 Jingjing Zhou
Jingjing Zhou Jianfang Zhou
Jianfang Zhou Hongyang Zhang3
Hongyang Zhang3 Junwei Zhang
Junwei Zhang- 1School of Sociology and Population Studies, Nanjing University of Posts and Telecommunications, Nanjing, China
- 2School of Population Studies, Nanjing University of Posts and Telecommunications, Nanjing, China
- 3Department of Sociology, School of Social Sciences, Tsinghua University, Beijing, China
- 4College for Philosophy and Political Sciences, Shanghai Normal University, Shanghai, China
The rise of migrant workers has been a unique social phenomenon as China goes through industrialization, urbanization, and modernization. They are a special social group formed during the economic and social transition of the country. Migration of rural labor has pushed China on its new path toward industrialization and urbanization. Because of the urban-rural dual system of the country, however, it is difficult for migrant workers to be fully integrated into host cities, making them susceptible to negative emotions and mental health issues. Therefore, their mental health is an issue of great volume in the domains of social undertakings, people's livelihood, and public health. However, existing studies have paid limited attention to the psychological profile of migrant workers and even less to the interplays among their social capital, social integration, and mental health. Targeting China's internal migrant workers, this article tapped the interactions among their social integration, social capital, and mental health with a sample of the cross-sectional data from the China Labor Dynamics Survey (CLDS) in 2018. Multi-group structural equation modeling (SEM) was employed to test the moderating action of age by analyzing whether the mediation model differed significantly in the paths among young, middle-aged, and older migrant workers. The SEM based on bootstrapping suggested that, after controlling for the influence of gender, education, marital status, personal annual income, employer type, and self-rated health, migrant workers' social capital positively affect their mental health in a significant way, with social integration playing a mediating role. In terms of age difference, middle-aged migrant workers were more subject to the aforementioned mechanism than young ones, and young migrant workers were more affected by the mechanism than older ones. This study revealed different psycho-social interplays among social capital, social integration, and mental health across young, middle-aged, and elderly migrant workers. The findings could serve as an important theoretical reference and as practical guidance for improving policies concerning migrant workers' mental health and social benefits in the context of economic transition.
Introduction
Thanks to economic globalization, international migrant workers worldwide have counted 189 million, representing the vast majority of international migrants (1). In China, there are as many as 285 million migrant workers, also known as internal migrants for work (2). They are a special social group formed in, and main contributor to, China's industrialization, urbanization, and modernization, and the rise of this class of workers is a unique social scene over the course of China's economic and social transformation (3). Generally speaking, migrant workers are workers born in rural areas, migrated to towns or cities to engage in non-agricultural work, but still have rural hukou or registered permanent residence (4). However, due to the segregation of cities and the countryside in China and the restrictions established by the household registration system, migrant workers can hardly obtain citizenship and the same social benefits as the locals (5). In addition, because of the large gaps in human capital and economic capital from the locals, most migrant workers are employed in the secondary labor market and live in urban fringe areas, making them susceptible to negative emotions and mental health issues (6).
Generally, personal endowment, migration distance, migration pattern, and social environment are regarded as the main factors affecting migrants' mental health (7). However, in the context of social transformation in China, frequent migration and mobility have brought about the reconstruction and transformation of such social capital as social networks and social trust of migrant workers, which directly affects their perception and digestion of negative emotions (8). In recent years, how social capital acts on mental health has been subject to extensive discussion in academic circles (9). Besides, in the absence of institutional support for citizenization and the deficiency in personal endowment of migrant workers, social capital embedded in social networks can effectively reduce the economic cost, psychological cost, and various risks in the process of migration; this helps their fusion with the local environment in economic, cultural, psychological, and identity terms (10). In the light of social capital promoting social integration, the social inclusion of migrant workers further improves their mental health by improving the sense of belonging and subjective wellbeing (11). This provides an empirical indication that social integration serves as a mediator in social capital acting on the mental health among internal migrant workers in the Chinese context (12).
In addition, large-scale migration of people from rural areas to cities for work has continued for more than 30 years in China (13). Along with social transformation and changes, the social differentiation within the migrant worker group has intensified, which is prominently manifested in the intergenerational differentiation between the elderly migrant workers (i.e., the first-generation migrant workers) and the middle-aged and young migrant workers (i.e., the new-generation migrant workers) (14). Significant differences exist among the three migrant worker subgroups when it comes to social capital, social integration, and mental health (15); however, research on the mechanism of action among migrant workers' social capital, social integration, and mental health has rarely combined with the age difference of migrant workers (16). Therefore, targeting migrant workers in China, this article gleaned the cross-sectional data from the 2018 China Labor Dynamics Survey (CLDS) to probe the links among social capital, social integration, and mental health, to examine how social integration acts as a mediator in social capital acting on mental health, and to conduct multi-group testing of age differences in the above mechanism with view to providing theoretical insight and practical guidance for improving policies concerning migrant workers' mental health and social benefits in the context of economic transformation.
Literature Review
Social Capital and Mental Health
Divided into individual and collective levels, social capital from an individual's perspective refers to the resources embedded in the individual's social relationship network, while collectively, it entails the trust, reciprocity, and norms within a group (17). Numerous empirical studies have proposed that for migrant workers social capital can significantly improve their mental health (18), which has been applied to mental health promotion programs (19). Using the stress process model, some scholars pointed out that social capital can alleviate perceived stress and buffer the negative impact of life events, and thereby promote mental health (20). Some scholars have noted how community-based social capital acts on the mental health, arguing that community-based cognitive social capital can promote mutual trust between migrants and local residents, eliminate the state of exclusion among floating populations, and create a good atmosphere for the community (21). However, divergence persists in academic circles about how social capital affects mental health (22). Some scholars opined that cognitive social capital (social trust, for instance) and mental health are positively correlated, but that structural social capital (social network, for instance) is not significantly correlated with mental health (23).
Social Capital and Social Integration
Social integration or inclusion is an interactive and multi-dimensional dynamic process. Social capital can help migrant workers obtain resources from social networks that deliver instrumental or emotional support, while social trust helps them to achieve physical goals (24). At present, that the social capital positively acts on the social inclusion of migrant workers has been widely discussed in academic circles (25). The positive influence of migrant workers' social capital on their social integration has been demonstrated from the perspective of resource acquisition—i.e., migrant workers obtain valuable information, social support and material assistance through social capital to promote their social integration (26). For example, Lancee (27) found that migrant workers glean recruitment information (and, thus, job opportunities) through social networks to promote their economic integration. Other scholars discussed how social capital positively acted on the inclusion of migrant workers from the aspects of culture and identity—i.e., that social networking and social participation can help migrant workers form positive social connections with local residents, promote mutual understanding, and gain a sense of belonging and identity in host cities (28). However, some scholars have pointed out that over-reliance on ascribed social relationships in social networks may result in difficulties in social inclusion (29).
Mental Health and Social Integration
In Chinese context, migrant workers' social integration or inclusion is defined as the reduction of their objective and subjective differences from urban citizens, so as to reduce the negative influence of social class inequality on mental health (30). A host of empirical studies have shown that a higher degree of social inclusion corresponds to better mental health (31, 32). Research in light of attachment theory has examined how social integration promoted mental health, finding that migrant workers with a higher degree of social inclusion enjoy a greater sense of group belonging and meaning in life, and hence lower possibility of depression (33). For example, Chen et al. (34) pointed out that migrant workers' strong attachment to the countryside may lead to lower satisfaction with their lives in the cities, but that with a higher degree of social integration, migrant workers will see their urban identity and sense of belonging significantly increase, hence better mental health. Other scholars have discussed how social integration positively acted on mental health from the viewpoint of social equality, arguing that migrant workers with a higher degree of social inclusion have a lower sense of relative deprivation, stronger sense of social equality, and better mental health (35).
