 Jing Wu1
Jing Wu1 Rafael Pérez-Escamilla
Rafael Pérez-Escamilla Yifei Hu
Yifei Hu- 1School of Agroforestry & Medicine, the Open University of China, Beijing, China
- 2Obstetrics Department, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, China
- 3Yale School of Public Health, Yale University, New Haven, CT, United States
- 4Department of Child, Adolescent health and Maternal health, School of Public Health, Capital Medical University, Beijing, China
Background: Previous studies have found that the rates of cesarean preference were much lower than the actual rates of cesarean births in China. We aimed to observe this inconsistency between preferred and actual modes of delivery and the factors associated with the inconsistency.
Methods: We conducted a prospective cohort study at the maternity hospital with the largest number of deliveries in Beijing. We collected data through a questionnaire applied in the outpatient department, and medical records from the hospital's information system. Unconditional logistic regression was used to identify factors influencing the inconsistency between preferred and actual delivery mode.
Results: The rates of actual cesarean section and of cesarean preference were 41 and 17%, respectively (χ2 = 82.9, P < 0.0001). The overall inconsistency rate was 31%, with 119 women preferred vaginal delivery but experienced cesarean section, accounting for 67% women undergoing cesarean section. Risk factors for this inconsistency between preferred vaginal delivery and actual cesarean section included: maternal obesity, receiving assisted reproduction, having an abnormal amniotic fluid volume, and fetal distress. Pre-labor rupture of membranes was a unique factor associated with such inconsistency between cesarean section preference and vaginal delivery at delivery.
Conclusions: The inconsistent rate between preferred delivery at late pregnancy and actual delivery is high in China. Further research is needed to understand how to lower cesarean rates in China, taking maternal preferences for vaginal deliveries into account.
Introduction
Cesarean section (CS) rates have increased dramatically in recent years globally, with wide ranges across countries (1, 2), and with China having one of the highest CS rates in the world (3). Previous studies conducted in China have shown that the overall CS rate nationwide increased from 2% in the 1960–70s to 36.7% in 2018 (3, 4). Interestingly, there is wide geographical variation in CS rates within China (5). Indeed, the CS has kept in a downward tendency in metropolitan areas, while being accompanied increases and high CS rates in small and middle cities and rural areas (5, 6). As a result, the overall CS rate in China of 36.7% (4) is almost 4-fold the CS rate of 10% recommended by World Health Organization (WHO) (7), based on minimizing maternal and perinatal mortalities (8, 9).
The risk factors for CS vary across countries and across time within a country (10–13). These risk factors can be classified into four categories: maternal, maternal-fetal, fetal, and social. It is important to note that CS delivery on maternal request (CDMR) explains about 24% of all CS in China (14). Interestingly, primiparous women are now more likely to prefer a vaginal delivery (VD) than a CS delivery under the two-child policy (15). Furthermore, since 2011, the government of China has invested in maternal care monitoring systems to bring down the excessive CS rates (15, 16). This is likely to explain the CS declines in big cities of China. However, starting in 2016, which is the initial year of universal two-child policy, a non-significant increase was found in Wuhan, China (17).
As indicated above, maternal and fetal factors play important roles in the increases in CS rates globally. These risk factors include older maternal age, higher household income, having medical insurance, higher educational attainment, multiple pregnancies, large neonatal weight, maternal obesity, placenta previa, fetal malpresentation, and preterm delivery (3, 18). On the one hand, the preferred mode of delivery predicted the actual delivery route (19, 20). As expected, there was a higher cesarean rate in women preferring cesarean than in those preferring VD (21, 22). On the other hand, the CS preference rates were much lower than the actual CS rates (13, 21, 23). A study reported an increased preference for CS among Chinese women asked about it during pregnancy compare to after childbirth (10% vs. 28%) (24). This finding strongly suggests that the actual delivery of mode drove this preference change. Hence, the main objective of this prospective study is to identify the factors associated with the inconsistency between how the mothers initially prefer for their babies to be delivered and how they are actually given birth. We expect that findings from this study will inform policy to lower CS rate.
Methods
This prospective study was conducted from April to September, 2014 in the largest maternity hospital in Beijing, which is a teaching hospital affiliated to Capital Medical University, and a WHO Collaborating Center for Research and Training. This study was reviewed and approved by the Institutional Review Board at Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, China.
