 Hao Wang
Hao Wang Peng Luo1,2*
Peng Luo1,2*
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 July 2022
Sec. Occupational Health and Safety
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.891503
This article is part of the Research Topic COVID-19: challenges, opportunities and lessons for occupational health View all 20 articles
Background: Diverse measures have been carried out worldwide to establish Alternative Care Facilities (ACFs) for different ends, such as receiving, curing or isolating patients, aiming to cope with tremendous shock in the urban medical system during the early passage of the COVID-19 epidemic. Healthcare workers always felt anxious and stressed during multiple major public health emergencies in medical facilities. Some active measures to improve healthcare workers' perceptions, such as temporary training, workflow improvement, and supplementary facilities, were proved insufficient in several past public health emergencies. Therefore, this study aims to analyze the contributing factors of the healthcare workers' perceptions of the ACFs in this pandemic, which can help find an innovative path to ensure their health, well-being and work efficiency.
Method: This paper conducted semi-structured in-depth interviews with the world's first batch of healthcare workers who have worked in ACFs through a qualitative study based on Grounded Theory. The healthcare workers interviewed from Heilongjiang, Shandong, Fujian, and Hubei provinces, have worked in one of the four different ACFs built in Wuhan. The results are obtained through the three-level codes and analyses of the interview recordings.
Results: The factors affecting the perception of healthcare workers in ACFs during the epidemic situation can be summarized into five major categories: individual characteristics, organization management, facilities and equipment, space design, and internal environment. The five major categories affecting the composition of perception can be further divided into endogenous and exogenous factors, which jointly affect the perception of healthcare workers in ACFs. Among them, individual characteristics belong to endogenous factors, which are the primary conditions, while other categories belong to exogenous factors, which are the decisive conditions.
Conclusion: This paper clarifies factors affecting the perception of healthcare workers in ACFs and analyzes the mechanism of each factor. It is posited that the passive strategies are a promising solution to protect healthcare workers' health, improve their work efficiency, and help reduce the operation stress of ACFs. We should train multidisciplinary professionals for future healthcare and enhance collaborations between healthcare workers and engineers. To sum up, this paper broadens new horizons for future research on the optimization of ACFs and finds new paths for alleviating healthcare workers' adverse perceptions of ACFs.
The scarcity of medical resources is ubiquitous worldwide, resulting from the large number of patients caused by the COVID-19 pandemic (1–5). Alternative Care Facilities (ACFs) are temporary facilities that can meet the emergency needs of medical treatment in public health emergencies to alleviate the burden of medical conditions of existing medical facilities (6, 7). Lam C, Waldhorn R, and others believe that there are several uses for ACFs: as overflow hospitals providing a full range of care; for limited supportive care for noncritical patients; as primary triage and rapid patient screening centers; for quarantine; etc. (8, 9). ACFs have played various roles in different countries and regions according to their medical system in this epidemic (10–15). For example, NHS Nightingale Hospital in the UK provides comprehensive care for patients (16), and Fangcang shelter hospitals in China mainly focus on isolation and provide limited supportive treatment (17–19). In general, ACFs are a common way for many countries to solve the shortage of medical facilities.
Perception is the human body's organization, identification, and interpretation of acquired information through the sensory system to present the information or environment (20). Relevant studies show that although people's perceived risk in a dangerous environment is not necessarily the same as the actual risk, the individual's perception will still affect their behavior (21, 22). Specifically, although healthcare workers are unrecognized in their nosocomial surroundings, their stress perception also impacts their health and work performances. For example, the sound and light in the hospitals will also affect the workers' stress and job satisfaction (23–26). Healthcare workers play critical roles in public health emergencies and provide emergency medical services to people in need (27–32). However, previous studies have shown that healthcare workers might have poor physical and mental health due to lack of support, increasing workload, fear of infection, and insufficient training, during public health emergencies like SARS and MERS (33–39). Moreover, there are also studies showing that healthcare workers in various countries face similar situations during the COVID-19 epidemic (40–45). And specific relevant researches on healthcare workers in ACFs show that their adverse perception may be exacerbated due to their maladjustment to the new environment, the limited medical resources and open space for activities, and the imbalance between the ratio of healthcare workers to patients (46–49).
Healthcare workers' perception of ACFs is the overall presentation of information generated in the working process through a series of their sensory systems. Traditionally, the point of view of medical staff has been measured by using questionnaires that monitor the satisfaction with the care received. However, the exclusive use of surveys to study overall health care quality has some weaknesses, including framing the protagonists' subjective experiences into rigid categories imposed by the researchers based on preconceived ideas (50). Thus, Grounded Theory constructs symbolic codes based on categories emerging from recorded qualitative data, which is quite different from the traditional scientific research model (51–53). Some practice researches understood nurses' experience with nursing consultations in the context of the Family Health Strategy and proposed a representative model with the open, axial and selective coding (54). There is also research into nurses' changing perceptions regarding the efforts in preparation for working in a COVID-19 ward in the rural Japanese context (55). Moreover, other researches explored the perception of entrepreneurship among nurses and developed a mid-range theory that explains the meaning and practices of entrepreneurship among nurses (56). The above researches fully show that the Grounded Theory method is feasible to comprehensively explain the factors affecting the perception of healthcare workers under specific conditions. Thus, to improve the adverse perception affecting healthcare workers' health, well-being and work efficiency during the epidemic, this paper clarifies the contributing factors to healthcare workers' perception of ACFs through the method of Grounded Theory, to find innovative improvement measures and alleviate their adverse perception.
Grounded Theory is based on investigations and analyses by returning to the phenomenon itself and avoiding presupposition by the researchers. Categories are divided via concept extraction, induction, and summary in a bottom-up way based on data collected and the relationship between various categories is further explored to establish a theoretical model to solve the research questions. Specifically speaking, research processes of the Grounded Theory can be divided into four steps: research question–data collection–data analysis–theoretical construction, among which data analysis, as the core link, is usually categorized by the three-level codes, namely open coding–axial coding–selective coding (57, 58) (Figure 1).
