 Zehao Yu
Zehao Yu Xi Yang
Xi Yang Yi Guo
Yi Guo Jiang Bian
Jiang Bian Yonghui Wu
Yonghui Wu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 28 March 2022
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.778463
This article is part of the Research Topic Measuring and Analysing Social Determinants of Health in the Era of Big Data View all 12 articles
Social determinants of health (SDoH) are important factors associated with cancer risk and treatment outcomes. There is an increasing interest in exploring SDoH captured in electronic health records (EHRs) to assess cancer risk and outcomes; however, most SDoH are only captured in free-text clinical narratives such as physicians' notes that are not readily accessible. In this study, we applied a natural language processing (NLP) system to identify 15 categories of SDoH from a total of 10,855 lung cancer patients at the University of Florida Health. We aggregated the SDoH concepts into patient-level and assessed how each of the 15 categories of SDoH were documented in cancer patient's notes. To the best of our knowledge, this is one of the first studies to examine the documentation of SDoH in clinical narratives from a real-world lung cancer patient cohort. This study could guide future studies to better utilize SDoH information documented in clinical narratives.
As the second leading cause of death in the United States (US) (1), cancer has a long list of risk factors, ranging from biological traits to clinical characteristics to social determinants of health (SDoH) (2). In recent years, there is an increasing interest in examining how SDoH contribute to cancer risk and treatment outcomes (3). The Healthy People 2030 defined SDoH as “the conditions in the environments where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks” and categorized SDoH into 5 domains, including economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context (4). A recent study (5) reported that up to 75% of cancers occurrences are associated with SDoH rather than clinical factors. Other studies have shown that many SDoH contribute to individual cancer risk, influence the likelihood of survival, and affect cancer early prevention and health equity (2, 6, 7). A recent study (8) reported that SDoH factors such as poverty, lack of education, neighborhood disadvantage, and social isolation play important roles in breast cancer stage and survival. Many SDoH factors are also associated with the screening of cervical cancer, breast cancer, and lung cancer (9).
In the past decade, the rapid adoption of electronic health record (EHR) systems has made it possible to use the rich data elements (e.g., disease diagnoses, medications) captured in longitudinal patient's EHR data for cancer studies. However, it is challenging to extract SDoH from EHRs for assessing cancer outcomes as most SDoH were captured as free text in clinical notes rather than structured fields. In February 2018, the World Health Organization (WHO) defined structured codes to capture some of the SDoH. More specifically, the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) Z codes (Z55–Z65) can be used to capture some SDoH. However, our previous study analyzed EHR data in a large clinical research network and showed that the use of SDoH Z codes is still quite low (10). Furthermore, it is unclear how well the SDoH information was documented in clinical notes for cancer patients. On the other hand, natural language processing (NLP) is the key technology to extract SDoH from clinical notes. NLP has been applied to extract various information such as diagnoses, lab tests, side effects from clinical narratives. We have explored many NLP models including state-of-the-art transformer-based NLP models in our previous studies (11–13). In a prior study (14), we have developed an NLP package to systematically extract SDoH from clinical notes using a subset of notes identified with a keyword matching pipeline.
In this study, we identified a cohort of lung cancer patients using ICD-9 and ICD-10 codes from the University of Florida Health (UF Health) system. We applied our NLP pipeline to systematically extract a total of 15 different categories of SDoH and examined the proportion of lung cancer patients who had various SDoH documented in clinical notes. This study is one of the earliest studies to examine how well the SDoH was documented in a real-world cohort of lung cancer patient, which will guide future studies exploring SDoH from clinical text for cancer studies.
In this study, we obtained clinical notes from the UF Health integrated data repository (IDR), a secure clinical data warehouse (CDW) that aggregates data from UF Health's various clinical and administrative information systems including the Epic electronic medical record (EMR) system. We used ICD-9 codes (162*) and ICD-10 codes (C34*) to identify a cohort of lung cancer patients from the UF Health IDR between 2011 and 2020. Patients who had at least one of the ICD-9 or ICD-10 codes and aged at least 18 years were included in the cohort. For each patient, we collected all types of clinical notes associated with the patient, which were used as the resource to extract SDoH concepts.
