 Liming Liu
Liming Liu Yue Xu1,2†
Yue Xu1,2†
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 09 September 2022
Sec. Health Economics
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.891186
Objectives: To curb the unreasonable growth of medical expenses and reduce the burden of medical treatment, Beijing launched two rounds of comprehensive reform of public hospitals. In the two reforms, the addition of drugs and consumables was canceled successively. This study compared the changes in the direct medical cost of inpatients with coronary heart disease (CHD) in the three stages of two comprehensive public hospital reforms in Beijing and provides data support for health reform policies.
Setting: CHD diagnosis and treatment data were extracted from the Hospital Information System (HIS) of 33 public hospitals. The total amount and composition of the direct medical expenses of CHD inpatients in the three stages were calculated. Interrupted time series analysis was used to study the instantaneous changes and trend changes in the three stages.
Participants: The data were obtained from the HIS system of 33 public hospitals above the second level in Beijing. A total of 66,647 medical and diagnosis records and 24,371,139 charge detail records were included.
Results: After the two reforms, the total cost for CHD inpatients with most clinical classifications and treatment methods decreased. The proportion of drug and consumable costs decreased significantly, whereas the proportion of medical consultation service costs increased. Drug-treated patients were mainly affected by the instantaneous reforms, percutaneous coronary intervention-treated patients were simultaneously affected by instantaneous and trending effects, and coronary artery bypass graft-treated patients were mainly affected by the reform trend.
Conclusion: The overall change in the direct medical cost of CHD inpatients was consistent with the goal of the comprehensive medical reform of public hospitals in Beijing, which is “total control and structural adjustment.”
The rapid rise in health expenditures is an important issue in China's health field. From 2010 to 2017, China's total health expenditures increased by 12.78%, which was much higher than the gross domestic product (GDP) per capita growth rate of 8.06% (1). If this growth trend cannot be effectively curbed, the increase in health expenses may exceed the economic affordability of individuals, society, and the government (2, 3).
In the past, there was a 15% drug sale mark-up policy in public hospitals. Due to the drug markups, medical institutions or doctors might have exhibited “profit-seeking behaviors” (4). One of the reasons for the unreasonable increase in medical expenses was that hospitals received profit from drug markups to maintain normal operations. In 2017, the drug markup in public hospitals in China was completely canceled (5), which eliminated the relationship between doctors and drug revenue to a certain extent (6). Some studies found that the reform had a positive impact on doctors' medication behavior (7). But some studies found that although drug markups were abolished, doctors in public hospitals in China still had an incentive to prescribe more drugs (8). Other studies showed that although hospital drug revenue was reduced, it led to a rise in other revenue categories, such as diagnostics, laboratory tests, and medical consumables (9, 10).
Beijing launched two rounds of the comprehensive reform of public hospitals on 8 April 2017 and 15 June 2019. In the first round of reform, 15% of the drug markups (except for Chinese medicine decoction pieces), registration fees, and diagnosis and treatment fees were abolished, and medical service fees were set up. In addition, long-term prescription services for four types of chronic diseases, namely, hypertension, diabetes, coronary heart disease (CHD), and stroke, were launched. Long-term prescriptions for the four types of chronic diseases could be prescribed for up to 2 months (11). In the second round of reforms, consumables markups were canceled, and the volume-based procurement (VBP) of drugs and medical consumables was implemented (12). Both rounds of medical reform reduced the prices of inspection items and increased the prices of items that could reflect the value of doctors' labor, such as beds, nursing, traditional Chinese medicine, and surgery. The specific measures of the two rounds of reform are shown in Table 1.
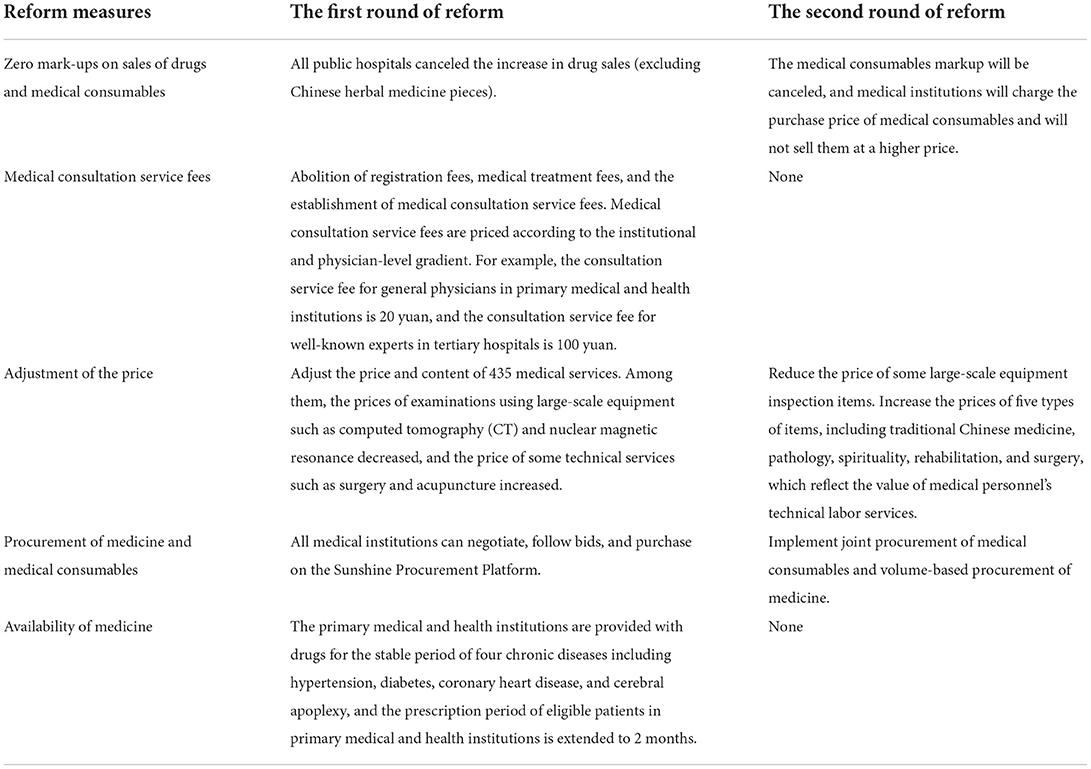
Table 1. Reform measures at public hospitals in Beijing.
