
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 21 September 2022
Sec. Digital Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.875941
 Mohammed Alluhidan1,2
Mohammed Alluhidan1,2 Reem F. Alsukait3Taghred Alghaith1Rana Saber1Adwa Alamri1
Reem F. Alsukait3Taghred Alghaith1Rana Saber1Adwa Alamri1 Saleh Al-Muhsen4Fahad Alhowaitan5Abdulmohsen Alqarni5
Saleh Al-Muhsen4Fahad Alhowaitan5Abdulmohsen Alqarni5 Christopher H. Herbst6Nahar Alazemi1Ahmad S. Hersi7*
Christopher H. Herbst6Nahar Alazemi1Ahmad S. Hersi7*Background: E-government platforms provide an opportunity to use a novel data source for population health surveillance (also known as e-health). Absher is a Saudi e-government platform with 23 million authenticated users, including residents and citizens in Saudi Arabia. All Absher users were invited to participate in a web-based survey to estimate the prevalence of noncommunicable diseases and their risk factors in Saudi Arabia.
Objective: To assess the potential of using an e-government platform (Absher) to administer web-based health surveys.
Methods: A cross-sectional, web-based health survey was administered to Absher users between April 2019 and March 2020. The survey instrument included eight items and took <5 min to complete. The respondents' data were compared to Saudi Arabia's 2016 census. Descriptive summary statistics of the prevalence of major noncommuncable diseases are presented and compared to population-based prevalence data from Saudi Arabia's World Health Survey (WHS) 2019. All analysis was conducted using Stata 13.0.
Results: Overall, the Absher health survey had a 24.6% response rate, with most respondents being male (84%), Saudi (67%), and between 30 and 44 years of age (49%). Overall, the prevalence of noncommunicable diseases and risk factors among respondents was high for overweight (35%) and obesity (30%) and low for asthma (6%). The prevalence of diabetes, dyslipidemia, and hypertension was between 15 and 17% on average, and 26.5% were smokers. In comparison to population-based World Health Survey estimates, the Absher survey overestimated obesity, diabetes, dyslipidemia, hypertension, and smoking rates, and underestimated overweight, whereas asthma prevalence was similar for Absher and the WHS.
Conclusions: With improvements in the study design, the use of e-government platforms can provide a useful and potentially low-cost data source for public health research.
Public health surveillance offers a systematic approach for the regular collection and routine analysis of health indicators over time, and comparisons between different population groups. It allows for the regular dissemination of results and sharing of available scientific knowledge (1). One of the key aims of public health surveillance is to allow policymakers to determine the burden of disease in a timely manner to formulate policies and programs that mitigate the impact of diseases and their risk factors. Another key aim is to measure the progress and efficacy of preventive efforts already implemented (1, 2). However, traditional public health surveillance systems can be costly, and can also involve significant delays between data collection and dissemination of results (3).
In 2018, the World Health Assembly acknowledged the potential of digital technologies to play a major role in improving public health. E-government can be defined as the use of information and communication technology (ICT) to more effectively and efficiently deliver government services to citizens and businesses (4). There has been global interest in the potential of ICT for health. The term e-health encompasses the cost-effective and secure use of ICT in support of health and health-related fields, including healthcare services, health surveillance, health literature, and health education, knowledge, and research (5). As part of the 2020 Riyadh Declaration on Digital Health, innovative surveillance systems were highlighted as a core component of the connected global health system (6).
In 2003, Saudi Arabia started its digital transformation to e-governance and began offering government services electronically (7). Absher provides the essential infrastructure that underpins Saudi Arabia's e-government services. Since its launch in 2010, Absher has developed into a three-dimensional framework for individuals, businesses and government entities (8). Absher Individuals has enabled citizens and residents of Saudi Arabia to access a broad collection of e-services provided by different government agencies (for example, the Ministry of Civil Affairs, Ministry of Housing, and General Directorate of Traffic). Absher registration requires a national or residence ID number, fingerprint biometrics authentication and a valid mobile number. The user account is then activated through Absher registration by visiting an activation office (passports or civil affairs offices), a bank, or a self-service machine (8). The 23 million registered users of Absher can access more than 330 different e-government services including driving license renewal, disputing traffic violations, issuing and renewing the Saudi passport, issuing and renewing visas and residence permits, reporting missing documents, authentication of lease contracts and newborns registration (8).
