 Rafael A. Bernardes
Rafael A. Bernardes Filipa Ventura
Filipa Ventura Hugo Neves
Hugo Neves Maria Isabel Fernandes
Maria Isabel Fernandes Pedro Sousa
Pedro Sousa
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Public Health , 20 June 2022
Sec. Digital Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.861621
This article is part of the Research Topic mHealth Tools for Patient Empowerment and Chronic Disease Management View all 20 articles
Parkinson's disease (PD) is the second most common neurodegenerative disease, significantly increasing in the last three decades. Worldwide, seven to ten million people are affected by PD. In people living with PD, freezing of gait (FoG) significantly impacts activities of daily living, potentially leading to falls, injuries, and loss of autonomy. FoG prevalence rates vary widely, reaching at least 50% of patients with PD. Current therapeutic options have limited effectiveness, and their complement with innovative technology-based solutions in the real world is demanded to enhance daily functioning for people living with PD. This article provides a narrative review of current technological developments for people living with PD and, derived from that evidence, presents a perspective on integrating wearable technology and IoT to support telemonitoring and self-management of people living with PD in their daily living environment. Complementing current therapeutic options with technology-based solutions in PD patients' real-world environment is crucial to enhancing the quality of life of people living with PD. In that way, wearable technology and IoT might constitute resources of excellence in seamless monitoring and self-management in people's home environments.
Parkinson's disease (PD) is a neurological disorder with evolving layers of complexity. It has long been characterized by the classical motor features of Parkinsonism associated with Lewy bodies and the loss of dopaminergic neurons in the substantia nigra (1). The parkinsonian symptoms include bradykinesia, muscular rigidity, rest tremor, and postural and gait impairment (2).
In Europe, the estimated prevalence of PD is 1.0% in people with 60 or more years and 3.0% in people older than 80 years, with prevalence rates estimated between 65 and 12.500 per 100.000 and incidence between 5 and 346 per 100.000 person-years (3).
Regarding the global burden of PD, Klietz et al. (3) found a mild increase in caregiver burden in 1 year, highlighting that it is time-consuming and a risk factor for developing depressive symptoms. Economically, PD also has a significant impact worldwide. Yang et al. (4) note a significant economic burden of PD in the United States, with direct medical costs of $25.4 billion and $26.5 billion in indirect and non-medical expenses.
Clinically, a consensus on the classification of PD subtypes has not yet been established. Still, empirical observations suggest two significant subtypes: tremor-dominant PD (with a relative absence of other motor symptoms) and non-tremor-dominant PD (which includes phenotypes described as akinetic-rigid syndrome postural instability gait disorder). People living with PD typically present at least one of four major motor symptoms: Bradykinesia or hypokinesia, resting tremor, rigidity, and postural instability (5). Non-motor symptoms include psychiatric disorders (e.g., hallucinations and delusions, mood disorder), cardiovascular disorders (e.g., orthostatic hypertension, fatigue), neurocognitive disorders, and visual disorders.
Figure 1 summarizes the main signs and symptoms related to PD. The classic motor symptoms are frequently mentioned by authors (6). PD can also be evidenced by non-motor symptoms, which include psychiatric disorders (e.g., hallucinations and delusions, mood disorder), cardiovascular disorders (e.g., orthostatic hypertension, fatigue), neurocognitive disorders, attention deficit, sexual dysfunction, visual disorders, among others (7, 8). However, a combination of these symptoms poses a more significant impact on the person's quality of life with PD. As for diagnostic purposes, Morgan et al. (9) highlight that diagnostic criteria should also include asymmetry and cogwheel rigidity. Other advances regarding the diagnostic of PD have been observed, with Alpha-synuclein oligomers and small nerve fiber pathology in the skin as potential biomarkers, as well as analysis of presynaptic dopaminergic terminals and the severity of the putamen involvement through 99mTc-TRODAT-1 SPECT Imaging, presenting as potential diagnostic markers of PD (10, 11).
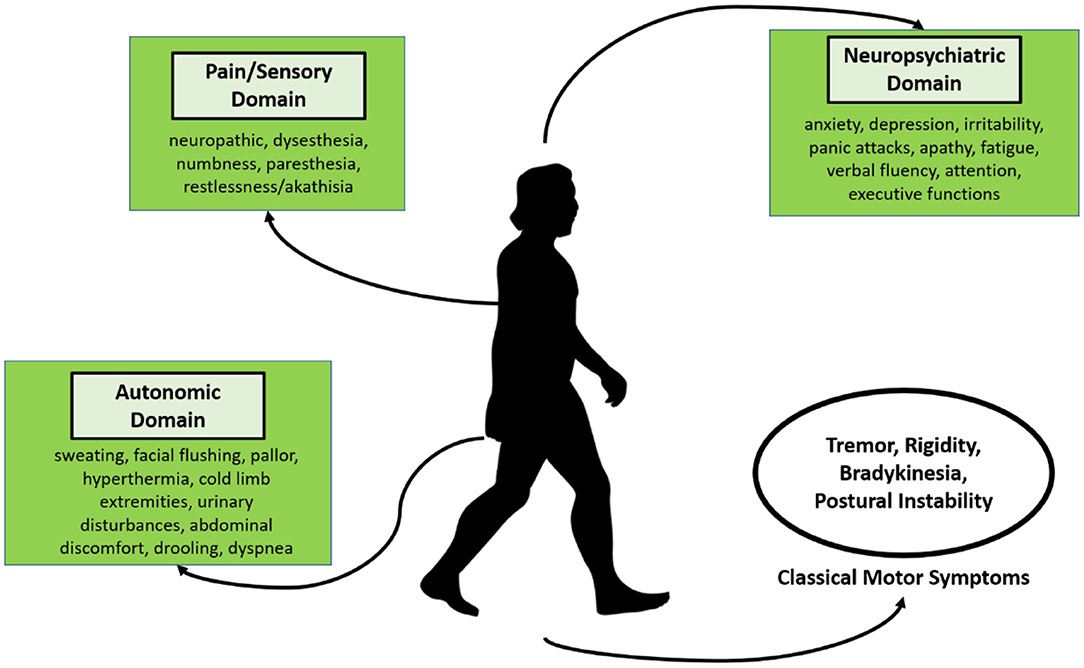
Figure 1. Clinical presentation of PD, according to the motor and non-motor signs and symptoms.
