
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 April 2022
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.822116
 Iyasu Tadesse Bukata1
Iyasu Tadesse Bukata1 Lelisa Sena Dadi2Andualem Mossie Ayana1
Lelisa Sena Dadi2Andualem Mossie Ayana1 Demelash Mengistu3Delnesa Yewal4
Demelash Mengistu3Delnesa Yewal4 Tariku Sime Gizaw1*
Tariku Sime Gizaw1* Yohannes Markos Woldesenbet5
Yohannes Markos Woldesenbet5Background: Coronavirus disease (COVID-19) was first reported by the World Health Organization on 31 December 2019, and later, it was declared a global pandemic on 12 March 2020. To date, it is a great challenge to the world including Ethiopia. Therefore, to attain effective prevention and control of the COVID-19 pandemic, improving the knowledge, attitude, and practices of the community is necessary.
Objective: To assess, knowledge, attitudes, and practice, and associated factors of COVID-19 among Jimma Town residents.
Methods: A community-based cross-sectional study was conducted among 1,500 Jimma town residents from May through June 2020. Adults aged ≥18 years were included in the study. Data were collected using a structured questionnaire that was adopted from different literature. A face-to-face interview was implemented to collect data. Analysis was done by using SPSS version 22. p < 0.05 was used to declare statistical significance.
Result: A total of 1,500 participants were enrolled in the study. The majority of the respondents were female (59.3%). About 841 (56.1%) of the participants had knowledge about COVID-19. Educational status, household wealth index, and employment showed association with knowledge of COVID-19. Government-owned television (37.3%) was the primary source of information about COVID-19 in the Jimma population. Only 46.6% of respondents had good attitudes toward the COVID-19 pandemic and about 638 (42.5%) of the study participants had good practice toward COVID-19. The mean practice score was 1.98 (± 0.319). Study participants who were residing in the outskirts of the town were 0.37 less likely to apply good practice regarding COVID-19 prevention measures than those around the center of the town. Whereas, households with a family size of four to five individuals were 1.4 times more likely to show good practice against COVID-19 compared to households with ≤3 individuals (AOR: 1.41; CI: 1.05, 1.91).
Conclusion: Jimma town community has low knowledge, attitude, and practice regarding COVID-19. Knowledge, attitude, and practice scores regarding COVID-19 are significantly related to educational status, being self-employed, occupation, marital status, residence, family size, and household relative wealth index. Preventive health advisories to upraise knowledge, attitude, and practice are crucial to prevent and control COVID-19.
Coronavirus disease (COVID-19) is a global pandemic that is caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). It was first seen in Wuhan, Hubei Province, China, on 31 December 2019, and later, on 12 March 2020, it was declared by World Health Organization (WHO) as a global pandemic (1–4). The disease is highly infectious, and its main clinical symptoms include fever, dry cough, fatigue, myalgia, and dyspnea. In China, 18.5% of the patients with COVID-19 develop to the severe stage, which is characterized by acute respiratory distress syndrome, septic shock, difficult-to-tackle metabolic acidosis, and bleeding and coagulation dysfunction (5, 6).
According to the WHO report on COVID 19, as of 28 November 2021, there were 260, 493,573 confirmed cases, and 5, 195, 354 confirmed deaths globally1. Data also indicate that infection and death from the pandemic are increasing highly despite the battle against it is still continuing (7). Yet, the use of face masks, good hand hygiene, and social distancing as community interventions are effective to control the spread of the pandemic (8). In order to familiarize effective control measures, having knowledge about basic hygiene principles and modes of disease transmission, and measures in such an environment is, vitally important (3). Therefore, improving the knowledge, attitude, and practices of the community is essential (9). The effectiveness of community interventions in lower and middle income countries should be informed by adherence to the mitigation measures and contextual factors taking into account the best practices (8).
The level of knowledge, attitude, and practices of the community regarding COVID 19 vary with the geographical site in the world. In the rural part of Ethiopia, the communities' residents may notice themselves as low risk of acquiring COVID-19, and negligence of the prevention method is visible community gathering is experienced as usual. Therefore, assessing knowledge, attitude, and practice of COVID-19 prevention and implementing interventions is mandatory in the different geographic areas of the country. To know the level of knowledge, there is no study conducted in the Jimma community to assess the level of knowledge, attitude, and practice of the community. Therefore, the current study is aimed to assess this gap and develop an intervention strategy to alleviate the burden of the problem in the studied area.
A community-based cross-sectional study was conducted in Jimma Town, Ethiopia, among adults aged 18 years and beyond to assess their knowledge, attitude, and practice toward the prevention of COVID-19. The study was conducted from the 1st week of May through the last week of June 2020. Jimma is the largest city in southwestern Ethiopia and consists of 17 Kebeles (the lowest administrative unit). The town is located 352Km from Addis Ababa, the capital city of Ethiopia, and has a latitude and longitude of 7°40′N 36°50′E. According to the Oromia region population projection, the town has nearly 207,000 residents. There are two public and two private hospitals, and five health centers in the town.
Sample size was determined using single population proportion formula (n = [Zα/2] 2 p [1-p]/d2). We used a p-value of 50% and a 0.5 margin of error. Using this calculation we got a sample size of 384.
But, to reach an interviewee in the households, we needed to go through four strata/ stages: Jimma town, sub-cities, kebeles, households, and individuals. Hence, we implemented a multi-stage sampling technique that is indebted to the use of a design effect. Therefore, after considering a design effect of 4.0 and a non-response rate of 10%, we got a sample size of 1,690. But, after data collection about 200 questionnaires were below quality. Hence, these questionnaires were discarded and 1,500 data were used for analysis.
