 Huanhuan Jia†
Huanhuan Jia† Xihe Yu
Xihe Yu- School of Public Health, Jilin University, Changchun, China
Objectives: This study aims to evaluate the direct effects of work stress, health status and presenteeism on task performance, and further explore the mediating effects of health status and presenteeism, hoping to provide theoretical basis for improving the performance of medical staff.
Methods: A cross-sectional study was conducted among medical staff in Jilin Province, Northeast China. The Challenge and Hindrance-Related Self-Reported Stress scale, Short Form-8 Health Survey scale, Stanford Presenteeism Scale and Task Performance Scale were adopted to assess the work stress, health status, presenteeism and task performance of medical staff.
Results: A total of 4,347 questionnaires were distributed among medical staff, and 4261 were valid, for an effective rate of 98.02%. The mean scores for work stress, health status, presenteeism and task performance were 2.05 ± 0.84, 4.18 ± 0.68, 2.15 ± 0.79 and 4.49 ± 0.64, respectively. The ANOVA results showed that there were significant differences in the task performance scores between different genders, ages, marital statuses, professional titles, departments and work years (P < 0.05). Work stress (β = −0.136, P < 0.001) and presenteeism (β = −0.171, P < 0.001) were negative predictors of task performance. Health status (β = 0.10; P < 0.001) was positive predictor of task performance. Health status (β = −0.070; P < −0.001) and presenteeism (β = −0.064; P < 0.001) mediated the relationship between work stress and task performance (P < 0.001). Presenteeism mediated the relationship between health status and task performance (β = 0.07; P < 0.001).
Conclusion: Work stress and presenteeism had significant negative impact on the task performance of medical staff; health status had a significant positive effect on task performance. Meanwhile, health status and presenteeism played a mediating role in the relationship between work stress and task performance, and presenteeism played a mediating role in the relationship between health status and task performance. Reasonable assignment of tasks can reduce the work stress, but to improve the performance of medical staff, we should pay more attention on improving health, such as making health-related safeguard measures, raising awareness, building a platform, etc.
Introduction
Since the end of 2019, there have been outbreaks of infectious diseases caused by coronavirus disease 2019 (COVID-19) worldwide. COVID-19 was declared a pandemic by the World Health Organization in January 2020 and listed as a public health emergency and a matter of international concern (1, 2). Emerging and re-emerging pathogens are global challenges to public health (3). Medical staff, as the backbone of COVID-19 prevention and control, has been playing a leading role in controlling the epidemic through the unremitting struggle against the epidemic (4). According to a survey from Europe, the COVID-19 pandemic affects the work of employees on every continent (5). Numerous studies have found that the COVID-19 pandemic is placing increasing demands on health care workers, it caused the severe employment situation, long or irregular working hours and shifts, and excessive work stress which were putting the task performance of medical staff and its health, society, and economy in a dangerous environment (6–8). These problems have seriously affected the attention, perception and decision-making ability of medical staff, not only reducing enthusiasm and initiative but also lowering the overall quality of medical staff. These consequences hinder the struggle against the virus, and the development of society.
The evaluation of the performance of health professionals has been the focus of scientific research in recent decades, and the efficient work of health technicians was the basis for improving the quality of health services (9). There have been extensive studies of task performance around the world, and the research factors mainly included work stress, job satisfaction, conflict, attendance, leadership relationships, health and so on (10–13). Studies indicated that more stressors arose during pandemics, and that stress itself was associated with the development of various diseases (14, 15). At the same time, health problems have become more prominent during the epidemic. In addition, healthcare workers faced more severe challenges during the pandemic. The heavy workload forced them to stick to their posts, and their attendance significantly improved, so we speculated that presenteeism was also more serious. While saving the lives of others, medical staff were more likely to neglect their own health, and the presenteeism rate of medical staff was much higher than that of other professions. In the context of the pandemic and the growing demand for medical services, medical staff are facing increasing work pressure, with a series of physical and mental health problems, and the possibility of going to work sick is increasing. Therefore, in combination with literature and epidemiological background, we selected these variables related to performance: work stress, health status, and presenteeism, to explore their direct and indirect effects on performance in multipath. Task performance refers to the employee's output in terms of goals and responsibilities related to the job. To some extent, it can more directly reflect an employee's work ability and performance. Task performance is considered to be one of the key indicators of organizational performance, contributing to an organization's productivity, competitiveness and social and psychological work environment (9). Therefore, this study adopted task performance as an indicator to measure the performance of medical staff.
The following subsections describe the hypotheses considered in this study.
Hypothesis Development
Work Stress
Work stress refers to the mismatch between work requirements and individuals under the interaction of work situations and individual characteristics, affecting individuals' physiology, psychology and behavior (16). COVID-19 has disrupted everyone's daily lives, making it challenging to maintain boundaries between work and non-work, and research by Kumar et al. (14) pointed to the many stressors that emerge during a pandemic that can disrupt people's work and affect their performance. Research by Bhagat (17) showed that people are more likely to experience distress due to stressful life events, which can lead to disruptions in work and thus affect their task performance. Medical staff faces high occupational pressure caused by heavy workloads, extended working hours and so on. Such high occupational pressure seriously affects the physical and mental health of medical staff, leads to an increase in the probability of work error, and seriously affects work efficiency (18).
Based on the above discussion, the following hypothesis was proposed.
Hypothesis 1 (H1): Work stress has a significant, negative effect on task performance.
Health Status
The World Health Organization defines health as a good state of physical, mental and social wellbeing (19). Health is the basic condition for the normal work and lives of professional people. Health problems not only people's own lives, but they also have a direct or indirect impact on the labor productivity of employers, increasing the economic burden of the workplace, namely the loss of productivity caused by health (20). Ford et al.'s study (21) showed a significant correlation between physical and mental health and task performance. Baldwin et al.'s study (22) showed that the health status of medical staff directly affects the quality of medical work. At the same time, researches have shown that negative emotions associated with work stress may worsen employees' physical and mental health, and that work stress was a key factor in health care workers' physical and mental health during the pandemic (23, 24).