Noncommunicable diseases (NCDs) are a major health and economic burden in Saudi Arabia (9). They are currently the leading cause of death and disability-adjusted life years in the country, accounting for 66.7% of deaths (10). The NCD burden will likely continue to rise with the country's demographic transitions since NCDs disproportionately affect older people. Vision 2030 is Saudi Arabia's strategic framework to reduce the country's dependence on oil, diversify its economy, and develop public service sectors, such as health, education, infrastructure, recreation, and tourism (11). Through the Health Sector Transformation Plan, the vision outlines a number of strategic objectives to improve life expectancy and realize economic potential in the country, including the promotion of health prevention.
However, there are gaps in the data, considering that the last two population-based national surveys were the 2013 Saudi Health Interview Survey (SHIS) and the Saudi Arabia's World Health Survey (WHS) in 2019 (12, 13). Given the significant time lag between these surveys, there is a need for more frequent data collection to prioritize policy actions and allocate resources (14). Web-based surveys are typically quicker to complete and cost less per participant than other survey modes (15). Public health professionals are highly encouraged to develop and experiment with new digital innovation tools for health-related data collection (16). Absher platform can provide such a digital tool.
Between 2019 and 2020, a web-based survey was launched using Absher's e-government platform as a novel way to collect health-related data and determine the burden of NCDs in Saudi Arabia. The objectives of this paper are to (1) describe the results of the Absher survey and (2) compare the prevalence estimates collected from the Absher survey with those of a national population-based survey. The overall objective is to inform the future use of e-government tools for public health research. This work is related to the first author's master's thesis (17).
A web-based cross-sectional health survey was launched through the Absher e-government platform (hereafter referred to as Absher) between April 2019 and March 2020. All Absher users who logged into the platform during the study period-whether they used a website or a mobile application-received an invitation (Appendix B in Supplementary material) to participate in the survey 3,584,422. Only those Absher users who consented to participate were redirected to the online survey. Ethical approval for the Absher survey was obtained from the King Fahad Medical City Institutional Review Board.
The prevalence estimate results from the Absher survey were then compared to the results from Saudi Arabia's 2019 WHS report (13). The WHS is a nationally representative population-based, cross-sectional household- and individual-level survey of adults aged 15 and older. It includes anthropometric measurements (weight, height, hip, and waist circumference), a blood pressure test, and a blood test including random plasma glucose, cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), and hemoglobin for individual-level respondents (n = 8,912). Out of the 10,000 selected households, a total of 9,652 were present (or occupied), and 9,339 were successfully interviewed, yielding a response rate of 96.8%. In the households interviewed, one person aged 15 years or older per household was identified for individual interviews. Interviews were completed with 8,912 individuals, yielding a response rate of 95.4%. WHS IRB approval was obtained from the General Directorate for Research and Studies at the MoH (13). Additional details on the methodology and study instruments are described elsewhere (13).
The Absher web-based survey consisted of nine questions that were available in both English and Arabic. The first five questions were yes/no questions that asked respondents whether they had been diagnosed with diabetes, hypertension, high blood cholesterol, or asthma, and whether they smoked. The next two questions were dropdown questions that asked participants to indicate their weight in kilograms and their height in centimeters. The final two questions also used a dropdown box to ask for region and city of residence. All questions are included in Appendix A in Supplementary material. Age, gender, and nationality were automatically verified through the Absher database. Only adults over the age of 15 were included in the analysis (n = 8,82,746). No other information was obtained, and the data were deidentified.
Absher survey data cleaning involved reorganizing existing variables, such as nationality (Saudi or non-Saudi), region (central, western, eastern, southern, and northern), and age into specific age groups (15–29, 30–44, 45–59, 60+). Additional new variables were created, including body mass index (BMI; underweight if BMI is <18.5; normal if BMI is between 18.5 and 24.9; overweight if BMI is between 25.0 and 29.9; or obese if BMI is ≥30) (18). Biologically implausible measurements (height < 111.8 cm [<44 inches] or >228.6 cm [>90 inches] and weight <24.9 kg [<55 pounds] or >453.6 kg [>1,000 pounds]) were excluded (18).
Saudi Arabia's 2016 population census demographics (gender, nationality, age groups, and region) were used to adjust the weights of Absher survey responses. Specifically, we used raking methodology in Stata 13.1 (19). In which the weighting variables were raked according to their marginal distribution. Respondents with missing data were excluded from the analysis. Data analysis included creating descriptive summaries for each disease or risk factor by age, gender, nationality, and region of residence using Stata 13.1. Prevalence estimates from the Absher survey were then compared to the 2019 WHS report.
