 Tingting Qiu
Tingting Qiu Michal Pochopien2
Michal Pochopien2 Gauri Saal
Gauri Saal
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Public Health , 09 February 2022
Sec. Health Economics
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.773629
This article is part of the Research Topic Gene and Cell Therapies: Through the Perspective of Health Economics View all 7 articles
Gene therapies (GTs) are considered to be a paradigm-shifting class of treatments with the potential to treat previously incurable diseases or those with significant unmet treatment needs. However, considerable challenges remain in their health technology assessment (HTA), mainly stemming from the inability to perform robust clinical trials to convince decision-makers to pay the high prices for the potential long-term treatment benefits provided. This article aims to review the recommendations that have been published for evidence generation and economic analysis for GTs against the feasibility of their implementation within current HTA decision analysis frameworks. After reviewing the systematically identified literature, we found that questions remain on the appropriateness of GT evidence generation, considering that additional, broader values brought by GTs seem insufficiently incorporated within proposed analytic methods. In cases where innovative methods are proposed, HTA organizations remain highly conservative and resistant to change their reference case and decision analysis framework. Such resistances are largely attributed to the substantial evidence uncertainty, resource-consuming administration process, and the absence of consensus on the optimized methodology to balance all the advantages and potential pitfalls of GTs.
Gene therapies (GTs) have shown extraordinary promise for the mitigation or potential cure of a broad spectrum of life-threatening or debilitating diseases, such as cancers and retinal disorders (1). Yet, despite the innovative treatment paradigm and exceptional clinical benefits potentially provided by some GTs (2, 3), numerous obstacles to efficient market access prevail (4). These obstacles range from resource-consuming manufacturing processes to reimbursement and funding challenges (4–8). In two key instances, the sum of these obstacles has even proven to be unmanageable, and as such, the GTs has been withdrawn from the market (4, 9).
In particular, the limited clinical evidence and high up-front treatment costs for GTs have challenged their evaluations in health technology assessment (HTA); hence, specific considerations have been needed. Recommendations to mitigate such uncertainties in payer decision-making of GTs continue to be published since the first GT, alipogene tiparvovec (Glybera®), was approved in Europe in 2012 (10). However, the feasibility of integrating the evidence generation approaches into existing HTA guidelines or decision analysis frameworks (DAFs) remains unclear. The applicability of these recommendations and the utility of the existing evidence could be limited, therefore delaying the inclusion of the GTs into health system formularies and thus patient access (11). To this end, we have reviewed the published recommendations for evidence generation and economic analysis for GTs, with an aim to critically explore the feasibility of implementing the recommended approaches within current HTA DAFs (Table 1).
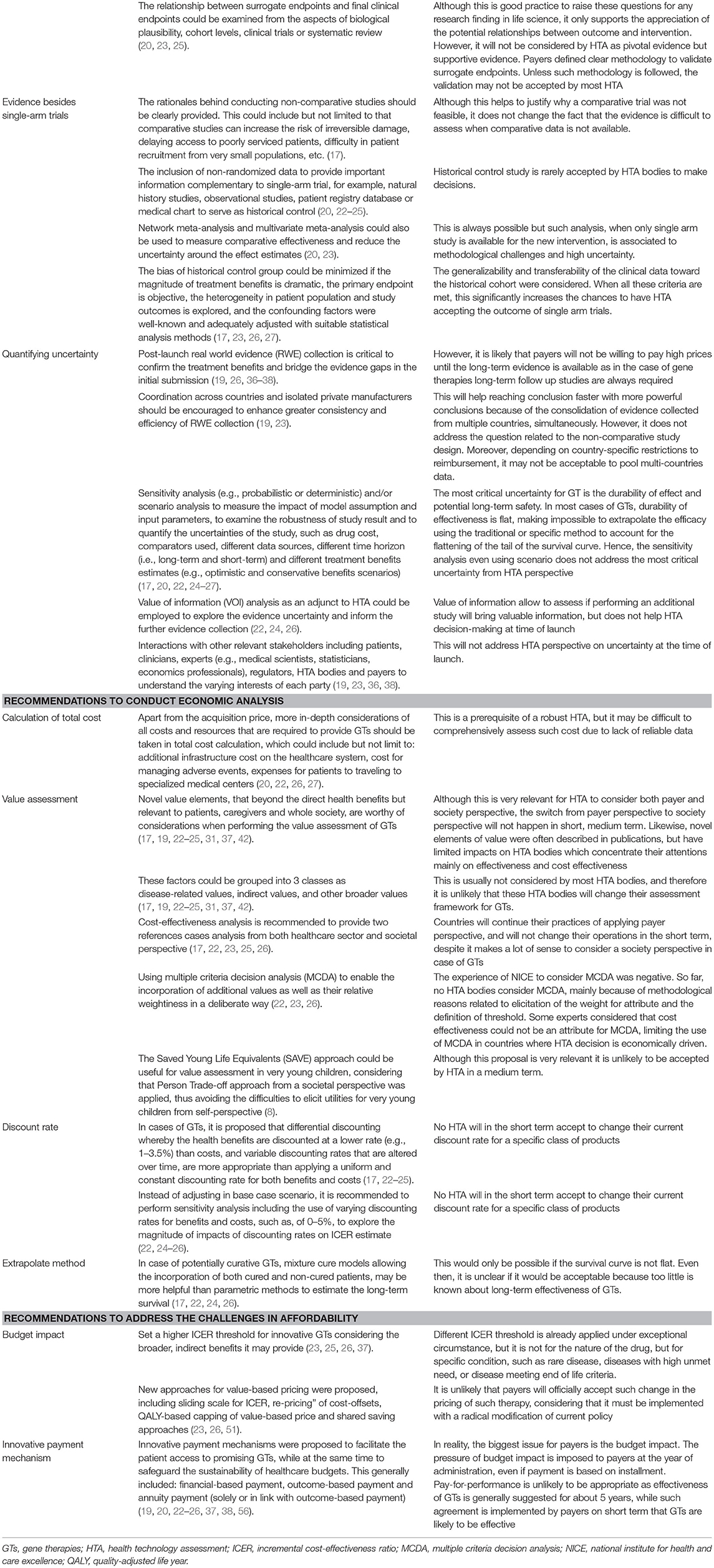
Table 1. Recommendations from publications and our perspectives.