We selected six Kebeles from the 17 kebeles in the town. The selection of the Kebeles was done using simple random sampling. The six kebeles are about 30% of the whole town. A systematic sampling technique was undertaken to identify the households in each Kebele. An individual from the household was then chosen using a lottery method.
Data collection was done by face-to-face interview using a structured questionnaire which is developed after reviewing several articles that were done to measure KAP toward COVID-19 and published in reputable journals. The questionnaire consisted of 51 close-ended questions that aimed to collect information on socio-demographic characteristics, travel history, and KAP related to COVID-19 from the study respondents.
Data collectors and supervisors were given 2 days of training on the nature of the study and WHO-recommended precaution measures related to COVID-19.
The interview process took ~10–15 min to complete. The data collection tool was initially prepared in English version followed by translation to local Afan Oromo and Amharic languages. Consistency of content, clarity, and appropriate meaning between the three versions were maintained through back-translation of the questionnaire to the original version. Additionally, the practicability, validity, and interpretability of answers for the respective questions were confirmed by performing a pre-test in 10% of the targeted sample size. Based on this pre-test study, the format and wording of questions were corrected and refined.
Data were checked for completeness. Data entry was done using EPI data version 3.1 and exported to SPSS for Windows version 22 for analysis.
A total of 1,500 participants were enrolled in the study. The majority of the respondents were female (59.3%) and about 34.9% of the respondents were between 30 and 39 years of age. The mean age of study participants was 35.8 (standard deviation of ± 11.6). With regard to the residence of the respondents, most (81.8%) of them were living in Jimma town and married (76.8%). The majority of study participants had only primary school educational achievement, and most of the study participants had a family size of four to six individuals per household and in the 2nd /4th quintiles of household relative wealth index (Table 1).
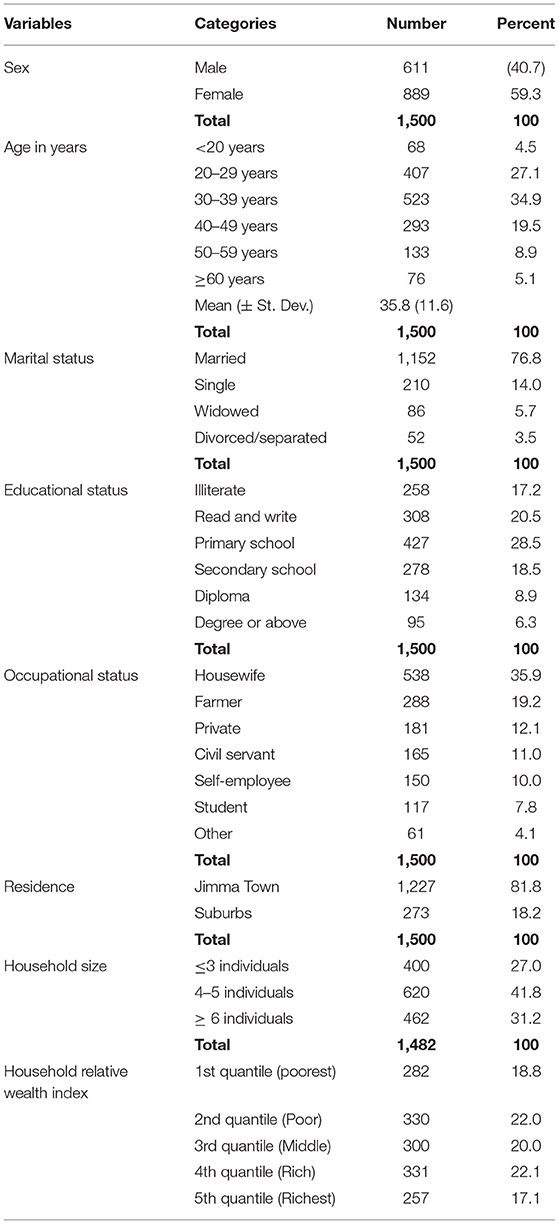
Table 1. Socio-demographic characteristics of study participants, Jimma Town, Southwest Ethiopia, 2020.
Good and poor knowledge among study respondents were found to be 841 (56.1%) and 659 (43.9%), respectively. A high number of study participants had poor knowledge about the spread of the virus through indirect hand contact and consider that no effective cure for COVID-19.
Dissimilarly, about 48.1% of the study participants were misunderstood that eating or contacting domestic animals would result in the virus. In addition, most (77.5%) of the study participants oppose knowledge items that ordinary residents should not wear general medical masks. Moreover, the vast majority of study participants were aware of the helpfulness of avoiding crowded places and isolation and treating person who contracted COVID-19 for prevention and control of the virus (Table 2).
