 Morenike Oluwatoyin Folayan1,2*
Morenike Oluwatoyin Folayan1,2* Olanrewaju Ibigbami3
Olanrewaju Ibigbami3 Brandon Brown1,4
Brandon Brown1,4 Maha El Tantawi1,5
Maha El Tantawi1,5 Nourhan M. Aly1,5
Nourhan M. Aly1,5 Oliver C. Ezechi1,6
Oliver C. Ezechi1,6 Giuliana Florencia Abeldaño1,7Eshrat Ara1,8Martin Amogre Ayanore1,9Passent Ellakany1,10
Giuliana Florencia Abeldaño1,7Eshrat Ara1,8Martin Amogre Ayanore1,9Passent Ellakany1,10 Balgis Gaffar1,11
Balgis Gaffar1,11 Nuraldeen Maher Al-Khanati1,12
Nuraldeen Maher Al-Khanati1,12 Ifeoma Idigbe1,6Mohammed Jafer1,13Abeedha Tu-Allah Khan1,14Zumama Khalid1,14
Ifeoma Idigbe1,6Mohammed Jafer1,13Abeedha Tu-Allah Khan1,14Zumama Khalid1,14 Folake Barakat Lawal1,15Joanne Lusher1,16Ntombifuthi P. Nzimande1,17Bamidele Olubukola Popoola1,18
Folake Barakat Lawal1,15Joanne Lusher1,16Ntombifuthi P. Nzimande1,17Bamidele Olubukola Popoola1,18 Mir Faeq Ali Quadri1,19Mark Roque1,20
Mir Faeq Ali Quadri1,19Mark Roque1,20 Ala'a B. Al-Tammemi1,21
Ala'a B. Al-Tammemi1,21 Muhammad Abrar Yousaf1,22
Muhammad Abrar Yousaf1,22 Jorma I. Virtanen1,23
Jorma I. Virtanen1,23 Roberto Ariel Abeldaño Zuñiga1,24Nicaise Ndembi1,25John N. Nkengasong1,25
Roberto Ariel Abeldaño Zuñiga1,24Nicaise Ndembi1,25John N. Nkengasong1,25 Annie Lu Nguyen1,26
Annie Lu Nguyen1,26- 1Mental Health and Wellness Study Group, Ile-Ife, Nigeria
- 2Department of Child Dental Health, Obafemi Awolowo University, Ile-Ife, Nigeria
- 3Department of Mental Health, Obafemi Awolowo University, Ile-Ife, Nigeria
- 4Department of Social Medicine, Population and Public Health, Riverside School of Medicine, University of California, Riverside, Riverside, CA, United States
- 5Department of Pediatric Dentistry and Dental Public Health, Faculty of Dentistry, Alexandria University, Alexandria, Egypt
- 6Department of Clinical Sciences, Nigerian Institute of Medical Research, Lagos, Nigeria
- 7School of Medicine, University of Sierra Sur, Oaxaca, Mexico
- 8Government College for Women, Srinagar, India
- 9Department of Health Policy Planning and Management, School of Public Health, University of Health and Allied Sciences, Ho, Ghana
- 10Department of Substitutive Dental Sciences, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
- 11Department of Preventive Dental Sciences, College of Dentistry, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia
- 12Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Syrian Private University, Damascus, Syria
- 13Department of Preventive Dental Sciences, Saudi Arabia Department of Health Promotion, Faculty of Health, Medicine and Life Sciences, Jazan University, Maastricht University, Maastricht, Netherlands
- 14Department of Health Sciences, University of Genova, Genova, Italy
- 15Department of Periodontology and Community Dentistry, University of Ibadan and University College Hospital, Ibadan, Nigeria
- 16Director of People and Member of the Provost's Group, Regent's University, London, United Kingdom
- 17Department of Economic and Social Geography, University of Szeged, Szeged, Hungary
- 18Department of Child Oral Health, University of Ibadan, Ibadan, Nigeria
- 19Department of Preventive Dental Sciences, Division of Dental Public Health, College of Dentistry, Jazan University, Jizan, Saudi Arabia
- 20Department of Maternity and Childhood Nursing, College of Nursing, Taibah University, Medina, Saudi Arabia
- 21Migration Health Division, International Organization for Migration (IOM), The UN Migration Agency, Amman, Jordan
- 22Institute of Zoology, University of the Punjab, Lahore, Pakistan
- 23Faculty of Medicine, University of Turku, Turku, Finland
- 24Postgraduate Department, University of Sierra Sur, Oaxaca, Mexico
- 25Africa Centres for Disese Control and Preventon, African Union Commission, Addis Ababa, Ethiopia
- 26Department of Family Medicine, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States
Background: Multiple facets of the pandemic can be a source of fear, depression, anxiety and can cause changes in sleep patterns. The aim of this study was to identify health profiles and the COVID-19 pandemic related factors associated with fear, depression, anxiety and changes in sleep pattern in adults in Nigeria.
Methods: The data for this analysis was extracted from a cross-sectional online survey that collected information about mental health and well-ness from a convenience sample of adults 18 years and above resident in Nigeria from July to December 2020. Study participants were asked to complete an anonymous, closed-ended online questionnaire that solicited information on sociodemographic profile, health profiles (high, moderate and low COVID-19 infection risk profile) including HIV status, COVID-19 status, and self-reported experiences of fear, anxiety, depression and changes in sleep patterns.
Results: In total, 4,439 participants with mean age of 38.3 (±11.6) years responded to the survey. Factors associated with higher odds of having COVID-19 related fear were health risk (p < 0.05); living with HIV (AOR: 3.88; 95% CI: 3.22–4.69); having COVID-19 symptoms but not tested (AOR: 1.61; 95% CI: 1.30–1.99); having a friend who tested positive to COVID-19 (AOR: 1.28; 95% CI: 1.07–1.53) and knowing someone who died from COVID-19 (AOR: 1.43; 95% CI: 1.24–1.65). The odds of feeling anxious was significantly higher for those with moderate or low health risk profile (p < 0.05); living with HIV (AOR: 1.64; 95% CI: 1.32–2.04); had a friend who tested positive for COVID-19 (AOR: 1.35; 95% CI: 1.08–1.68) or knew someone who died from COVID-19 (AOR: 1.53; 95% CI: 1.28–1.84). The odds of feeling depressed was significantly higher for those with health risk profile (p < 0.05); living with HIV (AOR: 2.49; 95% CI: 1.89–3.28); and respondents who had COVID-19 symptoms but had not taken a test (AOR: 1.41; 95% CI: 1.02–1.94). Factors associated with higher odds of having sleep pattern changes were having moderate and low health risk profiles (p < 0.05).
