 Ying Zhou
Ying Zhou Yaonan Sun2†
Yaonan Sun2†
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health , 09 September 2022
Sec. Environmental Health and Exposome
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.883241
This article is part of the Research Topic The Built Environment and Public Health: New Insights View all 44 articles
With limited medical resources, it is of great significance for countries all over the world to explore architectural design methods to enhance the value of medical facilities. Therefore, it is very necessary to carry out an extensive international comparison. In order to grasp the research trend of healthcare facilities in the world, this paper conducts co-occurrence analysis, cluster analysis, and trend analysis of the keywords of 334 English articles and 153 Japanese articles related to healthcare facilities published in important academic journals in the USA and Japan in the past 15 years. We not only compare the similarities and differences in healthcare facility research between the USA and Japan, but also explore the reasons for these differences. It is found that by introducing three kinds of value variables, such as time, space, and behavior, we can not only well explain the difference in the solution of healthcare facilities in the USA and Japan to reduce medical costs but also provide new ideas for architectural design to enhance the value of hospitals. Based on the above analysis, a conceptual framework of value-based design of healthcare facilities that combines the advantages of the USA and Japan is proposed in this paper.
Healthcare systems all over the world are facing the problem of both improving the quality of healthcare and controlling medical costs. Thanks to the booming medical technology, the average human life expectancy has increased rapidly from the 40s before World War II to nearly 80 years at present over the past three-quarters of a century. However, due to the infinite increasing characteristics of healthcare services, medical costs all over the world might increase faster during this period. For example, healthcare costs in the USA reached 16.7% of GDP in 2019 (1). For developing countries, it is also very necessary to effectively control medical costs to improve affordability while improving the quality and accessibility of healthcare systems.
In such context, value-based medicine, which aims to improve the medical outcomes per unit cost, has attracted extensive attention in the world medical community in recent years. For example, lean medicine (2), which aims to reduce unnecessary waste, and value-based competition (3), which focuses on the therapeutic effect of patients, can all be viewed as different aspects of value-based medicine. It could be said that the medical system is so complex, and the meaning of value is so rich that it is necessary to explore value-based healthcare from different perspectives at this stage.
As hospital spending accounts for a large part of the total medical costs (4) and the construction or operation costs of the facilities account for a large part of the hospital spending, it is also very meaningful to improve medical outcomes and reduce costs by improving the design methods of healthcare facilities.
As we all know, healthcare design is very difficult because it not only meets the complex requirements of medical operation processes, medical equipment, and hospital management in the limited space but also coordinates the various possible opposing demands of various stakeholders, such as patients, medical staff, administrators, and even medical payers in the use of space.
In order to achieve such goals, both existing experience-based design approaches and evidence-based design approaches need to be re-examined.
In fact, healthcare design around the world was mainly based on the experience of architects until the 1950s. With the development of medical technology, the size of hospitals is increasing, and the medical functions are becoming more and more complex. In developed countries, such as the USA and Japan, evidence accumulated through scientific research, such as Post-Occupancy Evaluation (POE) survey, has played an increasingly important role in healthcare design, and the currently popular evidence-based design (EBD) approach was formed under such a trend (5). However, EBD is only a local and in-depth research method or design process because most of the existing evidence only reveals the microscopic mechanisms between environmental variables and healthcare outcomes, rather than reflecting the relationship between these mechanisms and the master plan of the facilities.
As healthcare facilities become increasingly complex, the evidence not only accumulates to a very large amount but also often contradicts each other due to differences in research viewpoints, which is very inconvenient for architects to increase the value of healthcare facilities through comprehensive judgment in the early design stage. Therefore, healthcare design needs not only to accumulate new evidence in new usage scenarios but also to select and integrate useful content from a large amount of existing evidence through reasonable value judgment.
Moreover, extensive international comparisons are necessary for the field of healthcare design. For example, although healthcare design in Japan had been heavily influenced by the USA (6), many aspects of Japanese hospitals are still very different from those in the USA, especially in terms of high quality and low price. The reasons behind it need to be further explored through comparative studies.
It cannot be ignored that healthcare design in many populous developing countries is still in the transitional stage from experience-based design to evidence-based design. Due to the relatively weak research foundation, architects from these countries have to learn from a large amount of research results and the evidence accumulated by developed countries, such as the USA and Japan. Only a comprehensive and in-depth understanding of the facts behind the evidence can facilitate a reasonable trade-off in design practice. Otherwise, in order to solve a problem in one aspect, it may bring more problems in other aspects. For example, while healthcare facilities in the USA have advanced medical technology and advanced hospital management experience, their high construction standards may be unaffordable for developing countries. Although healthcare facilities in Japan are inexpensive and accessible, their layout is closely related to their unique nursing system.
All in all, in order to take into account both inherent and universal aspects of international experience, a comparative analysis of research articles related to health facilities published in important academic journals in the USA and Japan from the perspective of a third country is conducted as follows. On this basis, the conceptual framework of value-based design of healthcare facilities of universal significance is then proposed.
The following research methods are adopted in this paper to find out the similarities and differences in the field of healthcare design research in detail between the USA and Japan.
First, we selected all health environment and design relevant articles in the past 15 years from a representative English journal and a representative Japanese journal separately in order to grasp the overall research situation and recent hot issues in this field in the USA and Japan.
The English journal is Health Environments Research & Design Journal (HERD), which was founded in 2007 (7) by D. Kirk Hamilton who proposed EBD in 2003 (5). The journal is currently the most representative journal in the field of healthcare facility and evidence-based design in the USA. We chose reviews and articles in which research objects are about American medical facilities and the first author's institution is in the USA from HERD for this study and removed articles that do not provide keyword information.
Architectural Institute of Japan (AIJ) Journals, which include the Journal of Architecture Planning, Journal of Structural and Construction Engineering, Journal of Environmental Engineering, and AIJ Journal of Technology and Design, are the top academic journals in the field of architecture in Japan (8). Although the articles published in these journals are of high quality, the value of these articles is not easily recognized by international peers because they are written in Japanese. We selected articles or reviews related to the studies of healthcare facilities in Japan over the past 15 years from AIJ journals.
Second, we used the VOSviewer software to establish a keyword co-occurrence network and make visualization mapping using the analysis method of LinLog and modularity, and then we conducted comparative studies of keyword co-occurrence, cluster, and trend between the articles from HERD and those from AIJ journals.
Third, the concept of value variables is proposed, and the differences between the USA and Japan in care unit design and the reasons behind them are analyzed through value variables, such as the length of hospital stay, bed area, and nursing system.
Finally, we propose a conceptual framework for the value-based design of healthcare facilities and conduct case studies based on it.
Search strategies, topics and publication titles, and results are shown in Table 1. A total of 383 articles in HERD and 162 articles in AIJ Journals are obtained, and 334 eligible HERD articles and 153 eligible AIJ Journals articles were considered for analysis (Figure 1).
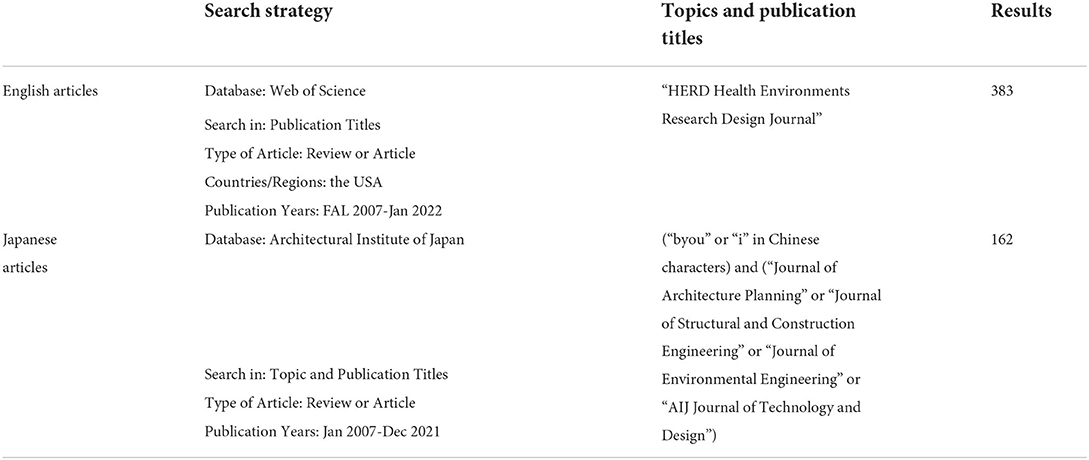
Table 1. Search strategies and results of the English and Japanese articles.
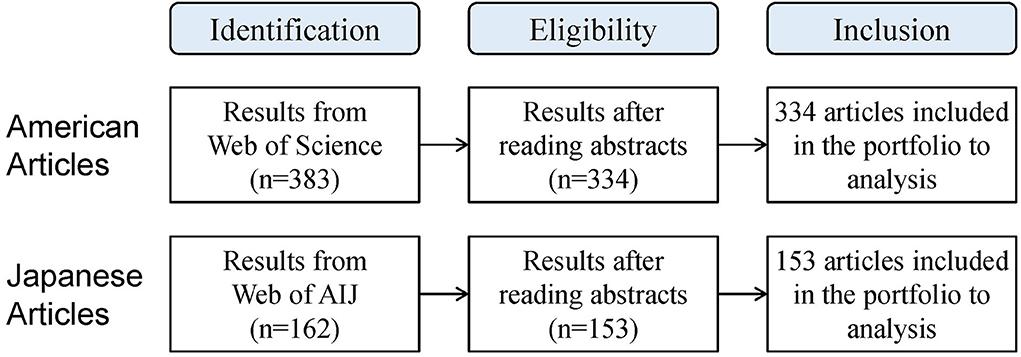
Figure 1. Obtaining the articles for analysis.
Figure 2A shows the co-occurrence map of keywords in the articles selected from HERD. All keywords are divided into four clusters, represented by red, green, yellow, and blue colors, respectively. Table 2 shows that the main keywords in the four clusters are divided into five categories (method, physical space, concerning issues, care, and person).
