 Shudi Li
Shudi Li Jiangkai Liu2
Jiangkai Liu2 Fei Duan
Fei Duan Xinju Chen
Xinju Chen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 25 July 2022
Sec. Public Health and Nutrition
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.862266
This article is part of the Research Topic Rising Stars: Public Health and Nutrition 2021 View all 6 articles
Background: Nonalcoholic fatty liver disease (NAFLD) is a chronic liver disease with a high prevalence worldwide, seriously harming human health, and its pathogenesis remains unclear. In recent years, increasing evidence has indicated that intestinal microbiota plays an important role in the occurrence and development of NAFLD. The regulation method of probiotics/prebiotics/synbiotics can alter the intestinal microbiota and has been suggested as an option in the treatment of NAFLD.
Methods: Five databases of PubMed, Embase, the Cochrane Library, clinicaltrails.gov, and China National Knowledge Infrastructure were searched initially, and then the eligible studies were screened. Finally, the data of included studieswere extracted, combined and analyzed
Results: A total of 29 randomized controlled trials involving 2,110 patients were included in this study. The results showed that using probiotics/prebiotics/synbiotics in the intervention group could reduce the levels of glucose (SMD = −0.23, 95% CI [−0.45, −0.01], P = 0.04), HOMA-IR (SMD = −0.47, 95% CI [−0.63, −0.31], P < 0.00001) and insulin (SMD = −0.46, 95% CI [−0.76, −0.16], P = 0.002) in sugar metabolism; in terms of lipid metabolism, the levels of TC (SMD = −0.62, 95%CI [−0.87, −0.36], P < 0.00001), and LDL-C (SMD = −0.57, 95%CI [−0.85, −0.28], P < 0.00001) were decreased; and the level of ALB was decreased in protein metabolism (SMD = −0.34, 95%CI [−0.61, −0.06], P = 0.02).
Conclusions: Based on the current evidence, probiotics/prebiotics/synbiotics may improve energy metabolism biomarkers in the NAFLD population, but these effects still need to be confirmed by further research.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/#aboutpage.
Nonalcoholic fatty liver disease (NAFLD) is a chronic liver disease characterized by excessive accumulation of fat in liver cells (1). It includes a wide range of pathological liver diseases, from simple accumulation of liver fat to nonalcoholic steatohepatitis (NASH) with or without fibrosis, which can eventually progress to cirrhosis and liver cancer (2). The global prevalence of NAFLD has reached 25.2%, posing a serious threat to human health (3). The pathogenesis of NAFLD is still unclear, and the widely accepted concept of “multiple strikes” highlights the important role of various genetic and environmental factors in the multifactorial pathogenesis of NAFLD (4). Currently, no effective drugs for NAFLD have been approved (5).
The intestinal microbiota is a collective term for a large number of microorganisms existing in the human intestinal tract, whose metabolic activities can affect nutrient absorption and energy homeostasis (6). Recent studies have shown that intestinal microbiota plays a vital role in the development and progression of NAFLD, including regulating energy homeostasis by increasing carbohydrate fermentation to short-chain fatty acids, and activating the resynthesis of triglycerides and bacterial-derived toxins in the liver (7–10). The interaction between the liver and intestine (gut-liver axis) is not only involved in the pathogenesis of NAFLD, but also may be an important factor leading to the progression of NAFLD to NASH and related liver fibrosis (11, 12).
Probiotics, prebiotics, and synbiotics (PPS) have been proved to be therapeutic methods that can change the composition of the microbiota and restore microbial balance (13). Probiotics are living non-pathogenic microorganisms, prebiotics are defined as indigestible fiber compounds, and synbiotics are combinations of probiotics and prebiotics. They can cause specific changes in the composition and activity of the gastrointestinal microbiota when ingested, and increase the secretion of endogenous intestinal nutrient peptides (14). Studies have shown that PPS can regulate the composition of intestinal flora and the production of antibacterial factors, change the permeability and function of intestinal epithelial cells and reduce the permeability of intestinal endotoxin to affect the occurrence and development of NAFLD. They can also exert effects on NAFLD by modifying endotoxemia, inhibiting inflammatory response, and regulating the immune system (15–17).The PPS regulation method has been suggested as a treatment for NAFLD (18), and a number of randomized controlled trials have been conducted in clinical practice to confirm that PPS regulation can improve NAFLD. However, most studies have focused on the improvement of liver function and inflammatory indicators in NAFLD by the PPS regulation method, while there is a lack of systematic conclusions on the improvement effect of NAFLD on energy metabolism biomarkers. Based on this, this study adopts the method of meta-analysis to systematically evaluate PPS regulation on the energy metabolism biomarkers in NAFLD patients, in order to provide a reference and basis for the clinical practice of NAFLD.
The present study was conducted in accordance with the Preferred Reporting Items for Systemic Reviews and Meta-Analysis (PRISMA) statement to ensure transparent reporting of the scientific evidence (19), and was registered with PROSPERO in advance (CRD:42021288543, www.crd.york.ac.uk/PROSPERO/).
The included clinical studies met the following criteria: clinical trials were randomized controlled trials; participants were patients with NAFLD, regardless of age, gender, or race; the interventions were probiotics and/or prebiotics and/or synbiotics; except for the intervention method, the treatment of the control group was the same as that of the intervention group; the outcome measures included glucose (Glu), insulin, homeostatic model assessment of IR (HOMA-IR), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), albumin.
Exclusion criteria: patients with alcoholic steatohepatitis, alcoholic fatty liver, cirrhosis or liver cancer; patients receiving additional medication or genetic predisposition (single nucleotide polymorphisms); liver transplant patients; conference papers or abstracts; non-original research or case reports; and non-peer-reviewed articles.
We searched databases including PubMed, Embase, the Cochrane Library, clinicaltrails.gov, China National Knowledge Infrastructure.
Related terms of “probiotics”, “prebiotics”, “synbiotics” and “nonalcoholic fatty liver disease” were used to search the above database. The search and selection period was from January 1, 2000 to September 31, 2021. The search strategies and results are detailed in the Appendix (see in Supplementary Table S1).
The search and selection of studies were performed by three professionally trained researchers who were informed of inclusion and exclusion criteria prior to searching and selection. Studies were firstly screened by title and abstract, followed by further assessment of the full text based on inclusion and exclusion criteria. Finally, the screened full texts were compared. The three researchers negotiated and voted to resolve disagreements and discrepancies.
The statistical analysis was carried out using statistical software RevMan Version 5.3 (The Cochrane Collaboration, Copenhagen, Denmark) and the standard mean difference (SMD) synthesis was used uniformly since the outcome indicators included in this study were all continuous values. If the data were available and sufficient, we would also conduct subgroup analyses, based primarily on the type of diease (NAFLD/NASH), type of intervention (probiotic, prebiotic, synbiotic), type of control (placebo/non placebo), administratingduration ( ≤ 12 weeks; >12 weeks, <24 weeks; ≥24 weeks). I2 test was used to assess the magnitude of heterogeneity. The fixed-effects model was used only when the I2 value was <50%; otherwise, the random-effects model was used. The sensitivity analysis and subgroup analysis would be performed to define the source of heterogeneity. Any referenced statistic adopted a two-sided test, and the significance level was set as 0.05.
Two authors independently evaluated the titles and abstracts of available articles to exclude irrelevant studies. Full texts of selected articles were assessed individually for eligibility on the basis of the above inclusion criteria. The Cochrane Collaboration's Risk of Bias tool was used to assess bias in the eligible RCTs. Sensitivity analysis was conducted by deleting the included studies in sequence to identify the stability of the total effect. If there were more than 10 articles for a certain outcome index, a funnel plotwas used to analyze whether publication bias existed. And Egger's test was conducted to qualify the publication bias, trim-and-fill method was applied to test how much influence the publicationbias would make on the pooling estimates.
According to the formulated strategy, 1,415 articles were preliminarily retrieved up to November 2, 2021, and 29 RCTs were finally included, as shown in Figure 1.