The participants were recruited in the outpatient departments of the hospital. The eligibility criteria for this study were: singleton pregnancy, maternal age ≥18 years, gestation age between 28 and 37 weeks, and delivery in the study hospital. We collected data using a self-administrated structured-questionnaire and by extracting medical records information from the hospital information system. Trained health staff interviewed the women and performed the clinical data extraction. Once the identified personal information was used to link the questionnaire with medical information data and merged into one file, it was de-identified for further data analysis.
The variables examined included socio-demographics (parity, gravidity, age, education, place of residence, household income, and medical insurance), and childbirth preference (preferring CS/preferring VD) (25). The clinical data included the actual mode of delivery, the indications for CS (including CDMR), the maternal height and weight before/on the day of delivery, gestational age at delivery, fetal presentation, neonatal weight, length of hospital stay, amniotic fluid volume, as well as the presence of postpartum hemorrhage, assisted reproduction, fetal dysplasia, placenta previa, pre-labor membrane rupture (PROM), hysteromyoma at pregnancy, fetal distress, gestational diabetes, gestational hypertension, and previous CS. Although CDMR was not encouraged in our study period, doctors respected the choice by women who requested CS and relaxed the indications of CS for them. Body mass index (BMI) upon enrollment was used to classify the pregnant women into four groups: underweight (< 18.5 kg/m2), healthy weight (18.5–23.9 kg/m2), overweight (24–27.9 kg/m2), obesity (≥ 28 kg/m2) (26). Preterm delivery was classified as a gestational age <37 weeks. Postpartum hemorrhage was defined as blood loss >500 ml within the first 24 h after delivery. Amniotic fluid volume was monitored and categorized as polyhydramnios, exceeding 2,000 ml; oligohydramnios, <300 ml; or normal volume, between 300 and 2,000 ml.
The inconsistency between the preferred and the actual delivery mode was defined as the change from preferring VD during the third trimester to actual CS at the delivery or vice versa. In contrast, the consistency was defined as no change between preferred and actual childbirth.
Statistical power was determined to be more than 95% based on a sample size of 400 women to detect a 5% difference of our primary outcome, based on the difference between preferred and actual delivery model (39.7%) (22). The data were analyzed using SAS 9.3 (SAS Institute Inc., Cary, North Carolina, USA). The McNemar test was used to compare CS rates between the two preference groups (i.e., preferring vaginal vs. CS delivery). We compared maternal and obstetric characteristics, maternal and neonatal outcomes between the consistent and inconsistent groups, stratified by delivery modes preference. We performed univariate logistic regression analyses to find associations between maternal and neonatal characteristics and the odds ratios (OR) of the inconsistency between the preferred and the actual delivery modes. Those variables significantly associated (P≤0.05) in univariate analyses were included in multivariate logistic regression with stepwise selection. Both p-values of entry and exit into the final model were set at 0.05.
Results
In total, we approached 472 pregnant women in the outpatient obstetrics department, and enrolled 450 women into the study. After we excluded 18 women because of incomplete data, 432 women provided data for the analyses. Among them, 177 (177/432, 41.0%) delivered via CS, in spite that only 72 (72/432, 16.7%) preferred this delivery mode. Of the 177 women who had a CS, 50 (28.2%) experienced an emergency CS, and 56 (31.6%) had CDMR. There was no significant difference of CDMR rate between women preferring CS and VD (36.2 vs. 29.4%; χ2 = 0.83; P = 0.36). Those women with prior CS continued to have repeated CS. Among the 255 women who experienced a VD, 128 (50.2%) women had an episiotomy. The McNemar test shows that the rate of actual CS was significantly higher than the rate of preferred CS (χ2 = 82.89; P < 0.0001) (Table 1). The inconsistency rate between the preference of delivery mode and the actual delivery mode was 30.8% (133/432) among all women.
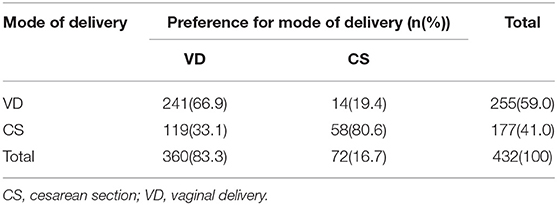
Table 1. Paired fourfold table of mode of delivery and preference.
