 Ashley Pike1,2*
Ashley Pike1,2* Cynthia Mikolas2
Cynthia Mikolas2 Kathleen Tompkins1
Kathleen Tompkins1 Joanne Olson3
Joanne Olson3 David M. Olson4
David M. Olson4 Suzette Brémault-Phillips1,2
Suzette Brémault-Phillips1,2- 1Corbett Hall, Faculty of Rehabilitation Medicine, University of Alberta, Edmonton, AB, Canada
- 2Faculty of Rehabilitation Medicine, Heroes in Mind Advocacy and Research Consortium (HiMARC), University of Alberta, Edmonton, AB, Canada
- 3Edmonton Clinic Health Academy, Faculty of Nursing, University of Alberta, Edmonton, AB, Canada
- 4Faculty of Medicine, Heritage Medical Research Centre, University of Alberta, Edmonton, AB, Canada
Background: On May 3, 2016, residents of Fort McMurray Wood Buffalo, Alberta were evacuated due to an uncontrolled wildfire. The short-notice evacuation had destabilizing consequences for residents, including changes in routines, loss of control, and increased uncertainty. These consequences were especially detrimental to women who were pregnant or pre-conception during the evacuation. Pregnant and pre-conception women are particularly susceptible to a vast range of negative consequences during and post natural disasters, including elevated stress and higher incidence of pregnancy complications including gestational diabetes mellitus, pregnancy induced hypertension and C-section. The aim of this study was to understand the experiences, perceived stress and resilience of women who were pregnant during the wildfire. As well as to explore potential interventions to promote the health and enhance resilience of pregnant women and to assist in recovery after exposure to a natural disaster or other traumatic events.
Methods: A qualitative thematic analysis of 16 narratives penned by pregnant women and recounted in Ashley Tobin's compilations 93/88,000 and 159 More/ 88,000: Stories of Evacuation, Re-Entry and the In-Between was conducted.
Results: Analysis revealed five key themes: (1) experience of stress responses due to personal and external factors, (2) social connectedness and support as a facilitator of resilience, (3) performance of resilience-enhancing activities, (4) the roles of pregnancy and motherhood in the experiences of loss and resilience, and (5) the importance of home.
Conclusion: Pregnant women have unique barriers that may negatively impact them during a natural disaster or other form of stressful event. They may benefit from assistance with navigating role transition during pregnancy, training in stress management strategies, and writing interventions to build resiliency and begin the process of recovery from trauma.
Introduction
An unrelenting, unpredictable wildfire engulfed Fort McMurray Wood Buffalo (FMWB), Alberta in 2016, prompting the short-notice city-wide evacuation of approximately 88,000 people (1). Beginning on May 1, 2016, the fire remained uncontrolled until July 5, 2016, and burned nearly 570,000 hectares of land. An estimated $6 billion in commercial and personal damages resulted due to the destruction of approximately 2,400 homes and businesses (2). Residents in specific areas were able to return to their homes in June 2016, while others who lost their homes were unable to return until the spring of 2017.
The economic impact on the community was not the only destabilizing consequence residents of FMWB experienced. Residents received little warning in advance of the wide-scale evacuation, which resulted in significant disruption of routines, loss of control, and increased uncertainty, potentially increasing stress and anxiety (3). Despite the disruption, affected individuals must find a way to continue moving forward. In 2016, 55,595 babies were born in Alberta. While it is unknown how many of these women and infants were impacted by the FMWB wildfire specifically, pregnant women experiencing disasters are in a unique position, as unexpected traumas can impact their developing fetus (4).
Impacts of Disaster Exposure to Individuals
The outcomes of disaster exposure are immensely complex and may take months or years to conclude (5). Individuals exposed to disasters may experience increased observable stressors and develop subjective beliefs regarding cause and effects of the event (5). Research into impacts of natural disaster exposure consistently indicates increased disturbances in social and psychological well-being, frequently influenced by an individual's coping styles in response to stressful events (6). Women and children exposed to natural disasters experience increased stressors and a vast range of negative consequences including mental health concerns such as post-traumatic stress disorder (PTSD) (7–9).
Specific to FMWB, research by Moosavi and colleagues (10) found increased rates of probable PTSD, depression and anxiety as compared to self-reported prevalence prior to the wildfire in Fort McMurray Primary Care patients. Brown et al. (11) indicated similar increases in mental health concerns, with nearly half of student study participants meeting criteria for one or more probable diagnoses including depression, anxiety, PTSD or alcohol/substance abuse.
Natural disasters can disrupt an individual's occupational performance and ability to perform daily activities within their environment. Experiencing a natural disaster during pregnancy adds a layer of complexity. An environmental event may upset a pregnant woman's routines, roles, and occupations during a very significant and meaningful time. Additional barriers, such as limits to mobility in pregnancy, may enhance the challenges caused by an environmental event. As stress due to unexpected trauma during pregnancy can have long-term impacts that can compound across generations (4), reducing these negative consequences is of critical importance. When combined with the vulnerability of exposure to a natural disaster, the intersection between pregnancy and trauma creates a form of double jeopardization (12). As such, pregnant women who experience a natural disaster represent a vulnerable population, highlighting the importance of understanding women's experiences of pregnancy during traumatic events. Knowledge about how the women experienced stress and pregnancy throughout wildfire and evacuation can inform interventions to support women who have experienced trauma during pregnancy, as well as pregnant women who may experience a future traumatic event.
Prenatal Experience
While pregnancy and childbirth are incredibly significant, personal, and spiritual experiences (13), they cause changes in one's body, mind, relationships and routines and are associated with risks to a woman's physical, mental, and emotional well-being. Physical risks and complications include anemia, gestational diabetes mellitus, and hypertension (14). Mental health challenges can also arise. These health risks can impact the developing fetus, with the average rate of fetal deaths per 1,000 total births ranging from 7.5 to 8.1 in 2005–2014 (15). Preterm births during this same period were reported to occur in approximately 8 percent of live births, and very early births (prior to week 32) were found to make up 1.2 per 100 live births.