Following a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol, we identified articles in Medline and Embase published in English in the last 5 years that proposed any recommendations for the evidence generation for GTs as based on clinical evidence needs, economic analysis, and payer affordability considerations. The details for the search strategy and PRISMA diagram were provided in Supplementary Table 1 and Supplementary Figure 1, respectively.
Randomized controlled parallel trials (RCTs) are inarguably accepted as the gold standard approach for establishing the safety and efficacy of a new intervention (12, 13). However, RCTs for evaluating some therapies are not always feasible, especially in life-threatening or rare diseases for which therapeutic options have been exhausted (14, 15), Hence, evidence standards for regulatory approval have been made flexible to allow rapid approval of potentially effective therapies such as GTs, allowing small sample sizes or single-arm studies (16–18) being accepted to enable licensing of the treatments (19, 20).
However, such limited data have created larger-than-usual gaps for GT evidence needs (16), and strategies to improve the strength of evidence for GTs have been recommended (21). First, the inclusion of other types of non-randomized study designs could provide complementary evidence to single-arm trial data. For example, these designs could include natural history studies, observational studies, patient registry databases, or medical chart extractions to serve as historical controls (20, 22–25).
However, reducing the bias of historical control groups to complement single-arm trials must also be minimized, and the following aspects could be considered (17, 23, 26, 27): (1) the evidence suggests that the magnitude of the treatment effect size vs. the historical group is dramatic; (2) the primary endpoint is objective, durable and reproducible; (3) the heterogeneity in the patient population and study outcomes is explored and adequately adjusted with suitable statistical analysis methods (23); (4) the confounding factors are adequately adjusted with suitable statistical analysis methods; and (5) the generalizability and transferability of the clinical data toward the historical cohort were considered and discussed. In addition, network meta-analysis and multivariate meta-analysis could be used to measure comparative effectiveness and (23) reduce the uncertainty around the effect estimates obtained from the single-arm studies (20).
DAF considerations: Although numerous approaches to reduce payer uncertainties with single-arm studies have been published, HTA guidance on assessing evidence from single-arm trials remains scant (21). In addition, HTA bodies are more likely to accept indirect comparisons for demonstrating non-inferiority but are cautious to accept such evidence for demonstrating superiority (28). Payer uncertainties have been further fueled by the recent challenges of when data were collected in terms of the coronavirus disease 2019 (COVID-19) pandemic, which has added other confounding issues (29). Therefore, synthetic controls with high patient and outcome similarity may be more appropriate than historical controls with retrospective observational studies (30).
Due to limited long-term follow-up, the effectiveness of GTs is typically investigated on surrogate endpoints (31), especially in very rare diseases or clinically slowly progressive diseases (20). However, by having to extrapolate based on biomarker-based treatment benefits, payers are left with the uncertainty of the treatment's true clinical benefits (32). Hence, determining the appropriate approaches for the measurement and validation of surrogate endpoints for GTs concerning final clinical endpoints [e.g., mortality, survival, or health-related quality-of-life (HRQoL)] is a key consideration in HTA (22–24).