Conclusion: The study findings suggest that the pandemic may cause fear, anxiety, depression and changes in sleep patterns differently for people with different health profile, HIV status and COVID-19 status.
Introduction
For many individuals, the COVID-19 pandemic has been a source of fear, depression, and anxiety; all of which can lead to changes in sleep quality and patterns. Multiple facets and characteristics of the pandemic can be attributed to these outcomes. Concerns about mortality and morbidity associated with the COVID-19, scarcity of financial resources, and uncertainty about time of recovery from associated financial hardships are partly to blame (1). Patients with COVID-19 also fear abandonment, feelings of isolation and psychological sufferings (1). Some may fear infecting friends and family members, otherwise known as contamination fear (2–4). The fear of the unknown appears to be a core component of anxiety that accompanies situations that are unpredictable and uncontrollable (5, 6). Fear of these threats is often learned, irrespective of the probability of its occurrence, and results from the inability to tolerate uncertainty (7). The intolerance of uncertainty is also related to depressive symptomatology, and the fear of COVID-19 may explain part of the relation (8).
The COVID-19 pandemic is associated with up to a seven times higher prevalence of depression (9) and over 25% mental deterioration in some populations (10, 11). Persons with prior history of mental health disorders had higher rates of depression during the pandemic (12). Depressive symptoms were associated with testing positive for COVID-19 or having COVID-19 symptoms, exposure to social media, poor social support, unemployment, uncertainty about the future of jobs, and careers and economic crisis, especially for students (9). As with fear, depression is associated with anxiety (13, 14). The prevalence of anxiety during the COVID-19 pandemic is higher than 30% (15); and anxiety is higher in people with poor health (16). Anxiety disorder may lead to dysfunctional arousal that in turn results in persistent sleep-wake difficulties such as insomnia and hypersomnia (17, 18). Sleep disturbance is also a diagnostic symptom for generalized anxiety disorder (19), with young people being the worse-affected (20).
Though the prevalence of sleep problems, fear, anxiety and depression increased during the pandemic (21, 22), the impact may, however, differ between populations (23, 24). Fear, anxiety, depression and sleep disorder may be lower in the general population than it is in populations living with co-morbidities. Understanding the association between negative emotions and sleep pattern during the COVID-19 pandemic is important. However, research in this field is scarce (20). We hypothesize that respondent's COVID-19 related status would be associated with the experience of fear, depression, anxiety and changes in sleep pattern during the pandemic; that more people living with HIV will experience fear, anxiety, depression and sleep disorder; and that more people with fear, anxiety, depression and sleep disorder will use COVID-19 preventive measures.
The consolidation of contextual fear, depression, anxiety and avoidance of the shock evoke negative emotions and trigger alterations in sleep characteristics (25). Despite this, there is a little known about the aspects of the pandemic crisis that trigger negative emotions. One of the aims of this study was to identify COVID-19 pandemic related factors such as COVID-19 test positivity status, history of COVID-19 symptoms, and contact/relation with persons who have COVID-19, and their association with fear, depression, anxiety, and changes in sleep pattern. We also identified the association between fear, depression, anxiety, and changes in sleep pattern and the COVID-19 status. Finally, we determined if living with HIV was associated with the experience of fear, depression, anxiety, and changes in sleep pattern.
Methods
Study Design and Study Participants
This was a sub-analysis data from an international cross-sectional study on the impact of COVID-19 on the mental health and well-ness of adults using an online multi-country survey. Data were collected from a convenient sample of adults 18 years and above from July to December 2020. The study methodology had been reported in detail in prior studies (26, 27).
Study Instrument
The survey used a questionnaire, which was initially developed for a study that targeted a specific population in the United States and was consequently adapted and validated for use by a global audience (28). The questionnaire underwent four iterative processes content validation. The overall content validity index of the survey was 0.83. The responses collected for content validation were excluded from the final analysis. The study was approved by the Human Research Ethics Committee at the Institute of Public Health of the Obafemi Awolowo University Ile-Ife, Nigeria (HREC No: IPHOAU/12/1557). Participants received no incentive for taking part in the study.
Recruitment of the Study Participants
A call for collaboration for this study was made on Research gate. The 45 collaborators engaged through the public call were required to distribute their unique survey links to networks within and outside their countries and communities to ensure maximum representation and geographic spread. There were none data collectors recruited from Nigeria. The study participants were recruited through respondent-driven sampling. These links were posted on social media groups (Facebook, Twitter, and Instagram) and sent via WhatsApp or email to eligible participants in each collaborators' networks. The study participants were further asked to disseminate the links to those in their own networks using snowball sampling to facilitate further recruitment. The survey link was also posted on social media groups (Facebook, Twitter, and Instagram, WhatsApp) and network email lists.
Data Collection
Study participants were asked to complete an anonymous, closed-ended questionnaire to learn about how the COVID-19 pandemic has affected the people's mental health and psychological wellbeing. The questionnaire also enquired about respondents' sociodemographic profile, health profile, and various aspects of pandemic-related stress. The questionnaire was preceded by a brief introduction explaining the purpose of the study, and assuring participants of their voluntary participation, and confidentiality of their data. The questionnaire took an average of 11 min to complete and was administered in English. Each participant could only complete a single questionnaire through IP address restrictions, though they could edit their answers freely until they chose to submit. For the current analyses, we included only respondents who self-reported as residing in Nigeria. We also identified and removed survey responses that were completed below 7 min—the minimum time for filling the questionnaire by people familiar with the questionnaire in the pilot stage (n = 77); and those with incomplete data on fear, anxiety, depression and sleep disorder (n = 32).
Explanatory Variables
Sociodemographic Variables
The section on sociodemographic profile had questions on country of residence, age (in years), sex at birth, highest level of education attained (none, primary, secondary and tertiary) and employment status (retired, student, employed, and unemployed).
Health Profile
The section on health profile required respondents to select any of the 23 medical conditions listed that they experienced in addition to other health conditions not listed. These medical conditions put individuals at high risk for severe COVID-19 disease (pneumonia, diabetes, cancer, heart condition), those that might put people at moderate risk for severe COVID-19 disease (hepatitis, hypertension, neurological problems, neuropathy, respiratory problems, stroke, depression) and those conditions associated with low risk for severe COVID-19 disease (herpes, shingles and other sexually transmitted infections, dermatologic problems, migraines, arthritis, broken bones, hearing loss and vision loss) (29). As part of the list, participants were also asked about their HIV status. A tick on a checkbox on the list of health conditions was an indication that the individual had the health condition. All respondents were categorized as either having the health condition (indicated by a tick of the checkbox) or not having the health condition (indicated by not ticking the checkbox).