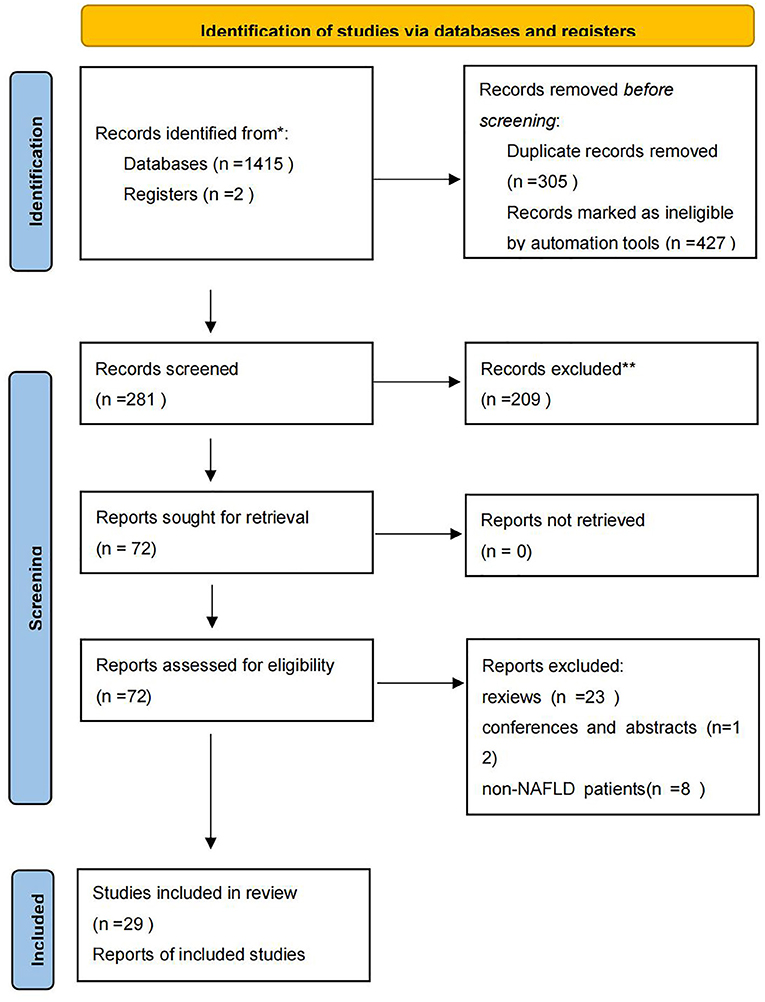
Figure 1. PRISMA flow diagram.
Among the 29 included studies (20–48), 20 of them evaluated probiotics, 3 evaluated prebiotics, and 9 evaluated synbiotics, with a total of 2,110 patients enrolled. The characteristics of the included studies are shown in Table 1. Subgroup analysis was performed according to the preset grouping basis and no difference was found except for the subgroups of LDL-C disease. The risk of bias assessment was carried out employing the tool provided by the Cochrane Collaboration, and the results showed that the overall risk of the included studies was medium and low, as shown in Figure 2.
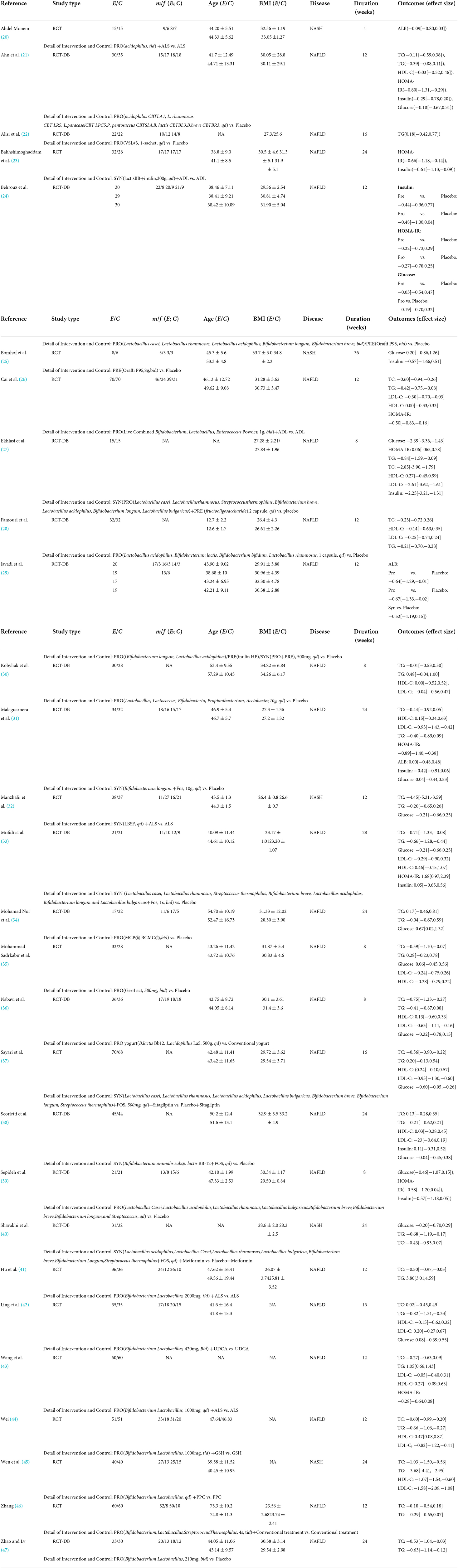
Table 1. Characteristics of the included studies.
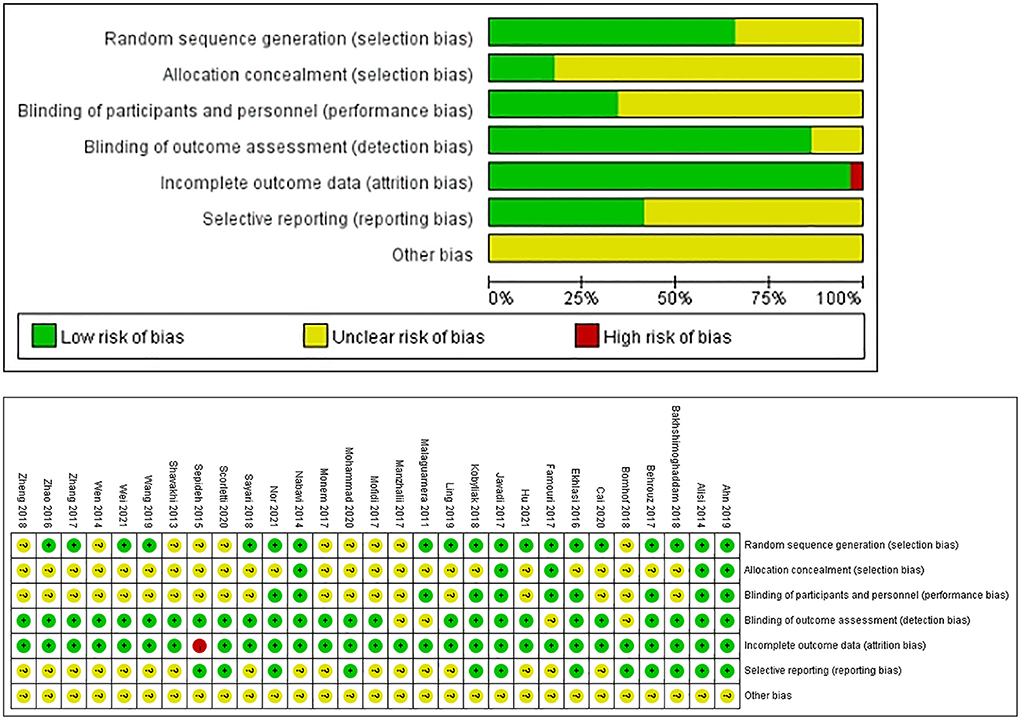
Figure 2. Risk-of-bias graph.