Social Capital, Social Integration and Mental Health
Plenty of studies have scrutinized how social capital and social integration each acts on mental health (36, 37). For example, Steel (38) pointed out that the more trusted friends migrants have, the higher their social trust, and the better their social integration is promoted, and that this improves self-rated health. However, there is a lack of well rounded and sharply defined research and empirical explanations on the mechanism of interplay among migrant workers' social capital, social integration and mental health. Furthermore, some scholars have posited that social capital does not necessarily positively affect mental health and its positive effect on mental health is more significant in a more harmonious social environment; this offers theoretical possibilities for discussing social inclusion to mediate the action of social capital on mental health (39). Other scholars have pointed out that to investigate how social capital affects mental health one needs to consider its applicable objects and that the perspectives of intergroup interaction and life course can help clarify the link between mental health and social capital (40).
Age Difference
At present, Western scholars pay less attention to age difference in the associations among social capital, social integration, and mental health (41, 42). Some scholars have observed based on critical reviews on migrant health research that the introduction of a life course perspective helps clarify the distribution of the effect of social determinants on health among migrant populations (43, 44). With regards to the Chinese context, some scholars have noted intergenerational differences concerning social capital, social inclusion, and mental health of migrant workers, but most of them discuss the intergenerational differences from one single dimension and from the perspective of characteristics comparison (45). In China, elderly migrant workers (that is, the first-generation migrant workers) have relatively closed and homogenous social networks, mainly generated from blood, kinship, and geographical ties in rural areas, which thus implies a stronger sense of attachment to the countryside and a lower desire to integrate into the city than that of young and middle-aged ones (46). In the meantime, compared with middle-aged and elderly migrant workers, young migrant workers have a higher perception of social integration, and thus poor social integration is more likely to lead to a decline in their mental health (47). In addition, a small number of scholars have verified the intergenerational differences in the mechanism of action on migrant workers' mental health in combination with life course theory (48, 49). These studies provide empirical support to discuss intergenerational differences in the mechanism of action among migrant workers' social capital, social integration and mental health.
Gaps in Existing Literature and Establishment of Current Hypotheses
Most of the existing research has examined how social capital and social inclusion each acts directly on the mental health for migrant workers (50, 51), or explains how social capital affects social integration among migrant workers (4). However, there has been no research offering a comprehensive exposition of the mechanism of interplay among migrant workers' social capital, social integration, and mental health. In addition, most of the existing research has discussed the intergenerational differences among migrant workers' social capital, social integration, and mental health from a single dimension (52). Whether the intensity of social capital and social integration acting on mental health differs among young, middle-aged, and elderly migrant workers has not been fully verified. Therefore, this study established a comprehensive conceptual framework to tap the interplays among social capital, social integration, and mental health status among internal migrant workers in China, as well as age differences therein (see Figure 1). Three core hypotheses were examined. H1: The higher the level of social capital, the better the mental health. H2: An increase in the level of social capital will improve social integration, thereby enhancing mental health. H3: How social capital acts on mental health through social integration may vary by age.
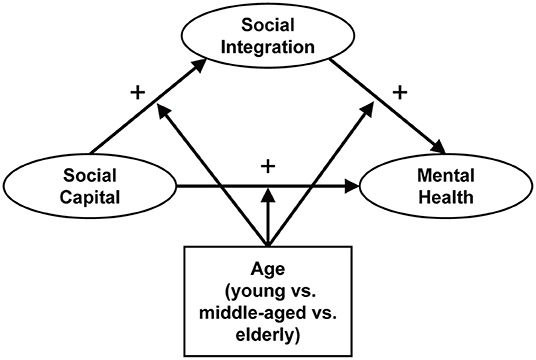
Figure 1. Conceptual framework.
Methods
Data
This study sourced the data from the 2018 China Labor Dynamics Survey (CLDS). A comprehensive social survey in large scale, the CLDS is designed and implemented by the Center for Social Science Survey at Sun Yat-sen University in China. It adopts a multi-stage, multi-level, and probability proportional to size of labor force sampling method, covering the labor population aged 15–64 in 29 provinces, cities, and autonomous regions across the country. The survey was officially launched in 2012 and is carried out every 2 years. The latest survey was in 2018. This study defined migrant workers as 15–64-year-old non-agricultural laborers in urban areas with an agricultural household registration (53). After removing those with missing values for key variables—accounting for 1.8% of the population- the effective sample finally consisted of 8,346 individuals.
Measures
Dependent Variable
The degree of depression was used herein to measure the mental health (54). Cai and Xu (55) questionnaire asked about the occurrence of 20 conditions in the past week: “I am troubled by some trivial stuff,” “I have not appetite to eat,” “Even if my family and friends help me, I still can't get rid of my depression,” “I feel I'm worse than most people,” “I'm depressed,” “I can't concentrate when I do things,” “I feel exhausted with everything,” “I feel hopeless,” “I think my life is a failure,” “My sleep quality is bad,” “I'm scared,” “I feel unhappy,” “I don't talk as much as usual,” “I feel lonely,” “I feel my life is boring,” “I feel people are not very kind to me,” “I used to cry,” “I feel apprehensive,” “I don't feel liked by people,” and “I don't think I can go about my daily work.” The frequency options were “1 = 5–7 days, 2 = 3–4 days, 3 = 1–2 days, and 4 = less than 1 day,” in which higher values indicated lower degrees of depression and hence better mental health.
Independent Variable
In the research on migrant workers, scholars often use Putnam's definition of social capital (56), arguing that social capital mainly consisted three parts (network, trust, and reciprocity) and divided into two types: cognitive social capital, including trust, reciprocity, etc., which is marked by pronounced individual subjective wishes, and structural social capital, including social participation, socializing frequency and pattern, etc., which is susceptible to objective conditions (57). Therefore, social capital was measured in this study from two aspects: social trust and social network. CLDS (2018) questionnaire divided social trust from the perspective of specific objects into nine categories. They were trust in, respectively, family members, neighbors, schoolmates, fellow villagers, strangers, colleagues, vendors, and religious believers, rated by level of trust from low to high (1 = completely untrustworthy, 5 = completely trustworthy). Regarding the social network, the questionnaire includes “How often does mutual help occur between you and your neighbors and other residents of this community?” with options on an ascending scale from 1 = never to 5 = always.
Mediating Variable
To measure social integration, most studies include such dimensions as economic inclusion, acculturation, identity fusion, and psychological inclusion (58), which may vary in denotation but are similar in connotation and measures (59). The present study applied the same division of social integration for migrant workers. Among them, economic integration refers to the integration in terms of employment, income and social security (60). It was measured by self-assessment of family economic status. The questionnaire asked the following question: “Generally speaking, how do you feel about the economic status of your family?” with options in such order from low to high as 1 = very dissatisfied to 5 = very satisfied. Cultural integration refers to familiarity with the language, lifestyle, and social customs of the inflow area and the degree of participation in cultural activities (61). It was measured by dialect proficiency. The following question was asked in the questionnaire: “How well have you mastered the local dialect?” (1 = none, 2 = little, 3 = partially, 4 = mostly, 5 = totally). Psychological integration refers to the psychological judgment of the degree of satisfaction and happiness in life in a city or town (62). It was measured by subjective wellbeing, and the following question was inquired: “Overall, how happy do you think your life is?” with the level of happiness assigned with values ranging from 1 = very unhappy and 5 = very happy. Identity integration refers to one's psychological distance from locals and fellow villagers, sense of belonging, and perception of where one is going in future. It was measured by whether to settle locally. The questionnaire asked the following question: “Are you likely to settle locally in the future?” with options in an ascending order from 1 = very unlikely to 5 = very likely).