Based on the above discussion, the following research hypotheses were proposed:
Hypothesis 2 (H2): Health status has a significant positive effect on task performance.
Hypothesis 3 (H3): Health status mediates the relationship between work stress and task performance.
Presenteeism
Presenteeism refers to “the phenomenon of people who normally need rest and absence from work going to work despite poor health” (25). Studies have shown that presenteeism is important because of its negative impact on individual health and organizational productivity (26, 27). Health productivity loss includes sickness absence and presenteeism (28). Presenteeism leads to much higher productivity loss than sickness absenteeism and is the main mode of working inefficiency among professional people (29). Studies in the USA have shown that presenteeism results in more lost productivity than sick leave (30). Employees who are sick tend to make more mistakes and have lower levels of performance and productivity (31). The study also found that the incidence of presenteeism of medical staff was significantly higher than that of other professions: the presenteeism of medical staff was ~3–4 times higher than that of other occupational groups, and the occurrence of presenteeism of medical staff is common (25, 32). A literature review showed that health status is associated with presenteeism and lost productivity (27). Other studies have shown that work stress can lead to presenteeism (33). The Health and Safety Executive (2015) reported that stress-related illnesses accounted for 35% of all health-related illnesses and 43% of presenteeism in the UK (34).
Based on the above discussion, the following research hypotheses are proposed:
Hypothesis 4 (H4): Presenteeism has a significant negative effect on task performance.
Hypothesis 5 (H5): Presenteeism mediates the relationship between health status and task performance.
Hypothesis 6 (H6): Presenteeism mediates the relationship between work stress and task performance.
Based on the above discussion, a hypothetical path was proposed as shown in Figure 1.
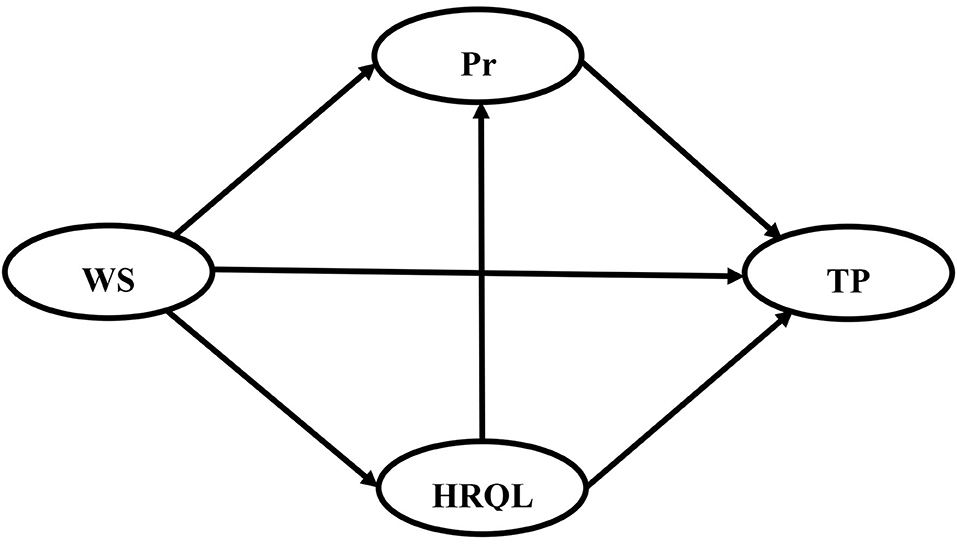
Figure 1. The hypothetical structural equation model. TP, task performance; WS, work stress; HRQL, health-related quality of life; Pr, presenteeism.
Methods
Study Design and Participants
To validate the hypotheses, a cross-sectional survey was conducted in January 2020 in Jilin Province, Northeast China. Medical staff members in public hospitals were selected by stratified random sampling as the subjects of the study. In this process, all areas of Jilin Province were divided into cities and counties, and hospitals were also divided into urban public hospitals and county-level public hospitals. Due to the high clustering of urban public hospitals, these hospitals were stratified by region, type and level and randomly selected at a rate of 1/4. Because of the dispersion of different counties, city hospitals and traditional Chinese medicine hospitals were selected from each county as samples. Finally, a total of 109 hospitals, including 29 urban public hospitals and 80 county-level public hospitals, were selected as sample hospitals. Through quota sampling, 40 medical staff members, including doctors, nurses and medical technicians, were selected from each hospital to be investigated. The questionnaire was administered on site by trained investigators and was recovered on site. Finally, 4,347 questionnaires were distributed, and 4,261 valid questionnaires were collected. The valid response was 98.02%.
The study was approved by the Medical Ethics Committee of the author's institution (No. 2019-12-03). Participants were provided with a complete explanation of the purposes of the study. Participants were informed that the information collected would be used solely for the study and that they could withdraw at any time.
Measures
The measuring instrument was a questionnaire, which was developed by adapting previously validated scales to the context of the study. The questionnaire was divided into two parts. The first part collected demographic characteristics of the respondents, including gender, age, marriage status, education background, professional title, department and working years. The second part measured respondents' task performance, work stress, health status and presenteeism.