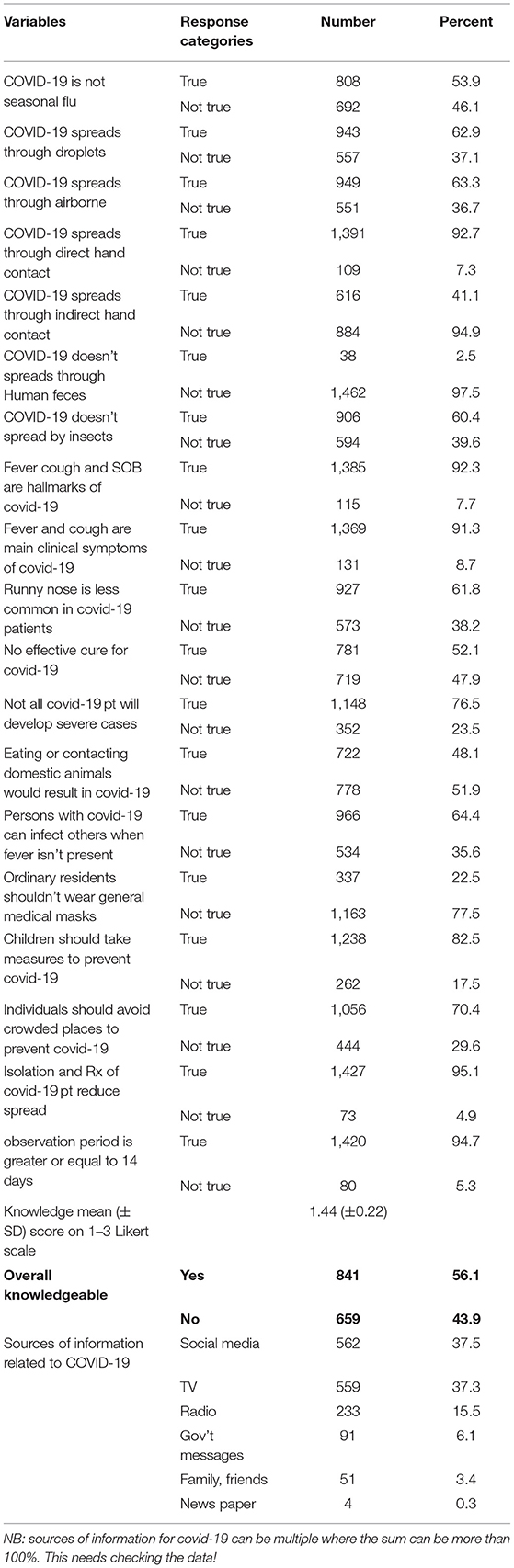
Table 2. Knowledge of study participants about prevention of COVID-19, Jimma Town, Southwest Ethiopia, 2020.
Analysis of data using multiple logistic regression shows that educational status and being self-employed were associated with good knowledge of study participants about COVID-19. The odds of having good knowledge among study participants; who can read and write, having primary level, had a secondary level, and having diploma and beyond educational achievements were 1.8, 2.05, 2.07, and 2.7 times higher than study respondents who had no formal education or illiterate, respectively. Whereas, the odds of having good knowledge about COVID-19 among study participants who were self-employed in their occupational status was 4.3 times higher compared to being a housewife. Also, the knowledge of study participants about COVID-19 was about 7.5 times higher among the richest study participants than the poor (Table 3).
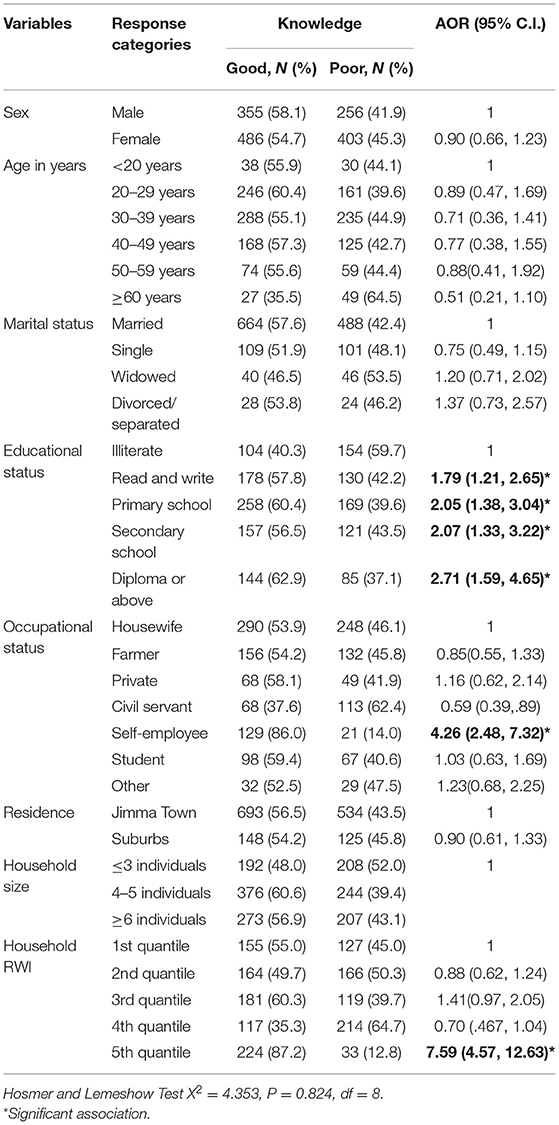
Table 3. Factors affecting knowledge about prevention of COVID-19, Jimma Town, Southwest Ethiopia, 2020.
For most of the study respondents' social media (37.7%) and government-owned television (37.3%) were primary sources of information about COVID-19 followed by government-owned radio. In addition to these, government health and telecom messages were highly believed as sources of information among study respondents.
As shown in Table 4, most of the residents had a poor attitude (53.4%) toward the implementation of preventive measures against the COVID-19 pandemic. In this study, about 77.5 and 66.7% of the respondents had a negative attitude toward wearing masks and care not spreading the virus to others if they did contracted COVID-19, respectively. The majority had a good attitude towardfrequent hand washing with soap and water, use of sanitizers, and wearing a mask outside the house as a preventive measure against COVID-19. More than half (79.0%) of the study participants perceived that Ethiopia can win the battle against COVID-19. The findings indicated that 46.6% of respondents had good attitudes toward the prevention and control of the COVID-19 pandemic.