In addition to changes in physical appearance, women may also experience changes in their identity, roles and occupations (16), especially during their first pregnancy (17). Changes in relationships may also occur as a new understanding of self and the roles of others are developed (18). Pregnancy may facilitate greater intimacy in significant relationships or become a source of tension. Roles, occupations, and environments are important during pregnancy and are significant to understanding women's experiences of a natural disaster and their subsequent loss and grief. Pregnancy represents a transitional period (19), despite the continuation of daily routines and occupations (13). Engaging in normal routines and occupations, however, may become challenging during pregnancy and the post-partum period (19), with mobility and sleep becoming challenging. Experiencing a natural disaster during pregnancy can further alter an individual's occupational performance and their ability to perform daily activities. In addition to the changes in occupation that women experience during pregnancy, they also take on new occupations specific to pregnancy and birth, including preparing for delivery, transitioning to family expansion, and caring for the baby (19, 20).
Prenatal Maternal Stress and Child Development
Experiencing stress during pregnancy increases the risk of long-term effects to both mother and child (21–24). Research further indicates that parental trauma can be transmitted to offspring, with outcomes dependent on a complex interplay of biological, familial, and cultural systems (25). Pregnancy outcomes of women who experienced Hurricane Katrina showed a correlation between elevated stress and higher incidence of pregnancy complications including gestational diabetes mellitus, pregnancy induced hypertension and C-section (26). Stress responses such as loss of sleep or appetite, which may affect maternal health, can also be attributed to environmental events (27).
Objective prenatal maternal stress (PNMS) can affect the development of the baby in utero and have negative impacts on birth weight (24, 27). In an Australian study on birth outcomes following a bush fire, O'Donnell and Behie (22) found an increase in preterm births and babies born with low birth weight in comparison to previous years. PNMS has also been shown to impact childhood development. Research on the impacts of PNMS experienced by pregnant women during a flood was found to be negatively correlated with infant problem solving and personal-social skills at 6 months of age (23). Project Ice Storm (28), a research initiative following the Quebec ice storms of 1998, examined the long-term implications of prenatal exposure to a natural disaster on childhood development. PNMS was found to be related to decreased bilateral coordination and visual motor integration in children at five and a half years of age (21).
The impacts of maternal stress may be influenced by how the stress is perceived. Several studies have explored this relationship through examining the impacts of objective or subjective stress on both parent and child. Research by Cao et al. (21) found high maternal subjective distress was associated with greater negative impacts on motor function in children. Conversely, low subjective distress showed significant harmful effects when stress was high (21). Simcock et al. (23) found that objective maternal stress measures were more predictive of decreased problem-solving skills in infants at 6 months.
Based on research with rats, Yao et al. (4) suggested that experiencing a stressor, including exposure to natural disaster during pregnancy, may be predictive of chronic disease in later life. This study also found that prenatal stress compounded across generations and was a determinant in future maternal health (4). As stress due to unexpected trauma during pregnancy can have long-term impacts that compound across generations (4), reducing these negative consequences is of critical importance. Exposure to a natural disaster in-utero may affect infant and childhood development, create long-lasting impacts on well-being, and impact future maternal health of infant girls. Understanding the experience of coping with stress during pregnancy throughout the wildfire and evacuation can inform interventions to support women who have experienced trauma during pregnancy, as well as pregnant women who may experience a future traumatic event. These findings substantiate the importance of further research in this field.
Potential Intervention
Given the potential long-term physical and mental health outcomes trauma survivors and their offspring may encounter (25), it is imperative that potential interventions be explored. Chen et al. (6) found that elements of emotion-focused coping, including positive reframing, acceptance, and emotional support were protective factors, reducing the subjective distress for pregnant women in flood-related natural disasters. Writing interventions provide an adaptive method for navigating life transitions and coping with traumatic and stressful events and can portray features of emotion-focused coping throughout narratives (29, 30). A meta-analysis on writing therapy found writing to be an evidence-based and efficient intervention for individuals experiencing post-traumatic stress (31). Horsch et al. (32) found that an expressive writing intervention was linked with decreased symptoms of depression and PTSD in mothers of preterm infants. Writing is efficient as it is cost-effective and does not require as much therapy time as other interventions (31, 32). Studies have demonstrated that the task of writing is an effective intervention during times of stress. In a meta-analysis on writing therapies, van Emmerik et al. (31) indicated writing was an efficient and evidence-based intervention for populations experiencing post-traumatic stress, with decreased symptoms of post-traumatic stress and depression resulting. At times expressive writing is an intervention prescribed for persons experiencing times of stress and at other times, they spontaneously take up writing as a way of recording their thoughts and feelings in the moment.
Objective
This study sought to understand the experiences of women who were pregnant during or shortly following the Fort McMurray wildfire, particularly the perceived stress and resilience they experienced during the wildfire, evacuation and re-entry. This knowledge may help inform future interventions to enhance resilience, promote health, support post-traumatic growth and reduce the harmful effects of natural disasters and other traumatic stressors.
Methods
A qualitative secondary analysis of expressive writing using thematic analysis was conducted examining narratives written by 16 women who were pregnant during the 2016 FMWB wildfire. The narratives were captured in two books compiled by Ashley Tobin – 93/88,000 (33) and 159 More/ 88,000: Stories of Evacuation, Re-Entry and the In-Between (34). Convenience sampling was utilized by the author to obtain the written entries. Thematic analysis (deductive and inductive) was conducted using methods adapted by Braun and Clarke (35). Graduate-level researchers transcribed the excerpts into NVivo 12. Data was coded and themes identified. All data was coded twice to increase consistency in the process and discrepancies were resolved through discussion. Emerging themes and patterns were analyzed, consolidated and refined and supporting quotes isolated.
Results
Based on the analysis of the women's narrated experiences of pregnancy during the evacuation, five key themes emerged: (1) experience of stress responses due to personal and external factors, (2) social connectedness and support as a facilitator of resilience, (3) performance of resilience-enhancing activities, (4) the roles of pregnancy and motherhood in the experiences of loss and resilience, and (5) the importance of home. Further descriptions of themes with supporting quotes are found in Tables 1–5.
Theme 1: Experience of Stress Responses Due to Personal and External Factors
Throughout the fire and evacuation, women experienced varied stress responses during and/or following the event, including significant emotional reactions and lack of sleep.