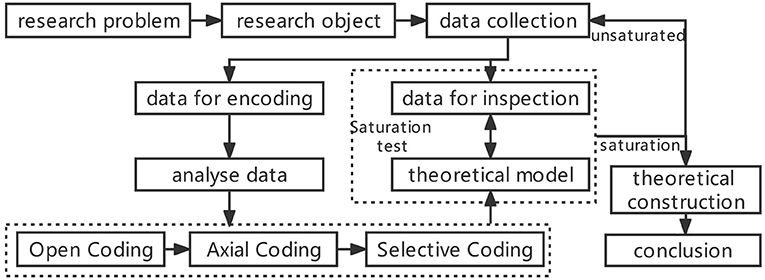
Figure 1. Grounded theory research process.
The selected participants were the first ones who worked in ACFs in the world during the epidemic in Wuhan, and thus there were no referential experiences for them. Hence, later policies and improvement measures did not affect their behaviors and perceptions.
The participants were eight healthcare workers who come from Hubei (2 participants), Heilongjiang (3 participants), Shandong (2 participants), and Fujian Provinces (1 participant) in China with an average age of 38.9 (SD = 6.9; min = 27; max = 50), including four men and four women. These participants included five nurses and three doctors with an average working seniority of 15.6 (SD = 9.0; min = 4; max = 30) with bachelor's degree (Table 1). To ensure the objectivity of the research results, the selection of participants in this study were from the four ACFs in Wuhan named Shipailing Fangcang shelter hospital (2 participants), Zhuankou Fangcang shelter hospital(3 participants), Guobo Fangcang shelter hospital (2 participants), Guanggu Fangcang shelter hospital (1 participant) with the same functions and ends in the same period.
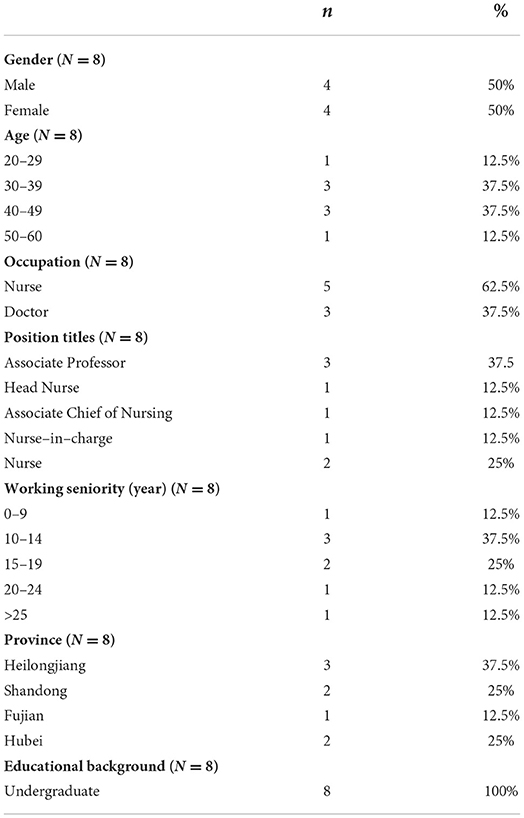
Table 1. Demographic characteristics of respondents.
Informed consent was obtained from all participants before the interview began. Participants were informed about the goals and contents of the study, privacy, and data protection and that their participation in the study was voluntary. Biological samples were not collected.
This study draws up an outline for the interview as follows. There are four parts of the interview, which are not conducted in a fixed order to avoid interrupting the interviewees.
(1) Basic information: the name of ACF, the stationed time of the healthcare workers, the number of patients, etc.;
(2) Work contents: the respondents' work division, organization and process, as well as the problems they encountered in ACFs, etc.;
(3) Perception: recognition of the respondents in different positions and at other times in ACFs from the beginning to the end;
(4) Improvement suggestions: the management, operation and layout design of the ideal ACFs from respondents' perspectives.
This study has conducted interviews either online or offline because, on the one hand, interviewees are from various medical care teams in different provinces; on the other hand, it can avoid the interactions between respondents. The critical information was recorded during the 1h to 1.5h interview. Furthermore, the respondents' personal information was not mentioned so that they could tell their actual perceptions. After the interview, the interviewers analyzed the recordings.
According to the Grounded Theory, researchers will not be able to obtain new information from the research data when the research results reach saturation (51). After analyzing the interview recordings of 8 healthcare workers, the researchers found that the interview contents of the other three could not provide any new concept, and hence results are considered saturated.
Open coding is a process of the label, conceptualizing and categorizing the similar or relevant information from the recordings of the interviews. This study is in accordance with the following procedures: labeling (analyze the recordings, sift essential information out, and label as “an”)—conceptualization (combine similar and relevant labels, and conceptualize as “aan”)–categorization (classify the conception and categorize as “An”)—open coding. In all, there are 406 labels, 53 concepts, and 27 categories after the process of open coding (Table 2).
