 Yung-Chieh Tung1
Yung-Chieh Tung1 Ying Xu
Ying Xu Yu-pei Yang
Yu-pei Yang Tao-Hsin Tung
Tao-Hsin Tung- 1Division of Cardiovascular Surgery, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
- 2Institute for Hospital Management, Tsing Hua University, Shenzhen, China
- 3Department of Hematology, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Linhai, China
- 4Evidence-Based Medicine Center, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Linhai, China
Purpose: This study aimed to evaluate the influence of learning transfer on the clinical performance of medical staff.
Methods: We searched PubMed, Embase, and the Cochrane Library for all associated studies without any language restrictions from the inception until 31 December 2021.
Results: This systematic review screened out 14 eligible studies that met the inclusion criteria. Most of these studies showed that learning transfer contributed to the clinical performance of medical staff. Through education, or when knowledge and skills have common basic principles, learning transfer will be more apparent than for those who learn by themselves and those without simulation training.
Conclusions: The findings of this review support an association between learning transfer and the clinical performance of medical staff. However, it was noted that due to the lack of relevant research and the major differences in the methods and indicators used in previous studies, we are restricted in conducting an effective meta-analysis. Further comprehensive trials will be needed to assess the impact of learning transfer on the clinical performance of medical staff.
Systematic Review Registration: PROSPERO, identifier: 341439.
Introduction
It has been widely acknowledged that the system of healthcare is complicated. Hundreds of pieces of clinical data are generated from the healthcare process, such as the patient's history, examination findings, and investigation results. Correct diagnosis can be defined by analyzing these huge amounts of data accurately. With the rapid expansion of the knowledge base of diseases and their management, the complexity of the system of healthcare is inevitably aggravated (1). Clinical performance should meet the highest standards based on adequate knowledge, determination, technology, and attitudes at different levels of clinical practice (2). Medical professionals should be able to implement technical, intelligent, and elevated skilled clinical practices so as to offer reliable and high-quality medical care to each patient (3). In order to improve the clinical performance of medical staff, it is essential to arrange continuing education and to make a great effort to upgrade medical professionals' learning and skills through different educational courses.
For decades, researchers have examined the practical concept of learning transfer. Learning complicated abilities for individuals, according to Gagne (4), requires comprehension based on adequate knowledge, implying that learning is a cumulative process. Transfer of learning, according to Ellis (5), occurs when “experience or performance on one task has an effect on performance on a subsequent one.” McKeachie (6) defined transfer as “The application of earlier learning in a condition that is not the same as the learning situation.” Learning transfer was later described as the extent to which knowledge (simple or complicated), skills (conceptual, interpersonal, or technical; open or closed), and competencies acquired during training are transferred to the job (7–10). It is also noteworthy that learning transfer, on the other hand, is not a static concept, and its meaning varies depending on how it is defined and utilized before, during, and after the learning process. Learning transfer is mainly across test patterns, implantation and judgment matters, problems involving clinical diagnoses, and mediator and associated word suggestions (11). Transfer of learning is critical in education, as the context of learning varies with the context of the application (12). Medical staff are expected to build a framework of the cognitive foundation from books, lectures, or simulations, draw principles from their prior knowledge and experiences, and apply learning in their workplace, building their ability to manage and solve problems. In nursing, it is reported that the transfer of learning has led to the effectiveness of simulation and debriefing experiences (13–15).
From the clinical viewpoint, the better the learning transfer, the more challenging the appointed assignments could be, and the more active and creative the results. Although the main processes of learning transfer include formal learning activities (e.g., maintenance education or job training programs) and self-directed informal learning activities, a previous study reported low levels of learning transfer among members of an institution (3). In addition, a case-based blended learning (CBBL) framework which utilized the flexibilities of an e-learning platform has highlighted that E-Case-Based Learning is effective in promoting the outcome of performance and is an essential way of learning and discovering (16, 17).
It is valuable to explore the practical implications of the effectiveness of learning transfer used in medical education and related training circumstances. Whether training transfer is associated with clinical services is an essential question warranting investigation. Thus, we conducted this systematic review to further evaluate the influences of learning transfer on clinical performances among medical staff.
Materials and Methods
Literature Review
We performed this study in accordance with guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (PROSPERO ID: 341439). We conducted a comprehensive search for relevant studies (without language limitations) from major online databases, such as PubMed, Embase, and the Cochrane Library, from inception to 31 March 2022. Two independent reviewers scanned the literature and included the eligible studies by common consensus after multiple rounds of screening.