CHD is a group of diseases that includes no symptoms, angina, myocardial infarction, ischemia cardiomyopathy, and sudden cardiac death (13). As one of the major forms of cardiovascular diseases (14), CHD is often accompanied by other diseases, such as hypertension, stroke, and diabetes (15). Therefore, CHD could impact not only locally in the heart, but also pulmonary function, whole-body skeletal muscle function, activity ability, psychological status, and others. Currently, with high morbidity and mortality, CHD has been the leading cause of death worldwide (13). The treatment of CHD is mainly divided into drug therapy and interventional therapy. In severe cases, surgical bypass surgery is considered (16). The average annual growth rate of hospitalization expenses far exceeds that of the GDP, which has exerted tremendous pressure on the economic burden of disease and the medical insurance funds of Chinese residents (17). As mentioned above, in this reform policy, CHD was one of the four types of chronic diseases for which medication could be prescribed for a long time.
Previous studies have been conducted on the impact of comprehensive reforms on the cost of all diseases and chronic diseases (11, 12, 18), but little attention has been paid to CHD. Therefore, the impact of reforms on CHD needs to be studied. This article is an important supplement to existing research.
Therefore, this study examined the changes in the cost for patients with CHD hospitalized before and after the two reforms, analyzed whether the results of the reform met the expected assumptions, and provided data support for my country to control the unreasonable growth of health costs, reduce irregular diagnoses and treatment behaviors, and adjust health policies.
After implementing the two comprehensive reforms in public hospitals, the total direct medical expenses of CHD inpatients remained unchanged or decreased, and the structure of direct medical expenses was optimized.
Data were obtained from the Hospital Information System (HIS) of 33 public hospitals in Beijing, which ensures the authenticity, accuracy, and completeness of the data. Data were obtained from the Medical Record Table, the Diagnosis Record Table, and the Charge Details Table. The Medical Record Table mainly includes basic information such as the patient's admission date, discharge date, and hospital name. The Diagnosis Record Table includes information related to the patient's condition and treatment, including main diagnosis, secondary diagnosis, main surgery/operation, and secondary surgery/operation. The Charge Details Table includes detailed information about the patient's diagnosis and treatment, medical service items, the unit price of medical service items, and the quantity of medical service items used.
According to the research purpose of this article, the data of patients whose first three main diagnosis ICD-10 code digits ranged from I20 to I25 and whose discharge dates were between 1 January 2016 and 31 December 2019 were extracted. Then, the data were cleaned to delete duplicate data records, missing key field records, and abnormal data. After that, records with the primary diagnosis of CHD were included, and records with any secondary diagnosis were excluded. Finally, a total of 51,951 medical records were included.
Since there are many clinical types of CHD, this study selected the clinical types with a large number of medical records for analysis. In different treatment methods and different reform stages, unstable angina pectoris (I20.0), acute subendocardial myocardial infarction (I21.4), and arteriosclerotic heart disease (I25.1) had a considerable number of patient records. To reduce the randomness of the data, we choose these three clinical classifications for this research. At the same time, due to the large differences in costs between the various treatment methods, treatments were divided into three groups, namely medical treatments, percutaneous coronary intervention (PCI), and coronary artery bypass grafting (CABG).
In addition, according to the time points of the implementation of the two reforms, the included patient records were divided into three stages:
① The period before the implementation of the reform was classified as the pre-reform stage, with patient discharge dates between 1 January 2016 and 7 April 2017.
② The period after the implementation of the first reform was classified as the first reform stage, with admission dates on or after 8 April 2017 and a discharge date before 14 June 2019.
③ The period after the second reform trial was classified as the second reform stage. The admission date was on or after 15 June 2019, and the discharge date was before 31 December 2019.
Descriptive statistical analysis of the data was carried out using Excel software. The total cost for CHD patients and the proportion of various detailed costs in the three stages were counted separately, including the cost of medicine, the cost of consumables, the cost of inspections, and the cost of laboratory and medical consultation services. The content of each cost is shown in Table 2. The cost of medical consultation services (19) was the sum of the cost of registration, bed, examination, treatment, surgery, pharmacy services, and nursing care. Since these types of expenses are designed to reflect the value of the technical services of the medical staff, they were summed as the medical consultation service costs in the results.
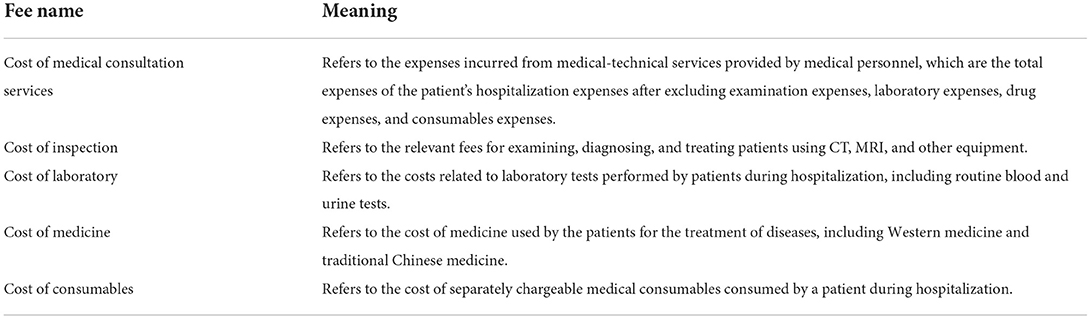
Table 2. Fee explanation list.