Challenge-and Hindrance-Related Self-Reported Stress Measures
Work stress was assessed using the Challenge-and Hindrance-Related Self-Reported Stress Measures (CHSS) developed by Cavanaugh et al. (35). It includes both challenging stress and hindrance stress. Challenge stressors were defined as work-related demands or circumstances that have associated potential gains for individuals despite potential stress. Hindrance stressors were defined as work-related demands or circumstances that tend to constrain or interfere with an individual's work achievements and that do not tend to be associated with the individual's potential gains. There are 11 items on the CHSS, including 6 challenging stressors and 5 hindrance stressors. The items are measured on a 5-point Likert scale ranging from 1 (no pressure) to 5 (extreme stress), and the higher that the score is, the greater that the work stress of the medical staff is. Cavanaugh's research (35) showed that the reliability coefficients of the two subscales were 0.87 and 0.75, and the correlation coefficient was 0.28, indicating that the two scales had good internal consistency and discriminant validity. The CHSS has been widely concerned and applied (36–41). In addition, Chinese scholars have translated it into Chinese and proved its applicability in Chinese professional groups (42). In this study, the Cronbach's alpha was 0.938 and 0.849 for the two subscales, respectively.
Short Form-8 Health Survey
The Short Form-36 (SF-36) Health Survey is the most popular instrument for investigating health-related quality of life (HRQOL) (43), and it contains 36 items in 8 subscales. However, despite its popularity, the length of SF-36 limits its use (43). The SF-8, a shortened version of the SF-36, was derived from the SF-36 and has been preferred by many scholars (44–46). The SF-8 has only 8 questions, including physical functioning, role limitations due to physical health problems, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems, and mental health; the scores range from 1 to 5, with higher scores indicating better performance. The SF-8 has demonstrated acceptable validity and reliability in previous studies (47). At the same time, the SF-8 was translated into Chinese by Lang et al. (43), and a survey of 10,885 individuals in 35 cities in China proved that the SF-8 had good internal consistency reliability and could be used in the Chinese population. The Cronbach's alpha for the SF-8 in this study was 0.916.
Stanford Presenteeism Scale
The Stanford Presenteeism Scale (SPS-6) was adapted to measure the effect of health status on task performance (48). The SPS-6 is not affected by occupation, disease type or characteristics and has been used in many fields (27, 49). Based on a survey of 14,195 people in 8 places, Jiang proved that the SPS-6 has high reliability and validity and can be applied to the study of the Chinese professional population (50). There are 6 items in the SPS-6, each with five options ranging from 1 to 5. On the scale, “At work, I was able to focus on achieving my goals despite my health problem” and “Despite having my health problem, I was able to finish hard tasks in my work” are scored in reverse order. The sum of the six items then produces a total attendance score, and the higher that the score is, the greater that the health impact on work status is. In this study, the Cronbach's alpha for the SPS-6 was 0.756.
Task Performance
The measurement of task performance (TP) was adapted from Williams's (51) and Jessica's (52) performance measurement scales. TP consists of five items, which are measured on a 5-point Likert scale, rated on a scale from 1 (Strongly disagree) to 5 (Strongly agree). The higher that the score is, the better that the employee's performance is. In this study, TP was translated into Chinese through translation and back-translation. Two PhD students each translated the original items and then decided on a draft after discussion. Then, the items were translated back into English to ensure that the Chinese version had the same meaning as the English version. In this study, the Cronbach's alpha for TP was 0.917.
Data Analysis
Descriptive statistics were used to analyze the demographic characteristics of the respondents, as well as the scores for task performance, work stress, health status and presenteeism. In addition, age and working years were collected using continuous variables, whereas in order to reflect the task performance of different groups, we grouped them into groups with a distance of 10 based on previous studies (53, 54). The t tests and one-way analysis of variance (ANOVA) were performed to examine differences in the task performance scores among medical staff members of different genders, ages, marital statuses, educational levels, professional titles, departments, and working years. Pearson's correlation analysis was applied to analyze the correlations between the study variables. Structural equation modeling (SEM) has the characteristics of Confirmatory factor analysis (CFA) and Path analysis (PA), and has incomparable advantages. PA tests the causal relationship between the observed variables, CFA tests the causal relationship between the observed variables and the latent construct, and SEM tests the causality between the observed variables and the latent construal as well as the interior of several latent construal (55). Some scholars proposed that SEM was the sum of CFA, PA and multiple regression analysis (56). Therefore, SEM was adopted to verify the effects of work stress, health status and presenteeism on task performance, and the Maximum Likelihood Estimation was used to estimate the parameters. In addition, the bootstrapping technique was applied to explore the mediating role. The model was assessed by the following indexes (57, 58): (1) the standardized residual mean root (SRMR < 0.01); (2) the root mean square error of approximation (RMSEA ≤ 0.08); (3) the comparative fit index (CFI ≥ 0.90); (4) the Tucker–Lewis index (TLI ≥ 0.90); (5) the incremental fit index (IFI ≥ 0.90) and (6) the non-normed fit index (NFI ≥ 0.90). All of the statistical tests were two sided with the level of significance set at 0.05. SPSS software, version 25.0, and AMOS software, version 23.0 (IBM Corporation, Armonk, NY, USA), were used for the process.
Results
Demographic Characteristics and Task Performance Scores
A total of 4,261 medical staff participated in the survey. In this sample, most of the respondents were female (68.95%) and married (78.85%), with college degrees (58.60%) and with middle or junior titles (68.72%). The medical staff members were aged 37.55 ± 9.11 years old, had worked for 13.73 ± 9.73 years and scored 4.49 ± 0.64 on task performance. Mean scores for task performance differed across the distributions of gender, age, marital status, professional titles, departments and working years. However, there were no differences in the scores among medical staff members with different marital statuses and educational levels. The demographic characteristics and task performance scores are shown in Table 1.

Table 1. Demographic characteristics and task performance of 4,261 participants.
