 Samantha Pawer1*
Samantha Pawer1* Kate Turcotte1
Kate Turcotte1 Ediriweera Desapriya1Alex Zheng1Amanat Purewal1
Ediriweera Desapriya1Alex Zheng1Amanat Purewal1 Alyssa Wellar1Kenneth Kunz2
Alyssa Wellar1Kenneth Kunz2 Len Garis1,3
Len Garis1,3 Larry S. Thomas4
Larry S. Thomas4 Ian Pike1,5
Ian Pike1,5- 1BC Injury Research and Prevention Unit, British Columbia Children's Hospital, Vancouver, BC, Canada
- 2Independent Medical Oncologist, and Firefighter Cancer Consultant, Victoria, BC, Canada
- 3School of Criminology and Criminal Justice, University of the Fraser Valley, Abbotsford, BC, Canada
- 4Surrey Fire Service, City of Surrey, Surrey, BC, Canada
- 5Department of Pediatrics, The University of British Columbia, Vancouver, BC, Canada
Objectives: This study explored how demographic characteristics, life experiences, and firefighting experiences have an impact on work-related injuries among female firefighters, and described events surrounding such work-related injuries.
Methods: This online survey was available from June 2019 to July 2020. Questions related to demographic characteristics, life experiences, firefighting experiences, and work-related injuries. Descriptive analyses characterized variables by the presence or absence of work-related injury, injury severity, job assignment, and country of residence.
Results: There were 1,160 active female firefighter survey respondents from the US and Canada, 64% of whom reported having at least one work-related injury. US respondents made up 67% of the total but 75% of the injured sample. Injured respondents were older, had been in the fire service longer, and had a greater number of fires and toxic exposures than non-injured respondents. Heavier weight, tobacco use, and alcohol consumption were more common among injured respondents. The two most common contributing factors to work-related injuries were human error and firefighter fatigue. Among respondents who reported an injury-related time loss claim, 69% were wearing protective equipment when injured, and 9% of the injuries directly resulted in new policy implementation.
Conclusions: These findings can help inform resource allocation, and development of new policies and safety protocols, to reduce the number of work-related injuries among female firefighters.
Introduction
Firefighters are essential workers who respond to fires, vehicle collisions, medical emergencies, hazardous material spills, rescues, and other potentially harmful events. Such critical incidents can have negative consequences for individual and organizational firefighting performance (1). This type of work can cause declines in the physical and mental health of firefighters, and thus their ability to work (2). In the United States (US), firefighters experienced an estimated >30,000 fire ground injuries per year from 2010 to 2014, with similar rates of 61.6 per 1,000 male and 61.2 per 1,000 female firefighters (3). US emergency departments treated ~351,800 injured firefighters from 2003 to 2014, 95% of whom were males (4).
While males make up approximately half of the general population in the US and Canada (5, 6), they reflect the majority among the general firefighting population in the existing literature. In 2018, females accounted for ~8% of all US firefighters, and just 4% of career firefighters (7), with similar trends observed in Canada (6). Although only a small proportion, between the US and Canada collectively, there are ~95,145 female firefighters: 93,700 in the US (career and volunteer) (7), and 1,445 in Canada (career only) (8). Yet, little is known about this sub-population, particularly when it comes to the details regarding work-related injuries.
While many firefighter injury studies do not exclude females, females typically make up such a small proportion of samples that it is difficult to draw any specific conclusions regarding their health outcomes (9, 10). Furthermore, these studies often do not analyze data by sex or gender (4, 11). In an international survey of 840 female firefighters in 14 countries, those in North America were more likely to have been injured than those in the UK and Ireland, Australasia, and Europe (12). However, this study focused on health and wellbeing in general, and did not provide details regarding injury events. Of 3,012 female firefighters surveyed in the US, 31.7% reported at least one work-related injury within the past year, 43% of which resulted in work loss and 25% of which became chronic injuries, like back pain (13).
More information is needed in order to inform best safety practices and injury prevention policies. The present study was uniquely designed to address existing knowledge gaps by collecting comprehensive descriptions about work-related injuries among female firefighters. The objectives of this study were to: (1) describe the demographic characteristics and life experiences of female firefighters; (2) describe firefighting experiences of female firefighters; and (3) describe events resulting in work-related injuries among female firefighters and the types of injuries sustained. The conclusions from this study will be important for developing and evaluating health and wellness policies, designating resources, and designing surveillance, education, and prevention strategies to make the workplace safer for, and more supportive of, female firefighters.
Methods
Study Design and Recruitment
An online cross-sectional survey was developed by the research team and distributed globally to collect information from career and volunteer female firefighters, as approved by the University of British Columbia Children's and Women's Research Ethics Board (H18-03318). The full survey was professionally translated into French by British Columbia Professional Legal Interpreters, Inc. The survey was advertised on industry-specific magazine sites and blogs promoting firefighter safety and health, including, Firefighting in Canada, and Fire and EMS Leader Pro. Additionally, participants were recruited via postings and email lists by agencies including: the International Association of Firefighters; CTIF—The International Association of Fire & Rescue Services; Center for Fire, Rescue and EMS Health Research at the National Department of Research Institutes; Fire and Rescue New South Wales; and the Memphis Fire Department. Snowball sampling was employed, which is a non-probability sampling technique where existing subjects recruit future subjects from among their acquaintances (14).
Prospective participants were directed to the online survey to learn more about the study, before consenting to participate. Using REDCap electronic data capture tools hosted at the Provincial Health Services Authority (15, 16), the online survey was available in both English and French from June 7, 2019 to July 19, 2020.