Table 2 shows the different maternal and obstetric characteristics, and obstetric and neonatal outcomes according to the inconsistency between the actual mode of delivery and the initial maternal preference. Among women who preferred a VD, those ending up delivering via CS were more likely to: be older than 35 years, have obesity, have received assisted reproductive technology (ART) services, and to have abnormal amniotic fluid, breech presentation, and postpartum hemorrhage than those women in the consistent vaginal delivery group. Furthermore, women who preferred VD but ended up delivering via CS were less likely to experience PROM and have fetal distress than those who preferred and actually had a VD. There was a higher proportion of primiparous women among women who preferred CS but delivered vaginally. The other factors associated were similar between the inconsistent group and the consistent group, regardless of delivery mode preference.
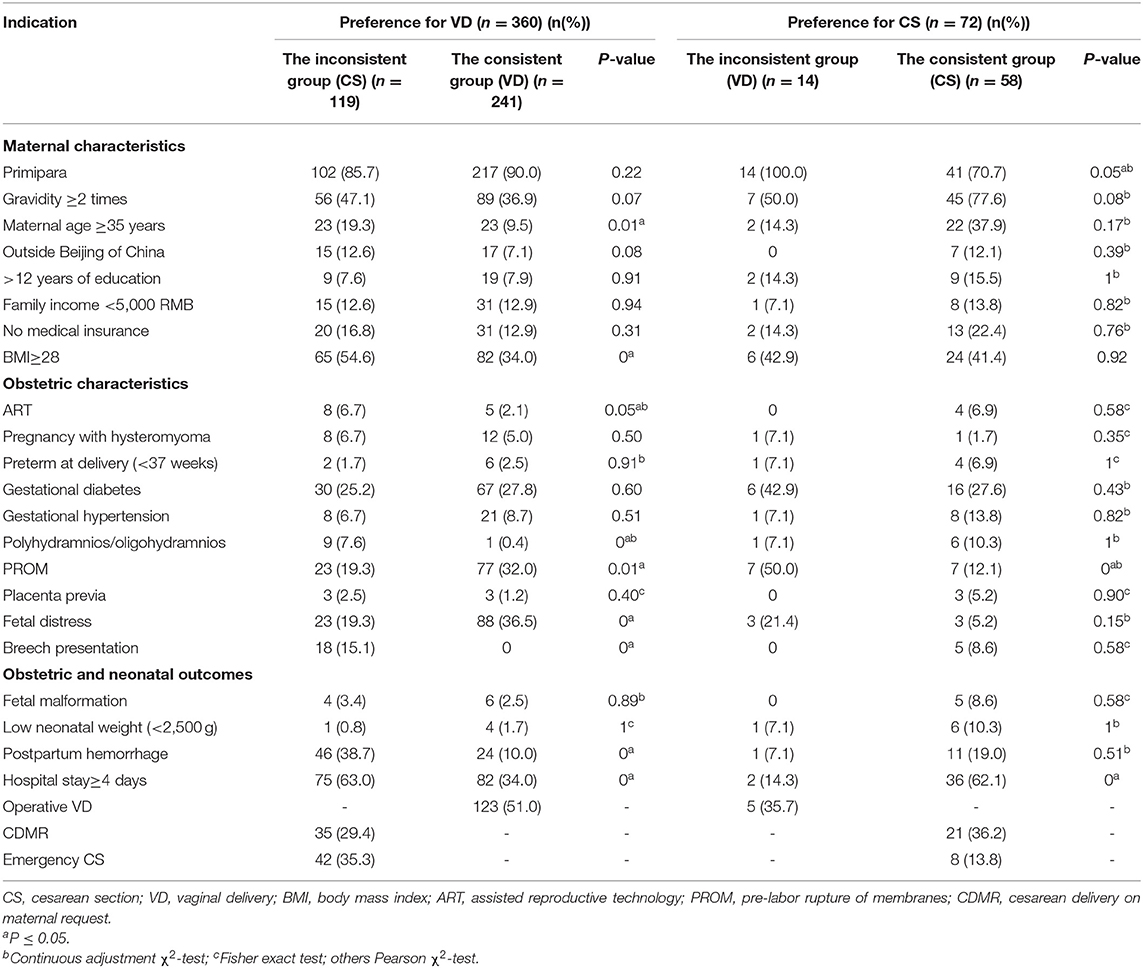
Table 2. Maternal characteristics, obstetric characteristics, obstetric and neonatal outcomes stratified by preference for delivery mode and the inconsistency.
