 Maria Emilia Gadelha Serra1
Maria Emilia Gadelha Serra1 José Baeza-Noci2
José Baeza-Noci2 Carmen Verônica Mendes Abdala3Marilia Moura Luvisotto1Charise Dallazem Bertol1
Carmen Verônica Mendes Abdala3Marilia Moura Luvisotto1Charise Dallazem Bertol1 Ana Paula Anzolin1*
Ana Paula Anzolin1*- 1Brazilian Society of Medical Ozone Therapy (SOBOM), São Paulo, Brazil
- 2World Federation of Ozone Therapy (WFOT), Brescia, Italy
- 3Latin American and Caribbean Center on Health Sciences (BIREME/OPAS/OMS), São Paulo, Brazil
Introduction: The Brazil has one of the largest public health systems in the world and in the 1980's, Traditional, Complementary and Integrative Medicine were introduced. In 2018, the treatment with ozone became a complementary integrative practice showing several benefits. However, its effectiveness needs to be researched. The objective of this evidence gap map is to describe contributions of Integrative Medicines-Ozone treatment in different clinical conditions, to promote evidence-based practice.
Methods: We applied the methodology developed by Latin American and Caribbean Center on Health Sciences Information based on the 3iE evidence gap map. The EMBASE, PubMed and Virtual Health Library databases, using the MeSH and DeCS terms for the treatment with Ozone were used.
Results: 26 systematic reviews were characterized, distributed in a matrix containing 6 interventions (parenteral oxygen/ozone gas mixture; parenteral ozonated water; systemic routes; topical application ozonated water; topical oxygen/ozone gas mixture; and topical ozonated oil) and 55 outcomes (cancer, infection, inflammation, pain, quality of life, wound healing and adverse effects). 334 associations between intervention and outcome were observed, emphasizing the parenteral oxygen/ozone gas mixture intervention (192 associations, 57%).
Conclusions: The evidence gap map presents an overview of contributions of Ozone treatment in controlling pain, infections, inflammation and wound healing, as well as increasing the quality of life, and it is directed to researchers and health professionals specialized in Ozone treatment. No serious adverse effects were related. Therefore, this treatment may be even more widely known as an integrative treatment, considering its low cost, efficiency and safety. Future studies should adopt economic impact assessments and the organization of health services.
1. Introduction
The Brazilian Unified Health System (SUS) is one of the largest public health systems in the world. It covers most outpatient and inpatient care in the country, which currently has a population of over 190 million (1).
Since 1980 the experiences of Traditional, Complementary and Integrative Medicine (TCI) were included in the SUS in Brazil. In 2006, with the enactment of the National Policy on Integrative and Complementary Practices (PNPIC), the TCI gained visibility. In 2018, the PNPIC made official 25 other practices: art therapy, Ayurveda, biodance, circle dance, meditation, music therapy, naturopathy, osteopathy, chiropractic, reflex therapy, Reiki, shantala, integrative community therapy, yoga, apitherapy, aromatherapy, bioenergetics, family constellation, manual therapy, floral therapy and Ozone Therapy (2, 3).
Ozone is an oxygen triatome with high oxididant power. Ozone has been used for several purposes, including the treatment with Ozone, which is the therapeutic administration of medicinal ozone for the treatment of various diseases (4). This treatment is currently available and recognized as a medical procedure in many countries such as Germany, Italy, Russia, Portugal, Spain, Turkey, Greece, Egypt, China, Cuba, Mexico, Honduras and several Eastern European countries (4).
The treatment with ozone can be administered by different routes according to the targeted therapeutic purpose, considering a safety and efficacy “therapeutic window” that ranges from concentrations of 1μg/mL up to 100 μg/mL (5). This treatment has been used as an alternative for the treatment of osteoarthrosis (OA) (6, 7), wound healing (8–10) and low back pain (11, 12). However, the results of existing analyzes on the effectiveness and adverse events of ozone deserves to be better explored, bringing security to the user and prescriber of the treatment with ozone.