Survey Content
The survey contained 85 questions. The Demographic Profile included information on sex/gender, age, height, weight, country of residence, and ethnicity. The Lifestyle Profile included history of tobacco use and alcohol consumption. The Firefighter Profile included questions about time in the fire service (e.g., years since starting and/or leaving the service), department type and rank, firefighting experiences including estimated number of career fires and toxic exposures, and whether the respondent had Presumptive Coverage for specified injuries or diseases presumed to be work-related. The Injury Profile focused on work-related injuries: injury type, severity, body part, event during injury (e.g., fire ground, in-transit, training), contributing factors (e.g., equipment failure, lack of training, firefighter fatigue), time off and return to work, protective equipment at time of injury, and policies instituted as a direct result of the injury. In addition, the Cancer Profile included questions about cancer and pre-cancer experiences (e.g., type of cancer/pre-cancer, stage and grade, method of detection and treatment, family history), with the additional lifestyle variables of hormone use, pregnancy, and breast feeding, all of which will be reported in a separate paper.
Survey questions were primarily multiple choice with pre-selected options (as seen in the results); many allowed multiple selections per question. Qualitative analyses of the open-ended questions will be reported in a separate paper. The survey was branched, with some questions only available based on answers to previous questions.
Exclusion Criteria and Data Cleaning
Upon survey closure, data from all 1,723 entries were extracted. Entries were removed if all questions were left blank, if it was a duplicate entry from the same respondent, or if the respondent reported that they were both born as and identify as male, leaving 1,344 surveys. We aimed to have an inclusive sample, including anyone born female (regardless of how they currently identify) or who was born male but currently identify as female. Due to low numbers from some countries, those making up fewer than 5% (67 respondents) of this sample were excluded (e.g., Australia, New Zealand, the UK) in order to provide a more stable description of injury among female firefighters without issues with geographical differences in firefighting or lifestyle experiences, leaving 1,232 responses from the US and Canada. Responses from 72 inactive firefighters were excluded to ensure results reflect current female firefighters and their experiences with work-related injuries. The final sample size was 1,160 respondents.
Data Analysis
Descriptive analyses were conducted on the final dataset of active female firefighters residing in the US and Canada. Survey response rates were calculated using the number of female firefighters published for the US (7) and Canada (17) (assuming 4.4% of Canadian firefighters are female, as reported by Statistics Canada) (8). Demographic characteristics, life experiences, and firefighting experiences were described by the presence or absence of a work-related injury. These data were further broken down by injury type and severity, with groups including injuries requiring <2 weeks off work (reported only, received first aid only, treated by a doctor only, those who missed <2 weeks), 2–4 weeks off work, more than 4 weeks off work, and life-threatening injuries. Firefighting experiences were assessed for injured and non-injured samples by country of residence. Characteristics of work-related injuries were broken down by department (career, volunteer, both), and country of residence. Continuous data were presented as means and standard deviation for normal data, and as medians and quartile distributions for non-normal data, while categorical data were displayed as counts with an associated proportion of the sample. Continuous variables for the US and Canada were compared using two-sample t-tests for normal data and Wilcoxon rank-sum tests for non-normal data, and categorical variable responses were compared using Chi-square (χ2) tests, to a significance level of p ≤ 0.05.
Results
Demographics and Life Experiences
A total of 1,160 active female firefighters from the US (67%) and Canada (33%) were included in the analyses (Table 1). Our sample represents ~0.8% of US and 5.8% of Canadian female firefighters. Overall, 99% of the sample were individuals both born female and currently identifying as female, and the mean age was 40.5 years (SD = 9.6, range = 18–71). In total, 64% of respondents experienced at least one work-related injury, including 554 (72%) among the US respondents and 188 (48%) among the Canadian respondents. Injuries resulting in fewer than 2-weeks of lost work time were the most common at 64% of all injuries, followed by those resulting in more than 4-weeks of lost work (38%), 2- to 4-weeks of lost work (14%), and life-threatening injuries (2%). Three quarters (n = 554) of all injuries were among respondents in the US. This proportion of US respondents increases with higher injury severity from 71% of those with <2-weeks work lost, up to 87% with life threatening injuries.
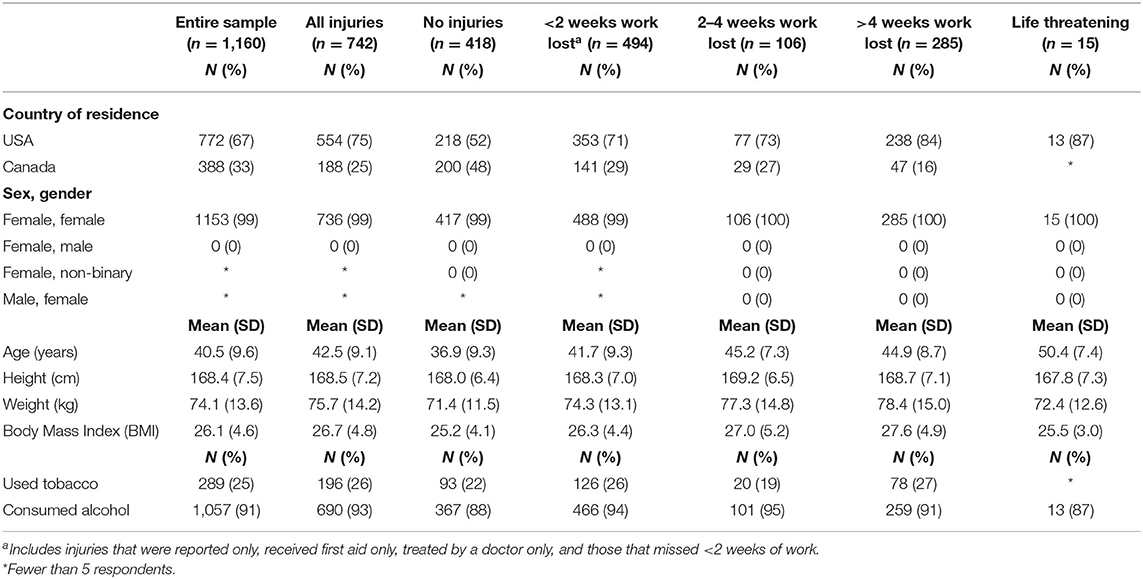
Table 1. Demographic characteristics of active female firefighter survey respondents in the US and Canada, by injury severity as measured by time of work lost.
