
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 17 May 2022
Sec. Aging and Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.716851
This article is part of the Research Topic Falls Prevention for Older People in Primary Care Settings View all 9 articles
 Tamires Terezinha Gallo da Silva1*
Tamires Terezinha Gallo da Silva1* Jarbas Melo Filho2
Jarbas Melo Filho2 Simone Biesek1
Simone Biesek1 Audrin Said Vojciechowski1
Audrin Said Vojciechowski1 Victória Zeghbi Cochenski Borba3
Victória Zeghbi Cochenski Borba3 Anna Raquel Silveira Gomes4
Anna Raquel Silveira Gomes4Objectives: The objectives of this study were to analyze and compare musculoskeletal and functional performance and present cutoff points to differentiate pre-frail community-dwelling older women regarding their fall history: non fallers (0 falls), fallers (single fall), and recurrent fallers (≥2 falls).
Method: This is a cross-sectional, retrospective study on 90 pre-frail community-dwelling older women (71.2 ± 4.49 years) according to Fried criteria. We assessed peak torque (PT) (isokinetic dynamometer), muscle architecture/mass (ultrasound/dual-energy X-ray absorptometry), and the following functional performance: usual gait speed (UGS), fast gait speed (FGS), walking speed reserve (WSR), cadence and step length, and timed up and go.
Results: The recurrent fallers presented lower UGS (1.12 ± 0.18 vs. 1.29 ± 0.28 m/s; p = 0.05) and isometric PT of knee extensors than the fallers (89.88 ± 20.99 vs. 115.55 ± 23.09 Nm; p = 0.01), and lower FGS than the fallers (1.35 ± 0.26 vs. 1.5 ± 0.29 m/s; p = 0.03) and non-fallers (1.35 ± 0.26 vs. 1.52 ± 0.26 m/s; p = 0.01). The outcomes that differentiated the fallers from the non-fallers were both WSR calculated as a difference (WSRdiff) (≤0.26 m/s) and WSR calculated as a ratio (WSRratio) (≤1.25 m/s), while to differentiate the recurrent fallers from the non-fallers were FGS (≤1.44 m/s) and step length (≤73 cm). The following cutoff points might be used to differentiate recurrent fallers and fallers: UGS (≤1.12 m/s), FGS (≤1.34m/s), step length (≤73 cm), PT knee extension (≤114.2 Nm), PT knee flexion (≤46.3 Nm), and PT ankle dorsiflexion (≤22.1 Nm).
Conclusion: Recurrent fallers community-dwelling pre-frail older women presented a worse musculoskeletal and functional performance when compared to the non-fallers and fallers. Gait speed, step length, PT of both knee extension and flexion, and ankle dorsiflexion can be used to identify both single and recurrent fallers pre-frail older women, contributing to guide interventions and prevent falls and fractures.
Frailty represents a state of age-related physiological vulnerability, which results from the body's reduced ability to cope with adverse health situations, such as hospitalizations, falls, and functional reductions (1, 2). According to the frailty phenotype, a pre-frail older person presents one or two of the following criteria: unintentional weight loss, muscle weakness, exhaustion, low physical activity, and slowness and frail when three of them are found (3).
The prevalence of pre-frailty is significantly higher in older person, ranging from 49.3 to 65.3% (4, 5) when compared to frailty (16.2–19.6%) (4, 6, 7). Moreover, the prevalence of pre-frailty is higher in older women (56.3%) (4).
Frailty is associated with increased risk of falls even in non-fallers (8) and is considered a significant predictor of future falls among community-dwelling older people (9). In addition, frail and pre-frail older women present an increased risk of recurrent falls (OR = 2.41, 95% CI 1.93–3.01; OR = 1.23, 95% CI 1.02–1.48, respectively), hip fractures (RR = 1.7, 95% CI 1.35–2.15; RR = 1.34, 95% CI 1.12–1.6, respectively), and mortality (RR = 1.82, 95% CI 1.56–2.13; RR = 1.32, 95% CI 1.18–1.48, respectively) in comparison to non-frail older women (10). Furthermore, pre-frailty is associated with gait and balance impairments (9, 11), but it is still not established the musculoskeletal parameters, and functional performance cutoff points to differentiate pre-frail older women based on their fall history (non-fallers, 0 falls; fallers, single fall; recurrent fallers, ≥2 falls).
According to the World Health Organization (12), one-third of older people (>65 years) fall once a year and 5% sustain fracture. Older women fall more than older men and have higher prevalence of musculoskeletal diseases such as osteoporosis and faster muscle loss, they have more functional limitations and longer life expectancies (13–17). Maintaining skeletal muscle strong is critical to a healthy longevity throughout lifetime (17). These reasons bring the needed to investigate musculoskeletal and functional performance associated to fall history in pre-frail community-dwelling older women to guide interventions targeting this vulnerable underserved population.
Gait parameters such as usual gait speed (UGS), fast gait speed (FGS), step length, walking speed reserve (WSR) are able to discriminate older adults at the three levels of frailty but not regarding their fall history (18). On the other hand, it has been already reported that self-selected walking speed (SSWS) and maximal walking speed (MWS) discriminated fallers and non-fallers, but they did not assess levels of frailty and stratify by gender (19). Furthermore, tests such as Timed Up and Go (TUG), five times sit-to-stand test (FTSST) and handgrip strength (HS) have already been evaluated for their effectiveness in differentiating non-fallers from fallers (19–24). However, these studies stratified the samples into non-fallers (0 fall) and fallers (≥1 fall) (19, 21, 24) or into non-recurrent fallers (0 falls or≤1 fall) and recurrent fallers (≥2 falls) (20–23), failing not only to consider the difference between a single fall and recurrent falls but also to stratify by sex and physical frailty (25).
In addition, the studies have not investigated musculoskeletal function (muscle architecture and isokinetic peak torque), and the samples were healthy older person, not being possible to apply the cutoff points to pre-frail community-dwelling older women. Therefore, the aim of this cross-sectional study was to analyze and compare musculoskeletal function and functional performance, as well as determine cutoff points to differentiate pre-frail community-dwelling older women regarding their fall history, stratified into non-fallers (0 falls), fallers (single fall), and recurrent fallers (≥ 2 falls). The hypothesis of the study was that musculoskeletal function would be worse and enough to differentiate single from recurrent fallers pre-frail older women.