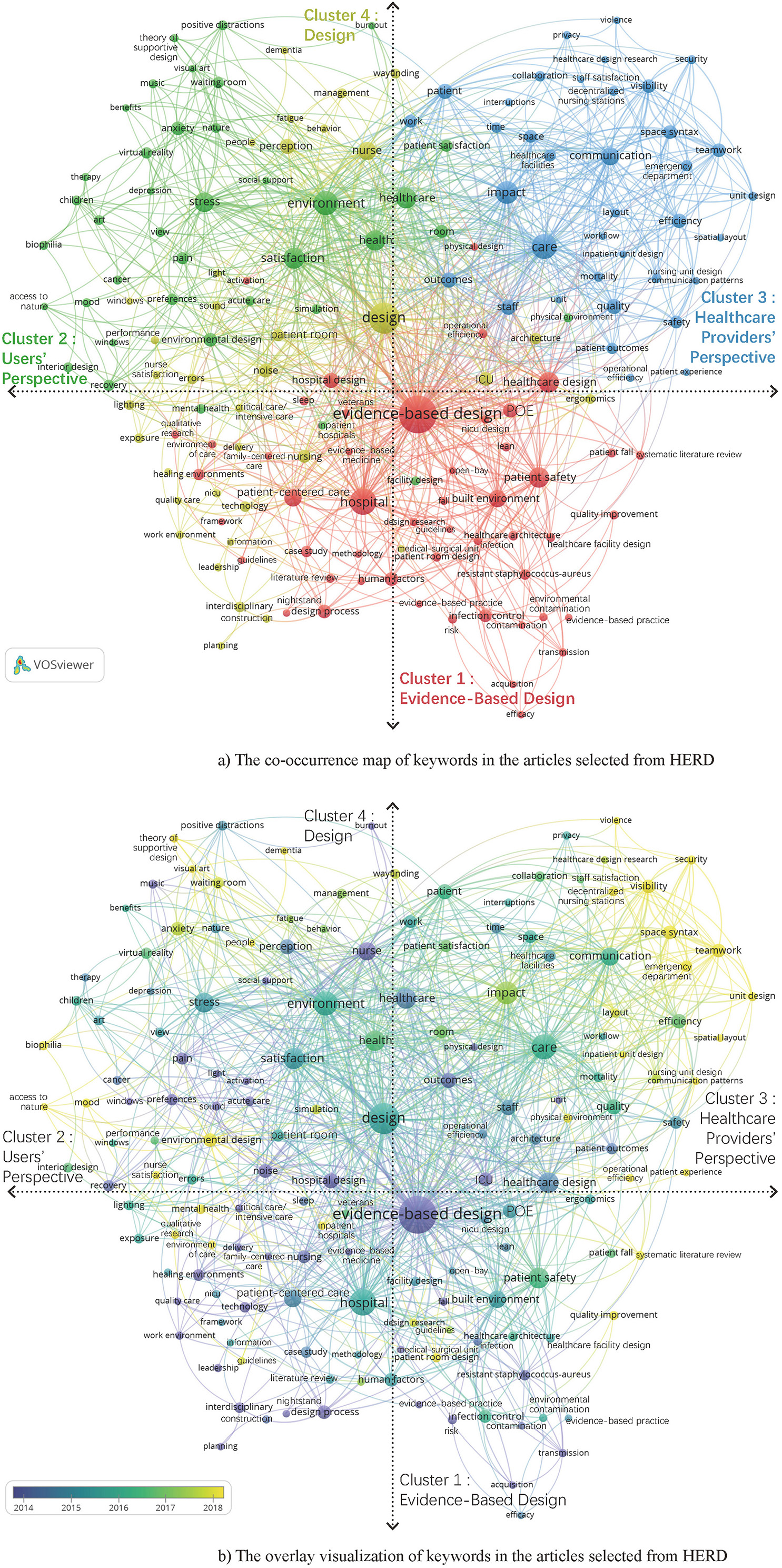
Figure 2. Keyword analysis of the articles selected from HERD. (A) The co-occurrence map of keywords in the articles selected from HERD. (B) The overlay visualization of keywords in the articles selected from HERD.
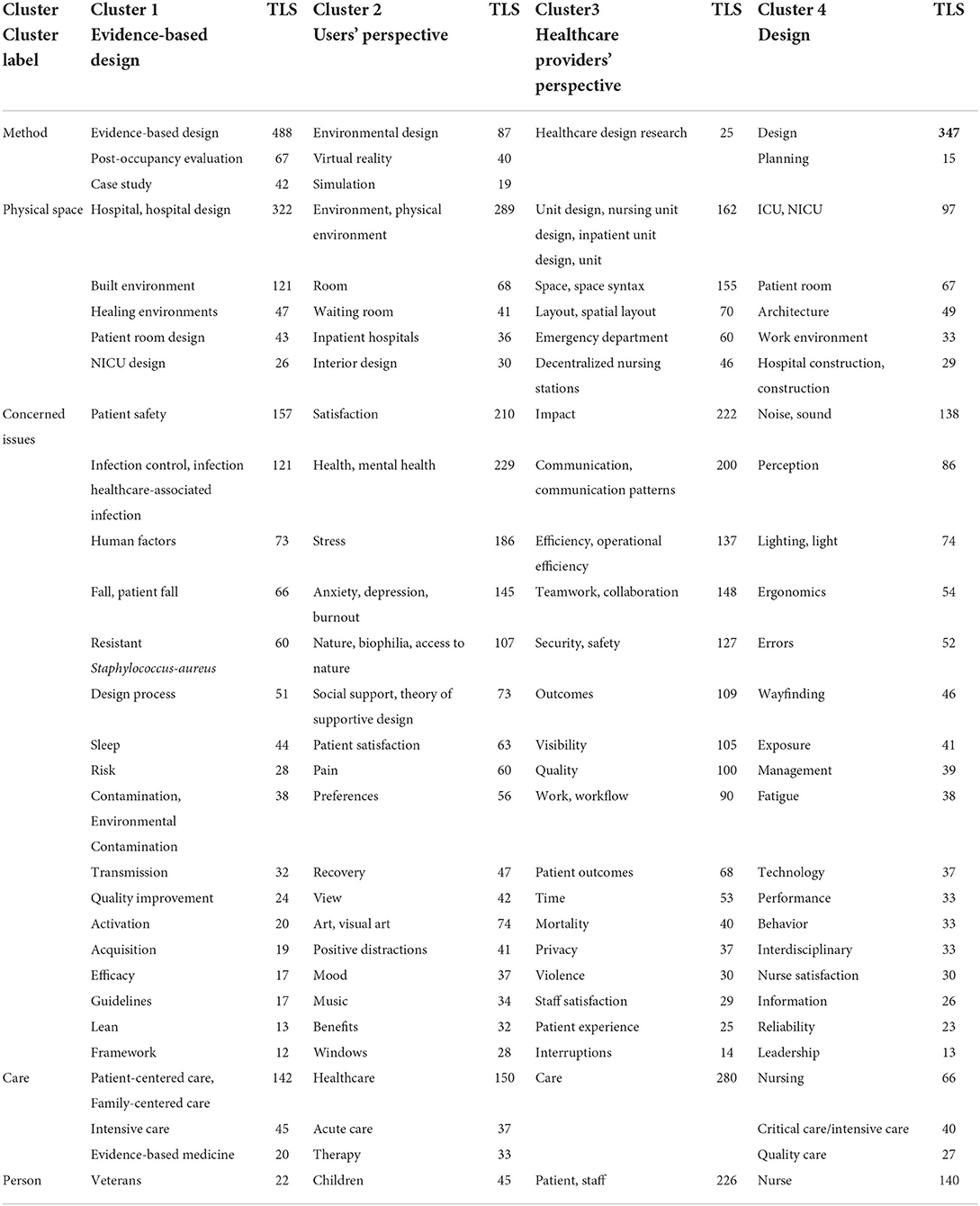
Table 2. Cluster analysis of keywords in the articles selected from HERD.
Cluster 1 labeled as Evidence-Based Design mainly includes the following aspects: (1) patient safety, fall, risk, sleep, and activation; (2) patient-centered care and family-centered care; (3) infection control, contamination, and transmission; (4) human factors, efficacy, and quality improvement, which are important issues for the research-based design of healthcare facilities.
Cluster 2 labeled as Users' Perspective mainly includes the following aspects: (1) satisfaction, particularly patient satisfaction; (2) preferences; (3) health, particularly mental health; (4) stress, anxiety, depression, burnout, pain, and mood; (5) nature, art, music, positive distractions, and social support.
Cluster 3 labeled as Healthcare Providers' Perspective mainly focuses on the environmental design of efficient and effective care in the nursing unit, emergency department, and so on. The main research topics include the following aspects: (1) impact, efficiency, outcomes, and quality; (2) communication, teamwork, and collaboration; (3) security, safety, visibility, and mortality; (4) work and workflow.
Cluster 4 labeled as Design mainly includes the following aspects: (1) noise, sound, lighting, and light; (2) perception, way-finding, and behavior; (3) ergonomics and errors; (4) nurse satisfaction, exposure, and fatigue; (5) management, performance, reliability, etc., which are the important issues for the general design of healthcare facilities.
Table 3 shows the most used keywords in the articles from HERD, with the occurrences, total link strength (TLS), and the clusters to which they belong. It can be found that cluster 1 has the most occurrences and TLS of keywords among the top 25 most frequently occurring keywords, followed by cluster 3. The results also indicate that EBD has a dominant position in the USA healthcare design, and the studies from Healthcare Providers' Perspective are still important even in the patient-centered era.
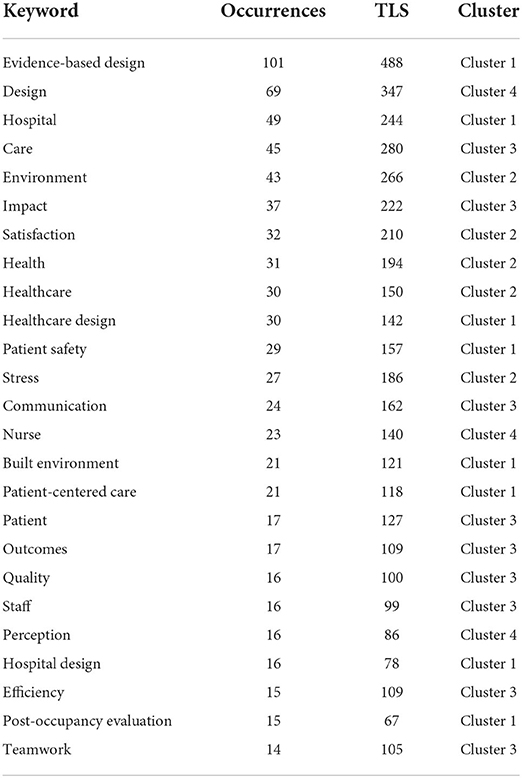
Table 3. Top 25 most frequently occurring keywords in the articles selected from HERD.
