
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 18 May 2022
Sec. Public Health Education and Promotion
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.814328
 Raghuram Nagarathna1*
Raghuram Nagarathna1* Manjunath N. K. Sharma1
Manjunath N. K. Sharma1 Judu Ilavarasu1
Judu Ilavarasu1 Ravi Kulkarni1
Ravi Kulkarni1 Akshay Anand2,3,4*
Akshay Anand2,3,4* Vijaya Majumdar1
Vijaya Majumdar1 Amit Singh1
Amit Singh1 Jagat Ram5Manjari Rain2
Jagat Ram5Manjari Rain2 Hongasandra R. Nagendra1
Hongasandra R. Nagendra1The implementation of timely COVID-19 pan-India lockdown posed challenges to the lifestyle. We looked at the impact of lifestyle on health status during the lockdown in India. A self-rated scale, COVID Health Assessment Scale (CHAS) was circulated to evaluate the physical health or endurance, mental health i.e. anxiety and stress, and coping ability of the individuals under lockdown. This is a pan-India cross-sectional survey study. CHAS was designed by 11 experts in 3 Delphi rounds (CVR = 0.85) and was circulated through various social media platforms, from 9th May to 31st May 2020, across India by snowball circulation method. CHAS forms of 23,760 respondents were downloaded from the Google forms. Logistic regression using R software was used to compare vulnerable (>60 years and with chronic diseases) with non-vulnerable groups. There were 23,317 viable respondents. Majority of respondents included males (58·8%). Graduates/Postgraduates (72·5%), employed (33·0%), businessmen (6·0%), and professionals (9·7%). The vulnerable group had significantly (OR 1.31, p < 0.001) higher representation of overweight individuals as compared to non-vulnerable group. Regular use of tobacco (OR 1.62, p = 0.006) and other addictive substances (OR 1.80, p = 0.039) showed increased vulnerability. Respondents who consume junk food (OR 2.19, p < 0.001) and frequently snack (OR 1.16, p < 0.001) were more likely to be vulnerable. Respondents involved in fitness training (OR 0.57, p < 0.001) or did physical works other than exercise, yoga, walk or household activity (OR 0.88, p = 0.004) before lockdown were less likely to be vulnerable. Majority had a very good lifestyle, 94.4% never smoked or used tobacco, 92.1% were non-alcoholic, 97.5% never used addictive substances, 84.7% had good eating habits, 75.4% were vegetarians, 82.8% had “good” sleep, 71.7% did physical activities. Only 24.7% reported “poor” coping ability. Depression with somewhat low feeling were more likely to be vulnerable (OR 1.26, p < 0.001). A healthy lifestyle that includes healthy eating, proper sleep, physical activeness and non-addictive habits supports better coping ability with lesser psychological distress among Indian population during lockdown.
The past two decades have witnessed three highly pathogenic, novel zoonotic CoVs, first SARS-CoV-1 was recognized in 2002, followed by MERS-CoV in 2012 and now as a more virulent strain, the SARS-CoV-2 causing COVID-19 (1). Based on the estimated report of the instantaneous reproduction number (Rt) on the severity in China, several countries implemented social distancing, hygiene etiquettes, contact tracing, wearing face masks, temperature checks, and avoided premature relaxation of the lockdown (2). The largest timely lockdown was enforced in India after its first case on 30th Jan 2020 (3).
The present COVID-19 pandemic affected global mental health, as evidenced initially by panic-buying, worldwide. Following any natural disaster, survivors are prone to develop post-traumatic stress disorder (PTSD). For instance, survivors of the August 2008 floods in India (Bihar) had shown higher scores for PTSD (4). Similarly, studies in China showed high level of depression with low health-related quality of life (HRQoL) and high scores on PTSD symptoms with no significant changes during COVID-19 (5, 6).
The first large-scale community-based cohort study on 387,109 adults in UK concluded that an unhealthy lifestyle (smoking, physical inactivity, obesity, and excessive alcohol intake) is a risk factor for hospital admission for COVID-19 (7). A study on Italian children observed increased screen time and sleep time, increased consumption of potato chips, red meat, and sugary drink and decrease in time spent in sports activities, which may have lasting impact on adiposity (8). The incidence, progression and death rate during this pandemic in India seems to be much lesser than other countries [COVID-19 Worldwide Dashboard | WHO Live World Statistics]. The reasons being India's relatively younger population, early biggest national lockdown (9), and a unique mutation in the spike surface glycoprotein [A930V (24351C > T)] in the Indian SARS-CoV-2 (10). A recent survey in Indian cohort showed that the level of psychological distress was lesser than the Chinese population on IES-R (11). There are unpublished observations that the traditional life style of the Indian families may also be a contributory factor. As there were no nationwide studies looking at the impact of life style on vulnerability during first wave and lockdown, we executed this pan-India on-line survey. The objective of the study was to investigate physical and mental health, lifestyle and to examine activities adapted by people to cope with COVID-19and lockdown.
This was a nationwide survey on general Indian population during the 3rd phase of lockdown for COVID-19 pandemic that had respondents from all States/Union Territories except Ladakh and Lakshadweep. COVID Health Assessment Scale (CHAS), prepared in 10 languages by a committee of 11 experts through 3 Delphi rounds [Content Valid Ratio (CVR) was 0.85], had questions related to life style behavior (exercise, diet, additive substances, and sleep), physical health (BMI, chronic diseases, and endurance), mental health (fear, anxiety, depression, stress), and coping ability [refer to CHAS questionnaire from reference (12)]. Endurance under physical health signifies durability or ability to perform physical work for longer duration of time without feeling breathlessness. Further, coping ability is defined as conscious and unconscious efforts and strategies acquired by respondents such as reading, cooking and others to reduce emotional impact of challenging situation created by pandemic and lockdown.