Evidence and Gaps Maps (EGMs) are an innovative quick review method that involves a systematic search on a topic of interest, identifying scientific evidence, trends, gaps in the knowledge and needs of future research (13). EGMs allow descriptive and visual analysis of the database, such as bubble graphs, to identify research gaps, to support evidence-based policy and to provide resources in clinical decision-making. Therefore, evidence maps, unlike other synthesis methods, use graphical representations (or dynamic representations, through interactive online databases), which facilitate the interpretation of results (14–16).
The World Health Organization (WHO) has encouraging and strengthening the insertion, recognition and use of integrative medicine. In this way, the Brazilian Society of Medical Ozone Therapy (SOBOM), World Federation of Ozone Therapy (WFOT) and the Latin-American and Caribbean Center on Health Sciences Information (BIREME/PAHO/WHO) have joined efforts to recruit volunteer researchers from world, to systematize the available scientific evidence. The objective of this EGMs is to describe contributions of Integrative Medicines-Ozone treatment in different clinical conditions, to promote evidence-based practice.
2. Methods
This EGMs summarizes interventions and health outcomes related to the effects the treatment with Ozone applied in different clinical conditions. We report the method and results according to PRISMA guidelines and the International Initiative for Impact Evaluation (3iE) Evidence Gap Methodology (13, 17). This EGMs was supported by a technical expert panel of librarians, practitioners, policy maker and researcher content experts.
2.1. Data sources
We searched PUBMED and EMBASE and Virtual Health Library (BVS) from 2006 to April 2022. BVS is a decentralized and dynamic collection of information sources on health. BVS is maintained by BIREME, a PAHO Specialized Center. This collection includes databases such as LILACS, MEDLINE, Cochrane Library and SciELO. We consulted topic experts and developed the search strategy together with BIREME.
A search strategy was developed, using the MeSH and DeCS terms ozonioterapia, ozonetherapy, Ozone Therapy and medical ozone.
The terms used in the search strategy were reviewed by treatment with ozone experts and researchers, and by librarians.
2.2. Inclusion criteria
Systematic Review (SR) were selected from randomized and non-randomized clinical trials, observational studies, in any language or publication date (2006–2022) considering the clinical application of OT, in Supplementary File Appendix S1.
2.3. Exclusion criteria
Primary non-review studies that did not include treatment with ozone as a clinical medical option, treatment with ozone applied in dentistry, methodological flaw and one study in mandarin were excluded, as shown in Supplementary File Appendix S2.
2.4. Risk of bias and data extraction
All reviews meeting the inclusion criteria were imported to an software Rayyan. After duplicates were removed, titles and abstracts were assessed for eligibility prior to full text review. Reviews fulfilling the inclusion criteria through full text review were then assessed for their quality. Quality was assessed using Assessment of Multiple Systematic Reviews (AMSTAR) checklist scores. The checklist contains 11 indicators that are used to derive an overall score assessed as high quality (score ≥ 8), medium quality (score 4–7), and low quality (score ≤ 3). Two reviewers (MEGS and APA) independently assessed the quality of each review.
Applying the AMSTAR tool, the SR were classified as: 1- green dot - high level of confidence, 2- yellow dot - moderate level of confidence and 3- red dot - low level of confidence and the according to the number of scientific studies, the dots received different sizes, distributed in each correspondent Outcome vs. Routes of administration. Bigger dots were related to 3 or more studies, medium dots were related to 2 studies and small dots had only 1 study.
2.5. Data synthesis
From each included study, we extracted the routes of administration (e.g., rectal insufflation, bag, ozonized oil, Minor Autohemotherapy) (Table 1) and the main health outcomes (e.g., inflammation, infection, pain, quality of life, side events, cancer, wound healing) that were summarized across included studies. Researchers and health professionals capacitated in the use of treatment with ozone in the management of outcomes and symptoms, especially in the dimension of disease and side events analyzed the data.