Overall, the majority of Absher survey respondents were male (83.7%), Saudi nationals (66.8%), between 30 and 44 years of age (49.4%), and from the more populated central and western regions (32.6 and 31.1%, respectively; Table 1).
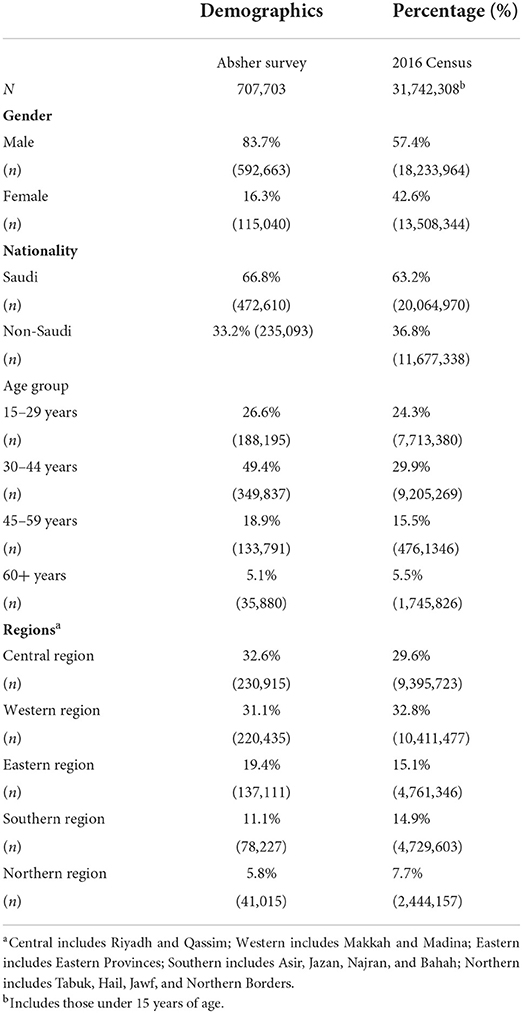
Table 1. Demographic characteristics of Absher survey respondents 2019–2020 compared to Saudi Arabia's 2016 census.
The overall prevalence of NCDs and risk factors among survey respondents was relatively high for overweight and obesity (35 and 29.9%, respectively) and lowest for asthma (6.1%). The prevalence of diabetes, dyslipidemia, and hypertension was, on average, between 15 and 17%. Based on demographic variables, regional variations in the prevalence of most NCDs and their risk factors were small (1–3% differences), except for smoking prevalence in the southern regions, which was the lowest at around 20.7% compared to 31.4% in Northern region. Both overweight and obesity prevalence rates were lower among females than males (25.9% compared to 30.7%, respectively, for obesity). Overweight was higher among non-Saudis than Saudis (42.2% compared to 31.9%, respectively). However, for non-Saudis, the prevalence of diabetes, dyslipidemia, and hypertension was approximately 7% lower than Saudis at around 11%, compared to 17–19% for Saudis. The prevalence of smoking was much higher among males than females (30.6% compared to 5.3%, respectively). Similarly, smoking was less prevalent among non-Saudis than Saudis (19.5% compared to 30%; Table 2). Additional results disaggregated by age and gender are provided in Appendix C in Supplementary material.
