 Cheryl Dellasega
Cheryl Dellasega Jane-Frances Aruma2
Jane-Frances Aruma2 Doerthe A. Andreae
Doerthe A. Andreae
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 05 July 2022
Sec. Public Health Policy
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.902294
This article is part of the Research Topic Women in Science: Public Health Policy 2021 View all 7 articles
Background: Patient bias and prejudice directed against physicians from diverse backgrounds is a frequent occurrence in healthcare. Female physicians have long experienced discrimination in the healthcare system based on their gender alone. The dynamic known as Patient Prejudice toward Providers (PPtP) is disproportionately affecting female physicians because it is frequently compounded by sexism.
Aim: The goal of this study was to explore the impact of PPtP on female resident and attending physicians.
Methods: Using transcribed one-on-one interviews from a larger study of PPtP affecting resident and attending physicians, ten interviews with female physicians (resident and attending) from diverse ethnic backgrounds and countries of training at a large academic medical center were analyzed. The authors independently reviewed the interviews using an iterative process within and across interviews to inductively identify repeating words, phrases, and concepts relevant to the study aim.
Results: Demographics of the ten participants included age (mean 34.6 years), ethnicity (6 Asian, 2 Hispanic, 2 African), and country of training (10% IMG vs. 90% US trained). Four of the interviewees were residents and six were attendings. Themes that emerged from the analysis included experiencing “A Gendered Continuum of Abuse,” “Establishing a Higher Standard of Competency,” “Overcoming the Stereotype of the White Male Physician,” “The Physicality of Self Identity,” and “The Need to be Protective of Minoritized Trainees.” All participants agreed that these perceptions created an adverse environment at the workplace and impacted on patient care.
Conclusions: Discrimination of physicians based on their gender or their race/ethnicity has been reported. This study highlights the compounded effects of patient prejudice on female minoritized physicians. Organizations and individuals should identify and implement strategies to address the impact of PPtP and sexism in order to create an environment where all women can thrive professionally.
Inequities have existed but gone unrecognized or unacknowledged within the American medical system for a very long time. In recent years, research has focused on suboptimal care provided to minoritized patients due to implicit bias within the health care system. Implicit bias, defined as unconscious associations and judgements that influence social behavior (1) may commonly include prejudice based on skin color, ethnicity, immigrant status, religion and gender (2).
Prejudice from providers toward patients is not the only form of bias that exists in the healthcare setting. A negative dynamic of prejudice and bias from patients and their families (PPtP, Patient Prejudice toward Providers) directed toward minoritized health care workers in the health care system in general has been documented in case reports and research studies (3, 4). PPtP arise when patients interact with providers whose perceived identity (e.g., gender identity, race, ethnicity) does not match their notion of an effective provider (5). PPtP can range from demeaning comments to outright refusal of care (6).
The increasing frequency of PPtP also at academic medical centers is important to document, especially where a diverse body of healthcare providers is providing care in less diverse settings. These occurrences pose a psychological toll on trainees, undermine learning opportunities, and may result in suboptimal patient care (5–7).
PPtP has a significant impact on the career and wellbeing of the affected physicians. Minoritized providers are more likely to experience these prejudices, and anecdotal reports highlight that these events are painful and emotional (6, 8–14). Importantly, these experiences compound over the course of a career, resulting in a high rate of burnout (6).
Retention rates of minoritized faculty in academic institutions are lower compared to white counterparts and Black assistant professors have the lowest promotion rates (15). Minoritized physicians receive the least NIH research funding (16, 17) and stark income differences between Black and white male physicians exist (18).
Sexism in medicine has been present since the first women pursued education as physicians (19, 20). According to the AAMC's Physician Specialty Data Reports, the percentage of women in the physician workforce has risen from 28.3% in 2007 to 36.3% in 2020. Despite this steady rise, bias based on gender, as well as sexism against women in medicine has continued to be rampant (21).
While women currently constitute over half of medical school students (21, 22), they continue to occupy fewer leadership positions after graduation (23–25) and are more likely to leave the profession than their male counterparts (26–28). Female physicians continue to be underrepresented in specialties that offer higher incomes and prestige (OECD, 2021). Implicit bias within the healthcare system against female physicians in general and minoritized female physicians in specific is affecting wellbeing and career advancement on many levels (29). This is being reflected in measurable outcomes like lower incomes of female vs. male physicians for the same work (18, 30) but also less tangible measures like perceived lack of support and respect from faculty reported by minoritized female students (31).