Interrupted time series analysis (ITSA) is a quasi-experimental research design used to evaluate the effects of interventions (20). It measures the instantaneous changes and trend changes from the intervention by observing data at multiple time points before and after the intervention. This method has been applied to the field of policy evaluation (21). The segmented regression model is commonly used in ITSA. Through segmented regression model analysis, the trend in the actual results after the intervention and the natural trend before the intervention were compared and tested to evaluate the intervention effect (22). The ITSA model principle was detailed in a previous report (23).
The monthly data were summarized, and then, a piecewise regression model of ITSA was established. Through ITSA, the instantaneous changes and trend changes in the monthly average cost for patients with different treatment methods and clinical types of CHD before and after the two reforms were discussed to explore whether the changes in CHD cost changes were mainly affected by instantaneous effects or trends.
The basic characteristics of the patients in the three reform stages are shown in Table 3. The proportion of male patients was slightly higher than that of female patients, the average age was about 66 years old, and the highest proportion of patients aged 60–69 was about 33%. The average length of hospitalization was about 7 days, most patients had an ICD-10 code of I25.1, and the proportion of patients receiving drug treatment was more than in patients treated with PCI or CABG.
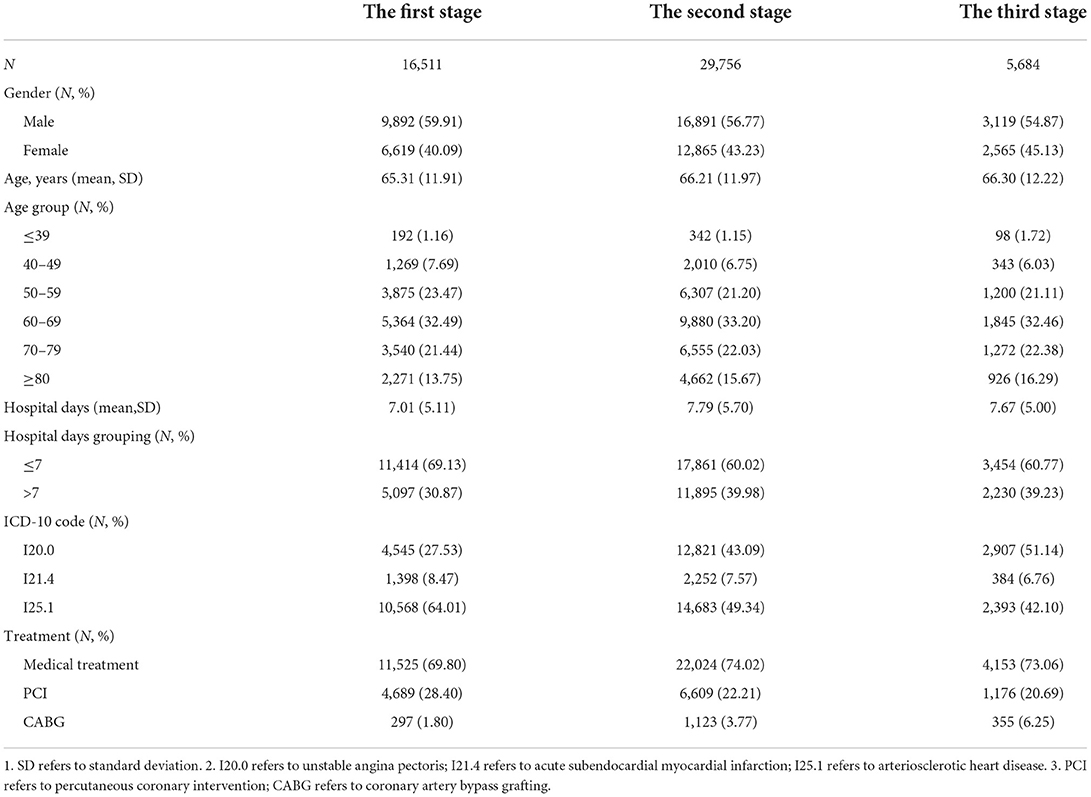
Table 3. Characteristics of patients in the three reform stages.
Table 4 shows the average total cost for patients with ICD codes CHDI20.0, I21.4, and I25.1 treated with medication, PCI, and CABG.
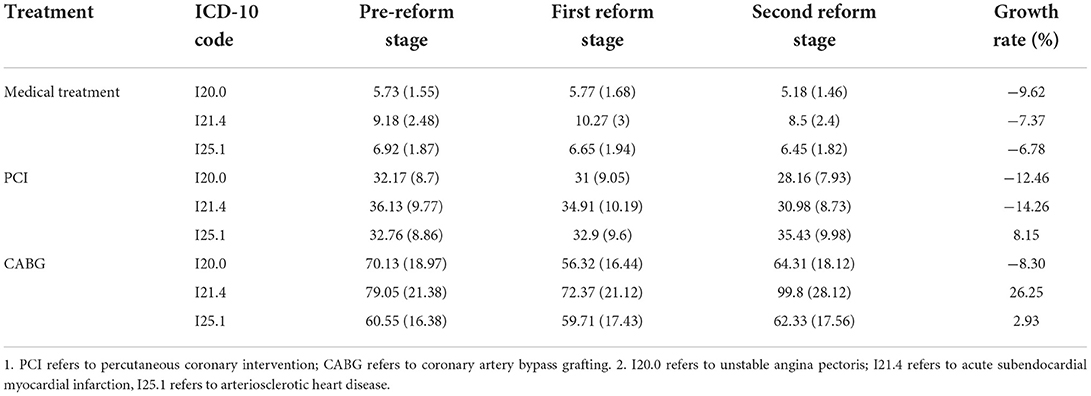
Table 4. Average total cost of inpatients with coronary heart disease in three stages of different treatment methods and clinical types [1,000 RMB (1,000 dollars)].
In medical treatment, the total cost of the patients with the three clinical types of CHD increased from the first phase of the reform and decreased in the second phase of the reform. After the two reforms, the overall cost for patients with ICD codes of I20.0 decreased by 9.62% compared to before the medical reforms, and the cost for patients with I21.4 and I25.1 ICD codes increased by 7.37 and 6.78%, respectively.