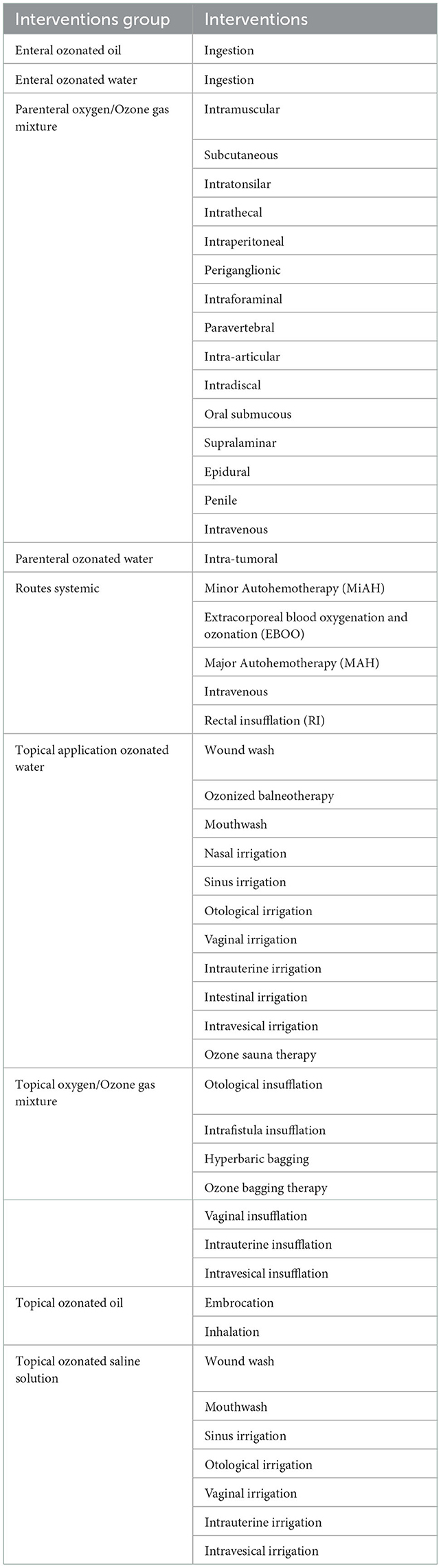
Table 1. Routes of administration of the oxygen-ozone gas mixture.
We developed a characterization matrix to synthesize the findings. This matrix included: Full Text Citation; Interventions; Outcomes Group; Outcomes; Effect; Population; Database ID; Focus Country; Publication Country; Publication Year; Study Design. The search and analysis of documents was performed in April 2022.
3. Results
Until April 4th, 2022, the bibliographic search on treatment with ozone with application of the “SR” resulted in 559 records at databases (Pubmed, BVS and Embase). After excluding duplicates and analyzing the titles, abstracts and full texts, 26 studies (qualitative analysis) were included in the treatment with ozone EGMs (Figure 1).