Covariates
Seven demographic characteristics and two family elements constituted the covariates. The seven demographic variables were gender (0 = male, 1 = female); education (0 = none, 1 = primary school, 2 = junior high school, 3 = high school, 4 = bachelor's, 5 = master's); employer type: administration (0 = no, 1 = yes), enterprise or social organization (0 = no, 1 = yes), individual business (0 = no, 1 = yes), and freelance or non-regular job (0 = no, 1 = yes); and self-rated health (1 = very unhealthy, 5 = very healthy). The two family elements were marital status (0 = single, 1 = married) and personal annual income.
Analytical Approach
SPSS 23.0 was used to organize data, sort out descriptive statistics before correlation analyses. According to the research purpose, Amos24.0 was used to establish and analyze the measurement model and the structural model among variables. Such indices as chi-square (χ2), comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized residual mean square root (SRMR) were used to evaluate the goodness of the model-data fit. Specifically, non-significant chi-square values (p > 0.05), CFI and TLI above 0.90, and RMSEA and SRMR below 0.08 each denote a good fit (63). Bootstrapping was used to test the mediating effect (5,000 re-samples), in which the effect is deemed significant with the 95% confidence interval (CI) not including 0 (64). In addition, multi-group structural equation was used to evaluate the age difference in the overall model, in which the critical ratio of difference (CRD) was used to compare the structural path coefficients across groups. If the absolute value of the CRD is higher than 1.965, then there is an inter-group difference at the level of p < 0.05 (65).
Results
Descriptive Statistics and Correlation Analyses
The descriptive statistical results of the demographic variables herein are show in Table 1. Among the 8,346 migrant workers sampled, 39.5% were aged 31–50, which means that middle-aged migrant workers represented the largest proportion of the surveyed. Slightly more male migrant workers were surveyed than female ones (54.4%); most of the participants had finished middle school (38.9%); about four-fifths were married (81.4%); and they mostly worked for enterprises or social organizations (37.2%). In terms of self-rated health, most migrant workers had a good self-assessed health status (43.6%). As seen from Table 2, social capital, social inclusion, and mental health were significantly positively correlated, indicating a significant correlation among the key variables involved in this study, thereby satisfying the prerequisites of the mediation effect test (66).
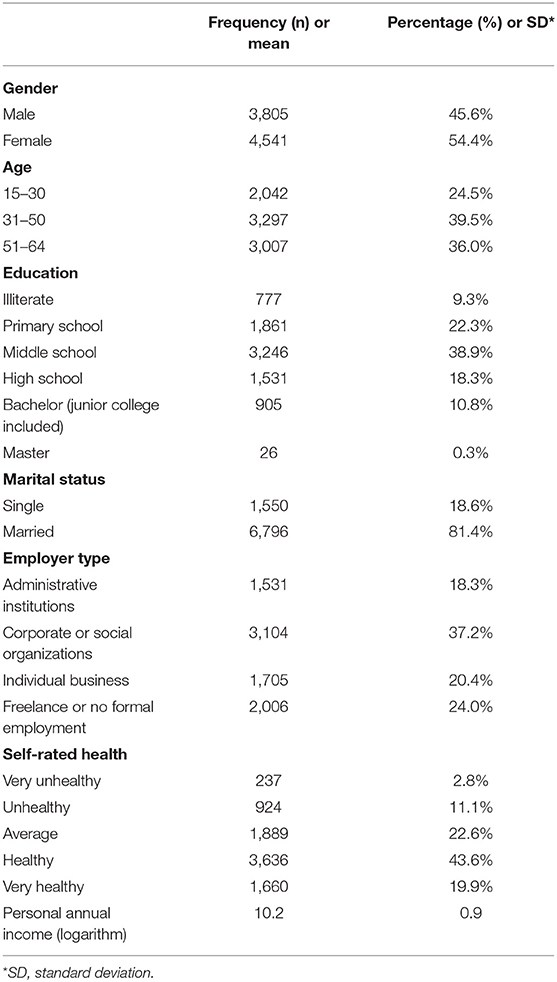
Table 1. Descriptive statistics of variables (N = 8,346).
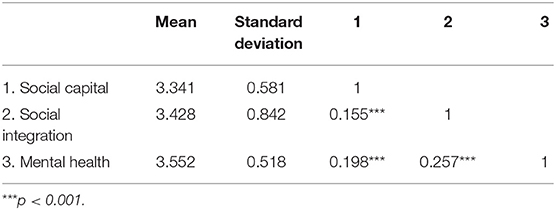
Table 2. Correlation analyses among key variables.
Measurement Model
Results from testing the scales of social capital and social integration showed that the Cronbach's alpha coefficients of social capital and social integration were 0.706 and 0.820, respectively, both greater than 0.7, indicating a good reliability (67).
The adequacy of fit was evaluated with the confirmatory factor analysis (CFA). The model included two latent variables: social capital and social integration. Results showed a good model-data fit with chi-square = 22.749 (p < 0.01; df = 8), CFI = 0.999, and RMSEA = 0.015. All factor loadings of latent variables were significant at the p < 0.001 level, among which the factor loading ranges for social integration and social integration were 0.742–0.827 and 0.667–0.848, respectively. The CR values of the latent variables were 0.763 and 0.825, both >0.6, and the AVE values were 0.617 and 0.543, both >0.5, indicating acceptable convergent validity of the model. Furthermore, multi-group analyses showed that the model was invariant among migrant workers of different ages at the configural, metric, and scalar levels.
Structural Model
The structural model had the fit indices: chi-square = 191.851, df = 44, p < 0.001, CFI = 0.994, TLI = 0.986, and RMSEA = 0.020, indicating a good model-data fit. The full-sample model as shown in Figure 2 and Table 3 suggested that social capital positively acted on the mental health in a significant way (β = 0.187, p < 0.001)—i.e., the higher the level of social capital, the better the mental health, confirming H1. Social integration mediated in an important way the link between social capital and mental health. Specifically, improved social capital contributed to higher degrees of social integration (β = 0.180, p < 0.001), thereby improving mental health (β = 0.208, p < 0.001) among migrant workers, confirming H2.
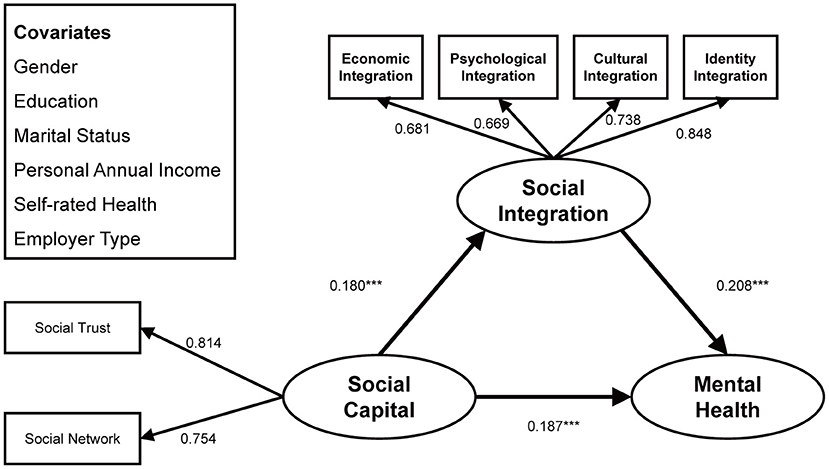
Figure 2. Standardized structural model (Full sample). ***p < 0.001.