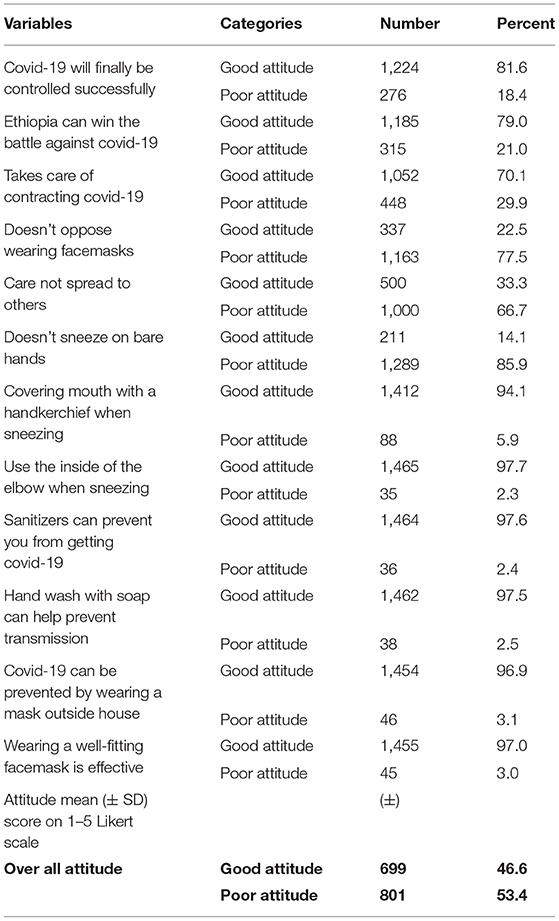
Table 4. Attitude of study participants about COVID-19 prevention, Jimma Town, Southwest Ethiopia, 2020.
Factors like sex, age in years, marital status, educational level, residence (urban or skirt of town), and family size did not show significant association with attitude regarding COVID-19 prevention and control. With regard to variables related to good attitudes against COVID-19 we found that farmers were 1.6 times more likely to have a good attitude than housewives regarding COVID-19 prevention and control (AOR: 1.63, CI: 1.09, 2.44), however, civil servants were less likely to have good attitude compared to housewife (AOR = 0.66, CI = 0.44–0.99). An additional factor of more good attitudes against COVID-19 was study respondents in the 4th quintile of household relative wealth index had 1.5 times more likely good attitude than those in the 1st quintile (Table 5).
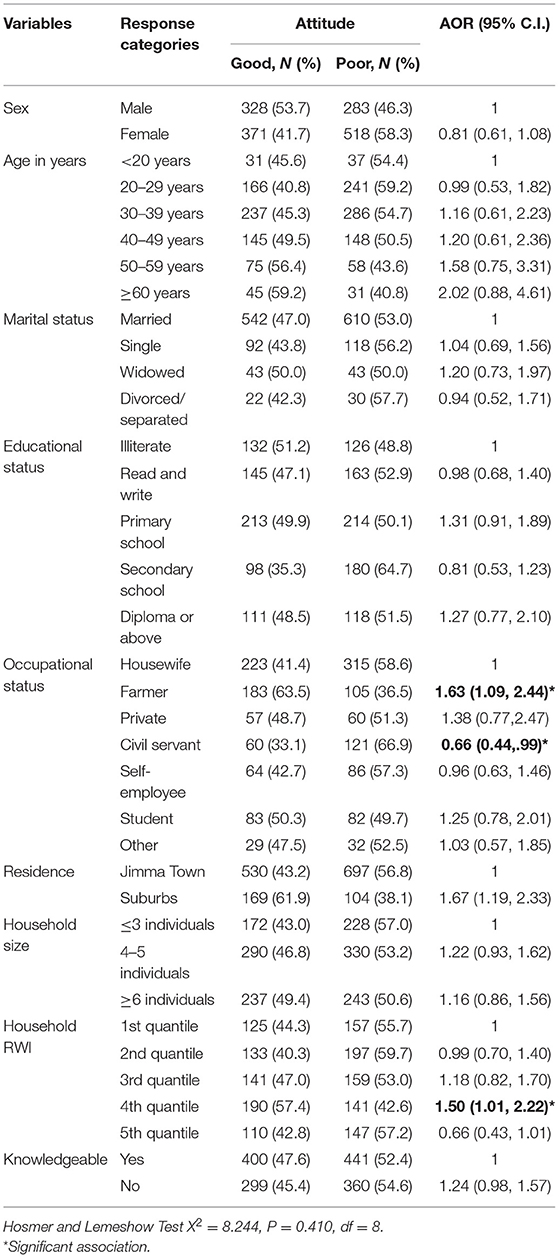
Table 5. Factors affecting attitude of study participants towards COVID-19 prevention in Jimma Town, Southwest Ethiopia, 2020.
In this study, most (90.5%) of the participants had no history of travel abroad or the COVID-19 hotspot area 2 months prior to the date of data collection. The mean practice score was 1.98 (± 0.319). The majority (57.5%) of the study participants had poor practice regarding COVID-19 prevention and control. Whereas, about 638 (42.5%) of the study participants had good practice toward COVID-19. During the data collection period, the study participants' practical experience of hand washing with soap and water and use of disinfectant always was 74.6 and 41.1%, respectively. The rest of them did it occasionally or never. Similarly, 52.1% of the participants had not practiced hand shaking (Table 6).