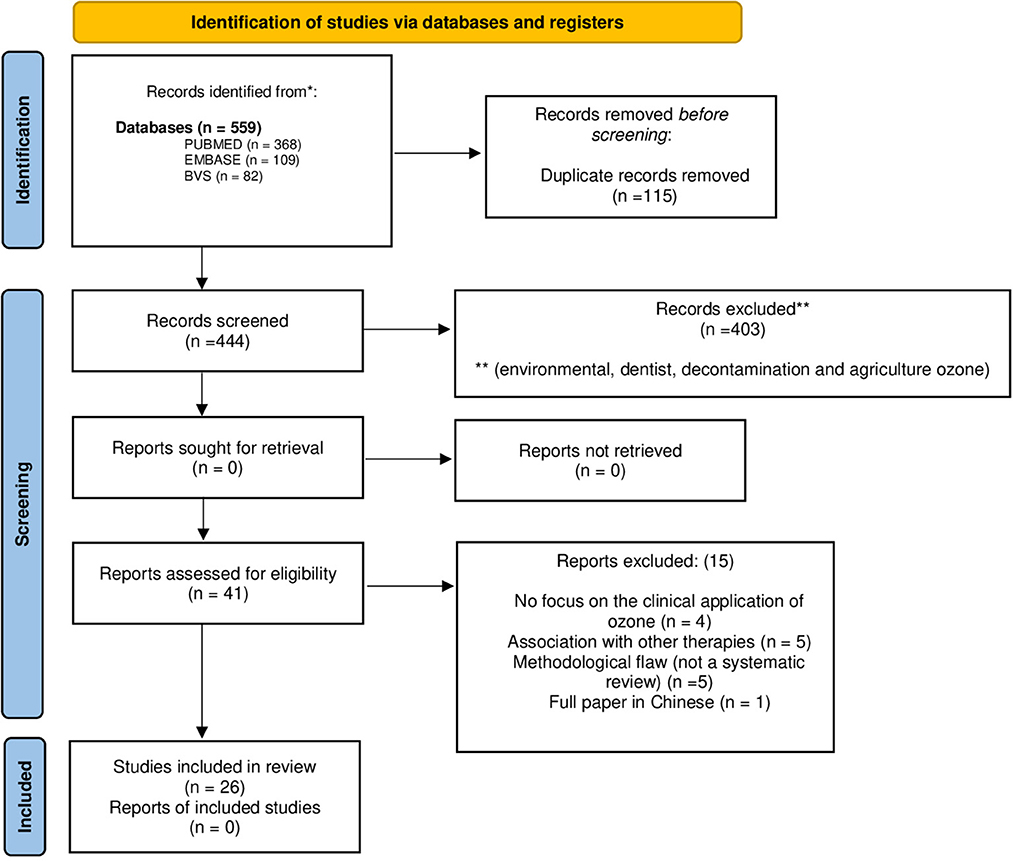
Figure 1. Ozone treatment literature flow according PRISMA flow diagram.
3.1. Study design
The 26 SR included were: 18 SR, 1 SR with meta-analysis, 3 SR of randomized controlled trials, 3 meta-analyses, and 1 scoping review. Studies included were designed as with the majority being randomized clinical trials (16). Another 8 reviews are from observational clinical studies, and another 2 reviews are from non-randomized clinical trials.
The SR used in our work were performed Spain (2006 and 2019), USA (2009, 2019 and two in 2021), Brazil (2012, two in 2013, 2018 and 2019), China (2015), Iran (2018 and 2020), Australia (2018), Portugal (two in 2018), Mexico (2019), Switzerland (2021), England (2018, 2019 and 2021), The United Kingdom (2018, 2021 and 2022) and Italy (2021).
The primary studies included in SR are concentrated in European and Asian countries, other studies are from the United States, Brazil and Cuba. Five SR did not inform the countries of the primary studies.
3.2. AMSTAR evidence level
The AMSTAR tool showed that of the 26 SR analyzed, 9 high-level reviews, 3 moderate-level reviews, 11 low-level reviews and 3 low-critical reviews. The majority of the evidence proved the efficacy of treatment with ozone applied to reduce pain (42 associations), low back pain (18) and improvement in physical function (19) stand out (Table 2).

Table 2. List of 26 systematic reviews related to ozone therapy, considering country of origin, level of confidence according to AMSTAR and database where it was published.
3.3. Outcomes and effects
Reviews evaluated the effect of some Ozone interventions: parenteral oxygen/ozone gas mixture; parenteral ozonated water; systemic routes; topical application ozonated water; topical oxygen/ozone gas mixture; and topical ozonated oil. We found a higher number of evidences in the parenteral application of the oxygen-ozone gas mixture, followed by local and topical application.
The interventions were associated with 55 health outcomes divided into 7 groups: cancer, infection, inflammation, pain, quality of life, wound healing and adverse effects.
In total, there were 334 associations between intervention and outcome, with emphasis on the interventions of the parenteral mixture oxygen/ozone gas (192 associations, 57%).