The literature has suggested that the relationships between surrogate endpoints and final clinical endpoints must be examined for: (1) biological plausibility (20, 25); (2) the association between the surrogate and the final outcome across cohorts or at the level of the individual patient (20, 25); (3) evidence that the technology improves the surrogate and the final outcome in other clinical trials, epidemiological studies or registries. In the case of GTs for rare diseases, the evidence of the same surrogate endpoints elicited from similar diseases with higher prevalence could be considered (25); (4) meta-analysis supporting the validation of surrogate endpoints to final endpoints (25); and (5) improved knowledge on the significance of biomarkers that enhance the acceptance of reliable biomarkers to demonstrate clinical benefits (23).
DAF considerations: Few HTA agencies currently provide guidelines on statistical methods to validate surrogate endpoints, nor provide explicit criteria to decide whether specific surrogate endpoints are more valid than others (33, 34). Furthermore, validating surrogate endpoints from natural history data from patient registries in rare conditions is particularly difficult given the limited availability of such databases (35).
The most critical uncertainties for GTs are the long-term effectiveness and safety. Therefore, there is a high level of consensus regarding the importance of post-launch real-world evidence (RWE) to confirm treatment benefits and bridge the evidence gaps in the initial regulatory and HTA submissions for GTs (19, 26, 32, 36–38). To enhance greater consistency and efficiency of RWE collection, coordination across countries has been encouraged (19, 23, 39). In addition, the value of information (VOI) analysis will allow assessing whether performing additional studies will provide robust added data (40).
DAF considerations: Depending on country-specific restrictions on reimbursement and local clinical practices, the transferability of data may be challenged. Moreover, while VOI analysis can support decision-making on the need to perform additional studies (40), it does not help HTA decision-making at the time of launch, in addition to the challenges for implementation given technical and policy-related reasons (41).
Novel economic value elements to patients, caregivers, and the whole society, that extend beyond the direct patient health benefits, are worthy of consideration when performing the value assessment of GTs. The type of treatment benefits associated with GTs ranges broadly and include clinical benefits, including quality-adjusted life-year (QALY) gains, and indirect benefits, such as the continuation of normal education, improvement of productivity, and reduction in the caring burdens of family members. In addition, GTs can bring other broader forms of value, such as scientific spillover, adherence improving factors, health equity issues, and value of cure (17, 19, 22–25, 31, 37, 42).
However, these broader values are not or insufficiently captured in the QALY and incremental cost-effectiveness ratio (ICER) calculation in current HTA reference cases. Hence, it has been argued that cost-effectiveness should provide references cases analyses from both healthcare payer and societal perspectives (17, 22, 23, 25, 26). Cost-benefit analysis has also been proposed as an option to allow capturing of all types of benefits as measured in monetary terms (17). The most commonly proposed approach for the measurements of broader values is termed “multiple criteria decision analysis” (MCDA) (22, 23, 26), which could enable the incorporation of additional values as well as their relative weight in a deliberate way.
DAF considerations: While numerous publications propose novel elements of value, these have had limited influence on HTA bodies which focus predominantly on clinical effectiveness and cost-effectiveness. Some broader disease-related value elements (i.e., disease severity and unmet need) are already incorporated in some agencies such as the Haute Autorité de Santé (HAS, France), Agenzia Italiana del Farmaco (AIFA, Italy), and the Spanish Agency for Evaluation of Medicines and Healthcare and the Products Interministerial Committee for Pricing (AEMPS and CIPM). Other agencies including the National Institute for Health and Care Excellence (NICE, England) and the Scottish Medical Consortium (SMC, Scotland) tend to incorporate modifiers to the ICER threshold and social cost when applicable, while Tandvårds-och läkemedelsförmånsverket (TLV, Sweden) and Zorginstituut Nederland (ZIN, The Netherlands) also consider indirect benefits (i.e., productivity improvement). However, broader societal values (i.e., scientific spill-overs and value of cure) are rarely considered (43–45). As such, it is unlikely that national HTA bodies will change their positions on the elements of value they are willing to consider. For example, despite being the output of joined EU effort, the HTA core model by EUnetHTA which considered these broader value elements (46) has hardly been implemented to date.
Moreover, the experience of the NICE to consider quantitative MCDA was negative, suggesting that flexible deliberation is preferred over stringent rules (47).
Hence, while it is very relevant for HTA to consider both payer and society perspectives of treatment benefits for an optimized resource allocation, especially for innovative and breakthrough therapies including GTs, the adoption of the societal perspectives cannot be assumed to occur in the short- or medium terms in countries where this perspective is presently not considered due to a tight administrative or time constraints (48).
Apart from the acquisition price, it has been raised that more universal costs and resources associated with GTs should be taken in the total cost calculation (22, 27). For example, these include but are not limited to additional infrastructure costs on the healthcare system (20), the cost for managing adverse events (26), and expenses for patients to travel to specialized medical centers for procedures such as for Chimeric Antigen Receptor T cell (CAR-T) treatment (22).