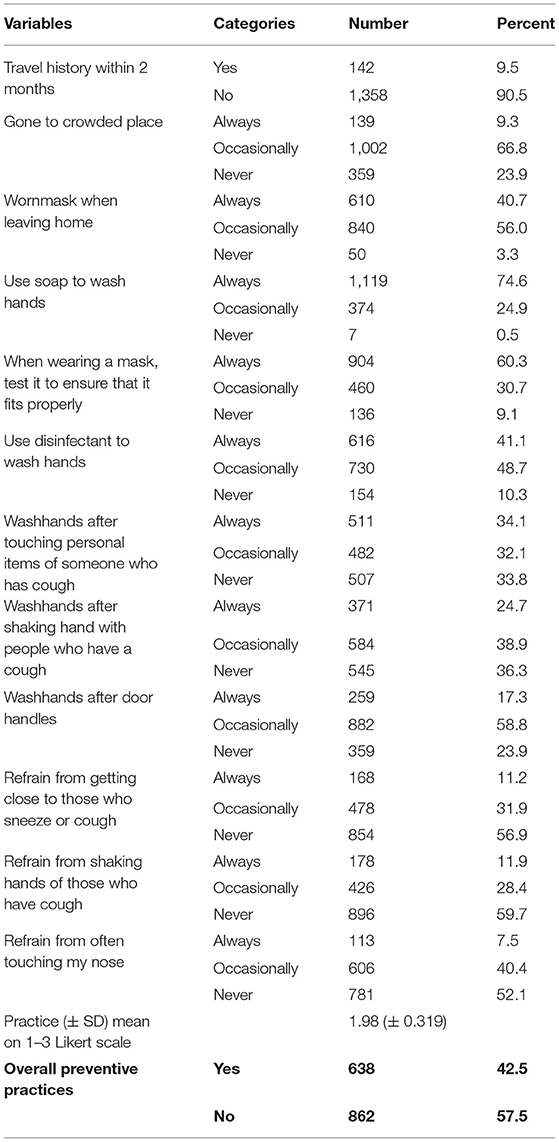
Table 6. Prevention practice of COVID-19 among study participants about COVID-19 in Jimma Town, Southwest Ethiopia, 2020.
As shown in Table 7, factors like sex, age, and educational status did not significantly associated with good practice regarding COVID-19 prevention and control. Regarding the good practice of COVID-19, we found that being widowed was more than half less likely to have good practice of COVID-19 than married (AOR: 0.54, CI: 0.31, 0.95) whereas good practice was two times higher among divorced or separated than married (AOR: 2.00, CI: 1.07, 3.76). Similarly, good practice of COVID-19 prevention and control was nearly half times less likely among students compared to housewives (AOR: 0.43, CI: 0.26, 0.72).
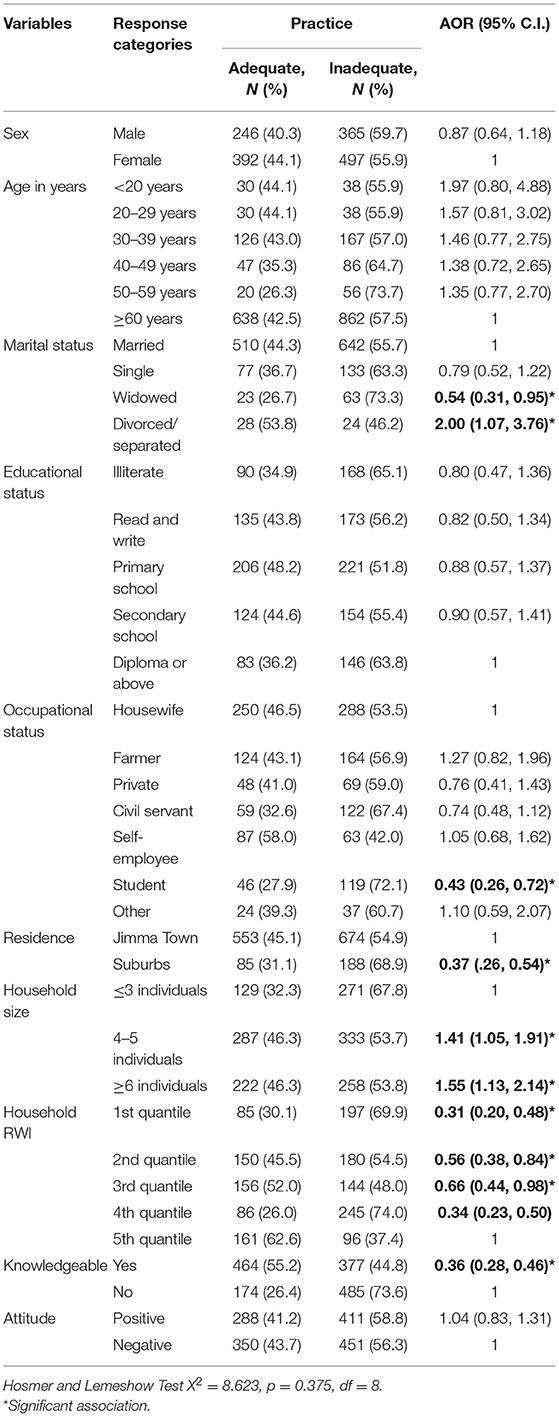
Table 7. Factors affecting COVID-19 prevention practices of study participants in Jimma Town, Southwest Ethiopia, 2020.
Moreover, study participants who were residing in the skirt of the town were 0.37 less likely to have good practice regarding COVID-19 prevention and control than those in the Town. Whereas, regarding the family size, households with a family size of four to five individuals were 1.4 times more likely to have good practice against COVID-19 compared to households with ≤3 individuals (AOR: 1.41; CI: 1.05, 1.91), similarly, the good practice regarding COVID-19 preventions and control was 1.6 times higher among the family of six or more individuals than households with ≤3 individuals (AOR: 1.55; CI: 1.13, 2.14) (Table 7).