A positive [154] or potentially positive (23) effects were reported in the interventions/outcomes. Inconclusive effect was reported for 132 associations and no effect was reported for 8 associations. The effects of treatment with ozone were: 14 positive, 5 potential positive, 5 inconclusive and 2 no effect.
The Figure 2 provides a broad visual view of the evidence base of treatment with ozone. The bubble chart describes the estimated volume of research based on the number of treatment with ozone SR included in the largest review, summarizing the routes of administration and the outcomes related to inflammation, pain, wound healing, quality of life and adverse events. The Table 3 show the other information related to SR as the total number of patients, the population studied, the methodology and the results of treatment with ozone in evidence-based medicine.
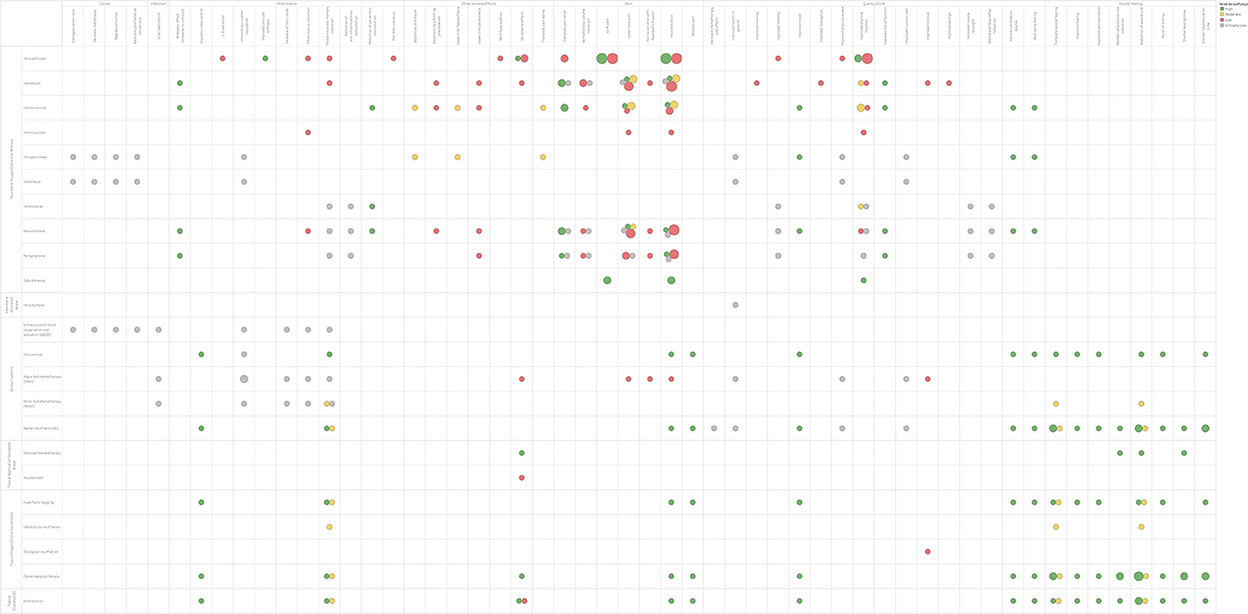
Figure 2. Ozone treatment Evidence and Gaps Map.

Table 3. Compilation of information related to the final 26 SR include reference, country, sample number, population studied, methodology and results/conclusions.
3.4. Cancer
For cancer a single review was included (41). Intratumoral ozone was administered monthly through a catheter (5 mL of oxygen-ozone gas at a concentration of 40 μg ozone per mL of oxygen - a total dose of 200 μg each time), along with the standard chemotherapy protocol, with a median of 27 oxygen-ozone applications. Two side effects were reported; one catheter was temporarily removed because of an infection and in another patient the catheter was removed because of hemorrhage.
The observed outcomes were: regression of the tumor; decrease of the metastases and of the proliferation of cancer cells; and damage to cancer cells.
Its effect was inconclusive, and the AMSTAR level was critically low, so further studies are needed to analyze this outcome.