Phone calls and special requests were sent to different sections of the society (~200 universities, corporate companies, healthcare institutions, government organizations, wellness centers, and their networks) to acquire data by snowball method. Participants filled the online forms, if they were willing to answer the subjected questions. Hence, there were no exclusion and inclusion criteria for participants.
The responses were collected from May 9, 2020 to May 31, 2020. Responses from non-Indians and aged <18 years were not considered for analysis. After quality control, the participants were divided into vulnerable and non-vulnerable groups based on presence of co-morbidities and age >60 years. Respondents were considered vulnerable when their age was above 60 years and/or they have any chronic disease as these two conditions increases the risk of getting infected with COVID-19 and risk of severe outcome. For zone wise analyses, the 34 states/UTs were divided into 3 zones based on the number of positive cases in the state as on 31st May 2020 (source: Ministry of health and Family Welfare, Government of India). The groups were red zone (>10,000 cases including Maharashtra, Tamil Nadu, Delhi, Gujarat), orange zone (5,000 to 10,000 cases including Rajasthan, Madhya Pradesh, Uttar Pradesh), and green zone (<5,000 cases including remaining states and UTs).
The CHAS data received from the Google drive in ten languages were combined into one dataset. R Statistical software, version 4.0.0, was used for data cleaning, extraction, and analyses. Incomplete and unreliable responses were excluded. Logistic regression was used to compare respondents under two categories viz. vulnerable and non-vulnerable. Arsenal package was used to test significance on cross tabulations on categorical variables. Reference for Odd's ratio (OR) calculation was set to sequential contrast for all ordinal variables and first row and first column for nominal variables.
Of the 23,760 respondents, participants from other countries (n = 401) and marked as other genders (n = 42) were excluded. Data was analyzed for 23,317 respondents. Logistic regression to compare 4,416 vulnerable participants with 18,901 non-vulnerable participants showed that graduates (OR 0.77, p < 0.001) were less likely to and postgraduates (OR 1.11, p = 0.027) were more likely to be associated with vulnerability than non-graduates (Table 1). Students were less likely to be associated with vulnerability than agriculturists (OR 0.26, p < 0.001). Businessmen (OR 1.87, p < 0.001), homemakers (OR 2.91, p < 0.001), professionals (OR 1.72, p < 0.001) and those in other occupations (OR 1.40, p = 0.005) were more likely to be vulnerable as compared to agriculturists (Table 1). Of note, only 3.2% were agriculturists and 48.7% were actively working professionals (6.0% business, 9.7% professionals, 33.0% employees) among the total respondents.
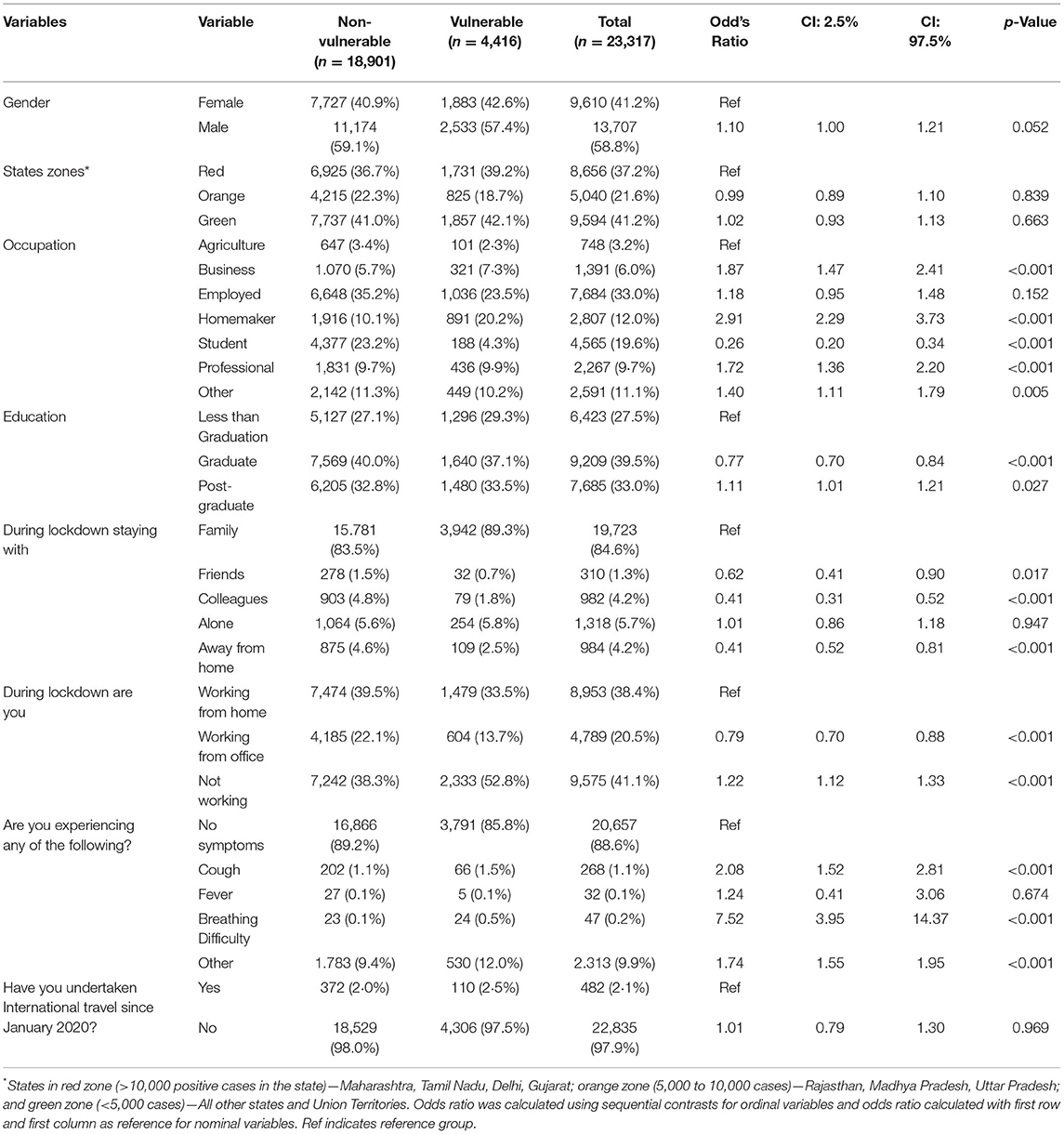
Table 1. Comparison of demographic details of vulnerable with non-vulnerable groups.