Biases against women in medicine, especially minoritized female physicians, may also be perpetrated by patients. As the physician workforce is becoming increasingly more diverse, patients are more likely to encounter physicians that may not conform to certain pre-conceived notions of what a physician should look like, leading some patients to react with biased behavior in response to such encounters. Despite this being the lived experience of many minoritized female physicians, there is a paucity of scholarship on these events. A few anecdotal reports suggest that women of color or from different countries of origin are at special risk to prejudiced behaviors from patients and male minoritized physicians have reflected on the additional hurdles their female minoritized colleagues face (unpublished results, DAA and CD). In addition to the discrimination female physicians experienced from their patients and their families many report the important role of colleagues, supervisors and the institution in responding to these incidents.
The lack of data on the dimensions of these encounters makes it challenging to create policies or training programs to address.
Institutional policies to support trainees, faculty, and staff in managing PPtP is critical (32). More specifically, academic medical centers need data on the nuances of gendered PPtP, how trainees respond to these behaviors, and what institutional factors influence their response to these incidents.
It was the purpose of this research to explore the gendered impact of PPtP on female resident and attending physicians. A qualitative design was chosen because it captures details of lived experiences that surveys do not; that is, it “considers why individuals think or behave the way that they do and how they come to understand these complex thoughts and actions within their lives.”
To obtain rich data on reactions, attitudes and beliefs, a phenomenological framework was developed to capture the lived experiencing of a group of individuals (participants) around a specific phenomenon, (in this case, PPtP) (33, 34).
To insure rigor and trustworthiness, the Consolidated Criteria for Reporting Qualitative Research (COREQ) was used (35).
The investigators consisted of one physician researcher who also is an International Medical Graduate and Immigrant to the US (DAA), a faculty researcher with expertise in qualitative methods (CD) and four first- and second-year medical students who received 4 h of training on interviewing skills. All members of the team were female and three came from minoritized backgrounds.
After receiving IRB approval, fliers were circulated to clinical and educational departments within an academic medical center. Additionally, word-of-mouth and snowballing were used to recruit the final sample of 11 resident physicians and 15 attending physicians .6 of the residents and 1 of the attending physicians 2 who volunteered did not schedule interviews due to a lack of time. Interviews with the 10 female physicians of the larger study (4 resident and 6 attendings) were analyzed separately for this study. Data on the resident sample has been published elsewhere (3). The participants self-identified as minoritized by virtue of their ethnicity, country of origin, or religious background. All physicians who volunteered to participate were currently employed within the same health system, although some of their reported experiences with PPtP occurred at other institutions. Prior to beginning each interview, basic demographic data was collected from each participant. For a description of the sample, see Table 1.
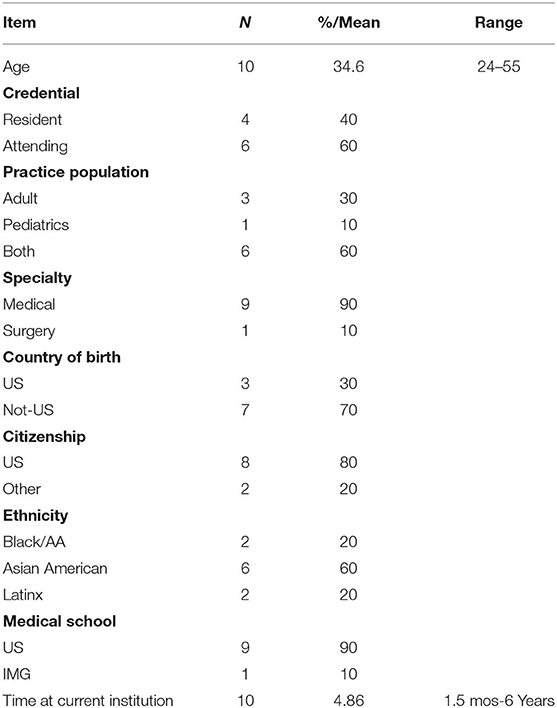
Table 1. Demographics.
Interviews were scheduled at a time and place convenient to participants. Prior to Covid, the research assistants met with interviewees in a quiet private space where they would not be interrupted or overheard. During the Covid pandemic, zoom interviews were used, again at a time of the participant's choosing and in a space that ensured confidentiality and privacy.
Each participant was interviewed once, with interviews lasting, on average, 60 min. All interviews were taped, stored in a secure location and transcribed from the audio-file including pauses and emphases.
An 11-question interview guide (see Appendix A) was developed for use in a preliminary study of PPtP among resident physicians. The questions were developed based on a review of the scholarly literature, input from experts, and discussions with individuals who identified as minoritized providers.
Data saturation, which was defined as the point when additional interviews collect no new themes or information needed to address the research question, was reached after 11 interviews for resident data and 15 interviews for physician data (36). Our sample size is within range compared to the existing literature reporting that within the first six interviews most themes are reported (37). Our resident sample size was smaller as the residents represented a more homogeneous group, similar in age and training stages. No repeat interviews were offered.