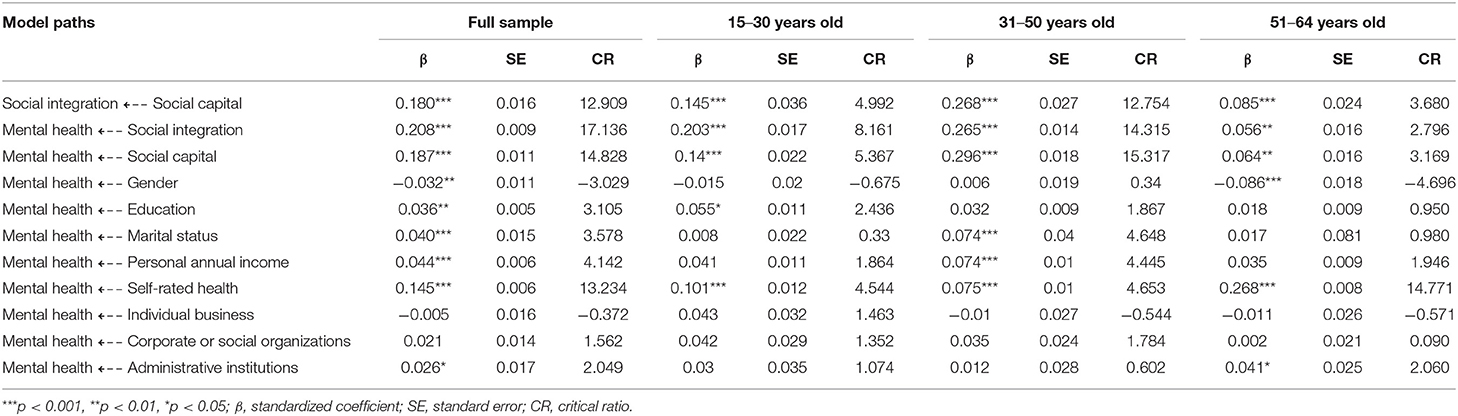
Table 3. Results of structural model for full sample and subsamples.
Among the covariates, mental health was better in male migrant workers than in female ones (β = −0.032, p < 0.01); those with higher education levels were more mentally healthy (β = 0.036, p < 0.01); compared with unmarried ones, married migrant workers had better mental health (β = 0.040, p < 0.001); a higher income corresponded to better mental health (β = 0.044, p < 0.001); better self-assessed health status indicated better mental health (β = 0.145, p < 0.001); migrant workers working in administrative or public institutions had better mental health than freelance or non-regularly employed ones (β = 0.025, p < 0.05), but other employer types had no significant correlation with the mental health. Overall, the full-sample model explained 9.2% of the variance in social integration and 14.3% of the variance in mental health status. The bootstrapping results are shown in Table 4. Social integration mediated the action of social capital on the mental health [β = 0.037, 95% bootstrap CI (0.03, 0.046)], accounting for 16.4% of the total effect [β = 0.225, 95%bootstrap CI (0.197, 0.252)], in which the indirect effect was indicated significant with the bootstrap 95% confidence interval not containing 0.
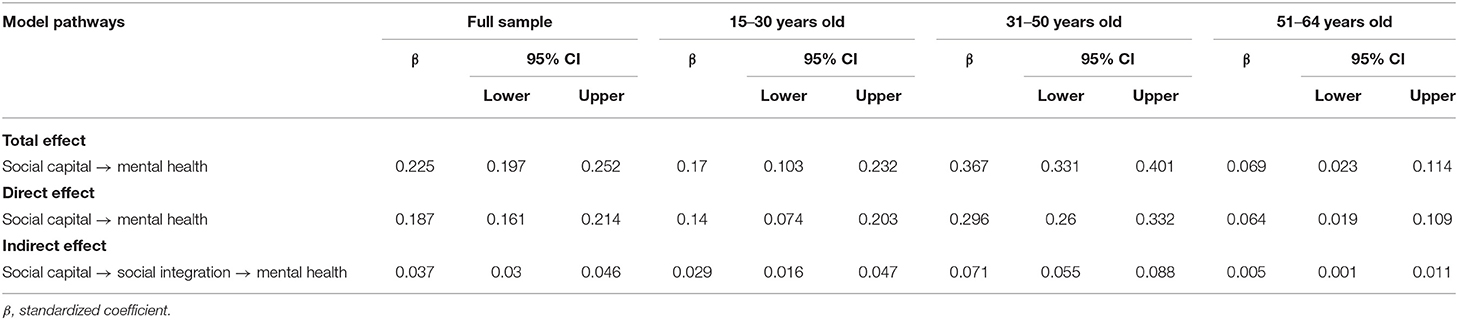
Table 4. Direct and indirect effects and 95% confidence intervals (CI).
Group Difference Test
Multi-group analyses in SEM were conducted to verify any significant difference in path coefficients due to age. First, the measurement model was found to be invariant (p > 0.05)—that is, the factor loadings were equal across age groups; secondly, we compared the unconstrained structural model where the structural path changed with age with the constrained one, in which the factor loadings, covariances, weights, residuals, etc. were set equal across young workers (15–30 years old), middle-aged migrant workers (31–50 years old) and elderly migrant workers (51–64 years old). The results showed a significant difference (p < 0.001) between the unconstrained model (χ2 = 324.563, df = 132) and the constrained one (χ2 = 682.186, df = 178).
The CRD tests showed significant divergences across young, middle-aged, and older migrant workers in the three pathways. First, significant divergences existed between young and middle-aged subgroups, between young and elderly subgroups, and between middle-aged and elderly subgroups in the path coefficient of social capital to mental health (CRD = −5.606, p < 0.05, CRD = 2.423, p < 0.001, and CRD = 9.265, p < 0.001, respectively). Secondly, significant divergences were seen in the path coefficient of social capital to social integration between young and middle-aged subgroups, between young and elderly subgroups, and between middle-aged and elderly subgroups (CRD = −3.761, p < 0.001, CRD = 2.136, p < 0.05, and CRD = 7.235, p < 0.001, respectively). Finally, significant divergences were seen in the path coefficient of social integration to mental health between young and middle-aged subgroups, between young and elderly subgroups, and between middle-aged and elderly subgroups (CRD = −2.481, p < 0.05, CRD = 4.096, p < 0.001, and CRD = 7.179, p < 0.001, respectively).
As shown in Figures 3–5 and Table 3, the above three structural paths had significant positive effects on young, middle-aged and elderly migrant workers, but the degree of effect varied. Specifically, on the path from social capital to mental health, the effect on the middle-aged subgroup (β = 0.296, p < 0.001) was more significant than that on the young subgroup (β = 0.140, p < 0.001), which in turn was greater than that on the elderly subgroup (β = 0.064, p < 0.001); on the path connecting social capital to social integration, the middle-aged subgroup (β = 0.268, p < 0.001) were more affected than the young subgroup (β = 0.145, p < 0.001), and the young subgroup was more affected than the elderly group (β = 0.085, p < 0.001); on the path connecting social capital to mental health, the middle-aged subgroup was more affected (β = 0.265, p < 0.001) than the young subgroup (β = 0.203, p < 0.001), who was more affected than the elderly subgroup (β = 0.056, p < 0.001).
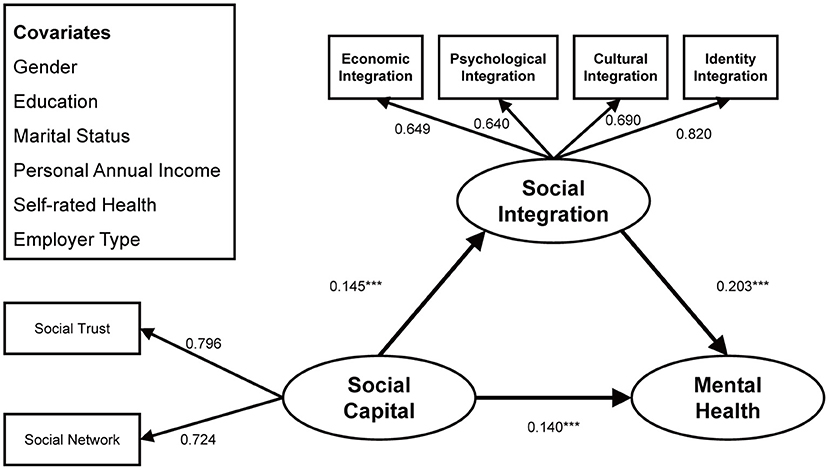
Figure 3. Standardized structural model (sub-sample: 15–30 years old). ***p < 0.001.