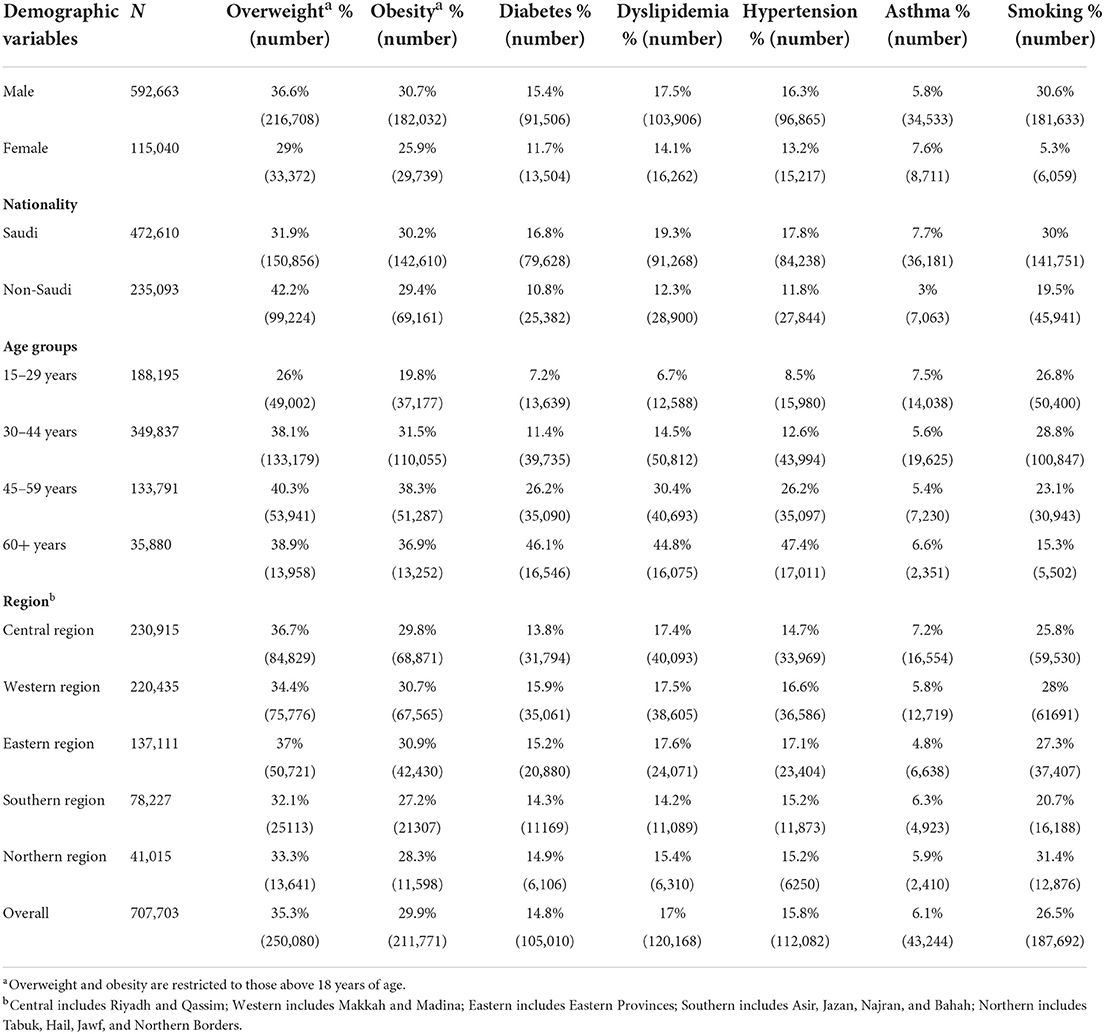
Table 2. Prevalence of noncommuncable diseases and their risk factors among Absher survey respondents 2019–2020.
When comparing Absher survey results with the 2019 population-based WHS for Saudi Arabia results, major differences appeared, as shown in Figure 1. Most notably, the Absher survey overestimated obesity, diabetes, dyslipidemia, hypertension and smoking rates by 7–15%. Asthma prevalence estimates were close in both, and overweight was underestimated in the Absher survey (35.3% compared to 38% in the WHS; Figure 1).