In PCI treatment, the total cost for patients with the three clinical types of CHD increased in the first phase of the reform, and the cost for patients with ICD codes I20.0 and I21.4 decreased in the second phase of the reform, while the cost for patients I25.1 increased. After the two reforms, the overall cost for patients with I20.0 and I21.4 ICD codes decreased by 12.46 and 14.26%, respectively, and the cost for patients with I25.1 ICD codes increased by 8.15%.
In CABG treatment, the total cost for patients with ICD codes I20.0 and I21.4 decreased from the first phase of the reform, while the cost for patients with I25.1 ICD codes increased, and the cost for patients with the three clinical types of CHD increased in the second phase of the reform. After the two reforms, the overall cost for patients with ICD codes of I20.0 decreased by 8.30% compared to before the medical reforms, and the cost for patients with I21.4 and I25.1 ICD codes increased by 26.25 and 2.93%, respectively.
Figure 1 shows the composition of the average total cost for the medical of treatment inpatients with three clinical types of CHD. From the perspective of the cost structure, the cost of medicine accounted for a relatively high proportion of the cost of CHD patients treated with medications. After the two reforms, the proportion of the cost of medicine dropped. Among them, the proportion of the cost of medicine in patients with I25.1 ICD codes dropped the most, which was 6.28%. The proportion of the cost of medical consultation services increased by more than 10%; the proportion of the cost of consumables decreased, of which the proportion of consumables for patients with ICD codes of I21.4 and I25.1 dropped by 6 and 4%, respectively, more than the decrease of 1% in patients with ICD codes of I20.0. The proportion of the cost of inspections and laboratory tests decreased by about 2–3%.
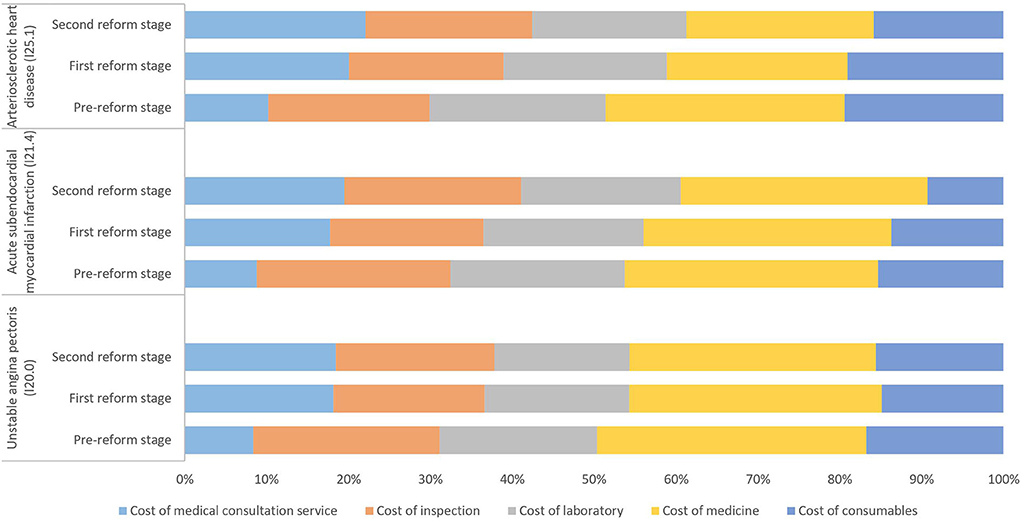
Figure 1. Composition of the total cost of inpatients with different clinical types of coronary heart disease treated by medical treatment in the three reform stages (%).
Figure 2 shows the composition of the average total cost of inpatients with three clinical types of CHD treated with PCI. From the perspective of cost composition, the proportion of the cost of consumables for patients with CHD treated by PCI was relatively high. After the two reforms, the proportion of the cost of consumables decreased, especially in patients with ICD codes I20.0 and I21.4, which decreased by 5 and 8%, respectively. The proportion of the cost of medical consultation services increased by about 6–9%. The proportion of the cost of medicine, inspections, and laboratory tests did not change much, at < 3%.
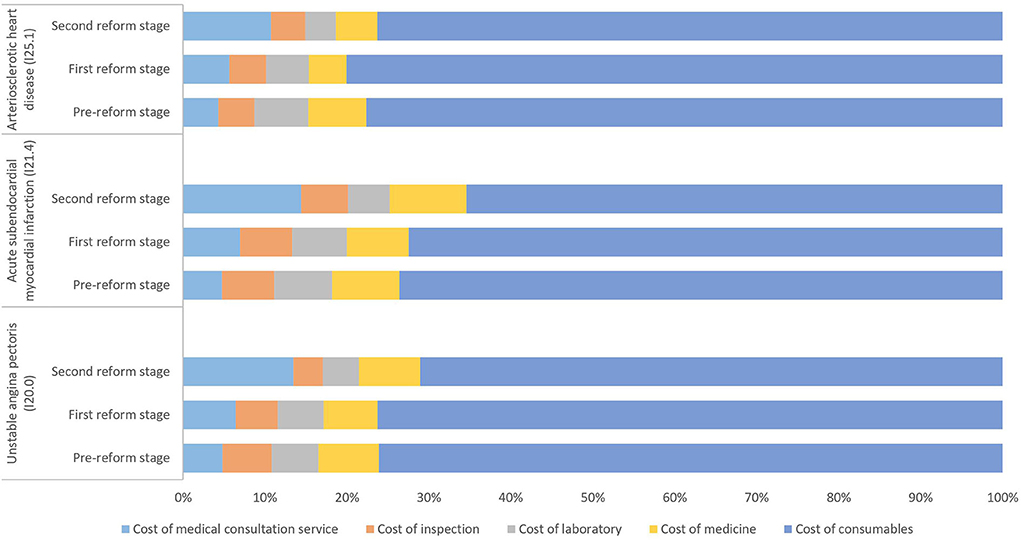
Figure 2. Composition of the total cost of inpatients with different clinical types of coronary heart disease treated with percutaneous coronary intervention (PCI) in the three reform stages (%).