Data Sources and Search Methods
The search process included (i) reading the reference section of all relevant research carefully; and (ii) manually searching abstracts of key journals and papers published at major annual conferences. The search terms used were a mix of (“learning transfer” [All Fields] OR “boundary crossing training” [All Fields]) AND (“clinical performance” [All Fields] OR “academic theoretical knowledge” [All Fields] OR “professional practice experience” [All Fields]). We also checked the reference lists of the screened studies to identify other similar studies. The search strategy is shown in Table 1. We included experimental studies that examined the influence or effectiveness of learning transfer on the clinical performance of medical staff. The PICOS criteria are used to select the eligible studies. Studies were included if they satisfied the following inclusion criteria: (1) The study was limited to RCTs and humans; (2) All participants are medical staff; (3) The study included both an experimental group and a control group. The experimental group was subjected to a learning lesson while the control group was performed without learning a lesson. (4) The study reported the effect of learning transfer on the performance of medical staff in each group. The exclusion criteria were as follows: (1) unqualified study design, such as non-RCT design, single-arm extension study, observational studies; (2) case reports, editorials, or reviews; (3) duplicated reports.
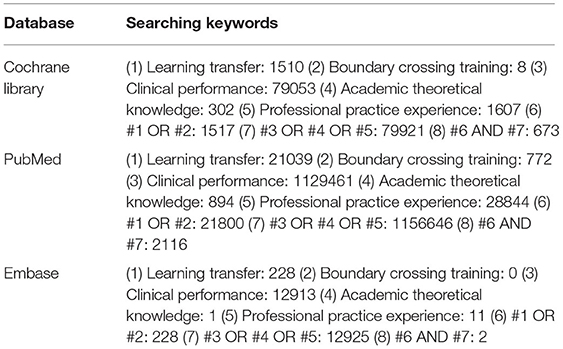
Table 1. Search strategy.
Data Extraction and Quality Assessment