A meta-analysis was carried out on the three glucose metabolism indicators of Glucose, HOMA-IR, and Insulin. And we also conduct subgroup analyses, based primarily on the types of diease (NAFLD/NASH), types of intervention (probiotic, prebiotic, synbiotic), type of control (placebo/non placebo), administrating duration ( ≤ 12 weeks; >12 weeks, <24 weeks; ≥24 weeks), but no significant difference was found between subgroups (see in Supplementary Figures S1–S11).
Glucose was reported in 15 studies involving 985 patients. The combined estimated value was SMD = −0.23 (95% CI [−0.45, −0.01], P = 0.04, I2 = 65%, random-effects model), and the difference was statistically significant, suggesting that the PPS regulation method could reduce glucose in NAFLD patients, as shown in Figure 3.
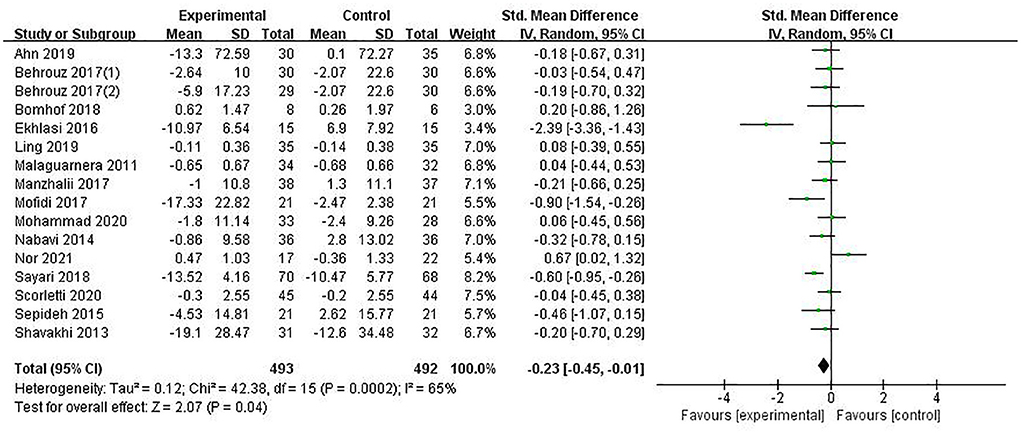
Figure 3. The role of PPS in Glucose in patients with NAFLD.
HOMA-IR was reported in 9 studies involving 684 patients. The combined estimate was SMD = −0.29, (95% CI [−0.63, −0.06], P = 0.11, I2 = 79%, random-effects model). Sensitivity analysis showed that the study of Mofidi (32) affected the robustness of the pooled estimates, and after excluding this study, the results showed SMD = −0.47 (95% CI [−0.63, −0.31], P < 0.00001, I2 = 17 %, fixed-effects model), with a statistically significant difference. The heterogeneity of this study was analyzed, and it was considered that due to the normal range of BMI (23.17 ± 1.01/23.20 ± 1.07), the included population of the study were NAFLD patients with normal BMI and not accompanied by overweight, while the other studies concerning this indicator all included overweight NAFLD patients with BMI above the normal range. It was indicated that PPS regulation could reduce HOMA-IR in NAFLD patients, as shown in Figure 4.
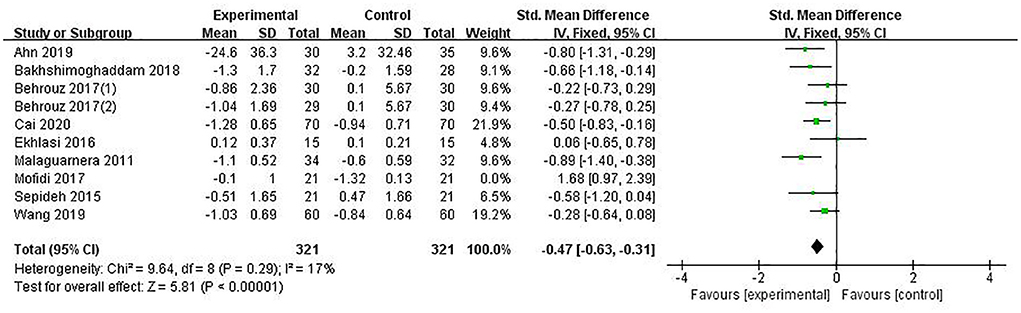
Figure 4. The role of PPS in HOMA-IR in patients with NAFLD.
Insulin was reported in 9 studies involving 527 patients, with a combined estimate of SMD = −0.46 (95%CI [−0.76, −0.16], P = 0.002, I2 = 62%, random-effects model), and the differences were statistically significant, suggesting that PPS regulation could reduce insulin in NAFLD patients (Figure 5).
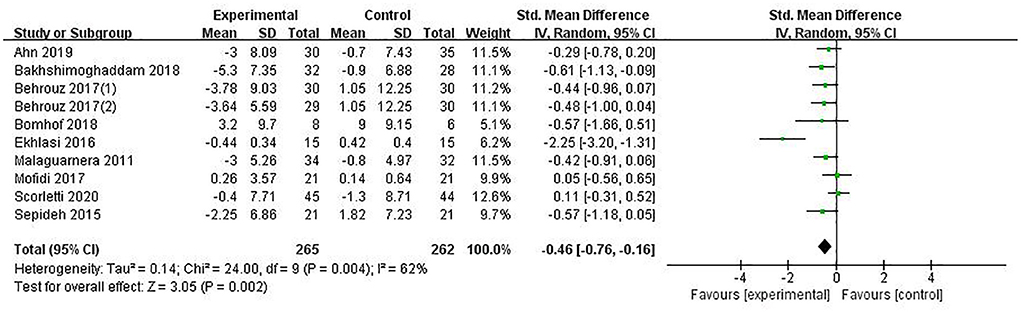
Figure 5. The role of PPS in Insulin in patients with NAFLD.
A meta-analysis was carried out on the four lipid metabolism indicators of TC,TG,HDL-C,LDL-C. And we also conduct subgroup analyses, based primarily on the types of disease (NAFLD/NASH), types of intervention (probiotic, prebiotic, synbiotic), type of control (placebo/non placebo), administrating duration ( ≤ 12 weeks; >12 weeks, <24 weeks; ≥24 weeks). Only in the LDL-C, a statistically significant difference was found between subgroups according to disease types, and no significant difference was found in others (see in Supplementary Figures S12–S27).
TC was reported in 22 studies involving 1,726 patients, with a combined estimated value of SMD = −0.62 (95% CI [−0.87, −0.36], P < 0.00001, I2 = 85%, random-effect model), indicating that PPS regulation could reduce TC in NAFLD patients, as shown in Figure 6.
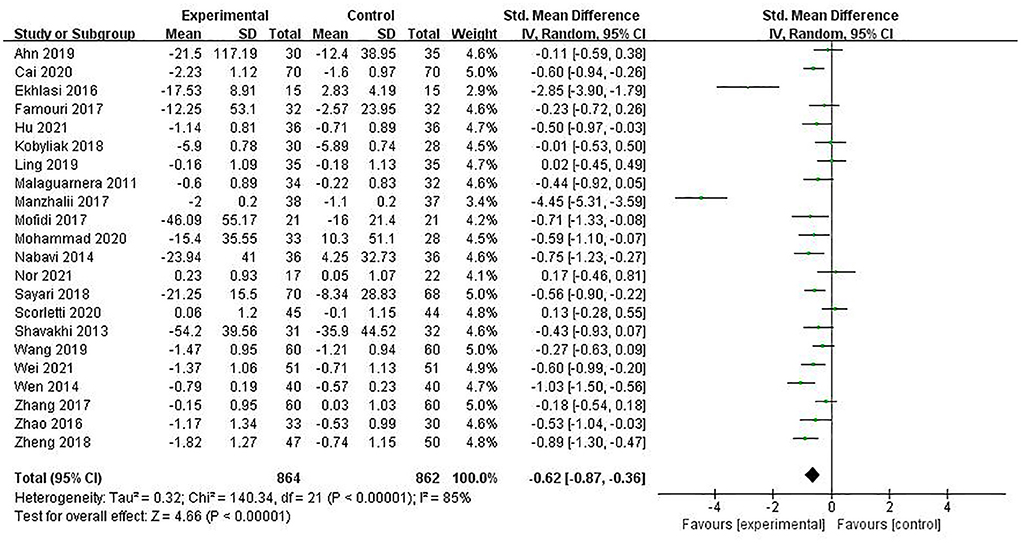
Figure 6. The role of PPS in TC in patients with NAFLD.