This is a cross-sectional, retrospective study developed based on the Standards for Reporting of Diagnostic Accuracy Studies (STARD) and carried out from January 2017 to December 2018. The data bank used in this study came from the research project “Effects of physical with the Nintendo Wii Fit Plus®and protein supplementation on skeletal muscle function and the risk of falls in pre-frail older women: Protocol for a randomized controlled clinical trial (WiiProtein Study),” with the previously published evaluation protocol (26). The study was approved by the Ethics Committee for research on human of the Hospital de Clínicas da Universidade Federal do Paraná, Curitiba, Paraná, beings (certificate number 58865916.8.0000.0096; approval number 1.804.775). The participants of the study signed an informed consent form according to the World Medical Association Declaration of Helsinki.
Older Women, pre-frail according to Fried et al. (3), that is, presenting one or two of the following criteria: (1) Weight loss; (2) Exhaustion; (3) Low level Physical Activity; (4) Decreased gait speed and (5) Low Grip Strength, ≥65 years old, living in the city of Curitiba and its metropolitan region, Paraná, Brazil. The sample was the participants included (n = 90) in the data bank used for the “WiiProtein study” (26). The inclusion criteria were as follows: show “moderate” kidney function [i.e., glomerular filtration rate (GFR) of 30–60 ml/min/1.73 m2] as estimated by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. If a woman presents type II diabetes, it should be compensated (<8% glycated hemoglobin), and visual acuity assessed by the Snellen card considering at least (20/70 unilateral). The exclusion criteria were as follows: acute or terminal illness, metabolic instability, or decompensated cardiovascular disease, cognitive deficits as determined by the Mini-Mental State Examination considering the following cutoff points 18/19 for illiterate and 24/25 for literate (27), neurological disorders and/or traumatic-orthopedic conditions that prevent participant from carrying out the evaluations, type I diabetes, taking medication that might affect muscle metabolism (corticoids) or postural balance (anticholinergics, antihistamines, benzodiazepines, calcium channel antagonists, or dopamine receptor antagonists) (28), an hearing loss that prevents understanding verbal instructions, and any serious deficiency described in the medical records such as cardiac, respiratory, or hepatic deficiency and/or decompensated arterial hypertension (BP ≥ 140/90 mmHg), as described in the “WiiProtein study” (26).
Sample power was calculated using the F-tests Family of the G*Power 3.1.9 program, by one-way ANOVA, considering the sample (n = 90), effect size of 0.4 (mean effect), and type I error (rate of error of 5%). Thus, the sample power (1–β) of the study was 0.92.
In our study, we consider a fall as any event resulting from a body change that makes an individual to inadvertently fall to the ground. This definition does not encompass the result of a violent blow, sudden paralysis, loss of consciousness, or epileptic seizure (24). The evaluation of fall history occurred through self-report, with the question “Did you suffer any falls in the last 12 months? If so, how many times?” The participants were also asked about the location, reasons, and consequences of the fall. According to fall history, the older women were stratified into non-fallers (NF, 0 fall), fallers (F, single fall), and recurrent fallers (RF, ≥2 falls in the last year) (25) as shown in the Figure 1. The evaluators of primary and secondary outcomes were masked about the history of falls, i.e., they did not know if a participant was a non-fallers, faller, or recurrent faller.

Figure 1. Study flow chart. FTSST, five times sit-to-stand test; HS, handgrip strength; Cc, calf circumference; AMMI, appendicular muscle mass index; DXA, dual-energy X-ray absorptiometry.
To characterize the sample and the assessment protocol for general health status, the following variables were taken into consideration through self-reports: age, education, marital status, occupation, income, ethnicity, number of medications in use, number of diseases, history of fractures, hearing acuity, sphincter control, use of orthoses, use of metallic prostheses, and history of conservative and/or surgical treatments (26), body mass, and height. Body mass index (BMI) was characterized according to the following cutoff points: underweight (BMI≤23 kg/m2), normal weight (23 > BMI <28 kg/m2), pre-obesity (28≤BMI <30 kg/m2), and obesity (BMI ≥ 30 kg/m2) (26, 29).
Pain and function of the knees and hips were assessed with the Lequesne's Algofunctional Questionnaire (30), and depressive symptoms with the Geriatric Depression Scale (GDS) 15 (31).
The DXA (Lunar Prodigy Advance PA+302284, Madison, United States) and appendicular skeletal muscle mass index (ASMMI) were used to quantify bone mineral density (BMD) following the recommendations of the International Society for Clinical Densitometry (ISCD). For the diagnosis of osteoporosis, we considered the parameters established by the World Health Organization: normal bone mass (T-score ≥-1 SD), osteopenia (T-score in between −1 and −2.49 SD), and osteoporosis (T-score≤−2.5 SD) (32).
Probable sarcopenia was identified by low handgrip strength (HS <16 kg), which, if associated with low muscle mass (ASMMI <5.5 kg/m2), confirmed the sarcopenia. In addition, if a low functional performance was detected by gait speed (GS≤0.8 m/s), it was considered as severe sarcopenia (33).
Functional mobility was assessed with the TUG performed at both usual and fast gait speed according to the protocol already described in the “Wii protein study” (26).
The 10-m walk test was conducted to assess both usual (UGS) and fast gait speed (FGS) (safely executed without running). For gait assessment, four marks were drawn on the floor (1st mark: 0 m, 2nd mark: 1 m, 3rd mark: 9 m, and 4th mark: 10 m). The test started with the participant positioned at the first mark, and, after the “go” command from evaluator 1, the participant walked for a distance of 10 m in a straight line till the 4th mark where evaluator 2 was stopped. The first and last meters were discarded because they were considered participant's acceleration and deceleration phases. The test was performed three times with the older woman walking at her usual speed (UGS) and, successively, three times at fast speed (FGS). UGS was considered as the average of the three times, divided by the distance, i.e., 8 m, to calculate the UGS and FGS in m/s (34–36).
To quantify walking speed reserve (WSR), two calculations were performed: FGS subtracted from UGS (difference) (WSRdiff), and FGS divided by UGS (ratio) (WSRratio) (19).
To assess the gait parameters (step length in cm, stride length in m, and cadence in steps/min), a treadmill (Gait Trainer 2; BIODEX®) was used. The participant was instructed to walk on the treadmill for 3 min at usual speed. Two times were taken, the first for familiarization and the second for recording the values, and there was a 2-min interval between two attempts (37).
Lower limb strength was assessed by the FTSST. The isometric and concentric isokinetic torques (60, 180°/s) of the knee extensors and flexors and ankle plantar/dorsiflexors were assessed with an isokinetic dynamometer (BIODEX®); System 4 Pro™; both protocols have already been described in the “Wii-protein study” (26).