COVID-19 Status
Respondents were asked if they had tested positive for COVID-19, had COVID-19 symptoms but did not test, had a close friend who tested positive for COVID-19, or knew someone who died from COVID-19. Response choices for these items were “yes” or “no”.
Outcome Variables
Fear, Anxiety and Depression
Respondents were asked to indicate if they had experienced fear, anxiety and depression during the pandemic by checking a response box. The questions were adapted from the Pandemic Stress Index (30).
Changes in Sleep Pattern
Respondents were asked to indicate if they had experienced changes in sleep patterns (sleeping more, sleeping less, or no changes) during the pandemic. Each respondent was required to check a response box that indicated if they had experienced any of these conditions. The questions were adapted from the Pandemic Stress Index (30). The responses were dichotomised to change (sleeping more, sleeping less) and no change in sleep pattern.
Data Analysis
Data were downloaded from Survey Monkey® as SPSS file version 23.0 (IBM Corp., Armonk, N.Y., USA), cleaned and prepared for analysis. T- test and chi square tests were used to assess the relationship between COVID-19 status (testing positive, suspected but not tested, friend testing positive and knowing someone who died of COVID-19) on one hand, and health profile, HIV status, fear, anxiety, depression, and changes in sleep pattern on the other hand. Also, the associations between the explanatory variables and the outcome variables were determined by conducting logistic regression analysis using four models: one for each outcome variable. The covariates for the study were the sociodemographic profile (age, sex, educational level, and employment status). Adjusted odds ratios, 95% confidence intervals (CIs) and p-values were calculated. Significance was set at 5%.
Results
The mean age of the 4,439 respondents living in Nigeria was 38.3 years (SD = 11.6) ranging from 18 years to 85 years. Table 1 highlights the demographic profile of respondents. More than half of the respondents were females (53.2%), the majority had college/university education (80.9%) and were employed (70.5%). Also, 110 (2.5%) respondents tested positive for COVID-19, 466 (10.5%) had COVID-19 symptoms but did not take a test, 715 (16.1%) had a friend who had tested positive to COVID-19, and 1,367 (30.8%) knew someone who died of COVID-19. The majority (52.9%) expressed fear in response to the pandemic—fear of getting infected (50.7%) or fear of infecting someone (11.3%). Moreover, 746 (16.8%) felt anxious, 389 (8.8%) felt depressed and 1,007 (22.7%) experienced changes in their sleep pattern.
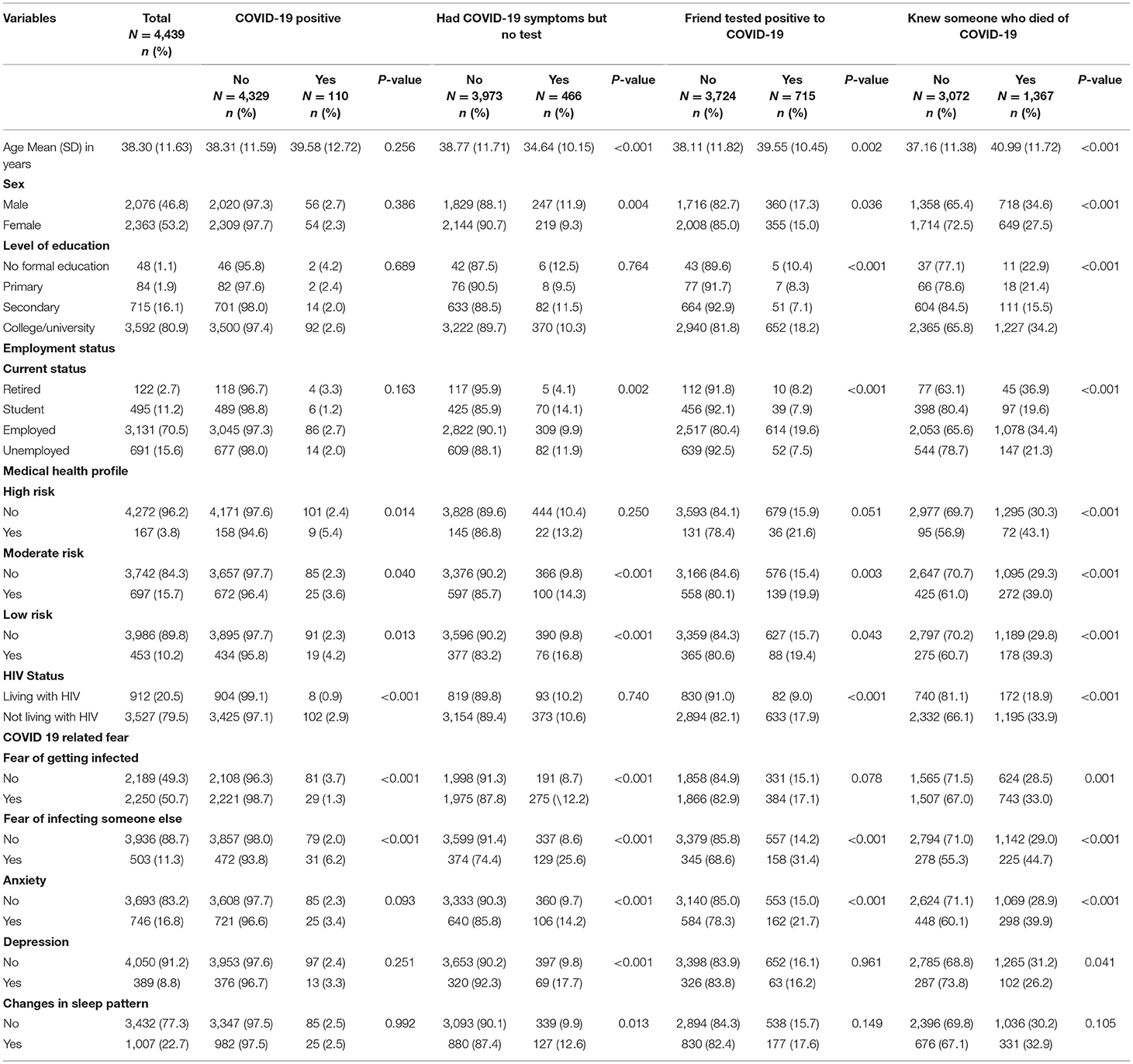
Table 1. Factors associated with COVID-19 status by adults in Nigeria (N = 4,439).
Significantly more respondents with high (p = 0.014), moderate (p = 0.040) and low (p = 0.013) medical risks tested positive for COVID-19. Also, significantly more people not living with HIV than people living with HIV (PLHIV) had a positive SARS-CoV-2 test result (p < 0.001). In addition, significantly more people who had no fear of getting infected with COVID-19 (p < 0.001) and those who had the fear of infecting other persons (p < 0.001) tested COVID-19 positive.