Correlations of Study Variables
Table 2 demonstrates the scores of the study variables. The health status score was 4.18 ± 0.68, and the presenteeism score was 2.15 ± 0.79. The work stress score was 2.05 ± 0.84, in which the challenging stress score was 2.22 ± 0.97 and the hindrance stress score was 1.85 ± 0.84. Health status was negatively correlated with work stress and presenteeism (r = −0.606, P < 0.01; r = −0.503, P < 0.01) and positively correlated with task performance (r = 0.279, P < 0.01). Work stress was positively correlated with presenteeism (r = 0.463, P < 0.01) and negatively correlated with task performance (r = −0.266, P < 0.01). Presenteeism was negatively correlated with task performance (r = −0.161, P < 0.01).
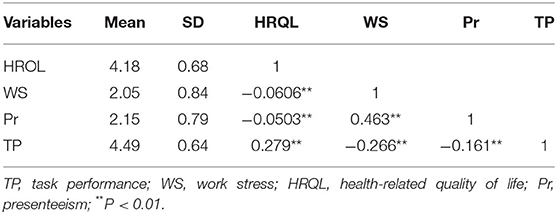
Table 2. Correlations among task performance, work stress, health-related quality of life and presenteeism.
Hypothesis Testing
The t and P values for each path were calculated in AMOS to test the research hypothesis. The results of the structural equation model are presented in Figure 2.
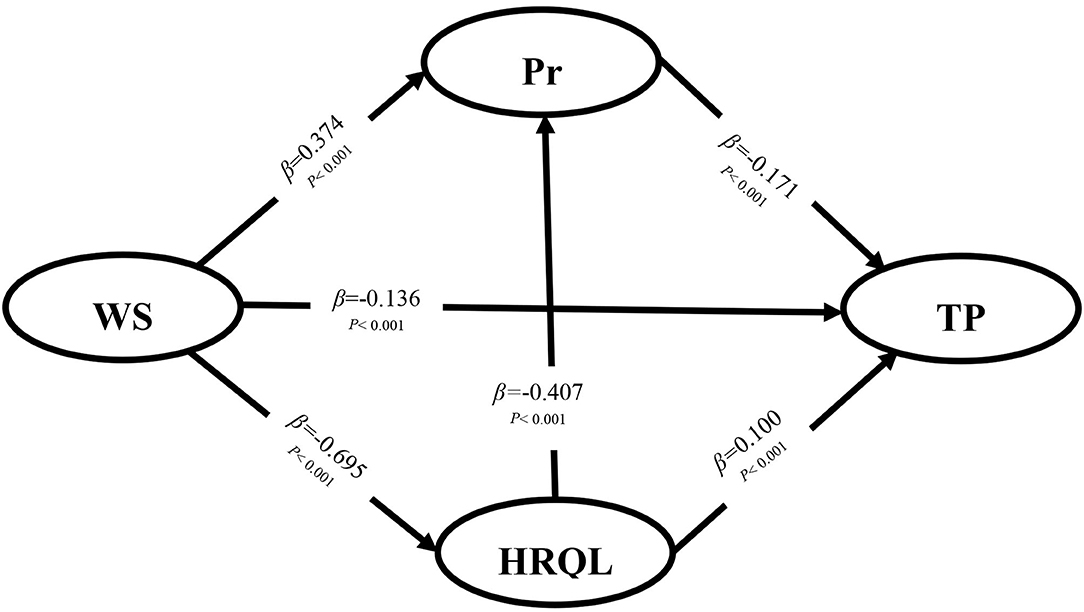
Figure 2. The results of hypothesis testing. TP, task performance; WS, work stress; HRQL, health-related quality of life; Pr, presenteeism.
The results showed that the higher that the work stress is, the more serious that presenteeism is, and the worse that the task performance is (β = −0.136; P < 0.001; β = −0.171; P < 0.001); moreover, the better that health status is, the better that task performance is (β = 0.10; P < 0.001), so H1, H2, and H4 were supported. At the same time, the bootstrapping technique in AMOS was used to explore the mediating roles of presenteeism and health status, and the 95% confidence intervals of the indirect effects were obtained with 5,000 bootstrap resamples. The results showed that work stress significantly affected the task performance of medical staff through presenteeism (β = −0.064; P < 0.001) or health status (β = −0.070; P < 0.001), and health status significantly affected the task performance of medical staff through presenteeism (β = 0.070; P < 0.001), so H3, H5 and H6 were supported as shown in Table 3. In addition, the total effect of work stress and health status on task performance was −0.318 (P < 0.001) and 0.170 (P < 0.001), respectively. Table 4 shows the fit of the model, and the values represent an acceptably fitting model.
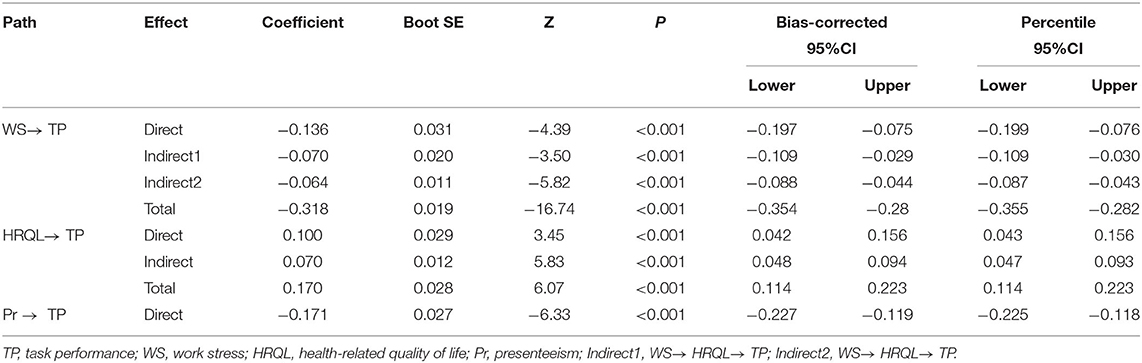
Table 3. Results of the effects on task performance.