With regards to household income, the good practice of COVID-19 prevention and control were less likely to be experienced in 1st, 2nd, 3rd, and 4th quintiles (AOR: 0.31; CI: 0.2, 0.48; AOR: 0.56; CI: 0.38, 0.84, AOR: 0.66; CI: 0.44, 0.98, AOR: 0.34; CI: 0.23, 0.50), respectively, than those study participants in 5th quintile.
As indicated in the last columns of Table 7, those who have better knowledge of COVID-19 had less practice in its prevention and controls (AOR: 0.36; CI: 0.28, 0.46). Dissimilarly, attitudes toward COVID-19 did not show significant association with the practice of COVID-19 prevention and control (AOR: 1.04; CI: 0.83, 1.31).
Currently, COVID-19 is the major public health burden in the world, and the morbidity and mortality of the global community are dramatically increasing from time to time (10). Adherence to preventive measures against the virus are still the best way to reduce and control COVID-19 disease (11). The adherence to preventive measures is largely influenced by knowledge and attitude. The present study aimed at assessing knowledge, attitudes, and practice toward the prevention of COVID-19 among Jimma Town residents.
The finding of the present study indicates that only 56.1% of the study population has knowledge regarding COVID-19 disease. This much low rate of COVID-19 knowledge among Jimma residents was unexpected. Although this survey was conducted a few months after the disease was reported as a pandemic, information about the disease had been disseminated using every possible way of information transmission in Ethiopia. Because of the seriousness of the pandemic, there was overwhelming news on the pandemic everywhere.
The mean (± SD) knowledge score on the 1–3 Likert scale found in our study was 1.44 (±0.22). Yet, a high number of the study population has poor knowledge about the spread of the virus through indirect hand contact and they consider that there is no effective cure for COVID-19. Presently, several studies are conducted on KAP toward COVID-19. Compared to our findings, the majority of these studies found a higher level of knowledge regarding COVID-19. For example, a study conducted in Malaysia found an overall COVID-19 knowledge rate of 80.5% (11). This is a very high level of knowledge when compared to our findings. Another study from the same country found an overall correct knowledge rate of 91.3%, indicating a very good knowledge level (12). Likewise, a bi-national survey conducted in Egypt and Nigeria found a mean knowledge score was 14.7 ± 2.3 and about 61.6% of the population participating in the survey knew about the disease (13).
The knowledge score we found is highly lower than the knowledge score reported from Malaysian studies (11, 12). But, it is fairly lower than the bi-national survey conducted in Egypt and Nigeria (13). The reason behind the lower knowledge score of our study population may be the level of education. The authors of the bi-national survey conducted in Egypt and Nigeria argue that most of the respondents of their study had a satisfactory knowledge level of the disease and the preventive measures because both of the countries have a well-educated population (bachelor/master's degree holders). Our data also indicated that educational status is associated with good knowledge about COVID-19. The odds of having good knowledge among study participants who can read and write, had a primary level, had a secondary level, and had a diploma and beyond educational achievements were 1.8, 2.05, 2.07, and 2.7 times higher than study respondents who had no formal education or illiterate, respectively.
Social media (37.7%) and government-owned television (37.3%) were the primary sources of information about COVID-19 for the Jimma community. In addition to these, government health and telecom messages were highly believed as sources of information among them. This is similar to the report by Hager et al. and Abdelhafiz et al. (13, 14).
Regarding the attitude, the finding of our study indicated that the majority of the residents of Jimma town had a poor attitude (53.4%) toward the implementation of preventive measures against the COVID-19 pandemic. It also indicated that about 77.5 and 66.7%, respectively, of the respondents, had a negative attitude toward wearing masks and care not spreading the virus to others in case they did contracted COVID-19.
But, a study conducted in Gonder town, North Ethiopia found a better prevalence of good attitude than our finding; which reported that about 53.13% of its study population had an overall good attitude regarding COVID-19 (15). Likewise, a study conducted in Addis Ababa, Ethiopia, reported that about 60.7% of its study population had a good attitude toward the implementation of preventive measures against COVID-19 (16). These findings are fairly better than ours. Therefore, there is still an intra-country difference in Ethiopia regarding the attitude toward COVID-19. This difference could be attributed to the difference in the descriptive characteristics of the study population and the time of the study. The poor attitude about COVID-19 among our participants could also be resulted because of the low level of knowledge about the disease. Because knowledge and attitude toward COVID-19 among Jimma residents were poor, most residents were unwilling to take precautions such as wearing masks and not going to crowded places to prevent the infection by COVID-19. These potentially risky attitudes have to be removed from the Jimma community through appropriate intervention in the area.
With regard to factors affecting attitude, sex, age, marital status, educational level, residence (urban or skirt of town) and family size didn't show significant association with attitude regarding COVID-19 prevention and control. This result is contrary to a study conducted by Taddese et al. (15). In their study, Taddese et al. found the level of education and family size as the major socio-demographic factors that showed a positive association with attitude toward COVID-19. The possible reason, for the differences in the factors that affect the attitude of the communities' toward COVID-19, might be ascribed to differences in the study population, the timing of the study period, tools used to measure the variables, the sample size, the level of information exchange among the study populations.
In our study, we also found that study respondents in the 4th quintile of the household relative wealth index had a 1.5 times more likely good attitude than those in the 1st quintile. Some scholars argue that having a better income or being better in socioeconomic status enables to have resources to secure information related to COVID-19 thereby enabling to have good knowledge and a positive attitude toward the pandemic (15). This finding is an important indication for policymakers and intervention strategies to focus on community members who have no formal education.
In this study, the magnitude of good practice regarding COVID-19 was 42.5% which is a relatively small figure when compared to studies elsewhere in the world. The study participants' practical experience of hand washing with soap and water and use of disinfectant always was 74.6 and 41.1%, respectively. The rest of them did it occasionally or never. Similarly, 47.9% of the participants had been practicing hand shaking.