Significantly more respondents who had COVID-19 symptoms but did not test were younger (p < 0.001), were males (p = 0.004), students (p = 0.002), had moderate (p < 0.001) and low (p < 0.001) health risks, had fear of getting infected (p < 0.001) and infecting someone else (p < 0.001), felt anxious (p < 0.001), depressed (p < 0.001) and had changes in sleep pattern (p = 0.013).
Significantly more respondents who had a friend who tested positive to COVID-19 were older (p = 0.002), males (p = 0.036), had college/university education (p < 0.001), were employed (p < 0.001), had moderate (p = 0.003) or low (p = 0.043) health risk, were not living with HIV (p < 0.001) and had the fear of infecting someone else (p < 0.001) and felt anxious (p < 0.001).
Significantly more respondents who knew someone who died of COVID-19 were older (P < 0.001), males (p < 0.001), had college/university education (p < 0.001), were retirees (p < 0.001), had mild, moderate or high health risk profiles (p < 0.001), were not living with HIV (p < 0.001), had the fear of getting infected (p = 0.001) or infecting others (p < 0.001), felt anxious (p < 0.001) and did not feel depressed (p = 0.041).
Table 2 highlights the factors associated with COVID-19 related fear, anxiety, depression and changes in sleep pattern. The p-values of the omnibus tests of model coefficients for the four models indicate that the models outperformed the null models. The goodness of fit tests also indicated that the models were robust except the model to determine the factors associated with depression.
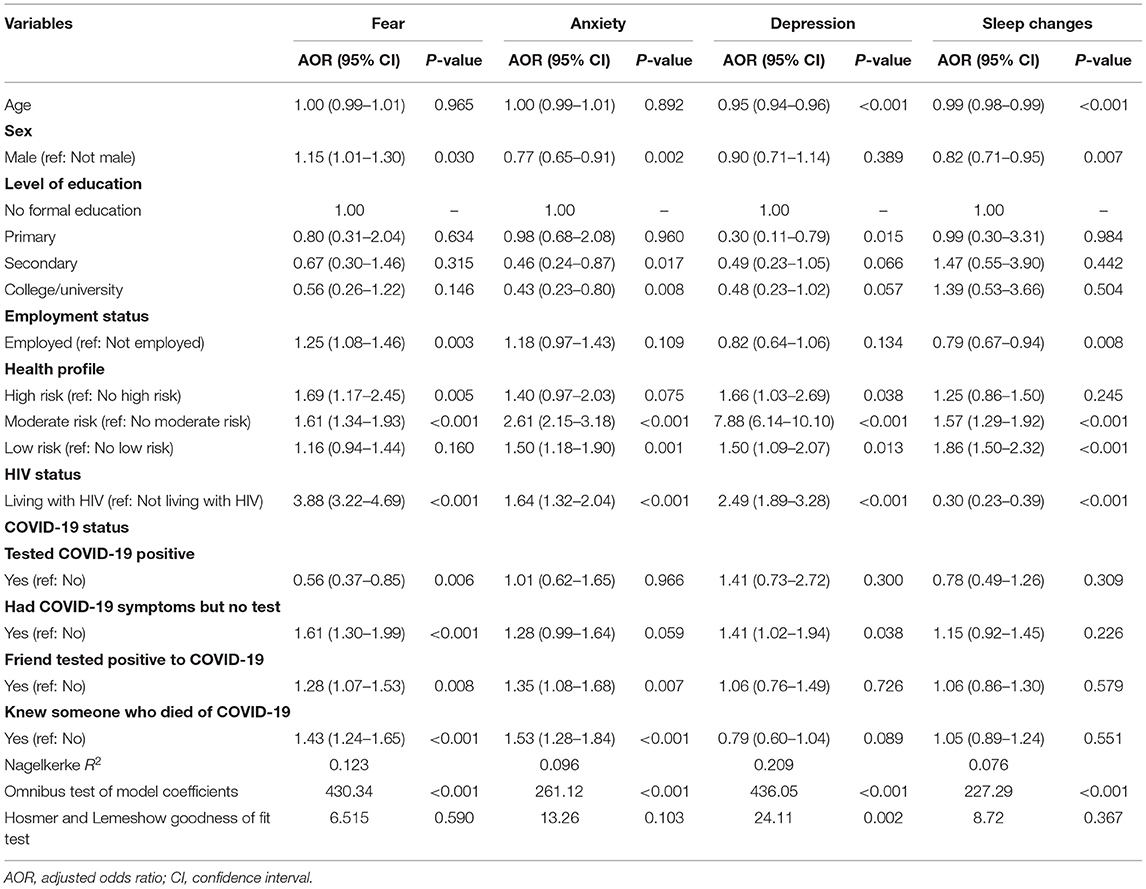
Table 2. Logistic regression analysis for factors associated with anxiety, depression and sleep changes during the COVID-19 pandemic by adults in Nigeria (N = 4,439).
The factors associated with significantly higher odds of having COVID-19 related fear were being a male (AOR: 1.15; 95% CI: 1.01–1.30); being employed (AOR: 1.25; 95% CI: 1.08–1.46); having high (AOR: 1.69; 95% CI: 1.17–2.45) and moderate (AOR: 1.61; 95% CI: 1.34–1.93) health risk; living with HIV (AOR: 3.88; 95% CI: 3.22–4.69); having COVID-19 symptoms but not yet tested (AOR: 1.61; 95% CI: 1.30–1.99); having a friend who tested positive to COVID-19 (AOR: 1.28; 95% CI: 1.07–1.53) and knowing someone who died from COVID-19 (AOR: 1.43; 95% CI: 1.24–1.65). Having tested positive to COVID-19 was associated with significantly lower odds of experiencing fear (AOR: 0.56; 95% CI: 0.37–0.85).