In our previous study (14), we created an SDoH corpus using 500 notes and developed an NLP pipeline that can extract 5 different categories of SDoH including gender, ethnicity, smoking, employment, and education from clinical narratives. In this study, we further extended the annotation with 10 new SDoH categories including race, alcohol use, drug use, marital status, occupation, language, physical activity, transportation, financial constraint, and social cohesion. Financial constraint indicates patients having a temporary or current financial problem but not in a poverty status (e.g., difficulty paying for the basics). Social cohesion indicates how well the patient connects to the society (e.g., attends religious service). Next, we re-trained the NLP model using this new corpus and developed an upgraded NLP pipeline that can extract a total number of 15 different categories of SDoH from clinical narratives. The transformer-based NLP model using the BERT architecture (15) was used in this study as it achieved the best performance in our previous study (14). BERT is a bidirectional transformer-based NLP model based on masked language modeling (MLM) and uses next-sentence prediction (NSP) to learn representations from text. This SDoH pipeline first identifies the SDoH concepts and then links them to various attributes including status, frequency, and negations. We reused the clinical transformer models developed in our previous study (11) implemented using the HuggingFace (16) package in PyTorch (17). We applied this NLP pipeline to all the clinical notes collected for our lung cancer patient cohort to extract SDoH concepts. Lastly, we aggregated the SDoH concepts at the patient level to assess the proportion of patients who had at least one SDoH concept documented in each of the 15 categories. When there were multiple SDoH instances extracted for one patients of the same category, we adopted majority voting strategy to keep the instance that most frequently documented in clinical notes.
We identified a total of 10,855 lung cancer patients in UF Health between 2011 and 2020 and collected a total of 1,798,409 clinical notes. Table 1 shows a summary of statistics for the demographics of this lung cancer cohort. Most patients (>95%) in this lung cancer cohort are >50 years old; there are more female patients than male and the majority race is White (>72%).
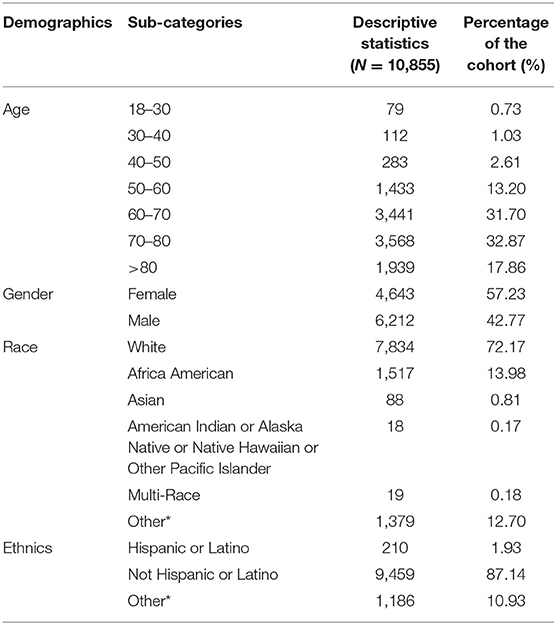
Table 1. Summary of statistics for the lung cancer cohort.
Based on our previous annotation of 5 SDoH categories using 500 clinical notes (14), we further annotated additional 10 SDoH categories and extended the previous annotation from 1,876 SDoH concepts of 5 categories to a total of 5,015 concepts of 15 different SDoH categories. Following the standard NLP development procedure, we divided the annotation into a training set and a test set using a ratio of 4:1. We used the training set to optimize the parameter of a BERT model and used the test set to calculate evaluation scores. We reused the same experiment settings for batch size and learning rate identified from our previous study (14). Using the new extended corpus, the performance (micro average F1 score for all SDoH categories) of our SDoH NLP pipeline based on the BERT model improved from 0.8791 (precision: 0.8848 and recall: 0.8734) to 0.9216 (precision: 0.9298, recall: 0.9136).