As shown in Figure 2B, the research hotspots represented by yellow color in the USA include the following: (1) using space syntax to study improving visibility and teamwork mainly in emergency departments (9–13); (2) reducing patients' anxiety by having access to nature, music, visual art, etc. mainly in a waiting room (14–17); and (3) nurses' satisfaction (18–21).
Figure 3A shows the co-occurrence map of keywords in the articles selected from AIJ Journals. All keywords are divided into nine clusters with nine colors. Nine tables in Figure 3A show the top five most frequently occurring keywords of each cluster, respectively. We combined the adjacent or relevant two or three clusters in Figure 3A into one cluster set.
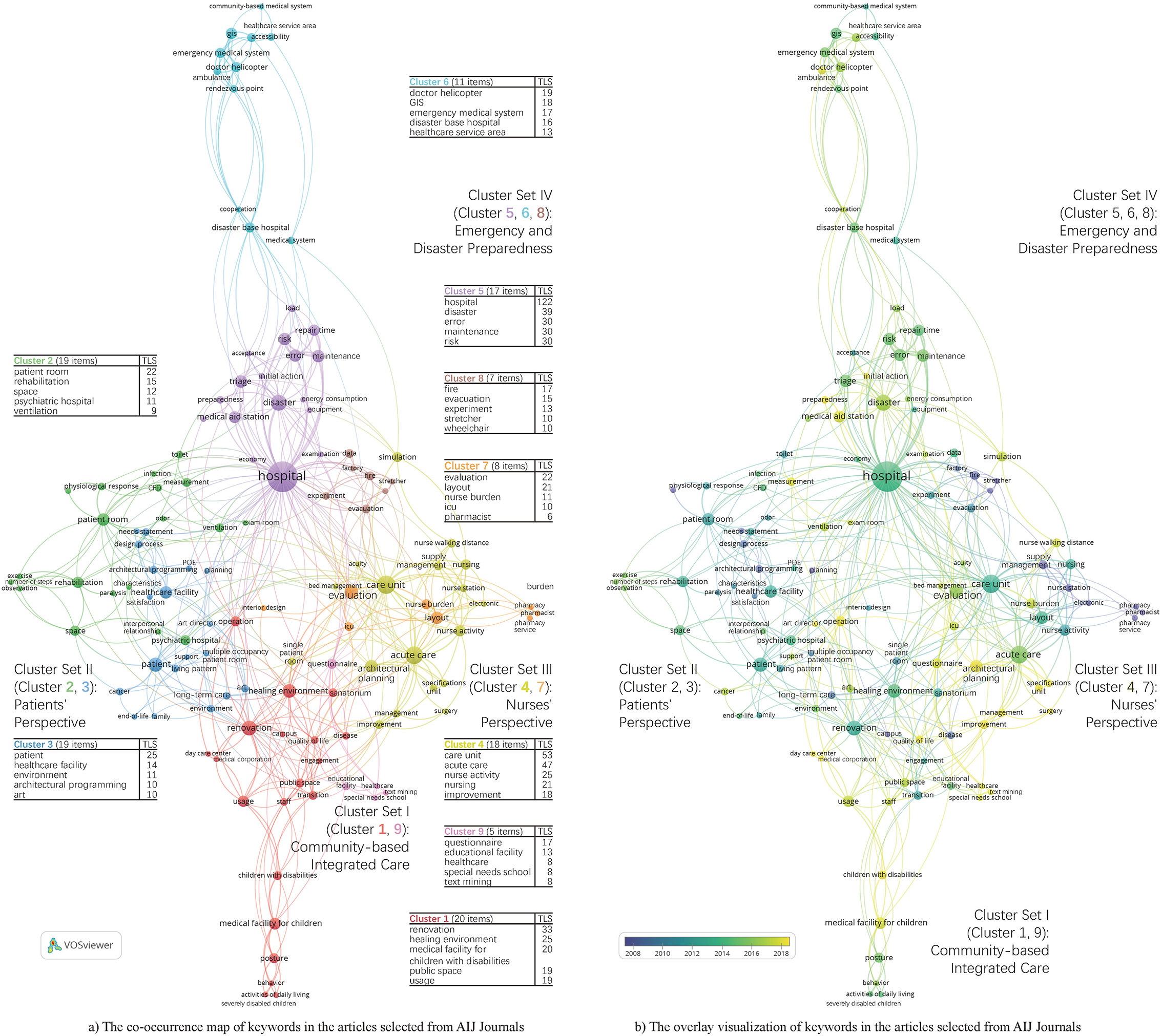
Figure 3. Keywords analysis of the articles selected from AIJ journals. (A) The co-occurrence map of keywords in the articles selected from AIJ journals. (B) The overlay visualization of keywords in the articles selected from AIJ Journals.
Cluster Set I labeled as Community-based Integrated Care includes cluster 1 and cluster 9. It mainly focuses on environmental design that contributes to the quality of life for the elderly (22, 23) and persons with disabilities or chronic diseases, especially children with disabilities (24–27) or ALS patients (28, 29), because the community-based integrated care system has been implemented in Japan since 2005.
Cluster Set II labeled as Patients' Perspective includes cluster 2 and cluster 3. The most frequently occurring keyword in cluster 2 is patient room (30–32) and that in cluster 3 is patient (33–35).
Cluster Set III labeled as Nurses' Perspective includes cluster 4 and cluster 7. It mainly focuses on the layout of the care unit, ICU, or pharmacy based on nurse activity, nursing, etc. to reduce nurse burden (36–39).
Cluster Set IV labeled as Emergency and Disaster Preparedness includes clusters 5, 6, and 8. It includes topics like earthquake (40–44), emergency (45–50), and fire (51, 52), etc.
Table 4 shows the most used keywords in the selected articles from AIJ Journals with the occurrences, TLS, clusters, and cluster sets to which they belong. It can be found that Cluster Set IV has the highest number of keywords among the top 25 most frequently occurring keywords, followed by Cluster Set III. Due to the frequent occurrences of natural disasters in Japan, Japanese researchers have done a lot of research related to Emergency and Disaster Preparedness. In addition, studies on optimum design based on analysis of nursing activities to improve efficiency have been paid much attention in Japan?
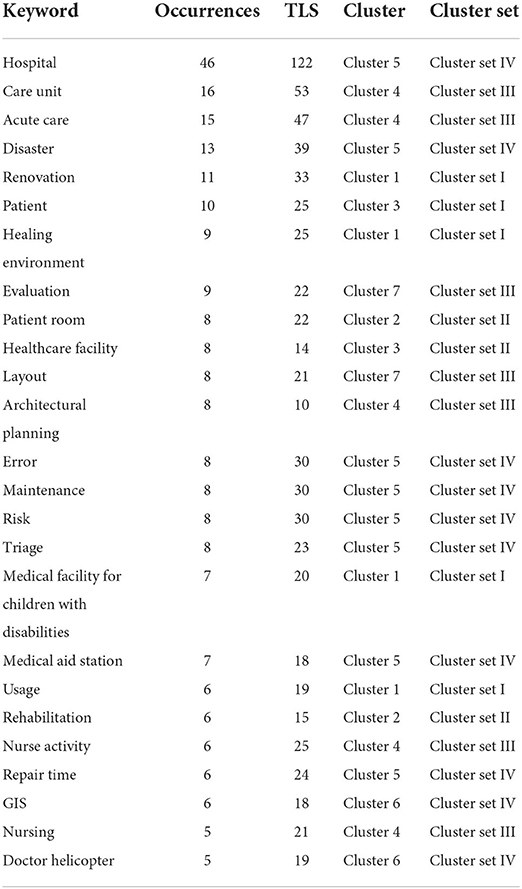
Table 4. Top 25 most frequently occurring keywords in the articles selected from AIJ journals.
As shown in Figure 3B, the research hotspots since 2018 in Japan include the following: (1) environmental design that contributes to the quality of life for children with disabilities in Cluster Set I; (2) the way to promote the widespread use of healing arts in the hospital (53) in Cluster Set II; (3) reducing nurse burden and walking distance through the reasonable layout of ICU and acute care unit in Cluster set III; and (4) optimizing the design of medical aid stations and improving the initial action system of disaster base hospital by careful preparedness in Cluster Set IV.
The 4 cluster/cluster set labels and the most frequently occurring keywords in the articles selected from HERD and AIJ Journals are shown in Figures 4A,B, respectively. It can be found that there are both similarities and differences in research related to healthcare facilities between the USA and Japan.
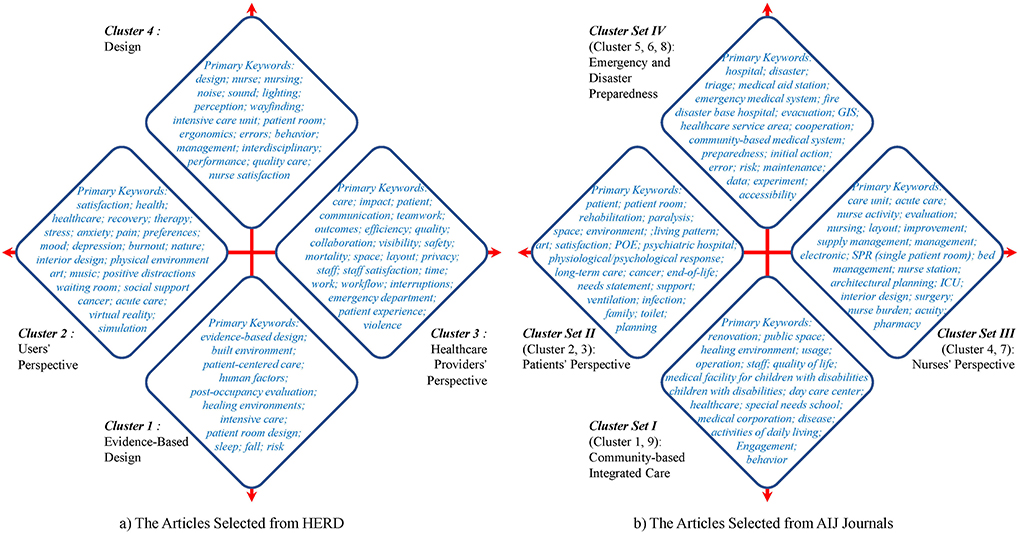
Figure 4. Comparative study on characteristics of four clusters or cluster sets between the USA and Japan. (A) The articles selected from HERD. (B) The Articles Selected from AIJ journals.