Injured respondents tended to be older and heavier (at the time of survey response) than those who were not injured (Table 1). There was no relationship found between age and body mass index (BMI) at the time of survey response (r2 = 0.004). Injured respondents had slightly higher proportions of tobacco use (26%) and alcohol consumption (93%), as compared to those who had never been injured.
Firefighting Experience
Greater length of time in the fire service, number of career fires, and number of toxic exposures generally increased with injury severity (Table 2). Career firefighters were injured more than volunteers. By rank, firefighters made up a smaller proportion of the sample as injury severity increased, while company/station officers made up larger proportions with increasing severity. Most recent assignment did not differ between injured and non-injured respondents. A higher proportion of injured respondents took a leave of absence than non-injured.
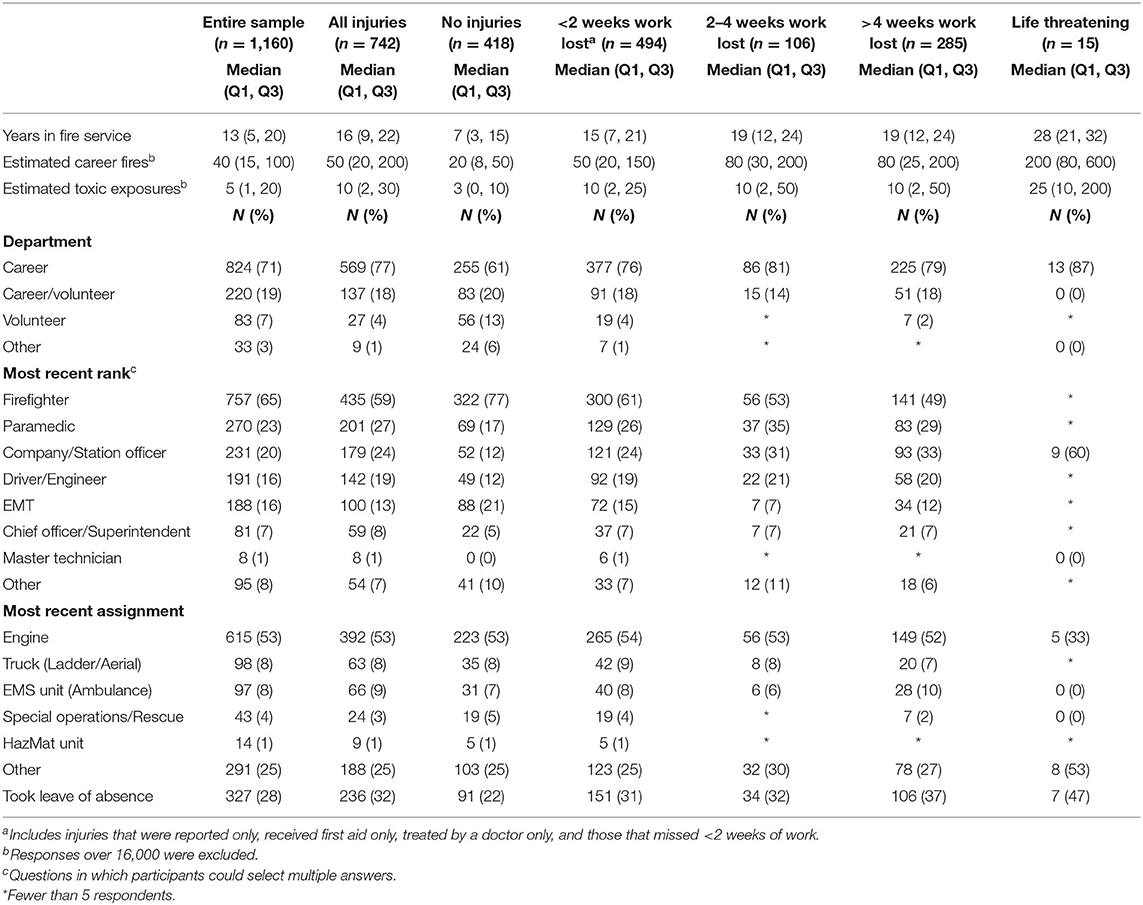
Table 2. Firefighting experience of active female firefighter survey respondents in the US and Canada, by injury severity as measured by time of work lost.
Respondents in the US reported a median average of 15-years (Quartiles: 7, 22) in the fire service, compared to 10-years (Quartiles: 4, 17) reported by respondents in Canada (Table 3). US respondents injured on the job tended to have a higher number of career fires than those in Canada, with a median average of 40 (Quartiles: 15, 150) vs. 30 (Quartiles: 15, 80), and both countries had many fewer career fires among those who had not been injured. A similar pattern was seen for toxic exposures. Conversely, a higher proportion of respondents in Canada reported taking a leave of absence than those in the US. There was little difference between respondents in the US and Canada by department, rank, or most recent assignment.