DAF considerations: A robust HTA requires that the estimations of the total cost be as accurate as possible; however, it may be difficult to capture this information due to the lack of reliable data sources for the rare diseases treated by GTs. Additionally, there remains much heterogeneity and paucity of data in cost structure, cost drivers of administration of GTs, and patients' management-related costs.
It is argued that the discounting rates currently applied by HTA bodies are generally too high for GTs (17, 22, 23, 25) given its potential long-term benefits. Although it is common practice to apply a uniform and constant discounting rate for both benefits and costs over time (20), in cases of GTs, the justification of differential discounting has been made. This would entail health benefits to be discounted at a lower rate (e.g., 1–3.5%) than costs (22, 24), and variable discounting rates that are altered over time (22). Alternatively, sensitivity analysis is also recommended, including the use of varying discounting rates for benefits and costs (22, 24–26), such as, of 0–5%, to explore the magnitude of impacts of discounting rates on ICER estimate.
DAF considerations: Although a lower discounting rate (e.g., 1.5% by NICE) than normally applied has been explored for products with long-term benefits or studies with longer time horizon, such as 2.5 % when time horizon <30 years, and 1.5% thereafter in France (49), the problems identified are related to the uncertainty in the long-term benefits sufficiently meeting the defined criteria. Moreover, a declining discounting rule has been criticized for being inconsistent and unjustified (50).
In general, HTA bodies are not highly flexible on the current rules for applying a specific discount rate for a specific class of products simply afforded by its novel mechanism of action. In fact, the choice of discount rates is fundamentally subject to the local conditions and policies of the different HTA agencies, such as factors concerning public health and the economy (23, 24).
According to the hypothesis that GTs are associated with broader, indirect values not adequately captured in the QALY estimate, some publications have recommended setting a higher ICER threshold for innovative GTs (17, 19, 23, 25, 26, 37). Other innovative approaches for value-based pricing have also been proposed, including the sliding scale for ICER, re-pricing” of cost-offsets, QALY-based capping of value-based price, and shared saving approaches (23, 26, 51).
DAF considerations: With higher payer willingness to pay thresholds comes the possibility that developers will be motivated to inflate the price of GTs to meet the ICER threshold (52, 53), in other words, the developers will charge the price as high as the payer are able to endure (26). It is unlikely that payers will accept innovative value-pricing methods, considering that they must be implemented with a radical modification of current policy. Obviously, GT discovery and development is flourishing, suggesting current incentives are attractive enough for developers.
Partitioned survival models, which are commonly used for the extrapolation of long-term survival for patients with cancer, have enabled early access to oncology treatments and regulatory approval based on early clinical data. However, for the economic evaluation of GTs specific to some rare diseases, partitioned survival models lack sufficient ability to reflect the patient trajectories (27), and often fail to properly incorporate uncertainty around parameter estimates (23) and complexity of diseases (22). In the case of GTs, mixture cure models allowing the incorporation of both cured and non-cured patients, have been recommended as more useful than parametric methods to estimate the long-term survival (17, 22, 24, 26).
DAF considerations: Extrapolations on long-term GT outcomes are only possible if efficacy shows a drop during the observation period. In most cases of GTs, the durability of effectiveness is flat, during the pre-approval period, making it impossible to extrapolate efficacy using the parametric or non-parametric methods. In addition, the adoption of new methodologies for the extrapolation of the survival curve can be a lengthy process. For example, a recent study confirmed that survival for nivolumab was underestimated using different parametric and non-parametric methods (54). However, NICE issued the guideline for flexible methods for survival analysis only after substantial evidence has accumulated to prove that standard parametric extrapolation is not fitted for treatments with a delayed response, such as immunotherapy (55). Long-term accumulation of robust evidence will nonetheless shift the current resistance of HTA to consider non-conventional extrapolation methods.
Despite the measured cost-effectiveness of GTs, the impact of their high upfront cost on payer budgets remain (17, 19, 25, 26). Therefore, innovative payment mechanisms have been proposed to facilitate patient access to promising GTs, meanwhile safeguarding the sustainability of healthcare budgets. Such mechanisms have mainly comprised: financial-based payment (19, 22–24, 26, 56). including simple discount, rebates, volume-based pricing, “Netflix subscription” model, funding-based payment, re-insurance, and healthcare loans; outcome-based payment (19, 22, 23, 25, 26, 37, 38, 56), including pay-for-performance and risk-sharing agreements; and annuity or installment payment (solely or in link with outcome-based payment) (20, 22, 23, 26, 56) and amortization (19, 57).