First, the two sides of the horizontal axis in Figure 4A represent the Users' Perspective and Healthcare Providers' Perspective, respectively, and the two sides of the horizontal axis in Figure 4B represent the Patients' Perspective and Nurses' Perspective, respectively. The research objects of the USA and Japan on the horizontal axis are similar, indicating that both users and healthcare providers are key research topics in healthcare facilities in different countries.
Second, the longitudinal axis in Figure 4A is quite different from that in Figure 4B. The upper and lower sides of the vertical axis in Figure 4A represent Design and EBD, respectively. The Design cluster focuses on general design issues, while the EBD cluster focuses on design issues that require in-depth study. The upper and lower sides of the vertical axis in Figure 4B represent Emergency and Disaster Preparedness and Community-based Integrated Care, respectively, because Japan is prone to many disasters and has an aging population.
The care unit design is taken as an example to further discuss the similarities and differences in healthcare design research between the USA and Japan, which is described in detail in the following section.
As one of the main means of reducing medical costs, the USA has paid great attention to research that can shorten the length of stay. The results published in HERD articles suggest that factors that can shorten the length of stay include sunlight (54), views of nature (54), patient-centered model of care (55), acute care unit for the elderly (56), adaptive healing room (57), expedient bariatric beds (58), therapeutic design (59), and proximal to the ward entrance (60, 61). Concentration or decentralization of nurse stations has no significant effect on the average length of stay (62, 63).
According to the Facility Guidelines 2006, the minimum bed area, the recommended bed area, and the bed area including family space are 120 ft2 (11.2 m2), 160 ft2 (14.9 m2), and 250 ft2 (23.2 m2), respectively (64). Research shows that accommodating patients in single-occupancy patient rooms (SPRs) instead of traditional MPRs (multi-bed patient rooms) can improve numerous healthcare outcomes, such as sleep quality, privacy, communication between patients and staff, satisfaction of patients and families, and reduce hospital-acquired infection rates, stress level, patient transfer, and length of stay (65).
The SPRs in the USA have been studied in depth on preventing patients from falling (66), family- and staff-supported spaces, etc. As shown in Figure 5, the typical US single PR has the following advantages: (1) short distance and few turns between beds and toilets for fall prevention; (2) comfortable family-supported space; and (3) staff-supported space for bedside care at ease (67). In addition, the design of the special patient rooms for the elderly (68) or terminal patients (69) has also been successful.
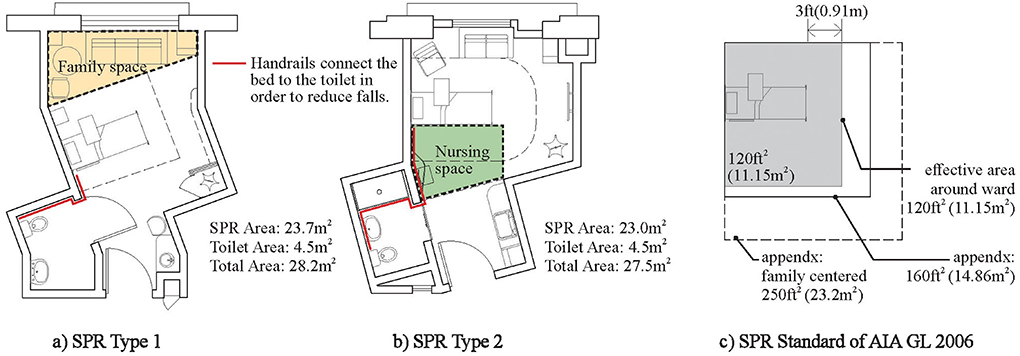
Figure 5. Typical SPRs in the USA. (A) SPR Type 1. (B) SPR Type 2. (C) SPR Standard of AIA GL 2006.
However, the construction standard of SPRs in the USA, especially the acuity-adaptable SPRs (70, 71) developed to reduce intra-hospital patient transfer, is too high to control medical costs.
Healthcare providers, especially nurses, experience a high level of work stress (54). Studies that examine how the physical environment contributes to reducing staff stress are very significant. The relationships between nurses' stress and physical elements, such as exterior views, daylighting, lighting, color, spatial color patterning, and noise control, were widely discussed (20, 54, 72–75). The thoughtful design of the lighting environment can improve nurses' satisfaction (21, 76). The restorative quality of break areas may significantly improve nurses' satisfaction and stress reduction, potentially leading to improved care for the patients they serve (77). The layout design that can reduce nurse walking or enhance teamwork in care units can improve nurses' satisfaction (18, 78).
Single-bed ICU design was associated with higher levels of stress for ICU nurses (79), and the single-family room model in the NICU can cause staff members to feel isolated from one another and reduce their ability to respond quickly in a crisis situation (80).
General hospital beds in Japan are divided into four categories: intensive care beds, acute care beds, convalescent care beds, and chronic care beds. The average length of stay of the first three types of beds reached 16 days, which is much higher than that of European and American countries. With the aging of the population, Japan has been reducing the proportion of acute care beds and increasing the proportion of convalescent care beds while reducing the total number of hospital beds. According to Japan's regional medical care vision, acute care beds will fall from 48% in 2015 to 34% in 2025, while convalescence care beds will rise from 10 to 31% (81).
There are four articles on ICU (37), 17 articles on acute care unit (39), and six articles on convalescent care unit (82) in AIJ articles, respectively. These articles mainly aim at how to offer more suitable care and built environment for the treatment of intensive, acute, and convalescent care patients in order to create a coordinated, seamless medical system.
Both SPRs and MPRs have their own advantages and disadvantages. Despite the disadvantages of poor patient privacy, the MPRs are cheap, short in nurse walking, and convenient for nursing observation and nursing collaboration. Unlike all SPRs adopted in the US hospitals, MPRs still account for a considerable proportion in Japanese hospitals. Especially in recent years, Japan's four-bed PRs have shown many new characteristics by absorbing the traditional advantages of SPRs. As shown in Figures 6A,C, with an individual territory and window for each patient, it is not only convenient for nursing observation and patient transfer but also avoids sight interference between patients effectively (83). At the same time, the average bed area, length of the corridor, and nurse walking do not increase significantly.
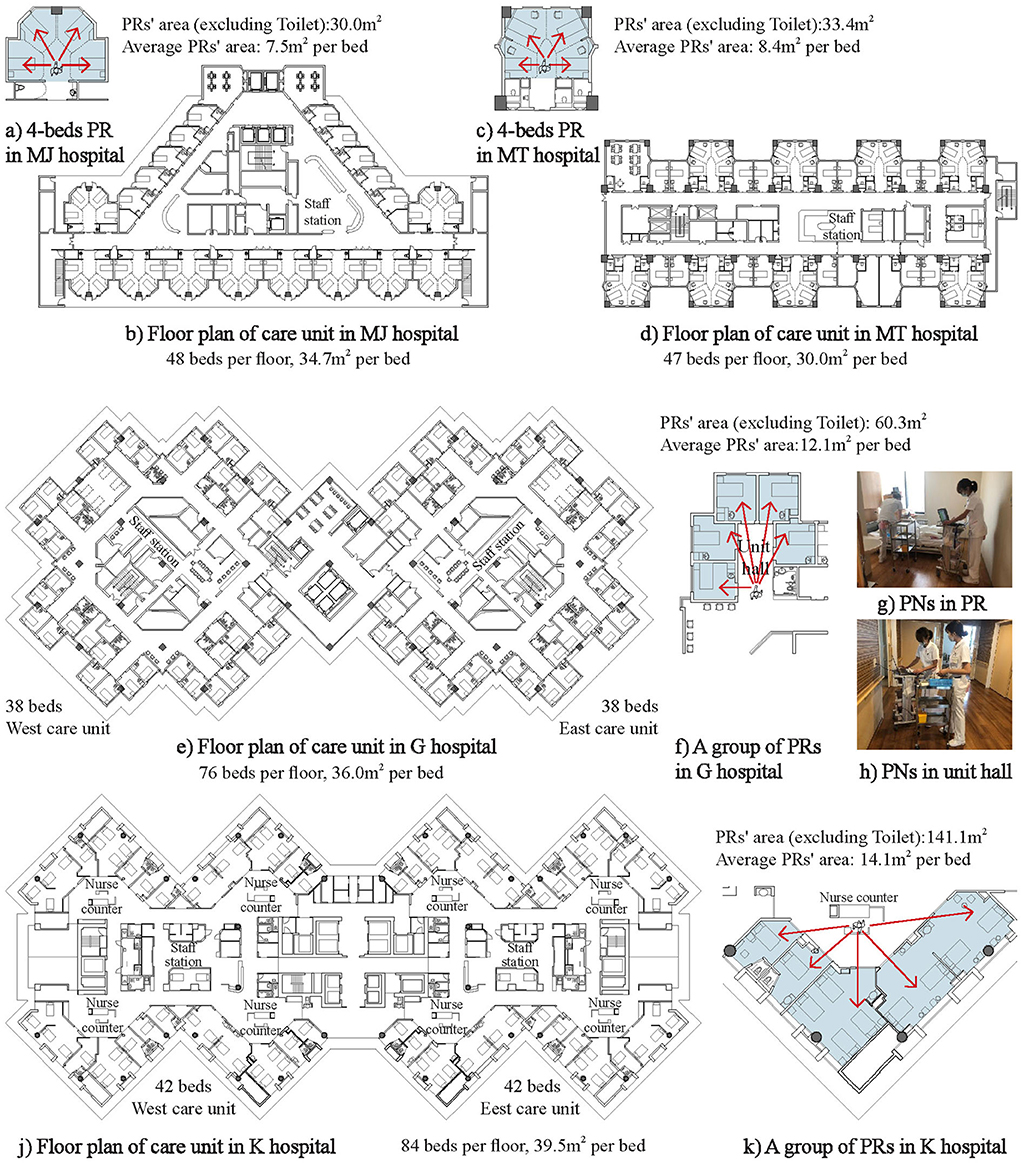
Figure 6. Typical patient rooms in Japan. (A) 4-beds PR in MJ hospitalin hospital PRs' area (excluding Toilet):30.0m2, Average PRs' area: 7.5m2 per bed. (B) Floor plan of care unit in MJ hospital 48 beds per floor, 34.7m2 per bed. (C) 4-beds PR in MT hospital PRs' area (excluding Toilet):33.4m2 Average PRs' area: 8.4m2 per bed. (D) Floor plan of care unit in MT hospital 47 beds per floor, 30.0m2 per bed. (E) Floor plan of care unit in G hospital 38 beds West care unit 38 beds East care unit 76 beds per floor, 36.0m2 per bed. (F) A group of PRs in G hospital PRs' area (excluding Toilet): 60.3m2 Average PRs' area:12.1m2 per bed (G) PNs in PR. (H) PNs in unit hall. (J) Floor plan of care unit in K hospital.84 beds per floor, 39.5m2 per bed 42 beds West care unit 42 beds East care unit (K) A group of PRs in K hospital PRs' area (excluding Toilet):141.1m2 Average PRs' area: 14.1m2 per bed.