“The fire is all around us. It's like we were watching a movie or were stuck in a nightmare. It's like our whole world is falling down on us. We can feel the heat from the fire at our house and ash is falling from the sky. We're all in shock and can't move.” [P165].
Several women also experienced pregnancy complications potentially related to heightened stress such as intrauterine growth restriction, C-section, and preterm births.
“My OBGYN finally explained to me that extreme stress can cause a baby to stop growing. There are medical terms that I researched and googled like crazy. Intrauterine growth restriction, placental insufficiency, small for gestational age.” [P228].
The women also shared stressors and fears related to the event included separation from family members or significant others; fear of losing their homes; fears of losing possessions; fears of running out of gas; waiting in traffic; and well-being of their baby. These stressors and fears often highlighted the women's values, such as connection with family, safety of their children, and protection of their homes, representing uncontrollable circumstances external to the individual.
“We headed down the one way on the wrong side of the road towards the camps. The highway was gridlocked. I can remember my husband saying, “One quick shift of the wind + were all wiped out.” Pure terror set in as we waited in traffic for 2 hours.” [P97].
Frequently, interactions between pregnancy and the environment served as an additional barrier to evacuation as women experienced difficulties including limited physical capabilities, the need for washroom facilities, or fatigue. While not atypical to pregnancy, these limitations created additional challenges for women during evacuation. Proximity to labour added additional uncertainty and stress (see Table 1).
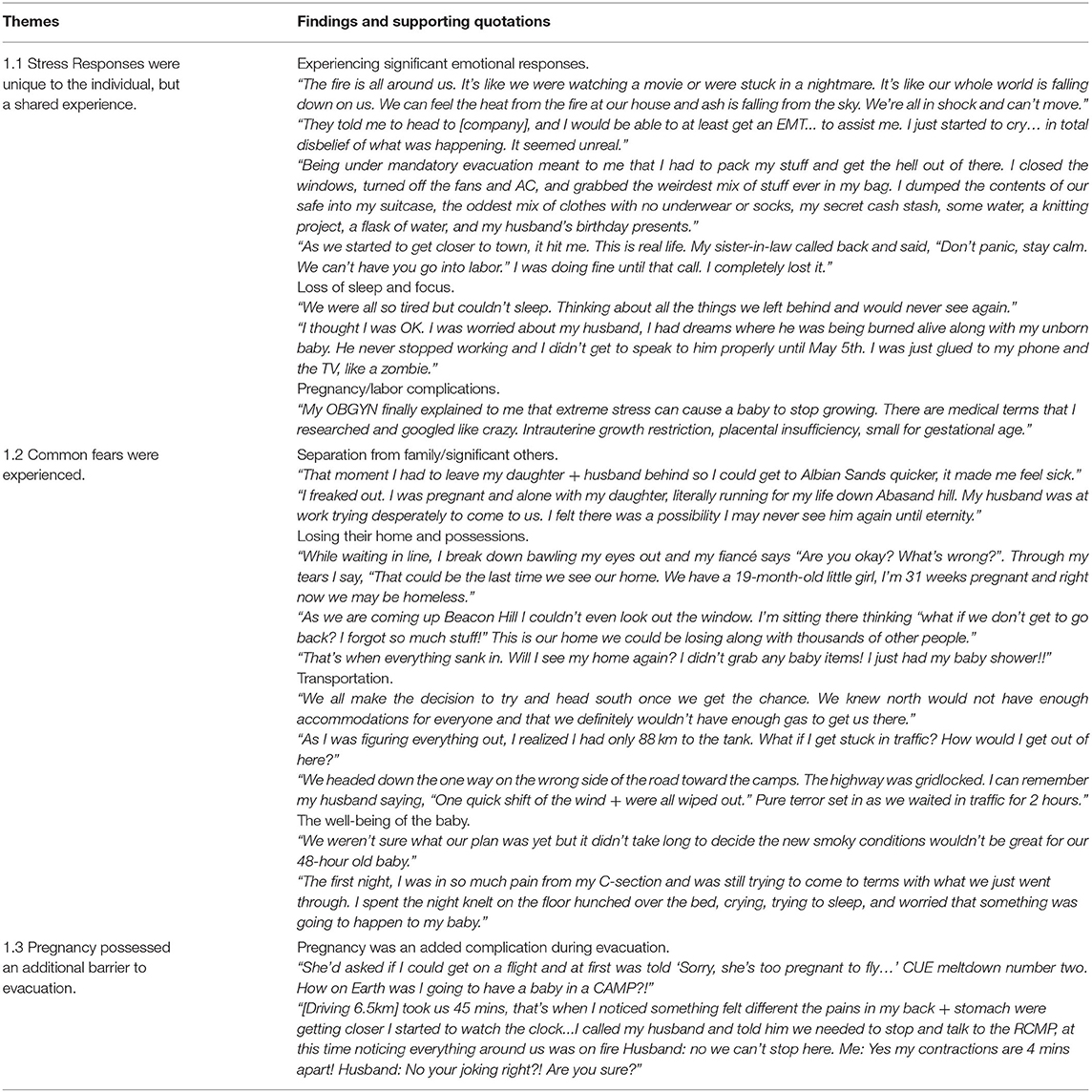
Table 1. Theme 1: Experience of stress responses due to personal and external factors.
“She'd asked if I could get on a flight and at first was told ‘Sorry, she's too pregnant to fly...' CUE meltdown number two. How on Earth was I going to have a baby in a CAMP?!” [P64].
Theme 2: Social Support Was a Facilitator of Resilience
Connection with loved ones was an important facilitator of resilience as women received support from family and significant others during and after the evacuation process, with one participant writing,
“My husband helped me through each day as I battled my emotions. He was simply amazing <3 But it's still hard.” [P81].