Table 3 presents the predictors of the inconsistency between preferred and actual delivery mode by three multivariable logistic models. Model 1 identified the predictors of the overall inconsistency between preferred and actual delivery mode among all women (n = 432): maternal obesity [adjusted odds ratio (aOR) = 2.10; 95% confidence internal (CI) = 1.38–3.21], abnormal amniotic fluid volume [aOR = 3.44; 95% CI = 1.26–9.56] and lack of fetal distress [aOR = 0.52; 95% CI = 0.31–0.86]. Model 2 identified the predictors of the change from preferred VD to actual CS among the 360 women who had a preference for VD: maternal obesity [aOR = 2.42; 95% CI = 1.50–3.90], had received ART [aOR = 4.01 (1.15–14.01)], abnormal amniotic fluid volume [aOR = 30.99; 95% CI = 3.65–263.50] and lack of fetal distress [aOR = 0.31; 95% CI = 0.17–0.56]. Model 3 identified that those women who had PROM were more likely to drive the inconsistency that happened from desiring a CS during late pregnancy to actually having a VD during childbirth, among the 72 women who expressed this preference for CS delivery [aOR = 7.28; 95% CI = 1.96–27.06].
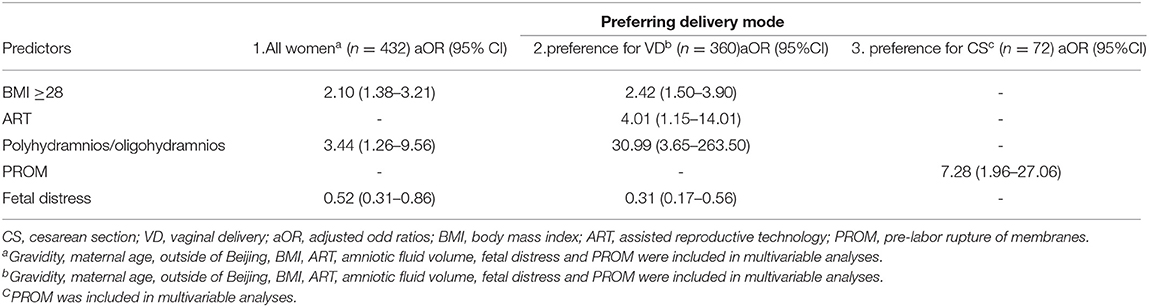
Table 3. Predictors of the inconsistency between the preferred and the actual delivery mode among all women, or those who preferred for VD, or those who preferred for CS.
Discussion
We found a big gap between the preference for CS and the actual prevalence of CS in China, which is consistent with other studies (21, 22, 24, 27). The inconsistency rate (31%) between preferred and actual delivery modes in this study was in between the rate of 21% in Henan (23) and 47% in Beijing (24). The number of women who preferred a VD but had CS was much larger than the number of women who wished to have a CS but ended up delivering vaginally. The predominance of the inconsistency being in the direction from VD preference to ending up having a CS may explain why CS rates continue to be high in China (e.g., far above 10%). Our study is unique in that it is based on a robust prospective study design to analyze risk factors for the delivery mode inconsistency. Furthermore, in this study we were able to carefully categorize women according to their preferred and actual delivery mode and if they were inconsistent or not.
The CS rate (41%) in our study was much higher than recommended by both WHO and the Chinese government. However, it was not as high as previously reported in other hospital-based studies in China where CS rates have been documented to be nearly 60% (28, 29). This may be in part because it was carried out in a WHO collaborating center hospital that admits more complicated cases and perhaps follows a stricter standard of CS indication than the hospitals included in other studies. Interestingly, in our study there was no significant difference in the CDMR rate among women who underwent CS regardless of their initial delivery mode preference.
