 María F. Mujica-Coopman
María F. Mujica-Coopman Camila Corvalán
Camila Corvalán Marcela Flores
Marcela Flores María Luisa Garmendia
María Luisa Garmendia
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Public Health , 14 July 2022
Sec. Public Health and Nutrition
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.904668
Background: Pregnancy is a critical developmental window in which optimal maternal nutrition and health are key for pregnancy and infant development. The COVID-19 pandemic is considered as a “natural experiment” in which maternal and infant nutrition and health challenges were faced especially in developing countries. Therefore, understanding the health consequences for mothers and infants living in the COVID-19 era is key to revisit public health measures focused on maternal and infant health. The current work aims to describe the design, methods, and descriptive information at recruitment and preliminary findings of the Chilean Maternal & Infant Cohort Study II (CHiMINCs-II) cohort.
Methods: The CHiMINCs-II is an ongoing cohort that is part of the Chilean Maternal and Infant Nutrition Observatory of the South-East area of Santiago, Chile. In total, 1954 pregnant women beneficiaries of the public health systems and their offspring were recruited before 15 weeks of gestation and are followed across pregnancy (<15, 26–28, and 35–37 weeks of gestation) and up to 2 years of age in their offspring. Two studies are currently nested within the CHiMINCs-II cohort: (1) Breast Cancer Risk Assessment in Mothers (BRECAM) study, and (2) the CHiMINCs-COVID study. The primary objective of BRECAM study is to test the association between maternal metabolic indicators (i.e., insulin, glucose, insulin growth factor 1, and hemoglobin A1c concentrations) at early pregnancy (i.e., <15 and 26–28 weeks of gestation) and breast density 3 months after the cessation of lactation. For this purpose, we collect maternal obstetric, lifestyle, dietary intake, anthropometric, and biochemical information. The aim of the CHiMINCs-COVID study is to assess maternal dietary intake and mental health problems derived from the COVID-19 pandemic and their association with maternal and infant's health and nutrition. Thus, we collected detailed information on dietary behaviors, mental health, and COVID-related information at each trimester, along with neonatal and infant nutritional information.
Discussion: The findings of this study will provide novel and critical information to better understand maternal nutritional status, mental health, as well as infant growth and nutrition during the COVID-19 era.
Clinical Trial Registration: BRECAM study registration number NCT03920098 and CHiMINCs-COVID study registration number NCT01916603.
Pregnancy is a critical period in which maternal nutrition, lifestyle and obstetric factors are key for adequate fetal growth (1). Also, all these factors are critical to ensure healthy mother and offspring development and prevent adverse health consequences such as reproductive-related cancers further in life (2–4). Thus, there is a need of advancing on interventions that can show effectiveness under real-life conditions (5, 6). In 2014, we conducted the Chilean Maternal & Infant Cohort study (CHiMINCs), a cluster randomized-controlled trial in which we showed that a low-intensity and high-coverage nutritional intervention delivered through public primary care clinics under standard operating conditions, reduced gestational weight gain, particularly among obese women (7). However, there is limited research on several other conditions such as cancer in identifying modifiable pregnancy risk factors as well as for defining more appropriate clinical management during pregnancy.
Breast cancer (BC) is the leading cause of cancer-related mortality in women worldwide (8) of which higher breast density (BD) (i.e., the percentage of dense tissue of an entire breast) is one of the most important risk factors (9, 10). Interestingly, pregnancy is a critical period for BD reduction, which may be underlined by hormone and pregnancy-related effects in the mammary gland (1, 11, 12). The relationship between reproductive factors, such as full-term pregnancy, and BD has been widely described (13, 14); however, there is a lack of evidence of the relationship between maternal hormonal and metabolic indicators such as insulin and glucose concentrations during pregnancy and BD.
In Chile, the COVID-19 pandemic began in March 2020 generating, as in most of the world, severe health, and economic disruptions. Thus, the COVID-19 pandemic and its associated mitigation measures have become an unexpected “natural experiment” during which the population has faced financial instability (15), mental health challenges (16), and higher food insecurity (17, 18). Pregnancy is a vulnerable period of life and a plasticity developmental window (19). In this sense, an inadequate maternal dietary intake of essential nutrients (i.e., micronutrients) (20, 21), as well as mental health-related challenges (i.e., stress, depression, mood disorders) (22, 23), may lead to adverse health outcomes in the mother and the offspring (24). Moreover, there is increasing realization of the connections between food and nutrition security and mental health (25). Early estimations about the consequences of the COVID-19 pandemic have indicated that the COVID-19 pandemic will significantly contribute to child wasting and mortality (26) and mental health problems (27). Also, we speculate that in countries with alarming rates of obesity and mental health problems such as Chile, food insecurity and inadequate dietary intake (e.g., the lack of consumption of nutrient-dense foods and the higher consumption of ultra-processed foods) may increase the risk of the double burden of malnutrition in our population (28) as well as further deteriorate mental health. Thus, we considered the ongoing CHiMINCs-II cohort as a unique and novel opportunity to explore how the pandemic has impacted nutrition and health of pregnant women in a Latin-American country and how these will relate to future maternal and infant health, including a particular focus on BC, one of the most prevalent cancers in women worldwide. The CHiMINCs-II cohort has the general goal to contribute evidence regarding nutritional and health factors related to maternal and infant development and the development of non-communicable diseases and obesity further in life. The primary intention of the present work is to describe how the CHiMINCs-II cohort is (1) exploring the relationship between maternal metabolic and hormonal changes during pregnancy and risk factors of non-communicable diseases such as breast cancer and (2) exploring the relationship between maternal dietary intake and mental health and maternal and offspring nutritional status living in the COVID-19 era.