We applied the BERT-based NLP pipeline and identified a total number of 5,408,148 SDoH concepts from 1,798,409 clinical notes of 10,855 lung cancer patients. We then aggregated the SDoH concepts at the patient level and calculated the distribution of SDoH concepts for each category. Majority voting was used when there were multiple SDoH instances identified for one SDoH category. Table 2 shows the total number of SDoH concepts identified in each SDoH category and the percentage of patients with at least one SDoH concept in each category. Among the 15 SDoH categories, 3 categories (i.e., gender, alcohol use, and drug use) were extremely frequent-documented in the lung cancer patients, where over 90% of the patients in this cohort had at least one SDoH documented; 5 categories (i.e., marital status, education, occupation, smoking, race) were frequent-documented, where over 70% of the patients had at least one SDoH documented; 7 categories (i.e., ethnicity, language, physical activity, transportation, financial constraint, social cohesion, employment status) were not frequent-documented, where <60% of the patients had at least one SDoH documented.
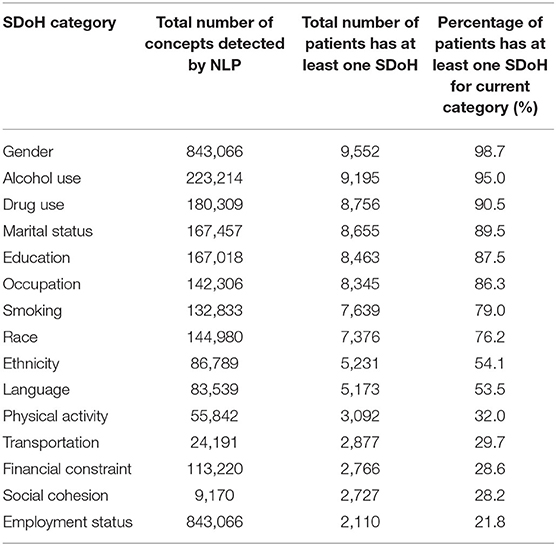
Table 2. Social determinants of health (SDoH) concepts identified from the lung cancer patient cohort.
Many SDoH are associated with cancer risk and cancer treatment outcomes. Yet, information related to SDoH is often unavailable in structured EHRs but is often documented in clinical notes as free text, making it challenging to examine SDoH in cancer research. In this study, we identified a cohort of lung cancer patients and applied our NLP system to extract SDoH concepts from 15 categories of SDoH. We examined the distribution of SDoH in each category and evaluated how frequent SDoH was documented for categories. This study will guide future cancer studies that aim to explore SDoH information from clinical notes.
The data analyzed in this study is subject to the following licenses/restrictions: we obtained clinical notes from the UF Health integrated data repository (IDR), a secure clinical data warehouse (CDW) that aggregates data from UF Health's various clinical and administrative information systems including the Epic electronic medical record (EMR) system. Requests to access these datasets should be directed to UF CSTI, aW5mb0BjdHNpLnVmbC5lZHU=.
JB, YG, and YW were responsible for the overall design, development, and evaluation of this study. XY collected the data used in this study and involved in the results analysis. ZY conducted the experiments and data analysis. YW did the initial drafts and revisions of the manuscript. All authors reviewed the manuscript critically for scientific content and gave final approval of the manuscript for publication.
This study was partially supported by a Patient-Centered Outcomes Research Institute® (PCORI®) Award (ME-2018C3-14754), a Grant from National Institute on Aging 1R56AG 069880, a Grant from the National Cancer Institute, 1R01CA246418 R01, and the Cancer Informatics and eHealth core jointly supported by the UF Health Cancer Center and the UF Clinical and Translational Science Institute.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding institutions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the NVIDIA Corporation with the donation of the GPUs used for this research.
1. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Lond Engl. (2015) 385:117–71. doi: 10.1016/S0140-6736(14)61682-2
2. Hiatt RA, Breen N. The social determinants of cancer: a challenge for transdisciplinary science. Am J Prev Med. (2008) 35:S141–150. doi: 10.1016/j.amepre.2008.05.006
3. Braveman P, Gottlieb L. The social determinants of health: it's time to consider the causes of the causes. Public Health Rep. (2014) 129 Suppl 2:19–31. doi: 10.1177/00333549141291S206
4. Social Determinants of Health. Healthy People 2030 | health.gov. Available online at: https://health.gov/healthypeople/objectives-and-data/social-determinants-health (accessed September 14, 2021).