Table 4. The fit of the structural equation model.
Discussion
This study explored the factors that influence the task performance of medical staff. A conceptual framework representing the direct and indirect relationships among four factors (task performance, work stress, health status, and presenteeism) was established and validated, and it was helpful for understanding the influence of physical and mental aspects on task performance. The data collection and processing in this study were strictly controlled, and the results could be considered a valuable reference for improving the task performance of medical staff. Based on the results of this study, it is now possible to revisit and reflect on the hypotheses established at the beginning of this study.
The survey results of this study showed that the mean score of task performance was 4.49, while the mean score of task performance of nurses in Malaysia was 3.85 as shown by Nasurdin et al. (59). This difference may be due to the fact that the research group includes different medical staff groups such as doctors and nurses, and nurses face more complicated work tasks, heavier work burden and greater occupational pressure than doctors (60). While reducing the burden of nurses, we should also strengthen the training of their comprehensive ability. The task performance score was relatively high, which may be due to the high sense of responsibility of medical staff in the context of the pandemic, which improves their work efficiency. It is very important to strengthen the guidance of medical ethics for medical staff. The mean score of challenging stress was 2.22, and that of obstructive stress was 1.85. Challenging stress includes workload, time pressure, job responsibilities, etc. Obstructive stress includes ambiguous roles, organizational politics, job insecurity, and blocked career development. This study found that the high score of challenging pressure indicates that the pressure of medical staff mainly comes from time pressure and workload, and also reflects the professional particularity of medical staff, which is more urgent than other industries. Therefore, hospitals and departments should make scientific and reasonable work arrangements to reduce the burden of medical staff. The average score of health status was 4.18, which was at a high level, indicating that the health status of medical staff in the investigated area was good, which may be affected by the local working and living environment and medical staff's own health management awareness. The average score for presenteeism was 2.05. In a study of nurses in Spain, Portugal and Brazil, the overall score for presenteeism was 3.36 (61). The reason for this difference may be, on the one hand, the medical staff group including doctors, nurses, medical skills, etc., whose tasks are not the same, on the other hand, it may be related to the better health status of medical staff in the surveyed areas. Local medical staff should continue to maintain good living and working habits and further strengthen health management.
Studies have shown that work stress, health status, and presenteeism were associated with task performance. Work stress and presenteeism had significant negative influence on medical staff's task performance, and health status had significant positive influence on it. The hypotheses proposed in this paper have been well verified in the structural equation model. The occupation of medical staff is special. Medical work is a high-risk occupation. The work of medical staff is characterized by high risk and urgency, especially during the epidemic period, facing with huge risks and long workloads, competing with time for patients' lives, research has shown that extreme work stress was a great challenge to the health status of medical staff, on the contrary, it would lead to anxiety, tension and other negative emotions, serious and even health problems, not conducive to work (62). Health problems, on the one hand, will increase long-term sick leave, on the other hand, medical staff is more likely to ignore its own health problems, resulting in higher presenteeism. Theoretically attendance will have a positive impact on performance, but sick attendance has a negative impact on performance. Sick attendance was strongly associated with burnout, and attendance due to presenteeism was considered to be working but poor performance, consistent with other study (63). As a result, medical institutions and relevant departments need to appropriately relieve the stress on medical staff through measures such as rational assignment of tasks and upgrading of professional skills, while paying close attention to the health of medical staff, through carrying out health lectures, regular medical check-up and other ways to improve their health literacy, reduce the possibility of carrying diseases to work, prevention or even avoidance of medical staff due to work stress, health status, presenteeism of work efficiency.
The study also found that health status and presenteeism played an mediating role between work stress and task performance, and presenteeism played an mediating role between health status and task performance. The hypotheses were verified in the structural equation model. Research has shown that work stress was linked to health status, when working in a high-pressure environment, health problems were more likely to occur, health was threatened, medical staff also insisted on working with diseases, not only would lead to work errors, work inefficiency, it also exacerbated the negative health effects of the disease, creating a vicious circle and even placing a physical or work burden on others, which was detrimental to the health and well-being of individuals and society as a whole (64, 65). Occupational characteristics lead to stress in the medical profession is inevitable, blindly reducing the work stress of medical staff may reduce the quality of service of medical staff. So when work stress is a factor that can be hard to control, we can focus on health and presenteeism. As hospital administrators, they should take effective measures, such as providing health-promoting places, adding more fitness facilities, enhancing their physical quality, carrying out psychological intervention and relevant training, and enhancing their awareness of health self-management, improve their health and productivity. The factors involved in this study were limited. Future researches may further explore other factors related to performance, and suggest that we should continue to pay attention to the health status of medical staff.
Regarding advantages of this study, previous studies have not addressed the relationships among work stress, health status, presenteeism, and task performance. We established these associations and explored the direct and indirect roles among them. This study investigated a large population, carried out strict quality control, and was highly scientific and representative. Regarding disadvantages, although this study explored and verified the relationships among the four variables, it inevitably has limitations. First, this study was a cross-sectional study, so it is impossible to determine the causal relationships among the variables. In the future, longitudinal study design should be used to collect data as far as possible. Second, this is only one province of China, there may be differences between different provinces, which might have affected the generalizability of the results. When conditions permit, representative sample data can be selected from the whole country for analysis. Third, the method of quota sampling may produce research bias. However, after consulting with local health authorities and health experts, stratified random sampling was applied to capture hospitals and medical staff to minimize bias.