Compared to the majority of the studies in the literature, our study found low good practice regarding COVID-19 preventive measures. The practice of COVID-19 preventive measures in the Jimma community was lower compared to the findings from Iran (17), Nigeria (18), Lebanon (19), Venezuela (20), and Vietnam (21).
With regard to the factors affecting the outcome variables, the socio-demographic variables such as sex, age, and educational status did not significantly associate with good practice regarding COVID-19 prevention and control. But, a study conducted among a healthy Filipino population indicated that knowledge, attitude, and practice scores of their study population showed significant differences in age, sex, place of residence, occupation, and marital status (p < 0.000) (22). Our finding is also different from two studies conducted in Indonesia (23, 24). From this finding, we understand that the Jimma community adherence to the COVID-19 pandemic lags behind which contributed to low knowledge, attitude, and practice scores about the disease. The same finding is also reported in a study conducted in North Shoa Zone, Ethiopia (25). Hence, emphasis should be given to upraise the community's KAP regarding COVID-16 through health education and promotion.
In our population, good practice of COVID-19 was two times higher among divorced or separated than married (AOR: 2.00, CI: 1.07, 3.76). Similarly, good practice was nearly half times less likely among students compared to housewives (AOR: 0.43, CI: 0.26, 0.72), and study participants who were residing in the skirt of the town were 0.37 less likely to have good practice regarding COVID-19 prevention and control than those in the Town. Therefore, in the Jimma community, there are differences in adhering to the preventive measures of COVID-19 with respect to marital status, occupation, and residence (center of town and outskirts).
This is the first study conducted in Jimma regarding knowledge, attitude, and practice toward COVID-19. Compared to other studies conducted regarding COVID-19 in Ethiopia, the study recruited a large sample size. This can be taken as one of the strengths of the current study. Yet, it has two limitations. First, it followed a cross-sectional study design which is a single point study. Second, it was conducted at the early stage of the pandemic, which might have contributed to the low knowledge, attitude, and practice among the surveyed population about the disease. Hence, conducting follow up studies may help to find temporal changes that may be seen in the population.
The findings of the current study indicate that the Jimma town community has low knowledge, attitude, and practice regarding COVID-19. But Ethiopia is a resource-challenged country. Precautionary and preventive health advisories to upraise knowledge, attitude, and practice are crucial to prevent and control the transmission of COVID-19.
In the Jimma community, knowledge, attitude, and practice scores regarding COVID-19 are significantly related to educational status, being self-employee, occupation, marital status, residence, family size, and household relative wealth index.
We hope that the current study will facilitate the implementation of effective healthcare policy by enabling healthcare officials in the area to better understand the knowledge, attitude, and practice done by the Jimma population toward COVID-19.
The raw data supporting the conclusions of this study will be made available by the authors, without undue reservation.
The study protocol was approved by the Institutional Review Board of the Institute of Health, Jimma University and informed consent was obtained from each study participant.
IB, LD, AA, DY, and TG: conceptualization and data collection. IB, LD, AA, DM, DY, and TG: questionnaire preparation and validation. IB, LD, and TG: data analysis. IB, LD, AA, DM, DY, TG, and YW: original draft preparation. LD, AA, DM, and DY: resource and supervision. All authors have read and approved the final manuscript before submission.
The study was funded by Jimma University (Funding Number: IHRPGD228/2020). The funding body was not involved in the design of the study, data collection, analysis, interpretation of data, and writing the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank all people who participated in the study.
1. Elnadi H, Odetokun IA, Bolarinwa O, Ahmed Z, Okechukwu O, Al-Mustapha AI. Correction: knowledge, attitude, and perceptions towards the 2019 coronavirus pandemic: a bi-national survey in Africa. PLoS ONE. (2021) 16:e0247351. doi: 10.1371/journal.pone.0247351
2. Li Y, Guo F, Cao Y, Li L, Guo Y. Insight into COVID-2019 for pediatricians. Pediatr Pulmonol. (2020) 55:E1–4. doi: 10.1002/ppul.24734
3. Geldsetzer P. Use of rapid online surveys to assess people's perceptions during infectious disease outbreaks: a cross-sectional survey on COVID-19. J Med Internet Res. (2020) 22:e18790. doi: 10.2196/18790
4. Reuben RC, Danladi MM, Saleh DA, Ejembi PE. Knowledge, attitudes and practices towards COVID-19: an epidemiological survey in North-Central Nigeria. J Community Health. (2021) 46:457–70. doi: 10.1007/s10900-020-00881-1
5. Zhong B-L, Luo W, Li H-M, Zhang Q-Q, Liu X-G, Li W-T, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. (2020) 16:1745. doi: 10.7150/ijbs.45221
6. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
