrayes S and Owaidah A (2022) Factors associated with anxiety symptoms among medical laboratory professionals in Khobar: Single institution study. Front. Public Health 10:917619. doi: 10.3389/fpubh.2022.917619
Received: 11 April 2022; Accepted: 15 August 2022;
Published: 09 September 2022.
Edited by:
Mohamed Farouk Allam, Ain Shams University, EgyptReviewed by:
Samir Al-Adawi, Sultan Qaboos University, OmanCopyright © 2022 Althumairi, Ayed AlOtaibi, Alumran, Alrayes and Owaidah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Arwa Althumairi, YWFsdGh1bWFpcmlAaWF1LmVkdS5zYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.