Writing expressed the value of relationships and togetherness with family members and spouses or partners. Whereas separation from significant others was a source of fear and stress, reunions with loved ones eased stressful emotions (see Table 2). Connection and support from the community was also an important facilitator of resilience during women's experiences of the fire and evacuation. Pregnant women received assistance from service providers and health care workers who examined and offered escorts to help women reach safety quickly. The women also were offered compassion and kindness from others, with one woman and her family being allowed into a camp after it was full. One new mother with a one-day old baby shared:
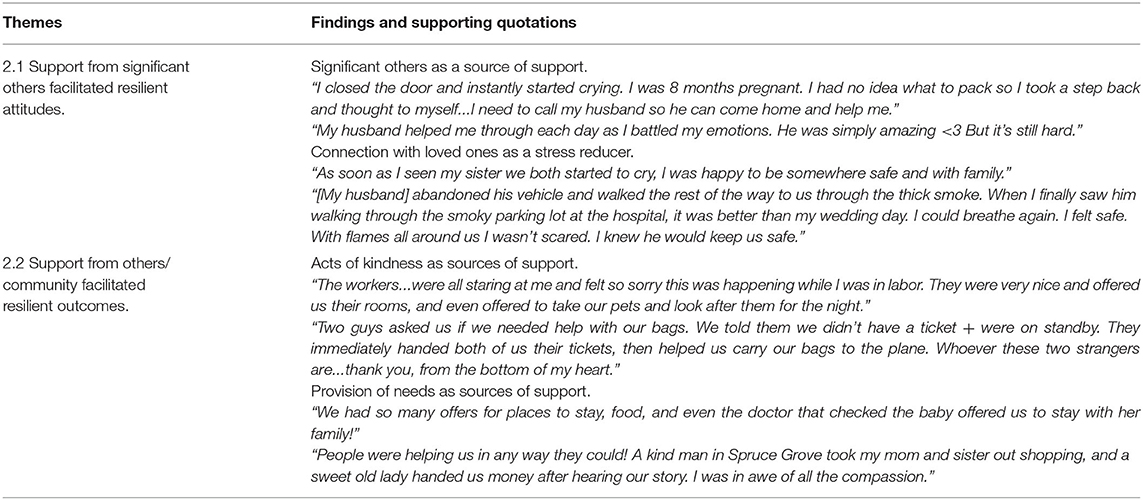
Table 2. Theme 2: Social support was a facilitator of resilience.
“Two guys asked us if we needed help with our bags. We told them we didn't have a ticket + were on standby. They immediately handed both of us their tickets, then helped us carry our bags to the plane. Whoever these two strangers are...thank you, from the bottom of my heart.” [P116].
Strangers made significant personal sacrifices from allowing participants to move in front of them in traffic or giving up flight tickets to ensure safety was reached. Women experienced generosity from others through donations and offers of places to stay. Women expressed feeling cared for and overwhelmed by the community support.
Theme 3: Performance of Resilience-Enhancing Activities
Women described engaging in resilience-supporting behaviours. Across the narratives, they commonly wrote of practicing gratitude and framing circumstances positively. Women expressed gratitude for those who assisted them during the evacuation as well as during labour and delivery. They were thankful to the first responders who fought the fire, and to the individuals who provided support after the event.
“[T]he kindness and generosity of strangers and the true efforts of our first responders will never be forgotten. There are no words to express our gratitude and love for you all.” [P165].
Women expressed gratitude for significant others and extended families who kept them grounded during the evacuation and the aftermath. Furthermore, they identified positive aspects of the experience, for example, recognizing
“Our daughter will have a crazy birth story to tell when she gets older!” [187].
Finally, the pregnant women expressed pride and solidarity with their community (see Table 3), reflecting on their pride in how the citizens of FMWB successfully navigated difficult circumstances.
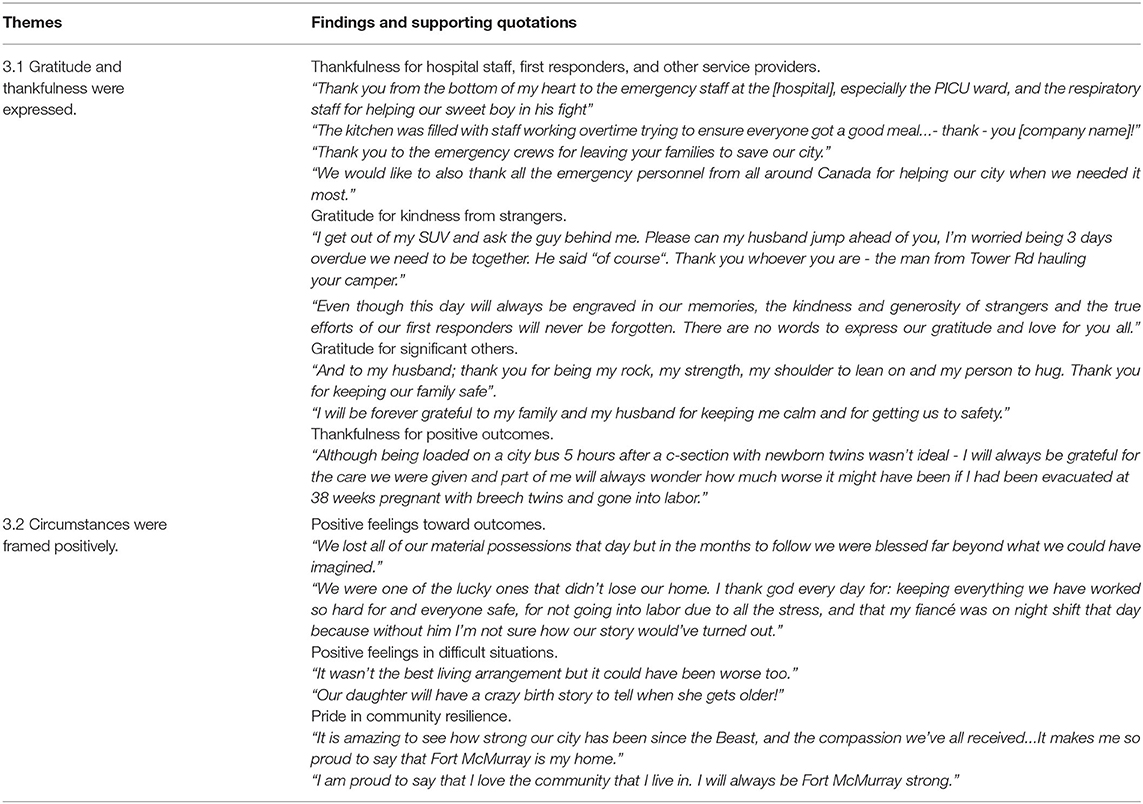
Table 3. Theme 3: Performance of resilience enhancing activities.