5. Akushevich I, Kravchenko J, Akushevich L, Ukraintseva S, Arbeev K, Yashin A. Cancer Risk Behavioral Factors, Comorbidities, Functional Status in the US Elderly Population. ISRN Oncol (2011) 2011. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3197174/ (accessed February 3, 2019).
6. Matthews AK, Breen E, Kittiteerasack P. Social determinants of LGBT cancer health inequities. Semin Oncol Nurs. (2018) 34:12–20. doi: 10.1016/j.soncn.2017.11.001
7. Gerend MA, Pai M. Social determinants of Black-White disparities in breast cancer mortality: a review. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. (2008) 17:2913–23. doi: 10.1158/1055-9965.EPI-07-0633
8. Coughlin SS. Social determinants of breast cancer risk, stage, and survival. Breast Cancer Res Treat. (2019) 177:537–48. doi: 10.1007/s10549-019-05340-7
9. Lofters AK, Schuler A, Slater M, Baxter NN, Persaud N, Pinto AD, et al. Using self-reported data on the social determinants of health in primary care to identify cancer screening disparities: opportunities and challenges. BMC Fam Pract. (2017) 18:31. doi: 10.1186/s12875-017-0599-z
10. Guo Y, Chen Z, Xu K, George TJ, Wu Y, Hogan W, et al. International classification of diseases, tenth revision, clinical modification social determinants of health codes are poorly used in electronic health records. Medicine. (2020) 99:e23818. doi: 10.1097/MD.0000000000023818
11. Yang X, Bian J, Hogan WR, Wu Y. Clinical concept extraction using transformers. J Am Med Inform Assoc JAMIA. (2020) 27:1935–42. doi: 10.1093/jamia/ocaa189
12. Yang X, Bian J, Wu Y. Detecting medications and adverse drug events in clinical notes using recurrent neural networks. In: International Workshop on Medication and Adverse Drug Event Detection (2018). p. 1–6. Available online at: http://proceedings.mlr.press/v90/yang18a.html (accessed June 2, 2018).
13. Yang X, Bian J, Fang R, Bjarnadottir RI, Hogan WR, Wu Y. Identifying relations of medications with adverse drug events using recurrent convolutional neural networks and gradient boosting. J Am Med Inform Assoc JAMIA. (2020) 27:65–72. doi: 10.1093/jamia/ocz144
14. Yu Z, Yang X, Dang C, Wu S, Adekkanattu P, Pathak J. A Study of Social Behavioral Determinants of Health in Lung Cancer Patients Using Transformers-based Natural Language Processing Models. arXiv210804949 Cs (2021). Available online at: http://arxiv.org/abs/2108.04949 (accessed September 15, 2021).
15. Devlin J, Chang MW, Lee K, Toutanova K. BERT: Pre-training of Deep Bidirectional Transformers for Language Understanding. Available online at: https://arxiv.org/abs/1810.04805 (accessed October 30, 2018).
16. Wolf T, Debut L, Sanh V, Chaumond J, Delangue C, Moi A, et al. HuggingFace's Transformers: State-of-the-art Natural Language Processing. arXiv191003771 Cs. Available online at: http://arxiv.org/abs/1910.03771 (accessed March 5, 2021).
17. Paszke A, Gross S, Massa F, Lerer A, Bradbury J, Chanan G, et al. PyTorch: An Imperative Style, High-Performance Deep Learning Library. arXiv191201703 Cs. Available online at: http://arxiv.org/abs/1912.01703 (accessed March 5, 2021).
Keywords: electronic health records, natural language processing, cancer, social determinants of health (SDOH), lung cancer
Citation: Yu Z, Yang X, Guo Y, Bian J and Wu Y (2022) Assessing the Documentation of Social Determinants of Health for Lung Cancer Patients in Clinical Narratives. Front. Public Health 10:778463. doi: 10.3389/fpubh.2022.778463
Received: 16 September 2021; Accepted: 28 February 2022;
Published: 28 March 2022.
Edited by:
Angela Kaida, Simon Fraser University, CanadaReviewed by:
Liwei Wang, Mayo Clinic, United StatesCopyright © 2022 Yu, Yang, Guo, Bian and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yonghui Wu, WW9uZ2h1aS53dUB1ZmwuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.