A total of 23 studies involving 1,770 patients reported the indicator of TG, and the pooled estimate was SMD = −0.24 (95% CI [−0.59, −0.12], P = 0.19, I2 = 92%, random-effects model). The difference was not statistically significant, as shown in Figure 7.
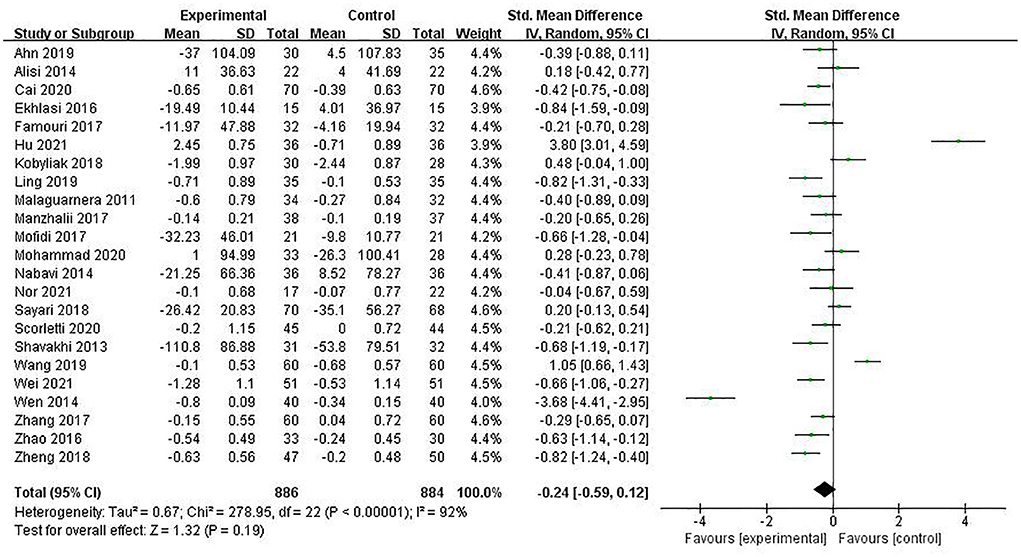
Figure 7. The role of PPS in TG in patients with NAFLD.
HDL-C was reported in 15 studies involving 1,197 patients, and the pooled estimate was SMD = 0.01, (95% CI [−0.18, 0.19], P = 0.95, I2 = 59%, random-effects model), with no statistically significant difference (see Figure 8).
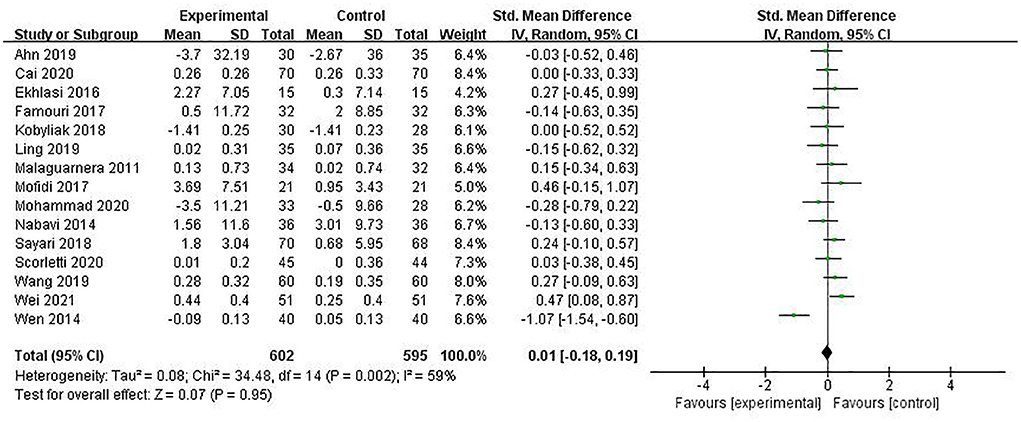
Figure 8. The role of PPS in LDL-C in patients with NAFLD.
LDL-C was reported in 14 studies involving 1,132 patients, and the combined estimate was SMD = −0.57 (95% CI [−0.85, −0.28], P < 0.00001, I2 = 81%), with a statistically significant difference. Subgroup analysis of the included studies revealed a statistically significant difference between the two groups according to disease type (P = 0.0001), but the reliability of inter-group differences was insufficient as only one study was included in the NASH group. Overall meta-analysis results suggested that PPS regulation could reduce LDL-C in NAFLD patients, as shown in Figure 9.
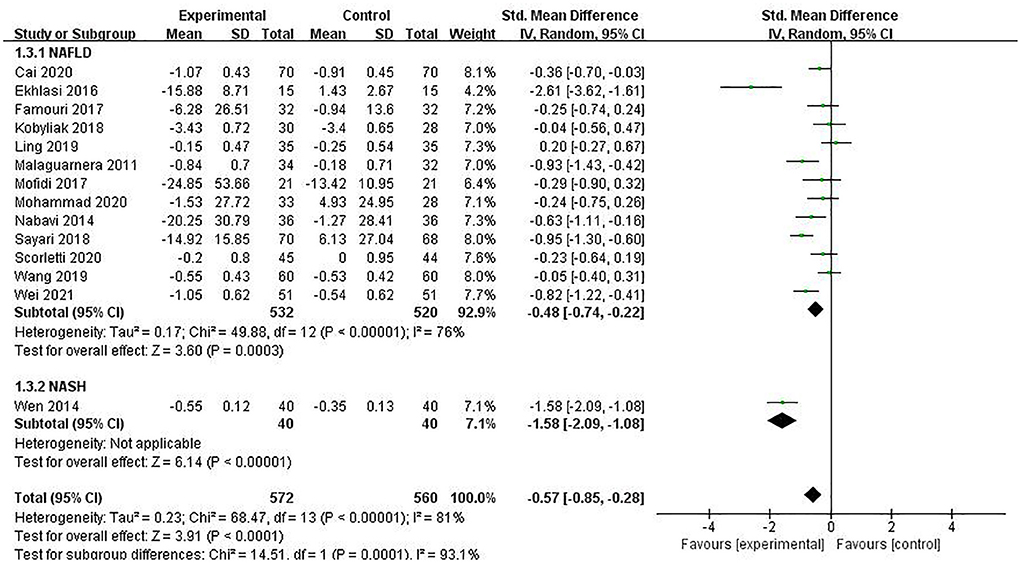
Figure 9. The role of PPS in HDL-C in patients with NAFLD.
A meta-analysis was carried out on the protein metabolism indicator of ALB. And we also conducted subgroup analyses, based primarily on the types of intervention (probiotic, prebiotic, synbiotic), type of control (placebo/non placebo), but no significant difference was found between subgroups (see in Supplementary Figures S28, S29).
The indicator of ALB was reported in five studies involving 209 patients. The combined estimated value was SMD = −0.34 (95%CI [−0.61, −0.06], P = 0.02, I2 = 11%, fixed-effects model), and the difference was statistically significant, suggesting that PPS regulation could reduce ALB in NAFLD patients (see Figure 10).
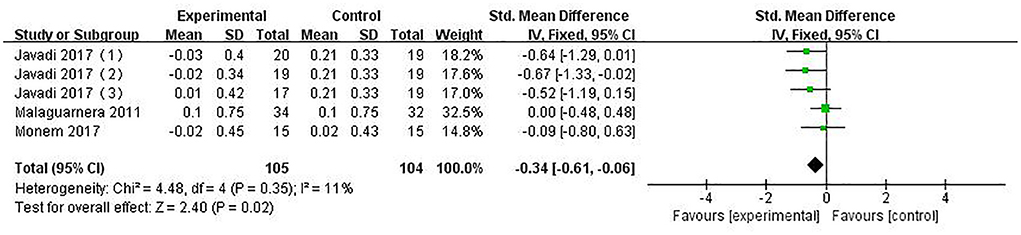
Figure 10. The role of PPS in ALB in patients with NAFLD.