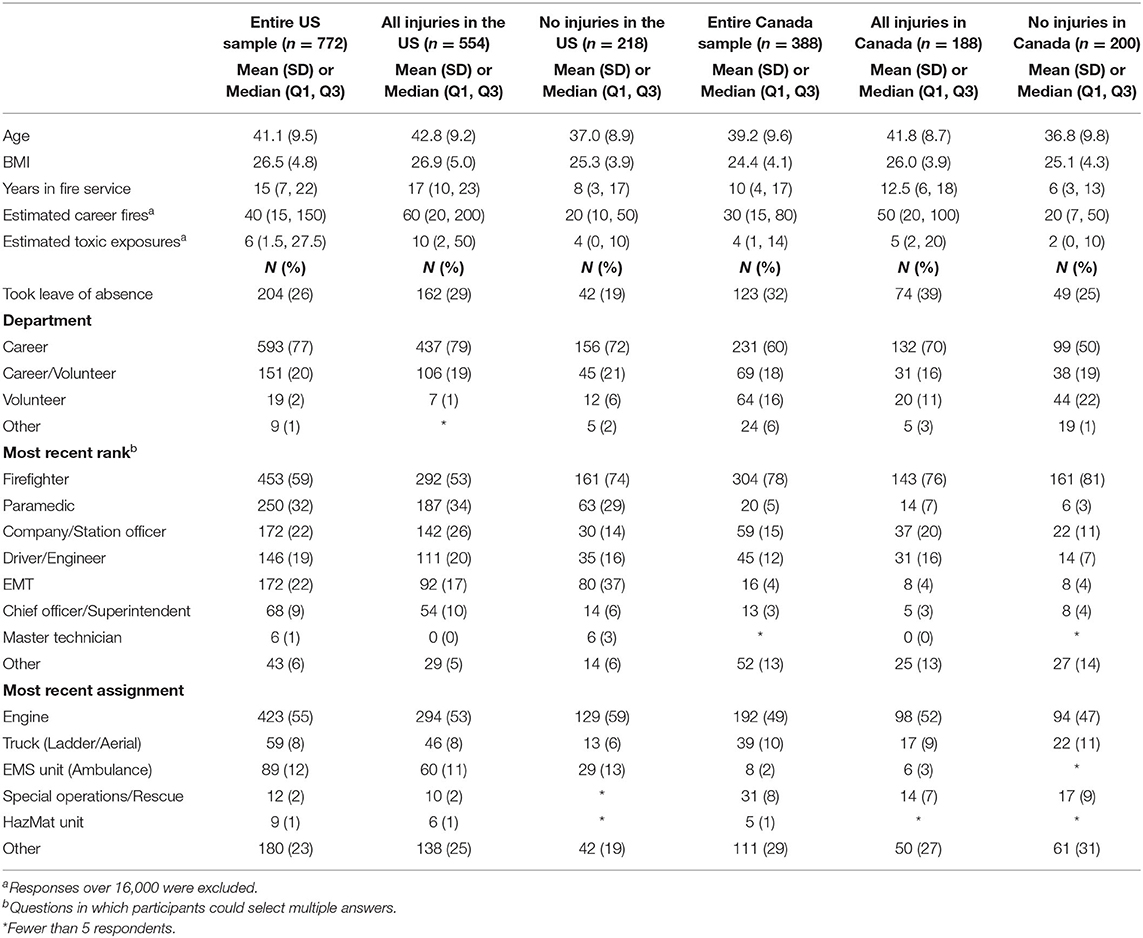
Table 3. Firefighting experience of active female firefighter survey respondents in the US and Canada, by country and injury status.
Work-Related Injuries
Career firefighters were injured more often than volunteers; 69% (n = 569) of career firefighters were injured, while 33% (n = 27) of volunteers were injured (Table 4). Among career, career/volunteer, and volunteer female firefighters, the most common injury types were strains, sprains and muscle pain, while extremities, backs, shoulders/chests were the most commonly injured body parts. Leading contributing factors for work-related injuries were human error, fatigue, and lack of situational awareness. Upon returning to work after an injury time-loss claim, 35% (n = 118) of female firefighters had modified duties, 29% (n = 100) had graduated return-to-work processes, and 18% (n = 62) had other supports. As well, in 9% (n = 30) of cases, a new policy was made directly resulting from the injury.
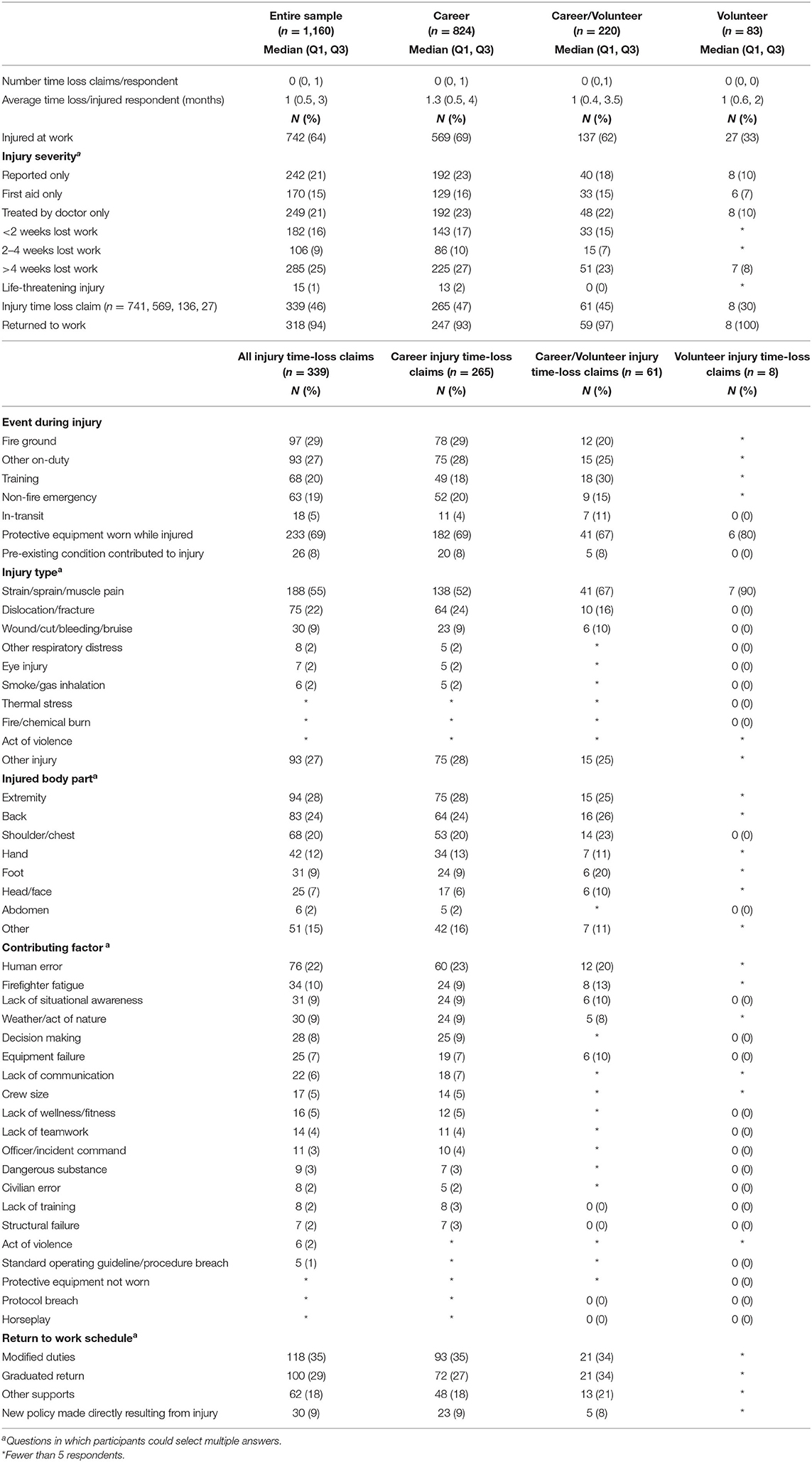