The B-Mode ultrasound (Logiq Book XP; General Eletric®) with a linear-array probe (3.8 mm, 11 MHz) was used to assess muscle architecture, i.e., muscle thickness (MT), pennation angle (PA), and fascicle length (FL) of the vastus lateralis (50% of the distance between bone prominences of the greater trochanter and the lateral condyle of the femur) and the medial gastrocnemius (between 30 and 40% of the popliteal line and the medial malleolus). The probe was positioned perpendicular to the skin surface of both muscles and coated with water-soluble transmission gel, which provided acoustic contact without depressing the dermal surface. All images were analyzed using the Image J software (National Institutes of Health, Bethesda, Maryland). MT was defined as the mean distance between deep and superficial fascial planes, measured in five places along the ultrasound image; PA was defined as the angle of insertion of muscle fiber fascicles into the deep fascial plane; FL was defined as the length of the fascicular path between the insertions of the fascicle into the superior and deep fascial planes (38–43). When the end of the fascicle extended off the acquired ultrasound image, FL was estimated with a trigonometric function according to Abellaneda et al. (44).
Calf circumference (CC) was measured while the older women were seated, considering the greater prominence. The calculation of ASMMI (DXA) was performed by the addition of the lower limb and upper limbs value, divided by the height2 of the participant (45).
The primary and secondary outcomes are mentioned at Figure 1. For the comparison between the groups (non-fallers, fallers, and recurrent fallers), we conducted a one-way ANOVA test (parametric) and a Kruskal–Wallis (non-parametric) test with Bonferroni post-hoc; and for the categorical data a Chi-square or Fisher's exact test was conducted. To analyze the accuracy of study instruments, we calculated sensitivity (Sn), specificity (Sp), positive likelihood ratio (LR+), negative likelihood ratio (LR-), positive predictive value (PPV), and negative predictive value (NPV). Receiver operating characteristic (ROC) curves were constructed to identify the viability of the instruments (p < 0.05). Multivariate logistic regression was performed to verify the influence of variables (age, BMI, marital status, and number of diseases) on significant results of the ROC curves.
For the analyses, missing data were not considered. Thus, the number of the sample considered for each variable is described in the tables of the results. All the analyses were performed using Statistical Package for the Social Sciences (SPSS®) version 25, except for the analysis of the instrument's accuracy, which was performed using the MedCalc® program, with a significance level of p≤0.05.
The sample consisted of 90 pre-frail older women stratified into non-fallers [0 falls, n = 42 (46.7%)], fallers [single fall, n = 25 (27.8%)], and recurrent fallers (≥2 falls, n = 23 (25.6%)]. The description of the sample's clinical and sociodemographic characteristics are presented in Table 1.

Table 1. Comparison of the clinical, anthropometric, and sociodemographic characteristics and distributions of pre-frail non-fallers, fallers, and recurrent fallers older women.
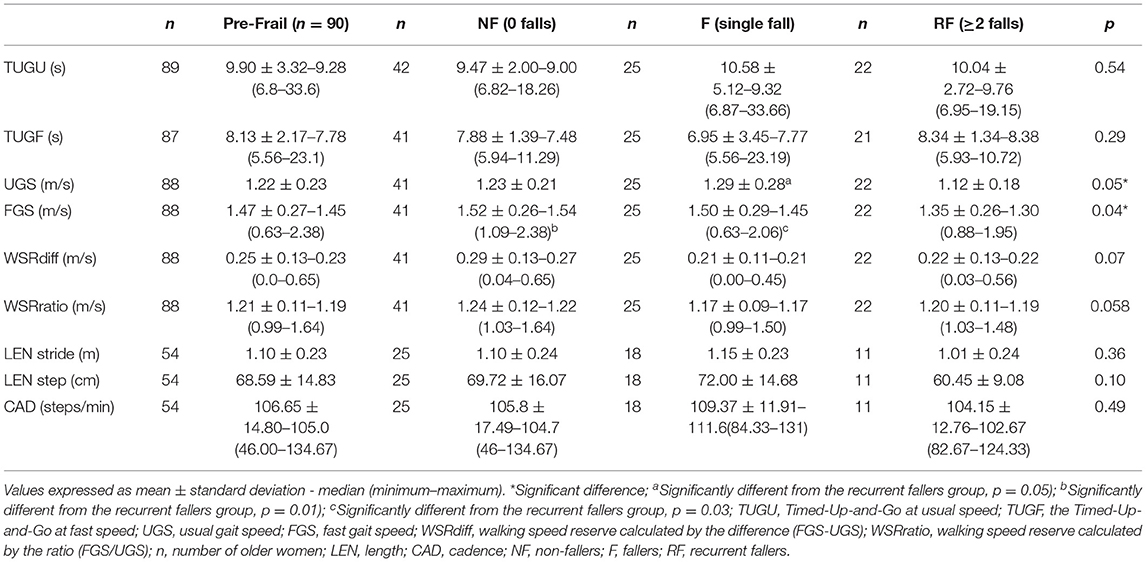
Table 2. Characterization and comparison of the functional performance of pre-frail non-fallers, fallers, and recurrent fallers older women.
Regarding the frequency of physical frailty, low HS was the most present criterion in the total sample (58.9%), among non-fallers older women (64.3%), and among recurrent fallers older women (65.2%). The most frequent criterion in the group of fallers (single fall) was exhaustion/fatigue (48.0%) (Supplementary Table 1).
The densitometric characteristics and frequencies of sarcopenia in the sample, with no difference between groups, are shown in Supplementary Table 2.
More than half [52% (n = 13)] of the single falls occurred indoors. Recurrent falls varied between locations, with 17.4% (n= 4) reported falling only indoors and 17.4% (n = 4) reported falling both indoors and outdoors such as in the backyard or outside the house in known locations. The most common cause of single falls and recurrent falls were trips [36% (n = 9) and 30.4% (n = 7), respectively], and their consequences were contusions, 40% (n = 10) in the single fallers and 60.9% (n = 14) in the recurrent fallers.
A reduction in UGS was observed in the recurrent fallers when compared to the fallers (1.12 ± 0.18 vs. 1.29 ± 0.28 m/s; p = 0.05). Similarly, a decrease in FGS was observed in the recurrent fallers when compared to the non-fallers (1.35 ± 0.26 vs. 1.52 ± 0.26 m/s; p = 0.01) and the fallers (1.35 ± 0.26 vs. 1.5 ± 0.29 m/s; p = 0.03). In addition, a decline in the isometric PT of the knee extensors was detected when the recurrent fallers were compared to the fallers (89.88 ± 20.99 vs. 115.55 ± 23.09 Nm; p = 0.01; Tables 1–3).