DAF considerations: Generally evidenced for about 5 years, pay-for-performance agreements cannot be practical mechanisms for funding GTs, given the inadequate window of time to assess the effectiveness of the treatment. Thus, the ability of pay-for-performance mechanisms to account for the long-term uncertainty associated with GTs is limited. In addition, the pressure of budget impact is imposed on payers at the year of administration, even if payment is based on installment. Indeed, generally accepted accounting principles require that a consumable (such as a drug) is accounted for on the balance sheet within the year of acquisition. However, the key accounting principle of amortization may offer a new approach for healthcare payers to unlock access to GTs while spreading the budget impact over several years (58).
Our review has summarized several approaches for HTA evidence generation to meet the idiosyncrasies of GTs. While these theoretical perspectives are rational and necessary, from a pragmatic perspective, much flexibility is necessary from HTA bodies to put recommendations into practice. Yet, the flexibility of tailoring current DAFs within HTA organizations is not a likely reality in the near term.
While a new class of product with a novel mechanism of action may stimulate arguments that a specific reference case is necessary, mainstream opinions indicate that adjustments could be considered for GTs, although a new reference case is not needed (25). For example, NICE has delivered systematically negative decisions for most innovative oncology products until the end-of-life criteria tailor-made for oncology was introduced several years later, which enabled a higher ICER threshold to be acceptable for products satisfying the pre-defined standards. Other initiatives included Cancer Drug Fund was introduced by NHS England to temporarily reimburse oncology drugs with promising clinical benefits but associated with significant uncertainties, and a highly specialized technology (HST) pathway to evaluate the expensive drugs indicated for a distinct group of diseases, such as ultra-rare conditions. These examples suggest how conservative HTA bodies can be in modifying their DAF or their reference case.
Hence, given all the evidence needed for GTs, to ensure fair and timely evolution of DAF of HTA proactive interactions with relevant stakeholders could be powerful and well-warranted (19, 38), and to include patients, clinicians, experts (e.g., medical scientists, statisticians, and pharmacoeconomics professionals), industry representatives, regulators, and HTA bodies. Such collaboration will allow more knowledge on the varying interests and expectations of each party (36), and also offer advantages to foster a better understanding of the scientific mechanisms of the interventions (23), to increase the reliability of the estimates on magnitude and durability of treatment benefits (17). Recently a checklist was published providing a pragmatic approach that could easily be adopted by HTA (25). In the absence of such an initiative, scientific publications and recommendations continue to accumulate on this topic; although important from an academic perspective, they will have limited impacts on GT HTA.
Published recommendations for evidence generation and economic assessment of GTs currently appear to have limited impact on HTA DAF due to either them being more theoretical in orientation rather than being pragmatic or because of conservative attitudes of HTA on DAF. Multi-stakeholders dialogue is warranted to enhance communications that will allow more certain and rapid assessments of GTs, thus enabling optimized patient access at a reasonable budget impact.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
MT conceived the design of this review, drafted the table of contents, and provided expert insights. TQ and GS wrote the entire manuscript. MP, SL, EP, and JJ contributed to the literature searches and abstract drafting. All authors contributed to the article and approved the submitted version.
MP, EP, JJ, and MT was employed by the company Creativ-Ceutical. GS was employed by company Apothecom.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.773629/full#supplementary-material
1. Buzhor E, Leshansky L, Blumenthal J, Barash H, Warshawsky D, Mazor Y, et al. Cell-based therapy approaches: the hope for incurable diseases. Regen Med. (2014) 9:649–72. doi: 10.2217/rme.14.35
2. Qiu T, Hanna E, Dabbous M, Borislav B, Toumi M. Health technology assessment of gene therapies in europe and the USA: analysis and future considerations. Cell Gene Ther Insights. (2019) 5:1043–59. doi: 10.18609/cgti.2019.112
3. Pochopien M, Qiu T, Aballea S, Clay E, Toumi M. Considering potential solutions for limitations and challenges in the health economic evaluation of gene therapies. Expert Rev Pharmacoecon Outcomes Res. (2021) 21:1145–58. doi: 10.1080/14737167.2021.1969229
4. Abou-El-Enein M, Elsanhoury A, Reinke P. overcoming challenges facing advanced therapies in the EU market. Cell Stem Cell. (2016) 19:293–7. doi: 10.1016/j.stem.2016.08.012
5. Galipeau J, Sensebe L. Mesenchymal stromal cells: clinical challenges and therapeutic opportunities. Cell Stem Cell. (2018) 22:824–33. doi: 10.1016/j.stem.2018.05.004
6. Iancu EM, Kandalaft LE. Challenges and advantages of cell therapy manufacturing under Good Manufacturing Practices within the hospital setting. Curr Opin Biotechnol. (2020) 65:233–41. doi: 10.1016/j.copbio.2020.05.005
7. Nestler-Parr S, Korchagina D, Toumi M, Pashos CL, Blanchette C, Molsen E, et al. Challenges in research and health technology assessment of rare disease technologies: report of the ISPOR rare disease special interest group. Value Health. (2018) 21:493–500. doi: 10.1016/j.jval.2018.03.004
8. Delhove J, Osenk I, Prichard I, Donnelley M. Public Acceptability of Gene Therapy and Gene Editing for Human Use: A Systematic Review. Hum Gene Ther. (2020) 31:20–46. doi: 10.1089/hum.2019.197
9. Chakraverty A. Bluebird Bio Withdrawal Raises Gene Therapy Doubts in Europe. (2021). Available online at: https://www.labiotech.eu/trends-news/bluebird-bio-gene-therapy-zynteglo/ (accessed August 8, 2021).