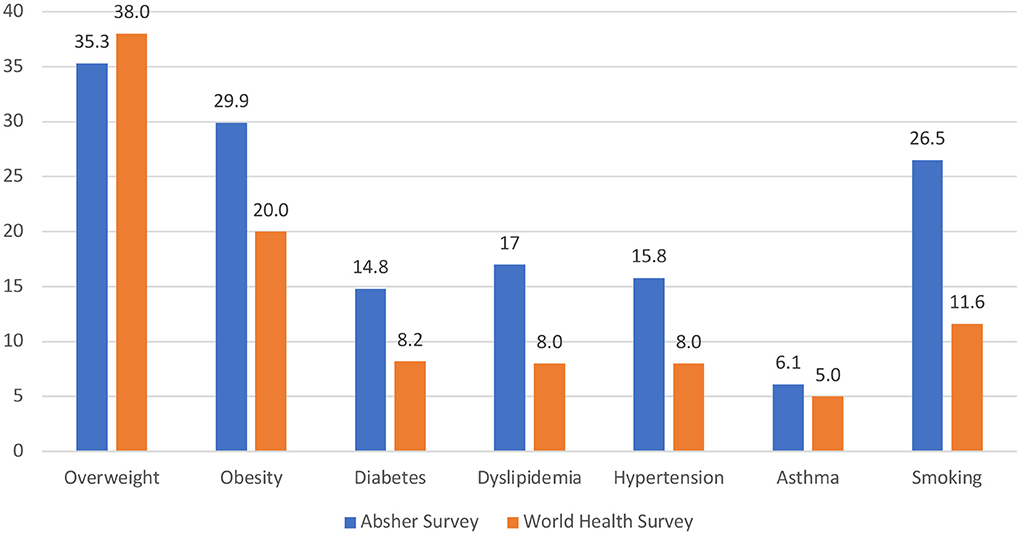
Figure 1. Difference in prevalence rates (%) of selected self-reported diseases and risk factors between the Absher Survey 2019–2020 and World Health Survey 2019.
Overall, the Absher survey response rate was 24.6%, which indicates a 75% nonresponse bias. Information on non-respondents or people who logged into Absher during the survey period and did not opt in is unknown. However, the response rate was calculated based on the number of active Absher users during that period, which might overestimate the nonresponse rate, considering that unless a user needed a specific government service during that period, they likely did not log in to see the survey invitation. Another factor to contemplate is the influence of people's perceptions of public health surveillance because this survey was the first attempt in Saudi Arabia. Response rates are typically calculated by dividing the number of responses by the total number of eligible respondents in the sample (20). While mixed-mode approaches could yield higher response rates (60% compared to 51% for web-based only), paper mail is not typically used in Saudi Arabia (15).
While higher response rates indicate a higher quality survey research study, representativeness is also a major component (21). In terms of the representativeness of Absher survey respondents, there are some variations between the 2016 Saudi census and the Absher survey. Nationality status (Saudi vs. non-Saudi), age group, and region of residence were similar to the census population distribution (22). However, females were significantly underrepresented; only 16.3% of survey respondents were female, compared to the national overall estimate of 43% (22). In addition, those between 30 and 44 years of age were overrepresented among the Absher survey respondents at 49.4%, compared to 30% in the national census (22). This lack of representation could be explained by a number of factors. Until 2018, women were not allowed to have individual accounts on the Absher system. This has changed, restrictions have been removed, and women can now create their own individual Absher accounts. The rate of female users has been consistently increasing since then (23). Additionally, the number of authenticated accounts on Absher has been increasing steadily, from 7 million at the time of the survey to over 23 million at the time of writing (24). This will likely improve the representativeness of the sample in future studies.
There are differences in the prevalence rates found in the Absher survey and in the population-based WHS results. WHS diabetes and prediabetes prevalence estimates based on randomly measured blood glucose levels are close to the Absher survey results (15% compared to 14.8%, respectively; (13). Similarly, WHS hypertension based on measured blood pressure is similar to the Absher results [15.8% compared to 15.7%, respectively; (13)]. WHS dyslipidemia based on raised serum cholesterol is much higher at 43% than the 17% self-reported among Absher survey respondents (13). One potential explanation is that self-reported responses typically underestimate the prevalence of disease, as observed in the WHS's own self-reported vs. measured responses (13). Specifically, a 2013 population-based survey in Saudi Arabia found that 65% of Saudis with hypercholesterolemia and 58% of hypertensive and diabetic Saudis were undiagnosed, and therefore unlikely to be captured by self-reported data (25–27). Adding a health interview component to those who opt in to take the survey could improve the validity of the findings by allowing objective measurements of blood and anthropometrics, thereby reducing the reliance on self-report (28). Nonetheless, the use of web-based e-government platforms, such as Absher, could be an effective tool for answering subjective health-related research questions that are primarily based on self-report.
The implementation of internet-based public health surveillance systems is an emerging development in healthcare (29). Until now, most relevant studies have focused on public health surveillance systems to mitigate the impacts of infectious diseases in developing settings, establishing a gap in literature that focuses on NCDs in high-income nations (30, 31). Consequently, the existing research on NCDs surveillance, which is deployed to provide early warning detection, detect patterns in the generated information, and produce sufficient data to inform evidence-based practice, does not cover all critical areas in high-income countries (30).