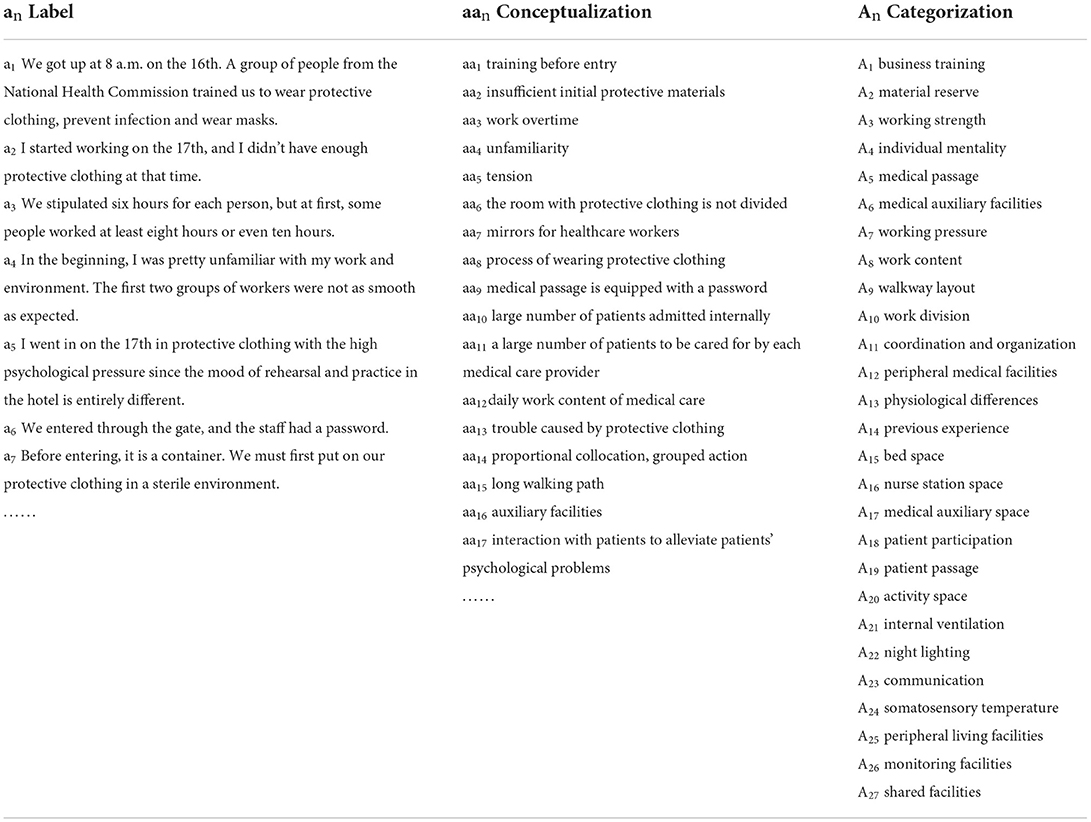
Table 2. Open coding process.
Axial coding aims to merge correlated categories, find the links among all categories, then simplify and differentiate them. In this study, the major categories are sifted out to better specify the themes of the interview recordings by merging the minor categories together. Thus, there are five major categories after axial coding, namely “individual characteristics,” “organization and management,” “space design,” “internal environment” and “facilities and equipment” (Table 3).
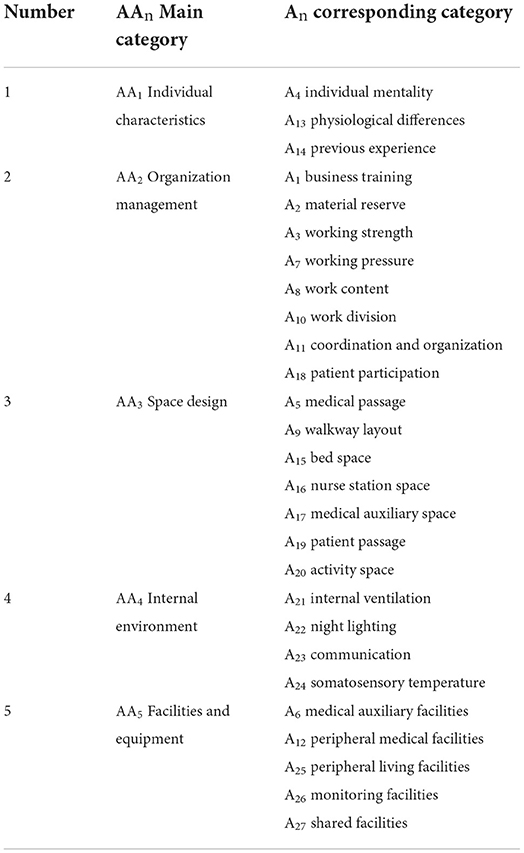
Table 3. Main category and corresponding category.
Selective coding aims to sift core categories from the major categories. Core categories are used to clarify the interrelation of the major ones for an integral logic to better clarify the interrelation among the major categories. It is posited that “space design” should be selected as the core category. Specifically, based on the perception of the healthcare workers in ACFs, this study takes the five major categories and other minor ones and some related conceptions into consideration, which shows that “space design” can be used to explain the correlation among the major categories. The integral logic among the five categories is as follows: because of the COVID-19 epidemic, healthcare workers with distinguishing “individual characteristics” had to work in ACFs that were not well-equipped. While the original building structures constrained the “space design” of the ACFs, the “internal environment” was relatively deficient. The inadequacies of the “space design” of the ACFs were balanced mainly through “organization management” and together with some “facilities and equipment” to improve the health, well-being and work efficiency of the healthcare workers (Figure 2).
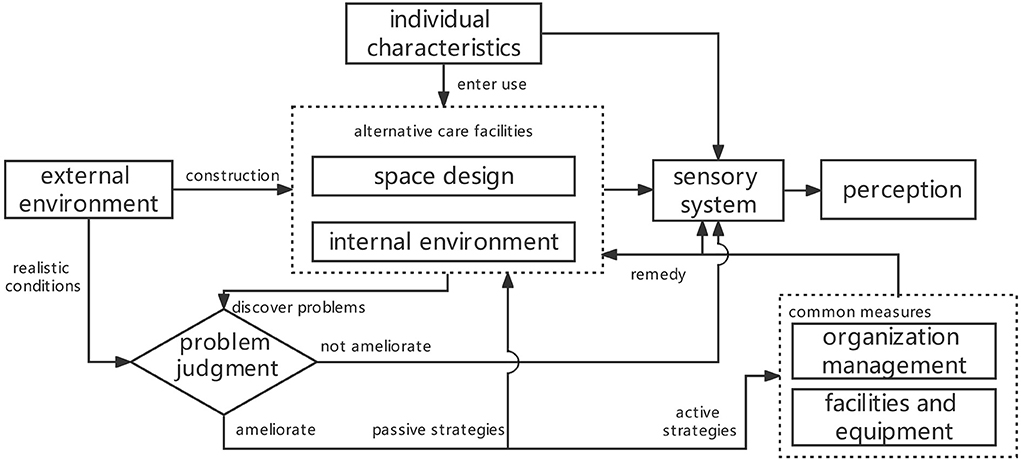
Figure 2. Interaction mechanism between main categories.