Figure 3 shows the composition of the average total cost of inpatients with the three clinical types of CHD who underwent CABG treatment. From the perspective of cost composition, the proportion of the cost of consumables for CHD patients treated by CABG was relatively high. After the two reforms, the proportion of the cost of consumables decreased, especially for patients with ICD codes of I20.0 and I21.4, which dropped by more than 15%, and the proportion of medical consultation service expenditure increased by 12–15%. The proportion of the cost of medicine in patients with ICD codes of I25.1 decreased by 8.84%, and the proportion of the cost of inspections and laboratory tests changed little, at < 3%.
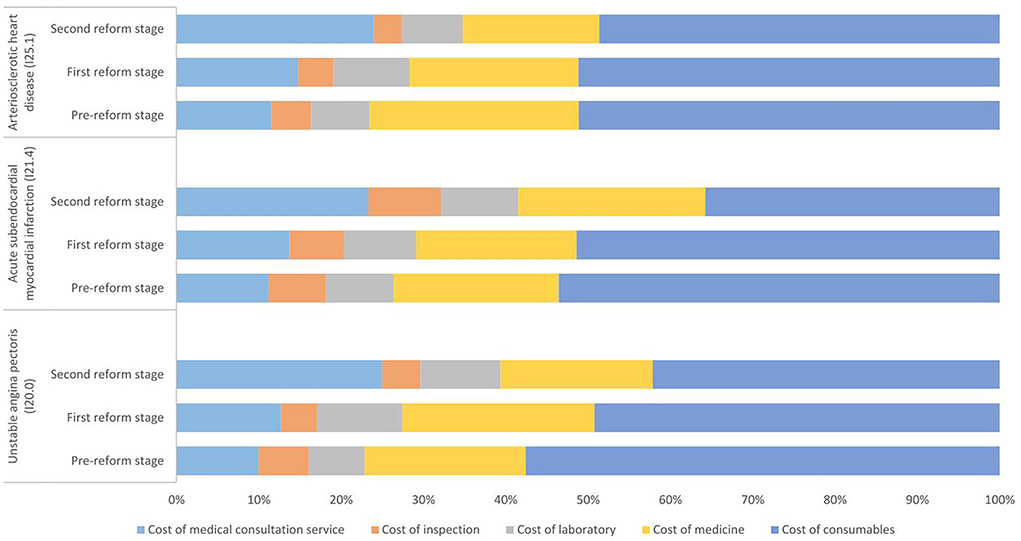
Figure 3. Composition of the total cost of inpatients with different clinical types of coronary heart disease treated with coronary artery bypass grafting (CABG) in three reform stages (%).
Figure 4 shows the instantaneous changes and trend changes in the total cost of CHD inpatients with different clinical types and treatment methods after the two reforms. The ITSA results are shown in Table 5.
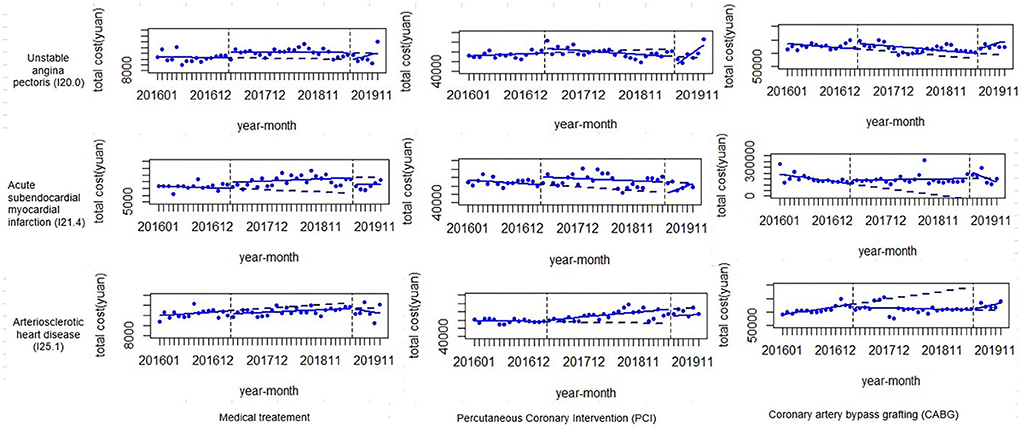
Figure 4. ITSA of the average total cost of inpatients with coronary heart disease with different treatment methods and clinical types.
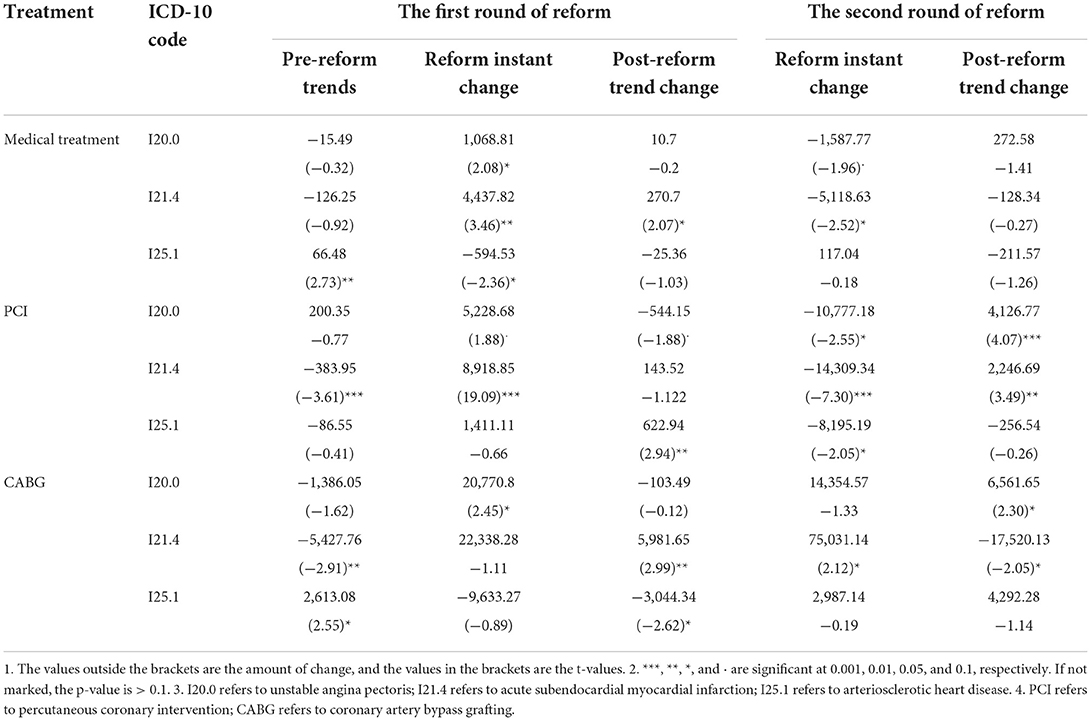
Table 5. ITSA regression results of hospital costs in CHD patients with different treatment methods and clinical types.