Table 4. Characteristics of work-related injuries among active female firefighters in the US and Canada, by department.
Per respondent, female firefighters in the US reported significantly more injury time loss claims than in Canada (p = 0.015), and significantly longer length of time loss per injured respondent (p = 0.012; Table 5). A significantly higher proportion of respondents from the US reported being injured at work (p < 0.001), with different injury severity profiles (p = 0.012). The most common injury severity among respondents in the US was missing more than 4-weeks of work (31%), which differed from Canadian respondents, who most often reported injuries only, or were treated by a doctor only (both at 16%). While the US respondents reported significantly more injury time loss claims than Canadian respondents (p = 0.025), similarly high proportions reported having returned to work.
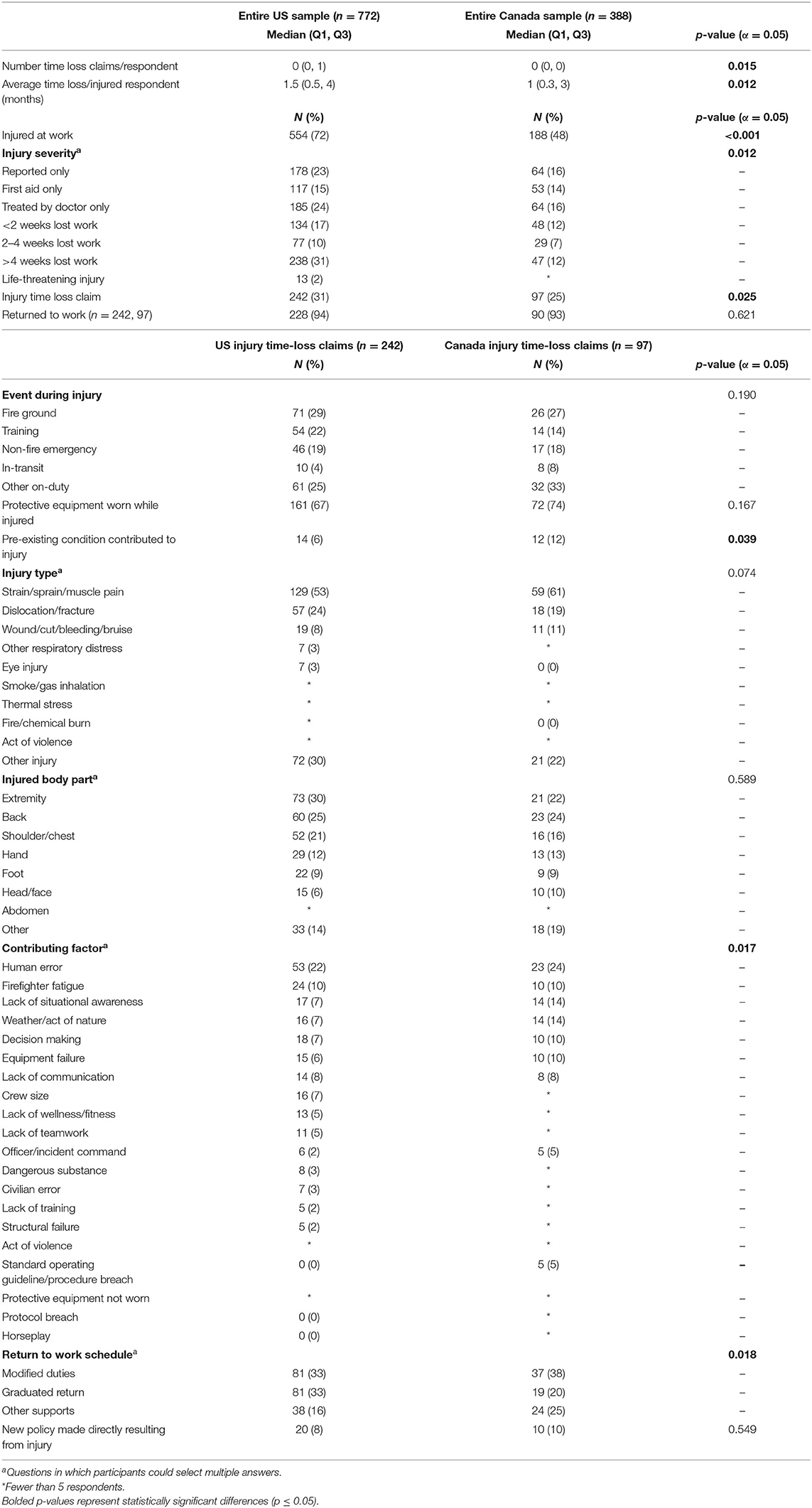
Table 5. Characteristics of work-related injuries among active female firefighters in the US and Canada, by country.