During the lockdown, those who were not working were more vulnerable than who worked from home (OR 1.22, p < 0.001). Those who had stayed away from home (OR 0.41, p < 0.001) or with friends (OR 0.62, p = 0.017) or colleagues (OR 0.41, p < 0.001) were less likely to be in the vulnerable group as they were younger and did not have illnesses. Individuals experiencing symptoms like cough (OR 2.08, p < 0.001), breathing difficulty (OR 7.52, p < 0.001) and others (OR 1.74, p < 0.001), except fever, were more likely to be vulnerable (Table 1).
Table 2 summarizes the life style variables. Good eating habits was reported by 84.7% and strict vegetarian diet was reported by 75.4% of the total respondents. Vulnerable group had better eating habit (0.89, p = 0.032) and more strict vegetarians (OR 0.49, p < 0.001). However, consumption of junk food (OR 2.19, p < 0.001) and frequent snacking (OR 1.16, p < 0.001) was positively associated with vulnerability.
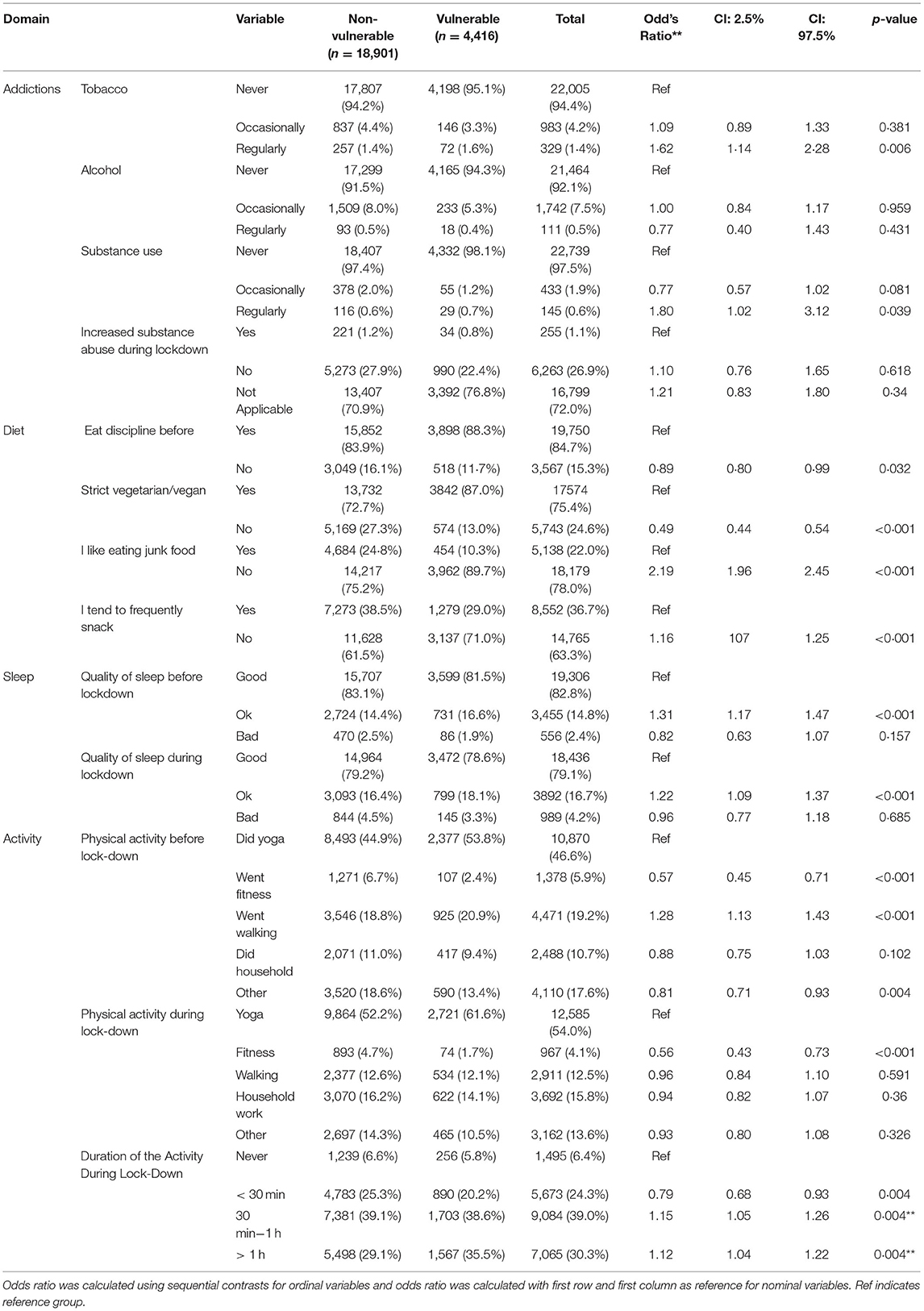
Table 2. Lifestyle in vulnerable and non-vulnerable groups.