The co-investigators (DAA, CD) reviewed each transcript separately, reviewing within and across interviews for repeating words, concepts and phrases that captured the lived experience of females who had been in situations of PPtP. Once the independent analysis had been performed, the investigators met to further analyze data relevant to participant experiences.
Data were merged into categories and then five themes that emerged from the data. The Kappa coefficient of agreement between the investigators was 0.88. After the five themes were identified, no new themes occurred and the team returned to the data in order to identify exemplar statements that best illustrated (and confirmed) the themes. Finally, validation of themes through independent reviewers (NS, JA) was conducted. Participants did not review and comment on extracted themes.
The 10 female interviewees ranged in age from 24 to 55 years with a mean age of 34.6 years .7 (70%) of the interviewees were born outside the United States, but 8 (80%) were US citizens. The self-reported race/ethnicity was 2 (20%) African-American, 6 (60%) Asian-American and 2 (20%) Latinx. All, but one participant had attended medical school in the United States .4 interviewees were in residency training and 6 participants were attending physicians. The majority of participants, 6 (60%), treated both pediatric and adult patients in their daily practice. One participant treated exclusively pediatric patients and 3 (30%) treated adult patients only. One interviewee reported working in an exclusively surgical specialty .9 (90%) of the interviewees were training or working in a medical specialty.
For details please refer to Table 1.
Five themes emerged from the data and are described in Table 2.
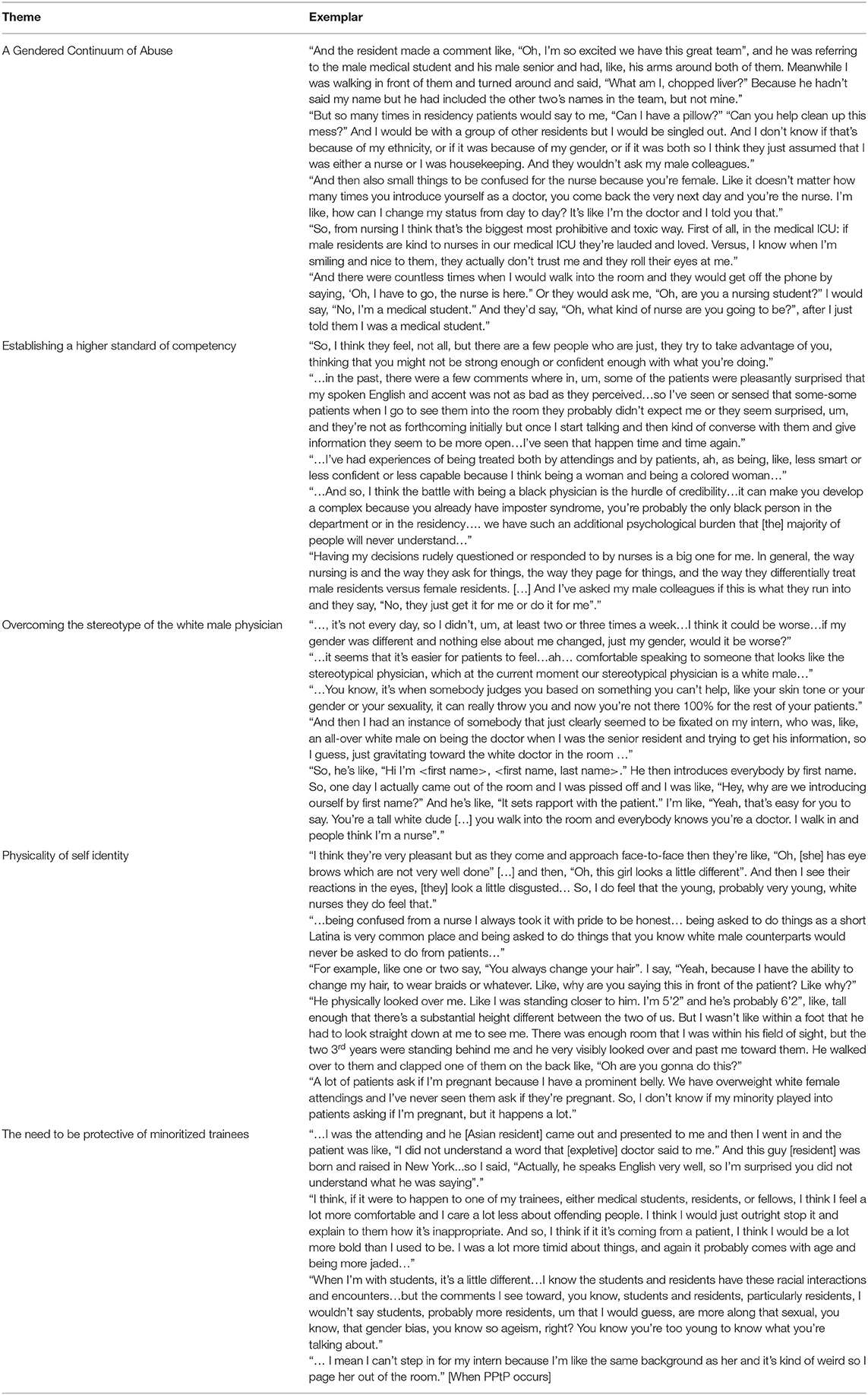
Table 2. Thematic analysis.