Generally, characteristics of work-related injuries were similar among respondents in the US and Canada, however a significantly higher proportion of injury time loss claims in Canada reported pre-existing conditions that contributed to the injury (p = 0.039). Significant differences between the US and Canada were also found for contributing factors (p = 0.017), and return to work schedules (p = 0.018).
Discussion
This study surveyed 1,160 active female firefighters in the US and Canada to address knowledge gaps and provide information about female firefighter injuries. Overall, our sample was similar to that described by Jahnke et al. study (18), with the average age of our injured respondents being 42.5 (SD 9.1) years compared to 38.8 (SD 9.2), and having an average of 16.1 (SD 8.8) years in the fire service as compared to 14.4 (SD 8.6).
While it has been reported that female firefighters in North America suffer more injuries than in other regions (12), direct comparisons between the US and Canada are lacking. We identified a higher proportion of female firefighters in the US reporting injuries than in Canada. Among those who had been injured, the proportion of injuries among US vs. Canadian respondents increased with higher injury severity. Similar to our findings, the US had a greater number of work-related injuries among firefighters from 2010 to 2014 as compared with 32 other countries (19). Our data also indicate that female firefighters in the US were older, had a higher BMI, and had a greater number of career fires and toxic exposures than those in Canada, and, on average, served in the fire service longer than respondents in Canada. All of this points to the increased risk of injury with more exposures to high risk situations; older, more experienced firefighters have been involved in more emergency responses.
Other studies have identified that firefighters with a higher-than-normal BMI were three times more likely to file an injury-related compensation claim compared with those of normal BMI (20). Higher overall good self-rated health, fitness, and exercise have all related to a lower likelihood of sustaining an injury (13). Low fitness levels among firefighters can increase injury risk (20), and compromise occupational readiness. Similarly, low fitness among women entering the US Army, as indicated by a failed 5-min step test, experienced more stress fractures and musculoskeletal injuries early in their careers as compared with more fit individuals (21). Programs promoting wellbeing among firefighters, including injury prevention and rehabilitation components, have resulted in significantly fewer workers' compensation claims (22), and well-designed exercise interventions have been shown to enhance overall firefighter health and fitness (23).
A slightly higher proportion of injured respondents reported tobacco use and alcohol consumption than those not injured. Previous research found that 16.5% of female firefighters who consume alcohol were problem drinkers, and that problem drinkers were 40% more likely to report work-related injuries compared with the general female firefighter population (24). Female firefighters with a history of tobacco use have also been found to have higher odds of injury (13).
In both countries, career firefighters and those assigned to an engine made up the largest proportion of injuries. Similarly, studies have found that career firefighters in the US were injured on the job more than volunteers, although these samples were predominantly males (3, 4). In the US and Canada, injuries occurred most often on the fire ground, adding to the conflicting literature describing firefighter injuries, some of which report training as the most common activity at the time of injury (11, 13, 18), and some of which report firefighting, fire ground duties, or fire station duties as the most common activities at the time of injury (4, 18, 25). In this study, training was the second most commonly reported event at the time of injury, supporting the evidence that the fire ground and training both present a high risk of injury for female firefighters; safety improvement efforts should be focused there.
In terms of injury severity, fireground firefighters made up a smaller proportion of injured respondents as severity increased, while company/station officers made up a larger proportion. Although there is little existing information regarding rank and injury severity, our findings concur with studies on predominately male firefighters. The first found firefighter/paramedics made up a larger proportion of those who had been injured than those who had not been injured (18), while the second found that company officers had one of the lowest proportions of injuries (11). We found that, other than master technicians for which all eight respondents reported an injury, company/station officers reported the highest frequency of injuries, however, our cross-sectional data cannot confirm whether respondents held these ranks when injured.
Men and women typically have different body shapes, sizes, and compositions, yet only 25% of female firefighters previously surveyed in North America had access to female-specific personal protective equipment (12). This may have contributed to our findings that 69% of career and 80% of volunteer female firefighters were injured despite the use of protective equipment during the injury event. Ill-fitting equipment is insufficient in protecting the female firefighters against injury, by impairing movement and reducing agility. Thus, the use of female-specific protective equipment is required for optimal performance and injury reduction.
Strains/sprains/muscle pain were the most common injuries identified, followed by dislocations/fractures, and wounds/cuts/bleeds/bruises. This is similar to another sample of female firefighters from the US, who reported predominantly dislocations/strains/sprains, followed by superficial injuries/open wounds (13). Other injuries, including eye injuries or smoke/gas inhalation, occurred in lower proportions, potentially because protective equipment reduced the risk for these injuries. The extremities were most often injured, followed by backs, and shoulders/chests. This differs from previous research on female firefighters that reported the most frequent involvement of the abdomen, pelvis, or back (including lower back, lumbar spine) (13, 26, 27). However, it is difficult to compare results between studies, because the extremities option in this study was broader, capturing more injures than other studies that often break options down as foot, lower leg, upper thigh, etc.