Motor and non-motor signs and symptoms are usually treated using doses of carbidopa/levodopa, depending on the disease's stage. Pharmacological treatment is an important strategy to manage chronic symptoms and increase independence at an initial stage. Yet, several non-pharmacological interventions are available. For example, Church (6) mentioned a technological device, i.e., the red-light-helmet, which uses Light-emitting diodes (LEDs) to alleviate motor symptoms. Morgan et al. (9) state that deep brain stimulation (DBS) is the most effective treatment for motor symptoms. Exercise and neurorehabilitation are increasingly reported as essential measures to fight against motor symptoms. Isernia et al. (12), following the discussion on motor and non-motor interventions, highlight telerehabilitation's efficacy, including physical and cognitive interventions being delivered at a distance.
The social and psychological issues in PD-affected patients should also be considered and might vary in individual patients. Therapies, such as deep brain stimulation and surgical lesioning, should be explored. Further research should be encouraged to better understand the disease's characteristics and etiology. Future scientific research involving Parkinson's disease might enlighten our knowledge of disease onset and progression and deliver some added aspects/components to help find more effective therapies to improve patients' quality of life with PD. As for non-motor symptoms, the latest research trends point to the need to better understand the pathophysiology mechanism before developing new therapeutic approaches (13). However, with pharmacology interventions being insufficient for the management of the person with PD, a clear trend toward developing client-centered interventions that personalize care is becoming more noticeable (14).
According to recent studies, Table 1 provides an overall perspective of the most common pharmacologic and non-pharmacologic treatments for motor and non-motor symptoms (6, 9–15).
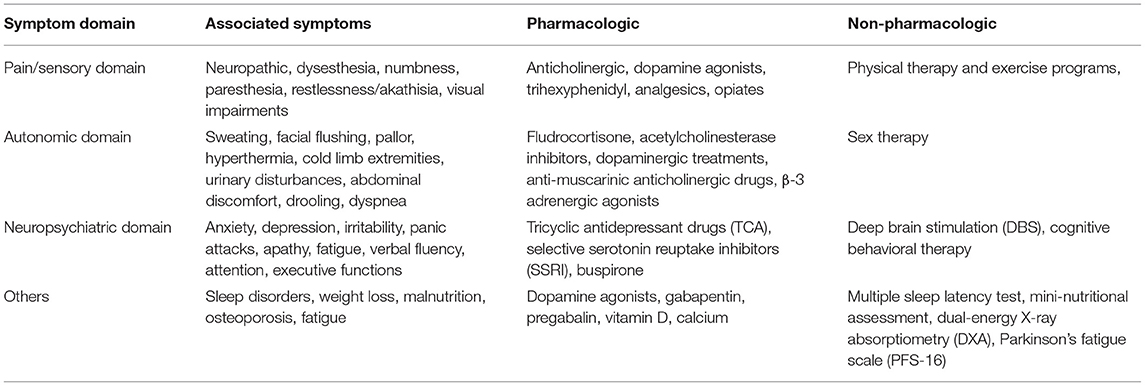
Table 1. Treatments for motor and non-motor symptoms.
As one of the most common and incapacitating PD symptoms that severely compromise patients' quality of life, freezing of gait (FoG) occurs in about 50% of patients with PD (2). Clinically, FoG is characterized by sudden, relatively brief episodes of inability to produce effective forward stepping and typically occur during gait initiation or turning while walking. These gait blocks significantly interfere with daily life, also being on the list of common causes of falls (1). Importantly FoG is now recognized as the leading cause of falling, fracture risk, and activities of daily living disability (16). This risk is compounded because FoG often co-occurs with substantial balance problems and cognitive deficits, mainly frontal executive (17). Associated gait abnormalities affect step calling, step symmetry, and step time consistency before and in-between FoG episodes.
The prevalence of FoG increases with a longer disease duration. It has been reported that 81% of people with PD experienced FoG after a disease duration of 20 years (18). Nieuwboer and Giladi (7) point to four potential mechanisms for FoG events that may explain this time-dependent increase in the prevalence. According to these authors, FoG may occur due to: a motor breakdown associated with the accumulation of various motor deficits (threshold model); an inability to deal with multiple sensory and motor inputs leading to the interruption of locomotion (interference model); behavioral indecision (cognitive model); a cleavage between introductory programming and the intended motor response (decoupling model).