10. Hanna E, Remuzat C, Auquier P, Toumi M. Advanced therapy medicinal products: current and future perspectives. J Mark Access Health Policy. (2016) 4. doi: 10.3402/jmahp.v4.31036
11. Abou-El-Enein M, Grainger DW, Kili S. Registry contributions to strengthen cell and gene therapeutic evidence. Mol Ther. (2018) 26:1172–6. doi: 10.1016/j.ymthe.2018.04.007
12. Hariton E, Locascio JJ. Randomised controlled trials - the gold standard for effectiveness research: study design: randomised controlled trials. BJOG. (2018) 125:1716. doi: 10.1111/1471-0528.15199
13. Moloney R, Mohr P, Hawe E, Shah K, Garau M, Towse A. Payer perspectives on future acceptability of comparative effectiveness and relative effectiveness research. Int J Technol Assess Health Care. (2015) 31:90–8. doi: 10.1017/S0266462315000203
14. Riva L, Petrini C. A few ethical issues in translational research for gene and cell therapy. J Transl Med. (2019) 17:395. doi: 10.1186/s12967-019-02154-5
15. Rath A, Salamon V, Peixoto S, Hivert V, Laville M, Segrestin B, et al. A systematic literature review of evidence-based clinical practice for rare diseases: what are the perceived and real barriers for improving the evidence and how can they be overcome? Trials. (2017) 18:556. doi: 10.1186/s13063-017-2287-7
16. Abou-El-Enein M, Hey SP. Cell and gene therapy trials: are we facing an ‘evidence crisis’? EClinicalMedicine. (2019) 7:13–4. doi: 10.1016/j.eclinm.2019.01.015
17. Aballéa S, Thokagevistk K, Velikanova R, Simoens S, Annemans L, Antonanzas F, et al. Health economic evaluation of gene replacement therapies: methodological issues and recommendations. J Market Access Health Policy. (2020) 8:1822666. doi: 10.1080/20016689.2020.1822666
18. Elsallab M, Bravery CA, Kurtz A, Abou-El-Enein M. Mitigating deficiencies in evidence during regulatory assessments of advanced therapies: a comparative study with other biologicals. Mol Ther Methods Clin Dev. (2020) 18:269–79. doi: 10.1016/j.omtm.2020.05.035
19. Hampson G, Towse A, Pearson SD, Dreitlein WB, Henshall C. Gene therapy: evidence, value and affordability in the US health care system. J Comp Eff Res. (2018) 7:15–28. doi: 10.2217/cer-2017-0068
20. Hettle R, Corbett M, Hinde S, Hodgson R, Jones-Diette J, Woolacott N, et al. The assessment and appraisal of regenerative medicines and cell therapy products: an exploration of methods for review, economic evaluation and appraisal. Health Technol Assess. (2017) 21:1–204. doi: 10.3310/hta21070
21. Patel D, Grimson F, Mihaylova E, Wagner P, Warren J, van Engen A, et al. Use of external comparators for health technology assessment submissions based on single-arm trials. Value Health. (2021) 24:1118–25. doi: 10.1016/j.jval.2021.01.015
22. Ten Ham RMT, Klungel OH, Leufkens HGM, Frederix GWJ. A review of methodological considerations for economic evaluations of gene therapies and their application in literature. Value Health. (2020) 23:1268–80. doi: 10.1016/j.jval.2020.04.1833
23. Coyle D, Durand-Zaleski I, Farrington J, Garrison L, Graf von der Schulenburg JM, Greiner W, et al. HTA methodology and value frameworks for evaluation and policy making for cell and gene therapies. Eur J Health Econ. (2020) 21:1421–37. doi: 10.1007/s10198-020-01212-w
24. Jonsson B, Hampson G, Michaels J, Towse A, von der Schulenburg JG, Wong O. Advanced therapy medicinal products and health technology assessment principles and practices for value-based and sustainable healthcare. Eur J Health Econ. (2019) 20:427–38. doi: 10.1007/s10198-018-1007-x
25. Drummond MF, Neumann PJ, Sullivan SD, Fricke FU, Tunis S, Dabbous O, et al. Analytic considerations in applying a general economic evaluation reference case to gene therapy. Value Health. (2019) 22:661–8. doi: 10.1016/j.jval.2019.03.012
26. Angelis A, Naci H, Hackshaw A. recalibrating health technology assessment methods for cell and gene therapies. Pharmacoeconomics. (2020) 38:1297–308. doi: 10.1007/s40273-020-00956-w