Table 3. Characterization and comparison of muscle force/torque in non-fallers, fallers, and recurrent fallers pre-frail older women.
The variables of muscle architecture and mass did not present statistically significant differences between the groups (Table 4).
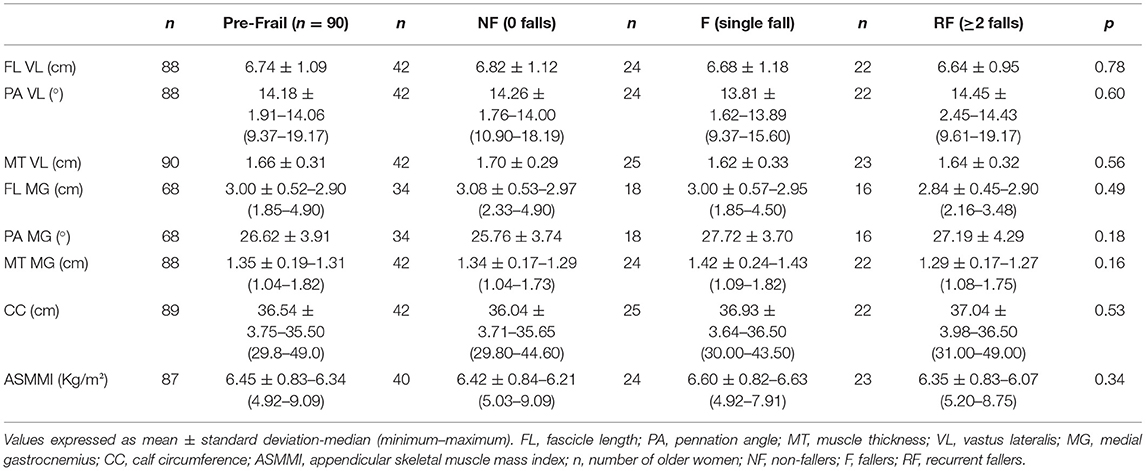
Table 4. Characterization and comparison of muscle architecture and mass in pre-frail non-fallers, fallers, and recurrent fallers older women.
The ROC analysis were run with all the variables, but we reported only variables that were significant. The ROC curves are shown in Supplementary Figure 1. The multivariate logistic regression did not show a significant difference when the covariates were considered (Table 5).
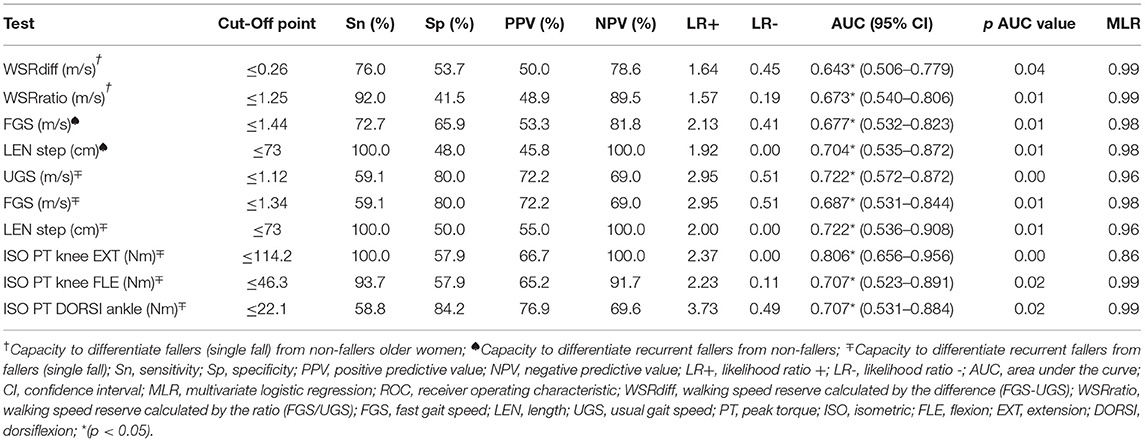
Table 5. Predictive values for fall risk and recurrent falls, areas under the curve (receiver operating characteristic, ROC) and risk statistics.
WSRdiff and WSRratio differentiated the fallers from the non-fallers. The Sn and Sp in the ROC curve indicated the cutoff point of≤0.26 m/s for WSRdiff (Sn = 76%, Sp = 53.7%), and≤1.25 m/s for WSRratio (Sn = 96%, Sp = 41.5%). The older women who had a single 239 fall in the last year presented 1.64 times (LR+=1.64) more chance to show a positive test for WSRdiff 240 and 1.57 times for WSRratio in comparison to the non-fallers (Table 5).
FGS and step length differentiated the recurrent fallers from the non-fallers. The analysis of the Sn and Sp values in the ROC curve indicated the cutoff point of≤1.44 m/s for FGS (Sn = 72.7%, Sp = 65.9%) and≤73 cm for step length (Sn = 100%, Sp = 48%). The recurrent fallers older women had 2.13 times (LR+ = 2.13) of having a positive test for WSR and 1.92 times (LR + =1.92) for step length (Table 5) in comparison to the non-fallers.
UGS, FGS, step length, and isometric PT of knee extension, isometric PT of knee flexion, and isometric PT of ankle dorsiflexion differentiated the recurrent fallers from the fallers. The Sn and Sp in the ROC curve indicated the cutoff point of≤1.12 m/s for UGS (Sn = 59.1%, Sp = 80%),≤1.34 m/s for FGS (Sn = 59.1%, Sp = 80%),≤73 cm for step length (Sn = 100%, Sp = 50.0%),≤114.2 Nm for knee extension isometric PT (Sn = 100%, Sp =5 7.9%),≤46.3 Nm for knee flexion isometric PT (Sn = 93.7%, Sp = 57.9%), and≤22.1 Nm for ankle dorsiflexion isometric PT (Sn = 58.8%, Sp = 84.2%) (Table 5).
The older women who fell 2 or more times in the last year, when compared to the single fallers, had 2.95 times (LR+= 2.95) the chance of having a positive test for UGS and FGS, 2 times (LR + = 2) for step length, 2.37 times (LR+ = 2.37) for knee extension isometric PT, 2.23 times (LR+ = 2.23) for knee flexion isometric PT, and 3.73 times (LR+ = 3.73) for ankle dorsiflexion isometric PT.
The musculoskeletal function and physical performance of the pre-frail recurrent fallers older women were worse than those of the non-fallers and single fallers. Both the gait and the torque of the lower limbs were sufficient to differentiate the pre-frail fallers from both the non-fallers and the recurrent fallers, as well as to differentiate the non-fallers from the recurrent fallers.