Substance users were minimal in this cohort as majority said they “never” used tobacco (94.4%), or alcohol (92.1%) or other substances (97.5%) before lockdown; only 1.1% “agreed” they had increased the use of alcohol and tobacco during lockdown. Regular consumers of tobacco (OR 1.62, p = 0.006) and other substance users (very few in this cohort; OR 1.80, p = 0.039) were more likely to be vulnerable.
Looking at the quality of sleep, 82.8% and 79.1% said they had “good” sleep quality before and during lockdown, respectively in total respondents. Those who had average sleep before (OR 1.31, p < 0.001) or during (OR 1.22, p < 0.001) lockdown were more likely to be vulnerable than those who had good sleep. Individuals having bad sleep quality had increased from 2.4% to 4.2% during lockdown among total respondents.
Logistic regression further showed that those who went for fitness training (OR 0.57, p < 0.001) or did works other than exercise, yoga, walk or household activity (OR 0.88, p = 0.004) before lockdown were less likely to be vulnerable. Walking before lockdown did not reduce the risk of vulnerability (OR 1.28, p < 0.001). Individual practicing fitness training during the lockdown were less likely to be vulnerable (OR 0.56, p < 0.001). Very few individuals never did any physical activity during lockdown. Those who were involved in physical activity for <30 min (OR 0.79, p = 0.004) or for 30 to 60 min (OR 1.15, p = 0.004) were more in non-vulnerable group. Individuals involved in physical activity for more than an hour were more in vulnerable group (OR 1.12, p = 0.004). It is to be noted that 54.0% did yoga during lockdown while 46.6% were already practicing yoga (before lockdown).
Majority had “good/average” endurance as marked on a 3 point scale (good, average, and bad). Respondents with average (OR 1.72, p < 0.001) and bad (OR 1.55, p = 0.014) endurance were more likely to be vulnerable than respondents who had good endurance. BMI was high in vulnerable group at 25·49 ± 4·34 kg/m2 than non-vulnerable at 24·05 ± 4·31 kg/m2 group (p < 0.001). The BMI between 23 and 24.9 kg/m2 (OR 1.63, p < 0.001) and above 25 kg/m2 (OR 1.31, p < 0·001) were more likely to be vulnerable (Table 3).
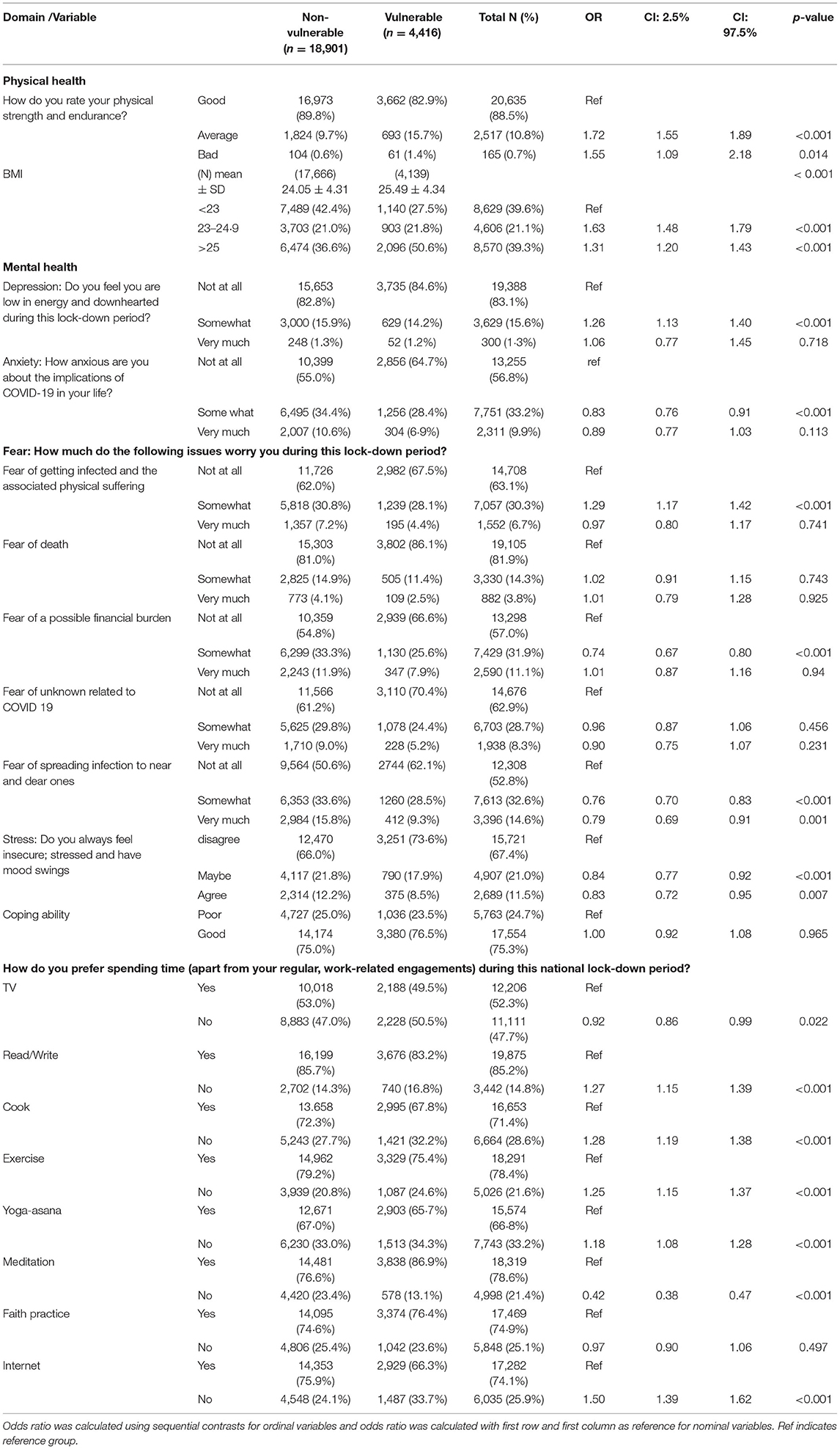
Table 3. Comparison of health and coping between vulnerable and non-vulnerable groups.