The general aim of the CHiMINCs-II cohort is to contribute to the identification of modifiable pregnancy risk markers of future maternal and offspring nutrition and health conditions; given that the CHiMINCs-II cohort takes place under a real-life observatory the ultimate goal of the cohort is that these findings can be translated into concrete actions on the Chilean public health care system and else-where through the modification of clinical guidelines and health care practices. Currently, two ongoing studies are nested within CHiMINCs-II cohort: (1) The Breast Cancer Risk Assessment in Mothers (BRECAM) and (2) The CHiMINCs-COVID study.
The BRECAM study aims to contribute evidence regarding the association between metabolic and hormone disturbances during pregnancy and BD. Considering that BD is one of the most well-known and modifiable risk factors of BC (9), the main goal of the BRECAM study is to provide evidence on how to prevent BC risk through reducing BD. The primary aim of the BRECAM study is to evaluate the association between an altered metabolic milieu [i.e., high levels of glucose, hemoglobin A1c (HbA1c), insulin, and insulin growth factor-1, IGF-1] measured in all trimesters of pregnancy, and BD (% absolute fibro-glandular volume, AFGV and % percentage of fibroglandular volume, FGV) measured by dual-energy X-ray absorptiometry (DXA) 3 months after the cessation of lactation in a cohort of pregnant women. We expect that pregnant woman with an altered metabolic milieu (i.e., higher levels of glucose, HbA1c, insulin, and IGF-1) will have higher BD (defined as higher AFGV and higher %FGV) measured through DXA 3 months after cessation of lactation, compared to women without metabolic disturbances.
The CHiMINCs-COVID study aims to provide critical evidence regarding changes in food habits, food intake and mental health in pregnant women living in the COVID-19 era. Specifically, we sought to (1) evaluate maternal food security (FIES scale), feeding behaviors and food intake during pregnancy, (2) describe maternal mental health symptoms during pregnancy (i.e., depression, anxiety, COVID-related stress, alcohol and drugs use), (3) describe the self-assessed adherence of COVID-19 related mitigation measures, (4) explore the association between maternal dietary intake and maternal mental health with maternal and offspring health outcomes (e.g., maternal nutritional status, glycemic control, prematurity, offspring anthropometry and body composition)in mother-offspring dyad. The expected results of the CHiMINCs-COVID study are that pregnant women will change their dietary intake (i.e., a lower intake of nutrient-dense food) because of the COVID-19 pandemic. These dietary changes will be associated with poorer maternal mental health and the nutritional status of the offspring.
The CHiMINCs-II cohort is part of the Chilean Maternal and Child Nutrition Observatory (CHIMINO). Briefly, CHIMINO is a collaboration between the Institute of Nutrition and Food Technology (INTA), University of Chile, the Pontifical Catholic University of Chile, and the South East Metropolitan Health Service (SSMSO) that aims to provide evidence through interventional and observational studies for achieving healthy nutrition for mother and infants during the first 1,000 days, the early life window (29, 30). The BRECAM (NCT03920098) and CHiMINCs-COVID (NCT01916603) ongoing studies are nested within the CHiMINCs-II cohort, and both correspond to observational prospective cohort studies of pregnant women >18 y who seek prenatal care in any of the public health care centers (PHCC) of Puente Alto, the largest county in the South-East area of Santiago, Chile (Figure 1).
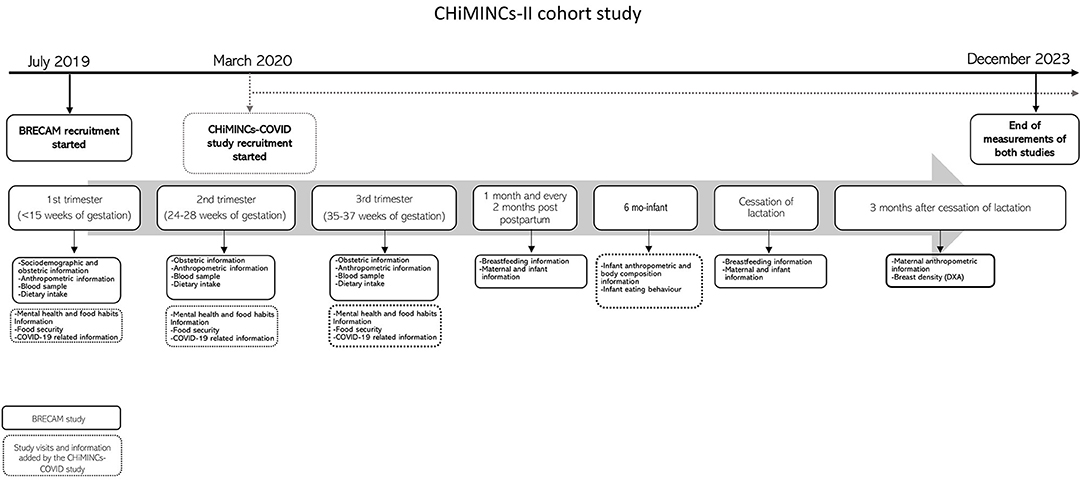
Figure 1. Timeline of the CHiMINCs-II cohort.
Pregnant women receiving care in eight public primary health care units of Puente Alto County (largest county from the South-east area of Santiago, Chile) were invited to participate in the CHiMINCs-II cohort if they meet the following inclusion criteria: (1) >18 y, (2) <15 weeks of gestation at the first prenatal visit, (3) no intention to move outside of Santiago in the next 2 years. In the BRECAM study women were excluded if they had a high-risk pregnancy (i.e., preeclampsia, pre- existing diabetes) according to the National Guidelines (31), pre-existing cancer, family history of breast cancer while in the CHiMINCs-COVID study women were excluded, if they intended to migrate from the public to the private health care system (in Chile, about 20.6% pregnant women from the public system deliver their babies on private clinics) (32).