Themes that emerged from the analysis included experiencing the following:
Many of the behaviors interviewees described were covert, such as ignoring, undermining, negating or excluding the Female Medical Doctor of Color (FMDOC). Other more overt behaviors included refusing care from the FMDOC or commenting on appearance. Often, these PPtP behaviors occurred when there were men in the room of lesser status than the female resident or physician. Another overt behavior which was pervasive was being mistaken for a nurse (mentioned 9 times) or ancillary or other personnel. It was observed that minoritized male physicians were not treated in a similar fashion.
These behaviors generated anxiety for women, who anticipated mistreatment. In addition to being targeted by sexist comments, they were also aware of their minority status as a possible source of discrimination. In comparing the female resident with the female attending physician perspective, the perception of abuse did not stop after formal training ended but may have a diminished impact over time.
The double threat of being female and from a minority background continued to place interviewees in a position of dealing with prejudice and bias from patients and sometimes coworkers who felt they were inferior because of both their gender and background. This manifested as challenging decisions, assuming incompetence, and increased pressure to justify medical decisions and actions, Comments suggested that participants sensed they were being held to a higher standard than their male counterparts.
One pervasive theme was the assumption by both patients and providers that the only individuals who could be doctors were white males. In some ways, this may relate to the many complaints that female residents and attendings were often mistaken for and treated like a nurse.
With white males as the default representation of a physician, interviewees were confronted by instant facial expressions of suspicion or mistrust when they entered a patient's room. Interviewees noted how their male colleagues often failed to address sexism, even encouraging patients to call the team members by their first names which made clear identification of the individual's credentials less clear and often led to the female provider being mistaken for a nurse.
Even age presented a problem, with some interviewees reporting they were told they looked “too young” to be a physician, in addition to overt suggestions that they were also the wrong gender and skin color. When a patient rejected them overtly or covertly, participants wondered which combination of age, race, and gender led to the behavior.
In comparison with male residents and physicians who were interviewed previously (3) (and unpublished results), FMDOC were acutely aware of the way their physical experience impacted on prejudice. Skin tone, height and weight, body shape, and hair styling were all mentioned as ways patients negated their professional identity, factors that did not apply to male physicians.
The report of these exchanges rendered the women we interviewed feeling inadequate and “less than,” unlike the males we interviewed in the preliminary study (3).
FMDOC expressed an obligation or inclination to intervene on behalf of trainees similar to themselves, whom they considered as especially vulnerable to PPtP because of their status as a trainee. This support of junior minoritized physicians was reported by both attendings and senior residents. Many reported feeling an obligation to intervene based on their own experiences with PPtP where they were unsupported. Due to their relatively more senior position and role, minoritized female attending physicians described feeling more confident to intervene on behalf of more junior physicians. Many still felt more difficulty responding on their own behalf.
All FMDOC in our study reported having experienced multiple situations of prejudice and discrimination from patients because of their race/ethnicity and gender. In addition to experiencing bias from patients and their families, prejudice and discrimination from colleagues and nurses has also been reported. This dynamic contributed to an adverse workplace environment and had a potential adverse effect on patient care. Thus, participants described a complex and negative situation as a consequence of their gender and race/ethnicity.
While gender inequities have existed since early societies and have persisted even though women have been more equally represented in the modern workforce (29), many female physicians report they are still treated with bias and prejudice because of their gender. This experience was multiplied and compounded for minoritized female physicians.
In our study the interviewees frequently reflected when describing negative patient encounters and wondered to what extent the discrimination was due to their gender alone or also based on their race and ethnicity.
These “gendered expectations” contribute to the significantly greater rates of burnout among female physicians (38). Our interviewees' reports of having to fulfill different expectations are reflected in the described model of patient-provider relationships that women are expected to offer more empathy and time in therapeutic relationships, leading to longer interactions and increased demands on time management. Especially the attending physicians we interviewed reflected on the significant impact this dynamic has on their careers and wellbeing. As Butkus et al. state: “Women in medicine face other challenges, including a lack of mentors, discrimination, gender bias, cultural environment of the workplace, imposter syndrome, and the need for better work–life integration” (39).