For all articles included, we extracted the following information from the original articles: first author, publication year, country, database, study duration, study design, study subjects, mean age of study subjects, gender of the study subjects, and outcomes. Two reviewers independently performed an analysis of methodological quality. The quality assessment included the following items: allocation generation and concealment, blinding, follow-up duration, loss follow-up (%), and data-analysis method (intention-to-treat or per protocol). Divergences were resolved through discussion and consensus. Further, we used version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2) to assess the risk of bias for Systematic Reviews of Interventions. Any disagreement was resolved through discussion with a third author. All analyses were performed by Review Manager version 5.4.1.
Results
Study Characteristics
The results of the systematic review are presented in Figure 1. We identified a total of 14 studies related to the transfer of learning after a thorough review of all papers. The characteristics of the studies are listed in Table 2. Among the studies considered in this paper, seven were conducted in Europe, three were in Canada, two were in the United States, and one each was conducted in Australia and South Korea.
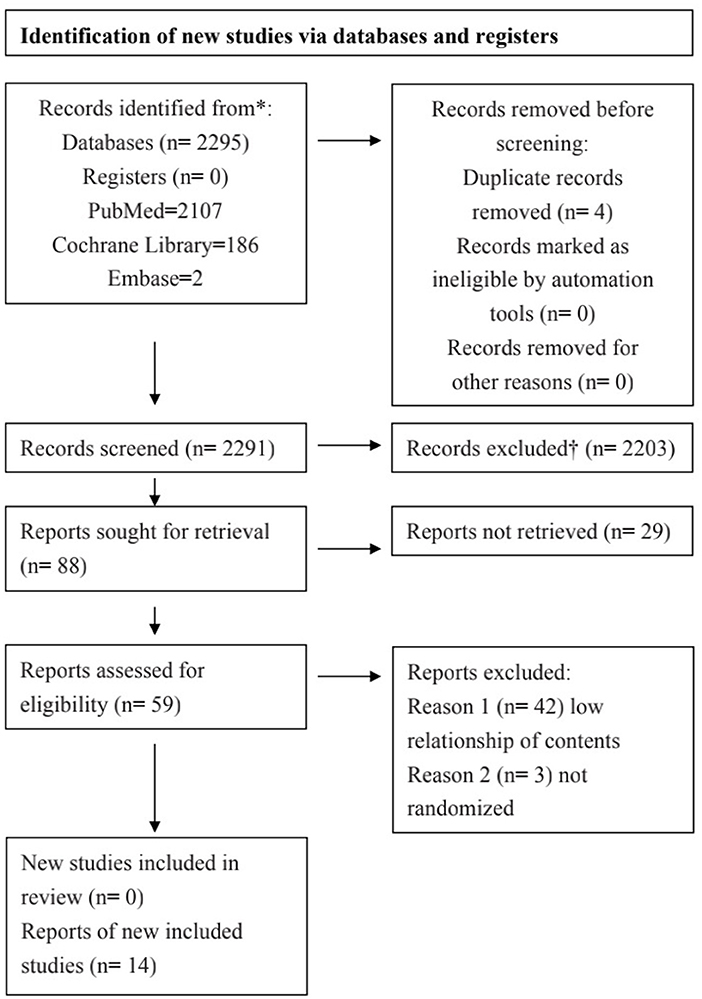
Figure 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
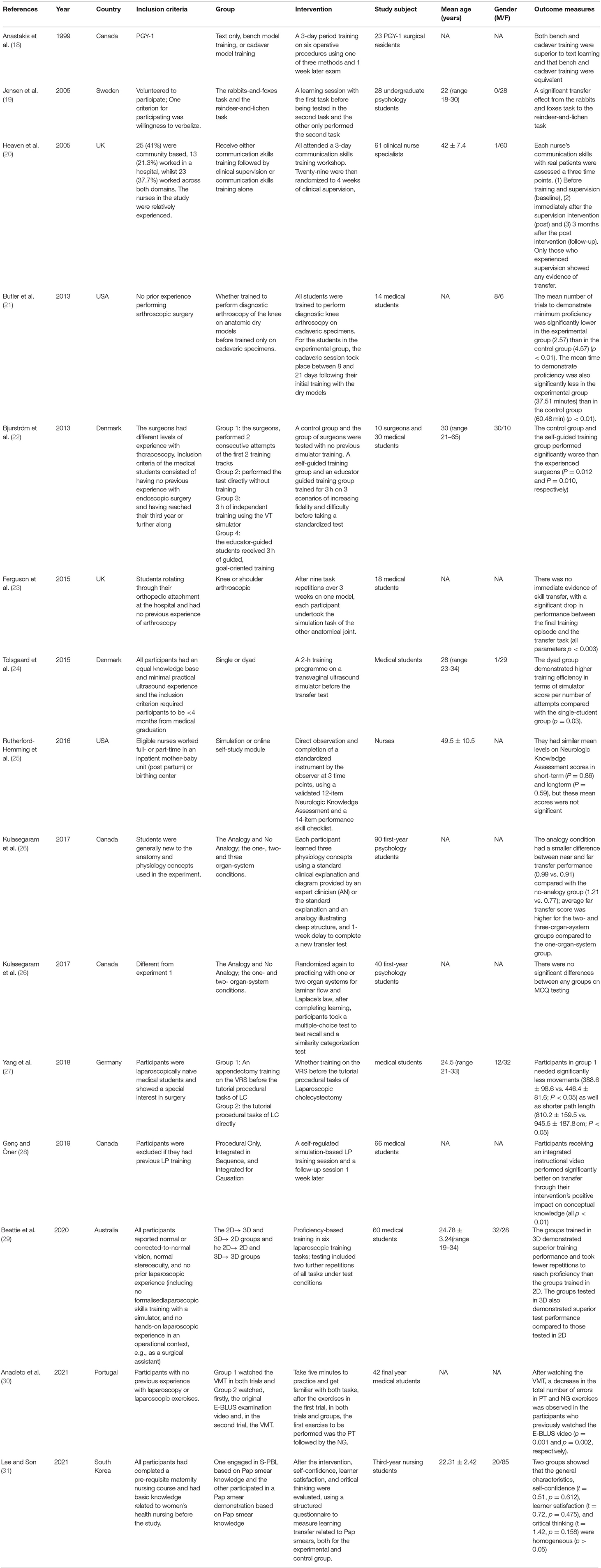
Table 2. Characteristics of randomized controlled trials.
Quality Assessment
Table 3 shows the results of a methodological quality assessment of all included studies. We considered inadequate allocation concealment and sequence generation the most common sources of potential bias. Due to the few studies included and the degree of heterogeneity observed in the study design, interventions, and outcome indices, meta-analysis was considered impractical.