Also, respondents had significantly higher odds of feeling anxious when they had moderate (AOR: 2.61; 95% CI: 2.15–3.18) or low (AOR: 1.50; 95% CI: 1.18–1.90) health risk profile; living with HIV (AOR: 1.64; 95% CI: 1.32–2.04); had a friend who tested positive for COVID-19 (AOR: 1.35; 95% CI: 1.08–1.68) or knew someone who died from COVID-19 (AOR: 1.53; 95% CI: 1.28–1.84). The odds of feeling anxious were significantly lower for respondents who were males (AOR: 0.77; 95% CI: 0.69–0.91); and those with secondary (AOR: 0.46; 95% CI: 0.24–0.87) or college/university (AOR: 0.43; 95% CI: 1.25–4.39) education when compared with those that had no formal education. Respondents who had significantly higher odds of feeling depressed had high (AOR: 1.66; 95% CI: 1.03–2.69), moderate (AOR: 7.88; 95% CI: 6.14–10.10) and low (AOR: 1.50; 95% CI: 1.09–2.07) health risks; living with HIV (AOR: 2.49; 95% CI: 1.89–3.28); and respondents who had COVID-19 symptoms but had not taken a test (AOR: 1.41; 95% CI: 1.02–1.94). The odds of feeling depressed were significantly lower for respondents who were older (AOR: 0.95; 95% CI: 0.94–0.96); and who had primary school education (AOR: 0.03; 95% CI: 0.11–0.79) when compared with those that had no formal education.
Factors associated with significantly higher odds of having sleep pattern changes were having moderate (AOR: 1.57; 95% CI: 1.29–1.92) or low (AOR: 1.86; 95% CI: 1.50–2.32) health risk profiles. Factors associated with significantly lower odds of having sleep pattern changes were being older (AOR: 0.99; 95% CI: 0.98–0.99); being a male (AOR: 0.82; 95% CI: 0.71–0.95); employed (AOR: 0.79; 95% CI: 0.67–0.94); and living with HIV (AOR: 0.30; 95% CI: 0.23–0.39).
Discussion
The study identified COVID-19 related factors associated with the experience of fear, depression, anxiety and changes in sleep pattern during the pandemic. First, we identified that respondents who had COVID-19 symptoms but not yet tested, who had a friend who tested positive and who knew someone who died from COVID-19 had higher odds of being afraid while those who had tested positive to COVID-19 had lower odds of experiencing fear. Anxiety was higher for persons who had a friend who tested positive for COVID-19 and who knew someone who died from COVID-19. Those who had COVID-19 symptoms but had not taken a test had higher odds of being depressed. Second, respondents with low and moderate health risks had higher odds of feeling depressed, anxious or having changes in sleep pattern during the pandemic while those with moderate and high health risk profiles had higher odds of having fears (fear of contracting infection or infecting others). Third, PLHIV had higher odds of having fears, feeling anxious or depressed than people not living with HIV. They also had lower odds of changes in sleep patterns than people not living with HIV. Fourth, males had higher odds of having COVID-19 related fears, and lower odds of having anxiety and changes in sleep patterns; older respondents had lower odds of feeling depressed and having changes in sleep patterns; those with secondary or college/university education had lower odds of feeling anxious, while those with primary school education had lower odds of feeling depressed than respondents without formal education.
The study provides evidence that the experience of fear, depression, anxiety, and changes in sleep patterns differ between different populations. We observed that some populations that had higher odds of being afraid and higher odds of having being anxious (having moderate and low health risk for COVID-19, PLHIV, having a friend tested positive to COVID-19, knowing someone who died from COVID-19); higher odds of being depressed (having high, moderate and low health risk for COVID-19) and higher odds of having changes in sleep patterns (having moderate and low health risk for COVID-19). Others had higher odds of being afraid but lower odds of having anxiety (males) and changes in sleep patterns (being employed, PLHIV). The complex relationship between fear, anxiety, depression, and changes in sleep patterns was reflected in the results we report about PLHIV. PLHIV had higher odds of having fears and feeling anxious or depressed, but lower odds of changes in sleep patterns.
Also, our study findings that respondents who had COVID-19 symptoms but not yet tested, who had a friend who tested positive and who knew someone who died from COVID-19 was associated with higher odds for fear and anxiety is an indication for identifying individuals with this profile and providing psychological support to them. Their fears and anxiety may be related with concerns about they themselves likely testing COVID-19 positive, the stigma associated with this status (31) and the concerns with being quarantined (32). Their fears and anxiety may also be due to concerns with the attendant consequences of testing positive (2) such as facing stigma (33), boredom, frustration, inadequate supplies, inadequate information, and financial loss while in quarantine or isolation (2). Quarantine and isolation are also associated with anger, confusion, and post-traumatic stress symptoms (2). Positive public messaging about COVID-19 positive status may also go a long way to ameliorates these concerns about COVID-19 that triggers negative emotions.
These associations suggest that there may be various factors that mediate and/or moderate the relationship between fear, depression, anxiety and changes in sleep patterns. One of these factors may be age: we observed that respondents who are older had lower odds of feeling depressed or having changes in sleeping patterns. Aging is associated with an intrinsic reduction in susceptibility to depression (34) though people with chronic illness are more likely to be depressed (34–41) and have changes in sleep pattern due to physiological alterations (42, 43). People with high health risks are usually older (44–47). Our study findings indicated that those with high, moderate, and low health risk profiles had higher odds of reporting depression, anxiety and changes in sleep pattern corroborating prior findings (34–43). Populations with health concerns during the COVID-19 pandemic may however, have heightened concerns due to their susceptibility to infection and the absence of known therapies and vaccines. This may explain the high risk for depression, anxiety and changes in sleep pattern. On the other hand, this profile may have changed with the increased access to COVID-19 vaccines. The possibility of these changes may need to be explored in future studies.
Gender may act as a mediator and/or moderator of the relationship between fear, anxiety, and changes in sleep patterns. Though females were previously reported to be more likely to have fears (48), we observed in our study that males had higher odds of reporting fears. However, like a prior study, males had lower odds of reporting anxiety (49). We also observed that men had lower odds of changes in sleep patterns similar to prior studies that indicated that males had better sleep quality even during the pandemic (50, 51). This change in gender related association with fears during the pandemic may be related with men's concern about possible loss of income and the ability to provide the basic needs of the family. Although the International Labor Organization had stated that the pandemic had a greater impact on women than men in developed economies (52) this may not be the case for developing economies where men are responsible for securing food and life expenses and as such, may have greater concerns about losing their jobs due to COVID-19. Nigeria is a patriarchal society where men are the bread winners (53–55). With the loss of jobs and diminished income resulting from the pandemic (56–58), the affected male breadwinners may have fears. In the absence of welfare and social security packages during this pandemic for residents in Nigeria, there is a risk for an increase in health problems such as hypertension, high blood sugar and other metabolic disorders (59). This risk may be ameliorated by the lower risk for anxiety and sleep changes. This does not eliminate the possible need for palliative care for employees in Nigeria to absorb the economic shock they face because of the pandemic and reduce its impact on their quality of life.