Conclusion
In conclusion, our results showed that work stress and presenteeism had a significant negative effect on task performance of medical staff; health status had a significant positive effect on task performance. At the same time, health status or presenteeism played a mediating role between medical staff's work stress and task performance, and presenteeism played a mediating role between medical staff's health status and task performance. To improve task performance, priority should be given to starting from ideological cognition, platform construction, safety assurance and other aspects, and continuously strengthen the health management of medical institutions and medical personnel.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Medical Ethics Committee of the School of Public Health Jilin University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
HJ and PS: methodology and writing—original draft preparation. SG, JY, and PC: data curation and investigation. XY: funding acquisition, conceptualization, and supervision. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the MOE (Ministry of Education of the People's Republic of China) Project of Humanities and Social Sciences (Grant Number 18YJAZH118). The funding agencies had no role in design, analysis, interpretation, or writing of this study.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zhu N, Zhang D, Wang D, Wang W, Li X, Yang B, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. (2020) 382:727–33. doi: 10.1056/NEJMoa2001017
2. Wilder-Smith A, Chiew CJ, Lee VJ. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect Dis. (2020) 20:e102–7. doi: 10.1016/S1473-3099(20)30129-8
3. Gao GF. From “A” IV to “Z” IKV: attacks from emerging and re-emerging pathogens. Cell. (2018) 172:1157–9. doi: 10.1016/j.cell.2018.02.025
4. Zhang X, Sun F, Wang Y, Zhu Z. Establishment of a psychological intervention mechanism for healthcare workers facing public health emergencies in the context of the COVID-19 outbreak. Int J Health Plann Manage. (2021) 36:2424–9. doi: 10.1002/hpm.3306
5. Prochazka J, Scheel T, Pirozek P, Kratochvil T, Civilotti C, Bollo M, et al. Data on work-related consequences of COVID-19 pandemic for employees across Europe. Data Brief. (2020) 32:106174. doi: 10.1016/j.dib.2020.106174
6. Chen Q, Liang M, Li Y, Guo J, Zhang Z. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry. (2020) 7:e14–5. doi: 10.1016/S2215-0366(20)30078-X
7. Pourteimour S, Yaghmaei S, Babamohamadi H. The relationship between mental workload and job performance among Iranian nurses providing care to COVID-19 patients: a cross-sectional study. J Nurs Manage. (2021) 29:1723–32. doi: 10.1111/jonm.13305
8. Yanez-Araque B, Gomez-Cantarino S, Gutierrez-Broncano S, Lopez-Ruiz VR. Examining the determinants of healthcare workers' performance: a configurational analysis during COVID-19 times. Int J Env Res Pub He. (2021) 18:115671. doi: 10.3390/ijerph18115671
9. Halbesleben JRB, Wheeler AR, Buckley MR. “Clarifying the relationship between organizational commitment and job performance: extending the conservation of resources model,” in Karl H. Kiefer. (2008), p. 35–58.
10. Hoque I, Shahinuzzaman M. Task performance and occupational health and safety management systems in the garment industry of Bangladesh. Int J Workplace Health Manag. (2021) 14:369–85. doi: 10.1108/IJWHM-09-2020-0169
11. Karakas A, Tezcan NS. The relation between work stress, work-family life conflict and worker performance: a research study on hospitality employees. Eur J Tourism Res. (2019) 21:102–18. doi: 10.54055/ejtr.v21i.361
12. Robledo E, Zappalà S, Topa G. Job Crafting as a mediator between work engagement and wellbeing outcomes: a time-lagged study. Int J Environ Res Public Health. (2019) 16:1376. doi: 10.3390/ijerph16081376
13. Tafvelin S, Schwarz UV, Hasson H. In agreement? Leader-team perceptual distance in organizational learning affects work performance. J Bus Res. (2017) 75:1–7. doi: 10.1016/j.jbusres.2017.01.016
14. Kumar P, Kumar N, Aggarwal P, Yeap JAL. Working in lockdown: the relationship between COVID-19 induced work stressors, job performance, distress, and life satisfaction. Curr Psychol. (2021) 40:6308–23. doi: 10.1007/s12144-021-01567-0
15. Padma V, Anand NN, Swaminatha S, Gurukul, Mohammed S, Prassad A, et al. Health problems and stress in Information Technology and Business Process Outsourcing employees. J Pharm Bioallied Sci. (2015) 7:S9–13. doi: 10.4103/0975-7406.155764
16. Dolan SL. The role of personality, occupation and organization in understanding the relationship between job stress, performance and absenteeism. J Occup Organ Psych. (1983) 56:227–40. doi: 10.1111/j.2044-8325.1983.tb00130.x
17. Bhagat RS. Effects of stressful life events on individual performance effectiveness and work adjustment processes within organizational settings: a research model. Acad Manag Rev. (1983) 8:660–71.doi: 10.5465/AMR.1983.4284672
18. Tsai YC, Liu CH. Factors and symptoms associated with work stress and health-promoting lifestyles among hospital staff: a pilot study in Taiwan. BMC Health Serv Res. (2012) 12:199. doi: 10.1186/1472-6963-12-199
19. Tetrick LE, Quick JC. Prevention at work: Public health in occupational settings. In Quick JC and Tetrick LE, editors. Handbook of Occupational Health Psychology (pp. 3–17). Washington, DC: American Psychological Association (2003).