In patients with medical treatment, the cost for patients with I20.0 ICD codes rose instantaneously after the first reform and dropped instantaneously after the second reform, whereas the cost for patients with I21.4 ICD codes rose instantaneously after the first reform and showed an upward trend. After the second reform, it showed an instantaneous decline and patients with I25.1 ICD codes dropped instantaneously after the first reform.
In those with PCI treatment, the cost for patients with I20.0 ICD codes rose instantaneously after the first reform and then showed a downward trend, fell instantaneously after the second reform, and then showed an upward trend. The cost for patients with I21.4 ICD codes rose instantaneously after the first reform, and after the second reform, it dropped instantaneously and then showed an upward trend. Patients with I25.1 ICD codes showed an upward trend after the first reform and dropped instantaneously after the second reform.
In those who underwent CABG treatment, the cost for patients with I20.0 ICD codes rose instantaneously after the first reform and showed an upward trend after the second reform. The cost for patients with I21.4 ICD codes showed an upward trend after the first reform and, immediately after the second reform, then showed a downward trend. The cost for patients with I25.1 ICD codes showed a downward trend after the first reform.
This study observed the changes in the direct medical expenses of inpatients with different treatment methods and disease types after the two reforms through the average total costs at different stages of the reform. The results showed that after two reforms, the cost for the three types of patients with medical treatment decreased, especially in patients with I20.0 ICD codes. The cost for PCI-treated patients with ICD codes I20.0 and I21.4 decreased, and the cost for patients with I25.1 ICD codes increased. The cost for patients with ICD codes of I20.0 treated with CABG decreased, and the cost for patients with ICD codes of I21.4 and I25.1 increased especially in patients with ICD codes of I21.4. Overall, the cost for most types of CHD patients decreased, especially for patients treated with drugs, but the cost for some types of PCI and CABG patients showed a rising trend, which may have been due to the reform policy requirements. It is necessary to fully reflect the value of the technical labor of the medical staff. Compared to medical treatment, PCI and CABG are valuable adjuncts rather than an alternative to medical therapy (24), which reflects the greater value of technical labor, so the cost may be greater. In short, since the reforms, medical expenses have been effectively controlled. However, the rising expenses need continuous attention in future hospitalization expense management and control to continue to control the cost burden of CHD patients.
This study also observed changes in the composition of direct medical expenses for CHD patients after the reforms. First, the cost of medical consultation services included all costs that could reflect the technical value of the medical staff (12). The higher the proportion of medical consultation service costs, the better the labor value of the medical staff. The results of the study showed that the proportion of the cost of medical consultation services for the medical treatment of CHD patients rose about 20%, indicating the labor value of the medical staff after the reforms. The proportion of the cost of medical consultation services involving PCI and CABG treatment of CHD patients accounted for about 14 and 24%, respectively, which was more than before the reform, and its proportion was lower than that during medical treatment, mainly because the current patients treated by these two treatment methods used mostly consumables and medicine. However, considering the operating difficulty and medical risks of these two treatment methods, the value of medical staff labor should be more reflected, and the composition of the cost needs to be further optimized. In future, it is necessary to scientifically quantify the technical value of medical personnel labor based on the level of economic development in the region, reflecting the difficulty and risk of medical operations. Through the linkage reform of medicine, medical insurance, and medical care (25), the value of medical personnel labor is reflected while ensuring that the patient's disease burden does not increase.
In addition, the proportion of the cost of medicine and consumables reflects the burden of the patients' costs of medicine and consumables, respectively. To reduce the cost of drugs and consumables, the markup of drugs and consumables was eliminated in the first reform and the second reform, respectively. The results of the study showed that drug costs accounted for the highest proportion of the medical treatment of patients. After the reform, the proportion of the drug costs declined, in agreement with reform expectations, and the burden of drug costs has been effectively controlled. In addition, the cost of consumables accounted for the highest proportion of the cost of PCI and CABG patient treatments. After the reform, the proportion of the cost of consumables dropped significantly, which is also consistent with the reform goals, and the burden of consumables has also been controlled. However, the cost of consumables remained the main cost of the PCI- and CABG-treated patients. In future, with the advancement of the VBP of drugs and medical consumables, the price will continue to fall, and the economic burden will continue to be controlled (26).
From the perspective of changes in the total amount and the composition of comprehensive costs, the overall cost of CHD patients after the reform has not changed much, and the proportion of medical consultation service expenses has increased, whereas the proportion of medicine and consumables has decreased, realizing the “translation” effect of the reform on expenses. The cost has also shifted from medicine and consumables to medical consultation services, which can better reflect the value of technical medical staff labor in the diagnosis and treatment processes. The cost structure has been optimized, which is conducive to the rationalization of diagnosis and treatment behaviors, thereby enhancing the value of medical consultation services. Overall, the results of this study are consistent with the research hypothesis. Previous studies evaluated the two rounds of public hospital reforms in Beijing and found that both rounds of reform contained the growth rate of medical expenditures, and hospital revenue structures were reshaped and optimized (12), which are consistent with the results of this study.