In Japan, critically ill patients who require close observation are usually placed near the nurse's station and then transferred when the patient's condition improves. In order to reduce the nurses' burden due to patient transfer, some Japanese hospitals have adopted SPRs with lower standards and close to the nurse station (Figure 6E) (84, 85), which can take into account the privacy of patients and the convenience of staff.
Studies on nurse activities have always been concerned in Japan (86). Especially in recent years, due to the wide application of Hospital Information System (HIS) and Supply, Processing, and Distribution (SPD) System, the improvement in the nursing system and the increase in the number of SPRs have had a great impact on nurse walking. The main related research results are as follows.
Only the decentralized nurse stations equipped with HIS (87, 88) and the corresponding medical supplies system (89) can play roles in shortening the walking distance of nurses. The walking distances of two nurses are used as an evaluation index of the Partnership Nursing System (PNS) to discuss the level of equality as an equal nursing partner (84).
Unlike the traditional follow-up survey, many new technologies have been applied in the study of nurse activities in recent years. For example, ultrasound positioning technology has been used to collect data on nursing activities consecutively for 1 week (90), and BIM technology is used to optimize the bed position of inpatients and simulate the walking distance of nurses (84, 91).
Overall, the USA studies of care units focus on the healthcare environment that could shorten the length of stay and improve patient and staff satisfaction, while Japan focuses on the spatial layout to improve the efficiency and effectiveness of nursing care. Taking patient satisfaction as an example, there have been 90 related articles in HERD since 2007, accounting for 26.9% of the total, while there are only two related articles in AIJ Journals, accounting for 1.3% of the total.
Research goals are also significantly different between the USA and Japan. In the case of studies related to the physical environment, such as indoor environment or view outside the window, most Japanese studies just stay at the level of reducing patient or staff stress and anxiety, while American studies will even achieve the level of performance, such as healing effects or length of stay (64).
As for research methods, EBD occupies a central place in the USA, while Japanese architectural planning mainly refers to POE analysis or computer simulation based on field surveys.
As shown in Table 5, from the perspective of medical costs, the number of doctors (92) and nurses (93) per 1,000 inhabitants in the USA and Japan are almost the same, while the average length of stay in acute care beds (94) and the number of acute care beds per 1,000 inhabitants (95) in Japan are much higher than those in the USA. On the other hand, from the perspective of medical benefits, Japan's medical costs as a proportion of total health spending in GDP (1) are much lower than those in the USA, but the average life expectancy (96) is much higher than that of the USA. It is not so difficult to find that the Japanese healthcare system is more cost-effective than that of the USA just by doing a simple cost-benefit calculation. Of course, the reasons behind the above phenomenon are very complex, and the following analyses of healthcare facilities are made by introducing the concept of value variables.
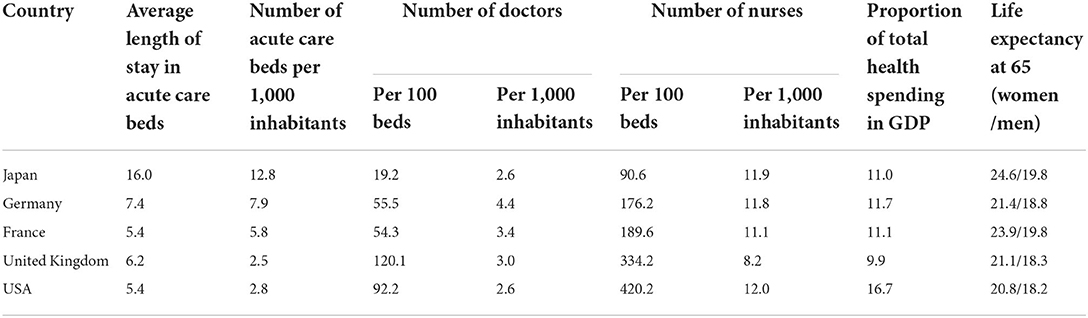
Table 5. OECD data (2019).
As mentioned above, the research topics and solutions for the healthcare environment with limited medical resources are quite different in the USA and Japan. Through further comparative study between the USA and Japan, we found that time variables such as length of stay, space variables such as bed area and the number of care units per floor, and behavior variables such as nurse activities and nurse system play key roles in care unit design. In this paper, these variables are defined as value variables (Table 6).
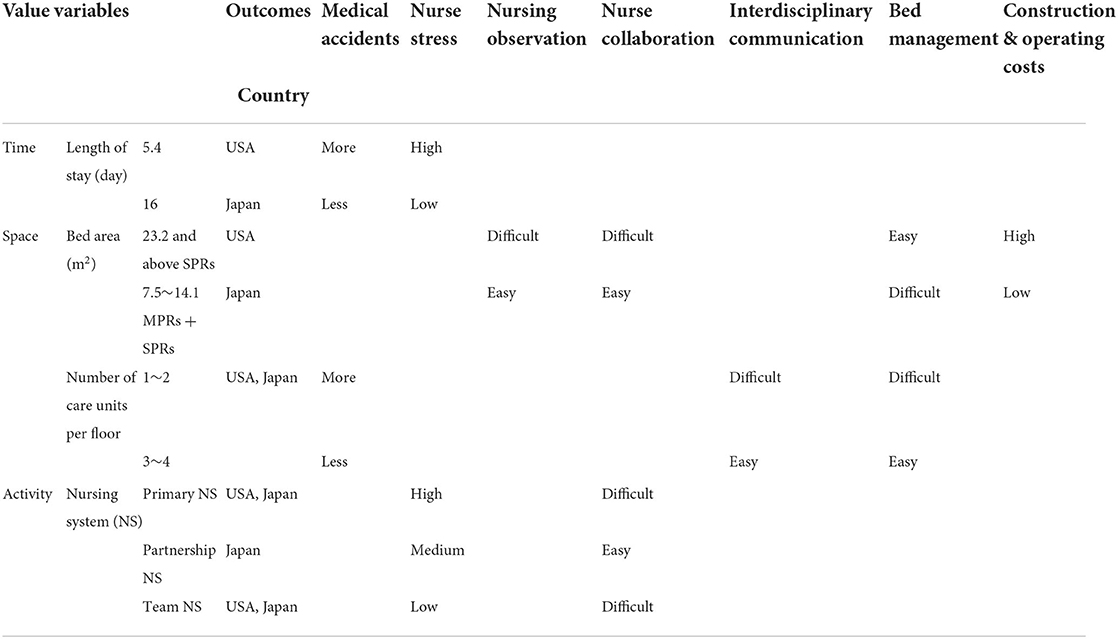
Table 6. Summary of the relationships between value variables and outcomes.
First, we discuss the length of hospital stay. The average length of hospital stay in acute beds has fallen from 8.3 days in 1969 to 5.4 days in 2019 in the USA and from 34.4 days in 1994 to 16.0 days in 2019 in Japan in order to cut medical costs (94). We found that when the length of hospital stay falls below a certain threshold, there will be significant changes in the type of patient rooms, the layout of care units, the nursing system, and so on. When the average length of hospital stay is long enough, progressive patient care is considered as an efficient way (97), and it is better to divide the care units into different types, such as intensive care unit, step-down care unit, and acute care unit in order to offer more suitable care and environment for the corresponding type of patients. On the contrary, when the average length of hospital stay is quite short and inpatients become relatively serious, not only does the classification of care units have little significance, but it is also advisable to use all SPRs in care units (66). However, if the average length of hospital stay falls too short, it may lead to a significant increase in the length of the nurse walking, the difficulties of nursing observation, and nurse stress, which will increase the construction and operating costs of the hospital.
Second, the minimum bed area of acute care units is 6.4 m2/bed in Japan, which is only half of the AIA standard (64). In addition, the average number of beds in acute care units in Figure 6 is usually about 42 beds, and the average area of the acute care units is about 1,520 m2. The care unit in Japan is more compact compared with that in the USA, which is conducive to shortening the nurse walking and improving the effect of nursing observation and nurse communication. It should be noted that although the bed area in Japan is not large, it does not seem to have any adverse effects on the quality of care or safety (64). Therefore, it is necessary to re-examine the suitable size of the bed area.
Japan has advantages in the nursing system. For example, PNS is a popular nursing system with a pair of two nurses working together to provide care to patients. It can help nurses learn from each other and reduce stress and errors, thereby improving safety and quality. However, PNS needs to be bound closely to the care unit planning. It is necessary to increase the bed area (Figure 6G) and outdoor staff-supported space (Figures 6F,H,K) appropriately because there are always two nurses working together (84, 85, 98).