The change from preferring a VD during the third trimester of pregnancy but ending up delivering via a CS may be explained by medical, social, cultural and individual factors (23, 27, 30, 31), and can also be influenced by family members and health professionals (32). In our study, we found several factors that were associated with the inconsistency from maternal characteristics, obstetric indications for delivery type, and neonatal outcomes.
The prevalence of maternal obesity in this study was high (41%), and the rate was higher in the inconsistent group than that in the consistent group among women who preferred a VD. Maternal obesity was also associated with the change from preferring a VD to ending up having a CS. A robust meta-analysis (33) found that a higher occurrence of large for gestational age or macrosomia, which may be a consequence of maternal obesity, might lead to a CS and negatively affect maternal and neonatal health. It is important to improve the management and control of overweight or obesity among women of child-bearing age. Maintaining normal BMI and weight gain during pregnancy have indeed been identified as a key measure to reduce CS among women who prefer a VD (33). Both maternal obesity and CS were higher than the threshold recommended by WHO for preventing adverse outcomes for mothers and their offspring in short or long term (34, 35). Therefore, obesity prevention or management prior to or during pregnancy needs to be addressed to keep mothers and children healthy and safe (33).
In our study, an abnormal amniotic fluid volume was also found to be a risk factor for the change from preferring a VD in pregnancy to undergoing a CS, which is consistent with previous studies (36–39). A study found that oligohydramnios pregnancies were more likely to end up with a CS compared with normal amniotic fluid pregnancies (47 vs. 17%, P < 0.001) (39). Doctors should inform women who have preference for VD to be prepared for possible CS if they have a polyhydramnios or oligohydramnios pregnancy.
In the above study (39), fetal distress was one of the main indications for CS, which is at odds with our findings. More women who didn't change from preferred VD to actual CS in our study. It might be ascribed to more fetal monitoring during vaginal birth which incurred more fetal distress reports in this study. Being a doctor in China, especially an obstetrician, is a high-risk occupation given the potential for tense relationships between doctors and patients that sometimes even lead to life threats from patients (40). Doctors try their best to avoid any risk for patients, especially those related to maternal and neonatal death, given the increased frequency of violence from patients against providers in clinical settings (41).
PROM was independently associated with the switch from preferring a CS to actually having a VD. However, PROM at term has been previously found to be a risk factor for CS (42), which is inconsistent with our study. This inconsistency may be due to different characteristics of the participants between the studies, including the proportion of nulliparous women expecting CS (42). It is worth to further study if and how PROM may impact CS in China across different population subgroups of women. This is because PROM can lead to intraamniotic infection, further cause neonatal mortality or morbidity (43). The mode of delivery for women with PROM should be decided based upon the safety for both, the infants and their mothers (44).
There were some limitations in this study. First, a quantitative study is hard to make further interpretation of the inconsistency. In future, we may adopt a mixed methodology, for instance, conduct a qualitative interview among those mind-changers. Second, we conducted the study in a maternity hospital in Beijing; therefore, the findings cannot be generalized to throughout China, but which could be index indicators of pregnant women's preference and its impact on delivery mode. Since the study was conducted several years before, the current situation related to preferred vs. actual delivery mode may have changed, especially in the context of the COVID-19 pandemic. However, the newly released census report in the context of third-child policy implemented in 2021, indicates that our study is still valuable for informing delivery policies in China.
Conclusions
The rate of CS was excessive in this study, and one-third of the women did not deliver their babies according to their delivery mode preferences. The inconsistency analyses conducted in our study can help screen for women who prefer a VD but that are at risk of ending up having a CS delivery even though there may not be a valid medical indication for it. Hence our findings can inform the design of interventions for lowering CS rates in China in the context of the “three-child” policy.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Institutional Review Board at Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, China. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
JW, HZ, and YH designed the study. HZ and LG collected the data. JW and LF analyzed the data. JW, YH, LF, and RP-E wrote and revised the manuscript. All authors approved the final manuscript.
Funding
This work was supported by Beijing Obstetrics and Gynecology Hospital, Capital Medical University [fcyy201413]. YH was supported in part by National Natural Science Foundation of China [82073574 and 81673232].