3.5. Wound healing
This category included results from four reviews (18–21) that used the route of administration: rectal insufflation, bag, ozonized oil, Minor Autohemotherapy, topical ozonized blood and washing with ozonized water. This group was the second most evident, 61.18%, with the healing outcome being the most cited. The reviews analyzed, 2 had a positive effect (19, 21) and 2 inconclusive (18, 20). For the AMSTAR level of the reviews evaluated, three were rated high (18–20) and one moderate (21).
The observed outcomes were: complete wound healing; improved vascularization; improved of ischemia and reperfusion; relief of itching; cutaneous/subcutaneous infection reduction; reduction of scar adhesions; shorter healing time; shorter hospitalization time; bleeding reduction; erythema reduction; reduction in the number of hospitalization; member amputation risk reduction; reduction of wound size; shorter healing time; shorter hospitalization time; improved feeling.
The treatment with ozone improves wound healing and treatment time but does not seem to be superior to conventional treatments, but in chronic treatments, it can lead to healing in a shorter time, however additional studies are needed. The main evidences observed were: decrease in the size of injuries and pain; complete wound closure; improved capillary blood glucose; shorter hospital stay and reduction of oxidative stress markers. No adverse events associated with treatment the ozone were reported.
3.6. Infection
A single review was included (40). The systemic route was used to analyze the effect of treatment with ozone in patients with COVID-19. Its effect was inconclusive and the AMSTAR level was critically low, so further studies are needed to analyze this outcome.
The observed outcomes were: viral load control; sepse prevention; bacterial colony reduction; hepatic enzyme reduction; antibiotics usage time reduction.
Five studies were included in the review (40) and it was concluded that the potential role of systemic treatment with ozone is effective in controlling COVID-19 because of its antiviral, oxygenating, anti-inflammatory, oxidation-balancing, and immunomodulatory effects. However, there is not sufficient evidence to endorse the efficacy of treatment with ozone on novel coronavirus disease.
3.7. Inflammation
This category included results from eleven reviews (18, 21, 28, 31, 35–37, 39–42). For the outcome inflammation four routes of administration were used: topical oxygen-ozone gaseous mixture, topical ozonated oil, parenteral oxygen-ozone gaseous mixture and systemic. The reviews analyzed, 5 had a positive effect (21, 35–37, 42), 2 potentially positive (28, 39), 3 inconclusive (18, 40, 41) and 1 no effect (31), concluding therefore that treatment with ozone can be effective for the reduction of inflammation. For the AMSTAR level of the eleven reviews evaluated, four were rated high (18, 31, 36, 42) and three critically low (35, 40, 41).
The observed outcomes were: increase of nitric oxide; glycemic index control; Nrf2 induction; improved articular stiffness; inflammation reduction; reduction of painkillers consumption; reduction of anti-inflammatories consumption; edema reduction; fever reduction; IL-6 reduction; oxidative stress markers reduction; NFKb reduction; TNF-Alfa reduction; immunologic system regulation; analgesic effect compared to corticoid.
The pathologies that most benefited from the reduction of inflammation with treatment the ozone were OA (28, 31, 36), wounds (18, 21) and herniated disc/low back pain (35, 37, 42). The decrease in inflammation also occurred in the reviews of tinnitus (39), COVID-19 (40) and cancer (41), but with less effectiveness.
3.8. Pain
This category included results from nineteen reviews (12, 18, 23–38, 42). Most of the available evidence focused on the use of ozone for pain reduction, with 103.31% being evidenced and the highlighted outcomes were: pain reduction (42 associations), low back pain (18) and improvement in physical function (19).
The observed outcomes were: complete pain relief; headache; joint pain; wounds pain; lower back pain; muscle pain; neuropathic pain; pain reduction; herniated disc volume reduction; pain associated with raynaud's disease.