Regardless of the potential model that leads to FoG, the multiple dimensions and systems implicated in this phenomenon highlight FoG management as a significant therapeutic challenge in clinical practice (19). The variety and heterogeneity of existing solutions are a consequence of the complexity of the pathology. However, new and emerging approaches have been developed in recent years, which allow the possibility to enrich and deepen the discussion that has been made in recent times. In this sense, this article intends to contribute to this discussion, highlighting some current gaps and proposing some innovations in the research processes.
The most common form of treatment to manage the motor symptoms of PD is Levodopa (LD). LD is the metabolic precursor to dopamine and is used to replace endogenous dopamine at the striatum (2). The medication cycle between two consecutive intakes is roughly divided into two periods, the ON period in which the LD is adequate and the OFF period in which the influence of the medicine has subsided (2). The development of involuntary movements and the ON/OFF phenomenon, i.e., motor response fluctuations uncorrelated with the expectation from the daily medications intake schedule, can limit mobility and complicate dosing.
Gait deficits and FoG are often resistant to pharmacologic treatment. Therefore, effective non-pharmacologic therapies are needed as an adjunct therapy to relieve symptoms and improve mobility (2). There are various approaches to FoG treatment, one of them being non-pharmacological. Previous work has shown that gait performance in PD can be improved by applying continuous external rhythmic auditory, visual or somatosensory cueing (1). Eskofier et al. (19) noted that the constant, automatic monitoring of sensor-based information on walking ability and mobility is increasingly exploited to support objective assessment for preventive and proactive disease management. The Internet of Health Things (IoHT) is remarkably making its way within healthcare interventions and markets worldwide to answer complex and chronic pathological frameworks, just like PD.
As an initial step to further developing IoHT devices, it is vital to understand how IoT works in a healthcare environment, mainly how it contributes to monitoring external environmental stimuli. Usually, IoT consists of a complex connection between devices, machines, and servers with ample data storage (internet), functioning through a network shared between different stakeholders (20). IoT is an exciting topic inserted in the so-called Industrial Revolution 4.0, which aims to connect things and objects anytime and anywhere.
Following the previous description, we could argue that people with PD are surrounded by several stimuli, internal and external, generating a complex relationship between variables, and making it difficult to perform efficient disease management. This problem is evidenced in Figure 2, with the possible association with Environmental IoT Management.
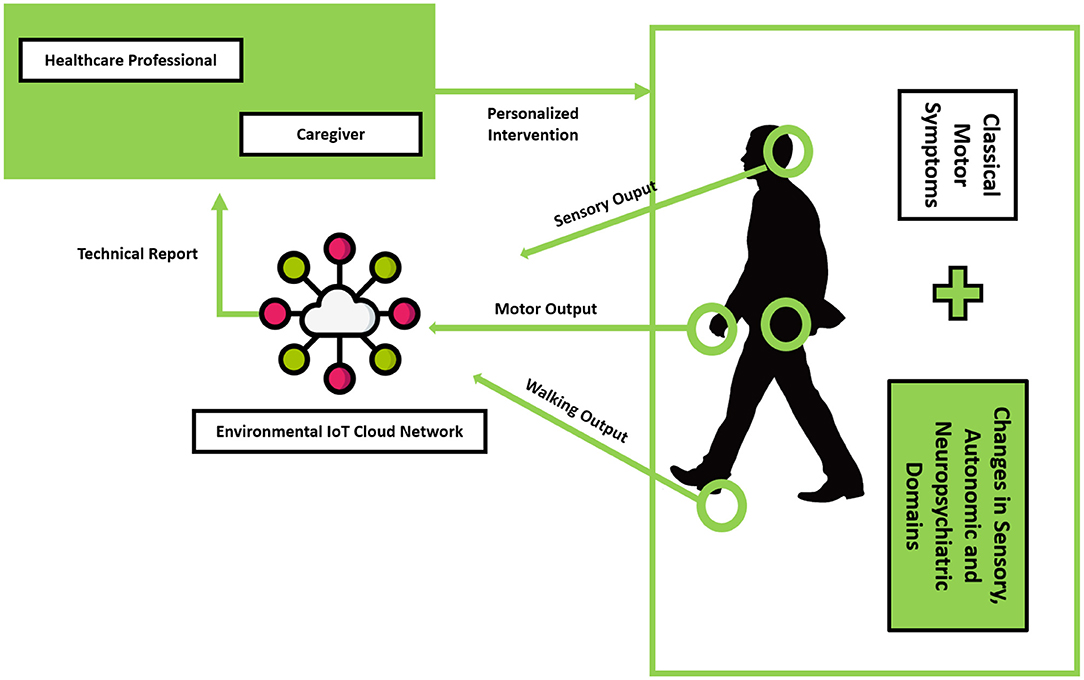
Figure 2. PD management using Environmental IoT Cloud Network.
One of the advantages of Environmental IoT Management is the likely decentralization of the healthcare structure, allowing for a smoother and more efficient interaction between healthcare professionals, caregivers, and patients (21). One of the challenges posed by PD is the chronic and variable nature of signs and symptoms, which are difficult to monitor (21).