Pre-frail older people had smaller step lengths, larger base of support, lower single support percentage, and higher double support percentage than the non-frail ones. History of falls was correlated to lower gait speed and smaller step length in pre-frail older adults (46). In addition, pre-frail older people with slow gait speed are 10.50 times more likely to become frail (47). Our study is in line with the reported data but has filled an important gap, showing that the recurrent pre-frail fallers presented a UGS slower than that of the fallers and an FGS slower than that of the fallers and non-fallers.
Moreover, our outcomes have a significant clinical application, as pre-frailty can progress into a state of frailty or revert to a non-frail state, and recurrent fallers have more chance to fall again and present an increased risk of fractures (48). Therefore, as unaddressed risk factors for falls lead to recurrent falls and poor quality of life and recurrent falls are usually due to multiple factors, the identification of gait and musculoskeletal parameters by multidisciplinary assessments might help to tailor a multicomponent intervention to target pertinent risk factors and prevent future falls and fractures in community-dwelling pre-frail older women (49).
Most older people do not report falls to physicians unless they are injured; they are recognized as “silent fallers.” Thus, this study brings an important contribution for healthcare professionals, giving cutoffs based on an easy and validated clinical tool, gait speed, to monitor and differentiate pre-frail recurrent fallers older women from non-fallers and single fallers (47, 49).
Our results also showed that the recurrent fallers had lower knee extension isometric peak torque than the single fallers. Regarding the evaluation of community-dwelling older people, a similarity was observed in the muscle strength of knee extension and flexion (60 and 180°/s) of both the non-fallers and the fallers (≥1 fall) (50). Conversely, another study observed that fallers of both sexes had lower values of peak torque (60 and 180°/s) of both knee extensors and flexors than non-fallers (51). However, these studies (50, 51) were not conducted on pre-frail older women. Majority of falls occur during walking (52), and the greater muscle strength of knee extensors is directly involved in gait parameters, such as increased speed, cadence, and step length (53). Our findings reinforce the need of knee extensor strength training not only for single fallers but also for recurrent fallers.
WSRdiff and WSRratio accurately differentiated the fallers (single fall) from the non-fallers. The ability to increase the speed of walking on demand is indispensable for safe walking. Individuals who present difficulties under this demand are unable to respond to environmental stimuli such as crossing the street when the traffic lights start to flash (54). These findings strengthen the use of gait speed to identify the risk of falling. Nevertheless, WSRdiff and WSRratio were not yet reported in pre-frail older women. Thus, our data suggest that primary healthcare professionals not only assess gait speed but also calculate WSRdiff (≤0.26 m/s) and WSRratio (≤1.25 m/s) using the cutoff points obtained in this study to differentiate fallers from non-fallers community-dwelling pre-frail older women.
In our study, FGS and step length enabled the differentiation between both recurrent fallers from non-fallers and recurrent fallers from single fallers, corroborating a study that observed shorter step lengths in pre-frail older people compared to those who were non-frail, and a negative correlation with history of falls (46). Furthermore, our results reinforce a study that reported that SSWS and MWS should benefit fall risk assessments for older people (19). Thus, our data allow for us to recommend not only UGS but also FGS to assess fall risks, as they are easy to apply clinically, as well as step length, and they can be considered as predictors of recurrent falls in pre-frail older women.
UGS showed a good capacity (AUC = 0.722, 95% CI 0.572–0.872) in differentiating recurrent fallers from single fallers. In a study on community-dwelling older people, a cutoff point of 0.99 m/s was found for the risk of falls (≥1 fall), with Sn of 56% and Sp of 56% (24). Likewise, another study on community-dwelling older people found an AUC of 0.69 (95% CI 0.62–0.76), with a cutoff point of 0.76 m/s for the risk of falls (≥1 fall), showing a Sn of 65.4% and SP of 70.9% (19). The comparison of our study to others in the literature is limited, because they did not stratify their samples by sex and did not assess physical frailty. Moreover, our study suggests a cutoff point for the risk of recurrent falls by the assessment of UGS for older women who had already experienced a single fall in the last year, which is different from other studies that evaluated the risk of falls (≥1 fall) only in non-fallers older women (19, 24).
Therefore, our study confirmed the initial hypothesis that functional performance, assessed by gait speed, was enough to differentiate single from recurrent fallers pre-frail older women. Additionally, our outcomes are different from the previous studies because they investigated older people both genders with different clinical characteristics and history of falls, preventing to extrapolate the data for pre-frail older women (10, 19). The investigation of recurrent fallers are very relevant clinically, because they get fractured and hospitalized more frequently than single fallers or non-pre-frail people, impairing their functionality and independence and increasing costs and mortality (48, 55).
The isometric peak torques of both knee extension and flexion (AUC = 0.806, 95% CI 0.656–0.956); AUC = 0.707, 95% CI 0.523–0.891, respectively), as well as ankle dorsiflexion (AUC = 0.707, 95% CI 0.531–0.884), presented the best diagnostic accuracy (AUC) among the tests investigated in our study regarding the differentiation of recurrent fallers from single fallers older women. The study by Garcia et al. (56), with a sample composed of community-dwelling older women with low BMD, in which 44.8% of them were pre-frail, demonstrated that reduction in the PT of hamstrings (OR = 0.975, 95% CI 0.952–0.999) is associated with new falls as well as recurrent falls (OR = 0.983, 95% CI 0.967–0.999). Community-dwelling non-fallers older women have a knee flexion peak torque (21%) and an extension (14%) greater than those of fallers older women (57). In addition, other authors reported that the motor activation time of the anterior tibial muscle during ankle dorsiflexion explains 19.4% of the falls; and with the inclusion of the extension torque data, the model explained 27.8% of the falls. This means that the community-dwelling fallers older women have less capacity to produce torque and muscle recruitment in knee flexion and extension and ankle dorsiflexion (57). Therefore, assessing and training the muscle strength of the lower limbs is one of the main therapies to prevent falls (58).
We consider a strong point of our study the indication of the importance of multidimensional assessments, seeking to identify the risk factors involved in falls and their recurrence, in order to guide interventions for pre-frail community-dwelling older women. In addition, the results of our study might be used by primary healthcare professionals as a guide for the applicability of simple and low-cost clinical tests, using the cutoff points that we found, in order to avoid negative outcomes such as fractures, hospitalizations, and other comorbidities triggered by falls mainly in pre-frail older women.