This not only impacts the provider patient relationship but many interactions between colleagues. For example as one of our interviewed residents (resident 5) described: “He physically looked over me. Like I was standing closer to him. I'm 5'2” and he's probably 6'2, “like, tall enough that there's a substantial height different between the two of us. But I wasn't like within a foot that he had to look straight down at me to see me.” Many female physicians are familiar with day to day experiences including men “talking over” female colleagues in meetings, women being addressed by their first names while men are addressed as “Doctor,” as well as women facing obstacles in promotion and being excluded from positions of leadership (40).
Some other common manifestations of sexism and inequity as experienced by women in medicine include subjection to sexist jokes in class; sexual harassment by clinicians, faculty, or patients; weaker recommendation letters than men for positions on medical school faculty; lower income than men; less recognition; tendency toward choosing lower paid medical fields; stigma associated with pregnancy especially during training and inadequacy of maternity leave options (20, 41, 42).
The experiences described by female physicians of all races and ethnicities resemble experiences described by minoritized physicians of both genders in our initial study interviews (3). However, it is noteworthy that in our original study, minoritized male physicians commented on the greater likelihood that their female counterparts would be targeted by patients more strongly and more frequently.
In our interviews many of the physicians reflected on being vulnerable to negative patient ratings and having to “overcompensate”. Kauff et al. examined ratings of 140,000 physicians on a German website for health professionals and discovered that females and physicians with a migration background (identified by foreign names) were consistently rated lower than males. They suggest that although medicine is a prestigious profession, those within who are from low status groups (women and immigrants) may be easily targeted and perceived in a negative way (43).
While our study specifically focused on prejudice and bias from patients many of the interviewees also reported being subjected to bias from other members of the health care team. Many of the situations described in our interviews were microaggressions such as looks because of a difference in dress or appearance to ignoring the physician and addressing the male physicians in the room. A meta-analysis by Filut et al. looked at workplace discrimination against physicians of color and found that prejudice was higher against Black and female physicians of color (44). Women of color faculty face significant obstacles such as promotion bias, implicit bias, financial constraint as well as unequal distribution of research non-clinical time. The promotion rate for African Americans (18.8%) and Latinos (23.5%) is less than that of whites (30.2%) when advancing from associate to full professor (45).
Schmitt et al. conducted two meta-analyses which explored the impact of perceived discrimination and found they supported a negative impact on psychological wellbeing (46). This can lead to burnout and turnover (20). For the FMDOC in our study, the experience of prejudice from the very patients they were assigned to care for had both an ethical and health impact. First, their personal wellbeing was diminished, but also, questions about continuing to provide care for a patient who exhibited negative behaviors toward you was troublesome. Interviewees reported reflecting on the ethical implications of altering care because of the patient's hostile behavior as opposed to suppressing their own wellbeing and continuing the therapeutic relationship. Some interviewees formulated their own strategies, such requesting to be paged out of the room, doing the minimal face-to-face work possible to still provide competent care, and when confronting patients about their comments, doing so with humor.
In addition to suggesting further research, Rodriguez et al. offered these strategies to support women such as the ones in our study: (1) Facilitate leadership positions to minoritized female physicians through “family-friendly” policies and mentorship programs, (2) Create cohorts through targeted funding and programs that build community through affinity groups, (3) Promote accountability through collection of data that tracks sensitive outcomes such as promotion and tenure (47).
The range of prejudice and bias expressed by patients ranged from microaggressions such as seemingly curious questions or comments to overt verbal or physical rejection, such as refusing to see a certain physician and walking out of the room.
A qualitative study conducted by Wheeler et al. (6) described some experiences of physicians with biased patient behavior. Spanning from explicit and degrading remarks to complete refusal of care, these behaviors were reported to exert challenging emotional and moral distress on both the targeted physicians and bystanders (6). Minority physicians are significantly more likely to experience this (10). A qualitative study of minority resident physicians by Osseo-Asare et al. reported that these physicians were frequently mistaken for non-medical hospital staff by patients and patients' families (48). Nearly all of our FMDOC interviewees reported incidents of being mistaken for nurses or other support staff in the hospital. Many described strategies to be perceived as the physician like avoiding certain clothes that might have the same color as the cleaning personnel or always introducing themselves with their full name and title.
These behaviors took on a unique impact for interviewees because they often involved physical appearance, just as females viewed themselves as unique in terms of their size, skin color, or country of origin.
The consequences of these prejudiced behaviors had an even greater effect during the residency years for FMDOC, who were also vulnerable due to their status as a trainee. Several of the female attending interviewees reflected back on their training years and suggested they had learned to cope with PPtP or been focused on building their practice and just ignored it and the psychological harm it causes.