Educational status is another possible mediator and/or moderator for anxiety and depression. Those with secondary education and above had lower odds of feeling anxious and those who had primary school education had lower odds of having depression than those without formal education. Prior studies indicated lower risk of depression and anxiety as the educational level improves (60, 61), while other evidence suggested no significant effect of educational level on anxiety (62). Like previous studies, we found that higher educational status was associated with lower odds of anxiety and depression during the pandemic. This finding may be because educated individuals may be more aware of modes of COVID-19 transmission and its consequences (63). Also, higher educational status may also be associated with better opportunities for employment, being male, lower risk for losing a job and thus, lower risk of experiencing anxiety and depression during the pandemic. This hypothesis needs to be tested further.
One of the strengths of this study is the large sample providing adequate study power. The data was also collected using validated tools and this strengthened the validity of the study findings. The data included information on the health status of respondents, which is relevant as differences in sickness status could influence anxiety, depression, and sleep pattern. The study has a few limitations despite its strengths. The self-reporting of fear, depression, anxiety, and HIV status is associated with high risk of social desirability and central tendency bias (64); and self-report may be more sensitive to identifying non-depressed, non-anxious and HIV negative individuals (65, 66). Also, we had an imbalance between participants on educational level, with comparably larger number of respondents with tertiary education which does not reflect the educational status of Nigeria. In addition, the study can only be generalized to those with internet access who could respond to the questionnaire; and it could not measure changes in the respondents' answers at different time points and phases of the pandemic as we know that the pandemic changed over time.
Conclusion
Various factors were identified to be significantly associated with experiencing fear, anxiety, depression and change in sleep patterns among the participants during the pandemic. The study findings suggest that the pandemic may have had significant impact on the psychological wellbeing and daily living of individuals. Capacity building and training on how to deal and cope with stressful events and to enhance individuals' resilience are of paramount importance during large-scale crisis like the current pandemic. Besides, our study findings open avenues for further longitudinal assessment of the impact of COVID-19 pandemic on various life domains, considering the dynamic nature of the crisis and human behavior.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Research Ethics Committee at the Institute of Public Health of the Obafemi Awolowo University Ile-Ife, Nigeria. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
The project was conceptualized by MF. The data for the research was collected by MF, II, FL, and BP. The data analysis was conducted by OI. All authors contributed to the article, read, and approved the submitted version.
Funding
AN was supported by funding from the National Institutes of Health/National Institute on Aging (K01 AG064986-01). All other authors made the needed personal financial contributions for the conduct of the study.
Author Disclaimer
The contents of this paper do not necessarily represent the official views of the National Institutes of Health.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We acknowledge and thank the study participants for the contributions they made to generating new knowledge. We also thank Dr. Gbenga Ayoola, Bamidele Osamika, Benjami Uzochukwu, Nneka Kate Onyejaka who was involved with data collection.
Abbreviations
AOR, Adjusted Odds Ratio; CI, Confidence Interval; COVID-19, Corona Virus Infectious Disease – 2019; HIV, Human Immunodeficiency Virus; PTSD, Post Traumatic Stress Disorder; SARS-CoV-2, Severe Acute Respiratory Syndrome Corona Virus Type 2.
References
1. Coelho CM, Suttiwan P, Arato N, Zsido AN. On the nature of fear and anxiety triggered by COVID-19. Front Psychol. (2020) 11:581314. doi: 10.3389/fpsyg.2020.581314
2. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
3. Olatunji BO, Sawchuk CN, Lohr JM, De Jong PJ. Disgust domains in the prediction of contamination fear. Behav Res Therap. (2004) 42:93–104. doi: 10.1016/S0005-7967(03)00102-5
4. Cisler JM, Reardon JM, Williams NL, Lohr JM. Anxiety sensitivity and disgust sensitivity interact to predict contamination fears. Personal Individ Differ. (2007) 42:935–46. doi: 10.1016/j.paid.2006.09.004
5. Gallagher MW, Bentley KH, Barlow DH. Perceived control and vulnerability to anxiety disorders: a meta-analytic review. Cogn Ther Res. (2014) 38:571–84. doi: 10.1007/s10608-014-9624-x
6. Carleton RN. Fear of the unknown: one fear to rule them all? J Anxiety Disord. (2016) 41:5–21. doi: 10.1016/j.janxdis.2016.03.011
7. Satici B, Saricali M, Satici SA, Griffiths MD. Intolerance of uncertainty and mental wellbeing: serial mediation by rumination and fear of COVID-19. Int J Ment Health Addict. (2020) 1–12. doi: 10.1007/s11469-020-00305-0
8. Voitsidis P, Nikopoulou VA, Holeva V, Parlapani E, Sereslis K, Tsipropoulou V, et al. The mediating role of fear of COVID-19 in the relationship between intolerance of uncertainty and depression. Psychol Psychother. (2021) 94:884–93. doi: 10.1111/papt.12315
9. Bueno-Notivol J, Gracia-García P, Olaya B, Lasheras I, López-Antón R, Santabárbara J. Prevalence of depression during the COVID-19 outbreak: a meta-analysis of community-based studies. Int J Clin Health Psychol. (2021) 21:100196. doi: 10.1016/j.ijchp.2020.07.007
10. Choi EPH, Hui BPH, Wan EYF. Depression and anxiety in Hong Kong during COVID-19. Int J Environ Res Public Health. (2020) 17:3740. doi: 10.3390/ijerph17103740