Meta-analysis and sensitivity analysis was conducted on all preset indicators, and sensitivity analysis showed no changes in robustness except for the indicator of HOMA-IR. The funnel plots of glucose, HOMA-IR, TC, TG, LDL-C, and HDL-C were analyzed respectively, publication bias was qualified by Egger's test and found in HOMA-IR, TG, LDL-C and HDL-C, no significant differences were found after utilizing trim-and-fill method (see in Supplementary Figures S30–S35).
The current study systematically evaluated the effects of PPS regulation on energy metabolism biomarkers in NAFLD patients. The results showed that PPS regulation significantly improved the sugar and lipid metabolism indicators of NAFLD, and may have a negative impact on protein metabolism. Subgroup analysis, based on the types of disease (NAFLD/NASH), types of intervention(probiotic, prebiotic, synbiotic), type of control(placebo/non placebo), administrating duration( ≤ 12 weeks; >12 weeks, <24 weeks; ≥24 weeks), shows no statistically difference. No significant publication bias was identified.
According to the results of this study, the PPS regulation method may reduce the levels of glucose, HOMA-IR and insulin in NAFLD patients, and thus play a certain role in regulating the sugar metabolism level of patients. In 70–80% of NAFLD patients, there is a problem of elevated blood glucose (3), and studies by Mirmiranpour et al. have shown that PPS regulation can reduce blood glucose levels (49). PPS may improve the blood glucose problem in NAFLD by changing intestinal microflora and stimulating the production of glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptides (GLPs), thereby increasing glucose uptake and lowering blood glucose levels (50). This study showed that PPS regulation reduced the glucose level in NAFLD (SMD = −0.23, 95%CI [−0.45, −0.01], P = 0.04), which is consistent with the above research. Insulin resistance is one of the characteristics of NAFLD (51), and HOMA-IR is the most widely used model method to evaluate insulin resistance in microbial therapy. The study by Nazarii et al. showed that PPS regulation can reduce the HOMA-IR level and improve insulin resistance (52). Previous studies have suggested that PPS may increase insulin sensitivity and improve NAFLD insulin resistance by regulating the NF-κB signaling pathway, reducing the expression of TNF-α and inflammatory response (53). Insulin resistance is associated with increased LPS levels, and impaired intestinal barrier leads to increased LPS levels in the circulation (54). PPS regulation may improve insulin resistance by regulating the production of tight junction protein mucin, improving the non-specific intestinal barrier defense mechanism, and reducing LPS levels (17, 55). The results of this study showed that PPS regulation could reduce the level of HOMA-IR (SMD = −0.47, 95%CI [−0.63, −0.31], P < 0.00001), suggesting that PPS regulation might improve insulin resistance in NAFLD. Elevated serum fasting insulin level is regarded as one of the main pathogenic factors of NAFLD (56), and PPS regulation is considered to reduce insulin levels (57). The exact mechanism by which the PPS regulation method affects insulin levels is unclear, and since PPS use glucose as the primary energy source, their effects on serum insulin levels may be mediated by affecting blood glucose levels (58). The results of this study showed that PPS regulation could reduce insulin levels (SMD = −0.46, 95% CI [−0.76, −0.16], P = 0.002), further providing evidence-based proof for this view.
This study showed that PPS regulation could reduce the levels of TC and LDL-C in NAFLD patients, while there was no significant difference in the indicators of TG and HDL-C. Elevated TC is an important risk factor for the pathogenesis of NAFLD (59), and low HDL-C and high LDL-C are characteristics of NAFLD (60, 61). Studies have shown that PPS regulation can reduce TC and LDL-C levels and increase HDL-C levels (62), and PPS may regulate cholesterol metabolism in NAFLD patients. The results of this study showed that PPS regulation could reduce the levels of TC (SMD = −0.62, 95%CI [−0.87, −0.36], P < 0.00001) and LDL-C (SMD = −0.57, 95%CI [−0.85, −0.28], P < 0.00001). Although there was no statistical difference in HDL-C, the overall effect size suggested that PPS regulation could increase the HDL-C level [SMD = 0.01, (95%CI [−0.18, 0.19], P = 0.95], providing support for the view that microbial therapy can regulate cholesterol metabolism. Elevated TG is also a risk factor for NAFLD (59), and studies have shown that PPS regulation can reduce the TG level (62). PPS may change the gene expression of lipogenic enzymes and reduce the de novo synthesis of fatty acids in the liver, thereby reducing the accumulation of triglycerides in the liver (63); TG levels are reduced by inhibiting the transcription of carbohydrate response element binding protein (ChREBP) and activating the transcription of peroxisome proliferator-activated receptor alpha (PPARα) encoding genes (64). Although the analysis results of this study showed no statistically significant difference in the effect of PPS regulation on the indicator of TG, the overall effect size suggested that the TG level decreased (SMD = −0.24, 95%CI [−0.59, −0.12], P = 0.19), indicating that PPS regulation may reduce the TG level in NAFLD.
This study also found that PPS regulation may reduce ALB levels (SMD = −0.34, 95% CI [−0.61, −0.06], P = 0.02). Intestinal microbiota can produce amino acids by fermenting dietary proteins, utilize amino acids for protein synthesis, and catabolize amino acids through deamination and decarboxylation (65–67). As an important protein in the human body, ALB plays an important role in maintaining body nutrition and osmotic pressure, and is the most important indicator reflecting liver synthesis function (68). A study showed that ALB level was negatively correlated with liver fibrosis indicators of LN and PC III in NAFLD patients (69). There are few previous studies on the effect of PPS regulation on protein metabolism. Considering the important role of intestinal microbiota in the process of protein synthesis and metabolism and the vital regulatory effect of microbial therapy on intestinal microbiota, PPS regulation may affect protein metabolism of NAFLD by regulating intestinal microbiota. However, this study only included five groups of comparisons on the indicator of ALB, three of which were from the same study. Due to limited data sources, the results should be interpreted with caution.
NASH is a progressive form of NAFLD. This study showed that PPS regulation could reduce the levels of Glucose, Insulin, TC, TG, HDL-C and LDL-C in NASH patients. Studies have shown that PPS regulation could prevent obesity and improve liver histology in NASH, which might be outcomes of regulating aforementioned indicators (16, 70). Moreover, in animal models, PPS could accelerate the lowering of plasma glucose levels during an insulin tolerance test in diet-induced obesity mice, and plays a certain role in regulating the sugar metabolism (71). Bile acid (BA) is essential for lipid and carbohydrate metabolism (72). PPS has been found possessing a certain effect on regulating BA synthesis to control lipid and sugar metabolism, and furthermore resisting the development of NASH (73). Despite aforementioned evidences, we have not found more evidences to explore the differences in the effects of PPS on NAFLD and NASH in terms of sugar, lipids, and proteins metabolism, future research might be needed.
On the basis of what we found, administration of PPS might be applied in more clinical scenario. Supplementation of PPS to regulate the gut microbiota should be explorably applied in the conventional treatment of NAFLD for PPS might has the potential to prevent the progression of NAFLD to NASH. PPS could reduce glucose, insulin and insulin resistance levels in NAFLD patients by restoring the homeostasis of gut microbiota, improved glucose metabolism disorders, and has application advantages in diseases including NAFLD and type 2 diabetes (T2D) which generally comorbid with abnormal glucose metabolism (26, 38). PPS could improve lipid metabolism disorder and reduced blood lipid and cholesterol levels in NAFLD patients. The potential mechanisms related to the hypocholesterolemic effect was that PPS could prevent free bile acids reabsorption and compensatory increased use of cholesterol to produce bile acids, which could lead to a reduction in the cholesterol present in serum (74). Evidence supports that PPS can improve cardiovascular disease risk factors, and it is suggested that it could be considered in the treatment of atherosclerosis and hypertension (75–77). This study showed that microbial therapy may reduce the ALB level of NAFLD patients, suggesting that we should pay attention to the impact of microbial therapy on protein metabolism and timely supplement protein when treating NAFLD.