Theme 4: The Roles of Pregnancy and Motherhood in the Experiences of Loss and Resilience
The women identified disruption of transitional changes into new or unique roles, occupations, and interactions with the environment related to pregnancy as a result of the wildfire. Many of the women also noted that pregnancy was a time of excitement and anticipation, indicating
“I decided that morning [May 3] to start bouncing on an exercise ball cause I was anxious to meet my little man” [P67].
Others additionally noted that ordinary routines were also required, including caring for children, household tasks, and external employment. However, these roles and occupations were disrupted by the wildfire, as women expressed feelings of loss and disappointment regarding what they had hoped to experience as a mother and for their new baby.
“We decided to drive through the night South towards Saskatoon. 3 adults, 2 dogs and a 3-day-old baby all crammed into the SUV. Definitely not how I had imagined my first days postpartum.” [P107].
For new mothers, the fire and evacuation acted as a barrier to performing and savouring new mothering occupations. In addition to disappointment in expectations, the wildfire and evacuation acted as a barrier to engaging in mothering roles and occupations, which exacerbated experiences of stress, lack of control, or grief as women sought to provide for their babies' needs. The disrupted environment resulted in barriers to carrying out mothering roles and occupations during the postpartum period. A small number of women noted experiencing a miscarriage during or following the events of the fire.
“As November 21st approaches, I can't help but dwell on this day as it would have been my due date. I would trade spots in the blink of an eye to have my home burnt down if it meant I was still pregnant.” [81].
While it is unknown whether the fire was a cause of the miscarriage, these narratives express tragic losses amidst their experiences of the wildfire related to the lost life and roles. Despite the loss and grief, many of the narratives also related stories of birth, acceptance, homecoming, and demonstrated resilience. These stories bring a sense of restoration with women regaining valued roles, occupations and environments as amidst grief and loss many of the women gave birth, contrasting the horror in the fire and evacuation. Women exhibited resilience in adapting to high-stress environments while maintaining roles and routines of motherhood.
“May 5th up for 24 + hours I needed to rest, but priority #1 car seats for the kids, new baby clothes, diapers etc. we had nothing for the baby” [P252].
They emphasized the roles of provision and protection, finding creative ways to provide for their children's needs (see Table 4).
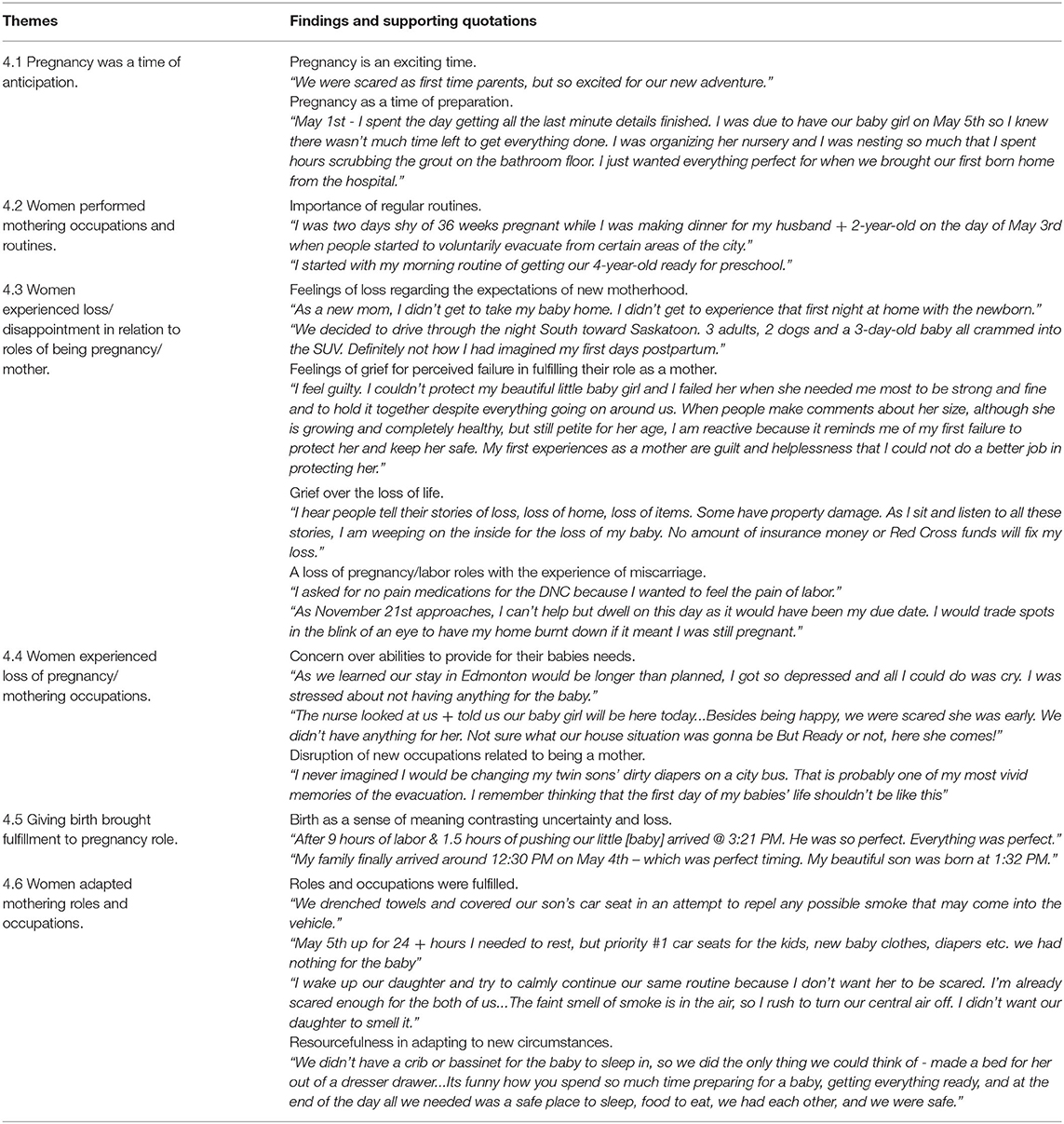
Table 4. Theme 4: The roles of pregnancy and motherhood in the experiences of loss and resilience.