Majority did not feel depressed (low feeling) in vulnerable group. Those with depression with somewhat low feeling were more likely to be vulnerable (OR 1.26, p < 0.001) (Table 3). Anxiety about implication of COVID-19 on life did not associate with increased vulnerability. Interestingly, who were “somewhat anxious” were less likely to be vulnerable (OR 0.83, p < 0.001) (Table 3).
We enquired on five aspects of fear. Fear of getting infected with COVID-19 and associated physical suffering was associated with vulnerability (OR 1.29, p < 0.001). Concerns about financial implications (OR 0.74, p < 0.001) and fear of infecting near and dear ones (OR 0.76, p < 0.001 for somewhat; OR 0.79, p = 0.001 for very much) were not associated with vulnerability (Table 3).
About 21% of the respondents were not sure about stress and insecurity, which did not associated with vulnerability (OR 0.84, p < 0.001). Those who agreed that they were stressed and insecure were less likely to be in vulnerable category (OR 0.83, p = 0.007).
Coping ability was good in 75.3% and poor in 24.7% of the total respondents but was non-significant between vulnerable and non-vulnerable respondents.
Those who did not spend time reading (OR 1.27, p < 0.001) or cooking activity (OR 1.28, p < 0.001) or spend time on exercise (OR 1.25, p < 0.001), or did not do Yogasana (OR 1.18, p < 0.001) were more likely to be vulnerable (Table 3). The respondents who spend less time on internet were more likely to be vulnerable (OR 1.50, p < 0.001).
This first largest pan-India online survey, during the third phase of nation-wide Indian lockdown, looked at the life style, physical health, mental health and the coping abilities using logistic regression.
There is a well-established association between old age and co-morbidities such as hypertension (30%), diabetes (19%), and coronary heart disease (8%) with risk of COVID-19 infection (13–15). UK risk factor estimates had shown a dose-dependent increase in risk of COVID-19 with 4-fold higher risk in individuals with most adverse life style (51% of severely infected cases) compared to those with optimal lifestyle (7). Although our survey did not target COVID-19 positive cases, we looked at the potential associations between life style correlates of respondents, vulnerable to COVID-19 infection, with the non-vulnerable.
We observed similar gender distribution among vulnerable and non-vulnerable. However, it is reported that males are more vulnerable (13). Graduates/post graduates and those who had employment or business were more likely to be vulnerable than unemployed persons or agriculturists, who are physically active, similar to observations in China (16). This observation indicates that individuals having stressful job in urban regions make them vulnerable. It is important to state here that individuals residing in urban regions are at risk of getting infected, where day to day physical contact with each other is high, such as at offices, institutes, colleges, airport, markets, due to fast-pace life style. Good lifestyle before lockdown seems to have contributed to adopting healthy activities (reading, writing, cooking, yoga, exercise, and household) with good psychological coping ability during lockdown. Higher education and good life style seen in this cohort may not reflect the lifestyle or the behavioral characteristics of the general Indian population. The limitation being that response to a call on social media may reflect the social responsibility of those with good life style by responding voluntarily to this unstructured survey.
A healthy diet, rich in fruits and vegetables and low in sugar and calorie-dense processed foods, is essential to health, which was observed in majority of our respondents with majority being strict vegetarians. Diet rich in saturated fat, refined carbohydrates, and sugars with low levels of fiber that promotes obesity and type-2 diabetes poses increased risk for severe COVID-19 pathology and mortality by inhibiting adaptive immune system (17).
In a study, during the present pandemic, the prevalence of clinical insomnia in France was 19%, close to prevalence reported in China (20·1%) and Italy (19·8%) but lower than in Greece (37·6%) (18–21). We observed much lower prevalence with only 2·4% and 4·2% respondents reporting “bad” insomnia before and during lockdown. This appears to be because of the milder form of the disease in India and good family support.
Studies have observed that past or current smokers (18%) with COVID-19 had double the risk of progression to severe disease compared with never-smokers (9%) (22, 23). A small percentage (1.1%) who agreed that they had increased the consumption of addictive substances during lockdown did show increased vulnerability.
Further, obesity is known to be an important contributor for many non-communicable diseases and also for respiratory and other infections (17). Pietrobelli et al. reported that children during social isolation in Italy gained weight which may have long term implications (8). We observed that the vulnerable group had higher representation of overweight individuals as compared to non-vulnerable group. Higher BMI denotes disturbed metabolism and an overall inflammatory state that could further increase the likelihood of COVID-19 infection in the vulnerable individuals (24).
Physical activity maintaining regular exercise with good physical endurance counteracts the negative effects of the pandemic stress on immune competency (25). In the present study, 71.7% did physical activities and those who did not do exercises and reported poor physical endurance were more likely to be vulnerable. Yoga, practiced by 54.0% of our respondents during lockdown, is an unexpected observation of this study (Table 2). Duggal et al. observed that exercise augments host immune defenses by catecholamine-mediated preferential mobilization of lymphocytes primed to recognize and kill virus-infected cells (26). Exercise also enhances proliferation of virus-specific memory T-cells and promotes their mobilization to the site.