Using value variables can help us understand or solve problems in healthcare design from three dimensions of time, space, and behavior rather than just one of them. Otherwise, it is easy to create more new problems in order to solve some problems, which will bring unnecessary complexity. For example, cutting medical costs simply by shortening the length of hospital stay may lead to the all-use of SPRs, which may eventually backfire. In addition to the indoor environment, the nursing system can also be taken into account to reduce nurse stress, which may require only small changes in the care unit planning.
The intent of EBD is to base the design decisions on credible studies of healthcare facilities. However, environment design variables used in EBD, such as windows, SPRs, and comfortable waiting rooms, are useful during the phase of design development or interior design, but not during the schematic design phase.
In the schematic design phase, the items like building shapes or traffics, which are needed to be determined by architects, are more closely related to the value variables, such as length of stay, number of care units per floor, and the nursing system.
The effect of healthcare design depends largely on the architect's comprehensive judgment from a macro-perspective, while the healthcare facility research represented by EBD mainly explores the relationship between environmental variables and specific outcomes from the micro-level. As the importance of evidence is different in different scenarios, evidence choice according to the actual situation is important for healthcare design. In order to cover the gap between healthcare design and research, we propose a framework for the value-based design of healthcare facilities from the meso-level on the basis of EBD and Japanese architectural planning (Figure 7).
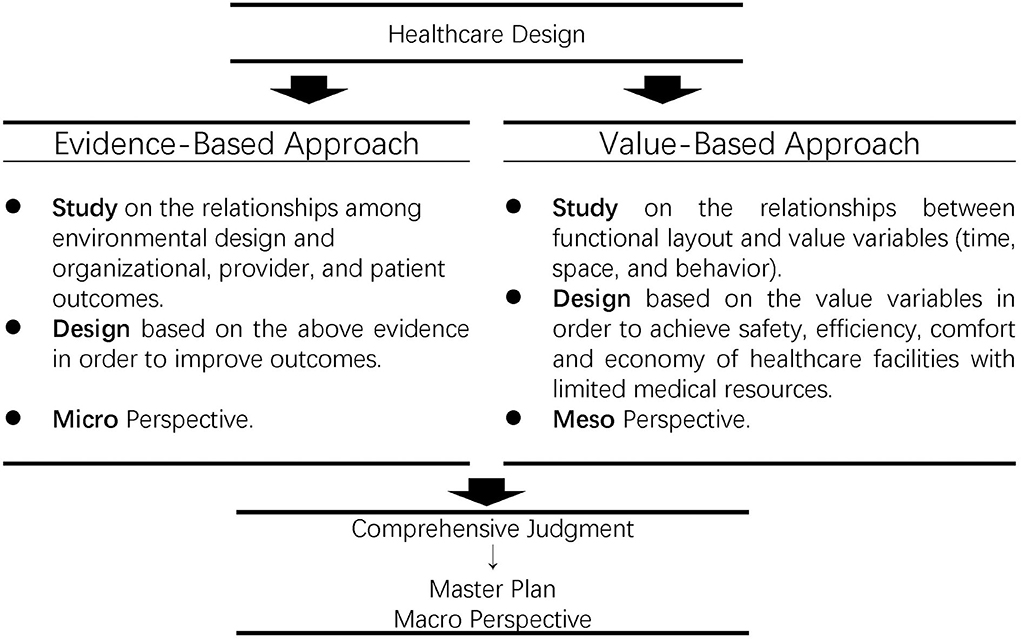
Figure 7. Conceptual framework of value-based design.
In this paper, value-based design is defined as the master planning and evidence choice through value variables (time, space, and behavior) to balance safety, efficiency, comfort, and economy in healthcare facilities with limited medical resources.
As shown in Figure 8A, instead of the usual two care units per floor, there are four care units per floor in Y hospital with 655 beds in total. According to this spatial variable, an open public space for an interdisciplinary team Figure 8B is designed in the center of the floor to facilitate formal or informal communication among different specialized professionals involved in healthcare with the overarching goal of improving the safety and quality of patient care.
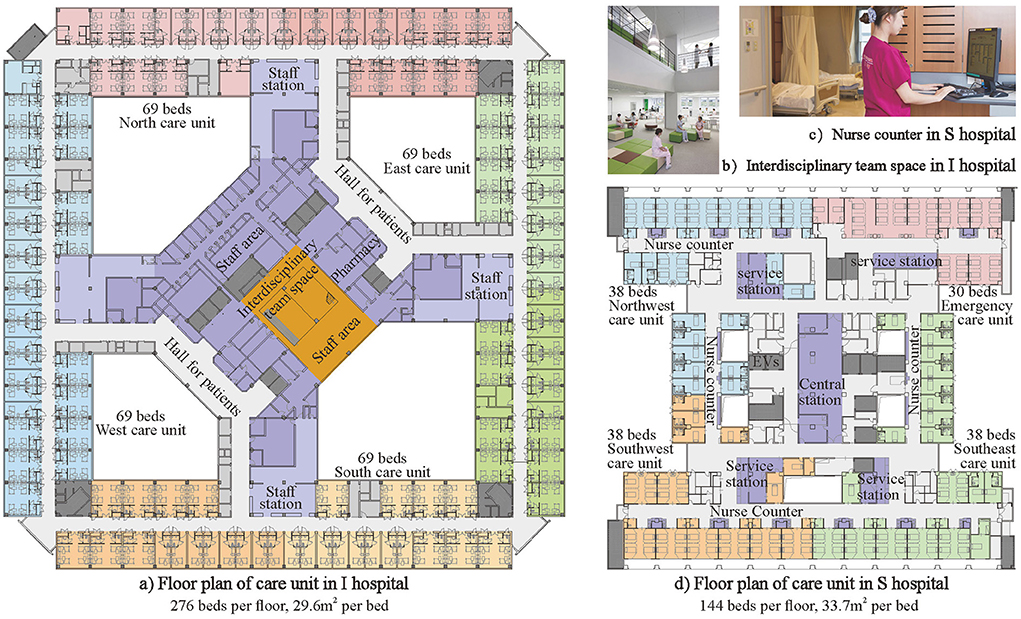
Figure 8. Four care units on one floor. (A) Floor plan of care unit in I hospital 276 beds per floor, 29.6m2 per bed. (B) Interdisciplinary team space in I hospital. (C) Nurse counter in S hospital. (D) Floor plan of care unit in S hospital 144 beds per floor, 33.7m2 per bed.
As shown in Figure 8D, Hospital S is a cardiology hospital with four care units per floor. Because heart disease is a high mortality disease and some heart attacks strike suddenly, the value variable of emergency time needs to be comprehensively considered together with the space and behavior value variables in a hospital design. Therefore, in terms of space, four nursing units are combined into one management unit to flexibly adjust the number of beds in each nursing unit. In addition, in terms of behavior, nursing activities are divided into three categories, such as office work, drug preparation, and bedside nursing. One central station, four service stations, and multiple nurse counters (Figure 8C) are designed in the according location for efficient three levels of care.
1) The comparative study of the keywords of HERD and AIJ articles can help researchers and designers to grasp the research system of health facilities in the USA and Japan as a whole and to clarify the position of one research topic in the system and the relationship with other research topics.
2) The USA and Japan have their own strengths in the study of healthcare facilities. EBD occupies a central place in the USA, focusing on revealing the micro-mechanisms between environmental variables and healthcare outcomes. The architectural planning approach adopted in Japan focuses on the relationship between hospital layout and improving care processes, increasing medical efficiency, and reducing health care costs.
3) The differences reflected in the solutions of American and Japanese hospitals in controlling medical costs can be well explained by introducing three kinds of meso-level value variables of time, space, and behavior. Value-based design that combines the advantages of healthcare design in the USA and Japan can largely bridge the gap between macro master plans and micro evidence, which can help architects select, integrate, and absorb the most appropriate research results in healthcare design.
4) Through the coordination between different types of value variables, the concepts and methods of value design help to achieve the balance of safety, efficiency, comfort, and economy of healthcare facilities under limited medical resources.
5) The differences in the value of value variables in different countries reflect the different cultural concepts and value orientations behind them, and the understanding of this point can help architects in developing countries to learn from the experience of developed countries.
6) The limitation of this paper is that it only discusses the value variables of the inpatient department, and further study is required for the outpatient department and the medical technology department. The authors also hope to take this study as an opportunity to trigger more discussions in the academic community.
YZ and YS conceived and designed the analysis, collected the data, performed the analysis, and wrote the paper. YX contributed to figure preparation. HY collected some data. All authors contributed to the article and approved the submitted version.
This research was supported by the National Natural Science Foundation of China (Grant No. 51978143) and the Healthy Building Industry Technology Strategic Alliance.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. OECD. Health spending (indicator). (2022). Available online at: https://data.oecd.org/healthres/health-spending.htm#indicator-chart (accessed July 25, 2022).
2. Graban M, Toussaint J. Lean Hospitals: Improving Quality, Patient Safety, and Employee Engagement, Third Edition 3rd Edition. New York, NY: Productivity Press (2016).
3. Porter ME, Teisberg EO. Redefining Health Care: Creating Value-Based Competition on Results. Boston, MA: Harvard Business School Press (2006).
4. Rama A. National Health Expenditures, 2019: Steady Spending Growth Despite Increases in Personal Health Care Expenditures in Advance of the Pandemic. Available online at: https://www.ama-assn.org/system/files/2021-05/prp-annual-spending-2019.pdf (accessed July 25, 2022).