Theme 5: The Importance of “Home”
The significance of home was an important theme that demonstrated how women valued and interacted with their environment, as they experienced feelings of fear and loss during the evacuation and experienced resolution in coming home and connecting the concept of home with memories. Mothers frequently narrated the loss of being able to bring their baby home from the hospital, after preparing to do so commenting
“I was so scared, confused and emotional. Our baby was less than a day old. We should be home.” [P116].
Many women experienced fear that they may not see their homes again, bringing a sense of displacement. During homecoming, women experienced strong, predominantly positive emotions, sometimes mingled with fear and anger.
“July 1st finally came and it was the best day ever! I was going home to be with my husband. The drive was quiet. The drive coming into town was full of tears. I was so happy to be home, but so sad for those who lost their homes.” [P66].
For many of the women, coming home seemed to be indicative of circumstances settling. Birth and homecoming often provided a sense of resolution to these events, restoring anticipated roles and routines (see Table 5).
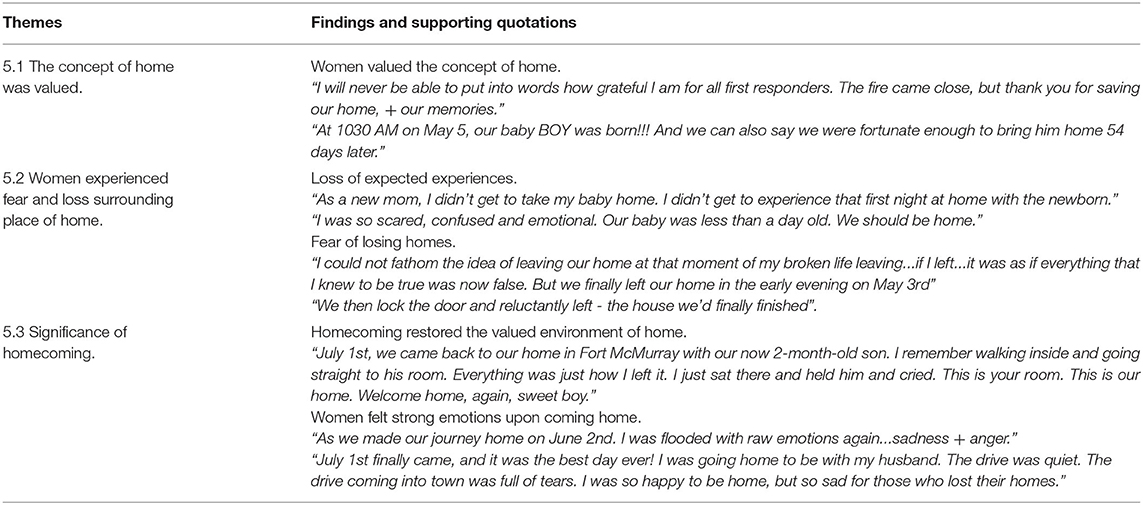
Table 5. Theme 5: Place of home was important in women's experiences.
Discussion
This study aimed to explore the experiences of women who were pregnant during or shortly following the traumatic 2016 wildfire, with a specific focus on perceived stress and resilience shown through expressive writing. Exploration of the experiences of pregnant women during and following an unexpected traumatic event may provide increased knowledge of how pregnant women experience and respond to stress. Seeking to understand factors of stress and resiliency, along with the roles and occupations important in pregnancy can inform recovery interventions and support resilience-building in prenatal populations in the future.
Factors of Stress and Resilience
Despite the added complication of pregnancy, participants displayed resilient mindsets and referenced emotion-focused coping through problem solving, gratitude, asking for and accepting help, and maintaining expected roles. Participants indicated they received immense support by others in the community. It was noted in the narratives that they believed this occurred due to their pregnancy. This finding warrants further exploration into the protective factors of community resilience, particularly in terms of prevention of long-term impacts resulting from PNMS. Connection with friends and family, emergency personnel, and supportive community members provided a buffer from elements of stress.
Roles and Occupations
The person, occupation, and environment all impact a mother's ability to participate in roles and occupations important in motherhood, with stress and self-efficacy being critical to the transition (19). Roles and occupations in pregnancy, birth, and motherhood were important themes that emerged in women's descriptions of the Fort McMurray wildfire, with women noting that the fire acted as a barrier to fulfilling mothering roles and occupations. During a natural disaster, elements within the person, occupation, and environment are subject to disruption and unpredictability, challenging a mother's role participation and occupational performance. Experiencing stress and trauma during pregnancy impact a mother's roles and occupations. As such, understanding the change or loss in roles and occupations are critical for supporting women following unexpected trauma during pregnancy.
Self-Selected Intervention
The act of writing has been shown to help individuals process traumatic events. In this study, we examined the writings that women shared about their experiences of the evacuation from Fort McMurray and re-entry into the community. While it was impossible to connect with the women who chose to contribute to the book, it is possible to infer from their written text that they used this opportunity to share their thoughts and feelings about their experiences regarding their pregnancies and they were impacted by the wildfire. Through writing, they were also able to explore both the difficult emotions and situations caused by fire and evacuation as well as hopeful and positive outcomes, providing an outlet to process their experiences. Writing may have also provided the women with an outlet to explore important roles, environments, and occupations in pregnancy and birth and to process grief.
Recommendations
Building resilience in pregnant women prior to experiencing trauma is one approach to reducing the harmful impacts of prenatal maternal stress. Prenatal education may provide an opportunity to teach expectant parents resilience strategies that can be drawn upon during a traumatic event. The FMWB wildfire created a stressful and unpredictable context in which pregnant women experienced significant stress responses. Community and familial support in transitioning roles and routines as disasters unfold is vital to ensuring pregnant women experience as minimal disruption as possible, and this support was frequently documented in the women's narratives.