The CHiMINCs-II cohort is an ongoing study, and we are currently collecting information and conducting research visits in pregnant women and their infants. Recruitment of the CHiMINCs-II cohort participants is part of a collaborative effort between the CHIMINO and the SSMSO. For the current cohort, pregnant women who received primary prenatal care within 8 PHCC located in Puente Alto County were approached between July 2019 and November 2021. From January 2022, we are approaching the mothers of the infants to ask permission for their infants to participate in a 6-mo study research visit. Information about potential participants of the study was obtained at the first prenatal appointment (<15 weeks of gestation) from the electronic clinical records of the PHCC. We also invited pregnant women living in the South-East area of Santiago to participate in the study via social media (i.e., Instagram, Facebook) using an online registration form. A field research assistant checked the eligibility of the potential participants according to the information provided on the online form, and then contacted the eligible participants at the PHCC or by phone to provide information of the studies. If they agreed to participate, research assistants scheduled a telephone research visit within the next 5 days. At the first appointment, inclusion and exclusion criteria were rechecked by trained dietitians; if the participant was confirmed as eligible for the cohort a recorded informed consent was obtained, first trimester measurements were collected and an online package with maternal and COVID-related questionnaires was sent to each participant.
Pregnant women were recruited <15 weeks of gestation and were followed across the second (24–28 weeks of gestation) and third trimester (35–37 weeks of gestation), delivery, 6-months post-partum, and 3 months after the cessation of lactation; telephone follow-up of milk-feeding behavior were also conducted every 2 months after birth (Figure 1).
All evaluations were conducted by trained dietitians; pregnancy evaluations were conducted by phone every trimester while the 6-months and 3 months after the cessation of lactation visits were conducted at the outpatient clinic of INTA. During pregnancy and at delivery biospecimens were collected (see Biological Specimen Collection for details) and milk-feeding behavior was collected by phone by trained personnel. In addition to the information collected at each visit, we had access to medical records that include routinely collected maternal and offspring information from prenatal appointments and at delivery. A summary of all the information collected in the CHiMINCs-II cohort is presented in Table 1.
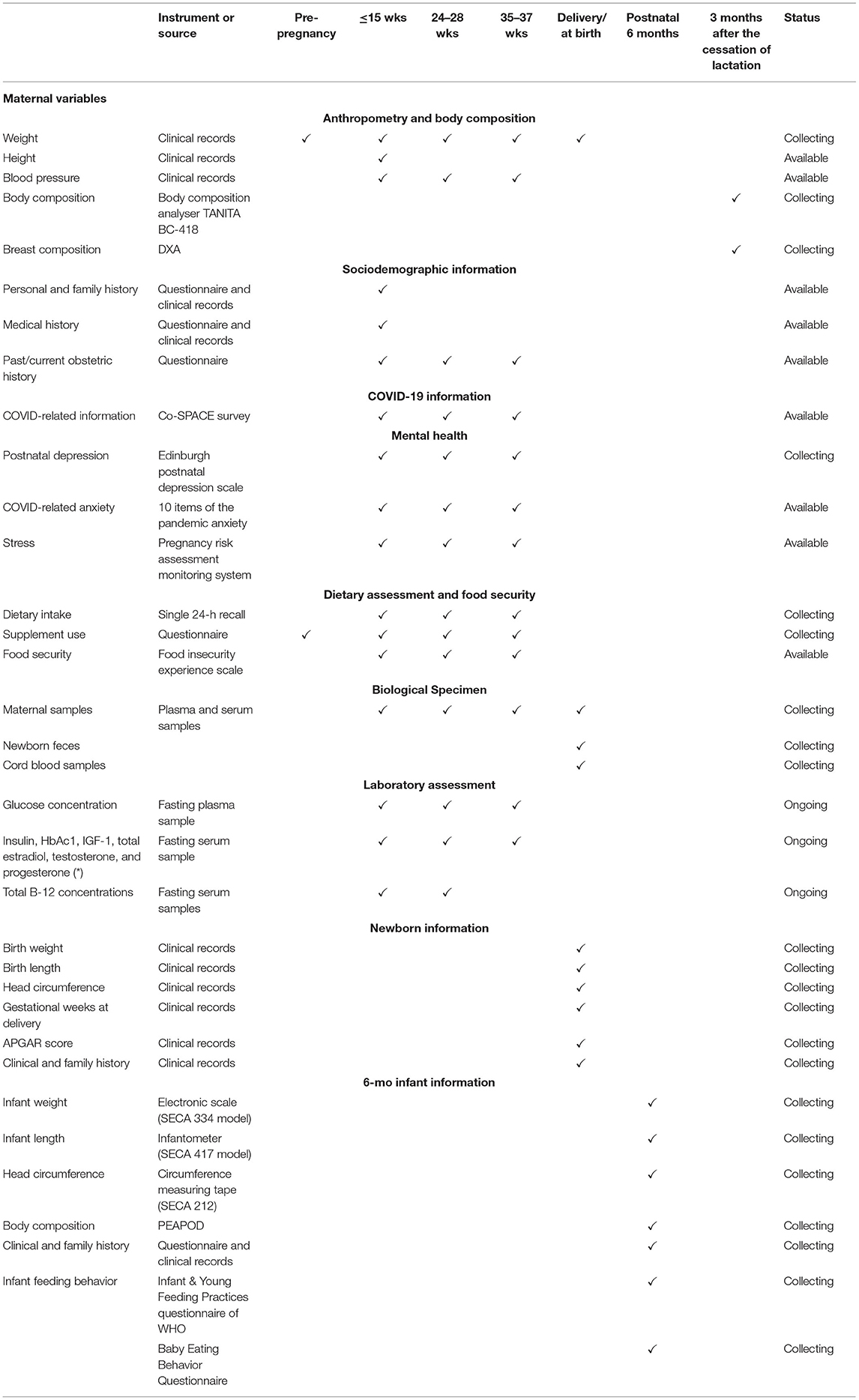
Table 1. Study variables of the CHiMINCs -II cohort.