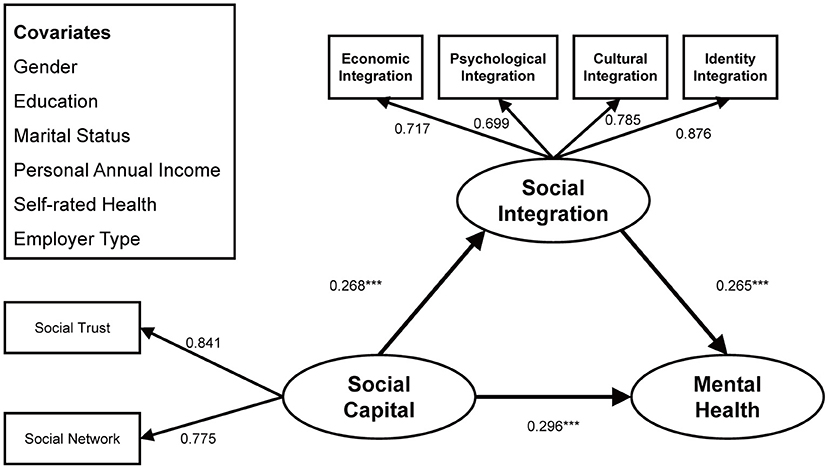
Figure 4. Standardized structural model (sub-sample: 31–50 years old). ***p < 0.001.
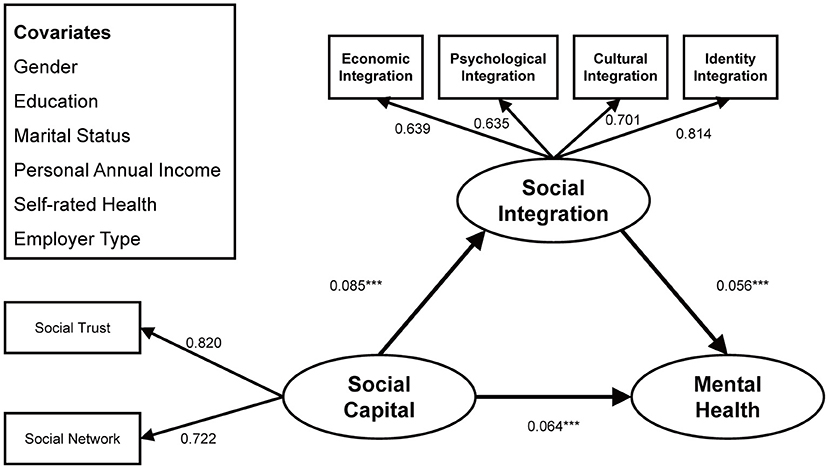
Figure 5. Standardized structural model (sub-sample: 51–64 years old). ***p < 0.001.
Discussion
Targeting migrant workers in the context of China's social transformation, this article investigated the interplays among their social capital, social inclusion/integration, and mental health, elucidated the mechanism of social integration mediating the way social capital acts on mental health, and provided theoretical support and coping strategies for bettering migrant workers' mental health.
The results show that enhanced social capital of migrant workers could effectively improve their mental health, a finding that supported H1 and kept with previous findings. Cognitive social capital (represented by trust) and structural social capital (represented by social network) are both significantly related to health status (68, 69). For migrant workers, improved social trust helps reduce the incidence of depression, and those with higher levels of social trust are better positioned to establish harmonious interpersonal relationships, which helps relieve tension and fear in urban life, and tend to have more positive psychological expectations when facing psychological difficulties, all of which significantly enhance their mental health (70). In terms of social network, on the one hand, migrant workers improve their economic capabilities by working, which can effectively resolve frictions and conflicts among family members, and can increase the sense of attachment between them, enhance the supportive role of the ascribed social network, and alleviate their mental pressure (71); on the other hand, the social network constructed and expanded by migrant workers in the city by working can effectively reduce the various pressures they face in the city, thereby curbing the psychological crisis (72).
Additionally, this study found that migrant workers with more social capital had a higher degree of social integration, thereby improving their mental health, which supported H2. This finding is considered an innovation in this study, which explains the interplays among social capital, social inclusion, and mental health of internal migrant workers by constructing a fresh framework. In China, where “social relations” are highly valued, social capital plays a more meaningful role than human capital (73). For migrant workers who lack both human capital and economic capital, their economic activities such as job hunting rely more on social network (74), so social capital promotes the economic inclusion of migrant workers. Besides, social capital provides an important way for migrant workers to participate in cultural activities, adapt to new urban lifestyles, and acquire a sense of identity, which supports achievement of expressive goals and enhances psychological integration and identity integration (75). On the basis that social capital promotes the improvement of social integration, social integration affects the mental health of migrant workers through health behavior influence paths, psychological influence paths, and physiological influence paths (76). For example, social integration can improve mental health by increasing individual control, sense of belonging, and generalized trust (77).
Multi-group analyses by age also provided valuable findings. The social integration-mediated action of social capital on mental health differed along age lines, a finding that supported H3. On the three paths by which social capital affected mental health, social capital affected social inclusion, and social inclusion affected mental health, middle-aged migrant workers (31–50 years old) were more affected than young migrant workers (15–30 years old), while the effect on young migrant workers exceeded that on older migrant workers (51–64 years old). Combined with the life course theory, when social changes have different effects on the cohorts of different generations, due to the obvious similarity in the experience of the same generation, the conditions of different generations tend to show significant differences, and therefore, the historical effect of life trajectories is manifested in the experiences of different generations (78). In China, the first generation of internal migrant workers (older migrant workers) emerged after the reform and opening up of the country, and the new generation (middle-aged and young migrant workers) emerged in the early 2000s. The new generation, compared with the first generation, has seen the economic and social situation undergo tremendous changes, leading to differences across the three subgroups in the mechanisms of interaction between social capital, social integration, and mental health (79). Compared with older migrant workers, middle-aged and young migrant workers generally have higher levels of education, higher occupational expectations, and more opportunities to move between urban and rural areas. With greatly improved social security and labor security systems, young and middle-aged migrant workers are in better positions than the elderly migrant workers with regards to both social network and social capital such as social trust, and enjoy a higher degree of multi-dimensional social integration in economy, psychology, identity, and culture (80). Compared with young ones, middle-aged migrant workers spend a longer time in the city and have richer work and life experience, which brings them more social capital, and thus a higher degree of social integration (42). In addition, due to aging and the decline of labor capacity among elderly migrant workers, except for a very small number of skilled and managerial talents who have become the backbone of an enterprise and thus stayed in the city, most of them have chosen to return to their hometowns to spend the rest of their lives. The lack of belonging to agricultural production and life makes young and middle-aged migrant workers eager to blend themselves with the cities and enjoy modern city life. Therefore, compared with the mental health of elderly ones, that of middle-aged and young migrant workers is more easily affected by the level of social capital and social integration (81).