11. Hossain MM, Rahman M, Trisha NF, Tasnim S, Nuzhath T, Hasan NT, et al. Prevalence of anxiety and depression in South Asia during COVID-19: a systematic review and meta-analysis. Heliyon. (2021) 7:e06677. doi: 10.1016/j.heliyon.2021.e06677
12. Fountoulakis KN, Karakatsoulis G, Abraham S, Adorjan K, Ahmed HU, Alarcón RD, et al. Results of the COVID-19 mental health international for the general population (COMET-G) study. Eur Neuropsychopharmacol. (2021) 54:21–40. doi: 10.1016/j.euroneuro.2021.10.004
13. Gao J, Zheng P, Jia Y, Chen H, Mao Y, Chen S, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE. (2020) 15:e0231924. doi: 10.1371/journal.pone.0231924
14. Wang Y, Di Y, Ye J, Wei W. Study on the public psychological states and its related factors during the outbreak of coronavirus disease 2019 (COVID-19) in some regions of China. Psychol Health Med. (2021) 26:13–22. doi: 10.1080/13548506.2020.1746817
15. Deng J, Zhou F, Hou W, Silver Z, Wong CY, Chang O, et al. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis. Ann N Y Acad Sci. (2021) 1486:90–111. doi: 10.1111/nyas.14506
16. Jacobs M, Burch AE. Anxiety during the pandemic: racial and ethnic differences in the trajectory of fear. J Affect Disord. (2021) 292:58–66. doi: 10.1016/j.jad.2021.05.027
17. Ford DE, Kamerow DB. Epidemiological study of sleep disturbances and psychiatric disorders: an opportunity for prevention? JAMA. (1989) 162:1479–84. doi: 10.1001/jama.262.11.1479
18. Breslau N, Roth T, Rosenthal L, Andreski P. Sleep disturbance and psychiatric disorders: a longitudinal epidmiological study of young adults. Biol Psychiatry. (1996) 39:411–8. doi: 10.1016/0006-3223(95)00188-3
19. Staner L. Sleep and anxiety disorders. Dial Clin Neurosci. (2003) 5:249–58. doi: 10.31887/DCNS.2003.5.3/lstaner
20. Hyun S, Hahm HC, Wong GTF, Zhang E, Liu CH. Psychological correlates of poor sleep quality among U.S. young adults during the COVID-19 pandemic. Sleep Med. (2021) 78:51–6. doi: 10.1016/j.sleep.2020.12.009
21. Jahrami H, BaHammam AS, Bragazzi NL, Saif Z, Faris M, Vitiello MV. Sleep problems during the COVID-19 pandemic by population: a systematic review and meta-analysis. J Clin Sleep Med. (2021) 17:299–313. doi: 10.5664/jcsm.8930
22. Vrublevska J, Sibalova A, Aleskere I, Rezgale B, Smirnova D, Fountoulakis KN, et al. Factors related to depression, distress, and self-reported changes in anxiety, depression, and suicidal thoughts during the COVID-19 state of emergency in Latvia. Nord J Psychiatry. (2021) 75:614–23. doi: 10.1080/08039488.2021.1919200
23. Middelburg RA, Rosendaal FR. COVID-19: how to make between-country comparisons. Int J Infect Dis. (2020) 96:477–81. doi: 10.1016/j.ijid.2020.05.066
24. Olaseni AO, Akinsola OS, Agberotimi SF, Oguntayo R. Psychological distress experiences of Nigerians during Covid-19 pandemic; the gender difference. Soc Sci Humanities Open. (2020) 2:100052. doi: 10.1016/j.ssaho.2020.100052
25. Walker MP, van der Helm E. Overnight therapy? The role of sleep in emotional brain processing. Psychol Bull. (2009) 135:731–48. doi: 10.1037/a0016570
26. Folayan MO, Ibigbami O, El Tantawi M, Brown B, Aly NM, Ezechi O, et al. Factors associated with financial security, food security and quality of daily lives of residents in nigeria during the first wave of the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:7925. doi: 10.3390/ijerph18157925
27. Folayan MO, Ibigbami O, Brown B, El Tantawi M, Uzochukwu B, Ezechi OC, et al. Differences in COVID-19 preventive behavior and food insecurity by HIV status in Nigeria. AIDS Behav. (2021) 2021:1–13. doi: 10.1007/s10461-021-03433-3
28. Nguyen AL, Christensen C, Taylor J, Brown B. Leaning on community-based participatory research to respond during COVID-19. AIDS Behav. (2020) 24:2773–5. doi: 10.1007/s10461-020-02922-1
29. Marg LZ, Heidari O, Taylor J, Marbley C, Scheibel S, Hagan R, et al. A multidimensional assessment of successful aging among older people living with HIV in palm springs, California. AIDS Res Hum Retrov. (2019) 35:1174–80. doi: 10.1089/aid.2019.0048
31. Obiezu T. Fear & Stigma Keep Nigerians from Helping Contact Tracers. Voice of America. (2020). Available online at: https://www.voanews.com/africa/fear-stigma-keep-nigerians-helping-contact-tracers (accessed June 14, 2020).
32. Barbisch D, Koenig KL, Shih FY. Is there a case for quarantine? Perspectives from sars to ebola. Disaster Med Public Health Prep. (2015) 9:547–53. doi: 10.1017/dmp.2015.38
33. Li M, Long J, Wang X, Liao Y, Liu Y, Hao Y, et al. A comparison of COVID-19 stigma and AIDS stigma during the COVID-19 pandemic: a cross-sectional study in China. Front Psychiatry. (2021) 12:782501. doi: 10.3389/fpsyt.2021.782501
34. Jorm AF. Does old age reduce the risk of anxiety and depression? A review of epidemiological studies across the adult life span. Psychol Med. (2000) 30:11–22. doi: 10.1017/S0033291799001452
35. Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol. (2009) 5:363–89. doi: 10.1146/annurev.clinpsy.032408.153621
36. Padayachey U, Ramlall S Chipps J. Depression in older adults: prevalence and risk factors in a primary health care sample. South Afri Family Prac. (2017) 59:61–66. doi: 10.1080/20786190.2016.1272250
37. Taylor WD. Depression in the elderly. N Engl J Med. (2014) 371:1228–36. doi: 10.1056/NEJMcp1402180
38. Seo J, Choi B, Kim S, Lee H, Oh D. The relationship between multiple chronic diseases and depressive symptoms among middle-aged and elderly populations: results of a 2009 Korean community health survey of 156,747 participants. BMC Public Health. (2017) 17:844. doi: 10.1186/s12889-017-4798-2
39. Hajure M, Tariku M, Mohammedhussein M, Dule A. Depression, anxiety and associated factors among chronic medical patients amid COVID-19 pandemic in mettu karl referral hospital, Mettu, Ethiopia, 2020. Neuropsychiatr Dis Treat. (2020) 16:2511–8. doi: 10.2147/NDT.S281995
40. Liang W, Duan Y, Shang B, Hu C, Baker JS, Lin Z, et al. Precautionary behavior and depression in older adults during the COVID-19 pandemic: an online cross-sectional study in Hubei, China. Int J Environ Res Public Health. (2021) 18:1853. doi: 10.3390/ijerph18041853