21. Ford MT, Cerasoli CP, Higgins JA, Decesare AL. Relationships between psychological, physical, and behavioural health and work performance: a review and meta-analysis. Work and Stress. (2011) 25:185–204. doi: 10.1080/02678373.2011.609035
22. Baldwin PJ, Dodd M, Wrate RW. Young doctors' health—I. How do working conditions affect attitudes, health and performance? Soc Sci Med. (1997) 45:35–40. doi: 10.1016/S0277-9536(96)00306-1
23. Raisiene A, Rapuano V, Varkulevičiute K, Stachová K. Working from home—who is happy? A survey of Lithuania's employees during the COVID-19 quarantine period. Sustain Basel. (2020) 12:5332. doi: 10.3390/su12135332
24. Fu SQ, Greco LM, Lennard AC, Dimotakis N. Anxiety responses to the unfolding COVID-19 crisis: patterns of change in the experience of prolonged exposure to stressors. J Appl Psychol. (2021) 106:48–61. doi: 10.1037/apl0000855
25. Aronsson G, Gustafsson K. Sickness presenteeism: prevalence, attendance-pressure factors, and an outline of a model for research. J Occup Environ Med. (2005) 47:958–66. doi: 10.1097/01.jom.0000177219.75677.17
26. Ks A, Amc B. The consequences of sickness presenteeism on health and wellbeing over time: a systematic review. Soc Sci Med. (2016) 161:169–77. doi: 10.1016/j.socscimed.2016.06.005
27. Johns G. Presenteeism in the workplace: a review and research agenda. J Organ Behav. (2010) 31:519–42. doi: 10.1002/job.630
28. Koopmanschap M, Burdorf A, Jacob K, Meerding WJ, Severens H. Measuring productivity changes in economic evaluation: setting the research agenda. Pharmacoeconomics. (2005) 23:47–54. doi: 10.2165/00019053-200523010-00004
29. Goetzel RZ, Long SR, Ozminkowski RJ, Hawkins K, Wang S, Lynch W. Health, absence, disability, and presenteeism cost estimates of certain physical and mental health conditions affecting US employers. J Occup Environ Med. (2004) 46:398. doi: 10.1097/01.jom.0000121151.40413.bd
30. Collins JJ, Baase CM, Sharda CE, Ozminkowski RJ, Nicholson S, Billotti GM, et al. The assessment of chronic health conditions on work performance, absence, and total economic impact for employers. J Occup Environ Med. (2005) 47:547–57. doi: 10.1097/01.jom.0000166864.58664.29
31. Niven K, Ciborowska N. The hidden dangers of attending work while unwell: a survey study of presenteeism among pharmacists. Int J Stress Manage. (2015) 22:207–21. doi: 10.1037/a0039131
32. Anca SC. A Critical analysis of self-assessment tools for improving workers' health and work performance. In: Vlad S, Roman NM, editors. International Conference on Advancements of Medicine And Health Care Through Technology, Meditech 2016. 5th International Conference on Advancements of Medicine and Health Care through Technology (MEDITECH). (2017). p. 283–6. doi: 10.1007/978-3-319-52875-5_59
33. Dietz C, Scheel T. Leadership and presenteeism among scientific staff: the role of accumulation of work and time pressure. Front Psychol. (2017) 8:1885. doi: 10.3389/fpsyg.2017.01885
34. Black JK, Balanos GM, Phillips AC. Resilience, work engagement and stress reactivity in a middle-aged manual worker population. Int J Psychophysiol. (2017) 116:9–15. doi: 10.1016/j.ijpsycho.2017.02.013
35. Cavanaugh MA, Boswell WR, Roehling MV, Boudreau JW. An empirical examination of self-reported work stress among US managers. J Appl Psychol. (2000) 85:65–74. doi: 10.1037//0021-9010.85.1.65
36. Boswell WR, Olson-Buchanan JB, Lepine MA. Relations between stress and work outcomes: The role of felt challenge, job control, and psychological strain. J Vocat Behav. (2004) 64:165–81. doi: 10.1016/S0001-8791(03)00049-6
37. Haar Jarrod M. Challenge and hindrance stressors in New Zealand: exploring social exchange theory outcomes. Int J Hum Resour Man. (2006) 17:1942–50. doi: 10.1080/09585190601000147
38. Satoris S, Culbertson AHHR. Leader-member exchange and work-family interactions: the mediating role of self-reported challenge- and hindrance-related. Stress J Psychol. (2010) 144:15–36. doi: 10.1080/00223980903356040
39. Lepine JA, Podsakoff NP, Lepine MA. A meta-analytic test of the challenge stressor–hindrance stressor framework: an explanation for inconsistent relationships among stressors and performance. Acad Manage J. (2005) 48:764–75. doi: 10.5465/AMJ.2005.18803921
40. Podsakoff NP, LePine JA, LePine MA. Differential challenge stressor-hindrance stressor relationships with job attitudes, turnover intentions, turnover, and withdrawal behavior: a meta-analysis. J Appl Psychol. (2007) 92:438. doi: 10.1037/0021-9010.92.2.438
41. Pearsall MJ, Ellis A, Stein JH. Coping with challenge and hindrance stressors in teams: behavioral, cognitive, and affective outcomes. Organ Behav Human Decis Process. (2009) 109:18–28. doi: 10.1016/j.obhdp.2009.02.002
42. Yi Z, Zhan-Biao S, Li-Ying Z, Jian-Zhou C, Mei F, Jie Y, Xiu-Ling GU. Application of challenge-and hindrance- related self-reported stress scale in Chinese occupational people. Chin Mental Health J (In Chinese) (2013) 27:5. doi: 10.3969/j.issn.1000-6729.2013.05.013
43. Lang L, Zhang L, Zhang P, Li Q, Bian J, Guo Y. Evaluating the reliability and validity of SF-8 with a large representative sample of urban Chinese. Health Qual Life Outcomes. (2018) 16:55. doi: 10.1186/s12955-018-0880-4