The Absher survey has several strengths, including having authenticated users with age, region, and nationality data generated by the system from the e-government platform using national ID numbers. Additionally, the survey was web-based, so it was neither cost- nor labor-intensive. The data required little cleaning (32). Future studies could estimate the cost per respondent using Absher compared to other outlets, such as web panels. The survey itself also had a low time commitment for respondents, as it took <5 min to complete. Studies have shown that time commitment is an important factor in improving response rate (33). Finally, to address the skewness of the data's lack of representativeness, the findings were weighted based on demographics from the national census. However, there were little differences between adjusted and unadjusted results.
Some of the limitations of using Absher as a tool for web-based surveys have been touched on in the discussion. Mainly, it had a low response rate, which could have resulted in nonresponse bias. It was difficult to obtain information on non-respondents because of ethics and privacy considerations. Future studies could ensure that information on the number of people who logged into Absher and saw the survey is captured to enable comparisons between responders and nonresponders and assess whether there are significant differences between the two groups. One potential bias is whether there are any disparities in accessing the internet thereby the platform. Nonetheless, recent national surveys show that ICT in KSA is high with 96.8% of households having internet access and 99.1% have mobile phone access in 2020 (34). Additionally, the low female participation rate should be addressed in future surveys. The survey questions were not validated, and future studies could improve their strength by using validated tools. For example, improvement could include conducting health interviews with blood samples from a subset of users to improve the validity of results in comparison to self-reported data. Finally, optimizing the use of Absher by linking the survey responses to other data available in the Ministry of Health's Sehaty database using the national or resident permit ID numbers could enable many research questions to be answered.
Digital health applications, such as those linked to e-government services, can serve as valuable data collection tools. Absher offers a unique platform for ongoing cross-sectional studies. Its possibilities and applications are far-reaching and continue to evolve as a potential asset to public health.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by King Fahad Medical City IRB Log Number: 20-425E. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
MA, TA, AH, and NA conceived the idea. MA, RA, FA, and AAlq procured the relevant datasets. RA led the data analysis. MA, RA, and CH took the lead in organizing, writing, and revising the manuscript. All authors contributed, read, and approved the final manuscript.
This manuscript was produced by the Saudi Health Council, with technical and financial support received from the World Bank under the RAS Program (P172148) between the World Bank and the Ministry of Finance, Saudi Arabia. The authors are indebted to H. E. Dr. Tariq A. Alshiddi, Director of the National Data Management Office, Dr. Esam Alwagait, Director of the National Information Center, and staff for their valuable help in creating the questionnaire. The authors are also grateful for the overall support provided by Rekha Menon, World Bank Practice Manager, Health Nutrition and Population, MENA region. Finally, MA wishes to thank Prof. Bruce Hollingsworth, Division of Health Research, Lancaster University, for providing general guidance and support for the work presented in this paper.
Authors FA and AAlq were employed by Elm.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.875941/full#supplementary-material
ICT, information and communication technology; NCD, noncommunicable disease; WHS, World Health Survey.
1. Nsubuga P, White ME, Thacker SB, Anderson MA, Blount SB, Broome CV, et al. Public health surveillance: a tool for targeting and monitoring interventions. In: Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, et al., editors. Disease Control Priorities in Developing Countries. Washington, DC: The International Bank for Reconstruction and Development/The World Bank (2006). p. 997–1015.
2. Barros JM, Duggan J, Rebholz-Schuhmann D. The application of internet-based sources for public health surveillance (Infoveillance): systematic review. J Med Internet Res. (2020) 22:e13680. doi: 10.2196/13680
3. Herida M, Dervaux B, Desenclos J-C. Economic evaluations of public health surveillance systems: a systematic review. Eur J Public Health. (2016) 26:674–80. doi: 10.1093/eurpub/ckv250
4. Malodia S, Dhir A, Mishra M, Bhatti ZA. Future of e-Government: an integrated conceptual framework. Technol Forecast Social Change. (2021) 173:121102. doi: 10.1016/j.techfore.2021.121102
5. Franco M, Tursunbayeva A, Pagliari C. Social Media for e-Government in the public health sector: protocol for a systematic review. JMIR Res Protoc. (2016) 5: e5421. doi: 10.2196/resprot.5421
6. Knawy BA, Adil M, Crooks G, et al. The Riyadh declaration: the role of digital health in fighting pandemics. Lancet. (2020) 396:1537–9. doi: 10.1016/S0140-6736(20)31978-4
7. Basahel A, Yamin M. Measuring success of e-government of Saudi Arabia. Int J Inf Technol. (2017) 9:287–93. doi: 10.1007/s41870-017-0029-4
8. Absher User Guide. Available online at: https://www.absher.sa/wps/portal/individuals/static/guide/!ut/p/z0/04_Sj9CPykssy0xPLMnMz0vMAfIjo8ziDQ1dLDyM3A18LLyDXAwCnQPMDEM8PIwtnEz1g1Pz9AuyHRUBm_vkkw!!/ (accessed December 25, 2021).