Maternal age (years), obstetric history (parity, pre-pregnancy weight), medical history (diabetes, hypertension, medication use, depression and anxiety, medication use), family medical history (depression, hypertension, type 2 diabetes, cancer, cardiovascular diseases, gestational diabetes, breast cancer), sociodemographic (marital status, family constellation, occupation, monthly family income) and lifestyle background information (physical activity, alcohol and drug consumption) was collected at the first study visit.
Information on pre-pregnancy weight (kg), maternal height (m), weight (kg), and blood pressure (mmHg) of each participant was obtained from electronic clinical records of the PHCC. All the measurements are routinely collected by trained dietitians of the PHCC at each prenatal appointment, except for maternal height. We used the pre-pregnancy weight and height to calculate the pre-pregnancy body mass index (BMI). Pre-pregnancy BMI was used to classify pregnant women as underweight, normal weight, overweight and obese using the World Health Organization criteria. In addition, we measured maternal body composition after 3 months of lactation cessation using a monitor of body composition (Body composition analyser TANITA BC-418).
At the first (n ~ 500), second (n ~ 1,200) and third-trimester (n ~ 1,000) study visits, dietary intake was collected by a trained dietitian using a semi-automated 24 h-recall, based on the multi-pass method (33). The multiple pass technique is a structured interview that enquires about all foods and liquids ingested the previous day from 00:00 h to 23:59 using the methodology of the 5-Step Multiple-Pass Method. Briefly, the interview is divided into five different steps which increase the chances of remembering usually forgotten food/beverage items. To increase the validity of the information collected, our group has developed a software, SER24H that uses the Food Atlas of the National Consumption Survey; ICC > 0.8 for test-retest. One dietitian will be specifically in charge of analyzing dietary data in terms of consistency and validity during the data collection period. Diet Analyses: SER24H provides the information of energy, macronutrients, and sodium for each food/beverage item, according to the weight/volume consumed and based on the nutrient composition databases of the United States Department of Agriculture (USDA) (34), homologated to Chilean foods (nutrient info obtained from the Chilean Food Composition Table) (35) and the nutrition fact panels of packaged food (collected in the context of the Food Environment Monitoring Project INFORMAS) (36, 37).
Information regarding COVID-19-related social isolation, occupation, social support, and diagnosis of COVID-19 of the participant or family members was collected in all trimesters using an online longitudinal survey that was developed as part of the COVID-19: Supporting Parents, Adolescents and Children during Epidemics (Co-SPACE) study (38). Additionally, self-assessed adherence to COVID-19 preventive measures promoted by the National Health authorities was measured using the Co-SPACE survey and the survey tool and guidance: rapid, simple, flexible behavioral insights on COVID-19 (39). Self-assessed knowledge of COVID-19, self-perception of risk of COVID-19 contagion, self-preventive behavior, sources of information related to COVID-19 news, and trust in COVID-19 related information provided by mass media was measured by the survey tool and guidance: rapid, simple, flexible behavioral insights on COVID-19 (39).
Post-natal depression was measured using the self-administered Edinburgh Postnatal Depression Scale (EPDS) (40), whereas COVID-19-related anxiety was measured using 10 items of the Pandemic Anxiety Scale developed in the Co-SPACE study (38) during pregnancy. We also measured the occurrence of stressful situations in all trimesters of pregnancy using the Pregnancy Risk Assessment Monitoring System (41). In addition, we collected information related to alcohol consumption and recreational drugs use and sleeping habits (38) during COVID-19 pandemic.
For the collection of food security information, we used a reliable, valuable, and internationally validated food insecurity experience scale (FIES) developed by the Food and Agriculture Organization of the United States (FAO). Briefly, this scale was developed using data collected from more than 140 countries, and it provides information about food insecurity by asking the participants directly about their experience of food security (42). Specifically, the FIES measures food insecurity at the household or individual level. Furthermore, in a sub-sample of 350 pregnant women a food frequency questionnaire was used to collect information of the number on meals/days (i.e., breakfast, lunch, dinner), daily routine information (i.e., whether the participant had breakfast), snacks consumption, cooking skills, monthly consumption of rice, pasta, meat, fish, pulses, bread, cheese, milk, sugar, fruits, vegetables, and ultra-processed foods. In addition, we collected prenatal supplement use information (e.g., folic acid) before and during pregnancy, as well as the use of the national complementary food programs, sources of food supply during the COVID-19 pandemic (e.g., public markets), and the use of front-of-package nutrition labels to decide which foods to buy before and after the COVID-19 pandemic.
Information regarding birth weight (g), length (cm), head circumference (cm), weeks of gestation, APGAR score and maternal weight (kg) at delivery was obtained from clinic records. A 6-mo infant research visit is being conducted at INTA. Infant weight (kg) and length (cm) are measured using an electronic scale (SECA 334 model) and infantometer (SECA 417 model), whereas head circumference (cm) is measured using a circumference measuring tape (SECA 212) by trained dietitians. Infant body composition is determined by air-displacement plethysmography (PEA POD, Cosmed, Rome, Italy). The PEA POD body composition measurements have been validated against a four-compartment (4-C) reference model in infants (43), and their reliability and accuracy have been well-established. As part of this research visit, we also collect information regarding infant feeding behavior using a questionnaire based on the Infant & Young Feeding Practices and Baby Eating Behavior questionnaires (44).
Maternal fasting blood samples were routinely collected as part of the prenatal appointments at PHCC using an ethylenediaminetetraacetic acid (EDTA) and serum vacutainers by a certified phlebotomist in all trimesters. Blood samples were processed within the next 3 h at the county's laboratory. Plasma and serum samples were aliquoted and stored at −80 for further analyses. Additionally, as part of the CHiMINCs-COVID study non-fasting maternal and cord blood samples were collected at delivery using EDTA, serum vacutainer, and heparin tubes (i.e., for whole blood) for maternal samples, and EDTA and heparin tubes for cord blood samples. All samples were collected by a certified phlebotomist of the delivery team. Maternal blood samples were collected within 1–48 h before delivery, whereas cord blood samples were collected at delivery. Maternal and cord blood samples were processed within 6 h after collection at the hospital's laboratory. Maternal plasma, serum, whole blood and buffy coat samples, and cord blood buffy coat, plasma and whole blood samples were aliquoted (1 mL) in Eppendorf tubes (1.5 mL) and stored at −80°C for future analysis. Furthermore, newborn fecal samples (300 mg) were collected at 48 h after delivery using Eppendorf tubes (2 ml) and wooden sterile sticks. All the fecal samples were collected after the initiation of feeding (breastfeeding or formula) and were immediately stored at −80°C for further microbiome analysis.