The limitations of our study consist of its cross-sectional, retrospective design that does not allow to establish a cause-effect relationship; it might be suggested to conduct a prospective longitudinal study. Also, the self-reported history of falls might have a memory bias. However, this bias may have been minimized by the intentional restriction of including in the sample only community-dwelling older women without cognitive impairment. Also, there was no control group of non-frail older women. However, the main focus of our study consisted of the subgroups (non-fallers, fallers, and recurrent fallers). Therefore, our control group consisted of non-fallers older women.
FGS (≤1.44 m/s) and step length (≤73 cm) were able to differentiate recurrent fallers from both single fallers and non-fallers. Our results indicated that the assessment of gait speed enabled the differentiation between recurrent fallers and both single fallers and non-fallers, once the older women who are recurrent fallers presented a greater decline in FGS. In addition, the assessment of gait speed is simple and easy to apply even in basic health services.
Also, walking speed reserve (WSRdiff) (≤0.26 m/s) and walking speed reserve ratio (WSRratio) (≤1.25 m/s) should be considered for clinical practice even in places like primary health and domiciliary, because they do not require much space or technology to carry out and calculate.
Recurrent fallers presented lower gait speed and weaker knee extensor strength than fallers, bringing useful clinical information to target these musculoskeletal and functional factors involved in falls to develop physical programs, mainly for community-dwelling pre-frail older women.
Recurrent fallers community-dwelling pre-frail older women presented worse musculoskeletal (lower peak torque of knee extensors) and functional performance (lower UGS and FGS) than fallers. Simple tests such as WSR (FGS subtracted from UGS, WSRdiff); and its ratio (WSRratio); FGS and step length should be recommended for assessing fall status in community-dwelling pre-frail older women. WSRdiff≤0.26 and WSRratio≤1.25 m/s might be used to differentiate pre-frail older women fallers from non-fallers. FGS≤1.44 m/s and step length≤73 cm differentiated recurrent fallers from non-fallers, and FGS≤1.34 m/s and step length≤73 cm differentiated recurrent fallers from fallers. Pre-frail older women identified with scores lower than the demonstrated cutoff points may benefit from additional fall risk assessments.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee for research in human beings at the clinical hospital of the Federal University of Paraná. The patients/participants provided their written informed consent to participate in this study.
TG: conceptualization, formal analysis, investigation, writing (review and editing), and methodology. JM: software and investigation. SB and AV: conceptualization and investigation. VB: resources and methodology. AG: conceptualization, writing (review and editing) supervision, and project administration. All authors revised the article critically and approved the final version.
This study was financed partially by the Coordination for the Improvement of Higher Education Personnel-Brazil (CAPES)–(financial code 001), Conselho Nacional de Desenvolvimento Científico e Tecnológico (process number 306179/2016-4), and Pró-Reitoria de Pesquisa e Pós-graduação (PRPPG) at the Federal University of Paraná (UFPR) for the payment of the publication fee.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank Hospital de Clínicas of the Federal University of Paraná (HC-UFPR) for the physical space provided to carry out the evaluations; also thanks to both professor Dr. André L. F. Rodacki (Center for Studies on Motor Behavior) at UFPR for the authorization to use the ultrasound equipment and isokinetic dynamometer, and the Endocrinology and Metabology Service HC-UFPR (SEMPR) for the DXA equipment. The authors would like to thank the Academic Publishing Advisory Center [Centro de Assessoria de Publicação Acadêmica (CAPA): www.capa.ufpr.br] of the Federal University of Paraná (UFPR) for the assistance with English language translation and editing.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.716851/full#supplementary-material
GS, gait speed; UGS, usual gait speed; FGS, fast gait speed; PT, peak torque; WSR, walking speed reserve; Nm, Newton meter; FTSST, five times sit-to-stand test; TUG, Timed Up and Go; MMSE, Mini Mental State Examination; DXA, dual-energy X-ray absorptometry; MT, muscle thickness; PA, pennation angle; FL, fascicle length; VL, vastus lateralis; MG, medial gastrocnemius; diff, difference; Sn, sensitivity; Sp, Specificity; NF, non-fallers; F, fallers; RF, recurrent fallers; cm, centimeter.
1. Morley JE. Frailty consensus: a call to action. J Am Med Dir Assoc. (2013) 14:392–7. doi: 10.1016/j.jamda.2013.03.022
2. Lourenço RA, Moreira VG, Mello RGB, Santos IS, Lin SM, Pinto ALF, et al. Consenso brasileiro de fragilidade em idosos: conceitos, epidemiologia e instrumentos de avaliação. Geriatr Gerontol Aging. (2018) 12:121–35. doi: 10.5327/Z2447-211520181800023
3. Fried LP, Tangen CM, Walston J, Newman AB, Hirsc C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol Ser A Biol Sci Med Sci. (2001) 56:146–57. doi: 10.1093/gerona/56.3.M146
4. Siriwardhana DD, Hardoon S, Rait G, Weerasinghe MC, Walters KR. Prevalence of frailty and prefrailty among community-dwelling older adults in low-income and middle-income countries: a systematic review and meta-analysis. BMJ Open. (2018) 8:e018195. doi: 10.1136/bmjopen-2017-018195
5. Melo Filho J, Moreira B, Vojciechowski AS, Biesek S, Bento PCB, Gomes ARS. Frailty prevalence and related factors in older adults from southern Brazil: a cross-sectional observational study. Clinics. (2020) 75:1–8. doi: 10.6061/clinics/2020/e1694
6. Andrade JM, Duarte YAO, Alves LC, Andrade CD, Souza Junior PRB, Lima-Costa MF, et al. Frailty profile in Brazilian older adults: ELSI-Brazil. Rev Saude Publica. (2018) 52:17s. doi: 10.11606/s1518-8787.2018052000616
7. Da Mata FAF, Pereira PPDS, De Andrade KRC, Figueiredo ACMG, Silva MT, Pereira MG. Prevalence of frailty in Latin America and the Caribbean: a systematic review and meta-analysis. PLoS ONE. (2016) 11:e0160019. doi: 10.1371/journal.pone.0160019
8. Bartosch PS, Kristensson J, Mcguigan FE, Akesson KE. Frailty and prediction of recurrent falls over 10 years in a community cohort of 75 - year - old women. Aging Clin Exp Res. (2020) 32:2241–50. doi: 10.1007/s40520-019-01467-1
9. Kojima G. Frailty as a predictor of future falls among community-dwelling older people: a systematic review and meta-analysis. JAMDA. (2015) 9:1–7. doi: 10.1016/j.jamda.2015.06.018
10. Ensrud KE, Ewing SK, Taylor BC, Fink HA, Stone KL, Cauley JA, et al. Frailty and risk of falls, fracture, and mortality in older women: the study of osteoporotic fractures. J Gerontol Ser A Biol Sci Med Sci. (2007) 62:744–51. doi: 10.1093/gerona/62.7.744
11. Vieira E, da Silva RA, Severi MT, Barbosa AC, Amick BC, Zevallos JC, et al. Balance and gait of frail, pre-frail, and robust older hispanics. Geriatrics. (2018) 3:42. doi: 10.3390/geriatrics3030042
12. World Health Organization. Step Safely: Strategies for Preventing and Managing Falls Across the Life-Course. Geneva: WHO. (2021). p. 1–182.