9. Alqunaibet A, Herbst CH, El Saharty S, Algwaizini A. Noncommunicable Diseases in Saudi Arabia: Toward Effective Interventions for Prevention. Washington, DC: The World Bank (2021). Available online at: https://openknowledge.worldbank.org/handle/10986/36546 doi: 10.1596/978-1-4648-1717-5 (accessed June 25, 2022).
10. Institute for Health Metrics Evaluation (IHME). GBD Compare. (2020). Available online at: http://vizhub.healthdata.org/gbd-compare (accessed August 10, 2022).
11. Saudi Arabi's Vison 2030. Health Sector Transformation Program. (2016). Available online at: https://www.vision2030.gov.sa/v2030/vrps/hstp/ (accessed July 27, 2022).
12. Ministry of Health, Kingdom of Saudi Arabia and Institute of Health Metrics and Evaluation, University of Washington. Saudi Health Interview Survey Results. (2013). Available online at: https://www.healthdata.org/sites/default/files/files/Projects/KSA/Saudi-Health-Interview-Survey-Results.pdf (accessed August 02, 2022).
13. Ministry of Health. World Health Survey Saudi Arabia (KSAWHS) 2019 Final Report. (2020). Available online at: https://www.moh.gov.sa/en/Ministry/Statistics/Population-Health-Indicators/Documents/World-Health-Survey-Saudi-Arabia.pdf (accessed October 25, 2021).
14. Noncommunicable Diseases in Saudi Arabia: Toward Effective Interventions for Prevention. Available online at: https://openknowledge.worldbank.org/handle/10986/36546 (accessed Decemer 24, 2021).
15. Greenlaw C, Brown-Welty S. A comparison of web-based and paper-based survey methods: testing assumptions of survey mode and response cost. Eval Rev. (2009) 33:464–80. doi: 10.1177/0193841X09340214
16. Dalton CB. Enablers of innovation in digital public health surveillance: lessons from Flutracking. Int Health. (2017) 9:145–7. doi: 10.1093/inthealth/ihx009
17. Alluhidan M. Deploying Saudi Arabia's E-Government Framework as a Public Health Surveillance System for Non-Communicable Diseases: A Cross-Sectional Study [Master's Dissertation]. Lancaster: Lancaster University (2022). 66p.
18. Cheng FW, Gao X, Mitchell DC, Wood C, Still CD, Rolston D, et al. Body mass index and all-cause mortality among older adults. Obesity. (2016) 24:2232–9. doi: 10.1002/oby.21612
19. Valliant R, Dever JA. Survey Weights: A Step-by-step Guide to Calculation. Texas: Stata Press (2018).
20. Manfreda KL, Bosnjak M, Berzelak J, Haas I, Vehovar V. Web surveys vs. other survey modes: a meta-analysis comparing response rates. Int J Market Res. (2008) 50:79–104. doi: 10.1177/147078530805000107
21. Fincham JE. Response rates and responsiveness for surveys, standards, and the journal. Am J Pharm Educ. (2008) 72. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2384218/ (accessed February 11, 2021).
22. General Authority for Statistics. Population In Saudi Arabia by Gender, Age, Nationality (Saudi/Non-Saudi)—Mid 2016 A.D. Published April 18, 2017. Available online at: https://www.stats.gov.sa/en/5305 (accessed December 28, 2019).
23. Hassan R. Two Million Women on Absher as Saudi App Users Surge. Arab news. Published Feb 28, 2019. Available online at: https://www.arabnews.com/node/1459206/saudi-arabia (accessed February 11, 2021).