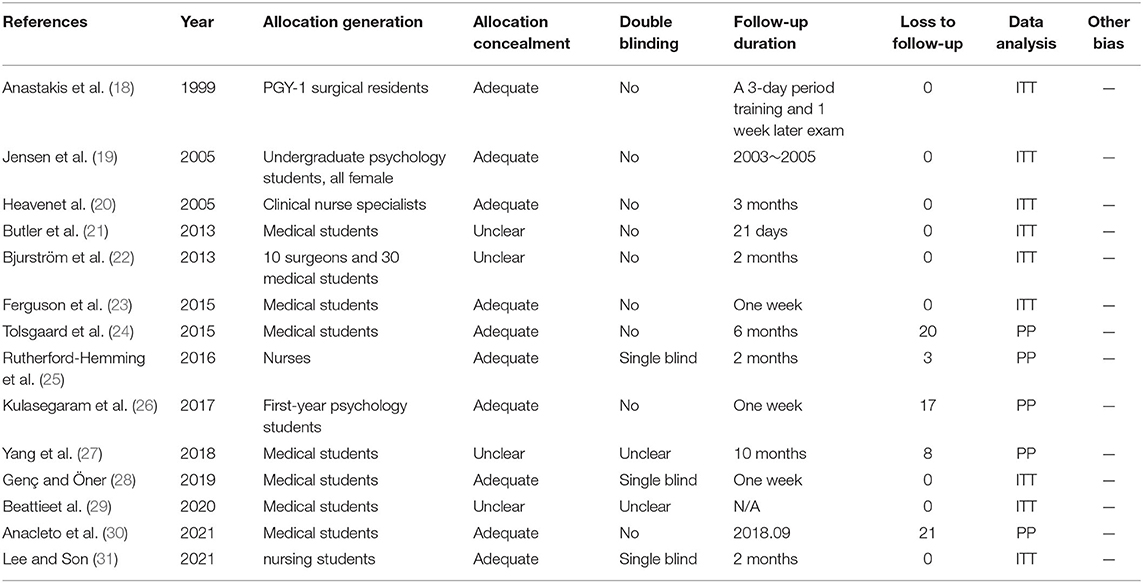
Table 3. Methodological quality assessment of the included studies.
Figure 2 presents a summary assessment of bias risk. Butler et al. (21), Bjurström et al. (22), Yang et al. (27), and Beattie et al. (29) did not clearly describe how the research populations are selected. Yang et al. (27) and Beattie et al. (29) did not clearly explain whether the participants were blinded. Yang et al. (27), Tolsgaard et al. (24), Rutherford-Hemming et al. (25), Kulamakan et al. (26), and Anacleto et al. (30) lost a number of research objects to follow-up, and therefore we must assume a high risk of bias. Setting the issue of uncleared blinded participants aside, all but Rutherford-Hemming et al. (25), Genç and Öner (28), and Lee et al. (31) did not blind participants; thus, their assessment of outcomes must be regarded as questionable.
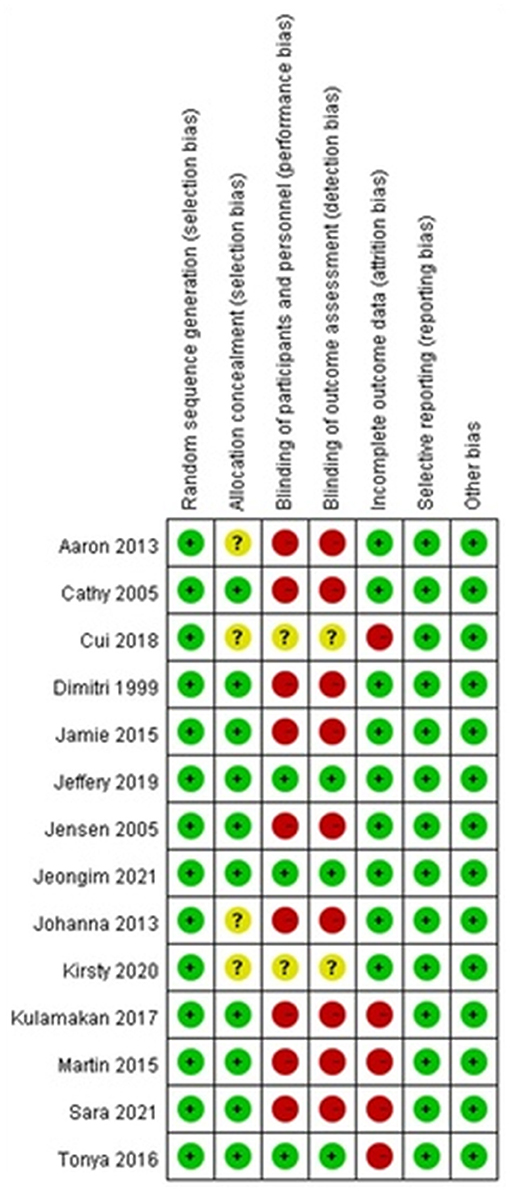
Figure 2. Risk of bias summary.