Options for reacting were limited at the resident/trainee level. A cross sectional national survey of general surgery residents showed that residents who reported experience of and exposure to discrimination, abuse or harassment had increased likelihood to suffer symptoms of burnout and suicidal thoughts, when compared to their counterparts with no reported exposure to mistreatment (49). Female attendings and senior residents felt very strongly that they should use their relatively higher status and experience to protect younger trainees and lessen the negative impact of PPtP on the next generation of female minoritized physicians.
The study analyzed interviews with 10 female physicians. All participants reported a female gender identity but no additional demographic data was extracted on biologic sex vs. gender identity or LGBTQ + status. These factors could add an additional area of bias, which has been reported in the literature (50), and is an important consideration for future studies.
Additionally, although our sample size is qualitative and limited to one institution (although participants had rotated through many others), they are not generalizable. Given the homogeneity of the sample (all female, all at the same institution, and all similar in demographics), it is not surprising that themes began to emerge in the first 6 interviews, with additional interviews providing no new perspectives (37).
Finally, qualitative methods come with limitations. We choose a phenomenological approach to capture the lived experience of these FMOC because there was no existing statistical measure and our intent to gather rich, in-depth data. Since the qualitative component has been completed, we have developed a survey on PPtP which is being tested nationally for reliability.
In our preliminary study of both male and female physicians and residents, one male attending interviewee remarked, “I imagine all this is even worse for women.” The results of our analysis confirmed this. Most prominent was the struggle to overcome the stereotype, held by both patients and colleagues, that the white male doctor was still the optimal and preferred provider. Denying the female's authority or legitimacy, asking for a “different” doctor, and statements about wanting an “American” doctor impacted the majority of participants.
Staying true to one's physical appearance, culture and gender while overcoming negative stereotypes and being recognized as the physician and partner in care to build the trusting relationship with the patient remains a daily struggle. This cannot be solved by the affected physicians alone but requires strategies on the organizational level.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was reviewed by the Penn State Health Review Board and considered exempt STUDY00016826. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
CD and DA: study conception and design. CD, DA, J-FA, and NS: data collection and draft manuscript preparation. CD, DA, and NS: analysis and interpretation of results. All authors reviewed the results and approved the final version of the manuscript.
This project was funded through the Junior Faculty Development Program at Penn State 2018-2021, awarded to DA.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.902294/full#supplementary-material
1. Greenwald AG, Banaji MR. Implicit social cognition: attitudes, self-esteem, and stereotypes. Psychol Rev. (1995) 102:4–27. doi: 10.1037/0033-295X.102.1.4
2. deShazo RD, Hoesley CJ, Vickers SM. Ending racial bias in american medicine: a call for help from the AMA, NMA, AAMC, and the rest of us. Am J Med. (2021) 134:565–8. doi: 10.1016/j.amjmed.2020.11.011
3. Andreae DA, Sood N, Dellasega C. Patient prejudice towards providers (PPTP): the resident physician experience. J Medic Educ Training. (2022) 6. (in press).
4. Paul-Emile K, Smith AK, Lo B, Fernández A. Dealing with racist patients. N Engl J Med. (2016) 374:708–11. doi: 10.1056/NEJMp1514939
5. de Bourmont SS, Burra A, Nouri SS, El-Farra N, Mohottige D, Sloan C, et al. Resident physician experiences with and responses to biased patients. JAMA Netw Open. (2020) 3:e2021769. doi: 10.1001/jamanetworkopen.2020.21769
6. Wheeler M, de Bourmont S, Paul-Emile K, Pfeffinger A, McMullen A, Critchfield JM, et al. Physician and trainee experiences with patient bias. JAMA Intern Med. (2019) 179:1678–85. doi: 10.1001/jamainternmed.2019.4122
7. Mustapha T, Ho Y, Andrews JS, Cullen MJ. See no evil, hear no evil, stop no evil: institutional-level tracking to combat mistreatment of residents and fellows. J Grad Med Educ. (2019) 11:601–5. doi: 10.4300/JGME-D-19-00218.1
8. Nunez-Smith M, Curry LA, Bigby J, Berg D, Krumholz HM, Bradley EH. Impact of race on the professional lives of physicians of African descent. Ann Intern Med. (2007) 146:45–51. doi: 10.7326/0003-4819-146-1-200701020-00008
9. Frank E, Carrera JS, Stratton T, Bickel J, Nora LM. Experiences of belittlement and harassment and their correlates among medical students in the United States: longitudinal survey. BMJ. (2006) 333:682. doi: 10.1136/bmj.38924.722037.7C
10. Tedeschi B. 6 in 10 Doctors Report Abusive Remarks From Patients, and Many Get Little Help Coping With The Wounds. (2017). Available online at: https://www.statnews.com/2017/10/18/patient-prejudice-wounds-doctors/?s_campaign=medscape (accessed June 21, 2022).