A recent systematic review of new assessment methods on PD concludes that there is a particular need for standardized and collaborative studies to confirm the results of preliminary initiatives, assess domains that are currently under-investigated, and better validate the existing and upcoming assessment of PD with technology. Another systematic review (22) has identified and described different wearable insoles with the capacity to recognize patterns, namely stride time, step length, foot clearance, postural sway, gait kinematics, and plantar pressures. Marcante et al. (23) specifically addressed wearable pressure sensors to detect FoG. Some common limitations of these solutions are that their intervention ends in prevention or identification. The ability to associate a personalized intervention by receiving, processing, and sending data with advanced algorithms for health professionals or caregivers is usually not present or requires other devices.
Cueing is a well-established technique that has been shown to improve gait in PD patients in terms of increased walking speed, step length, cadence (total number of steps taken per minute), and reduced number of FoG episodes (24).
Cueing can be defined as using external stimuli which provide temporal (related to time) or spatial (related to space) information to facilitate movement (gait) initiation and continuation. The literature extensively reported three cueing modalities: visual (25), auditory cueing, and somatosensory cueing. The precise mechanism(s) underlying the effectiveness of cueing to ameliorate FoG is unclear. However, previous studies (24) have suggested cueing may compensate for the defective internal rhythm generator of the basal ganglia, consequently affecting the coordination and execution of movement. In this way, PD patients may use auditory, visual, or somatosensory cueing to provide temporal information (i.e., external rhythm) to which movement can be associated. Another hypothesis is that people suffering from PD may use visual cueing to provide spatial information to scale and guide movements, allowing the patient to bypass their defective basal ganglia during gait.
Previous studies (26) have also suggested that cognitive/attentional mechanisms might explain the positive effects of cueing on FoG. Namely, auditory, visual or somatosensory cueing may shift the patient's attention to the task of walking, helping them to consciously think about the next action to be undertaken.
Studies indicate that enhanced proprioceptive information processing could be the mechanism underlying the positive effects of cueing on FoG (27). In this way, the patient may use visual or somatosensory cueing as an artificial means to stimulate the proprioceptive inputs, providing enhanced information on limb position and movement during gait.
Table 2 summarizes current devices and registered patents on cueing technology to treat FoG, describing the main trends on this topic.

Table 2. Current cueing devices and registered patents for FoG treatment.
Although several wearable devices have increased for patients with Parkinson's, few seem to use technologies such as environmental IoT, as described and defined earlier in this article. It is interesting that some projects and devices mentioned in Table 2 use techniques such as health education and learning, namely by training specific exercises. Others have developed stimulation devices with a concrete therapeutic objective. This type of resource—education for health, day-to-day devices—due to its proximity and usability for the end-user, is a competitive advantage among the various devices developed or under development.
Despite this, and given the novelty of environmental IoT, particularly the collection of data, learning of personal patterns, machine learning, and generation of outputs personalized to the context, some projects and devices manage to fulfill the proposed purpose. Still, they would have the capacity to be more effective and satisfactory for people if they integrated all systems discussed so far.
Thus, the reflection proposed here contributes to broadening the discussion on the subject and revealing the importance of making fundamental and clinical investigations interdisciplinary, proposing more cooperation and synergies between the various disciplines of knowledge. In the case of PD, the participation of nurses in the construction of medical projects and devices can be very significant due to their thorough understanding of the person's adaptive capacity to the health-disease situation being experienced. But, it is not only nursing which benefits from cooperation with robotics, electronics, mechanics, medicine, and occupational therapy, among others.
Generally, wearable health assistants aim to reduce the number and length of motor blocks, thus increasing safety while walking (2). Even assuming that this is a core function of the developed devices, Maetzler (36) indicates that, currently, there are no technology-based tools available that: (a) provide valid and accurate parameters of clinically relevant features of PD; (b) provide evidence of an ecologically relevant effect on specific clinical applications; (c) a definition of a target range, wherein the parameter reflects the adequate treatment response; (d) simple implementation allowing for repetitive use.
Within this scope, the development of smart shoes for managing complex health conditions is not new (37). Namely, this technology has already been applied to situations like degenerative spinal cord disabilities (37), frailty syndrome (38), diabetes (39), or even glaucoma (40). In terms of non-pharmacological treatment, previous work has shown that gait performance in PD can be improved by applying continuous external rhythmic auditory, visual or somatosensory cues (1). Accordingly, various behavioral “tricks” were developed by clinicians and patients to overcome freezing events. These tricks include marching to command, stepping over a walking stick or cracks in the floor, walking to music or a beat, and shifting body weight.
Mobility monitoring technologies demand research in sensor-based data acquisition and subsequent analysis to support objective and clinically relevant gait analysis (41). To undergo research in this field, Eskofier et al. (19) have already bulleted the main elements to take into consideration:
1) Remote gait assessment with smart shoes requires a data acquisition system that will collect sensor data;
2) An efficient management of power is essential to reduce the frequency of required charging of devices.
The variety of sensors that are applicable in the context of smart shoes are:
• Relative location and orientation determination using inertial-magnetic measurement units (e.g., accelerometer, gyroscope, magnetometer);
• Absolute location determination using satellite navigation systems (e.g., GPS, Glonass, Galileo);
• Foot plantar pressure determination using various forms of pressure sensors, which provide information regarding how effectively and efficiently individuals control the distribution of the body weight during gait;
• Ambient environmental sensors, such as atmospheric pressure sensors for altitude-dependent activities (e.g., stair climbing), light and sound sensors;
• Two major applications of algorithmic methods are to be used:
• Activity pattern recognition;
• Gait signature derivation for medical diagnostic and treatment contexts.