A meta-analysis of 65 studies during severe infections of SARS had noted that apart from the immediate mental health effects, PTSD could emerge at a later stage (27). “Somewhat” depressive low feeling and anxiety was noted in 15.6% and 33.2%, respectively while 1.3% and 9.9% were “very much” depressed and anxious, respectively. Similar observations have been reported by studies during this pandemic using different psychological battery. The first mental health survey in India during the initial phase of pandemic showed 33.2% had significant (mild/moderate/severe) psychological impact (11). Qiu et al. reported 29% had mild to moderate and 5% had severe psychological distress in China (28). Wang et al. reported psychological impact in higher percentage (53.8%) of respondents with higher stress scores that remained high in the 4th week (5). Thus, anxiety (28.8% in Wang et al. vs. 9·9% in present study) and depression (16·5% in Wang et al. vs. 1·3% in present study) seemed to be higher in China. This may be attributed to the good lifestyle in our respondents with higher educational level. In another Indian study, Rehman et al. observed that people who do not have enough supplies to sustain the lockdown were most affected and the affluent were negatively correlated with psychological distress (29).
A smaller percentage of respondents in our study were stressed (11.5%) or expressed “very much” fear of death (3.8%) or getting infected (6.7%) or financial burden (11.1%) as compared to Chinese respondents with high level of education (75%) similar to our cohort (72.5%), who experienced higher levels of stress (52.1% felt horrified and apprehensive) (15). Milder form of the disease, stricter lockdown and higher family support in Indian community may explain this difference.
The growing stress highlights the importance of funding translational and alternative medicine research (30) over fundamental research in vitro (31), in vivo (32–36) and biomarker studies (37–41), which is often restricted to publications. Translating this knowledge into practice may accelerate the pace of discovery and practice of integrative medicine. Several online surveys were conducted in India during this period; however, these surveys reported data on a small sample size (42–44), specific cohort (43, 45, 46), selective parameters such as psychological or life style or coping strategy (41, 44, 45, 47–49) as compared to our study. Another uniqueness of this study is that we used Delphi protocol to develop CHAS questionnaire for the survey.
Although, this survey was aimed at general population, the responses were received by only those with high level of education which prevents us from drawing any conclusion related to Indian race in general.
CHAS was prepared to suit the research question as we did not find a scale that had all the components we planned to assess. As the scale was self-reported, social desirability factor influencing the answers may be a limitation.
This is the first nationwide large scale health survey, covering 34 states of India during the 3rd phase of lockdown of COVID-19 pandemic that shows that those with a good lifestyle including good eating, sleeping, and non-addictive habits with good physical activities adopt good coping abilities during the challenging times of life, irrespective of gender. Increased weight, unhealthy food, addictions and history of international travel increase the risk of getting infected with COVID-19 in vulnerable individuals. This study provides evidence for the media, policy makers and general population to include good life style recommendations for prevention.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Swami Vivekananda Yoga Anusandhana Samsthana, Bengaluru, India. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
RN: concept, design, definition of intellectual content, literature search, manuscript preparation, manuscript editing, manuscript review, and guarantor. MS: concept, design, definition of intellectual content, manuscript preparation, manuscript editing, and manuscript review. RK: concept, design, definition of intellectual content, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing, and manuscript review. JI: concept, design, definition of intellectual content, data acquisition, data analysis, statistical analysis, manuscript editing, and manuscript review. AA: concept. VM: design, definition of intellectual content, literature search, data acquisition, manuscript editing, and manuscript review. AS: concept, design, definition of intellectual content, literature search, data acquisition, manuscript editing, and manuscript review. JR and MR: manuscript editing and manuscript review. HN: concept, design, definition of intellectual content, data acquisition, manuscript editing, and manuscript review. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lipsitch M, Swerdlow DL, Finelli L. Defining the epidemiology of Covid-19 - studies needed. N Engl J Med. (2020) 382:1194–6. doi: 10.1056/NEJMp2002125
2. Xu S, Li Y. Beware of the second wave of COVID-19. Lancet. (2020) 395:1321–2. doi: 10.1016/S0140-6736(20)30845-X
3. Andrews MA, Areekal B, Rajesh KR, Krishnan J, Suryakala R, Krishnan B et al. First confirmed case of COVID-19 infection in India: a case report. Indian J Med Res. (2020) 151:490–2. doi: 10.4103/ijmr.IJMR_2131_20
4. Telles S, Singh N, Joshi M. Risk of posttraumatic stress disorder and depression in survivors of the floods in Bihar, India. Indian J Med Sci. (2009) 63:330–4. doi: 10.4103/0019-5359.55883
5. Wang C, Pan R, Wan X, Tan Y, Xu L, McIntyre RS, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. (2020) 87:40–8. doi: 10.1016/j.bbi.2020.04.028
6. Tian F, Li H, Tian S, Yang J, Shao J, Tian C. Psychological symptoms of ordinary Chinese citizens based on SCL-90 during the level I emergency response to COVID-19. Psychiatry Res. (2020) 288:112992. doi: 10.1016/j.psychres.2020.112992
7. Hamer M, Kivimäki M, Gale CR, Batty GD. Lifestyle risk factors, inflammatory mechanisms, and COVID-19 hospitalization: a community-based cohort study of 387,109 adults in UK. Brain Behav Immun. (2020) 87:184–7. doi: 10.1016/j.bbi.2020.05.059
8. Pietrobelli A, Pecoraro L, Ferruzzi A, et al. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in Verona, Italy: a longitudinal study. Obesity (Silver Spring). (2020) 28:1382–85. doi: 10.1002/oby.22861
9. The Lancet. India under COVID-19 lockdown. Lancet. (2020) 395:1315. doi: 10.1016/S0140-6736(20)30938-7
10. Gupta R, Misra A. COVID19 in South Asians/Asian Indians: heterogeneity of dta and implications for pathophysiology and research. Diabetes Res Clin Pract. (2020) 165:108267. doi: 10.1016/j.diabres.2020.108267
11. Varshney M, Parel JT, Raizada N, Sarin SK. Initial psychological impact of COVID-19 and its correlates in Indian Community: an online (FEEL-COVID) survey. PLoS ONE. (2020) 15:e0233874. doi: 10.1371/journal.pone.0233874
12. Nagarathna R, Anand A, Rain M, Srivastava V, Sivapuram MS, Kulkarni R et al. Yoga practice is beneficial for maintaining healthy lifestyle and endurance under restrictions and stress imposed by lockdown during COVID-19 pandemic. Front Psychiatry. (2021) 12:613762. doi: 10.3389/fpsyt.2021.613762
13. Clark A, Jit M, Warren-Gash C, Guthrie B, Wang HHX, Mercer SW et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modelling study. Lancet Glob Health. (2020) 8:e1003–17.