This study also analyzed the instantaneous changes and trend changes in the direct medical expenses of CHD patients through ITSA. Overall, after the reform, medically treated patients had a transient effect, CABG-treated patients had a trend effect, and PCI-treated patients had both transient and trend effects. From a clinical point of view, drug treatment is the basis of all treatments, so only the patient's cost of drug treatment has an immediate change, indicating that the policy of reforming and canceling drug markups had an overall impact on the cost level, but did not change the trend of cost changes. PCI is carried out on the basis of drug therapy, which includes the technical difficulty of surgery in addition to drug therapy, so there are both instantaneous and trend changes. The absence of instantaneous changes in the cost of CABG may be that bypass therapy is more affected by technology and less affected by drugs (27).
In addition, the total cost for patients with the I20.0 ICD codes mentioned above for medical treatment decreased overall compared to before the reforms, and the ITSA results found that the cost of this type of patient only changed instantaneously, and the trend change was not significant. After the first reform, the cost for patients with I20.0 ICD codes rose instantaneously and then dropped instantaneously after the second reform. Therefore, it was comprehensively judged that the cost was mainly due to the instantaneous impact of the second reform.
In addition, as mentioned above, the total cost for patients with I20.0 and I21.4 ICD codes for PCI treatment decreased, and the cost for patients with I25.1 ICD codes increased. The ITSA results showed that after the first reform, the cost for patients with I20.0 and I21.4 ICD codes rose instantaneously, and the cost for patients with I20.0 ICD codes showed a downward trend. After the second reform, the cost for patients with I20.0 and I21.4 ICD codes dropped instantaneously and then showed an upward trend. Therefore, it can be inferred that the decline in the costs for patients with I20.0 ICD codes was not only affected by the trend of the first reform, but also by the instantaneous impact of the second reform, and the decline in the costs for patients with I21.4 ICD codes was mainly due to the instantaneous effects from the second reform. In addition, patients with I25.1 ICD codes showed an upward trend after the first reform and dropped instantaneously after the second reform, which could indicate that the increase in the cost for patients with I25.1 ICD codes was mainly affected by the trend change of the first reform.
Finally, the above discussion mentioned increases in the costs for patients with I21.4 and I25.1 ICD codes treated with CABG. The ITSA results showed that in CABG treatment, the cost for patients with I21.4 ICD codes showed an upward trend after the first reform, rose instantaneously after the second reform, and then showed a downward trend. Therefore, the increase in the cost for patients with I21.4 ICD codes was mainly affected by the change in the trend from the first reform and the instantaneous change from the second reform. In addition, patients with I25.1 ICD codes showed a downward trend after the first reform, but the costs increased overall, indicating that the changes in the trend after the reform did not significantly change the costs.
First, previous studies only explained the effect in overall diseases and chronic diseases. This study additionally confirmed the effectiveness of the comprehensive reforms in CHD, that is, the role of reform in CHD was consistent with the overall change in previous studies.
Second, since there were large differences in costs between the various treatment methods, we specifically divided them into three groups, namely medical treatment, PCI, and CABG, which enriched the results.
Third, this study had advantages in data collection, and the sample was highly representative, but it only represented the situation of medical reform in Beijing. Due to the specificity of Beijing in China, the extrapolation of the study results is limited.
This study observed the changes in the total amount and composition of the direct medical expenses of CHD patients after the two comprehensive reforms of public hospitals in Beijing, as well as the instantaneous and trend changes. Finally, we found that the total cost of inpatients with coronary heart disease agreed with the goal of “total control and structural adjustment” in Beijing's comprehensive medical reform. After the reform, the total cost was effectively controlled and the cost structure was optimized. The proportion of medical consultation service costs greatly increased under the guidance of comprehensive reform policy, reflecting the improvement in the value of medical staff labor. At the same time, the proportion of the cost of medicine and consumables decreased, and the burden in CHD patients was reduced. On the whole, the results are consistent with the expected effect of the reform policy.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
WC conceived and designed the experiments. XM, YJ, LZ, and YX performed the experiments. LL and YX analyzed the data, contributed reagents, materials, and analysis tools. LL and JY wrote the article. All authors contributed to the article, reviewed the manuscript and approved the submitted version.