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We appreciated the support from the pregnant women in our study.
References
1. Boerma T, Ronsmans C, Melesse DY, Barros AJD, Barros FC, Juan L, et al. Global epidemiology of use of and disparities in caesarean sections. Lancet. (2018) 392:1341–8. doi: 10.1016/S0140-6736(18)31928-7
2. Betran AP, Ye J, Moller AB, Souza JP, Zhang J. Trends and projections of caesarean section rates: global and regional estimates. BMJ Glob Health. (2021) 6:5671. doi: 10.1136/bmjgh-2021-005671
3. Feng XL, Wang Y, An L, Ronsmans C. Cesarean section in the People's Republic of China: current perspectives. Intern J Womens Health. (2014) 6:59–74. doi: 10.2147/IJWH.S41410
4. National Health Commission of the People's Republic of China. Report on Women and Children's Health Development in China. (2019). Available online at: http://www.nhc.gov.cn/fys/ptpxw/201905/bbd8e2134a7e47958c5c9ef032e1dfa2.shtml
5. Li H, Luo S, Trasande L, Hellerstein S, Kang C, Li J, et al. Geographic variations and temporal trends in cesarean delivery rates in China, 2008–2014. JAMA. (2017) 317:69–76. doi: 10.1001/jama.2016.18663
6. Liang J, Mu Y, Li X, Tang W, Wang Y, Liu Z, et al. Relaxation of the one child policy and trends in caesarean section rates and birth outcomes in China between 2012 and 2016: observational study of nearly seven million health facility births. BMJ. (2018) 360:k817. doi: 10.1136/bmj.k817
7. Betran AP, Torloni MR, Zhang JJ, Gulmezoglu AM. WHO working group on caesarean section. WHO statement on caesarean section rates. BJOG. (2016) 123:667–70. doi: 10.1111/1471-0528.13526
8. Betran A, Torloni M, Zhang J, Yu J, Deneux-Tharaux C, Oladapo O, et al. What is the optimal rate of caesarean section at population level? A systematic review of ecologic studies. Reprod Health. (2015) 12:57. doi: 10.1186/s12978-015-0043-6
9. Ye J, Zhang J, Mikolajczyk R, Torloni M, Gülmezoglu A, Betran A. Association between rates of caesarean section and maternal and neonatal mortality in the 21st century: a worldwide population-based ecological study with longitudinal data. BJOG. (2016) 123:745–53. doi: 10.1111/1471-0528.13592
10. Gagnon AJ, Van Hulst A, Merry L, George A, Saucier JF, Stanger E, et al. Cesarean section rate differences by migration indicators. Arch Gynecol Obstet. (2013) 287:633–9. doi: 10.1007/s00404-012-2609-7
11. Lurie S, Shalev A, Sadan O, Golan A. The changing indications and rates of cesarean section in one academic center over a 16-year period (1997–2012). Taiwan J Obstet Gynecol. (2016) 55:499–502. doi: 10.1016/j.tjog.2014.12.014
12. Barber EL, Lundsberg LS, Belanger K, Pettker CM, Funai EF, Illuzzi JL. Indications contributing to the increasing cesarean delivery rate. Obstet Gynecol. (2011) 118:29–38. doi: 10.1097/AOG.0b013e31821e5f65
13. Lindstad Løvåsmoen EM, Nyland Bjørgo M, Lukasse M, Schei B, Henriksen L. Women's preference for caesarean section and the actual mode of delivery - Comparing five sites in Norway. Sex Reprod Healthc. (2018) 16:206–12. doi: 10.1016/j.srhc.2018.04.009
14. Liu Y, Li G, Chen Y, Wang X, Ruan Y, Zou L, et al. A descriptive analysis of the indications for caesarean section in mainland China. BMC Pregnancy Childbirth. (2014) 14:410. doi: 10.1186/s12884-014-0410-2
15. Wang E, Hesketh T. Large reductions in cesarean delivery rates in China: a qualitative study on delivery decision-making in the era of the two-child policy. BMC Pregnancy Childbirth. (2017) 17:405. doi: 10.1186/s12884-017-1597-9