When we mention “smart shoes,” we are necessarily restricting the discussion to intelligent footwear, but, in a broader sense, to wearable devices which support people with PD during walking. Such technology is not new nor under-studied, mainly because of the importance of FoG treatment, as stated before. The application of wearable walking assistants can include several features and present different treatment goals. For example, Pardoel et al. (42) have employed a conjoint precision analysis of PD motor symptoms using IMU and plantar pressure, successfully identifying Total-FoG (pre-FoG, FoG Transition, and FoG). The authors conclude that the developed system could lead to appropriate prevention of freeze or help to exit the episode. This is an example of an early detection and prevention wearable assistant device.
For PD, it is utterly important, at some point, to estimate gait patterns and recognize important gait events, particularly FoG subtypes. In this sense, Eskofier et al. (19) state that gait event recognition technologies compare the incoming sensor data, preprocessed time-series or computed gait features to reference characteristics of important gait events.
In the last years, there has been an effort to develop and structure new interventions and technological devices to manage and treat FoG, which can be found in the European database CORDIS (cordis.europa.eu).
Main technological advances have been focused on wireless technologies with high-resolution tracking of gait patterns in PD patients, dimensioning time-varying biomechanics related to locomotion, like the project “Decoding impairments of gait and balance from local field potentials in patients with Parkinson's disease (gaitCODE).”
Some projects were interested in developing portable devices for people living with PD, delivering non-invasive neurostimulation signals, as in the Automated Mechanical Peripheral Stimulation for motor rehabilitation in people living with Parkinson's Disease (GONDOLA), which specifically provided physical neurostimulations on specific points in both feet. These neurological stimuli allow for increasing afferent inputs from the peripheral nervous system to the spinal cord, inducing a better functioning of the central pattern generator (the mechanism that regulates movements in the body). Similarly, Industrial Academic Initial Training Network toward the focused treatment of age-related motor symptoms project aims to study specific basal ganglia pathways and stimulate balance and postural control through virtual reality, body-worn movement monitors, therapeutic cues, and individualized training.
Portable and wearable devices seem to be the most common strategy to address FoG, particularly when it is necessary to monitor related motor symptoms in real-time, to support clinical decisions. This is the case of the project Unobtrusive, Continuous and Quantitative Assessment of Parkinson's disease: Hard Evidence for Optimal Disease Management with Information Technologies (Stat-On TM, Park-IT), which developed a small wearable device to continuously monitor movement patterns, being total autonomous and comfortably worn in patient's waist. An exciting and noteworthy addition is the possibility to transfer the motor assessment data to an external mobile device, which then, through machine learning, provides an identification of specific PD symptoms.
Treatment-related projects have also been developed, like a Closed-loop system for personalized and at-home rehabilitation of people with Parkinson's Disease (CuPiD), designed to meet optimal rehabilitation of PD patients with personalized training at home. It's based on an ICT-enabled solution, with a tailored solution to target mobility, cognitive function, and debilitating symptoms like FoG.
The way has been drawn to reach a more person-oriented treatment, with the ultimate goal of achieving autonomy and independence. This is the project's logic PROPHETIC: An innovative personal Healthcare Service for holistic remote management and treatment of Parkinson's patients, which exploits miniature information systems to manage the disease, with remote and continuous monitorization of patients and sharing management plan data between caregivers and health professionals. This project, similarly to others, applied virtual reality to enhance treatment with gamification features at home.
Other projects, like the one developed by Kinetikos or TecaPark, in addition to presenting the features of the previous projects, include a more subjective assessment with a biopsychosocial dimension and address quality of life as part of the treatment of FoG.
With IoT and the increase in the ability to computationally collect and process data, devices anchored in this technology will quickly become part of our daily living activities. Thus, it is no surprise that most client-centered devices developed a focus on wearable technology. However, this aspect adds a layer of complexity, as questions of comfort, usability, and aesthetics need to be considered.
With this shift to a self-care paradigm, where the relationship between client and healthcare provider will change, the key to developing future viable solutions will imply including dimensions that were not previously considered when using technology. The presence of wearable devices in patients experiencing FoG will most certainly become a reality, with the client as an active part in demanding this technology and choosing which option fits their personal preferences (43). Among the wearable devices that will become mandatory for people with PD experiencing FoG, smart shoes will most certainly be one, if not the most present technology (44).
The potential associated with smart shoes is immense. Not only will PD patients be able to understand what happens before and during the FoG event, but the data collected throughout the whole process will help researchers and healthcare providers develop personalized interventions and new technologies, like domotics, that will significantly decrease the burden associated with FoG (45).
Smart shoes will most certainly be data-collection-based. The potential to help the patient to focus the attention on the task of walking by restoring internal cueing and internal driving is a dimension that can be associated with a machine-learning algorithm with the potential to significantly reduce the risks associated with the FoG (46).