Effective Learning Transfer in the Final Task
Jensen et al. (19) reported a significant transfer effect when performing the second task, as there was a learning session in the first task. Butler et al. (21) reported that medical students were trained to perform diagnostic arthroscopy of the knee on anatomic dry models before training on cadaver specimens. Their average number of minimum proficiency tests and the average time of proficiency were significantly less than for those who only trained on cadaveric specimens. Kulamakan et al. (26) performed two sequential experiments. In Experiment 1, increasing context variation and conceptual analogies both significantly led to higher performance for far transfer. Experiment 2 demonstrated that even though there was a superficial similarity to previous examples, learners' shifts to using structural characteristics to classify new problems were caused by such analogies and context variation.
Yang et al. (27) reported that the participants performed appendectomy training in the virtual reality simulator before the tutorial procedural tasks of laparoscopic cholecystectomy, and needed significantly fewer movements and shorter path lengths than those who started with the tutorial procedural tasks of laparoscopic cholecystectomy directly. Anacleto et al. (30), after watching the video-mentored tutorial (VMT), observed a decrease in the total number of errors in peg-transfer (PT) and needle-guidance (NG) exercises in the participants who had watched the European Basic Laparoscopic Urologic Skills (E-BLUS) video before. Compared with the group in which students participated in a conventional demonstration of a Papanicolaou smear, Lee et al. (31) reported that self-confidence, learner satisfaction, and critical thinking were significantly higher in the simulation problem-based learning (S-PBL) group. After nine task repetitions over 3 weeks on one model, Ferguson et al. (23) reported that when the participants performing the knee and shoulder tasks swapped models, there was no immediate evidence of skill transfer.
The Most Effective Learning Transfer in Different Training Methods
Anastakis et al. (18) reported that bench and cadaver training were both superior to text learning and were equivalent. Tolsgaard et al. (24) reported that compared to the single-student composition, dyads illustrated higher training efficiency in terms of simulator score per number of attempts. Compared with nurses in the online self-study module, Rutherford-Hemming et al. (25) reported that the simulation group showed higher levels in both short-term and long-term skill performance.
Genç and Öner (28) reported that participants receiving an integrated instructional video performed significantly better on transfer than the procedural-only video. Beattie et al. (29) reported that groups trained in 3D and tested in 3D demonstrated superior training performance and took fewer repetitions to reach proficiency than the group in 2D.
The Effect of Guidance on Learning Transfer
The last two papers addressed in this study discuss the relationship between teacher guidance and learning transfer. While conducting research with 61 clinical nurse specialists as participants, Heaven et al. (20) assessed the three time points and observed that only those who experienced supervision showed any demonstration of transfer. Although neither group promoted more revelation of clues or concerns, people in the experimental group responded more effectively to the revealing clues. Bjurström et al. (22) reported that experienced surgeons performed significantly better than the control group and the self-guided training group. Between the educator-guided training group and the experienced surgeons, there was no significant difference. Nevertheless, having an educator present during training seemed to have a beneficial effect.
Discussion
Clinical Implication
Our study integrated the current findings of 14 studies and illustrated the correlation between the learning transfer and clinical performance of medical staff. However, the experimental items in each article based on learning transfer are not all the same. Therefore, we cannot compare them to determine which methods of learning transfer ensure significant clinical performance for medical staff. In short, we can only understand the transfer of learning in different fields based on a synthesis of current findings.
Previous research showed that learning transfer is considered a major influence on clinical performance (3). Learning in hospital settings encompassed both formal and informal activities. Formal learning means formalized and standardized education, including career staff training, preceptorships, maintenance education, and job training. Nonetheless, owing to the nature of shift work and the organizational complexity and diversity, it is not possible to make sure that medical staff can improve their clinical performance only through formal learning. Informal learning, which consists of communication, interaction with others, role modeling, and team-based learning, is more flexible and plays an important role in developing the medical staff's clinical performance, especially professional practice experience (32, 33). Informal learning is not simply passive inputting of information but involves constructing the meaning of information actively by recording accumulated long-term memory and existing experience. Therefore, it is crucial to decide which approaches should be used in informal learning, supporting continual self-directed learning.