Insulin, HbA1c, IGF-1, total estradiol, testosterone, sex hormone binding globulin (SHBG), and progesterone concentrations will be determined in a sub-sample of pregnant women (n = 400) at least at one trimester during pregnancy. HbA1c concentration were measured by non-porous ion-exchange High-Performance Liquid Chromatography assay, whereas insulin and sex-hormone concentrations were measured by radioimmunoassay (Diagnostic Systems Laboratories). IGF-1 concentration were measured by chemiluminescent immunometric assay (Immulite 2000, Diagnostic Products Corporation). Additionally, we had access to glucose concentration information routinely determined by the glucose oxidase method (Photometric Instrument 4010; Roche) as part of the prenatal appointments at each trimester of pregnancy. As part of the CHiMINCs-COVID study, we will also measure total B-12 concentration in maternal serum samples collected at early-pregnancy (i.e., <31 weeks of gestation). Total B-12 concentration will be determined by chemiluminescent microparticle intrinsic factor assay.
Breast composition is measured using DXA from GE Lunar Prodigy Bone Densitometer (GE Healthcare) calibrated to measure AFGV, %FGV and breast volume (BV) (45) at 3 months after the cessation of lactation. DXA measurements were conducted by a single trained research assistant and all participants were dressed only in a loose hospital gown in the chest area. Breast scans were taken with the participant in a decubitus mediolateral position and the nipple in a lateral position. Breast scans were exported as low-energy and high-energy attenuation images and breast composition data was calculated based on a two-compartment model (adipose and fibro-glandular tissue) using a software developed at University of California San Francisco. A single trained reader (intra and inter-rater ICC > 0.9), following a standard protocol, delineated the total projected breast area manually and the software estimates %FGV, AFGV, and BV automatically. Our group had previously shown a DXA precision of 2.8% for the measurement of BD in 200 adult women (46).
All the lifestyle, demographic, obstetric, biochemical, and COVID-related collected information was entered manually into REDCap by dietitians of the study. Dietary intake was entered into SER24H software by trained dietitians. The sample size was calculated based on the primary objective of the BRECAM study that was the one hypothesized to have the smaller effect size. Based on previous data from our group in pregnant women, the mean ± sd of %FGV was 29 ± 15%. A sample size of 700 women 3 months after breastfeeding cessation is sufficient to detect a difference of 4% in the mean of %FGV between groups (considering 140 women with high glucose levels and 560 with low glucose levels, ratio 1:4, based on our previous data in this population) using a two-sided test with 80% of power and a 5% level of significance. In addition, a sample size of 700 women will allow us to detect a difference of 6% in the mean of %FGV between groups [ratio high (5.7% or more) vs. low HbA1c levels 1:5]. Considering previous data in rates of abortion, loss to follow-up, drop-out and other exclusions previously mentioned (i.e., pre-eclampsia, preterm birth, gestational diabetes mellitus under treatment), we have the goal to recruit 1,500 pregnant women at the beginning of the pregnancy to have at least 700 women 3 months after the cessation of breastfeeding. For stratified analysis (by maternal adiposity or steroid hormone concentrations if interaction terms are statistically significant) we estimated that a final sample size of 300 women per strata would allow us to detect a difference in %FGV of 6% between groups.
The primary outcomes of the BRECAM study are (1) AFGV and (2) %FGV. The main predictors of the study will be: (1) glucose concentration, (2) HbA1c, (3) insulin concentration, and (4) IGF-1 levels during pregnancy. We will also collect data about potential confounders: maternal pre-pregnancy BMI, gestational weight gain, estradiol, progesterone, testosterone and SHBG levels, and initiation and duration of exclusive and predominant breastfeeding. Linear and logistic regression models will be used to test the association between the outcome variables (i.e., AFGV and %FGV) and predictors (i.e., glucose concentration, HbA1c, insulin concentration and IGF-1 levels).
In the case of the CHiMINCs-COVID study, 1,500 pregnant women would allow us to have sufficient power (0.8) to explore the associations between maternal dietary intake or mental health and (1) maternal nutritional status, (2) maternal metabolic control, and (3) offspring health outcomes (e.g., birth weight, prematurity). The primary maternal outcomes of the CHiMINCs-COVID study are (1) maternal weight gain during pregnancy, (2) glucose concentration, (3) HbAc1, (4) insulin concentration and (5) fulfillment of the mitigation COVID-19 measures. The primary infant outcomes are: (1) newborn anthropometric measurements (i.e., birth weight and birth length), (2) prematurity, (3) infant adiposity, and (4) infant anthropometric measurements (i.e., infant weight and length). The main predictors are (1) maternal dietary intake, (2) maternal mental health (i.e., depression and anxiety), (3) changes in maternal dietary intake, and (4) changes in maternal mental health. In addition, we will also collect information regarding potential confounders: (1) maternal education level, (2) income level, (3) pre-pregnancy nutritional status, and (4) history of depression. Linear and logistic regression models will be used to test the association between outcome maternal and infant outcome variables and maternal and infant predictor variables, respectively.
Recruitment of CHiMINCs-II started in July 2019. To date, we have recruited 1,954 pregnant women, which represents 130% of our goal (n = 1,500 pregnant women); we exceeded the original target sample because we observed that compliance with the study visits was lower than what we had originally estimated based on previous experience prior to the COVID pandemic. The collection rate of sociodemographic, medical, obstetric, anthropometric and blood pressure information was >80%. We have conducted 100% of the study visits at the first trimester, and we are currently following-up the recruited participants across the second and third trimester. At the time of writing this work, we have conducted 1,700 and 1,549 visits at the second and third trimester, respectively.