Coping mechanisms including planning or asking for help were discussed in several narratives, however, physiological stress management behaviors, including breathing or grounding exercises, were rarely discussed. While lack of inclusion does not confirm that these behaviors were not accessed, increased focus on stress management methods may be beneficial during prenatal education. This recommendation supports women through changes during the perinatal period in addition to unexpected stressful or traumatic events. Tragea et al. (36) found significant decreases in perceived levels of stress following implementation of a six-week stress management program for prenatal women, indicating that such strategies may act as a protective factor against harmful effects of stress during pregnancy. An increased ability to cope with stress may help in building resilience in pregnant women. Because natural disasters and other forms of traumatic stress are often unexpected, education on stress management may be beneficial as a widespread intervention for women during the prenatal period. Given the negative effects of stress on birth and childhood outcomes, it is important to support adaptive and healthy ways of responding to stress to build resilience in mothers. Education and health promotion on adaptive coping styles may be beneficial for prenatal women who may experience stress during pregnancy.
Areas for Future Research
While the risks for women and children facing prenatal stress and trauma are well documented, more research is needed to identify effective interventions to support populations who have experienced an environmental disaster. Current research indicates PNMS impacts childhood development, demonstrating the need for research into proactive resilience-building is critical to assist pregnant mothers with managing stressors and offset potential risks to their infants. Additionally, as women who have experienced a traumatic event may face challenges due to effects of prenatal stress, such as difficulty in adapting to the role of motherhood, research in this area is of critical importance.
Limitations
There were several limitations to this research study. The data used was not collected by the research team, leaving many aspects of data collection unknown, including when women wrote the narratives following the wildfire. The data contains a small sample size, representing a small number of evacuees. Participants were self-selected, as individuals volunteered to contribute to the writing project. Furthermore, due to the anonymity, researchers were unable to seek participant feedback after analysis was completed. As a result, the findings cannot be generalized to all women who were pregnant during the Fort McMurray Wood Buffalo wildfire.
Conclusion
Experiencing a natural disaster significantly influences an individual's occupational participation and their ability to recover from the associated trauma. Pregnant women have unique barriers that may negatively impact them during a natural disaster or other forms of stressful event. Support to pregnant women could be offered through assistance with role transition and enabling mothering occupations and routines. Education on stress management and adaptive coping along with facilitating exploration and processing of traumatic experiences through writing interventions can also be used to build resiliency and aid in recovery from traumatic events.
Data Availability Statement
The datasets presented in this article are not readily available because writing excerpts used in the data analysis were taken from the books 98/88,000 and 159 more/88,000: Stories of Evacuation, Re-entry and the In-between. Requests to access the datasets should be directed to 98/88,000 and 159 more/88,000: Stories of Evacuation, Re-entry and the In-between.
Author Contributions
AP, SB-P, JO, and DO contributed to conception and design of the study. KT coded the writing excerpts and wrote the first draft of the manuscript. KT, AP, and SB-P performed the thematic analysis. AP, CM, JO, DO, and SB-P wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The research team would like to thank the women of Fort McMurray Wood Buffalo who contributed their stories to the 93/ 88,000 and 159 more / 88,000 projects and Ashley Tobin for her work in compiling these stories.
References
1. Mamuji AA, Rozdilsky JL. Wildfire as an increasingly common natural disaster facing Canada: understanding the Fort McMurray wildfire. Nat Hazards. (2019) 98:163–80. doi: 10.1007/s11069-018-3488-4
2. Insurance Bureau of Canada. Northern Alberta Wildfire Costliest Insured Natural Disaster in Canadian History. (2016). Available online at: http://www.ibc.ca/bc/resources/media-centre/mediareleases/northern-alberta-wildfire-costliest-insured-natural-disaster-in-canadian-history (accessed April 12, 2018).
3. McGee TK. Preparedness and experiences of evacuees from the 2016 Fort McMurray Horse River wildfire. Fire. (2019) 2:13. doi: 10.3390/fire2010013
4. Yao Y, Robinson AM, Zucchi FC, Robbins JC, Babenko O, Kovalchuk O, et al. Ancestral exposure to stress epigenetically programs preterm birth risk and adverse maternal and newborn outcomes. BMC Med. (2014) 12:121. doi: 10.1186/s12916-014-0121-6
5. Norris FH, Wind LH. The experience of disaster: trauma, loss, adversities, and community effects. In: Neria Y, Galea S Norris FH, editors. Mental Health and Disasters. Cambridge University Press. (2012). p. 29–44. doi: 10.1017/CBO9780511730030.003
6. Chen T, Laplante DP, Elgbeili G, Brunet A, Simcock G, Kildea S, King S. Coping during pregnancy following exposure to a natural disaster: the QF2011 Queensland Flood Study. J Affect Disord. (2020) 273:341-9. doi: 10.1016/j.jad.2020.03.165
7. Corrarino J. Disaster-related mental health needs of women and children. MCN Am J Matern Child Nurs. (2008) 33:242–8. doi: 10.1097/01.NMC.0000326079.26870.e3
8. Tang B, Deng Q, Glik D, Dong J, Zhang L. A meta-analysis of risk factors for post-traumatic stress disorder (PTSD) in adults and children after earthquakes. Int J Environ Res Public Health. (2017) 14:1537. doi: 10.3390/ijerph14121537
9. Verstraeten BSE, Elgbeili G, Hyde A, King S, Olson DM. Maternal mental health after a wildfire: effects of social support in the Fort McMurray Wood Buffalo study. Can J Psych. (2020) 66:710–8. doi: 10.1177/0706743720970859
10. Moosavi S, Nwaka B, Akinjise I, Corbett SE, Chue P, Greenshaw AJ, et al. Mental health effects in primary care patients 18 months after a major wildfire in Fort McMurray: risk increased by social demographic issues, clinical antecedents, and degree of fire exposure. Front Psych. (2019) 10:683. doi: 10.3389/fpsyt.2019.00683
11. Brown MRG, Agyapong V, Greenshaw AJ, Cribben I, Brett-MacLean P, Drolet J, et al. Significant PTSD and other mental health effects present 18 months after the Fort Mcmurray Wildfire: findings from 3,070 grades 7–12 students. Front Psychiatry. (2019) 10:623. doi: 10.3389/fpsyt.2019.00623
12. Dowd JJ, Bengston VL. Aging in minority populations: an examination of the double jeopardy hypothesis. J Gerontol. (1978) 33:427–36. doi: 10.1093/geronj/33.3.427
14. Centre for Disease Control Prevention. Data on Pregnancy Complications Reproductive Health. Available online at: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregcomplications.htm (accessed April 12, 2018).