44. Gulati S, Coughlin PA, Hatfield J, Chetter IC. Quality of life in patients with lower limb ischemia; revised suggestions for analysis. J Vasc Surg. (2008) 49:122–6. doi: 10.1016/j.jvs.2008.08.011
45. Vallès J, Guilera M, Briones Z, Gomar C, Alonso J. Validity of the Spanish 8-item short-form generic health-related quality-of-life questionnaire in surgical patients: a population-based study. Anesthesiology. (2010) 112:1164. doi: 10.1097/ALN.0b013e3181d3e017
46. Tokuda Y, Okubo T, Ohde S, Jacobs J, Takahashi O, Omata F, et al. Assessing items on the SF-8 Japanese version for health-related quality of life: a psychometric analysis based on the nominal categories model of item response theory. Value Health. (2009) 12:568–573. doi: 10.1111/j.1524-4733.2008.00449.x
47. Roberts B, Browne J, Ocaka FK, Oyok T, Sondorp E. The reliability and validity of the SF-8 with a conflict-affected population in northern Uganda. Health Qual Life Out. (2009) 6:108. doi: 10.1186/1477-7525-6-108
48. Koopman C, Pelletier KR, Murray JF, Sharda CE, Berger ML, Turpin RS, et al. Stanford presenteeism scale: health status and employee productivity. J Occup Environ Med. (2002) 44:14–20. doi: 10.1097/00043764-200201000-00004
49. Brooks A, Hagen SE, Sathyanarayanan S, Schultz AB, Edington DW. Presenteeism: critical issues. J Occup Environ Med. (2010) 52:1055–67. doi: 10.1097/JOM.0b013e3181f475cc
50. Jiang XW, Liu JN, Liu FJ, Zheng ZJ, Chang C. Reliability and validity of Stanford Presenteeism Scale (SPS-6) in Chinese occupational population. Chin J Ind Hygiene Occup Dis (In Chinese) (2020) 38:5. doi: 10.3760/cma.j.cn121094-20191114-00529
51. Williams LJ, Anderson SE. Job satisfaction and organizational commitment as predictors of organizational citizenship and in-role behaviors. J Manag. (1991) 17:601–17.
52. Methot JR, Lepine JA, Podsakoff NP, Christian JS. Are workplace friendships a mixed blessing? exploring tradeoffs of multiplex relationships and their associations with job performance. Pers Psychol. (2016) 69:311–55. doi: 10.1111/peps.12109
53. Meira J. Employee work status, mental health, substance use, and career turnover intentions: An examination of restaurant employees during COVID-19. Int J Hosp Manag. (2020) 93:102764. doi: 10.1016/j.ijhm.2020.102764
54. Ren Z, Zhang X, Sun Y, Li X, Liu H. Relationships of professional identity and psychological reward satisfaction with subjective well-being among Chinese nurses. J Nurs Manage. (2021) 29:1508–16. doi: 10.1111/jonm.13276
55. Crowley SL, Fan X. Structural equation modeling: basic concepts and applications in personality assessment research. J Pers Assess. (1997) 68:508–31. doi: 10.1207/s15327752jpa6803_4
56. Schreiber JB, Nora A, Stage FK, Barlow EA, King J. Reporting structural equation modeling and confirmatory factor analysis results: a review. J Educ Res. (2006) 99:323–38. doi: 10.3200/JOER.99.6.323-338
57. Golini N, Egidi V. The latent dimensions of poor self-rated health: how chronic diseases, functional and emotional dimensions interact influencing self-rated Health in Italian elderly. Soc Indic Res. (2016) 128:321–39. doi: 10.1007/s11205-015-1033-3
58. Fan N. Strategy use in second language vocabulary learning and its relationships with the breadth and depth of vocabulary knowledge: a structural equation modeling study. Front Psychol. (2020) 11:752. doi: 10.3389/fpsyg.2020.00752
59. Nasurdin AM, Ling TC, Khan SN. Linking social support, work engagement and job performance in nursing. Int J Bus Soc. (2018) 19:363–86.
60. Li B, Li Z, Wan Q. Effects of work practice environment, work engagement and work pressure on turnover intention among community health nurses: Mediated moderation model. J Adv Nurs. (2019) 75:3485–94. doi: 10.1111/jan.14130
61. Mosteiro-Díaz MP, Baldonedo-Mosteiro M, Borges E, Baptista P, Queirós C, Sánchez-Zaballos M, et al. Presenteeism in nurses: comparative study of Spanish, Portuguese and Brazilian nurses. Int Nurs Rev. (2020) 67:466–75. doi: 10.1111/inr.12615
62. Nätti J, Oinas T, Anttila T. Time pressure, working time control and long-term sickness absence. Occup Environ Med. (2015) 72:265. doi: 10.1136/oemed-2014-102435
63. Collins AM, Cartwright S, Cowlishaw S. Sickness presenteeism and sickness absence over time: A UK employee perspective. Work Stress. (2018) 32:68–83. doi: 10.1080/02678373.2017.1356396
64. Silla I, Gamero N. Shared time pressure at work and its health-related outcomes: Job satisfaction as a mediator. Eur J Work Organ Psychol. (2014) 23:405–18. doi: 10.1080/1359432X.2012.752898
Keywords: work stress, health status, presenteeism, task performance, medical staff
Citation: Jia H, Shang P, Gao S, Cao P, Yu J and Yu X (2022) Work Stress, Health Status and Presenteeism in Relation to Task Performance Among Chinese Medical Staff During COVID-19 Pandemic. Front. Public Health 10:836113. doi: 10.3389/fpubh.2022.836113
Received: 15 December 2021; Accepted: 22 March 2022;
Published: 27 April 2022.
Edited by:
Angela Stufano, University of Bari Aldo Moro, ItalyReviewed by:
Xiaoyu Xi, China Pharmaceutical University, ChinaZeinab A. Kasemy, University of Menoufia, Egypt
Copyright © 2022 Jia, Shang, Gao, Cao, Yu and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xihe Yu, eGh5dUBqbHUuZWR1LmNu
†These authors have contributed equally to this work