The recruitment for the CHiMINCs-COVID study started in March 2020. A total of 1,805 pregnant women were enrolled during COVID pandemic. We have collected sociodemographic, food intake, mental health, and COVID-19-related information in >84% of the participants at the first study visit (i.e., contacted by phone). Maternal characteristics of the CHiMINCs-II cohort at recruitment are presented in Table 2. The mean (±SD) age of the participants was 29 ± 6 years, most were single (53%) and had completed 12 y of education (71%). On average they were recruited at 12 weeks of gestation, and >70% of the participants had excess weight (BMI ≥ 25 kg/m2) before pregnancy.
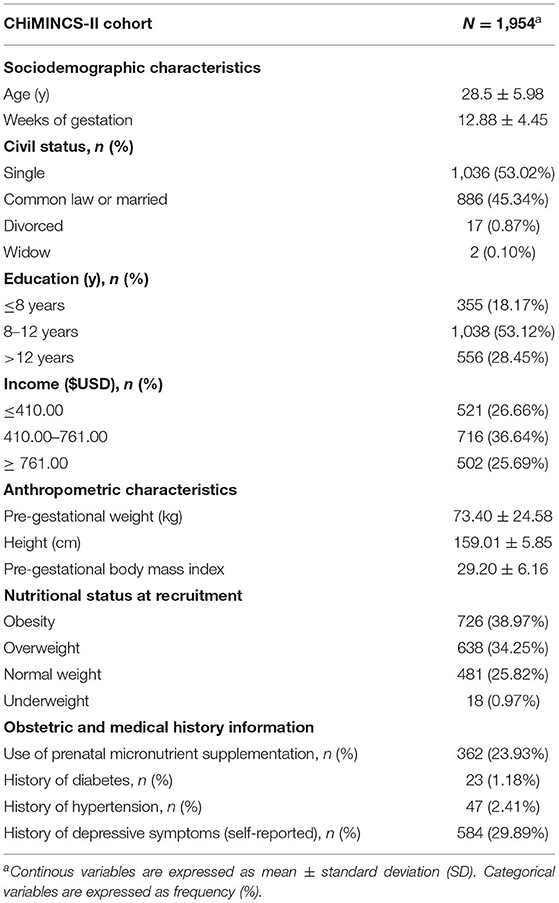
Table 2. Baseline maternal characteristics of the CHiMINCs-II cohort participants (Chile, 2019–2022).
The CHiMINCs-II cohort has collected detailed information on maternal nutrition, mental health, and offspring health in mother-infant dyads experiencing the COVID-19 pandemic in Chile, which may represent the most challenging nutritional situation in the last decades. Considering that the CHiMINCs-II cohort is an ongoing we expect to collect a complete database of maternal and infant variables in 2,000 pregnant women and 600 infants (6 months of age), respectively.
Given the wealth of information we will be able to properly explore how nutrition and mental health impacts maternal and infant health, with a particular focus on BC-related outcomes. Furthermore, the availability of biological specimens (i.e., maternal blood samples, cord blood samples, and fecal samples) at different time points of the study offers the opportunity to explore critical research questions related to mechanisms underlying these relationships as well as identifying potential modifiable markers of disease. Ultimately, we expect that the CHiMINCs-II results will contribute to the update of clinical protocols and pregnancy risk-assessments to ensure better maternal and infant nutrition and health in the recovery of the pandemic.
The CHiMINCs-II cohort nested studies were reviewed and approved by the Institutional Review Boards of INTA, University of Chile, and SSMSO. Participants provided informed consent before conducting any evaluation and understood that they could withdraw from the study at any moment. Given the restrictions because of the COVID-19 pandemic situation, we obtained written, electronic, or verbal consent (recorded by phone). All the consent forms were approved by the Ethics Committee at the Institute of Nutrition and Food Technology (INTA), University of Chile and SSMSO. Participants also provided informed consent to provide access to their clinical records.
MFM-C wrote the first draft of the manuscript. MG led the design and methods of the BRECAM study. CC led the design and methods of the CHiMINCs-COVID study. MF contributed to the coordination and data for the study. MG and CC were all responsible for the initial methodology described in the paper. All authors contributed to the manuscript writing and read and approved the final manuscript.
The BRECAM study was funded by the national grant FONDECYT#1190532, and the CHiMINCs-COVID study was funded by the national grant ANID-COVID#0591 and FONDECYT#3210464. The funding sources had no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank to our participants for their interest and dedication to participate in our study. Also, we would like to thank all the research personnel involved in the study and to our collaborators and staff in the hospital and SSMO.
CHiMINCs, Chilean Maternal & Infant Cohort Study II; BRECAM, Breast Cancer Risk Assessment in Mothers; IGF-1, Insulin growth factor-1; BC, Breast cancer; BD, Breast density; HbA1c, Hemoglobin A1c; AFGV, % absolute fibro-glandular volume; FGV, % percentage of fibroglandular volume; DXA, dual-energy X-ray absorptiometry; CHIMINO, Chilean Maternal and Child Nutrition Observatory; INTA, Institute of Nutrition and Food Technology; SSMSO, Southeast Metropolitan Health Service; PHCC, public health care centers; BMI, body mass index; USDA, United States Department of Agriculture; EPDS, Edinburgh Postnatal Depression Scale; FAO, Food and Agriculture Organization of the United States; EDTA, ethylenediaminetetraacetic acid; SD, standard deviation.