In this study, we found better task performance after medical students were trained in the virtual simulator, which indicates that when knowledge and skills had common basic principles, the learning transfer would be apparent (27). Learners apply the acquired knowledge to the new learning or work, illustrating the importance of learning transfer to the clinical performance of medical staff and cultivating their practical ability and creative spirit. With an effective transfer, learners can learn faster and better in a limited time and transfer more accurately in the appropriate environment. It seems that learning transfer also depends on the direct instruction of teachers (3, 20), as instruction can more effectively promote learning transfer. The report showed no significant difference between the training group guided by educators and experienced surgeons (22). Nevertheless, strengthening guidance during learning can help students to improve their specific knowledge to general principles as early as possible.
The systematic review found that despite the lack of consistency in the duration of the intervention, practice time, assessment, and outcome measure, there is a significant learning transfer in the final task after interventions such as different training methods and guidance. According to the results, in order to make an effective learning transfer, professionals should focus on the following three points: (1) Look for the similarities between concepts and principles; (2) notice the summary of learning methods, that is, master the method of solving problems in the learning process, and (3) accumulate a wide range of learning experience in all aspects.
Clinical Practice
Owing to the developments of new technologies and the shift in the medical paradigm, E-Learning within the CBBL framework is seen as a very promising tool to prompt the advancement of learning transfer. Turk et al. explored that E-Learning within CBBL framework not only facilitates the creation of up-to-date teaching content but also addresses difficulties in transforming declarative knowledge into procedural knowledge and skill (34). Lütgendorf-Caucig highlighted that the integration of different teaching modalities is beneficial for the knowledge acquisition for clinical decision making in a multidisciplinary environment like oncology (35). It has been also emphasized in other studies that CBBL is an effective way in gaining improvements in performance among medical staff and is essential for associative and procedural learning that is necessary for clinical reasoning processes (36–39). Hence, we would recommend that the concept of interactive CBBL methods should be developed further and applied in other medical fields. To guarantee the high quality and employ correct didactic dimensions in terms of constructing the interactive questions, it may be helpful to create a guideline for question generation with the collaboration of medical education experts from their research field. Meanwhile, in order to provide a diversity of CBBL materials, further scientific, methodological, theoretical, and practice-based breakthroughs must be achieved.
Strength and Limitation
We individually evaluated these studies using assessment tools and covered most of the articles related to learning transfer. However, several limitations need to be addressed. First, few studies included questions on the reliability of the research results and the strength of the conclusions. Second, due to the considerable heterogeneity of research design and outcome variables, it was impossible to perform an effective meta-analysis. Third, the research objects participating in our review may have differed in analysis and generalizability. Finally, there may be interference from other related factors. Although the participants in some studies are similar in age, their sex ratios are quite different; moreover, nearly half of the studies did not clearly indicate this. In addition, there is currently a lack of studies that provide the quantitative results to meet the condition of performing an effective meta-analysis. We recommend that researchers conduct randomized controlled trials to further evaluate this correlation. We also recommend a study comparing the transfers of different interventions to provide more comprehensive and general findings.
Conclusion
Current evidence supports an association between learning transfer and the clinical performance of medical staff. However, it was noted that due to the lack of relevant research and the large differences in the methods and indicators used in previous studies, we were unable to conduct an effective meta-analysis. To summarize, medical staff should learn the importance of learning transfer and reinforce this ability through interdisciplinary teamwork and communication. Multi-disciplinary teaching approaches, assessments of existing systems and frameworks, and continuous technical improvements are still warranted in the future to optimize the current method of learning transfer and help medical staff make effective clinical decisions, as well as guarantee persistent satisfaction.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
Y-CT: conception and design. Y-CT, YX, and Y-pY: acquisition, analysis or interpretation of data, and statistical analysis. Y-CT and YX: drafting of the manuscript. T-HT: supervision. All authors have read and agreed to the published version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Church HR, Rumbold JL, Sandars J. Applying sport psychology to improve clinical performance. Med Teach. (2017) 39:1205–13. doi: 10.1080/0142159X.2017.1359523
2. Yang JJ. The influencing factors on clinical competence of nursing students. J Korean Acad Soc Nurs Educ. (2009) 15:159–65. doi: 10.5977/JKASNE.2009.15.2.159
3. Yun J, Kim DH, Park Y. The influence of informal learning and learning transfer on nurses' clinical performance: a descriptive cross-sectional study. Nurse Educ Today. (2019) 80:85–90. doi: 10.1016/j.nedt.2019.05.027
4. Gagne R. The The Conditions of Learning and Theory of Instruction Robert Gagné. New York, NY: Holt, Rinehart ja Winston (1985).