11. Watson S. Credentials Don't Shield Doctors, Nurses from Bias. In: Cassoobhoy A, editor. WebMD (2017). Available online at: https://www.webmd.com/a-to-z-guides/news/20171018/survey-patient-bias-toward-doctors-nurses# (accessed June 21, 2022).
12. Reddy S. How doctors deal with racist patients. Wall Street J. (2018). Available online at: https://www.wsj.com/articles/how-doctors-deal-with-racist-patients-1516633710 (accessed June 21, 2022).
13. Okwerekwu JA. What Happened When I Talked About What Others Ignore — Racism in Medicine. Boston: STAT News (2016).
15. Abelson JS, Wong NZ, Symer M, Eckenrode G, Watkins A, Yeo HL. Racial and ethnic disparities in promotion and retention of academic surgeons. Am J Surg. (2018) 216:678–82. doi: 10.1016/j.amjsurg.2018.07.020
16. Ginther DK, Schaffer WT, Schnell J, Masimore B, Liu F, Haak LL, et al. Race, ethnicity, and NIH research awards. Science. (2011) 333:1015–9. doi: 10.1126/science.1196783
17. Ginther DK. Reflections on race, ethnicity, and NIH research awards. Mol Biol Cell. (2022) 33:ae1. doi: 10.1091/mbc.E21-08-0403
18. Ly DP, Seabury SA, Jena AB. Differences in incomes of physicians in the United States by race and sex: observational study. BMJ. (2016) 353:i2923. doi: 10.1136/bmj.i2923
19. Wynn R. Saints and sinners: women and the practice of medicine throughout the ages. JAMA. (2000) 283:668–9. doi: 10.1001/jama.283.5.668-JMS0202-4-1
20. Joseph MM, Ahasic AM, Clark J, Templeton K. State of women in medicine: history, challenges, and the benefits of a diverse workforce. Pediatrics. (2021) 148(Suppl. 2). doi: 10.1542/peds.2021-051440C
21. File AAMD. 2019 Fall Applicant, Matriculant, and Enrollment Data Tables. (2019). Available online at: https://www.aamc.org/system/files/2019-12/2019%20AAMC%20Fall%20Applicant%2C%20Matriculant%2C%20and%20Enrollment%20Data%20Tables_0.pdf (accessed June 21, 2022).
22. Barzansky B, Etzel SI. Medical schools in the United States, 2017-2018. JAMA. (2018) 320:1042–50. doi: 10.1001/jama.2018.11679
23. Rao AD, Nicholas SE, Kachniarz B, Hu C, Redmond KJ, Deville C, et al. Association of a simulated institutional gender equity initiative with gender-based disparities in medical school faculty salaries and promotions. JAMA Netw Open. (2018) 1:e186054. doi: 10.1001/jamanetworkopen.2018.6054
24. Carr PL, Gunn CM, Kaplan SA, Raj A, Freund KM. Inadequate progress for women in academic medicine: findings from the national faculty study. J Womens Health. (2015) 24:190–9. doi: 10.1089/jwh.2014.4848
25. Khan MS, Usman MS, Siddiqi TJ, Ayub MT, Fatima K, Acob C, et al. Women in leadership positions in academic cardiology: a study of program directors and division chiefs. J Womens Health. (2019) 28:225–32. doi: 10.1089/jwh.2018.7135
26. Paturel A. Why Women Leave Medicine. AAMC. (2019). Available online at: https://www.aamc.org/news-insights/why-women-leave-medicine (accessed June 21, 2022).
27. Frank E, Zhao Z, Sen S, Guille C. Gender disparities in work and parental status among early career physicians. JAMA Netw Open. (2019) 2:e198340. doi: 10.1001/jamanetworkopen.2019.8340
28. Jolly S, Griffith KA, DeCastro R, Stewart A, Ubel P, Jagsi R. Gender differences in time spent on parenting and domestic responsibilities by high-achieving young physician-researchers. Ann Intern Med. (2014) 160:344–53. doi: 10.7326/M13-0974
29. Newman C, Templeton K, Chin EL. Inequity and women physicians: time to change millennia of societal beliefs. Perm J. (2020) 24:1–6. doi: 10.7812/TPP/20.024
30. Apaydin EA, Chen PGC, Friedberg MW. Differences in physician income by gender in a multiregion survey. J Gen Intern Med. (2018) 33:1574–81. doi: 10.1007/s11606-018-4462-2
31. Weiss J, Balasuriya L, Cramer LD, Nunez-Smith M, Genao I, Gonzalez-Colaso R, et al. Medical students' demographic characteristics and their perceptions of faculty role modeling of respect for diversity. JAMA Netw Open. (2021) 4:e2112795. doi: 10.1001/jamanetworkopen.2021.12795
32. Penn State Health a National Model for Anti-Bias-Policy Protecting Providers Penn State Health News: Penn State Health. (2017). Available online at: https://pennstatehealthnews.org/topics/penn-state-health-a-national-model-for-anti-bias-policy-protecting-providers/ (accessed June 21, 2022).