15. Public Health Agency of Canada. Perinatal Health Indicators for Canada : A Report From the Canadian Perinatal Surveillance System. (2017). Available online at: http://publications.gc.ca/collections/collection_2018/aspc-phac/HP7-1-2017-eng.pdf (accessed April 12, 2018).
16. Laney EK, Hall MEL, Anderson TL, Willingham MM. Becoming a mother: the influence of motherhood on women's identity development. Identity. (2015) 15:126–45. doi: 10.1080/15283488.2015.1023440
17. Hennekam S. Identity transition during pregnancy: the importance of role models. Hum Rel. (2016) 69:1765–90. doi: 10.1177/0018726716631402
18. Ladge JJ, Greenberg DN. Becoming a working mother: managing identity and efficacy uncertainties during resocialization. Hum Res Manage. (2015) 54:977–98. doi: 10.1002/hrm.21651
19. Slootjes H, McKinstry C, Kenny A. Maternal role transition: why new mothers need occupational therapists. Aust OccupTher J. (2016) 63:130–3. doi: 10.1111/1440-1630.12225
20. Esdaile S., Olson J. Mothering Occupations: Challenge, Agency, and Participation. 1st ed Philadelphia, PA: FA Davis Company. (2004).
21. Cao X, Laplante DP, Brunet A, Ciampi A, King S. Prenatal maternal stress affects motor function in 51/2-year-old children: project ice storm. Wiley Online Library. (2014). p. 201717. doi: 10.1155/2014/201717
22. O'Donnell MH, Behie AM. Effects of bushfire stress on birth outcomes: a cohort study of the (2009) Victorian Black Saturday bushfires. Int J Disast Risk Reduct. (2013) 98:106. doi: 10.1016/j.ijdrr.2013.08.002
23. Simcock G, Laplante DP, Elgbeili G, Kildea S, Cobham V, Stapleton H, et al. Infant neurodevelopment is affected by prenatal maternal stress: the QF2011 Queensland flood study. Infancy. (2017) 22:282–302. doi: 10.1111/infa.12166
24. Weinstock M. The long-term behavioural consequences of prenatal stress. Neurosci Biobehav Rev. (2008) 32:1073–86. doi: 10.1016/j.neubiorev.2008.03.002
25. Danieli Y, Norris FH, Engdahl B. Multigenerational legacies of trauma: modeling the what and how of transmission. Am J Orthopsy. (2016). Available online at: http://dx.doi.org/10.1037/ort0000145. doi: 10.1037/ort0000145
26. Oni O, Harville E, Xiong X, Buekens P. Relationships among stress coping styles and pregnancy complications among women exposed to hurricane Katrina. J Obstet Gynecol Neonatal Nurs. (2015) 44:256–67. doi: 10.1111/1552-6909.12560
27. Dancause KN, Laplante DP, Oremus C, Fraser S. Brunet, A, King S. Disaster-related prenatal maternal stress influences birth outcomes: project ice storm. Early Human Dev. (2011) 87:813–20. doi: 10.1016/j.earlhumdev.2011.06.007
28. McGill University. “Project Ice Storm.” Project Verglas. (2018). Available online at: https://www.mcgill.ca/projetverglas~2018 (accessed April 12, 2018).
29. Pennebaker JW, Chung CK. Expressive writing, emotional upheavals, and health. In: Friedman HS Silver RS. Foundations of Health Psychology. Oxford: Oxford University Press (2007). p. 263–401.
30. Brémault-Phillips S, Pike A, Olson J, Severson E, Olson DM. Expressive writing for wildfire-affected pregnant women: themes of challenge and resilience. Int J Disaster Risk Reduct. (2020) 50:101730. doi: 10.1016/j.ijdrr.2020.101730
31. van Emmerik AAP, Reijntjes A, Kamphuis JH. Writing therapy for posttraumatic stress: a meta-analysis. Psychother Psychosom. (2013) 82:82–8. doi: 10.1159/000343131
32. Horsch A, Tolsa J, Gilbert L, Chêne L, Müller-Nix C, Graz M, et al. Improving maternal mental health following preterm birth using an expressive writing intervention: a randomized controlled trial. Child Psychiatry Hum Dev. (2016) 47:780–91. doi: 10.1007/s10578-015-0611-6
33. Tobin A. 93/ 88,000 stories of the evacuation, re-entry and the in-between. Fort McMurray, Alberta: Billboard Direct Promotional Services Inc. (2016).
34. Tobin A. 159 more/ 88,0000 stories of evacuation, re-entry and the in-between. Fort McMurray, Alberta. 2017. p.
35. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2008) 3:77–101. doi: 10.1191/1478088706qp063oa
Keywords: stress, resilience, pregnancy, natural disasters, factors of resilience
Citation: Pike A, Mikolas C, Tompkins K, Olson J, Olson DM and Brémault-Phillips S (2022) New Life Through Disaster: A Thematic Analysis of Women's Experiences of Pregnancy and the 2016 Fort McMurray Wildfire. Front. Public Health 10:725256. doi: 10.3389/fpubh.2022.725256
Received: 15 June 2021; Accepted: 16 March 2022;
Published: 13 May 2022.
Edited by:
Lin Zhang, Shandong University, ChinaReviewed by:
Thomas John Cova, The University of Utah, United StatesAaida Mamuji, York University, Canada
Copyright © 2022 Pike, Mikolas, Tompkins, Olson, Olson and Brémault-Phillips. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ashley Pike, YXBpa2VAdWFsYmVydGEuY2E=