The present study also has some limitations. (1) The sample size of the included studies was small with few relevant studies on certain indicators, and there were differences in the types, doses, intervention time of probiotics and lifestyle management in the included RCTs. In addition, a few of the trial designs were not standardized enough, which affected the effectiveness of the evaluation. (2) The included study involved adverse reactions of microbial therapy, and its side effects on NAFLD need to be further studied. (3) Although the risk of bias result for this study was medium and low, we couldn't be sure what impact of the risk would be. (4) Because the inconsistent bacteria strains and dose, a dose-response analysis was not applicable, more attention should be paid to this problem in further studies.
The results of this study suggest that microbial therapy has a certain effect on the energy metabolism of NAFLD, and can be used as a new treatment option for NAFLD, but meanwhile, attention should be paid to its effect on protein reduction. However, the results of our study should be interpretated cautiously for the limitations in our study.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Conceptualization: ShL and SuL. Methodology: ZW, FD, ZJ, and XC. Software: ShL, ZW, and JL. Validation, writing—review and editing, and supervision: ShL, SuL, JL, FD, ZJ, XC, and ZW. Writing—original draft preparation: ShL. Funding acquisition: SuL, XC, and FD. All authors have read, critically appraised, and agreed to the published version of the manuscript.
This study was funded by the National Science and Technology major projects (Project Code: 2018ZX10303502); China Postdoctoral Science Foundation Special Funding for New Coronary Pneumonia Epidemic Prevention and Control (Project Code: 2020T130032ZX); Scientific research project of Henan Provincial Administration of Traditional Chinese Medicine (No. 20-21ZY1011; No. 2022ZY1002; No. 2018ZY2033).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.862266/full#supplementary-material
1. Eslam M, Sarin SK, Wong VW, Fan JG, Kawaguchi T, Ahn SH, et al. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol Int. (2020) 14:889–919. doi: 10.1007/s12072-020-10094-2
2. Brunt EM. Pathology of nonalcoholic fatty liver disease. Nat Rev Gastro Hepat. (2010) 7:195–203. doi: 10.1038/nrgastro.2010.21
3. Younossi ZM, Golabi P, de Avila L, Paik J. M., Srishord M., Fukui N., et al. Global epidemiology of NAFLD and NASH in patients with type 2 diabetes:a systematic review and meta-analysis. J Hepatol. (2019) 71, 793–801. doi: 10.1016/j.jhep.2019.06.021
4. Cohen JC, Horton JD, Hobbs HH. Human fatty liver disease:old questions and new insights. Science. (2011) 332:1519–23. doi: 10.1126/science.1204265
5. Golabi P, Sayiner M, Fazel Y, Koenig A, Henry L, Younossi ZM, et al. Current complications and challenges in nonalcoholic steatohepatitis screening and diagnosis. Expert Rev Gastroenterol Hepatol. (2016) 10:63. doi: 10.1586/17474124.2016.1099433
6. Ley RE, Peterson DA, Gordon JI. Ecological and evolu-tionary forces shaping microbial diversity in the human intestine. Cell. (2006) 124:837–48. doi: 10.1016/j.cell.2006.02.017
7. Jumpertz R, Le DS, Turnbaugh PJ, Trinidad C, Bogardus C, Gordon JI, et al. Energy-balance studies reveal associations between gut microbes, caloric load, and nutrient absorption in humans. Am J Clin Nutr. (2011) 94:58–65. doi: 10.3945/ajcn.110.010132
8. Hoverstad T, Midtvedt T. Short-chain fatty acids in germfree mice and rats. J Nutr. (1986) 116:1772–6. doi: 10.1093/jn/116.9.1772
9. Daly K, Proudman CJ, Duncan SH, Flint HJ, Dyer J, Shirazi-Beechey SP, et al. Alterations in microbiota and fermentation products in equine large intestine in response to dietary variation and intestinal disease. Br J Nutr. (2012) 107:989–95. doi: 10.1017/S0007114511003825
10. Cani PD, Amar J, Iglesias MA, Poggi M, Knauf C, Bastelica D, et al. Metabolic endotoxemia initiates obesity and insulin resistance. Dia-betes. (2007) 56:1761–72. doi: 10.2337/db06-1491
11. Park JS, Seo JH, Youn HS. Gut microbiota and clinical disease: obesity and nonalcoholic fatty liver disease. Pediatr Gastroenterol Hepatol Nutr. (2013) 16:22–7. doi: 10.5223/pghn.2013.16.1.22
12. Seki E, Schnabl B. Role of innate immunity and the microbiota in liver fibrossis: crosstalk between the liver and the gut. J Physiol. (2012) 590:447–58. doi: 10.1113/jphysiol.2011.219691
13. Malaguarnera M, Greco F, Barone G, Gargante MP, Malaguarnera M, Toscano MA, et al. Bifidobacterium longum with fructo-oligosac-charide (FOS) treatment in minimal hepatic encephalopathy: a randomized, double-blind, placebo-controlled study. Dig Dis Sci. (2007) 52:3259–65. doi: 10.1007/s10620-006-9687-y
14. Compare D, Coccoli P, Rocco A, Nardone O, De Maria M, Cartenì S. Gut–liver axis: the impact of gut microbiota on non alcoholic fatty liver disease. Nutr Metab Cardiovasc Dis. (2012) 22:471–6. doi: 10.1016/j.numecd.2012.02.007
15. Cani PD, Possemiers S, Van de Wiele T, Guiot Y, Everard A, Rottier O, et al. Changes in gut microbiota control inflammation in obese mice through a mechanism involving GLP-2-driven improvement of gut permeability. Gut. (2009) 58:1091–103. doi: 10.1136/gut.2008.165886
16. Nardone G, Rocco A. Probiotics: a potential target for the prevention and treatment of steatohepatitis. J Clin Gastroenterol. (2004) 38:121–2. doi: 10.1097/01.mcg.0000128934.53920.1d
17. Roberfroid M, Gibson GR, Hoyles L, McCartney AL, Rastall R, Rowland I, et al. Prebiotic effects:metabolic and health benefits. Br J Nutr. (2010) 104:1–63. doi: 10.1017/S0007114510003363
18. Iacono A, Raso GM, Canani RB, Calignano A, Meli R, et al. Probiotics as an emerging therapeutic strategy to treat NAFLD: focus on molecular and biochemical mecha-nisms. J Nutr Biochem. (2011) 22:699–711. doi: 10.1016/j.jnutbio.2010.10.002
19. Matthew JP, Joanne EM, Patrick MB, Isabelle B, Tammy CH, Cynthia DM, et al. The PRISMA. 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 29:89. doi: 10.1186/s13643-021-01626-4
20. Abdel Monem SM. Probiotic therapy in patients with nonalcoholic steatohepatitis in Zagazig University Hospitals. Euroasian J Hepatogastroenterol. (2017) 7:101–6. doi: 10.5005/jp-journals-10018-1226
21. Ahn SB, Jun DW, Kang BK, Lim JH, Lim S, Chung MJ, et al. Randomized, Double-blind, Placebo-controlled Study of a Multispecies Probiotic Mixture in Nonalcoholic Fatty Liver Disease. Sci Rep-uk. (2019) 9:5688. doi: 10.1038/s41598-019-42059-3