1. Ursin G, Bernstein L, Wang Y, Lord SJ, Deapen D, Liff JM, et al. Reproductive factors and risk of breast carcinoma in a study of White and African-American women. Cancer. (2004) 101:353–62. doi: 10.1002/cncr.20373
2. Wu G, Bazer FW, Cudd T, Meininger CJ, Spencer TE. Maternal nutrition and fetal development. J Nutr. (2004) 134:2169–72. doi: 10.1093/jn/134.9.2169
3. Hoffman DJ, Reynolds RM, Hardy DB. Developmental origins of health and disease: current knowledge and potential mechanisms. Nutr Rev. (2017) 75:951–70. doi: 10.1093/nutrit/nux053
4. McKerracher L, Moffat T, Barker M, McConnell M, Atkinson SA, Murray-Davis B, et al. Knowledge about the Developmental Origins of Health and Disease is independently associated with variation in diet quality during pregnancy. Matern Child Nutr. (2020) 16:1–13. doi: 10.1111/mcn.12891
5. Godfrey KM, Reynolds RM, Prescott S, Nyirenda M, Jaddoe VW, Eriksson JG, et al. Influence of maternal obesity on the long-term health of offspring. Lancet Diabetes Endocrinol. (2017) 5:53–64. doi: 10.1016/S2213-8587(16)30107-3
6. Hanson M, Barker M, Dodd J, Kumanyika SK, Norris S, Steegers E, et al. Interventions to prevent maternal obesity before conception, during pregnancy, and post partum. Lancet Diabetes Endocrinol. (2017) 5:65–76. doi: 10.1016/S2213-8587(16)30108-5
7. Garmendia ML, Corvalan C, Araya M, Casanello P, Kusanovic JP, Uauy R. Effectiveness of a normative nutrition intervention in Chilean pregnant women on maternal and neonatal outcomes: the CHiMINCs study. Am J Clin Nutr. (2020) 112:991–1001. doi: 10.1093/ajcn/nqaa185
8. Azamjah N, Soltan-Zadeh Y, Zayeri F. Global trend of breast cancer mortality rate: a 25-year study. Asian Pacific J Cancer Prev. (2019) 20:2015–20. doi: 10.31557/APJCP.2019.20.7.2015
9. Rice MS, Rosner BA, Tamimi RM. Percent mammographic density prediction: development of a model in the nurses' health studies. Cancer Causes Control. (2017) 28:677–84. doi: 10.1007/s10552-017-0898-7
10. Butler LM, Gold EB, Greendale GA, Crandall CJ, Modugno F, Oestreicher N, et al. Menstrual and reproductive factors in relation to mammographic density: the Study of Women's Health Across the Nation (SWAN). Breast Cancer Res Treat. (2009) 112:165–74. doi: 10.1007/s10549-007-9840-0
11. Britt K, Ashworth A, Smalley M. Pregnancy and the risk of breast cancer. Endocr Relat Cancer. (2007) 14:907–33. doi: 10.1677/ERC-07-0137
12. Beral V, Bull D, Doll R, Peto R, Reeves G. Breast cancer and breastfeeding: collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including 50 302 women with breast cancer and 96 973 women without the disease. Lancet. (2002) 360:187–95. doi: 10.1016/S0140-6736(02)09454-0
13. Loehberg CR, Heusinger K, Jud SM, Haeberle L, Hein A, Rauh C, et al. Assessment of mammographic density before and after first full-term pregnancy. Eur J Cancer Prev. (2010) 19:405–12. doi: 10.1097/CEJ.0b013e32833ca1f4
14. Husby A, Wohlfahrt J, Øyen N, Melbye M. Pregnancy duration and breast cancer risk. Nat Commun. (2018) 9:4255. doi: 10.1038/s41467-018-06748-3
15. Thurlow J. COVID-19 Lockdowns Are Imposing Substantial Economic Costs on Countries in Africa. (2020). Available online at: https://www.ifpri.org/blog/covid-19-lockdowns-are-imposing-substantial-economic-costs-countries-africa (accessed June 20, 2022).
16. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
17. Wolfson JA, Leung CW. Food insecurity and COVID-19: disparities in early effects for us adults. Nutrients. (2020) 12:1–13. doi: 10.3390/nu12061648
18. Niles MT, Bertmann F, Belarmino EH, Wentworth T, Biehl E, Neff R. The early food insecurity impacts of covid-19. Nutrients. (2020) 12:1–23. doi: 10.3390/nu12072096