Overall, human error was the most frequently reported contributing factor, followed by firefighter fatigue. Reform is needed for female firefighters to be able to work safely; appropriate protocols are needed to prevent overexertion that can lead to injury. These findings also emphasize that good health and adherence to female-specific safety practices at the individual and organizational level are imperative. Focused efforts in this area will reduce strain on the fire service in terms of chronic injury and time loss claims.
While historically male-dominated professions in the US and Canada, such as physicians, are seeing a greater proportion of women in the workforce over time (28, 29), firefighting has experienced much slower recruitment of women. This is reflected in how female firefighters view their occupation and their role within it. Canadian female firefighters reported feeling “othered” due to discrimination and hostility in the workplace, leading to self-doubt (30). Female firefighters in Ontario discussed challenges in performing physically demanding job duties compared with male colleagues, which caused them to implement creative solutions to overcome obstacles, as requests for assistance were often linked with negative male attitudes (9). This challenging work environment likely contributes to injuries among female firefighters, and is an important female-specific issue in the firefighting profession. Even though female firefighter-specific challenges have previously been reported, of the 339 respondents who reported an injury-time loss claim in the present study, only 30 (9%) reported that a new policy succeeded their injury.
Our survey results indicate that work-related injuries are a significant issue among female firefighters in the US and Canada. We identified key factors involved in such injuries, as well as the circumstances surrounding these events, to arm stakeholders with additional information to aid in developing protocols and policies to reduce injury risk for female firefighters.
Given the nature of the present study, there are limitations. As the data were self-reported, accuracy of the responses cannot be verified. In some instances, respondents may not have felt comfortable answering questions honestly, which could bias the results. Since this survey was promoted as a work-related injury and cancer survey, respondents who were involved in such events may have been more or less inclined to complete the survey, which can decrease generalizability of the results. Further, as this study only captured an estimated 0.8% of female firefighters in the US and 5.8% in Canada, results may not be representative of the entire population of female firefighters in either country. Additionally, as minor injuries, such as bruises and cuts, are relatively common, they may have been under-reported due to recall bias. Conversely, female firefighters who were severely injured (or deceased) may not have been captured in this study. Finally, there are limitations with exploring the data by injury severity; time missed from work might be influenced by available length of paid leave, ability to take unpaid leave, jurisdictional differences in the availability of various healthcare services, or other factors.
Moving forward, future studies could test hypotheses about potential relationships between injury and variables not yet been analyzed. For example, subsequent research may explore the timing of when injuries occur along the career trajectory. Examining incidence, severity, location, and temporal aspects of work-related injuries by service function and gender would provide helpful information to directly compare the scope of injuries occurring among females compared with males.
Data Availability Statement
Due to the ethical confidentiality restrictions, data are available upon request.
Ethics Statement
This study was approved by the University of British Columbia Children's and Women's Research Ethics Board (H18-03318). Survey respondents provided informed consent at the start of the on-line survey.
Author Contributions
KK, LG, and IP: conceptualization. KT: investigation. SP, AZ, AP, and AW: data curation. SP: writing—original draft and visualization. IP: supervision. All authors: writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by City of Surrey Fire Department (grant number F19-00432).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Jacobsson A, Backteman-Erlanson S, Brulin C, Hörnsten Å. Experiences of critical incidents among female and male firefighters. Int Emerg Nurs. (2015) 23:100–4. doi: 10.1016/j.ienj.2014.06.002
2. Duran F, Woodhams J, Bishopp D. An interview study of the experiences of firefighters in regard to psychological contract and stressors. Empl Responsib Rights J. (2018) 30:203–26. doi: 10.1007/s10672-018-9314-z
3. Campbell R, National Fire Protection Association. U.S. firefighter injuries on the fireground, 2010–2014. Fire Technol. (2018) 54:461–77. doi: 10.1007/s10694-017-0692-9
4. Marsh SM, Gwilliam M, Konda S, Tiesman HM, Fahy R. Nonfatal injuries to firefighters treated in U.S. emergency departments, 2003–2014. Am J Prev Med. (2018) 55:353–60. doi: 10.1016/j.amepre.2018.04.051
5. United States Census Bureau. 2018 Population Estimates by Age, Sex, Race Hispanic Origin. United States Census Bureau (2019). Available online at: https://www.census.gov/newsroom/press-kits/2019/detailed-estimates.html (accessed July 29, 2021).
6. Statistics Canada. Canada [Country] Canada [Country] (Table). Census Profile, 2016 Census (2017). Available online at: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/page.cfm?Lang=E&Geo1=PR&Code1=01&Geo2=PR&Code2=01&SearchText=canada&SearchType=Begins&SearchPR=01&B1=Population&TABID=1&type=0 (accessed July 29, 2021).
7. Evarts B, Stein GP. US Fire Department Profile 2018. NFPA No. USS07. Quincy, MA: National Fire Protection Association (2020). p. 6.
8. Statistics Canada. Occupation - National Occupational Classification (NOC) 2016 (693A), Highest Certificate, Diploma or Degree (15), Labour Force Status (3), Age (13A) Sex (3) for the Labour Force Aged 15 Years Over in Private Households of Canada, Provinces Territories, Census Metropolitan Areas Census Agglomerations, 2016 Census - 25% Sample Data. Statistics Canada (2019). Available online at: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/dt-td/Rp-eng.cfm?TABID=2&LANG=E&APATH=3&DETAIL=0&DIM=0&FL=A&FREE=0&GC=0&GK=0&GRP=1&PID=110696&PRID=10&PTYPE=109445&S=0&SHOWALL=0&SUB=0&Temporal=2017&THEME=124&VID=0&VNAMEE=&VNAMEF= (accessed July 29, 2021).