These devices will further assist healthcare providers and researchers in understanding how the real-world environment influences controlled interventions. Until now, clinical research has been associated with limited control of variables. Data collected during clinical trials represent only part of how people deal with their health conditions and how the intervention affects (positively or negatively) the client's quality of life.
Data collection will become more complex, with IoHT allowing machine-learning algorithms to help the client understand what is happening in real-time (47, 48). They will also help address FoG causes and consequences by preventing them through the individualized establishment of cueing strategies and alert systems that will allow a quicker and better response to a fall, namely through an intelligent environment (49).
Future trends portray the need to engage all the actors in this phenomenon: the FoG. Understanding how wearable technology can be part of this new self-care paradigm will significantly impact how patients deal with this condition. Thus, assuring citizen engagement in developing IoHT strategies will be a requirement for every device, with new variables being integrated into how these are built (50).
FoG is a complex episodic motor symptom that significantly affects the quality of life and activities of daily living. Despite the existing pharmacological treatments to alleviate PD symptoms, namely tremors and bradykinesia, there are limited resources to treat FoG. Accordingly, technology has been consecutively applied, concomitant with conventional approaches, namely external cueing, either visual, auditory, or somatosensory.
This perspective successfully presented and described current therapeutic options in PD, eliciting their advantages and limitations. One of the major conclusions is that complementing the standard treatment with innovative technology-based solutions is helpful for enhancing the daily life of people with PD. Wearable technology and IoT might constitute important assets for monitoring and self-management in homecare. Existent solutions still need further development to address the need to deliver a personalized intervention by receiving, processing, and sending data with advanced algorithms for health professionals or caregivers.
Regarding cueing devices, one of the most recent and modern approaches is wearable technology embedded in footwear, which increases neurological stimuli in PD patients and thereby their motor functions. Smart shoes have been developed for many pathologic signs and symptoms and are currently being tested for PD.
State of the art aims to apply IoHT and virtual reality to monitor patients and increase their autonomy, also propelling caregiver abilities through personalized programs. Future trends seem to be reaching a person-centered approach, focusing on comfort, usability, and aesthetics, namely in footwear development.
Some limitations have been identified: the unsystematic review might have implied the loss of previous important works on the topic; the focus on wearable shoes provided a more narrowed review, thus contributing to less enriched work.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
RB and PS led the design of the manuscript. HN and FV assisted in drafting the manuscript. MF provided advice on key study issues. All authors contributed equally to the narrative literature review and evidence synthesis. All authors contributed important intellectual content to the manuscript and approved the final version for publication.
This work was funded by National Funds through the FCT—Foundation for Science and Technology, I.P., within the scope of the project Refª. UIDB/00742/2020. The work of FV was funded by the Portuguese Foundation for Science and Technology (FCT), CEECINST/00103/2018. The funder had no role in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to acknowledge the Health Sciences Research Unit: Nursing (UICISA:E) of the Nursing School of Coimbra (ESEnfC).
1. Bächlin M, Plotnik M, Roggen D, Maidan I, Hausdorff JM, Giladi N, et al. Wearable assistant for Parkinson's disease patients with the freezing of gait symptom. IEEE Trans Inf Technol Biomed. (2010) 14:436–46. doi: 10.1109/TITB.2009.2036165
2. Bächlin M, Plotnik M, Roggen D, Giladi N, Hausdorff JM, Tröster G, et al. Wearable system to assist walking of Parkinson's disease patients. Methods Inf Med. (2010) 49:88–95. doi: 10.3414/ME09-02-0003
3. Klietz M, von Eichel H, Schnur T, Staege S, Höglinger GU, Wegner F, et al. One year trajectory of caregiver burden in Parkinson's disease and analysis of gender-specific aspects. Brain Sci. (2021) 11:295. doi: 10.3390/brainsci11030295
4. Yang W, Hamilton JL, Kopil C, Beck JC, Tanner CM, Albin RL, et al. Current and projected future economic burden of Parkinson's disease in the US. NPJ Parkinsons Dis. (2020) 6:15. doi: 10.1038/s41531-020-0117-1
5. Buated W, Sriyudthsak M, Sribunruangrit N, Bhidayasiri R. A low-cost intervention for improving gait in Parkinson's disease patients: a cane providing visual cues. Eur Geriatr Med. (2012) 3:126–30. doi: 10.1016/j.eurger.2012.01.006
6. Church FC. Treatment options for motor and non-motor symptoms of Parkinson's disease. Biomolecules. (2021) 11:612. doi: 10.3390/biom11040612