5. Hamilton DK. The four levels of evidence-based practice. Healthc Des. (2003) 3:19–26. https://healthcaredesignmagazine.com/architecture/four-levels-evidence-based-practice/
6. Nagasawa Y. Global Hospitals in 2050—a review of the historical development of hospital building studies from a global perspective. Japan Archit Rev. (2020) 3:5–24. doi: 10.1002/2475-8876.12131
7. Stichler JF, Hamilton DK. Welcome from the editors of HERD. HERD HERD. (2007) 1:4–4. doi: 10.1177/193758670700100101
8. AIJ Journals. Available online at: https://www.aij.or.jp/eng/journal/journal.html (accessed July 25, 2022).
9. Ahmadpour S, Bayramzadeh S, Aghaei P. Efficiency and teamwork in emergency departments: perception of staff on design interventions. HERD. (2021) 14:310–23. doi: 10.1177/19375867211023156
10. Gharaveis A, Hamilton DK, Pati D, Shepley M. The impact of visibility on teamwork, collaborative communication, and security in emergency departments: an exploratory study. HERD. (2018) 11:37–49. doi: 10.1177/1937586717735290
11. Lim L, Kanfer R, Stroebel RJ, Zimring CM. The representational function of clinic design: staff and patient perceptions of teamwork. HERD. (2021) 14:254–70. doi: 10.1177/1937586720957074
12. Gharaveis A, Pati D, Hamilton DK, Shepley M, Rodiek S, Najarian M. The influence of visibility on medical teamwork in emergency departments: a mixed-methods study. HERD. (2020) 13:218–33. doi: 10.1177/1937586719885376
13. Gharaveis A, Hamilton DK, Pati D. The impact of environmental design on teamwork and communication in healthcare facilities: a systematic literature review. HERD. (2018) 11:119–37. doi: 10.1177/1937586717730333
14. Fenko A, Loock C. The influence of ambient scent and music on patients' anxiety in a waiting room of a plastic surgeon. HERD. (2014) 7:38–59. doi: 10.1177/193758671400700304
15. Lai JCY, Amaladoss N. Music in waiting rooms: a literature review. HERD. (2022) 15:347–54. doi: 10.1177/19375867211067542
16. Cartland J, Ruch-Ross HS, Carr L, Hall A, Olsen R, Rosendale E, et al. The role of hospital design in reducing anxiety for pediatric patients. HERD. (2018) 11:66–79. doi: 10.1177/1937586718779219
17. Sjölander A, Jakobsson Ung E, Theorell T, Nilsson Å, Ung KA. Hospital design with nature films reduces stress-related variables in patients undergoing colonoscopy. HERD. (2019) 12:186–96. doi: 10.1177/1937586719837754
18. Obeidat B, Younis MB, Al-Shlool E, Alzouby A. A study of workspace design characteristics exemplified by nurses' satisfaction within three intensive care units in a University Hospital. HERD. (2022) 15:63–78. doi: 10.1177/19375867211055731
19. Jalalianhosseini M, Freihoefer K, Doyle N, Simpson A. The impact of infusion center layout on workflow and satisfactions in two cancer infusion centers: a case study on staff and patients. HERD. (2020) 13:70–83. doi: 10.1177/1937586719888221
20. Gharaveis A, Yekita H, Shamloo G. The perceptions of nurses about the behavioral needs for daylighting and view to the outside in inpatient facilities. HERD. (2020) 13:191–205. doi: 10.1177/1937586719851271
21. Davis RG, McCunn LJ, Wilkerson A, Safranek S. Nurses' satisfaction with patient room lighting conditions: a study of nurses in four hospitals with differences in the environment of care. HERD. (2020) 13:110–24. doi: 10.1177/1937586719890940
22. Nakazono M, Mishima S, Setoguchi K, Yamamoto S. Case study on the establishment and management of welfare facilities for the elderly by medical corporation in Hagi city part 2: usage of day and preventive care service facilities converted wooden houses. J Archit Plan. (2021) 86:717–26. doi: 10.3130/aija.86.717
23. Nakazono M, Mishima S, Setoguchi K, Ushijima A. Case study on the establishment and management of welfare facilities for the elderly by medical corporation in Hagi city part 1: Management of day and preventive care service facilities converted wooden houses. J Archit Plan. (2020) 85:849–58. doi: 10.3130/aija.85.849
24. Bae M, Takemiya K, Fujiwara Y. Usefulness of the new layout at center K. J Archit Plan. (2020) 85:829–36. doi: 10.3130/aija.85.829
25. Bae M, Takemiya K. A study on entrance situation and facility support for dealing with children with multiple disabilities who need special medical care in medical type facilities for children with disabilities. AIJ J Technol Des. (2020) 26:649–54. doi: 10.3130/aijt.26.649
26. Yamawaki H, Miura K, Takada M. The use characteristics of the residential space of facilities for children with disabilities from the view point of their play behavior. J Archit Plan. (2017) 82:1893–903. doi: 10.3130/aija.82.1893
27. Sugawara M, Suzuki T. Environment management by teachers for improving facilities at schools for special needs education from the perspective of medical care. J Archit Plan. (2018) 83:385–95. doi: 10.3130/aija.83.385
28. Kameya E, Adachi K. Study of the restoration process of the living environments of bereaved families that had undertaken long-term at-home care for ALS patients. J Archit Plan. (2015) 80:2753–61. doi: 10.3130/aija.80.2753
29. Kameya E, Kanno M, Yamamoto K, Onoda Y, Sakaguchi T. A case study on environment for convalescence for the inpatient of ALS in welfare-home. J Archit Plan. (2009) 74:339–45. doi: 10.3130/aija.74.339
30. Kosuge R, Kobayashi K, Kakehi A. Comparative studies on hospital-bed management between all single-room wards and mixed multi-bed room wards. J Archit Plan. (2013) 78:765–73. doi: 10.3130/aija.78.765
31. Ogata M, Iijima M, Matsumura M, Tsutsumi H, Hori S, Tanabe SI. Environmental surface contaminaion examined by atp assay before and after terminal room cleaning in patient rooms. J Environ Eng. (2016) 81:723–9. doi: 10.3130/aije.81.723
32. Itakura T, Mitsuda M. Research on the level of odor in a patient room of the hospital. J Environ Eng. (2008) 73:327–34. doi: 10.3130/aije.73.327
33. He X, Miyazaki T, Miura K. The actual conditions of activity of patient in recovery period rehabilitation ward positioned the hospitalization life whole in rehabilitation. J Archit Plan. (2015) 80:495–504. doi: 10.3130/aija.80.495
34. Yamamoto T, Yanase R. A study on behavior of inpatients and spatial characteristic in convalescence rehabilitation wards. J Archit Plan. (2015) 80:1745–51. doi: 10.3130/aija.80.1745
35. Yan S. A study on the meaning of place and the space recognition process of psychiatric patients. J Archit Plan. (2013) 78:35–43. doi: 10.3130/aija.78.35
36. Kamiya H, Yamada A, Yamashita T, Satoh E. Pre-investigation on the relations between hospital ward planning and nurses' burden-feeling. AIJ J Technol Des. (2014) 20:677–82. doi: 10.3130/aijt.20.677
37. Murakawa M, Kurasawa S, Yamada A. Study on the relationship between nursing burden feeling and plan of advanced acute-phase-wards. J Archit Plan. (2020) 85:505–15. doi: 10.3130/aija.85.505
38. Kamiya H, Satoh E, Kumakawa T, Yamada A, Matsushita D. Analysis on relationship between nurses' burden feeling and travel distance: a case study in 3 department in hospital S. AIJ J Technol Des. (2015) 21:237–42. doi: 10.3130/aijt.21.237
39. Murakawa M, Yamada A. A case report on nurses' burden-feeling in acute hospital having distinctive inpatient quarters plan. AIJ J Technol Des. (2021) 27:841–6. doi: 10.3130/aijt.27.841
40. Tatebe K, Tamura K, Takahashi I, Nozawa H. A comparison of disaster base hospitals and general hospitals with regard to initial action in an earthquake. J Archit Plan. (2019) 84:2109–17. doi: 10.3130/aija.84.2109
41. Inagaki K, Sadohara S. Building power equipment and disaster management during blackout in disaster base greater Tokyo area. AIJ J Technol Des. (2015) 21:1153–6. doi: 10.3130/aijt.21.1153
42. Sato G, Nagasawa Y, Kakehi A, Murakami M, Kubo T, Yamashita T. Planning of providing front line disaster medical service bases according to the estimation of the number of non-residential casualties around Shinjuku station in the case of metropolitan Tokyo earthquakes. J Archit Plan. (2012) 77:2749–55. doi: 10.3130/aija.77.2749
43. Murayama T, Kojima T, Egawa K, Ando S, Yoda I, Yamashita T, et al. study on arrangement of functions of first-aid medical stations based in elementary school. J Archit Plan. (2017) 82:2277–83. doi: 10.3130/aija.82.2277
44. Tatebe K, Tamura K, Takahashi I. Initial responses of hospitals to the 2011 pacific coast Tohoku earthquake. J Archit Plan. (2018) 83:375–83. doi: 10.3130/aija.83.375
45. Egawa K, Yoda I, Yamashita T. Study on the method of management of emergency medical aid station. AIJ J Technol Des. (2016) 22:1073–8. doi: 10.3130/aijt.22.1073
46. Yamada S, Ohuchi H, Oikawa K. Facility location planning of medical helicopters and rapid response cars. J Archit Plan. (2016) 81:2775–85. doi: 10.3130/aija.81.2775
47. Kojima S, Shimazaki S, Ohuchi H. Visualization of the sphere of medical emergency and services achievable by means of inter-regional cooperation. AIJ J Technol Des. (2017) 23:725–30. doi: 10.3130/aijt.23.725
48. Yamada S, Yoshikawa Y, Oyama T, Ohuchi H, Oikawa K. Visualization method for effective operation of helicopter emergency medical service and facility site planning. J Archit Plan. (2013) 78:2163–72. doi: 10.3130/aija.78.2163
49. Makinouchi M, Uno A, Ohuchi H. Empirical study on the existing area by collaboration of air ambulance and emergency vehicles for the emergency medical system. J Archit Plan. (2015) 80:1159–68. doi: 10.3130/aija.80.1159
50. Tajima M, Kikuchi H, Ohuchi H. Study on optimal location planing using regional information in emergency medical system. J Archit Plan. (2008) 73:1929–37. doi: 10.3130/aija.73.1929