9. Sinden K, Macdermid J, Buckman S, Davis B, Matthews T, Viola C. A qualitative study on the experiences of female firefighters. Work. (2013) 45:97–105. doi: 10.3233/WOR-121549
10. Hulett DM, Bendick M Jr. Thomas SY Moccio F. A National Report Card on Women in Firefighting. Washington, DC. (2008). Available online at: http://www.bendickegan.com (accessed September 6, 2021).
11. Phelps S, Drew-Nord D, Neitzel R, Wallhagen M, Michael B, OiSaeng H. Characteristics and predictors of occupational injury among career firefighters. Work Heal Saf. (2018) 66:301. doi: 10.1177/2165079917740595
12. Watkins ER, Walker A, Mol E, Jahnke S, Richardson AJ. Women firefighters' health and well-being: an international survey. Womens Health Issues. (2019) 29:424–31. doi: 10.1016/j.whi.2019.02.003
13. Hollerbach BS, Kaipust CM, Poston WSC, Haddock CK, Heinrich KM, Jahnke SA. Injury correlates among a national sample of women in the US fire service. J Occup Environ Med. (2020) 62:634–40. doi: 10.1097/JOM.0000000000001918
14. Shadish WR, Cook TD, Campbell DT. Experimental and Quasi-Experimental Designs for Generalized Causal Inference. 2nd ed. Boston, MA: Houghton Mifflin Company (2001).
15. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
16. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
17. Haynes HJG, Stein GP. Canadian Fire Department Profile, 2014-2016 (2018). Available online at: https://www.nfpa.org//-/media/Files/News-and-Research/Fire-statistics-and-reports/Emergency-responders/oscanada.pdf (accessed December 16, 2021).
18. Jahnke SA, Poston WSC, Haddock CK, Jitnarin N. Injury among a population based sample of career firefighters in the central USA. Inj Prev. (2013) 19:393–8. doi: 10.1136/injuryprev-2012-040662
19. Brushlinsky N, Ahrens M, Sokolov S, Wagner P. World Fire Statistics (2016). Available online at: http://www.academygps.ru (accessed August 9, 2021).
20. Kuehl KS, Kisbu-Sakarya Y, Elliot DL, Moe EL, DeFrancesco CA, MacKinnon DP, et al. Body mass index is a predictor of fire fighter injury and worker compensation claims. J Occup Environ Med. (2012) 54:579–82. doi: 10.1097/JOM.0b013e318249202d
21. Cowan DN, Bedno SA, Urban N, Lee DS, Niebuhr DW. Step test performance and risk of stress fractures among female army trainees. Am J Prev Med. (2012) 42:620–4. doi: 10.1016/j.amepre.2012.02.014
22. Kuehl KS, Elliot DL, Goldberg L, Moe EL, Perrier E, Smith J. Economic benefit of the PHLAME wellness programme on firefighter injury. Occup Med. (2013) 63:203–9. doi: 10.1093/occmed/kqs232
23. Andrews KL, Gallagher S, Herring MP. The effects of exercise interventions on health and fitness of firefighters: a meta-analysis. Scand J Med Sci Sports. (2019) 29:780–90. doi: 10.1111/sms.13411
24. Haddock CK, Poston WSC, Jahnke SA, Jitnarin N. Alcohol use and problem drinking among women firefighters. Womens Health Issues. (2017) 27:632–8. doi: 10.1016/j.whi.2017.07.003
25. Hollerbach BS, Heinrich KM, Poston WSC, Haddock CK, Kehler AK, Jahnke SA. Current female firefighters' perceptions, attitudes, and experiences with injury. Int Fire Serv J Leadersh Manag. (2017) 11:41–7.
26. Young Song J, Kim M-G, Ahn Y-S. Injury-related hospital admission of female firefighters in South Korea. Int J Occup Saf Ergon. (2019) 25:575–82. doi: 10.1080/10803548.2017.1411666
27. Frost DM, Beach TAC, Crosby I, McGill SM. Firefighter injuries are not just a fireground problem. Work. (2015) 52:835–42. doi: 10.3233/WOR-152111
28. Nazari G, Macdermid JC, Sinden K, D'Amico R. Prevalence of musculoskeletal symptoms among Canadian firefighters. Work. (2020) 67:185–91. doi: 10.3233/WOR-203264
29. Boyle P. Nation's Physician Workforce Evolves: More Women, a Bit Older, Toward Different Specialties. Association of American Medical Colleges (2021). Available online at: https://www.aamc.org/news-insights/nation-s-physician-workforce-evolves-more-women-bit-older-and-toward-different-specialties (accessed August 15, 2021).
Keywords: women's health, firefighters, occupational injuries, risk factors for injury, survey
Citation: Pawer S, Turcotte K, Desapriya E, Zheng A, Purewal A, Wellar A, Kunz K, Garis L, Thomas LS and Pike I (2022) Female Firefighter Work-Related Injuries in the United States and Canada: An Overview of Survey Responses. Front. Public Health 10:861762. doi: 10.3389/fpubh.2022.861762
Received: 25 January 2022; Accepted: 29 March 2022;
Published: 09 May 2022.
Edited by:
Francesco Chirico, Catholic University of the Sacred Heart, ItalyReviewed by:
Luana C. Main, Deakin University, AustraliaChristopher Keith Haddock, National Development and Research Institutes, United States
Copyright © 2022 Pawer, Turcotte, Desapriya, Zheng, Purewal, Wellar, Kunz, Garis, Thomas and Pike. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Samantha Pawer, c2FtYW50aGEucGF3ZXJAYmNjaHIuY2E=