7. Kuresan H, Samiappan D, Ghosh S, Gupta AS. Early diagnosis of Parkinson's disease based on non-motor symptoms: a descriptive and factor analysis. J Ambient Intell Humaniz Comput. (2021). doi: 10.1007/s12652-021-02944-0
8. Berganzo K, Tijero B, González-Eizaguirre A, Somme J, Lezcano E, Gabilondo I, et al. Motor and non-motor symptoms of Parkinson's disease and their impact on quality of life on different clinical subgroups. Neurol. (2016) 31:589–91. doi: 10.1016/j.nrleng.2014.10.016
9. Morgan JC, Fox SH. Treating the motor symptoms of Parkinson disease. Continuum. (2016) 22:1064–85. doi: 10.1212/CON.0000000000000355
10. Vacchi E, Senese C, Chiaro G, DIsanto G, Pinton S, Morandi S, et al. Alpha-synuclein oligomers and small nerve fiber pathology in skin are potential biomarkers of Parkinson's disease. NPJ Parkinsons Dis. (2021) 7:119. doi: 10.1038/s41531-021-00262-y
11. Sasannezhad P, Juibary AG, Sadri K, Sadeghi R, Sabour M, Kakhki VRD, et al. 99mTc-TRODAT-1 SPECT imaging in early and late onset Parkinson's disease. Asia Ocean J Nucl Med Biol. (2017) 5:114–9. doi: 10.22038/aojnmb.2017.8844
12. Isernia S, Tella SD, Pagliari C, Jonsdottir J, Castiglioni C, Gindri P, et al. Effects of an innovative telerehabilitation intervention for people with Parkinson's disease on quality of life, motor and non-motor abilities. Front Neurol. (2020) 11:846. doi: 10.3389/fneur.2020.00846
13. Tibar H, Bayad KE, Bouhouche A, Haddou EHAB, Benomar A, Yahyaoui M, et al. Non-motor symptoms of Parkinson's disease and their impact on quality of life in a cohort of Moroccan patients. Front Neurol. (2018) 9:170. doi: 10.3389/fneur.2018.00170
14. Jagadeesan AJ, Murugesan R, Devi SV, Meera M, Madhumala G, Padmaja MV, et al. Current trends in etiology, prognosis and therapeutic aspects of Parkinson's disease: a review. Acta Biomed. (2017) 88:249–62. doi: 10.23750/abm.v88i3.6063
15. Gupta S, Shukla S. Non-motor symptoms in Parkinson's disease: opening new avenues in treatment. Curr Opin Behav Sci. (2021) 2:100049. doi: 10.1016/j.crbeha.2021.100049
16. Nonnekes J, Snijders AH, Nutt JG, Deuschl G, Giladi N, Bloem BR. Freezing of gait: a practical approach to management. Lancet Neurol. (2015) 14:768–78. doi: 10.1016/S1474-4422(15)00041-1
17. Gan J, Liu W, Cao X, Xie A, Li W, Yuan C, et al. Prevalence and clinical features of FOG in Chinese PD patients, a multicenter and cross-sectional clinical study. Front Neurol. (2021) 12:568841. doi: 10.3389/fneur.2021.568841
18. Nieuwboer A, Giladi N. Characterizing freezing of gait in Parkinson's disease: models of an episodic phenomenon. Mov Disord. (2013) 28:1509–19. doi: 10.1002/mds.25683
19. Eskofier BM, Lee SI, Baron M, Simon A, Martindale CF, Gabner H, et al. An overview of smart shoes in the internet of health things: gait and mobility assessment in health promotion and disease monitoring. App Sci. (2017) 7:986. doi: 10.3390/app7100986
20. Sunny AI, Zhao A, Li L, Sakiliba SK. Low-cost IoT-based sensor system: a case study on harsh environmental monitoring. Sensors. (2021) 21:214. doi: 10.3390/s21010214
21. Pasluosta CF, Gassner H, Winkler J, Klucken J, Eskofier BM. An emerging era in the management of Parkinson's disease: wearable technologies and the internet of things. IEEE J Biomed Health Inform. (2015) 19:1873–81. doi: 10.1109/JBHI.2015.2461555
22. Channa A, Popescu N, Ciobanu V. Wearable solutions for patients with Parkinson's disease and neurocognitive disorders: a systematic review. Sensors. (2020) 20:2713. doi: 10.3390/s20092713
23. Marcante A, Marco RD, Gentile G, Pellicano C, Assogna F, Pontieri 0046E, et al. Foot pressure wearable sensors for freezing of gait detection in Parkinson's disease. Sensors. (2021) 21:128. doi: 10.3390/s21010128
24. Caudron S, Guerraz M, Eusebio A, Gros JP, Azulay JP, Vaugoyeau M. Evaluation of a visual biofeedback on the postural control in Parkinson's disease. Neurophysiol Clin. (2014) 44:77–86. doi: 10.1016/j.neucli.2013.10.134
25. Young WR, Shreve L, Quinn EJ, Craig C, Bronte-Stewart H. Auditory cueing in Parkinson's patients with freezing of gait. What matters most: action-relevance or cue-continuity? Neuropsychologia. (2016) 87:54–62. doi: 10.1016/j.neuropsychologia.2016.04.034
26. Bunting-Perry L, Spindler M, Robinson KM, Noorigian J, Cianci HJ, Duda JE. Laser light visual cueing for freezing of gait in Parkinson disease: a pilot study with male participants. J Rehabil Res Dev. (2013) 50:223–30. doi: 10.1682/JRRD.2011.12.0255
27. Bekkers EM, Dockx K, Heremans E, et al. The contribution of proprioceptive information to postural control in elderly and patients with Parkinson's disease with a history of falls. Front Hum Neurosci. (2014) 8:939. doi: 10.3389/fnhum.2014.00939
28. Gerpen V. System and Method for Alleviating Freezing Gait and Gait Hypokinesia in Users with Extrapyramidal Disorders (2015).
29. McCandless PJ, Evans BJ, Janssen J, Selfe J, Churchill A, Richards J. Effect of three cueing devices for people with Parkinson's disease with gait initiation difficulties. Gait Posture. (2016) 44:7–11. doi: 10.1016/j.gaitpost.2015.11.006
30. Mcloul RF, Oberman C. Movement Initation Device Used in Parkinson's Disease and Other Disorders Which Affect Muscle Control (2002).