27. Raymakers AJN, Regier DA, Peacock SJ. Modelling uncertainty in survival and cost-effectiveness is vital in the era of gene therapies: the case of axicabtagene ciloleucel. Health Policy Technol. (2019) 8:103–4. doi: 10.1016/j.hlpt.2019.05.009
28. Es-Skali IJ, Spoors J. Analysis of indirect treatment comparisons in national health technology assessments and requirements for industry submissions. J Compar Effect Res. (2018) 7:397–409. doi: 10.2217/cer-2017-0092
29. Qiu T, Wang Y, Liang S, Han R, Toumi M. The impact of COVID-19 on the cell and gene therapies industry: disruptions, opportunities, and future prospects. Drug Discov Today. (2021) 26:2269–81. doi: 10.1016/j.drudis.2021.04.020
30. Thorlund K, Dron L, Park JJH, Mills EJ. Synthetic and external controls in clinical trials - a primer for researchers. Clin Epidemiol. (2020) 12:457–67. doi: 10.2147/CLEP.S242097
31. Gavan SP, Lu CY, Payne K. Assessing the joint value of genomic-based diagnostic tests and gene therapies. J Pers Med. (2019) 9:28. doi: 10.3390/jpm9020028
32. Downing NS, Aminawung JA, Shah ND, Krumholz HM, Ross JS. Clinical trial evidence supporting FDA approval of novel therapeutic agents, 2005–2012. JAMA. (2014) 311:368–77. doi: 10.1001/jama.2013.282034
33. Grigore B, Ciani O, Dams F, Federici C, de Groot S, Möllenkamp M, et al. Surrogate endpoints in health technology assessment: an international review of methodological guidelines. Pharmacoeconomics. (2020) 38:1055–70. doi: 10.1007/s40273-020-00935-1
34. Burzykowski T, Buyse M. Surrogate threshold effect: an alternative measure for meta-analytic surrogate endpoint validation. Pharm Stat. (2006) 5:173–86. doi: 10.1002/pst.207
35. Gagne JJ, Thompson L, O'Keefe K, Kesselheim AS. Innovative research methods for studying treatments for rare diseases: methodological review. BMJ. (2014) 349:g6802. doi: 10.1136/bmj.g6802
36. Annemans L, Makady A. TRUST4RD: tool for reducing uncertainties in the evidence generation for specialised treatments for rare diseases. Orphanet J Rare Dis. (2020) 15:127. doi: 10.1186/s13023-020-01370-3
37. Goncalves E. Advanced therapy medicinal products: value judgement and ethical evaluation in health technology assessment. Eur J Health Econ. (2020) 21:311–20. doi: 10.1007/s10198-019-01147-x
38. CADTH. Gene Therapy: International Regulatory and Health Technology Assessment Activities and Reimbursement Status. (2018). Available online at: https://www.cadth.ca/gene-therapy-international-regulatory-and-health-technology-assessment-activities-and-reimbursement (accessed May 20, 2021).
39. Makady A, van Veelen A, Jonsson P, Moseley O, D'Andon A, de Boer A, et al. Using Real-World Data in Health Technology Assessment (HTA) practice: a comparative study of five HTA agencies. Pharmacoeconomics. (2018) 36:359–68. doi: 10.1007/s40273-017-0596-z
40. Corro Ramos I, Rutten-van Mölken MPMH, Al MJ. The role of value-of-information analysis in a health care research priority setting: a theoretical case study. Medical Decision Making. (2012) 33:472–89. doi: 10.1177/0272989X12468616
41. Tuffaha HW, Gordon LG, Scuffham PA. Value of information analysis in healthcare: a review of principles and applications. J Med Econ. (2014) 17:377–83. doi: 10.3111/13696998.2014.907170
42. Garrison LP, Jackson T, Paul D, Kenston M. Value-based pricing for emerging gene therapies: the economic case for a higher cost-effectiveness threshold. J Manag Care Spec Pharm. (2019) 25:793–9. doi: 10.18553/jmcp.2019.18378
43. Epstein D, Espín J. Evaluation of new medicines in Spain and comparison with other European countries. Gaceta Sanitaria. (2020) 34:133–40. doi: 10.1016/j.gaceta.2019.02.009
44. Wang Y, Qiu T, Zhou J, Francois C, Toumi M. which criteria are considered and how are they evaluated in health technology assessments? A review of methodological guidelines used in Western and Asian countries. Appl Health Econ Health Policy. (2021) 19:281–304. doi: 10.1007/s40258-020-00634-0