The “individual characteristics” are essential to all perceptions of the healthcare workers after clarifying the categories. While the facility and operation conditions of the ACFs were decisive factors for the final perception of healthcare workers. The “facility conditions”, i.e. space and environment of the ACFs, affect the healthcare workers' perceptional system as soon as they begin to work in the ACFs. However, the “operation conditions”, i.e. “organization management” and “facilities and equipment,” plays decisive roles in the perception of the healthcare workers. The space of ACFs is essential to healthcare workers' activities, while the environment of the buildings is rather critical to their perception. Both of them had potential impacts on the healthcare workers, although they usually seemed to be unrecognized in the space and environment (17). However, despite the limited conditions during the epidemic, some counterbalanced measures were carried out to optimize the “operation conditions” of the ACFs, aiming to improve the workers' perceptions. Primary measures were to improve management capacity and secondary ones to strengthen support facilities (Table 4).
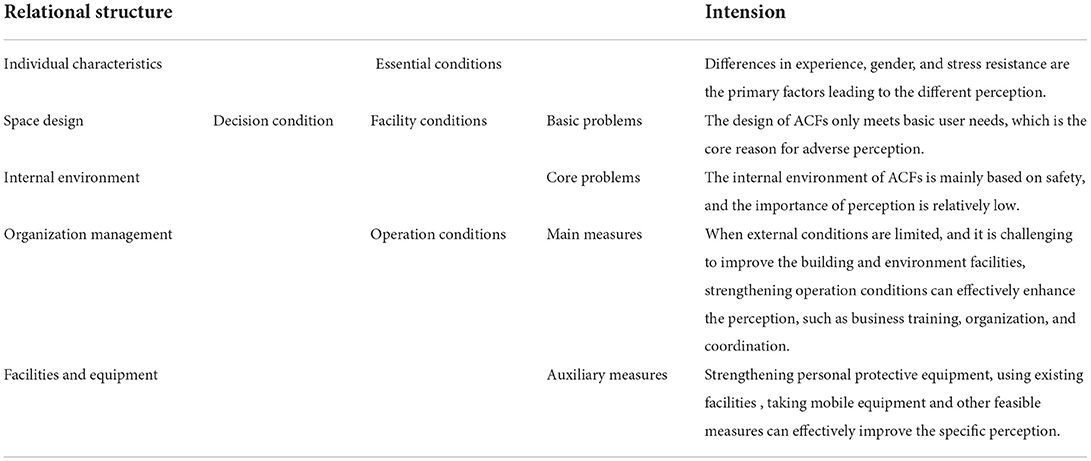
Table 4. Relational structure of the main category.
The relational structure of the perception model for the healthcare workers in ACFs is developed based on the interactions among the categories. According to this structure, the factors affecting the healthcare workers' perceptions can be further divided into two groups that are endogenous factors (individual characteristics) and exogenous factors (organization management, space design, internal environment and facilities and equipment). As endogenous factors are composed of individual characteristics, it is regarded as the basis of the workers' perceptions and the exogenous ones play rather critical roles. Both of them are merged together by the sensory system of the healthcare workers and then the primary perception is produced. The improvement measures that counter healthcare workers' adverse perceptions can be further classified into two parts: active and passive strategies (Figure 3).
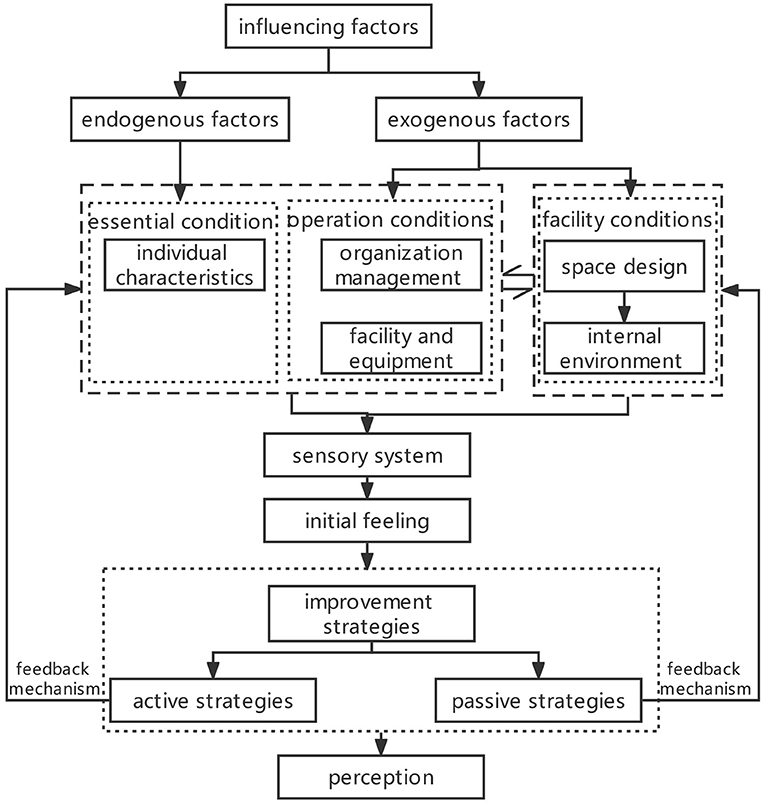
Figure 3. Perception models of healthcare workers in ACFs.
The passive design strategy improves the performance of the building through the optimization of the building design, like the appearance and space design of the building and the selection of building materials. The active strategy aims to enhance building performance by artificial supplementary measures, such as air-conditioners and the operations of the buildings. The design of a hospital is usually improved by analyzing the workflow and needs of healthcare workers, by which the designer can ensure better user perception for the healthcare workers via promoting the design of space and environment of the buildings. ACFs are some of the most promising solutions to the pressing health care needs under disaster situations. During the COVID-19 epidemic, previous studies show that the environment of the ACFs not only has adverse impacts on the patients but requires healthcare workers to adjust themselves to the new surroundings (59). To improve healthcare workers' perceptions of ACFs during the epidemic, administrators of ACFs focus on active measures by a multi-tiered care model, PPE packs, emergency medical staff training, and psychological crisis intervention (49, 60–62). Recently, there have been studies on passive measures concerning more about the safety of the buildings' functional layout and internal environment (63–66). Although security is foremost in the ACFs, it is also essential to consider the healthcare workers' perceptions, which may reduce operating costs and active remedial measures. However, previous studies seldom explained the contributing factors of ACFs' design affecting the perception of healthcare workers. Only some showed that buildings, like residential living situations, impacted people's physical and mental well-being during the epidemic (67–69). Some analyzed the effect of housing built-environments on personal depression and anxieties (70, 71). Also, studies using multiple regression analyses show that the better the building design is, the fewer stress people may feel and the more active feedback the user will get (72). Passive design measures, such as function division, interior design, socialization approaches to design and positive distraction of light and sound can improve people's behaviors and emotions, reduce pressure and anxiety, and enhance users' perception and satisfaction (73).