This study has practical significance of value for bettering the mental health for migrant workers. The findings offer evidence supporting the government to improve the household registration system, build an integrated labor market, and establish supporting security systems such as healthcare, housing, children's education, and old-age care, providing institutional support for the social integration of young, middle-aged and elderly migrant workers and alleviate their feelings of being “marginalized” (82). On the other hand, companies where migrant workers are employed should establish mental health counseling and monitoring systems to give targeted psychological counseling and emotional regulation services for young, middle-aged, and elderly migrant workers. In pursuing work efficiency, the companies can organize employee assistance programs to elevate the human and social capital of migrant workers (83). In addition, each community should make full use of its resources, such as working with social organizations, increasing community activities, improving community conflict and dispute mediation mechanisms, etc. This would promote the acculturation and identity integration of migrant workers, help migrant workers and local residents form good social relations, and enhance the social trust, security, and happiness of migrant workers (84).
Objectively speaking, some gaps exist in the study that should be filled in follow-up research. First, although this study combined theory and SEM to tap the mechanisms of interaction between social capital, social integration, and mental health, because cross-sectional data was used, the establishment of causal relationships needs to be deepened with experimental and longitudinal design. Secondly, in addition to social integration as the mediating variable and demographical and family characteristics as the covariates selected herein, there may be other variables that play mediating roles in connecting social capital and mental health among internal migrant workers in combination with relevant literature, such as social status in subjective and objective terms, social support, etc. (85). Besides, the security status of migrant workers, such as the type of labor contract (permanent/casual), whether they have social insurance, employment security, etc., will also affect their health status (86). Therefore, future research can include more variables to conduct diversification analysis. Thirdly, combining the inter-group differentiation among internal migrants in China, i.e., age grouping, this study explored the inter-group differences in the mechanism of action among their social capital, social integration, and mental health. In addition to age, factors such as income and gender may also cause differences in the mechanism of association among related variables (87). The follow-up research may conduct multi-group difference analysis from other perspectives. Finally, due to the limitation of data, the measurement of the health status of the sample focused on mental health and self-assessed health with little attention to objective physical measures. Although self-rated health data effectively reflects the self-perception of individual health status, and has good reliability and validity in the Chinese social environment (88), it is still affected by cognitive biases of individuals, such as “feel too good about oneself,” answering biases, etc. Hence, in future research, both self-assessed and objective health indicators should be collected at the same time to ensure a holistic view of the research object and thereby arrive at more reliable conclusions.
Conclusion
Targeting Chinese internal migrant workers with a sample from the CLDS database, this study revealed the mechanisms of interaction between their social inclusion, social capital and mental health and verified age differences therein. The research results showed that social capital positively affected mental health in a significant manner, with social integration playing a mediating role therein; middle-aged migrant workers were more affected by the above mechanism than young migrant workers, and the effect on young migrant workers exceeded that on the elderly migrant workers. Despite certain limitations, this study raises some intriguing questions about migrant workers in China, offering important theoretical reference and practical guidance for policies to better the mental health and social benefits for migrant workers with age considerations in the context of economic transition.
Data Availability Statement
The data underlying the results presented in the study are available from the China Labor-force Dynamics Survey (CLDS). Anyone can access through application with the Center for Social Survey at Sun Yat-sen University at http://isg.sysu.edu.cn/node/425.
Author Contributions
JinZ and JiaZ designed the model and the research frame work and wrote the manuscript. HZ contributed to the data preparation. JZha helped with the revision of literature review. All authors contributed to the article and approved the submitted version.
Funding
This work was sponsored by the Social Sciences Foundation of Jiangsu Province under Grant Nos. 20SHC002 and 18GLD015, by the National Social Science Fund of China under Grant No. 20ARK003, and by the High-level Talent Program for Innovation and Entrepreneur of Jiangsu Province under Grant No. CZ0240619001.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to extend our heartfelt thanks to the research assistants involved in the data collection from the 2018 China Labor Dynamics Survey (CLDS).
References
1. International Labour Office (ILO). Global Estimates on International Migrant Workers-Results and Methodology. 3rd ed. Geneva, Switzerland: International Labour Organization (2021).
2. National Bureau of Statistics. Monitoring Survey Report on Migrant Workers in 2020. (2021). Available online at: http://www.stats.gov.cn/tjsj/zxfb/202104/t20210430_1816933.html (accessed January 12, 2022).
3. Unger J, Siu K. Chinese migrant factory workers across four decades: shifts in work conditions, urbanization, and family strategies. LaborHist. (2019) 60:765–78. doi: 10.1080/0023656X.2019.1645313
4. Yang G, Zhou CS, Jin WF. Integration of migrant workers: differentiation among three rural migrant enclaves in Shenzhen. Cities. (2020) 96:102453. doi: 10.1016/j.cities.2019.102453
5. Chan KW. China's Hukou system at 60: continuity and reform. In: Yep R, Wang J, Johnson T, editors. Handbook on Urban Development in China. Cheltenham: Edward Elgar Publishing (2019). p. 59–79. doi: 10.4337/9781786431639.00011
6. Ren SZ, Zhang J, Hennessy DA. Psychological strains and psychological distress among Chinese rural migrant workers. Asian Pac Migr J. (2018) 27:231–41. doi: 10.1177/0117196818766377
7. Schmalbach B, Schmalbach I, Kasinger C, Petrowski K, Brähler E, Zenger M, et al. Psychological and socio-economical determinants of health: the case of inner German migration. Front Public Health. (2021) 9:691680. doi: 10.3389/fpubh.2021.691680
8. Long RS, Chen H, Hu T, Chen YQ, Cao BL, Wang RX, et al. The association between entrapment and depression among migrant workers in China: a social rank theory based study. BMC Psychiatry. (2022) 22:17. doi: 10.1186/s12888-021-03665-6
9. Ma TP, Gao B. The association of social capital and self-rated health between urban residents and urbanized rural residents in southwest China. Front Public Health. (2021) 9:718793. doi: 10.3389/fpubh.2021.718793
10. Pittaway EE, Bartolomei L, Doney G. The glue that binds: an exploration of the way resettled refugee communities define and experience social capital. Commun Dev J. (2016) 51:401–18. doi: 10.1093/cdj/bsv023
11. Xia YW, Ma ZH. Social integration, perceived stress, locus of control, and psychological wellbeing among Chinese emerging adult migrants: a conditional process analysis. J Affect Disord. (2020) 267:9–16. doi: 10.1016/j.jad.2020.02.016
12. Yi YY, Liang Y. The effect of socioeconomic status and social integration on the mental health of Chinese migrants: a comparison between interprovincial and intra-provincial migrants. J Health Psychol. (2020) 25:387–99. doi: 10.1177/1359105317718058
13. Chan AT, O'Brien KJ. Phantom services: deflecting migrant workers in China. China J. (2019) 81:103–22. doi: 10.1086/699215
14. He SJ, Wang K. China's new generation migrant workers' urban experience and well-being. In: Wang DG, He SJ, editor. Mobility, Sociability and Well-being of Urban Living. Berlin: Springer (2016). p. 67–91.
15. Yao JX, Lu XF, Qiu FX. Residential segregation and employment stability among China's migrant population, and related intergenerational differences-analysis based on propensity score matching. Int J Urban Sci. (2022) 2022:1–19. doi: 10.1080/12265934.2021.2024085
16. Huang SL, Hou JW, Zhang M, Xin ZQ, Zhang HC, Sun L, et al. A cross-temporal meta-analysis of changes in Chinese migrant workers' mental health: 1995–2011. Acta Psychol Sin. (2015) 47:466-77. doi: 10.3724/SP.J.1041.2015.00466
17. Putnam RD. Bowling alone: America's declining social capital. In: Crothers L, Lockhart C, editors. Culture and Politics: A Reader. New York: Palgrave Macmillan (2000). p. 223-34.