22. Alisi A, Bedogni G, Baviera G, Giorgio V, Porro E, Paris C, et al. Randomised clinical trial: the beneficial effects ofVSL#3 in obese children with non-alcoholic steatohepatitis. Aliment Pharm Ther. (2014) 39:1276–85. doi: 10.1111/apt.12758
23. Bakhshimoghaddam F, Shateri K, Sina M, Hashemian M, Alizadeh M. Daily consumption of synbiotic yogurt decreases liver steatosis in patients with nonalcoholic fatty liver disease: a randomized controlled clinical trial. J Nutr. (2018) 148:1276–84. doi: 10.1093/jn/nxy088
24. Behrouz V, Jazayeri S, Aryaeian N, Zahedi MJ, Hosseini F. Effects of probiotic and prebiotic supplementation on leptin, adiponectin, and glycemic parameters in non-alcoholic fatty liver disease: a randomized clinical trial. Middle East J Dig Dis. (2017) 9:151–9. doi: 10.15171/mejdd.2017.66
25. Bomhof MR, Parnell JA, Ramay HR, Crotty P, Rioux KP, Probert CS, et al. Histological improvement of non-alcoholic steatohepatitis with a prebiotic: a pilot clinical trial. Eur J Nutr. (2019) 58:1735–45. doi: 10.1007/s00394-018-1721-2
26. Cai GS, Su H, Zhang J. Protective effect of probiotics in patients with non-alcoholic fatty liver disease. Medicine. (2020) 99:21464. doi: 10.1097/MD.0000000000021464
27. Ekhlasi G, Mohammadi RK, Agah S, Zarrati M, Hosseini AF, Arabshahi SS, et al. Do symbiotic and vitamin e supplementation have favorite effects in nonalcoholic fatty liver disease? A randomized, double-blind, placebo-controlled trial. J Res Med Sci. (2016) 21:106. doi: 10.4103/1735-1995.193178
28. Famouri F, Shariat Z, Hashemipour M, Keikha M, Kelishadi R. Effects of Probiotics on Nonalcoholic Fatty Liver Disease in Obese Children and Adolescents. J Pediatr Gastr Nutr. (2017) 64:413–7. doi: 10.1097/MPG.0000000000001422
29. Javadi L, Ghavami M, Khoshbaten M, Safaiyan A, Barzegari A, Gargari BP, et al. The effect of probiotic and/or prebiotic on liver function tests in patients with nonalcoholic fatty liver disease: a double blind randomized clinical trial. Iran Red Crescent Me. (2017) 19:46017. doi: 10.5812/ircmj.46017
30. Kobyliak N, Abenavoli L, Mykhalchyshyn G, Kononenko L, Boccuto L, Kyriienko D, et al. Multi-strain Probiotic Reduces the Fatty Liver Index, Cytokines and Aminotransferase levels in NAFLD Patients: evidence from a Randomized Clinical Trial. J Gastrointest Liver. (2018) 27:41–9. doi: 10.15403/jgld.2014.1121.271.kby
31. Malaguarnera M, Vacante M, Antic T, Giordano M, Chisari G, Acquaviva R, et al. longum with fructo-oligosaccharides in patients with non alcoholic steatohepatitis. Digest Dis Sci. (2012) 57:545–53. doi: 10.1007/s10620-011-1887-4
32. Manzhalii E, Virchenko O, Falalyeyeva T, Beregova T, Stremmel W. Treatment efficacy of a probiotic preparation for non-alcoholic steatohepatitis: a pilot trial. J Digest Dis. (2017) 18:698–703. doi: 10.1111/1751-2980.12561
33. Mofidi F, Poustchi H, Yari Z, Nourinayyer B, Merat S, Sharafkhah M, et al. Synbiotic supplementation in lean patients with non-alcoholic fatty liver disease: a pilot, randomised, double-blind, placebo-controlled, clinical trial. Brit J Nutr. (2017) 117:662–8. doi: 10.1017/S0007114517000204
34. Mohamad Nor MH, Ayob N, Mokhtar NM, Raja Ali RA, Tan GC, Wong Z, et al. The effect of probiotics (MCP(®) BCMC(®) Strains) on hepatic steatosis, small intestinal mucosal immune function, and intestinal barrier in patients with non-alcoholic fatty liver disease. Nutrients. (2021) 13:3192. doi: 10.3390/nu13093192
35. Mohammad Sadrkabir MD, ShirinJahed MD, Zahra Sadeghi MD, KhaterehIsazadeh MD. The effect of gerilact on non-alcoholic fatty liver disease. J Kerman Univ Med Sci. (2020) 27:82–90. doi: 10.22062/JKMU.2020.89598
36. Nabavi S, Rafraf M, Somi MH, Homayouni-Rad A, Asghari-Jafarabadi M. Effects of probiotic yogurt consumption on metabolic factors in individuals with nonalcoholic fatty liver disease. J Dairy Sci. (2014) 97:7386–93. doi: 10.3168/jds.2014-8500
37. Sayari S, Neishaboori H, Jameshorani M. Combined effects of synbiotic and sitagliptin versus sitagliptin alone in patients with nonalcoholic fatty liver disease. Clin Mol Hepatol. (2018) 24:331–8. doi: 10.3350/cmh.2018.0006
38. Scorletti E, Afolabi PR, Miles EA, Smith DE, Almehmadi A, Alshathry A, et al. Synbiotics alter fecal microbiomes, but not liver fat or fibrosis, in a randomizedtrial of patients with nonalcoholic fatty liver disease. Gastroenterology. (2020) 158:1597–610. doi: 10.1053/j.gastro.2020.01.031
39. Sepideh A, Karim P, Hossein A, Leila R, Hamdollah M, Mohammad EG, et al. Effects of multistrain probiotic supplementation on glycemic and inflammatory indices in patients with nonalcoholic fatty liver disease: a double-blind randomized clinical trial. J Am Coll Nutr. (2016) 35:500–5. doi: 10.1080/07315724.2015.1031355
40. Shavakhi A, Minakari M, Firouzian H, Assali R, Hekmatdoost A, Ferns G, et al. Effect of a probiotic and metformin on liver aminotransferases in non-alcoholic steatohepatitis: a double blind randomized clinical trial. Int J Prev Med. (2013) 4:531–7.
41. Hu X. Effect of probiotics in adjuvant treatment of non-alcoholic fatty liver dis-ease. Chin Modern Med. (2021) 28:167–70. doi: 10.3969/j.issn.1674-4721.2021.25.045
42. Ling L., Wang J., Dan G. (2019). Clinic efficacy of probiotics combined with ursodeoxycholic acid on non-alcoholic fatty liver disease. Lab Med Clin. 16:3413–5. doi: 10.3969/j.issn.1672-9455.2019.23.006
43. Wang LJ, Zhang JP, Chen MH. Effects of probiotics on liver function, glucose and lipids metabolism, fecal flora in children with nonalcoholic fattyliver disease. Chin J School Health. (2019) 40:1545–8. doi: 10.16835/j.cnki.1000-9817.2019.10.030
44. Wei XP. Effect of Probiotics combined with reduced glutathione on liver function and blood lipid level in patients with nonalcoholic fatty liver disease. Heilongjiang Med J. (2021) 45:722–4. doi: 10.3969/j.issn.1004-5775.2021.07.017
45. Wen JF, Ye GL, Zhang HX, Ding JX, Chen SH. Clinical efficacy of bifidobacherium triple active bacteria combined with polyene phosphatidyl choline on NASH. Modern Chin Doc. (2014) 52:13–5.
46. Zhang LN. Effects of Intestinal Probiotics on Liver and Kidney Metabolism in Nonalcoholic Fatty Liver Disease. Qingdao University, Qing Dao (2017).
47. Zhao QW. LV DX. Probiotics for non-alcoholic fatty liver disease intervention effect. Chin J Mod Med. (2016) 54:29–33.