Because healthcare environments are one of the most complex and demanding fields of work, an interdisciplinary solution is needed to achieve the goal of passively improving the healthcare environment. Giuliano K. K. and other researchers proposed that a nurse-engineer partnership is one of the most promising solutions to health care issues. Although the nurse-engineer partnership is faced with many barriers, it is encouraging to empower both nurses and engineers to create collaborations. According to Giuliano, finding a way for engineers to be trained in nursing and nurses to enter engineering are strategies helpful to developing infrastructure for health care innovation (74). For example, Brambilla and other researchers proposed the massive vaccination center layouts with the passive strategies, which is not only address safety by reducing cross-contamination risks, and improve the process efficiency but also ensure healthcare workers' well-being by the designs of resting spaces, short distances, and the correct sizing of space for the different activities (75). Meanwhile, they developed an easy-to-use checklist divided into two sections containing general and specific structural requirements to ensure the different activities' quality, safety, and efficiency (76). In addition, relevant researches also show that it is necessary to strengthen the synergy between design and health and training multidisciplinary professionals for future healthcare (77, 78).
The above discussions show that building characteristics affect personal perceptions during the pandemic, and the optimization of the built facilities can improve healthcare workers' health and well-being. Therefore, it is necessary to strengthen the emerging multidisciplinary education, which can develop the nurse-engineer partnership, to excavate passive improvement strategies for seeking more optimization measures for the building design of the ACFs. Specifically, such passive measures include the number of beds in each care unit in the bed area, the layout of healthcare workers passage and patient passage, the openness and accessibility of nurse stations, and the position of medical apparatus and instruments. The optimization of the building design and environment of the ACFs can be realized by the passive strategies, reducing the healthcare workers' adverse perceptions and the operating costs and active measures.
The research aims to analyze the contributing factors to the healthcare workers' perceptions of the ACFs in this pandemic. Analyzing the actual narration of healthcare workers can avoid presupposition by the researchers through a qualitative study based on Grounded Theory. Eventually, there are five factors affecting the healthcare workers' perceptions which can be further divided into endogenous factors and exogenous factors. By interpreting the interactions among the factors and perception of healthcare workers, the passive strategies are realized to protect people's health and well-being in ACFs. In all, the research broadens new horizons for future research on the optimization of ACFs. It is also suggested that the emerging multidisciplinary education should be strengthened, especially the nurse-engineer partnership. Furthermore, exploring the measures of the rebuilding facilities as many as possible can help improve healthcare workers' perceptions and protect the health and well-being of people in ACFs.
Although this paper proposed a way to optimize the healthcare workers' perception of ACFs based on passive design, it did not explore specific measures which need further research. In addition, the healthcare workers interviewed are all from China. As mentioned above, the ACFs have played various roles in different countries during the epidemic (14–16), which leads to the differences in the responsibilities and working environment of the healthcare workers. Meanwhile, the interviewees come from other provinces to fight the epidemic in Wuhan, which means that their adverse perceptions may not be influenced by the fear that their families could be infected by the virus, as shown by some studies (44). Limitations as such may constrain the feasibility of this research and lead to differences in some details of the factors of perception in ACFs in different regions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
HW is responsible for interview data collection, article writing, and post revision. PL is responsible for interview design and article content inspection. YW is responsible for interview data collection and post revision. XZ is responsible for post revision. All authors contributed to the article and approved the submitted version.
This research was funded by the National Natural Science Foundation of China, grant number 52078156.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hui DS, I Azhar E, Madani TA, Ntoumi F, Kock R, Dar O, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. (2020) 91:264–66. doi: 10.1016/j.ijid.2020.01.009
2. Gaofeng Yin H, Wang J, Nicholas S, Maitland E. The COVID-19 Run on medical resources in Wuhan China: causes, consequences and lessons healthcare. MDPI. (2021) 9:1362. doi: 10.3390/healthcare9101362
3. Mahendradhata NiL Y, Tirtabayu Hasri E, Arifi MD, Montesori Siahaan RG, Solikha DA, Ali PB. The capacity of the Indonesian healthcare system to respond to COVID-19. Front Public Health. (2021) 9:887. doi: 10.3389/fpubh.2021.649819
4. Van Beusekom M. Doctors: COVID-19 pushing Italian ICUs toward collapse. Center for Infectious Disease Research Policy (2020). Available online at https://www.cidrap.umn.edu/news-perspective/2020/03/doctors-covid-19-pushing-italian-icus-toward-collapse. (accessed on May 12, 2022).
5. Verhagen MD, Brazel DM, Dowd JP, Kashnitsky I, Mills MC. Mapping hospital demand: demographics, spatial variation, and the risk of “hospital deserts” during COVID-19 in England and Wales OSF Preprints. (2020).
6. U.S. Army Corps of Engineers. Alternate Care Sites (ACS). Available online at: https://www.usace.army.mil/Coronavirus/Alternate-Care-Sites/ (accessed on 4 May 2022).
7. Federal Healthcare Resilience Task Force Alternate Care Site Toolkit Second Edition. Available online at: https://files.asprtracie.hhs.gov/documents/acs-toolkit-ed1-20200330-1022.pdf. (accessed on 4 May 2022).