Funding was obtained from 2021 Accounting of Beijing's Total Recurring Health Expenditure Based on SHA2011 and the fund project only provided basic data support for this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wang L, Chen Y. Determinants of China's health expenditure growth: based on Baumol's cost disease theory. Int J Equity Health. (2021) 20:213. doi: 10.1186/s12939-021-01550-y
2. Li Z, Li J. Lessons and prospects of Universal Health Coverage in China: the importance of equity, quality, and affordability. Asian Bioethics Rev. (2019) 11:3. doi: 10.1007/s41649-019-00077-3
3. Murray CJL, Lopez AD. Measuring global health: motivation and evolution of the Global Burden of Disease Study. Lancet. (2017) 2017:390. doi: 10.1016/S0140-6736(17)32367-X
4. Liu Y-M. Understanding profit margins of medical providers from prescription drugs: evidence from Taiwan. Int Health. (2019) 12:272–80. doi: 10.1093/inthealth/ihz072
5. Xu J, Jian W, Zhu K, Kwon S, Fang H. Reforming public hospital financing in China: progress and challenges. BMJ. (2019) 365:l4015–l15. doi: 10.1136/bmj.l4015
6. Lin T, Wu Z, Liu M, Wu X, Zhang X. Evaluation of the effectiveness of comprehensive drug price reform: a case study from Shihezi city in Western China. Int J Equity Health. (2020) 19:9. doi: 10.1186/s12939-020-01246-9
7. He Z, Zhou J. Can zero-markup policy for drug sales in public hospitals resolve the problem of ‘seeing a doctor is too expensive' in China? A case study of four municipal general tertiary hospitals at H City in Z Province. J Chinese Governance. (2017) 2:1342899. doi: 10.1080/23812346.2017.1342899
8. Fu H, Li L, Yip W. Intended and unintended impacts of price changes for drugs and medical services: evidence from China. Soc Sci Med. (2018) 211:114–22. doi: 10.1016/j.socscimed.2018.06.007
9. Peng Z, Zhan C, Ma X, Yao H, Chen X, Sha X, et al. Did the universal zero-markup drug policy lower healthcare expenditures? Evidence from Changde, China. BMC Health Serv Res. (2021) 21:1205. doi: 10.1186/s12913-021-07211-8
10. Zeng J, Chen X, Fu H, Lu M, Jian W. Short-term and long-term unintended impacts of a pilot reform on Beijing's zero markup drug policy: a propensity score-matched study. BMC Health Serv Res. (2019) 19:916. doi: 10.1186/s12913-019-4764-z
11. Liu X, Xu J, Yuan B, Ma X, Fang H, Meng Q. Containing medical expenditure: lessons from reform of Beijing public hospitals. BMJ. (2019) 365:l2369. doi: 10.1136/bmj.l2369
12. Gao L, Shi L, Meng Q, Kong X, Guo M, Lu F. Effect of healthcare system reforms on public hospitals' revenue structures: evidence from Beijing, China. Soc Sci Med. (2021) 283:114210. doi: 10.1016/j.socscimed.2021.114210
13. Wang L, Ai DM, Zhang N. Exercise benefits coronary heart disease. In: Xiao J, editor, Exercise for Cardiovascular Disease Prevention and Treatment: From Molecular to Clinical, Pt 2. Cham: Springer International Publishing Ag (2017). p. 3–7. doi: 10.1007/978-981-10-4304-8_1
14. Zhu KF, Wang YM, Zhu JZ, Zhou QY, Wang NF. National prevalence of coronary heart disease and its relationship with human development index: a systematic review. Eur J Prev Cardiol. (2016) 23:530–43. doi: 10.1177/2047487315587402
15. Tusek-Bunc K, Petek D. Comorbidities and characteristics of coronary heart disease patients: their impact on health-related quality of life. Health Quality Life Outcomes. (2016) 14:1. doi: 10.1186/s12955-016-0560-1
16. Wienbergen H, Hambrecht R. Differential therapy in coronary heart disease. Herz. (2014) 39:178. doi: 10.1007/s00059-013-4049-y
17. Ding JM, Zhang XZ, Hu XJ, Chen HL, Yu M. Analysis of hospitalization expenditures and influencing factors for in patients with coronary heart disease in a tier-3 hospital in Xi'an, China: a retrospective study. Medicine. (2017) 96:e9341. doi: 10.1097/MD.0000000000009341
18. Liu L, Xu Y, Jiang Y, Zhao L, Yin X, Shen C, et al. Impact of Beijing healthcare reform on the curative care expenditure of outpatients with non-communicable diseases based on SHA2011 and interrupted time series analysis. BMC Health Serv Res. (2021) 21:1045. doi: 10.1186/s12913-021-07059-y
19. Tang W, Xie J, Lu Y, Liu Q, Malone D, Ma A. Effects on the medical revenue of comprehensive pricing reform in Chinese urban public hospitals after removing drug markups: case of Nanjing. J Med Econ. (2018) 21:326–39. doi: 10.1080/13696998.2017.1405817
20. Kontopantelis E, Doran T, Springate DA, Buchan I, Reeves D. Regression based quasi-experimental approach when randomisation is not an option: interrupted time series analysis. BMJ. (2015) 350:2750. doi: 10.1136/bmj.h2750
21. Du J, Xie J, Qian Y, Wu M, Huang W, Yin J, et al. Impact of China's zero mark-up drug policy on drug cost of NCDs' outpatients: an interrupted time series analysis. BMC Health Services Res. (2021) 21:3. doi: 10.1186/s12913-021-06414-3
22. Turner SL, Forbes AB, Karahalios A, Taljaard M, McKenzie JE. Evaluation of statistical methods used in the analysis of interrupted time series studies: a simulation study. BMC Medical Res Methodol. (2021) 21:1364. doi: 10.1186/s12874-021-01364-0
23. Lopez BJ, Steven C, Antonio G. Corrigendum to: Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. (2020) 50:1045. doi: 10.1093/ije/dyaa118
24. Simoons ML, Windecker S. Chronic stable coronary artery disease: drugs vs. revascularization. Eur Heart J. (2010) 31:530–41. doi: 10.1093/eurheartj/ehp605
25. Liu GG, Vortherms SA, Hong X. China's health reform update. Annu Rev Public Health. (2017) 38:431–48. doi: 10.1146/annurev-publhealth-031816-044247
26. Tang M, He J, Chen M, Cong L, Xu Y, Yang Y, et al. “4+7” city drug volume-based purchasing and using pilot program in China and its impact. Drug Discov Therapeut. (2020) 13:1093. doi: 10.5582/ddt.2019.01093
Keywords: coronary heart disease, inpatients, direct medical expenses, comprehensive reform, interrupted time series analysis
Citation: Liu L, Xu Y, Yu J, Man X, Jiang Y, Zhao L and Cheng W (2022) The impact of comprehensive public hospital reforms on the direct medical cost of inpatients with coronary heart disease. Front. Public Health 10:891186. doi: 10.3389/fpubh.2022.891186
Received: 17 March 2022; Accepted: 18 August 2022;
Published: 09 September 2022.
Edited by:
Mohammad Enamul Hoque, The University of Sydney, AustraliaReviewed by:
Haomiao Li, Wuhan University, ChinaCopyright © 2022 Liu, Xu, Yu, Man, Jiang, Zhao and Cheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Cheng, Y2hlbmd3ZWlAYnVjbS5lZHUuY24=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.