48. Zheng D, Wu J, Gan HY, Li H, Ren HP, Wang J, et al. Clinical study of probiotics for non-alcoholic fatty liver disease. Chin J Clin Gastroenterol. (2018) 30:240–3. doi: 10.3870/lcxh.j.issn.1005-541X.2018.04.09
49. Mirmiranpour H, Huseini HF, Derakhshanian H, Khodaii Z, Tavakoli-Far B. Effects of probiotic, cinnamon, and synbiotic supplementation on glycemic control and antioxidant status in people with type 2 diabetes, a randomized, double-blind, placebo-controlled study. J Diabetes Metab Disord. (2020) 61:1–19. doi: 10.1007/s40200-019-00474-3
50. Drucker DJ. The role of gut hormones in glucose homeostasis. J Clin Invest. (2007) 117:24–32. doi: 10.1172/JCI30076
51. Polyzos SA, Kountouras J, Zavos C. Nonalcoholic fatty liver disease: the pathogenetic roles of insulin resistance and adipocytokines. Curr Mol Med. (2009) 9:299–314. doi: 10.2174/156652409787847191
52. Nazarii K, Tetyana F, Galyna M, Dmytro K, Iuliia K. Effect of alive probiotic on insulin resistance in type 2 diabetes patients: randomized clinical trial. Diabetes Metab Synd. (2018) 12:617–24. doi: 10.1016/j.dsx.2018.04.015
53. Esposito E, Iacono A, Bianco G, Autore G, Cuzzocrea S, Vajro P, et al. Probiotics reduce the inflammatory response induced by a high-fat diet in the liver of young rats. J Nutr. (2009) 139:905–11. doi: 10.3945/jn.108.101808
54. Luck H, Tsai S, Chung J, Clemente-Casares X, Ghazarian M, Revelo XS, et al. Regulation of obesity-related insulin resistance with gut anti -inflammatory agents. Cell Metab. (2015) 21:527–42. doi: 10.1016/j.cmet.2015.03.001
55. Wang X., Ota N., Manzanillo P., Kates L., Zavala-Solorio J., Eidenschenk C., et al. Interleukin- 22 alleviates met- abolic disorders and restores mucosal immunity in diabetes. Nature. (2014) 514:237–241. doi: 10.1038/nature13564
56. Pirgon O, Bilgin H, Cekmez F, Kurku H, Dündar BN. Association between insulin resistance and oxidative stress parameters in obese adolescents with non-alcoholic fatty liver disease. J Clin Res Pediatr E. (2013) 5:33–9. doi: 10.4274/Jcrpe.825
57. Morvaridzadeh M, Nachvak SM, Mohammadi R, Moradi S, Mostafai R, Pizarro AB, et al. Probiotic yogurt fortified with vitamin D can improve glycemic status in non-alcoholic fatty liver disease patients: a randomized clinical trial. Clin Nutr Res. (2021) 10:36–47. doi: 10.7762/cnr.2021.10.1.36
58. Asemi Z, Samimi M, Tabassi Z, Naghibi Rad M, Rahimi Foroushani A, Khorammian H, et al. Effect of daily consumption of probiotic yoghurt on insulin resistance in pregnant women: a randomized controlled trial. Eur J Clin Nutr. (2013) 67:71–4. doi: 10.1038/ejcn.2012.189
59. Zheng RD, Zhuang QY, Chen JN, Chen J, Lu YH. Risk factors analysis of nonalcoholic fatty liver disease in Chinese men. Chin J hepatol. (2013) 21:62–5.
60. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention, National Heart Lung, and Blood Institute, American Heart Association, World Heart Federation, International Atherosclerosis Society, and International Association for the Study of Obesity. Circulation. (2009) 120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644
61. Liangpunsakul S, Chalasani N. Unexplained elevations in alanine aminotransferase in individuals with the metabolic syndrome: results from the third National Health and Nutrition Survey (NHANES III). Am J Med Sci. (2005) 329:111–6. doi: 10.1097/00000441-200503000-00001
62. Wang C, Zhang CC, Li SJ, Yu LL, Tian FW, Zhao JX, et al. Effects of probiotic supplementation on dyslipidemia in type 2 diabetes mellitus: a meta-analysis of randomized controlled trials. Foods. (2020) 9:1540. doi: 10.3390/foods9111540
63. Delzenne NM, Kok NN. Biochemical basis of oligofructose-induced hypolipide-mia in animal models. J Nutr. (1999) 129:1467–70. doi: 10.1093/jn/129.7.1467S
64. Wa Y, Yin B, He Y, Xi W, Huang Y, Wang C, et al. Effects of single probiotic- and combined probiotic- fermented milk on lipid metabolism in hyperlipidemic rats. Front Microbiol. (2019) 10:1312. doi: 10.3389/fmicb.2019.01312
65. Diether NE, Willing BP. Microbial fermentation of diet-ary protein: An important factor in diet–microbe–host interaction. Microorganisms. (2019) 7:19. doi: 10.3390/microorganisms7010019
66. Dai ZL, Li XL, Xi PB, Zhang J, Wu G, Zhu WY, et al. Metabolism of select amino acids in bacteria from the pig small intestine. Amino Acids. (2012) 42:1597–608. doi: 10.1007/s00726-011-0846-x
67. Fan P, Li L, Rezaei A, Eslamfam S, Che D, Ma X, et al. Metabolites of dietary protein and peptides by intestinal microbes and their impacts on gut. Curr Protein Pept Sc. (2015) 16:646–54. doi: 10.2174/1389203716666150630133657
68. Friedman LS, Martin P, Munoz SJ. Laboratory evaluation of the patients with liver disease. In: Zakim D, Boyer TD, editors. Hepatology, 4th ed. (2003). Philadelphia: Saunder. p. 661–708. doi: 10.11748/bjmy.issn.1006-1703.2020.08.020
69. Jiang L, Yang GS, Ma YC, Ren SQ. The relationship between serum ALT, AST, ALB and liver fibrosis in patients with non-alcoholic fatty liver disease. Lab Immun Clin Med. (2020) 27:1363–6.
70. Velayudham A, Dolganiuc A, Ellis M, Petrasek J, Kodys K, Mandrekar P, et al. VSL#3 probiotic treatment attenuates fibrosis without changes in steatohepatitis in a diet-induced nonalcoholic steatohepatitis model in mice. Hepatology. (2009) 49:989–97. doi: 10.1002/hep.22711
71. Naito E, Yoshida Y, Makino K, Kounoshi Y, Kunihiro S, Takahashi R, et al. Beneficial effect of oral administration of Lactobacillus casei strain Shirota on insulin resistance in diet-induced obesity mice. J Appl Microbiol. (2011) 110:650–7. doi: 10.1111/j.1365-2672.2010.04922.x
72. Liu HX, Keane R, Sheng L, Wan YJ. Implications of microbiota and bile acid in liver injury and regeneration. J Hepatol. (2015) 63:1502–10. doi: 10.1016/j.jhep.2015.08.001
73. Jena PK, Sheng L, Nagar N, Wu C, Barile D, Mills DA, et al. Synbiotics Bifidobacterium infantis and milk oligosaccharides are effective in reversing cancer-prone nonalcoholic steatohepatitis using western diet-fed FXR knockout mouse models. J Nutr Biochem. (2018) 57:246–54. doi: 10.1016/j.jnutbio.2018.04.007
74. Reis S, Conceição L, Rosa D, Siqueira N, Peluzio M. Mechanisms responsible for the hypocholesterolaemic effect of regular consumption of probiotics. Nutr Res Rev. (2017) 30:36–49. doi: 10.1017/S0954422416000226
75. Thushara RM, Gangadaran S, Solati Z, Moghadasian MH. Cardiovascular benefits of probiotics: a review of experimental and clinical studies. Food Funct. (2016) 7:632–42. doi: 10.1039/C5FO01190F
76. Ahtesh FB, Stojanovska L, Apostolopoulos V. Anti-hypertensive peptides released from milk proteins by probiotics. Maturitas. (2018) 115:103–9. doi: 10.1016/j.maturitas.2018.06.016
Keywords: NAFLD, probiotics, prebiotics, synbiotics, microbiota modulation, energy metabolism biomarkers
Citation: Li S, Liu J, Wang Z, Duan F, Jia Z, Chen X and Li S (2022) The promising role of probiotics/prebiotics/synbiotics in energy metabolism biomarkers in patients with NAFLD: A systematic review and meta-analysis. Front. Public Health 10:862266. doi: 10.3389/fpubh.2022.862266
Received: 25 January 2022; Accepted: 01 July 2022;
Published: 25 July 2022.
Edited by:
Foong Ming Moy, University of Malaya, MalaysiaReviewed by:
Doaa El Amrousy, Tanta University, EgyptCopyright © 2022 Li, Liu, Wang, Duan, Jia, Chen and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suling Li, aGstbHNsQDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.