8. Ri CL, Toner E, Thomas V, Inglesby, Tara O'Toole. The prospect of using alternative medical care facilities in an influenza pandemic. Biosecur Bioterror. (2006) 4:384–90. doi: 10.1089/bsp.2006.4.384
9. Waldhorn R. What role can alternative care facilities play in an influenza pandemic? Biosecurity and Bioterrorism: Biodefense Strategy. Practice Sci. (2008) 6:357–59. doi: 10.1089/bsp.2008.1029
10. Reilly MJ, Markenson DS, Amler S. Designing alternate care sites for pandemics and public health emergencies. Prehospital Disaster Med. (2009) 24(S1):s63. doi: 10.1017/S1049023X00054406
11. Alexander Kaysin, Diana N. Carvajal, Charles W. Callahan. The role of alternate care sites in health system responsiveness to COVID-19. Am J Public Health. (2020)110:1362–64. doi: 10.2105/AJPH.2020.305838
12. Rafael Castro Delgado P. Eduardo Pintado García, Iñigo Marañón Zabalza, Manuel Vallina-Victorero Vázquez, Rodrigo Escribano Balín. Alternate care sites for COVID-19 patients: experience from the H144 hospital of the health service of the principality of Asturias, Spain. Prehosp Disaster Med. (2021) 36:774–81. doi: 10.1017/S1049023X21001102
13. Naganathan S, Meehan-Coussee K, Scott Pasichow MD, et al. From concerts to COVID: transforming the RI convention center into an alternate hospital site in under a month. Rhode Island Med J. (2020) 103:8–13.
14. Gregg S., Meyer, Bonnie B., Blanchfield, Richard M. J., Bohmer, James Mountford W. Craig Vanderwagen. Alternative Care Sites for the Covid-19 Pandemic: the Early Us and Uk Experience. NEJM Catalyst Innovations in Care Delivery. (2020)
15. Yuan J. Inside the Javits Center: New York's Militarized, Makeshift Hospital. (2020). Available online: https://www.washingtonpost.com/national/javits-center-coronavirus-field-hospital/2020/04/04/50bdbf32-75b2-11ea-87da-77a8136c1a6d_story.html. (accessed on 10 May 2022).
16. Alastair G., Proudfoot, Ben O'Brien, Richard Schilling, Doug W. Gould, Alan McGlennan Rapid establishment of a COVID-19 critical care unit in a convention centre: the Nightingale Hospital London experience Intensive. Care Med. (2021) 47:349–51. doi: 10.1007/s00134-020-06334-6
17. Ji K-WW, Song X-X, Huang J, Wang H, Wua X-L, et al. Fangcang shelter hospitals are a One Health approach for responding to the COVID-19 outbreak in Wuhan, China. One Health. (2020) 10:100167. doi: 10.1016/j.onehlt.2020.100167
18. Simiao, Chen Z., Juntao Yang, Jian Wang, Xiaohui Zhai, Till Bärnighausen, ChenWang. Fangcang shelter hospitals: a novel concept for responding to public health emergencies. Lancet. (2020) 395:1305–14. doi: 10.1016/S0140-6736(20)30744-3
19. Lei Shang J. Bin Cao. Fangcang shelter hospitals in COVID-19 pandemic: the practice and its significance. Clin Microbiol Infect. (2020) 26:976–8. doi: 10.1016/j.cmi.2020.04.038
20. Schacter D, Gilbert D, Wegner D, et al. Psychology: European Edition. London: Macmillan International Higher Education. (2011).
21. Hu DY, Li W, Han Q, Zhang X, Zhu LX, Wei Wan S, et al. Frontline nurses' burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: a large-scale cross-sectional study. EClinical Med. (2020) 24:100424. doi: 10.1016/j.eclinm.2020.100424
22. Jafree R, Zakar R, Rafiq N, Javed A, Durrani RR, Khadija Burhan S, et al. WhatsApp-Delivered intervention for continued learning for nurses in Pakistan during the COVID-19 pandemic: results of a randomized-controlled trial. Front Public Health. (2022) 114:739761. doi: 10.3389/fpubh.2022.739761
23. Diane Applebaum S, Fiedler N, Osinubi O, Robson M. The impact of environmental factors on nursing stress, job satisfaction, and turnover intention. J Nurs. Administration. (2010) 40:323. doi: 10.1097/NNA.0b013e3181e9393b
24. Timothy R. Jordan, Jagdish Khubchandani, Michael Wiblishauser. The impact of perceived stress and coping adequacy on the health of nurses: a pilot investigation. Nurs Res Pract. (2016) 2016:5843256. doi: 10.1155/2016/5843256
25. Beatriz M, Martínez-Zaragoza F, Benavides-Gil G. Stress in nurses: The 100 top-cited papers published in nursing journals. J Advanced Nurs. (2018) 74:1488–504. doi: 10.1111/jan.13566
26. Kathleen Connellan M, Riggs D, Due C, Reinschmidt A, Mustillo L. Stressed spaces: mental health and architecture HERD: health environments. Res Design J. (2013) 6:127–68. doi: 10.1177/193758671300600408
27. Christopher S., Kim, James C., Pile, Marie M, Lozon, William M, Wilkerson, Carrie M, Wright, et al. Role of hospitalists in an offsite alternate care center (ACC) for pandemic flu. J Hosp Med. (2009) 4:546–9. doi: 10.1002/jhm.509
28. Association Association of Public Health Nurses Public Health Preparedness Committee. The role of the public health nurse in disaster preparedness, response, and recovery: A position paper. (2013). Available online at: https://www.naccho.org/uploads/blog/nacchopreparedness/APHN_Role-of-PHN-in-Disaster-PRR_FINALJan14.pdf (accessed on 10 May 2022).