16. Yu Y, Zhang X, Sun C, Zhou H, Zhang Q, Chen C. Reducing the rate of cesarean delivery on maternal request through institutional and policy interventions in Wenzhou, China. PLoS ONE. (2017) 12:e0186304. doi: 10.1371/journal.pone.0186304
17. Sun G, Lin Y, Lu H, He W, Li R, Yang L, et al. Trends in cesarean delivery rates in primipara and the associated factors. BMC Pregnancy Childbirth. (2020) 20:715. doi: 10.1186/s12884-020-03398-6
18. Feng XL, Xu L, Guo Y, Ronsmans C. Factors influencing rising caesarean section rates in China between 1988 and 2008. Bull World Health Organ. (2012) 90:30–9. doi: 10.2471/BLT.11.090399
19. Shaukat S, Nur U. Effect of prepregnancy maternal BMI on adverse pregnancy and neonatal outcomes: results from a retrospective cohort study of a multiethnic population in Qatar. BMJ Open. (2019) 9:e029757. doi: 10.1136/bmjopen-2019-029757
20. Wu E, Kaimal AJ, Houston K, Yee LM, Nakagawa S, Kuppermann M. Strength of preference for vaginal birth as a predictor of delivery mode among women who attempt a vaginal delivery. Am J Obstet Gynecol. (2014) 210:440. doi: 10.1016/j.ajog.2013.11.021
21. Ryding EL, Lukasse M, Kristjansdottir H, Steingrimsdottir T, Schei B. Pregnant women's preference for cesarean section and subsequent mode of birth - a six-country cohort study. J Psychosom Obstet Gynaecol. (2016) 37:75–83. doi: 10.1080/0167482x.2016.1181055
22. Ji H, Jiang H, Yang L, Qian X, Tang S. Factors contributing to the rapid rise of caesarean section: a prospective study of primiparous Chinese women in Shanghai. BMJ Open. (2015) 5:e008994. doi: 10.1136/bmjopen-2015-008994
23. Shi Y, Jiang Y, Zeng Q, Yuan Y, Yin H, Chang C, et al. Influencing factors associated with the mode of birth among childbearing women in Hunan Province: a cross-sectional study in China. BMC Pregnancy Childbirth. (2016) 16:108. doi: 10.1186/s12884-016-0897-9
24. Li WY, Liabsuetrakul T, Stray-Pedersen B. Change of childbirth preference after delivery among nulliparous Chinese women and their partners. J Obstet Gynaecol Res. (2014) 40:184–91. doi: 10.1111/jog.12153
25. Zhang H, Wu J, Norris J, Guo L, Hu Y. Predictors of preference for caesarean delivery among pregnant women in Beijing. J Int Med Res. (2017) 45:798–807. doi: 10.1177/0300060517696217
26. He Y, Lam TH, Jiang B, Li LS, Sun DL, Wu L, et al. Changes in BMI before and during economic development and subsequent risk of cardiovascular disease and total mortality: a 35-year follow-up study in China. Diabetes Care. (2014) 37:2540–7. doi: 10.2337/dc14-0243
27. Rajabi A, Maharlouei N, Rezaianzadeh A, Rajaeefard A, Keshavarzi S, Lankarani KB, et al. Non-medical factors affecting antenatal preferences for delivery route and actual delivery mode of women in southwestern Iran. J Matern Fetal Neonatal Med. (2016) 29:3622–8. doi: 10.3109/14767058.2016.1140137
28. Hu Y, Tao H, Cheng Z. Caesarean Sections in Beijing, China - Results from a Descriptive Study. Das Gesundheitswesen. (2015) 78:e1–5. doi: 10.1055/s-0035-1549937
29. Xiong C, Zhou A, Cao Z, Zhang Y, Qiu L, Yao C, et al. Association of pre-pregnancy body mass index, gestational weight gain with cesarean section in term deliveries of China. Sci Rep. (2016) 6:37168. doi: 10.1038/srep37168
30. Liang H, Fan Y, Zhang N, Chongsuvivatwong V, Wang Q, Gong J, et al. Women's cesarean section preferences and influencing factors in relation to China's two-child policy: a cross-sectional study. Patient Prefer Adherence. (2018) 12:2093–101. doi: 10.2147/PPA.S171533