6. McKeachie WJ. Cognitive skills and their transfer: discussion. Int J Educ Res. (1987) 11:707–12. doi: 10.1016/0883-0355(87)90010-3
7. Baldwin TT, Ford JK. Transfer of training: a review and directions for future research. Pers Psychol. (1988) 41:63–105. doi: 10.1111/j.1744-6570.1988.tb00632.x
8. Burke LA, Baldwin TT. Workforce training transfer: A study of the effect of relapse prevention training and transfer climate. Hum Resour Manag. (1999) 38:227–41. doi: 10.1002/(SICI)1099-050X(199923)38:3<227::AID-HRM5>3.0.CO;2-M
9. Day D. Leadership development in the context of on-going work. Leadersh Q. (2000) 11:581–613. doi: 10.1016/S1048-9843(00)00061-8
10. Day S, Coiastone RL. The import of knowledge export. Connecting findings and Theories of transfer of learning. Educ Psychol. (2012) 47:153–76. doi: 10.1080/00461520.2012.696438
11. Pan SC, Rickard TC. Transfer of test-enhanced learning: Meta-analytic review and synthesis. Psychol Bull. (2018) 144:710–56. doi: 10.1037/bul0000151
12. Elliott B, Beck JA, Buffenbarger J. Learning transfer and transition of certified nursing assistants' to baccalaureate nursing programs. Nurs Forum. (2020) 55:197–204. doi: 10.1111/nuf.12416
13. Koukourikos K, Tsaloglidou A, Kourkouta L, Papathanasiou IV, Iliadis C, Fratzana A, et al. Simulation in clinical nursing education. Acta Informatica Medica. (2021) 29:15. doi: 10.5455/aim.2021.29.15-20
14. Avraham R, Shor V, Kimhi E. The influence of simulated medication administration learning on the clinical performance of nursing students: a comparative quasi-experimental study. Nurse Educ Today. (2021) 103:104947. doi: 10.1016/j.nedt.2021.104947
15. Johnston S, Nash R, Coyer F. An evaluation of simulation debriefings on student nurses' perceptions of clinical reasoning and learning transfer: a mixed methods study. Int J Nurs Educ Scholarsh. (2019) 16. doi: 10.1515/ijnes-2018-0045
16. Wadowski PP, Litschauer B, Seitz T, Ertl S, Löffler-Stastka H. Case-based blended eLearning scenarios-adequate for competence development or more? Neuropsychiatr. (2019) 33:207–11. doi: 10.1007/s40211-019-00322-z
17. Turk B, Ertl S, Wong G, Wadowski PP, Löffler-Stastka H. Does case-based blended-learning expedite the transfer of declarative knowledge to procedural knowledge in practice? BMC Med Educ. (2019) 19:447. doi: 10.1186/s12909-019-1884-4
18. Anastakis DJ, Regehr G, Reznick RK, Cusimano M, Murnaghan J, Brown M, et al. Assessment of technical skills transfer from the bench training model to the human model. Am J Surg. (1999) 177:167–70. doi: 10.1016/S0002-9610(98)00327-4
19. Jensen E. Learning and transfer from a simple dynamic system. Scand J Psychol. (2005) 46:119–31. doi: 10.1111/j.1467-9450.2005.00442.x
20. Heaven C, Clegg J, Maguire P. Transfer of communication skills training from workshop to workplace: the impact of clinical supervision. Patient Educ Couns. (2006) 60:313–25. doi: 10.1016/j.pec.2005.08.008
21. Butler A, Olson T, Koehler R, Nicandri G. Do the skills acquired by novice surgeons using anatomic dry models transfer effectively to the task of diagnostic knee arthroscopy performed on cadaveric specimens? J Bone Joint Surg Am. (2013) 95:e15. doi: 10.2106/JBJS.L.00491
22. Bjurström JM, Konge L, Lehnert P, Krogh CL, Hansen HJ, Petersen RH, et al. Simulation-based training for thoracoscopy. Simul Healthc. (2013) 8:317–23. doi: 10.1097/SIH.0b013e31828df760
23. Ferguson J, Middleton R, Alvand A, Rees J. Newly acquired arthroscopic skills: Are they transferable during simulator training of other joints? Knee Surg Sports Traumatol Arthrosc. (2017) 25:608–15. doi: 10.1007/s00167-015-3766-6
24. Tolsgaard MG, Madsen ME, Ringsted C, Oxlund BS, Oldenburg A, Sorensen JL, et al. The effect of dyad versus individual simulation-based ultrasound training on skills transfer. Med Educ. (2015) 49:286–95. doi: 10.1111/medu.12624