29. Veenema TG, Griffin A, Gable AR, MacIntyre L, Simons RN, Couig MP, et al. Nurses as leaders in disaster preparedness and response—a call to action. J Nurs Scholarsh. (2016) 48:187–200. doi: 10.1111/jnu.12198
30. James C. Pile, Steven M. Gordon. Pandemic influenza and the hospitalist: apocalypse when? J Hosp Med. (2006)1:118–123. doi: 10.1002/jhm.81
31. Conz CA, Braga VAS, Vasconcelos R, Machado FHRDS, de Jesus MCP, Merighi MAB. Role of nurses in a field hospital aimed at patients with Covid-19. Rev Esc Enferm USP. (2021) 42:e20210194. doi: 10.1590/1983-1447.2021.20200378
32. Garcia-Castrillo L, Petrino R, Leach R, Dodt C, Behringer W, Khoury A, et al. European Society For Emergency Medicine position paper on emergency medical systems' response to COVID-19. Eur J Emerg Med. (2020):27:174–77. doi: 10.1097/MEJ.0000000000000701
33. Maunder RG, Lancee WJ, Balderson KE, Bennett JP, Borgundvaag B, Evans S, et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak Emerging infectious disease. Emerg Infect Dis. (2006) 12:1924. doi: 10.3201/eid1212.060584
34. Marjanovic Z, Greenglass ER, Coffey S. The relevance of psychosocial variables and working conditions in predicting nurses' coping strategies during the SARS crisis: an online questionnaire survey. Int J Nurs Stud. (2007) 44:991–998. doi: 10.1016/j.ijnurstu.2006.02.012
35. Shwu-Hua Lee Y, Su-YJ, Lee HL, Lin Y-H, Chao CC. Facing SARS: psychological impacts on SARS team nurses and psychiatric services in a Taiwan general hospital. Gen Hosp Psychiatr. (2005) 27:352–8. doi: 10.1016/j.genhosppsych.2005.04.007
36. William J., Lancee, Robert G., Maunder, David S. Goldbloom. Prevalence of psychiatric disorders among Toronto hospital workers one to two years after the SARS outbreak. Psychiatr Services. (2008) 59:91–5. doi: 10.1176/ps.2008.59.1.91
37. Chan AO, Huak CY. Psychological impact of the 2003 severe acute respiratory syndrome outbreak on health care workers in a medium size regional general hospital in Singapore. Occup Med (Lond). (2004) 54:190–6. doi: 10.1093/occmed/kqh027
38. Khalid I, Khalid TJ, Qabajah MR, Barnard AG, Qushmaq IA. Healthcare workers emotions, perceived stressors and coping strategies during a MERS-CoV outbreak. Clin Med Res. (2016) 14:7–14. doi: 10.3121/cmr.2016.1303
39. Al-Ghamdi M., Mohammed H. Al-Assiri, Hanan HBalkhy An assessment of the level of concern among hospital-based health-care workers regarding MERS outbreaks in Saudi Arabia. BMC Infectious Dis. (2017) 17:1–10. doi: 10.1186/s12879-016-2096-8
40. Mira JJ, Carrillo I, Guilabert M, Mula A, Martin-Delgado J, Pérez-Jover MV. Acute stress of the healthcare workforce during the COVID-19 pandemic evolution: a cross-sectional study in Spain. BMJ Open. (2020) 10:e042555. doi: 10.1136/bmjopen-2020-042555
41. Kathrine Jáuregui Renaud D, Martínez-Pichardo E, José A, Puga M, Dulce M, Rascón-Martínez L, et al. Acute stress in health workers during two consecutive epidemic waves of COVID-19. Int J Environ Res Public Health. (2021) 19:206. doi: 10.3390/ijerph19010206
42. Thompson L, Bidwell S, Seaton P. The COVID-19 pandemic: analysing nursing risk, care and careerscapes. Nurs Inquiry. (2021) e12468. doi: 10.1111/nin.12468
43. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
44. Tait Shanafelt J, Trockel M. Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA. (2020) 323:2133–4. doi: 10.1001/jama.2020.5893
45. Hussien Elkholy F, Ibrahim I, El-din WS, Sabry M, Mohammed S, Hamza M, et al. Mental health of frontline healthcare workers exposed to COVID-19 in Egypt: a call for action. Int J Social Psychiatry. (2021) 67:522–31. doi: 10.1177/0020764020960192
46. Cai Z, Cui Q, Liu Z, Li J, Gong X, Liu J, Wan Z. Nurses endured high risks of psychological problems under the epidemic of COVID-19 in a longitudinal study in Wuhan China. J Psychiatr Res. (2020) 131:132–7. doi: 10.1016/j.jpsychires.2020.09.007
47. Zhang C, Peng D, Lv L, Zhuo K, Yu K, Shen T, et al. Individual perceived stress mediates psychological distress in medical workers during COVID-19 epidemic outbreak in Wuhan. Neuropsychiatr Dis Treat. (2020) 16:2529. doi: 10.2147/NDT.S266151
48. Li Y, Cao S, Gaculenko A, Zhan Y, Bozec A, Chen X. The prevalence and influencing factors for compassion fatigue among nurses in Fangcang shelter hospitals: A cross-sectional study. Front Endocrinol (Lausanne). (2022) 13:e13054. doi: 10.3389/fendo.2022.902033
49. Greenberg N, Cooke J, Sullivan E, Tracy DK. Mental health plan for workers of the London Nightingale Hospital: following the evidence to support staff. BMJ Mil Health. (2021) 167:107–9. doi: 10.1136/bmjmilitary-2020-001624
50. Rodríguez-Martín B, Martínez-Andrés M, Cervera-Monteagudo B, Notario-Pacheco B, Martínez-Vizcaíno V. Perception of quality of care among residents of public nursing-homes in Spain: a grounded theory study. BMC Geriatr. (2013) 13:1–9. doi: 10.1186/1471-2318-13-65
51. Strauss A, Corbin J. Grounded theory methodology: An overview. In: Denzin NK, Lincoln Yvonna S, editors. Handbook of Qualitative Research, Thousand Oaks: Sage Publications (1994). p. 273–85.
52. Allan G. A critique of using grounded theory as a research method. Electronic J Business Res Methods. (2003) 2: 1–10.