24. Absher. Number of “Absher” users exceeds 23 million. Published Jun 17, 2021. Available online at: https://www.absher.sa/wps/portal/individuals/static/footer/contents/!ut/p/z0/fY29DoJAEIRfxYaS7HK5kFBiJPhTaGIhXnNZ4SKrZBE40cf3YqxtJvNNJjNgoAIjNPOVPPdCXeCzSS1utF4nWu32uFxhnmd4SItCYYlwdAJbMP9LYYVvw2ByMHUv3r09VF8jfoqQpeGZmyd1AcS9frqgsW55dhHSZWrdaENoVRZjFitUCdnw_LiXpw9dU2cl/ (accessed November 24, 2021).
25. El Bcheraoui C, Memish ZA, Tuffaha M, Daoud F, Robinson M, Jaber S, et al. Hypertension and its associated risk factors in the kingdom of Saudi Arabia 2013: a national survey. Int J Hypertens. (2014) 2014:564679. doi: 10.1155/2014/564679
26. Basulaiman M, El Bcheraoui C, Tuffaha M, Robinson, M, Daoud F, et al. Hypercholesterolemia and its associated risk factors-Kingdom of Saudi Arabia, 2013. Ann Epidemiol. (2014) 24:801–8. doi: 10.1016/j.annepidem.2014.08.001
27. El Bcheraoui C, Basulaiman M, Tuffaha M, Daoud F, Robinson M, Jaber S, et al. Status of the diabetes epidemic in the Kingdom of Saudi Arabia, 2013. Int J Public Health. (2014) 59:1011–21. doi: 10.1007/s00038-014-0612-4
28. Paalanen L, Koponen P, Laatikainen T, Tolonen H. Public health monitoring of hypertension, diabetes and elevated cholesterol: comparison of different data sources. Eur J Public Health. (2018) 28:754–65. doi: 10.1093/eurpub/cky020
29. Barros JM, Duggan J, Rebholz-Schuhmann D. The application of internet-based sources for public health surveillance (infoveillance): systematic review. J Med Internet Res. (2020) 22:e13680.
30. Blangiardo M, Boulieri A, Diggle P, Piel FB, Shaddick G, Elliott P. Advances in spatiotemporal models for non-communicable disease surveillance. Int J Epidemiol. (2020) 49:i26–37. doi: 10.1093/ije/dyz181
31. Fall IS, Rajatonirina S, Yahaya AA, Zabulon Y, Nsubuga P, Nanyunja M, et al. Integrated disease surveillance and response (IDSR) strategy: current status, challenges and perspectives for the future in Africa. BMJ Glob Health. (2019) 4:e001427. doi: 10.1136/bmjgh-2019-001427
32. Ebert JF, Huibers L, Christensen B, Christensen MB. Paper- or web-based questionnaire invitations as a method for data collection: cross-sectional comparative study of differences in response rate, completeness of data, and financial cost. J Med Internet Res. (2018) 20:e24. doi: 10.2196/jmir.8353
33. Manzo AN, Burke JM. Increasing response rate in web-based/internet surveys. In: Gideon L, ed. Handbook of Survey Methodology for the Social Sciences. New York: Springer (2012):327–43. doi: 10.1007/978-1-4614-3876-2_19
34. General Authority for Statistics. Survey of Access & Usage Households & Individuals to ICT 2021. (2021). Available online at: https://www.stats.gov.sa/en/6818%20 (accessed July 10, 2022)
Keywords: NCDS, e-health, cross-sectional, Saudi Arabia, e-government platforms, surveillance
Citation: Alluhidan M, Alsukait RF, Alghaith T, Saber R, Alamri A, Al-Muhsen S, Alhowaitan F, Alqarni A, Herbst CH, Alazemi N and Hersi AS (2022) Effectiveness of using e-government platform “Absher” as a tool for noncommunicable diseases survey in Saudi Arabia 2019–2020: A cross-sectional study. Front. Public Health 10:875941. doi: 10.3389/fpubh.2022.875941
Received: 14 February 2022; Accepted: 31 August 2022;
Published: 21 September 2022.
Edited by:
Alain B. Labrique, Johns Hopkins University, United StatesReviewed by:
Geoffrey Fairchild, Los Alamos National Laboratory (DOE), United StatesCopyright © 2022 Alluhidan, Alsukait, Alghaith, Saber, Alamri, Al-Muhsen, Alhowaitan, Alqarni, Herbst, Alazemi and Hersi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ahmad S. Hersi, YWhlcnNpQGtzdS5lZHUuc2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.