13. Peel NM. Epidemiology of Falls in Older Age. Can J Aging. (2013) 30:1–10. doi: 10.1017/S071498081000070X
14. Campos ACV, Almeida MHM, Campos GV, Bogutchi TF. Prevalência de incapacidade funcional por gênero em idosos brasileiros: uma revisão sistemática com metanálise. Rev Bras Geriatr Gerontol Geriatr Gerontol. (2016) 19:545–59. doi: 10.1590/1809-98232016019.150086
15. Tosi LL, Boyan BD, Boskey A. Does sex matter in musculoskeletal health? The influence of sex and gender on musculoskeletal health. J Bone J Surg Am. (2005) 87:1631–47. doi: 10.2106/00004623-200507000-00030
16. Kontis V, Bennett JE, Mathers CD, Li G, Foreman K, Ezzati M. Future life expectancy in 35 industrialised countries: projections with a Bayesian model ensemble. Lancet. (2017) 389:1323–35. doi: 10.1016/S0140-6736(16)32381-9
17. Rosa-caldwell ME, Greene NP. Muscle metabolism and atrophy: let 's talk about sex. Biol Sex Differ. (2019) 10:1–14. doi: 10.1186/s13293-019-0257-3
18. Guedes RC, Dias RC, Pereira LSM, Silva SLA, Lustosa LP, Dias JMD. Influence of dual task and frailty on gait parameters of older community-dwelling individuals. Brazilian J Phys Ther. (2014) 18:445–52. doi: 10.1590/bjpt-rbf.2014.0034
19. Middleton A, Fulk GD, Herter T, Beets MW, Donley J, Fritz SL. Self-selected and maximal walking speeds provide greater insight into fall status than walking speed reserv among community-dwelling older adults. Am J Phys Med Rehabil. (2016) 95:475–82. doi: 10.1097/PHM.0000000000000488
20. Alexandre TS, Meira DM, Rico NC, Mizuta SK. Accuracy of timed up and go test for screening risk of falls among community-dwelling elderly. Rev Bras Fisioter. (2012) 16:381–8. doi: 10.1590/S1413-35552012005000041
21. Bongers KTJ, Schoon Y, Graauwmans MJ, Schers HJ, Melis RJ, Olde rikkert MGM. The predictive value of gait speed and maximum step length for falling in community-dwelling older persons. Age Ageing. (2015) 44:294–9. doi: 10.1093/ageing/afu151
22. Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the timed up & go test. Phys Ther. (2000) 80:142–8. doi: 10.1093/ptj/80.9.896
23. Tiedemann A, Shimada H, Sherrington C, Murray S, Lord SR. The comparative ability of eight functional mobility tests for predicting falls in community-dwelling older people. Age Ageing. (2008) 37:430–5. doi: 10.1093/ageing/afn100
24. Wang X, Ma Y, Wang J, Han P, Dong R, Kang L. Mobility and muscle strength together are more strongly correlated with falls in suburb- dwelling older Chinese. Sci Rep. (2016) 6:25420. doi: 10.1038/srep25420
25. Jeon MY, Gu MO, Yim JE. Comparison of walking, muscle strength, balance, and fear of falling between repeated fall group, one-time fall group, and nonfall group of the elderly receiving home care service. Asian Nurs Res. (2017) 11:290–6. doi: 10.1016/j.anr.2017.11.003
26. Vojciechowski AS, Biesek S, Melo Filho J, Rabito EI, Amaral MP, Gomes ARS. Effects of physical training with the Nintendo Wii Fit Plus® and protein supplementation on musculoskeletal function and the risk of falls in pre-frail older women: protocol for a randomized controlled clinical trial (the WiiProtein study). Maturitas. (2018) 111:53–60. doi: 10.1016/j.maturitas.2018.02.013
27. Lourenço RA, Veras RP. Mini-mental state examination: psychometric characteristics in elderly outpatients. Rev Saude Publica. (2006) 40:712–9. doi: 10.1590/S0034-89102006000500023
28. Hain TC, Uddin M. Pharmacological treatment of vertigo. Ther Prat. (2003) 17:85–100. doi: 10.2165/00023210-200317020-00002
29. Lebrão ML, Duarte YAO. Saúde, Bem-Estar e Envelhecimento. Projeto Sabe no Municipio de São Paulo: Uma Abordagem Inicial. São Paulo: Organização PanAmericana da Saúde (2003).
30. Marx FC, Oliveira LM, Bellini CG, Ribeiro MCC. Translation and cultural validation of the Lequesne's algofunctional questionnaire for osteoarthritis of knee and. Rev Bras Reumatol. (2006) 46:253–60. doi: 10.1590/S0482-50042006000400004
31. Almeida OP, Almeida SA. Confiabilidade da versão brasileira da escala de depressão em geriatria (gds) versão reduzida. Arq Neuropsiquiatr. (1999) 57:421–6. doi: 10.1590/S0004-282X1999000300013
32. World Health Organization. Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis: Report of a WHO Study Grou. WHO (1994) 1–129p.
33. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
34. Bohannon RW. Comfortable and maximum reference values and determinants. Age and Comfortable and maximum walking speed of adults aged 20-79 years: reference values and determinants. Age Ageing. (1997) 26:15–9. doi: 10.1093/ageing/26.1.15
35. Graham JE, Ostir GV, Fisher SR, Ottenbacher KJ. Assessing wlaking speed in clinical research: a systematic review. J Eval Clin Pr. (2008) 14:552–62. doi: 10.1111/j.1365-2753.2007.00917.x
36. Rogers ME, Rogers NL, Takeshima N, Islam MM. Methods to assess and improve the physical parameters associated with fall risk in older adults. Prev Med. (2003) 36:255–64. doi: 10.1016/S0091-7435(02)00028-2
37. Kang HG, Dingwell JB. Effects of walking speed, strength and range of motion on gait stability in healthy older adults. J Biomech. (2008) 41:2899–905. doi: 10.1016/j.jbiomech.2008.08.002
38. Alegre LM, Jiménez F, Gonzalo-Orden JM, Martín-Acero R, Aguado X. Effects of dynamic resistance training on fascicle length and isometric strength. J Sports Sci. (2006) 24:501–8. doi: 10.1080/02640410500189322
39. Baroni BM, Geremia JM, Rodrigues R, Borges MK, Jinha A, Herzog W, et al. Functional and morphological adaptations to aging in knee extensor muscles of physically active men. J Appl Biomech. (2013) 29:535–42. doi: 10.1123/jab.29.5.535
40. Blazevich AJ, Cannavan D, Coleman DR, Horne S. Influence of concentric and eccentric resistance training on architectural adaptation in human quadriceps muscles. J Appl Physiol. (2007) 103:1565–75. doi: 10.1152/japplphysiol.00578.2007
41. Narici M V., Maganaris CN, Reeves ND, Capodaglio P. Effect of aging on human muscle architecture. J Appl Physiol. (2003) 95:2229–34. doi: 10.1152/japplphysiol.00433.2003
42. Lima KMM, Oliveira LF. Confiabilidade das medidas de arquitetura do músculo vasto lateral pela ultrassonografia. Motriz Rio Claro. (2013) 19:217–23. doi: 10.1590/S1980-65742013000100022
43. Kubo K, Morimoto M, Komuro T, Tsunoda N, Kanehisa H, Fukunaga T. Age-related differences in the properties of the plantar flexor muscles and tendons. Med Sci Sports Exerc. (2007) 39:541–7. doi: 10.1249/01.mss.0000247006.24965.74
44. Abellaneda S, Guissard N, Duchateau J. The relative lengthening of the myotendinous structures in the medial gastrocnemius during passive stretching differs among individuals. J Appl Physiol. (2009) 106:169–77. doi: 10.1152/japplphysiol.90577.2008
45. Newman AB, Kupelian V, Visser M, Simonsick E, Goodpaster B, Nevitt M, et al. Sarcopenia: alternative definitions and associations with lower extremity function. J Am Geriatr Soc. (2003) 51:1602–9. doi: 10.1046/j.1532-5415.2003.51534.x
46. Freire Junior RC, Porto JM, Rodrigues NC, Brunelli RM, Braga LFP, de Abreu DCC. Spatial and temporal gait characteristics in pre-frail community-dwelling older adults. Geriatr Gerontol Int. (2016) 16:1102–8. doi: 10.1111/ggi.12594
47. Da Silva SLA, Neri AL, Ferrioli E, Lourenço RA, Dias RC. Phenotype of frailty: the influence of each item in determining frailty in community-dwelling elderly- the fibra study. Cienc Saude Coletiva. (2016) 21:3483–92. doi: 10.1590/1413-812320152111.23292015
48. Thaler HW, Sterke CS, Van Der Cammen TJM. Association of proton pump inhibitor use with recurrent falls and risk of fractures in older women: a study of medication use in older fallers. J Nutr Heal Aging. (2016) 20:77–81. doi: 10.1007/s12603-016-0679-0
49. Ang GC, Low SL, How HC. Approach to falls among the elderly in the community. Singapure Med J. (2020) 61:116–21. doi: 10.11622/smedj.2020029
50. Keskin D, Borman P, Ersöz M, Kurtaran A, Bodur H, Akyüz M. The risk factors related to falling in elderly females. Geriatr Nurs. (2008) 29:58–63. doi: 10.1016/j.gerinurse.2007.06.001
51. Antero-Jacquemin JS, Santos P, Garcia PA, Dias RC, Dias JMD. Isokinetic muscle function comparison of lower limbs among elderly fallers and non-fallers. Fisioter Pesqui. (2012) 19:39–44. doi: 10.1590/S1809-29502012000100008
52. Inoue W, Ikezoe T, Tsuboyama T, Sato I, Malinowska KB, Kawaguchi T, et al. Are there different factors affecting walking speed and gait cycle variability between men and women in community-dwelling older adults? Aging Clin Exp Res. (2016) 29:215–21. doi: 10.1007/s40520-016-0568-8
53. Callisaya ML, Blizzard L, Schmidt MD, Mcginley JL, Lord SR, Srikanth VK. A population-based study of sensorimotor factors affecting gait in older people. Age Ageing. (2009) 38:290–5. doi: 10.1093/ageing/afp017
54. Middleton A, Braun CH, Lewek MD, Fritz SL. Balance impairment limits ability to increase walking speed in individuals with chronic stroke. Disabil Rehabil. (2017) 39:497–502. doi: 10.3109/09638288.2016.1152603
55. Vu HM, Nguyen LH, Nguyen HLT, Vu GT, Nguyen CT, Hoang TN, et al. Individual and environmental factors associated with recurrent falls in elderly patients hospitalized after falls. Int J Environ Res Public Health. (2020) 17:2–10. doi: 10.3390/ijerph17072441
56. Garcia PA, Dias JMD, da Silva SLA, Dias RC. Identification of clinical and functional falls risk factors among low bone density older women. Top Geriatr Rehabil. (2016) 32:134–43. doi: 10.1097/TGR.0000000000000100
57. Crozara LF, Morcelli MH, Marques NR, Hallal CZ, Spinoso DH, Almeida Neto AF, et al. Motor readiness and joint torque production in lower limbs of older women fallers and non-fallers. J Electromyogr Kinesiol. (2013) 23:1131–8. doi: 10.1016/j.jelekin.2013.04.016
Keywords: frail elderly (MeSH), accidental falls (MeSH), musculoskeletal system (MeSH), muscle strength (MeSH), gait (MeSH), sensitivity and specificity (MeSH)
Citation: Gallo da Silva TT, Melo Filho J, Biesek S, Vojciechowski AS, Borba VZC and Gomes ARS (2022) Accuracy of Tools to Differentiate Single From Recurrent Fallers Pre-Frail Older Women. Front. Public Health 10:716851. doi: 10.3389/fpubh.2022.716851
Received: 29 May 2021; Accepted: 13 April 2022;
Published: 17 May 2022.
Edited by:
Mariana Arias Avila, Federal University of São Carlos, BrazilReviewed by:
Claudia Meyer, RDNS Institute, AustraliaCopyright © 2022 Gallo da Silva, Melo Filho, Biesek, Vojciechowski, Borba and Gomes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tamires Terezinha Gallo da Silva, dGFtaXJlcy5nYWxsb0B1ZnByLmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.