41. Vahia IV, Jeste DV, Reynolds CF. Older adults and the mental health effects of COVID-19. JAMA. (2020) 324:2253–4. doi: 10.1001/jama.2020.21753
42. Li J, Vitiello MV, Gooneratne NS. Sleep in normal aging. Sleep Med Clin. (2018) 13:1–11. doi: 10.1016/j.jsmc.2017.09.001
43. Suzuki K, Miyamoto M, Hirata K. Sleep disorders in the elderly: diagnosis and management. J Gen Fam Med. (2017) 18:61–71. doi: 10.1002/jgf2.27
44. Unim B, Palmieri L, Lo Noce C, Brusaferro S, Onder G. Prevalence of COVID-19-related symptoms by age group. Aging Clin Exp Res. (2021) 33:1145–7. doi: 10.1007/s40520-021-01809-y
45. Loannidis J, Axfors C, Contopoulos-loannidis D. Population-level COVID-19 mortality risk for non-elderly individuals overall and for nonelderly individuals without underlying diseases in pandemic epicenters. Environ Res. (2020) 188:1–10. doi: 10.1016/j.envres.2020.109890
46. Mueller AL, McNamara MS, Sinclair DA. Why does COVID-19 disproportionately affect older people? Aging. (2020) 12:9959–81. doi: 10.18632/aging.103344
47. Ho FK, Petermann-Rocha F, Gray SR, Jani BD, Katikireddi SV, Niedzwiedz CL, et al. Is older age associated with COVID-19 mortality in the absence of other risk factors? General population cohort study of 470,034 participants. PLoS ONE. (2020) 15:e0241824. doi: 10.1371/journal.pone.0241824
48. McLean CP, Anderson ER. Brave men and timid women? A review of the gender differences in fear and anxiety. Clin Psychol Rev. (2009) 29:496–505. doi: 10.1016/j.cpr.2009.05.003
49. McLean CP, Asnaani A, Litz BT, Hofmann SG. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res. (2011) 45:1027–35. doi: 10.1016/j.jpsychires.2011.03.006
50. Mandelkorn U, Genzer S, Choshen-Hillel S, Reiter J, Meira E Cruz M, Hochner H, et al. Escalation of sleep disturbances amid the COVID-19 pandemic: a cross-sectional international study. J Clin Sleep Med. (2021) 17:45–53. doi: 10.5664/jcsm.8800
51. Jonasdottir SS, Minor K, Lehmann S. Gender differences in nighttime sleep patterns and variability across the adult lifespan: a global-scale wearables study. Sleep. (2021) 44:zsaa169. doi: 10.1093/sleep/zsaa169
52. International Labour Organisation. The Impact of the COVID-19 Pandemic on Jobs and Incomes in G20 Economies. ILO-OECD Paper Prepared at the Request of G20 Leaders Saudi Arabia's G20 Presidency 2020. (2020). Available online at: https://www.ilo.org/wcmsp5/groups/public/—dgreports/—cabinet/documents/publication/wcms_756331.pdf (accessed June 13, 2021).
53. Male breadwinner, female homemaker: patriarchy and women's work-life balance in Nigeria. Human Res Manag Int Digest. (2019) 27:9–11. doi: 10.1108/HRMID-07-2019-0182
54. Akanle O, Nwaobiala UR. Changing but fragile: female breadwinning and family stability in Nigeria. J Asian Afri Stud. (2020) 55:398–411. doi: 10.1177/0021909619880283
55. Jaiyeola EO, Isaac A. Patriarchy and colonization: the “brooder house” for gender inequality in Nigeria. J Res Women Gender. (2020) 10:3–22.
56. Andam K, Edeh H, Oboh V, Pauw K, Thurlow J. Impacts of COVID-19 on food systems and poverty in Nigeria. Adv Food Sec Sustain. (2020) 5:145–73. doi: 10.1016/bs.af2s.2020.09.002
57. Obayelu AE, Obayelu OA, Bolarinwa KK, Oyeyinka RA. Assessment of the immediate and potential long-term effects of COVID-19 outbreak on socioeconomics, agriculture, security of food and dietary intake in Nigeria. Food ethics. (2021) 6:5. doi: 10.1007/s41055-021-00085-w
58. Okunola A,. How COVID-19 Is Hitting Employment in Nigeria — Pushing People Into Poverty. Global Citizens. (2020). Available online at: https://www.globalcitizen.org/en/content/how-covid-19-hitting-employment-nigeria-poverty/ (accessed June 13, 2021).
59. Huang T, Redline S. Cross-sectional and prospective associations of actigraphy-assessed sleep regularity with metabolic abnormalities: the multi-ethnic study of atherosclerosis. Diabetes Care. (2019) 42:1422–9. doi: 10.2337/dc19-0596
60. Wang JL, Schmitz N, Dewa CS. Socioeconomic status and the risk of major depression: the Canadian national population health survey. J Epidemiol Commun Health. (2009) 64:447–452. doi: 10.1136/jech.2009.090910
61. Bjelland J, Krokstad S, Mykletun A, Dahl AA, Tell GS, Tambs K. Does a higher educational level protect against anxiety and depression? The HUNT study. Soc Sci Med. (2008) 66:1334–45. doi: 10.1016/j.socscimed.2007.12.019
62. Strijbos J. Educational Level as a Predictor for Anxiety Depression in ICD-Patients. (2016). Available online at: http://arno.uvt.nl/show.cgi?fid=141103#:~:text=A%20significant%2C%20but%20moderate%2C%20effect,between%20educational%20level%20and%20anxiety (accessed May 22, 2021).
63. Alsharji KE. Anxiety and depression during the COVID-19 pandemic in Kuwait: the importance of physical activity. Middle East Curr Psychiatry. (2020) 27:60. doi: 10.1186/s43045-020-00065-6
Keywords: SARS-CoV-2, mental health, HIV, COVID-19, Nigeria, mental distress
Citation: Folayan MO, Ibigbami O, Brown B, El Tantawi M, Aly NM, Ezechi OC, Abeldaño GF, Ara E, Ayanore MA, Ellakany P, Gaffar B, Al-Khanati NM, Idigbe I, Jafer M, Khan AT-A, Khalid Z, Lawal FB, Lusher J, Nzimande NP, Popoola BO, Quadri MFA, Roque M, Al-Tammemi AB, Yousaf MA, Virtanen JI, Zuñiga RAA, Ndembi N, Nkengasong JN and Nguyen AL (2022) Factors Associated With Experiences of Fear, Anxiety, Depression, and Changes in Sleep Pattern During the COVID-19 Pandemic Among Adults in Nigeria: A Cross-Sectional Study. Front. Public Health 10:779498. doi: 10.3389/fpubh.2022.779498
Received: 18 September 2021; Accepted: 24 January 2022;
Published: 02 March 2022.
Edited by:
Xenia Gonda, Semmelweis University, HungaryReviewed by:
Tomasz M. Gondek, Private Practitioner, Wrocław, PolandSarah Bjedov, University Hospital Centre Zagreb, Croatia
Copyright © 2022 Folayan, Ibigbami, Brown, El Tantawi, Aly, Ezechi, Abeldaño, Ara, Ayanore, Ellakany, Gaffar, Al-Khanati, Idigbe, Jafer, Khan, Khalid, Lawal, Lusher, Nzimande, Popoola, Quadri, Roque, Al-Tammemi, Yousaf, Virtanen, Zuñiga, Ndembi, Nkengasong and Nguyen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Morenike Oluwatoyin Folayan, dG95aW51a3BvbmdAeWFob28uY28udWs=