18. Hall BJ, Pangan CAC, Chan EW, Huang RL. The effect of discrimination on depression and anxiety symptoms and the buffering role of social capital among female domestic workers in Macao, China. Psychiatry Res. (2019) 271:200–7. doi: 10.1016/j.psychres.2018.11.050
19. Sánchez-Aragón A, Belzunegui-Eraso A, Prieto-Flores Ò. Results of mentoring in the psychosocial well-being of young immigrants and refugees in Spain. Healthcare. (2021) 9:13. doi: 10.3390/healthcare9010013
20. Böge K, Karnouk C, Hahn E, Demir Z, Bajbouj M. On perceived stress and social support: depressive, anxiety and trauma-related symptoms in Arabic-speaking refugees in Jordan and Germany. Front Public Health. (2020) 8:239. doi: 10.3389/fpubh.2020.00239
21. Liu ZL. Supporting or dragging? Effects of neighbourhood social ties on social integration of rural-to-urban migrants in China. Hous Stud. (2019) 34:1404–21. doi: 10.1080/02673037.2019.1577955
22. Moore S, Carpiano RM. Introduction to the special issue on “Social capital and health: what have we learned in the last 20 years and where do we go from here?” Soc Sci Med. (2020) 257:113014. doi: 10.1016/j.socscimed.2020.113014
23. Zhu YK, Gao JL, Nie X, Dai JM, Fu H. Associations of individual social capital with subjective well-being and mental health among migrants: a survey from five cities in China. Int Health. (2019) 11:S64–71. doi: 10.1093/inthealth/ihz041
24. Le Thi M. Social capital, migration, and social integration. Global J Bus Soc Sci Rev. (2018) 6:1–8. doi: 10.35609//gjbssr.2018.6.1(1)
25. Lewis JL. Social capital: supportive of Bhutanese refugees' integration in the United States. J Int Migr Integr. (2021) 22:333–45. doi: 10.1007/s12134-019-00750-4
26. Ryan L. Migrants' social networks and weak ties: accessing resources and constructing relationships post-migration. Sociol Rev. (2011) 59:707–24. doi: 10.1111/j.1467-954X.2011.02030.x
27. Lancee B. Job search methods and immigrant earnings: a longitudinal analysis of the role of bridging social capital. Ethnicities. (2016) 16:349–67. doi: 10.1177/1468796815581426
28. Griffiths CE. Strangers in our midst: immigration, social capital and segmented conflict. Criminol Crim Justice. (2021). doi: 10.1177/1748895820986226
29. Meszmann T. Snakes or ladders? Job quality assessment among temp workers from Ukraine in Hungarian electronics. Cent East Eur Migr Rev. (2019) 8:75–93. doi: 10.17467/ceemr.2019.03
30. Evans O, Rubin M. In a class on their own: investigating the role of social integration in the association between social class and mental well-being. Pers Soc Psychol Bull. (2021). doi: 10.1177/01461672211021190
31. Grigaityte I, Osterman K, Bjorkqvist K. Social integration and psychological wellbeing in a sample of the Swedish-speaking minority of western Finland. Technium Soc Sci J. (2020) 9:364–76. doi: 10.47577/tssj.v9i1.954
32. Kamis C, Copeland M. The long arm of social integration: gender, adolescent social networks, and adult depressive symptom trajectories. J Health Soc Behav. (2020) 61:437–52. doi: 10.1177/0022146520952769
33. Shao L, Dong Y, Zhang DH. Effects of security on social trust among Chinese adults: roles of life satisfaction and ostracism. J Soc Psychol. (2021) 161:560–9. doi: 10.1080/00224545.2020.1871312
34. Chen HS, Zhu ZJ, Chang J, Gao YB. The effects of social integration and hometown identity on the life satisfaction of Chinese rural migrants: the mediating and moderating effects of a sense of belonging in the host city. Health Qual Life Outcomes. (2020) 18:171. doi: 10.1186/s12955-020-01415-y
35. Jin L. Migration, relative deprivation, and psychological well-being in China. Am Behav Sci. (2016) 60:750–70. doi: 10.1177/0002764216632826
36. Holt-Lunstad J. Social integration, social networks, and health. In: Wright JD, editor. International Encyclopedia of the Social and Behavioral Sciences. 2nd ed. Oxford: Elsevier (2015). p. 365–70. doi: 10.1016/B978-0-08-097086-8.14040-1
37. Rapp C, Huijts T, Eikemo TA, Stathopoulou T. Social integration and self-reported health: differences between immigrants and natives in Greece. Eur J Public Health. (2018) 28:48–53. doi: 10.1093/eurpub/cky206
38. Steel KC, Fernandez-Esquer ME, Atkinson JS, Taylor WC. Exploring relationships among social integration, social isolation, self-rated health, and demographics among Latino day laborers. Ethn Health. (2018) 23:425–41. doi: 10.1080/13557858.2017.1280130
39. Ehsan A, Klaas HS, Bastianen A, Spini D. Social capital and health: a systematic review of systematic reviews. SSM Popul Health. (2019) 8:100425. doi: 10.1016/j.ssmph.2019.100425
40. Adjaye-Gbewonyo K, Kawachi I, Subramanian SV, Avendano M. High social trust associated with increased depressive symptoms in a longitudinal South African sample. Soc Sci Med. (2018) 197:127–35. doi: 10.1016/j.socscimed.2017.12.003
41. Renzaho AMN, Dhingra N, Georgeou N. Youth as contested sites of culture: the intergenerational acculturation gap amongst new migrant communities–parental and young adult perspectives. PLoS ONE. (2017) 12:e0170700. doi: 10.1371/journal.pone.0170700
42. Morawa E, Brand T, Dragano N, Jöckel KH, Moebus S, Erim Y. Associations between acculturation, depressive symptoms, and life satisfaction among migrants of Turkish origin in Germany: gender-and generation-related aspects. Front Psychiatry. (2020) 11:715. doi: 10.3389/fpsyt.2020.00715
43. Ahonen EQ, Fujishiro K. Life-course and population health perspectives to fill gaps in migrant health research. Mondi Migranti. (2020) 3:9–20. doi: 10.3280/MM2020-003001
44. Jones NL. Gilman, SE, Cheng TL, Drury SS, Hill CV, Geronimus AT. Life course approaches to the causes of health disparities. Am J Public Health. (2019) 109:S48–55. doi: 10.2105/AJPH.2018.304738
45. Tang SS, Hao P, Feng JX. Consumer behavior of rural migrant workers in urban China. Cities. (2020) 106:102856. doi: 10.1016/j.cities.2020.102856
46. Chang KC, Wen M, Wang GX. Social capital and work among rural-to-urban migrants in China. Asian Popul Stud. (2011) 7:275–93. doi: 10.1080/17441730.2011.608989
47. Hämmig O. Health risks associated with social isolation in general and in young, middle and old age. PLoS ONE. (2019) 14:e0219663. doi: 10.1371/journal.pone.0219663