25. Rutherford-Hemming T, Kelsey NC, Grenig DL, Feliciano M, Simko L, Henrich CM. Multisite single-blinded randomized control study of transfer and retention of knowledge and skill between nurses using simulation and online self-study module. Simul Healthc. (2016) 11:264–70. doi: 10.1097/SIH.0000000000000168
26. Kulasegaram KM, Chaudhary Z, Woods N, Dore K, Neville A, Norman G. Contexts, concepts and cognition: principles for the transfer of basic science knowledge. Med Educ. (2017) 51:184–95. doi: 10.1111/medu.13145
27. Yang C, Kalinitschenko U, Helmert JR, Weitz J, Reissfelder C, Mees ST. Transferability of laparoscopic skills using the virtual reality simulator. Surg Endosc. (2018) 32:4132–7. doi: 10.1007/s00464-018-6156-6
28. Genç HD, Öner NAS. Why not activated? The temporary protection directive and the mystery of temporary protection in the European Union. Int J Polit Sci Urban Stud. (2019) 7:1–18. doi: 10.14782/ipsus.539105
29. Beattie KL, Hill A, Horswill MS, Grove PM, Stevenson ARL. Laparoscopic skills training: the effects of viewing mode (2D vs. 3D) on skill acquisition and transfer. Surg Endosc. (2021) 35:4332–44. doi: 10.1007/s00464-020-07923-8
30. Anacleto S, Mota P, Fernandes V, Carvalho N, Morais N, Passos P, et al. Can narration and guidance in video-enhanced learning improve performance on E-BLUS exercises? Cent European J Urol. (2021) 74:131–8. doi: 10.5173/ceju.2021.0005
31. Lee J, Son HK. Comparison of learning transfer using simulation problem-based learning and demonstration: an application of papanicolaou smear nursing education. Int J Environ Res Public Health. (2021) 18:1765. doi: 10.3390/ijerph18041765
32. Choonara S, Goudge J, Nxumalo N, Eyles J. Significance of informal (on-the-job) learning and leadership development in health systems: lessons from a district finance team in South Africa. BMJ Glob Health. (2017) 2:e000138. doi: 10.1136/bmjgh-2016-000138
33. Kim HR, Song Y, Lindquist R, Kang HY. Effects of team-based learning on problem-solving, knowledge and clinical performance of Korean nursing students. Nurse Educ Today. (2016) 38:115–8. doi: 10.1016/j.nedt.2015.12.003
34. Turk BR, Krexner R, Otto F, Wrba T, Löffler-Stastka H. Not the ghost in the machine: transforming patient data into e-learning cases within a case-based blended learning framework for medical education. Procedia Soc Behav Sci. (2015) 186:713–25. doi: 10.1016/j.sbspro.2015.04.106
35. Lütgendorf-Caucig C, Kaiser PA, Machacek A, Waldstein C, Pötter R, Löffler-Stastka H. Vienna Summer School on Oncology: how to teach clinical decision making in a multidisciplinary environment. BMC Med Educ. (2017) 17:100. doi: 10.1186/s12909-017-0922-3
36. Wadowski PP, Steinlechner B, Schiferer A, Löffler-Stastka H. From clinical reasoning to effective clinical decision making-new training methods. Front Psychol. (2015) 6:473. doi: 10.3389/fpsyg.2015.00473
37. Chéron M, Ademi M, Kraft F, Löffler-Stastka H. Case-based learning and multiple choice questioning methods favored by students. BMC Med Educ. (2016) 16:41. doi: 10.1186/s12909-016-0564-x
38. Kassirer JP. Teaching clinical reasoning: case-based and coached. Acad Med. (2010) 85:1118–24. doi: 10.1097/ACM.0b013e3181d5dd0d
Keywords: learning transfer, clinical performances, medical staff, systematic review, randomized controlled trials
Citation: Tung Y-C, Xu Y, Yang Y-p and Tung T-H (2022) The Effects of Learning Transfer on Clinical Performances Among Medical Staff: A Systematic Review of Randomized Controlled Trials. Front. Public Health 10:874115. doi: 10.3389/fpubh.2022.874115
Received: 11 February 2022; Accepted: 26 May 2022;
Published: 05 July 2022.
Edited by:
Youcheng Liu, Wayne State University, United StatesReviewed by:
Ratree Sawangjit, Mahasarakham University, ThailandHenriette Loeffler-Stastka, Medical University of Vienna, Austria
Copyright © 2022 Tung, Xu, Yang and Tung. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tao-Hsin Tung, Y2gyODc2QHllYWgubmV0; Yu-pei Yang, eWFuZ3lwQGVuemVtZWQuY29t