31. Liu T, Chen C, Tsai Y, Lin H. Taiwan's high rate of cesarean births: impacts of national health insurance and fetal gender preference. Birth. (2007) 34:115–22. doi: 10.1111/j.1523-536X.2007.00157.x
32. Long Q, Kingdon C, Yang F, Renecle MD, Jahanfar S, Bohren MA, et al. Prevalence of and reasons for women's, family members', and health professionals' preferences for cesarean section in China: a mixed-methods systematic review. PLoS Med. (2018) 15:e1002672. doi: 10.1371/journal.pmed.1002672
33. Goldstein R, Abell S, Ranasinha S, Misso M, Boyle J, Black M, et al. Association of gestational weight gain with maternal and infant outcomes: a systematic review and meta-analysis. JAMA. (2017) 317:2207–25. doi: 10.1001/jama.2017.3635
34. Catalano P, Shankar K. Obesity and pregnancy: mechanisms of short term and long term adverse consequences for mother and child. BMJ. (2017) 356:j1. doi: 10.1136/bmj.j1
35. Boerma T, Ronsmans C, Melesse D, Barros A, Barros F, Juan L, et al. Short-term and long-term effects of caesarean section on the health of women and children. Lancet. (2018) 392:1341–48. doi: 10.1016/S0140-6736(18)31930-5
36. Aviram A, Salzer L, Hiersch L, Ashwal E, Golan G, Pardo J, et al. Association of isolated polyhydramnios at or beyond 34 weeks of gestation and pregnancy outcome. Obstet Gynecol. (2015) 125:825–32. doi: 10.1097/AOG.0000000000000740
37. Ott WJ. Reevaluation of the relationship between amniotic fluid volume and perinatal outcome. Am J Obstet Gynecol. (2005) 192:1803–9. doi: 10.1016/j.ajog.2004.12.062
38. Blackwell SC, Wolfe HM, Redman ME, Hassan SS, Berry SM, Treadwell MC, et al. Relationship between meconium staining and amniotic fluid volume in term pregnancies. Fetal Diagn Ther. (2002) 17:78–82. doi: 10.1159/000048013
39. Melamed N, Pardo J, Milstein R, Chen R, Hod M, Yogev Y. Perinatal outcome in pregnancies complicated by isolated oligohydramnios diagnosed before 37 weeks of gestation. Am J Obstet Gynecol. (2011) 205:241. doi: 10.1016/j.ajog.2011.06.013
40. Violence against doctors: Why China? Why now? What next? The Lancet. (2014) 383:1013. doi: 10.1016/s0140-6736(14)60501-8
41. Hellerstein S, Feldman S, Duan T. Survey of Obstetric Care and Cesarean Delivery Rates in Shanghai, China Birth. (2016) 43:193–9. doi: 10.1111/birt.12231
42. Park KH, Hong JS, Ko JK, Cho YK, Lee CM, Choi H, et al. Comparative study of induction of labor in nulliparous women with premature rupture of membranes at term compared to those with intact membranes: duration of labor and mode of delivery. J Obstet Gynaecol Res. (2006) 32:482–8. doi: 10.1111/j.1447-0756.2006.00443.x
43. Meller CH, Carducci ME, Ceriani Cernadas JM, Otano L. Preterm premature rupture of membranes. Arch Argent Pediatr. (2018) 116:e575–81. doi: 10.5546/aap.2018.eng.e575
Keywords: cesarean section, vaginal delivery, reproductive health, delivery preference, maternal obesity, amniotic fluid, inconsistency
Citation: Wu J, Feng L, Zhang H, Guo L, Pérez-Escamilla R and Hu Y (2022) The Inconsistency Between Women's Preference and Actual Mode of Delivery in China: Findings From a Prospective Cohort Study. Front. Public Health 10:782784. doi: 10.3389/fpubh.2022.782784
Received: 24 September 2021; Accepted: 09 March 2022;
Published: 30 March 2022.
Edited by:
Yong Zhao, Chongqing Medical University, ChinaCopyright © 2022 Wu, Feng, Zhang, Guo, Pérez-Escamilla and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yifei Hu, aHV5aWZlaUB5YWhvby5jb20=; aHV5aWZlaUBjY211LmVkdS5jbg==