51. Satoh H, Murai H, Kurioka H, Shida K. A study on method of evaluating fire safety in factory and hospital/nursing home. AIJ J Technol Des. (2009) 15:773–8. doi: 10.3130/aijt.15.773
52. Tsuchiya S, Hasemi Y. Characterization of group aided-evacuation in hospital ward. J Archit Plan. (2009) 74:1271–6. doi: 10.3130/aija.74.1271
53. Takano S, Suzuki K-I. A study on the issues of the spread and operation of healthcare art in medical facilities. J Archit Plan. (2021) 86:449–58. doi: 10.3130/aija.86.449
54. Ulrich RS, Zimring C, Zhu X, DuBose J, Seo H-B, Choi Y-S, et al. A review of the research literature on evidence-based healthcare design. HERD HERD. (2008) 1:61–125. doi: 10.1177/193758670800100306
55. Stone S. A retrospective evaluation of the impact of the planetree patient-centered model of care on inpatient quality outcomes. HERD. (2008) 1:55–69. doi: 10.1177/193758670800100406
56. Krall E, Close J, Parker J, Sudak M, Lampert S, Colonnelli K. Innovation pilot study: acute care for elderly (ACE) unit—promoting patient-centric care. HERD HERD. (2012) 5:90–8. doi: 10.1177/193758671200500309
57. Arbel I, Ye B, Mihailidis A. Stroke patients' experiences in an adaptive healing room in a stroke rehabilitation unit. HERD. (2020) 13:170–85. doi: 10.1177/1937586719879060
58. Magazine M, Murphy M, Schauer DP, Wiggermann N. Determining the number of bariatric beds needed in a US acute care hospital. HERD. (2021) 14:14–26. doi: 10.1177/19375867211012488
59. Connellan K, Gaardboe M, Riggs D, Due C, Reinschmidt A, Mustillo L. Stressed spaces: mental health and architecture. HERD. (2013) 6:127–68. doi: 10.1177/193758671300600408
60. Mayampurath A, Ward C, Fahrenbach J, LaFond C, Howell M, Churpek MM. Association between room location and adverse outcomes in hospitalized patients. HERD. (2019) 12:21–9. doi: 10.1177/1937586718806702
61. Nikabadi S, Zabihi H, Shahcheraghi A. Evaluating the effective factors of hospital rooms on patients' recovery using the data mining method. HERD. (2022) 15:97–114. doi: 10.1177/19375867211031305
62. Jimenez FE, Rich RK, Puumala SE, Kentfield M, Schoenholtz L, Brittin J. Effects of a decentralized nursing model on patient outcomes in two rural community hospitals. HERD. (2021) 14:157–73. doi: 10.1177/19375867211006491
63. Hua Y, Becker F, Wurmser T, Bliss-Holtz J, Hedges C. Effects of nursing unit spatial layout on nursing team communication patterns, quality of care, and patient safety. HERD HERD. (2012) 6:8–38. doi: 10.1177/193758671200600102
65. Ulrich RS, Berry LL, Quan X, Parish JT. A conceptual framework for the domain of evidence-based design. HERD HERD. (2010) 4:95–114. doi: 10.1177/193758671000400107
66. Taylor E, Card AJ, Piatkowski M. Single-occupancy patient rooms: a systematic review of the literature since 2006. HERD. (2018) 11:85–100. doi: 10.1177/1937586718755110
67. Greer V, Johnson E, Hsu J. Variables and outcomes in patient room design: a study of design hypotheses. HERD. (2021) 14:219–33. doi: 10.1177/1937586720954952
68. Lorenz SG, Dreher HM. Hospital room design and health outcomes of the aging adult. HERD. (2011) 4:23–35. doi: 10.1177/193758671100400204
69. McLaughlan R, Richards K, Lipson-Smith R, Collins A, Philip J. Designing palliative care facilities to better support patient and family care: a staff perspective. HERD. (2022) 15:149–62. doi: 10.1177/19375867211059078
70. Kwan MA. Acuity-adaptable nursing care: exploring its place in designing the future patient room. HERD. (2011) 5:77–93. doi: 10.1177/193758671100500108
71. Zimring C, Seo HB. Making acuity-adaptable units work: lessons from the field. HERD. (2012) 5:115–28. doi: 10.1177/193758671200500311
72. Pati D, Harvey TE, Barach P. Relationships between exterior views and nurse stress: an exploratory examination. HERD. (2008) 1:27–38. doi: 10.1177/193758670800100204
73. Gray WA, Kesten KS, Hurst S, Anderko L. Using clinical simulation centers to test design interventions: a pilot study of lighting and color modifications. HERD. (2012) 5:46–65. doi: 10.1177/193758671200500306
74. Zadeh RS, Shepley MMC, Williams G, Chung SSE. The impact of windows and daylight on acute-care nurses' physiological, psychological, and behavioral health. HERD. (2014) 7:35–61. doi: 10.1177/193758671400700405
75. Wang Z, Downs B, Farell A, Cook K, Hourihan P, McCreery S. Role of a service corridor in ICU noise control, staff stress, and staff satisfaction: environmental research of an academic medical center. HERD. (2013) 6:80–94. doi: 10.1177/193758671300600307
76. Hadi K, DuBose JR, Ryherd E. Lighting and nurses at medical–surgical units: impact of lighting conditions on nurses' performance and satisfaction. HERD. (2016) 9:17–30. doi: 10.1177/1937586715603194
77. Nejati A, Shepley M, Rodiek S, Lee C, Varni J. Restorative design features for hospital staff break areas: a multi-method study. HERD. (2016) 9:16–35. doi: 10.1177/1937586715592632
78. Copeland D, Chambers M. Effects of unit design on acute care nurses' walking distances, energy expenditure, and job satisfaction: a pre–post relocation study. HERD. (2017) 10:22–36. doi: 10.1177/1937586716673831
79. Matos LBN de, Fumis RRL, Junior APN, Lacerda FH, Caruso P. Single-bed or multibed room designs influence ICU staff stress and family satisfaction, but do not influence ICU staff burnout. HERD. (2020) 13:234–42. doi: 10.1177/1937586719878445
80. Bosch S, Bledsoe T, Jenzarli A. Staff perceptions before and after adding single-family rooms in the NICU. HERD. (2012) 5:64–75. doi: 10.1177/193758671200500406
81. Hospital Beds Function Report Japan 2021. p. 9. Available online at: https://www.mhlw.go.jp/content/10800000/000955093.pdf (accessed July 25, 2022).
82. He X, Miyazaki T, Byun M, Miura K. Effects of differences in environment of convalescent rehabilitation wards on activities of patients. J Archit Plan. (2016) 81:1269–79. doi: 10.3130/aija.81.1269
83. Mi X, Taniguchi G. Evaluation of wards environment by inpatients: comparative study on wards environment with traditional type and new “territorialized” type of 4-beds rooms. J Archit Plan. (2010) 75:2287–95. doi: 10.3130/aija.75.2287
84. Kato A, Yamaguchi K, Takagi M, Washio K. Bim study on evaluation for hospital ward facility planning and management by optimization of patient placement and simulation of nursing travel distance. J Archit Plan. (2021) 86:1205–11. doi: 10.3130/aija.86.1205
85. Gifu Prefectural Gero Hospital. p. 1–3. Available online at: http://www.jfma.or.jp/award/14/pdf/paneldata03.pdf (accessed July 25, 2022).
86. Zhou Y. Basic Study on Ward Planning of Acute Hospital based on Analysis of Nursing Activities. (PhD Thesis) The University of Tokyo The University of Tokyo (2004).
87. Toriyama A, Watanabe R, Nakayama S, Kakehi A, Yamashita T. Influence to nursing activities in hospital wards applying “personal nursing base” concept : reexamination studies on planning of acute care wards in the era of computerization of medical and patients' information part 1. J Archit Plan. (2007) 72:57–63. doi: 10.3130/aija.72.57_5
88. Toriyama A, Watanabe R, Nakayama S, Kakehi A, Yamashita T. Research on function and location of “personal nursing bases” and other types of nursing bases. J Archit Plan. (2008) 73:527–33. doi: 10.3130/aija.73.527
89. Nakano A, Ishibashi T. Materials management planning for the inpatient wards with multiple sub-nursing stations: a research on the planning of the inpatient wards served by the SPD system. J Archit Plan. (2007) 72:31–6. doi: 10.3130/aija.72.31_1
90. Matsushita D, Odawara R, Isokawa E, Yamashita T, Kumakawa T. Development of nursing activities measurement method with ultrasound positioning. AIJ J Technol Des. (2013) 19:1079–84. doi: 10.3130/aijt.19.1079
91. Takeuchi T, Yamaguchi K, Takagi M, Kato A. Study on evaluation for hospital ward planning and management by nursing travel distance simulation using BIM. J Archit Plan. (2020) 85:33–40. doi: 10.3130/aija.85.33
92. OECD. Doctors (indicator). (2022). Available online at: https://data.oecd.org/healthres/doctors.htm#indicator-chart (accessed July 25, 2022).
93. OECD. Nurses (indicator). (2022). Available online at: https://data.oecd.org/healthres/nurses.htm#indicator-chart (accessed July 25, 2022).
94. OECD. Length of hospital stay (indicator). (2022). Available online at: https://data.oecd.org/healthcare/length-of-hospital-stay.htm#indicator-chart (accessed July 25, 2022).
95. OECD. Hospital beds (indicator). (2022). Available online at: https://data.oecd.org/healtheqt/hospital-beds.htm (accessed July 25, 2022).
96. OECD. Life expectancy at 65 (indicator). (2017). Available online at: https://data.oecd.org/healthstat/life-expectancy-at-65.htm (accessed July 25, 2022).
Keywords: value-based design, evidence-based design, architectural planning, healthcare facility, USA, Japan
Citation: Zhou Y, Sun Y, Xu Y and Yuan H (2022) Study on value-based design of healthcare facilities: Based on review of the literature in the USA and Japan. Front. Public Health 10:883241. doi: 10.3389/fpubh.2022.883241
Received: 24 February 2022; Accepted: 15 August 2022;
Published: 09 September 2022.
Edited by:
Linchuan Yang, Southwest Jiaotong University, ChinaReviewed by:
Zhuolin Tao, Beijing Normal University, ChinaCopyright © 2022 Zhou, Sun, Xu and Yuan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ying Zhou, emhvdXlpbmdAc2V1LmVkdS5jbg==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.