48. Liang H. Mental health of peasant workers: an intergenerational perspective. Popul Res. (2014) 38:87–100.
49. Yu LW, Zhu Y. Life satisfaction and generational differences of migrants from the perspective of social integration theory. Zhejiang Soc Sci. (2017) 10:74–84. doi: 10.14167/j.zjss.2017.10.009
50. Meng X, Xue S. Social networks and mental health outcomes: Chinese rural-urban migrant experience. J Popul Econ. (2020) 33:155–95. doi: 10.1007/s00148-019-00748-3
51. Miao J, Wu XG, Sun XL. Neighborhood, social cohesion, and the Elderly's depression in Shanghai. Soc Sci Med. (2019) 229:134–43. doi: 10.1016/j.socscimed.2018.08.022
52. Ma Z, Xia Y. Acculturation strategies, age at migration, and self-rated health: an empirical study on internal migrants in China. Soc Sci Res. (2021) 93:102487. doi: 10.1016/j.ssresearch.2020.102487
53. Wu XG, Zheng BD. Household registration, urban status attainment, and social stratification in China. Res Soc Stratif Mobil. (2018) 53:40–9. doi: 10.1016/j.rssm.2017.11.002
54. Fancourt D, Steptoe A. Cultural engagement and mental health: does socio-economic status explain the association? Soc Sci Med. (2019) 236:112425. doi: 10.1016/j.socscimed.2019.112425
55. Cai H, Xu JF. Urban community and resident health: a multi-layered analysis based on the 2018 CLDS data. Shandong Soc Sci. (2022) 176–85. doi: 10.14112/j.cnki.37-1053/c.2022.02.009
56. Gelderblom D. The limits to bridging social capital: power, social context and the theory of Robert Putnam. Sociol Rev. (2018) 66:1309–24. doi: 10.1177/0038026118765360
57. Bianchi M, Vieta M. Co-operatives, territories and social capital: reconsidering a theoretical framework. Int J Soc Econ. (2020) 47:1599–617. doi: 10.1108/IJSE-03-2020-0135
58. Entzinger H. The parallel decline of multiculturalism and the welfare state in the Netherlands. In: Banting K, Kymlicka, W, editors. Multiculturalism and the Welfare State: Recognition and Redistribution in Contemporary Democracies. Oxford: Oxford University Press (2006). p. 177–201.
59. Daiute C, Sullu B, Kovács-Cerović T. What is social integration? Insights from interventions with youth across migration systems policy insights. Behav Brain Sci. (2021) 8:143–51. doi: 10.1177/23727322211033001
60. Wu YF, Lei XK, Nie JL. From structure to cognition: social capital and social integration of floating population—based on the CLDS survey data in 2014. Popul Dev. (2019) 25:111–22.
61. Zhou H. Measurement and theoretical perspectives of immigrant assimilation in China. Popul Res. (2012) 36:27–37.
62. Li TC, Chu CC, Meng FC, Li Q, Mo D, Li B, et al. Will happiness improve the psychological integration of migrant workers? Int J Environ Res Public Health. (2018) 15:900. doi: 10.3390/ijerph15050900
63. Siedlecki KL, Salthouse TA, Oishi S, Jeswani S. The relationship between social support and subjective well-being across age. Soc Indic Res. (2014) 117:561–76. doi: 10.1007/s11205-013-0361-4
64. Preacher KJ, Zyphur MJ, Zhang Z. A general multilevel SEM framework for assessing multilevel mediation. Psychol Methods. (2010) 15:209–33. doi: 10.1037/a0020141
65. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40:879–91. doi: 10.3758/BRM.40.3.879
66. Fang J, Zhang MQ, Qiu HZ. Mediation analysis and effect size measurement: retrospect and prospect. Psychol Dev Educ. (2012) 28:105–11. doi: 10.16187/j.cnki.issn1001-4918.2012.01.015
67. Bonett DG, Wright TA. Cronbach's alpha reliability: interval estimation, hypothesis testing, and sample size planning. J Organ Behav. (2015) 36:3–15. doi: 10.1002/job.1960
68. Cohen S, Underwood LG, Gottlieb BH. Social Support Measurement and Intervention: A Guide for Health and Social Scientists. Oxford: Oxford University Press (2000).
69. Ferlander S. The importance of different forms of social capital for health. Acta Sociol. (2007) 50:115–28. doi: 10.1177/0001699307077654
70. Herian MN, Tay L, Hamm JA, Diener E. Social capital, ideology, and health in the United States. Soc Sci Med. (2014) 105:30–7. doi: 10.1016/j.socscimed.2014.01.003
71. Lyon F. Trust, networks and norms: the creation of social capital in agricultural economies in Ghana. World Dev. (2000) 28:663–81. doi: 10.1016/S0305-750X(99)00146-1
72. Luo SY. Social network, identity and psychological crisis of the new generation migrant workers. J South China Agric Univ. (2018) 17:95–105. doi: 10.7671/j.issn.1672-0202.2018.04.009
73. Li PL, Tian F. A cross generational comparison of the social cohesion of migrant workers in China. Chin J Sociol. (2012) 32:1–24. doi: 10.15992/j.cnki.31-1123/c.2012.05.002
74. Mucci N, Traversini V, Giorgi G, Tommasi E, De Sio S, Arcangeli G. Migrant workers and psychological health: a systematic review. Sustainability. (2020) 12:120. doi: 10.3390/su12010120
75. Huang X, Liu Y, Xue D, Li Z, Shi Z. The effects of social ties on rural-urban migrants' intention to settle in cities in China. Cities. (2018) 83:203–12. doi: 10.1016/j.cities.2018.06.023
76. Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: Durkheim in the new millennium. Soc Sci Med. (2000) 51:843–57. doi: 10.1016/S0277-9536(00)00065-4
77. Na L, Hample D. Psychological pathways from social integration to health: an examination of different demographic groups in Canada. Soc Sci Med. (2016) 151:196–205. doi: 10.1016/j.socscimed.2016.01.007
78. Tian F. Reverse growth: ten years of changes in the social and economic status of migrant workers (2006–2015). Sociol Study. (2017) 3:121-43+244-5. doi: 10.19934/j.cnki.shxyj.2017.03.006
79. Wang L, Chen H, Ye B, Gao JL Dai JM, Wang F, et al. Mental health and self-rated health status of internal migrant workers and the correlated factors analysis in Shanghai, China: a cross-sectional epidemiological study. Int Health. (2019) 11:S45–54. doi: 10.1093/inthealth/ihz053
80. Zhuang M. Employment Stratification and Social Cohesion of Rural Migrant Youth. Beijing: Social Sciences Academic Press (2021).
81. Lee WO, Qi J. From lost identity to identity grafting: the second generation migrant workers in Beijing. J Educ Change. (2021) 22:191–220. doi: 10.1007/s10833-020-09387-y
82. Su ZH, Ye YY, Wang P. Social change and generalized anomie: why economic development has reduced social trust in China. Int Sociol. (2019) 34:58–82. doi: 10.1177/0268580918812281
83. Busro M. Strategy increasing entrepreneurship interest to post migrant workers through training and giving of capital. Int Res J Bus Stud. (2018) 10:147–58. doi: 10.21632/irjbs.10.3.147-158
84. García-Cid A, Gómez-Jacinto L, Hombrados-Mendieta I, Millán-Franco M, Moscato G. Discrimination and psychosocial well-being of migrants in Spain: the moderating role of sense of community. Front Psychol. (2020) 11:2235. doi: 10.3389/fpsyg.2020.02235
85. Yu B, Chen XG. Relationship among social capital, employment uncertainty, anxiety, and suicidal behaviors: a chained multi-mediator mediation modeling analysis. Arch Suicide Res. (2022) 26:261–79. doi: 10.1080/13811118.2020.1793044
86. Shi ZL, Liu SC, Zhao Y. The paradox of unstable employment and the citizenship of migrant workers: based on the perspective of labor process. Chin J Sociol. (2022) 42:88–123. doi: 10.15992/j.cnki.31-1123/c.2022.01.004
Keywords: social capital, social integration, depression, age, migrant workers, China
Citation: Zhou J, Zhou J, Zhang H and Zhang J (2022) Social Integration as Mediator and Age as Moderator in Social Capital Affecting Mental Health of Internal Migrant Workers: A Multi-Group Structural Equation Modeling Approach. Front. Public Health 10:865061. doi: 10.3389/fpubh.2022.865061
Received: 29 January 2022; Accepted: 04 April 2022;
Published: 12 May 2022.
Edited by:
Wei Guo, Nanjing University, ChinaReviewed by:
Senhu Wang, National University of Singapore, SingaporeSumit Mazumdar, University of York, United Kingdom
Copyright © 2022 Zhou, Zhou, Zhang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianfang Zhou, emhvdWppYW5mYW5nQG5qdXB0LmVkdS5jbg==