19. Harding R, Bocking AD. Fetal Growth and Development. Cambridge; New York, NY: Cambridge University Press (2001).
20. Chen LW, Aris IM, Bernard JY, Tint MT, Colega M, Gluckman PD, et al. Associations of maternal macronutrient intake during pregnancy with infant BMI peak characteristics and childhood BMI. Am J Clin Nutr. (2017) 105:705–13. doi: 10.3945/ajcn.116.148270
21. Villamor E, Rifas-Shiman SL, Gillman MW, Oken E. Maternal intake of methyl-donor nutrients and child cognition at 3 years of age. Paediatr Perinat Epidemiol. (2012) 26:328–35. doi: 10.1111/j.1365-3016.2012.01264.x
22. Henrichs J, Schenk JJ, Roza SJ, Van Den Berg MP, Schmidt HG, Steegers EAP, et al. Maternal psychological distress and fetal growth trajectories: the generation R study. Psychol Med. (2010) 40:633–43. doi: 10.1017/S0033291709990894
23. Dole N, Savitz DA, Siega-Riz AM, Hertz-Picciotto I, McMahon MJ, Buekens P. Psychosocial factors and preterm birth among African American and white women in central North Carolina. Am J Public Health. (2004) 94:1358–65. doi: 10.2105/AJPH.94.8.1358
24. Lindsay KL, Buss C, Wadhwa PD, Entringer S. The interplay between maternal nutrition and stress during pregnancy: issues and considerations. Ann Nutr Metab. (2017) 70:191–200. doi: 10.1159/000457136
25. Sparling TM, Cheng B, Deeney M, Santoso M V., Pfeiffer E, Emerson JA, et al. Global mental health and nutrition: moving toward a convergent research agenda. Front Public Heal. (2021) 9:1–7. doi: 10.3389/fpubh.2021.722290
26. Osendarp S, Akuoku JK, Black RE, Headey D, Ruel M, Scott N, et al. The COVID-19 crisis will exacerbate maternal and child undernutrition and child mortality in low- and middle-income countries. Nat Food. (2021) 2:476–84. doi: 10.1038/s43016-021-00319-4
27. Liu X, Zhu M, Zhang R, Zhang J, Zhang C, Liu P, et al. Public mental health problems during COVID-19 pandemic: a large-scale meta-analysis of the evidence. Transl Psychiatry. (2021) 11:1–10. doi: 10.1038/s41398-021-01501-9
28. GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. (2017) 377:13–27. doi: 10.1056/NEJMoa1614362
29. Garmendia, Corvalan C, Araya M, Casanello P, Kusanovic JP, Uauy R. Effectiveness of a normative nutrition intervention (diet, physical activity and breastfeeding) on maternal nutrition and offspring growth: the Chilean maternal and infant nutrition cohort study (CHiMINCs). BMC Preg Childbirth. (2015) 15:1–6. doi: 10.1186/s12884-015-0605-1
30. Garmendia M, Corvalán C, Casanello P, Araya M, Flores M, Bravo A, et al. Effectiveness on maternal and offspring metabolic control of a home-based dietary counseling intervention and DHA supplementation in obese/overweight pregnant women (MIGHT study): a randomized controlled trial—Study protocol. Contemp Clin Trials. (2018) 70:35–40. doi: 10.1016/j.cct.2018.05.007
31. Ministry of Health Control. Chilean Ministry of Health Departamento Ciclo Vital División Prevención y Control de Enfermedades Subsecretaría de Salud Pública. Manual de atención personalizada en el proceso reproductivo. Santiago (2008).
32. Borrescio-Higa F, Valdés N. Publicly insured caesarean sections in private hospitals: a repeated cross-sectional analysis in Chile. BMJ Open. (2019) 9:1–7. doi: 10.1136/bmjopen-2018-024241
33. Conway JM, Ingwersen LA, Moshfegh AJ. Accuracy of dietary recall using the USDA five-step multiple-pass method in men: an observational validation study. J Am Diet Assoc. (2004) 104:595–603. doi: 10.1016/j.jada.2004.01.007
34. USDA. Agricultural Research Service USDA National Nutrient Database for Standard Reference, Release 24. Nutrient Data Laboratory. (2011). Available online at: /ba/bhnrc/ndl
35. Schmidt-Hebbel H, Pennacchiotti I, Masson L MM. Chilean Table of Foods Chemical Composition. Santiago: Facultad de Ciencias Quimicas y Farmaceuticas, Universidad de Chile (1992).
36. Hawkes C, Jewell J, Allen K. A food policy package for healthy diets and the prevention of obesity and diet-related non-communicable diseases: the NOURISHING framework. Obes Rev. (2013) 14:159–68. doi: 10.1111/obr.12098
37. Kanter R, Reyes M, Corvalań C. Photographic methods for measuring packaged food and beverage products in supermarkets. Curr Dev Nutr. (2017) 1:e001016. doi: 10.3945/cdn.117.001016
38. Oxford U. of Co-SPACE study Parent & Adolescent Survey Items. Oxford: University of Oxford (2020).
39. World Health Organization. Regional Office for Europe. Survey Tool and Guidance: Rapid, Simple, Flexible Behavioural Insights on COVID-19. Copenhagen (2020).
40. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
41. Shulman HB, D'Angelo D V, Harrison L, Smith RA, Warner L. The pregnancy risk assessment monitoring system (PRAMS): overview of design and methodology. Am J Public Health. (2018) 108:1305–13. doi: 10.2105/AJPH.2018.304563
42. Nord M. Introduction to Item Response Theory applied to Food Security Measurement: Basic Concepts, Parameters, and Statistics. Rome: FAO (2014).
43. Ellis KJ, Yao M, Shypailo RJ, Urlando A, Wong WW, Heird WC. Body-composition assessment in infancy: air-displacement plethysmography compared with a reference 4-compartment model. Am J Clin Nutr. (2007) 85:90–5. doi: 10.1093/ajcn/85.1.90
44. WHO UNICEF. Indicators for Assessing Infant and Young Child Feeding Practices. Vol. WHA55 A55/, World Health Organization and the United Nations Children's Fund (UNICEF) (2021). 19 p. Available online at: http://apps.who.int/iris/bitstream/handle/10665/44306/9789241599290_eng.pdf?sequence=1%0Ahttp://whqlibdoc.who.int/publications/2008/9789241596664_eng.pdf%5Cnhttp://www.unicef.org/programme/breastfeeding/innocenti.htm%5Cnhttp://innocenti15.net/declaration (accessed June 20, 2022).
45. Shepherd JA, Herve L, Landau J, Fan B, Kerlikowske K, Cummings SR. Clinical comparison of a novel breast DXA technique to mammographic density. Med Phys. (2006) 33:1490–8. doi: 10.1118/1.2193691
Keywords: pregnancy, nutrition, COVID-19, maternal health, infant health, infant growth, mental health, dietary intake
Citation: Mujica-Coopman MF, Corvalán C, Flores M and Garmendia ML (2022) The Chilean Maternal-Infant Cohort Study-II in the COVID-19 Era: A Study Protocol. Front. Public Health 10:904668. doi: 10.3389/fpubh.2022.904668
Received: 25 March 2022; Accepted: 22 June 2022;
Published: 14 July 2022.
Edited by:
Siyan Yi, National University of Singapore, SingaporeReviewed by:
Bárbara Angel, Universidad de Chile, ChileCopyright © 2022 Mujica-Coopman, Corvalán, Flores and Garmendia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Luisa Garmendia, bWdhcm1lbmRpYUBpbnRhLnVjaGlsZS5jbA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.