31. Shim Y, Lee J, Park Y, Ahn S, Hyung S. Walking Assistance Method and Apparatus. World International Property Organization (WIPO).
32. Akay M. Intelligent Wearable Monitor Systems and Methods. Munich: European Patent Office (EPO). (2005).
33. Chun CM, Kim CH, Choi JH, Kim SJ. Wearable Vibratory Stimulation Device and Operational Protocol Thereof. World International Property Organization (WIPO). (2014).
35. Maetzler W, Klucken J, Horne M. A clinical view on the development of technology-based tools in managing Parkinson's disease. Mov Disord. (2016) 31:1263–71. doi: 10.1002/mds.26673
36. Lee SI, Park E, Huang A, Mortazavi B, Garst JH, Jahanforouz N, et al. Objectively quantifying walking ability in degenerative spinal disorder patients using sensor equipped smart shoes. Med Eng Phys. (2016) 38:442–9. doi: 10.1016/j.medengphy.2016.02.004
37. Schwenk M, Mohler J, Wendel C, D'Huyvetter K, Fain M, Taylor-Piliae R, et al. Wearable sensor-based in-home assessment of gait, balance, and physical activity for discrimination of frailty status: baseline results of the Arizona frailty cohort study. Gerontology. (2015) 61:258–67. doi: 10.1159/000369095
38. Perrier A, Vuillerme N, Luboz V, Bucki M, Cannard F, Diot B, et al. Smart diabetic socks: embedded device for diabetic foot prevention. IRBM. (2014) 35:72–6. doi: 10.1016/j.irbm.2014.02.004
39. Ma Y, Amini N, Chasemzadeh H. Wearable sensors for gait pattern examination in glaucoma patients. Microprocess Microsyst. (2016) 46:67–74. doi: 10.1016/j.micpro.2016.07.001
40. Benz HL, Caldwell B, Ruiz JP, Saha A, Ho M, Christopher S, et al. Patient-centered Parkinson's disease. MDM Policy Pract. (2021) 6:23814683211021380. doi: 10.1177/23814683211021380
41. Sánchez-Ferro Á, Elshehabi M, Godinho C, Salkovic D, Hobert MA, Domingos J, et al. New methods for the assessment of Parkinson's disease (2005 to 2015): a systematic review. Mov Disord. (2016) 31:1283–92. doi: 10.1002/mds.26723
42. Pardoel S, Shalin G, Nantel J, Lemaire ED, Kofman J. Early detection of freezing of gait during walking using inertial measurement unit and plantar pressure distribution DATA. Sensors. (2021) 21:2246. doi: 10.3390/s21062246
43. Reina-Bueno M, Calvo-Lobo C, López-López D, Palomo-López P, Becerro-de-Bengoa-Vallejo R, et al. Effect of foot orthoses and shoes in Parkinson's disease patients: a PRISMA systematic review. J Pers Med. (2021) 11:1136. doi: 10.3390/jpm11111136
44. Simonet C, Noyce AJ. Domotics, smart homes, and Parkinson's disease. J Parkinsons Dis. (2021) 11:S55–63. doi: 10.3233/JPD-202398
45. Muthukrishnan N, Abbas JJ, Shill HA, Krishnamurthi N. Cueing paradigms to improve gait and posture in Parkinson's disease: a narrative review. Sensors. (2019) 19:5468. doi: 10.3390/s19245468
46. Gómez J, Oviedo B, Zhuma E. Patient monitoring system based on internet of things. Proc Comp Sci. (2016) 83:90–7. doi: 10.1016/j.procs.2016.04.103
47. Chiuchisan I, Costin H-N, Geman O. Adopting the internet of things technologies in health care systems. IEEE. (2014) 532–5. doi: 10.1109/ICEPE.2014.6969965
48. Uddin MS, Alam JB, Banu S. Real time patient monitoring system based on internet of things. IEEE. (2017) 2017:516–21. doi: 10.1109/ICAEE.2017.8255410
49. Sweeney D, Quinlan LR, Browne P, Richardson M, Meskell P, ÓLaighin G, et al. Technological review of wearable cueing devices addressing freezing of gait in Parkinson's disease. Sensors. (2019) 19:1277. doi: 10.3390/s19061277
Keywords: Parkinson's disease, freezing of gait, internet of things, self-management, wearables
Citation: Bernardes RA, Ventura F, Neves H, Fernandes MI and Sousa P (2022) Wearable Walking Assistant for Freezing of Gait With Environmental IoT Monitoring: A Contribution to the Discussion. Front. Public Health 10:861621. doi: 10.3389/fpubh.2022.861621
Received: 24 January 2022; Accepted: 30 May 2022;
Published: 20 June 2022.
Edited by:
Luis Augusto Teixeira, University of São Paulo, BrazilReviewed by:
Samiappan Dhanalakshmi, SRM Institute of Science and Technology, IndiaCopyright © 2022 Bernardes, Ventura, Neves, Fernandes and Sousa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rafael A. Bernardes, cmFmYWVsYWx2ZXNiZXJuYXJkZXNAZXNlbmZjLnB0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.