45. Yuasa A, Yonemoto N, Demiya S, Foellscher C, Ikeda S. Investigation of factors considered by health technology assessment agencies in eight countries. Pharmacoecon Open. (2021) 5:57–69. doi: 10.1007/s41669-020-00235-6
46. Kristensen FB, Lampe K, Wild C, Cerbo M, Goettsch W, Becla L. The HTA core model® −10 Years of developing an international framework to share multidimensional value assessment. Value Health. (2017) 20:244–50. doi: 10.1016/j.jval.2016.12.010
47. Baltussen R, Marsh K, Thokala P, Diaby V, Castro H, Cleemput I, et al. Multicriteria decision analysis to support health technology assessment agencies: benefits, limitations, and the way forward. Value Health. (2019) 22:1283–8. doi: 10.1016/j.jval.2019.06.014
48. Kim DD, Silver MC, Kunst N, Cohen JT, Ollendorf DA, Neumann PJ. Correction to: Perspective and costing in cost-effectiveness analysis, 1974–2018. Pharmacoeconomics. (2020) 38:1377. doi: 10.1007/s40273-020-00968-6
49. Santé HAd. Choix méthodologiques pour l'évaluation économique à la HAS. (2020). Available online at: https://www.has-sante.fr/upload/docs/application/pdf/2020–07/guide_methodologique_evaluation_economique_has_2020_vf.pdf (accessed March 18, 2021).
50. Attema AE, Brouwer WBF, Claxton K. Discounting in economic evaluations. Pharmacoeconomics. (2018) 36:745–58. doi: 10.1007/s40273-018-0672-z
51. Pearson SD, Ollendorf DA, Chapman RH. New cost-effectiveness methods to determine value-based prices for potential cures: what are the options? Value Health. (2019) 22:656–60. doi: 10.1016/j.jval.2019.01.012
52. Spoors J, Miners A, Cairns J, Palnoch D, Summerfield A, McEntee J, et al. Payer and implementation challenges with advanced therapy medicinal products (ATMPs). BioDrugs. (2020) 35:1–5. doi: 10.1007/s40259-020-00457-4
53. Sara Silbert GAY, Andrew G. Shuman. How should we determine the value of caR T-cell therapy? AMA J Ethics. (2019) 21:E844–51. doi: 10.1001/amajethics.2019.844
54. Klijn SA-O, Fenwick E, Kroep S, Johannesen K, Malcolm B, Kurt M, et al. What did time tell us? A comparison and retrospective validation of different survival extrapolation methods for immuno-oncologic therapy in advanced or metastatic renal cell carcinoma. Pharmacoeconomic. (2021) 39:345–56. doi: 10.1007/s40273-020-00989-1
55. Rutherford M, Lambert PC, Sweeting MJ, Pennington R, Crowther MJ, Abrams KR, et al. NICE DSU Technical Support Document 21. Flexible Methods for Survival Analysis. (2020). Available online at: http://www.nicedsu.org.uk (accessed April 6, 2021).
56. Petrou P. Is it a Chimera? A systematic review of the economic evaluations of CAR-T cell therapy. Expert Rev Pharmacoecon Outcomes Res. (2019) 19:529–36. doi: 10.1080/14737167.2019.1651646
57. PharmaIntelligence. New Payment and Financing Models For Curative Regenerative Medicines. (2017). Available online at: https://alliancerm.org/wp-content/uploads/2018/05/ARM_Curative_Regenerative_IV1707_LRS.pdf (accessed February 22, 2021).
58. Dabbous M, Toumi M, Simoens S, Wasem J, Saal G, Wang Y, et al. Amortization of gene replacement therapies: a health policy analysis exploring funding of high-cost treatments to mitigate payer budget impact of high-cost treatments. Health Policy. (2021). 126:49–59. doi: 10.1016/j.healthpol.2021.11.005
Keywords: gene therapies, health technology assessment, economic analysis, recommendations, affordability
Citation: Qiu T, Pochopien M, Liang S, Saal G, Paterak E, Janik J and Toumi M (2022) Gene Therapy Evidence Generation and Economic Analysis: Pragmatic Considerations to Facilitate Fit-for-Purpose Health Technology Assessment. Front. Public Health 10:773629. doi: 10.3389/fpubh.2022.773629
Received: 10 September 2021; Accepted: 07 January 2022;
Published: 09 February 2022.
Edited by:
Guvenc Kockaya, ECONiX Research, Analysis and Consultancy Plc., TurkeyReviewed by:
Georgi Iskrov, Plovdiv Medical University, BulgariaCopyright © 2022 Qiu, Pochopien, Liang, Saal, Paterak, Janik and Toumi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mondher Toumi, bW9uZGhlci50b3VtaUBlbWF1ZC5ldQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.