14. Schiffrin EL, Flack JM, Ito S, Muntner P, Webb RC. Hypertension and COVID-19. Am J Hypertens. (2020) 33:373–4. doi: 10.1093/ajh/hpaa057
15. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult in patients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
16. Zhang Y, Ma ZF. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: a cross-sectional study. Int J Environ Res Public Healt. (2020) 17:2381. doi: 10.3390/ijerph17072381
17. Belanger MJ, Hill MA, Angelidi AM, Dalamaga M, Sowers JR, Mantzoros CS. Covid-19 and disparities in nutrition and obesity. N Engl J Med. (2020) 383:e69. doi: 10.1056/NEJMp2021264
18. Kokou-Kpolou CK, Megalakaki O, Laimou D, Kousouri M. Insomnia during COVID-19 pandemic and lockdown: prevalence, severity, and associated risk factors in France population. Psychiatry Res. (2020) 290:113128. doi: 10.1016/j.psychres.2020.113128
19. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. (2020) 288:112954. doi: 10.1016/j.psychres.2020.112954
20. Rossi R, Socci V, Pacitti F, Di Lorenzo G, Di Marco A, Siracusano A, et al. Mental health outcomes among frontline and second-line health care workers during the Coronavirus Disease 2019 (COVID-19) pandemic in Italy. JAMA Netw Open. (2020) 3:e2010185. doi: 10.1001/jamanetworkopen.2020.10185
21. Voitsidis P, Gliatas I, Bairachtari V, Papadopoulou K, Papageorgiou G, Parlapani E et al. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatry Res. (2020) 289:113076. doi: 10.1016/j.psychres.2020.113076
22. Young K. COVID-19: Smoking / Convalescent Plasma / Asthma / Poison Control Center Calls. (2020). Available online at: https://www.jwatch.org/fw116556/2020/04/16/covid-19-smoking-convalescent-plasma-asthma-poison (accessed September 11, 2020).
23. Patanavanich R, Glantz SA. Smoking is associated with COVID-19 progression: a meta-analysis. Nicotine Tob Res. (2020) 22:1653–56. doi: 10.1093/ntr/ntaa082
24. GBD 2015 Obesity Collaborators, Afshin A, Forouzanfar MH, Reitsma MB, Sur P, Estep K, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. (2017) 377:13–27. doi: 10.1056/NEJMoa1614362
25. Chen P, Mao L, Nassis GP, Harmer P, Ainsworth BE Li F. Coronavirus disease (COVID-19): the need to maintain regular physical activity while taking precautions. J Sport Health Sci. (2020) 9:103–4. doi: 10.1016/j.jshs.2020.02.001
26. Duggal NA, Niemiro G, Harridge SD, Simpson RJ, Lord JM. Can physical activity ameliorate immunosenescence thereby reduce age-related multi-morbidity? Nat Rev Immunol. (2019) 19:563–72. doi: 10.1038/s41577-019-0177-9
27. Rogers JP, Chesney E, Oliver D, Pollak TA, McGuire P, Fusar-Poli P, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:611–27. doi: 10.1016/S2215-0366(20)30203-0
28. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y, et al. nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatr. (2020) 33:e100213. doi: 10.1136/gpsych-2020-100213
29. Rehman U, Shahnawaz MG, Khan NH, Kharshiing KD, Khursheed M, Gupta K et al. Depression, anxiety and stress among Indians in times of Covid-19 lockdown. Community Ment Health J. (2021) 57:42–8. doi: 10.1007/s10597-020-00664-x
30. Mathur D, Goyal K, Koul V, Anand A. The molecular links of re-emerging therapy: a review of evidence of Brahmi (Bacopa monniera). Front pharmacol. (2016) 7:44. doi: 10.3389/fphar.2016.00044
31. Abburi C, Prabhakar S, Kalra J, Huria A, Anand A. Vascular endothelial growth factor (VEGF) induced proliferation of human fetal derived ciliary epithelium stem cells is mediated by jagged-N cadherin pathway. Curr Neurovasc Res. (2013) 10:93–102. doi: 10.2174/1567202611310020002
32. Bammidi S, Bali P, Kalra J, Anand A. Transplantation efficacy of human ciliary epithelium cells from fetal eye and Lin-ve stem cells from umbilical cord blood in the murine retinal degeneration model of laser injury. Cell Transplant. (2020) 29:0963689720946031. doi: 10.1177/0963689720946031
33. Bali P, Bammidi S, Banik A, Nehru B, Anand A. CD34 and CD117 Stemness of lineage-negative cells reverses memory loss induced by amyloid beta in mouse model. Front Behav Neurosci. (2018) 12:222. doi: 10.3389/fnbeh.2018.00222
34. Kumar S, Modgil S, Bammidi S, Minhas G, Shri R, Kaushik S, et al. Allium cepa exerts neuroprotective effect on retinal ganglion cells of pterygopalatine artery (PPA) ligated mice. J Ayurveda Integr Med. (2020) 11:489–94. doi: 10.1016/j.jaim.2019.08.002