7. Pokhrel S, Chhetri R. A literature review on impact of COVID-19 pandemic on teaching and learning. High Educ Future. (2021) 8:133–41. doi: 10.1177/2347631120983481
8. Abdullahi L, Onyango JJ, Mukiira C, Wamicwe J, Githiomi R, Kariuki D, et al. Community interventions in low—and middle-income countries to inform COVID-19 control implementation decisions in Kenya: a rapid systematic review. PLoS ONE. (2020) 15:e0242403. doi: 10.1371/journal.pone.0242403
9. Gebretsadik D, Gebremichael S, Belete MA. Knowledge, attitude and practice toward covid-19 pandemic among population visiting dessie health center for covid-19 screening, northeast ethiopia. Infect Drug Resist. (2021) 14:905. doi: 10.2147/IDR.S297047
10. Gebru AA, Birhanu T, Wendimu E, Ayalew AF, Mulat S, Abasimel HZ, et al. Global burden of COVID-19: situational analyis and review. Hum Antibodies. (2021) 29:139–48. doi: 10.3233/HAB-200420
11. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS ONE. (2020) 15:e0233668. doi: 10.1371/journal.pone.0233668
12. Din HM, Adnan RN, Akahbar SA, Minhat HS. Assessment of knowledge, attitudes and practices towards COVID-19 among Malaysian older adults during the pandemic. Asian J Behav Sci. (2021) 3:1–2. Available online at: https://myjms.mohe.gov.my/index.php/ajbs/article/view/12504
13. Hager E, Odetokun IA, Bolarinwa O, Zainab A, Okechukwu O, Al-Mustapha AI. Knowledge, attitude, and perceptions towards the 2019 Coronavirus Pandemic: a bi-national survey in Africa. PLoS ONE. (2020) 15:e0236918. doi: 10.1371/journal.pone.0236918
14. Abdelhafiz AS, Mohammed Z, Ibrahim ME. Knowledge, perceptions, and attitude of egyptians towards the novel coronavirus disease (COVID-19). J Community Health. (2020) 7:1–10. doi: 10.1007/s10900-020-00827-7
15. Taddese AA, Azene ZN, Merid MW, Muluneh AG, Geberu DM, Kassa GM, et al. Knowledge and attitude of the communities towards COVID-19 and associated factors among Gondar City residents, northwest Ethiopia: a community based cross-sectional study. PLoS ONE. (2021) 16:e0248821. doi: 10.1371/journal.pone.0248821
16. Desalegn Z, Deyessa N, Teka B, Shiferaw W, Hailemariam D, Addissie A, et al. COVID-19 and the public response: knowledge, attitude and practice of the public in mitigating the pandemic in Addis Ababa, Ethiopia. PLoS ONE. (2021) 16:e0244780. doi: 10.1371/journal.pone.0244780
17. Shahbaznejad L, Navaeifar MR, Movahedi FS, Hosseinzadeh F, Fahimzad SA, Shirazi ZS, et al. Knowledge, attitude and practice of Sari Birth Cohort members during early weeks of COVID-19 outbreak in Iran. BMC Public Health. (2021) 21:1–2. doi: 10.1186/s12889-021-11039-6
18. Habib MA, Dayyab FM, Iliyasu G, Habib AG. Knowledge, attitude and practice survey of COVID-19 pandemic in Northern Nigeria. PLoS ONE. (2021) 16:e0245176. doi: 10.1371/journal.pone.0245176
19. Sakr S, Ghaddar A, Sheet I, Eid AH, Hamam B. Knowledge, attitude and practices related to COVID-19 among young Lebanese population. BMC Public Health. (2021) 21:1–1. doi: 10.1186/s12889-021-10575-5
20. Bates BR, Tami A, Carvajal A, Grijalva MJ. Knowledge, attitudes, and practices towards COVID-19 among Venezuelans during the 2020 epidemic: an online cross-sectional survey. PLoS ONE. (2021) 16:e0249022. doi: 10.1371/journal.pone.0249022
21. Nguyen HB, Nguyen TH, Tran TT, Vo TH, Tran VH, Do TN, et al. Knowledge, attitudes, practices, and related factors towards COVID-19 Prevention among patients at University Medical Center Ho Chi Minh City, Vietnam. Risk Manag Healthc Policy. (2021) 14:2119. doi: 10.2147/RMHP.S305959
22. Tuppal CP, Ninobla MM, Ruiz MG, Loresco RD, Tuppal SM, Panes II, et al. Knowledge, attitude, and practice toward COVID-19 among healthy population in the Philippines. Nurse Media J Nurs. (2021) 11:61–70. doi: 10.14710/nmjn.v11i1.36067
23. Widayati A. Knowledge, perceptions, and awareness related to COVID-19 among the indonesian adults during the outbreak's escalation period: a cross-sectional online survey in Yogyakarta Province, Indonesia. Asia Pacific J Public Health. (2021) 2021:10105395211001655. doi: 10.1177/10105395211001655
24. Sulistyawati S, Rokhmayanti R, Aji B, Wijayanti SP, Hastuti SK, Sukesi TW, et al. Knowledge, attitudes, practices and information needs during the covid-19 pandemic in indonesia. Risk Manag Healthc Policy. (2021) 14:163. doi: 10.2147/RMHP.S288579
25. Shewasinad Yehualashet S, Asefa KK, Mekonnen AG, Gemeda BN, Shiferaw WS, Aynalem YA, et al. Predictors of adherence to COVID-19 prevention measure among communities in North Shoa Zone, Ethiopia based on health belief model: a cross-sectional study. PLoS ONE. (2021) 16:e0246006. doi: 10.1371/journal.pone.0246006
Keywords: knowledge, attitude, practice, COVID-19, Jimma, Ethiopia
Citation: Bukata IT, Dadi LS, Ayana AM, Mengistu D, Yewal D, Gizaw TS and Woldesenbet YM (2022) Knowledge, Attitudes, and Practice Toward Prevention of COVID-19 Among Jimma Town Residents: A Community-Based Cross-Sectional Study. Front. Public Health 10:822116. doi: 10.3389/fpubh.2022.822116
Received: 26 November 2021; Accepted: 24 March 2022;
Published: 27 April 2022.
Edited by:
José Tuells, University of Alicante, SpainReviewed by:
Dilaram Acharya, Université de Montréal, CanadaCopyright © 2022 Bukata, Dadi, Ayana, Mengistu, Yewal, Gizaw and Woldesenbet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tariku Sime Gizaw, c2VlbmFhbWFxYWFAeWFob28uY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.