53. Aldiabat KM, Navenec L. Philosophical roots of classical Grounded Theory: Its foundations in symbolic interactionism. Qualitative Rep. (2011) 16:1063–80. doi: 10.46743/2160-3715/2011.1121
54. Silva E Lima SG, Spagnuolo RS, Juliani CMCM, Colichi RMB. Nursing consultation in the Family Health Strategy and the nurse's perception: grounded Theory. Rev Bras Enferm. (2022) 75:e20201105. doi: 10.1590/0034-7167-2020-1105
55. Ryuichi Ohta Y, Itamochi S. Overcoming the challenge of COVID-19: A grounded theory approach to rural nurses' experiences. J Gen Fam Med. (2021) 22:134–40. doi: 10.1002/jgf2.410
56. Ogbonnaya A. Peace N Iheanacho. The drive process model of entrepreneurship: A grounded theory of nurses' perception of entrepreneurship in nursing. Int J Africa Nurs Sci. (2021) 15:100377. doi: 10.1016/j.ijans.2021.100377
57. Suddaby R. From the editors: What grounded theory is not. Academy of Manag J. (2006) 49:633–642. doi: 10.5465/amj.2006.22083020
58. Liu F, Kang J. A grounded theory approach to the subjective understanding of urban soundscape in Sheffield. Cities. (2016) 50:28–39. doi: 10.1016/j.cities.2015.08.002
59. Yiz YG, Xu G. Factors associated with mental health outcomes among health care workers in the Fangcang shelter hospital in China International. J Social Psychiatry. (2022) 68:64–72. doi: 10.1177/0020764020975805
60. Rimmer A. Covid-19: staff at Nightingale Hospital in London get wellbeing area courtesy of John Lewis. BM J. (2020) 369. doi: 10.1136/bmj.m1451
61. Bushell V, Thomas L, Combes J. Inside the O2: the NHS Nightingale Hospital London education center. J Interprof Care. (2020) 34:698–701. doi: 10.1080/13561820.2020.1823949
62. Shurlock J, Rudd J, Jeanes A, Iacovidou A, Creta A, Kanthasamy V, et al. Communication in the intensive care unit during COVID-19: early experience with the Nightingale Communication Method. Int J Qual Health Care. (2021) 33:mzaa162. doi: 10.1093/intqhc/mzaa162
63. Fang DS, Li Z, Yuan T, Jiang B, Gan D, Sheng B, et al. Large-scale public venues as medical emergency sites in disasters: lessons from COVID-19 and the use of Fangcang shelter hospitals in Wuhan, China. BMJ Global Health. (2020) 5:e002815. doi: 10.1136/bmjgh-2020-002815
64. Guo Y, Zhong W, Zhang Y, Qian H. A multi-zone spatial flow impact factor model for evaluating and layout optimization of infection risk in a Fangcang shelter hospital. Building Environ. (2022) 214:108931. doi: 10.1016/j.buildenv.2022.108931
65. Li YZ, Xu Y, Ding L, Tang Z. Intelligent fangcang shelter hospital systems for major public health emergencies: the case of the optics valley fangcang shelter hospital. J Manag Engineer. (2022) 38:05021010. doi: 10.1061/(ASCE)ME.1943-5479.0000976
66. Yan Zhi. Fangcang Shelter Hospitals for COVID-19: Construction and Operation Manual. World scientific. (2020) doi: 10.1142/11904
67. Carswell R, Turner PR. The impact of US housing type and residential living situations on mental health during COVID-19 International. J Environ Res Public health. (2021) 18:8281. doi: 10.3390/ijerph18168281
68. Juan Cesar DP, Kokubun K, Ikaga T, Yamakawa Y. Housing quality and behavior affect brain health and anxiety in healthy Japanese adults Scientific Rep. (2021) 11:1–8. doi: 10.1038/s41598-021-91363-4
69. Li SR, Godwin J, Anderson I, Seaman P, Donaldson C. Housing as a social determinant of health and wellbeing: Developing an empirically-informed realist theoretical framework. BMC Public Health. (2020) 20:1–19. doi: 10.1186/s12889-020-09224-0
70. Amerio A, Brambilla A, Morganti A, Aguglia A, Bianchi D, Santi F, et al. COVID-19 lockdown: housing built environment's effects on mental health. Int J Environ Res Public Health. (2020) 17:5973. doi: 10.3390/ijerph17165973
71. Guerrini C, Nardella F, Morganti A, La Nasa J, Degano I, Ribechini E. Effect of Housing Quality on the Mental Health of University Students during the COVID-19 Lockdown. Int J Environ Res Public Health. (2022) 19:2918. doi: 10.3390/ijerph19052918
72. Cláudia C, RobertoPereira C, LuísaLima M. Do the hospital rooms make a difference for patients' stress? A multilevel analysis of the role of perceived control, positive distraction, and social support. J Environ Psychol. (2017) 53:63–72. doi: 10.1016/j.jenvp.2017.06.008
73. Jiang S. Positive distractions and play in the public spaces of pediatric healthcare environments: a literature review. HERD. (2020) 13:171–97. doi: 10.1177/1937586720901707
74. Giuliano KK, Landsman K. Health care innovation: embracing the nurse–engineer partnership. AJN. (2022) 122:55–6. doi: 10.1097/01.NAJ.0000823004.49297.70
75. Brambilla A, Mangili S, Macchi M, Trucco P, Perego A, Capolongo S. Covid-19 massive vaccination center layouts. a modular and scalable model for lombardy region, Italy. Acta Biomed. (2021) 92(Suppl. 6):e2021446. doi: 10.23750/abm.v92iS6.12229
76. Capolongo S, Brambilla A, Girardi A, Signorelli C. Validation Checklist for Massive Vaccination Cente. Annali di igiene: medicina preventiva e di comunita. (2021).
77. Azzopardi-Muscat N, Caracci F, Capolongo S. Synergies in design and health The role of architects and urban health planners in tackling key contemporary public health challenges. Acta Biomed. (2020) 91:9. doi: 10.23750/abm.v91i3-S.9414
Keywords: alternative care facility (ACF), healthcare workers' perception, grounded theory, nurse-engineer partnership, active and passive strategies
Citation: Wang H, Luo P, Wu Y and Zeng X (2022) Factors and optimizations of healthcare workers' perception in alternative care facilities. Front. Public Health 10:891503. doi: 10.3389/fpubh.2022.891503
Received: 07 March 2022; Accepted: 28 June 2022;
Published: 27 July 2022.
Edited by:
Rokho Kim, World Health Organization, SwitzerlandReviewed by:
Mohsen Khosravi, Zahedan University of Medical Sciences, IranCopyright © 2022 Wang, Luo, Wu and Zeng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peng Luo, d296YWlsaWdvbmc1MTZAZm94bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.