35. Saraf MK, Prabhakar S, Khanduja KL, Anand A. Bacopa monniera attenuates scopolamine-induced impairment of spatial memory in mice. Evid Based Complement Alternat Med. (2011) 2011:236186. doi: 10.1093/ecam/neq038
36. Anand A, Saraf MK, Prabhakar S. Antiamnesic effect of B. monniera on L-NNA induced amnesia involves calmodulin. Neurochem Res. (2010) 35:1172–81. doi: 10.1007/s11064-010-0171-x
37. Sharma NK, Gupta A, Prabhakar S, Singh R, Sharma SK, Chen W, et al. Association between CFH Y402H polymorphism and age related macular degeneration in North Indian cohort. PLoS ONE. (2013) 8:e70193. doi: 10.1371/journal.pone.0070193
38. Kaur I, Katta S, Reddy RK, Narayanan R, Mathai A, Majji AB et al. The involvement of complement factor B and complement component C2 in an Indian cohort with age-related macular degeneration. Invest Ophthalmol Vis Sci. (2010) 51:59–63. doi: 10.1167/iovs.09-4135
39. Anand A, Thakur K, Gupta PK. ALS and oxidative stress: the neurovascular scenario. Oxid Med Cell Longev. (2013) 2013:635831. doi: 10.1155/2013/635831
40. Vinish M, Prabhakar S, Khullar M, Verma I, Anand A. Genetic screening reveals high frequency of PARK2 mutations and reduced Parkin expression conferring risk for Parkinsonism in North West India. J Neurol Neurosurg Psychiatry. (2010) 81:166–70. doi: 10.1136/jnnp.2008.157255
41. Sharma NK, Gupta A, Prabhakar S, Singh R, Sharma S, Anand A. Single nucleotide polymorphism and serum levels of VEGFR2 are associated with age related macular degeneration. Curr Neurovasc Res. (2012) 9:256–65. doi: 10.2174/156720212803530681
42. Akhouri D, Madiha M, Ahmed J. COVID-19 lockdown: online survey of psychosocial factors of adolescents. Ind Psychiatry J. (2021) 30:S45–51. doi: 10.4103/ipj.ipj_32_20
43. Singh GP, Arun P. Subjective well-being among migrant workers residing in a shelter home during lockdown: a pilot survey from North India. Prim Care Companion CNS Disord. (2021) 24:21m02991. doi: 10.4088/PCC.21m02991
44. Singh VV, Patra P, Singal A. Coping with COVID: cross-sectional study to assess the psychological impact and coping strategies utilized by Indian internet users during the lockdown of the COVID-19 pandemic. Ind Psychiatry J. (2021) 30:29–35. doi: 10.4103/ipj.ipj_202_20
45. Gupta N, Luthra A, Shailaja B, Chaudhury S, Saldanha D. Impact of COVID-19 pandemic on mental health of health-care workers in a tertiary care teaching and dedicated COVID-19 hospital. Ind Psychiatry J. (2021) 30:S56–62. doi: 10.4103/0972-6748.328790
46. Verma SK, Kumar BD, Singh N, Kumari P, Ranjan M, Verma A. The impact of COVID-19-induced factors on “work from home” of employees. J Pharm Bioallied Sci. (2021) 13:S1000–2. doi: 10.4103/jpbs.jpbs_247_21
47. Ghosh R, Jana PK, Bhattacharya S, Mallik S. Understanding social problems during lockdown and its relationship to perceived stress - An online survey among adult residents of India. J Family Med Prim Care. (2021) 10:3625–31. doi: 10.4103/jfmpc.jfmpc_2519_20
48. Grover S, Sahoo S, Mehra A, Avasthi A, Tripathi A, Subramanyan A, et al. Psychological impact of COVID-19 lockdown: an online survey from India. Indian J Psychiatry. (2020) 62:354–62. doi: 10.4103/psychiatry.IndianJPsychiatry_427_20
Keywords: COVID-19, public health, stress, coping strategy, lockdown
Citation: Nagarathna R, Sharma MNK, Ilavarasu J, Kulkarni R, Anand A, Majumdar V, Singh A, Ram J, Rain M and Nagendra HR (2022) Coping Strategy, Life Style and Health Status During Phase 3 of Indian National Lockdown for COVID-19 Pandemic—A Pan-India Survey. Front. Public Health 10:814328. doi: 10.3389/fpubh.2022.814328
Received: 13 November 2021; Accepted: 06 April 2022;
Published: 18 May 2022.
Edited by:
Larry K. Olsen, Logan University, United StatesReviewed by:
Parmeshwar Satpathy, Indian Institute of Technology Kharagpur, IndiaCopyright © 2022 Nagarathna, Sharma, Ilavarasu, Kulkarni, Anand, Majumdar, Singh, Ram, Rain and Nagendra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raghuram Nagarathna, cm5hZ2FyYXRuYUBnbWFpbC5jb20=; cm5hZ2FyYXRuYUBzdnlhc2EuZWR1Lmlu; Akshay Anand, YWtzaGF5MWFuYW5kQHJlZGlmZm1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.