33. Korstjens I, Moser A. Series: practical guidance to qualitative research. Part 2: context, research questions and designs. Eur J Gen Pract. (2017) 23:274–9. doi: 10.1080/13814788.2017.1375090
34. Denny E, Weckesser A. Qualitative research: what it is and what it is not: study design: qualitative research. BJOG. (2019) 126:369. doi: 10.1111/1471-0528.15198
35. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
36. Guest G, Namey E, Chen M. A simple method to assess and report thematic saturation in qualitative research. PLoS ONE. (2020) 15:e0232076. doi: 10.1371/journal.pone.0232076
37. Galvin R. How many interviews are enough? Do qualitative interviews in building energy consumption research produce reliable knowledge? J Build Eng. (2015) 1:2–12. doi: 10.1016/j.jobe.2014.12.001
38. Linzer M, Harwood E. Gendered expectations: do they contribute to high burnout among female physicians? J Gen Intern Med. (2018) 33:963–5. doi: 10.1007/s11606-018-4330-0
39. Butkus R, Serchen J, Moyer DV, Bornstein SS, Hingle ST, Kane GC, et al. Achieving gender equity in physician compensation and career advancement: a position paper of the american college of physicians. Ann Intern Med. (2018) 168:721–3. doi: 10.7326/M17-3438
41. Kang SK, Kaplan S. Working toward gender diversity and inclusion in medicine: myths and solutions. Lancet. (2019) 393:579–86. doi: 10.1016/S0140-6736(18)33138-6
42. Rangel EL, Smink DS, Castillo-Angeles M, Kwakye G, Changala M, Haider AH, et al. Pregnancy and motherhood during surgical training. JAMA Surg. (2018) 153:644–52. doi: 10.1001/jamasurg.2018.0153
43. Kauff M, Anslinger J, Christ O, Niemann M, Geierhos M, Huster L. Ethnic and gender-based prejudice towards medical doctors? The relationship between physicians' ethnicity, gender, and ratings on a physician rating website. J Soc Psychol. (2021) 2021:1–9. doi: 10.1080/00224545.2021.1927944
44. Filut A, Alvarez M, Carnes M. Discrimination toward physicians of color: a systematic review. J Natl Med Assoc. (2020) 112:117–40. doi: 10.1016/j.jnma.2020.02.008
45. Francis J, Joseph V. Minority women in anesthesiology. Int Anesthesiol Clin. (2018) 56:74–95. doi: 10.1097/AIA.0000000000000198
46. Schmitt MT, Branscombe NR, Postmes T, Garcia A. The consequences of perceived discrimination for psychological well-being: a meta-analytic review. Psychol Bull. (2014) 140:921–48. doi: 10.1037/a0035754
47. Rodriguez CI, Jagsi R, Mangurian C. Rising to the challenge: strategies to support latinas and other women of color in science and medicine. Acad Med. (2021) 97:331–334. doi: 10.1097/ACM.0000000000004558
48. Osseo-Asare A, Balasuriya L, Huot SJ, Keene D, Berg D, Nunez-Smith M, et al. Minority resident physicians' views on the role of race/ethnicity in their training experiences in the workplace. JAMA Netw Open. (2018) 1:e182723. doi: 10.1001/jamanetworkopen.2018.2723
49. Hu YY, Ellis RJ, Hewitt DB, Yang AD, Cheung EO, Moskowitz JT, et al. Discrimination, abuse, harassment, and burnout in surgical residency training. N Engl J Med. (2019) 381:1741–52. doi: 10.1056/NEJMsa1903759
Keywords: minoritized providers, female physicians, patient prejudice, provider mistreatment, bias
Citation: Dellasega C, Aruma J-F, Sood N and Andreae DA (2022) The Impact of Patient Prejudice on Minoritized Female Physicians. Front. Public Health 10:902294. doi: 10.3389/fpubh.2022.902294
Received: 23 March 2022; Accepted: 10 June 2022;
Published: 05 July 2022.
Edited by:
Meghna Ranganathan, University of London, United KingdomReviewed by:
Eron Grant Manusov, The University of Texas Rio Grande Valley, United StatesCopyright © 2022 Dellasega, Aruma, Sood and Andreae. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Doerthe A. Andreae, YWRyaWFuYS5hbmRyZWFlQGhzYy51dGFoLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.