The reviews showed pain reduction for herniated disc/low back pain (7 reviews) and OA (9 reviews). Of the reviews analyzed, 11 had a positive effect (12, 23, 24, 26, 27, 34–38, 42), 4 potentially positive (25, 28, 29, 36), 2 inconclusive (18, 32) and 2 no effect (30, 31), concluding therefore that treatment with ozone can be effective for the reduction of rem disc hernia/low back pain and also OA. Of the nineteen reviews evaluated, seven SR were classified with a high (18, 23, 25, 26, 31, 36, 42) AMSTAR level and only one critically low (35) certifying this outcome.
In the most recent review (2021) (37) it was observed that percutaneous oxygen-ozone injection is a minimally invasive, cost-effective, repeatable and highly available procedure for the treatment of lumbar disc herniation-related low back pain when poorly responsive to conservative treatments. Furthermore, imaging-guided procedures showed a better therapeutic performance with higher impact on pain reduction and lower age-related variability.
3.9. Quality of life
This category included results from sixteen reviews (12, 18, 24, 27–31, 34–36, 38, 39, 41, 42). The second highest available evidence focused on the use of treatment with ozone for improve the quality of life, with 78.23% evidenced. Improved quality of life was observed in reviews of OA, herniated discs/low back pain, wounds, tinnitus and cancer. The most frequent administration routes were parenteral and systemic oxygen-ozone gaseous mixture.
The observed outcomes were: increased muscle strength; improved physical function; improved social function; improved mobility; improved health in general; improved vitality; improved physical aspect; improved mood; fatigue reduction; osteotendinous reflex reduction; wellbeing feeling; patient satisfaction degree; improved vertigo; improved tinnitus; improved nystagmus; improved hearing; decrease chemotherapy side effects; improved survival rate.
Of the analyzed reviews, nine had a positive effect (12, 24, 27, 34–36, 38, 42), three potentially positive (28, 29, 39), two inconclusive (18, 41) and two no effect (30, 31), concluding that treatment with ozone can be improve quality of life. In the AMSTAR level, it was seen that of the sixteen reviews evaluated, five were classified as high (18, 31, 34, 36, 42) AMSTAR, two moderate (12, 34), seven low (24, 27–30, 38, 39) and two critically low (35, 41). We believe that this result is due to the fact that this outcome is very subjective. Further studies that assess the quality of life of patients using validated scales should be performed.
3.10. Adverse effects
This category included results from ten reviews (12, 19, 22, 27–29, 31, 33, 38, 39) that only observed mild adverse effects in four studies (12, 29, 33, 38), such as: abdominal distension, lower limb hypoesthesia, lower limb paresthesia, transient worsening of pain, mild exacerbation reaction and fainting sensation. In the other 6 review no adverse effects were observed.
The reviews analyzed, 5 had a positive effect (12, 19, 22, 27, 38), 4 potentially positive (28, 29, 33, 39) and 1 no effect (31), concluding that treatment with ozone can be safe. However, in the AMSTAR level, it was seen that of the ten reviews evaluated, two were classified as high (19, 31) AMSTAR, one moderate (12) and seven low (22, 27–29, 33, 38, 39). More studies should be carried out, as well as the creation of protocols for the correct execution of the technique.
The only route of administration that demonstrated these adverse effects was the parenteral oxygen-ozone gaseous mixture. The works reported adverse events of transient paresthesia and secondary infection, probably due to an inadequate asepsis procedure. Treatment with ozone can be considered an option to treat low back pain related to herniated lumbar disc that did not respond to conservative treatment, representing an alternative to surgery. However, future studies are needed to demonstrate whether the effects of treatment with ozone persist over time.
The review (22) included nine studies. Two studies specifically evaluated the cytotoxicity of ozonated liquids on human cells, five studies evaluated ozonated liquids in randomized controlled trials, one was a post-market surveillance study, and one was a crossover study in humans. None of the included studies found significant human dermatological risks associated with ozonated liquid.
4. Discussion
This treatment with ozone EGMs is based on 26 studies and provides a broad overview of available evidence of complementary therapies in reduction of pain, lower back pain and improvement of physical function, healing, reduction of inflammation and infection. It shows the volume of available research and highlights areas where the interventions showed potential positive and positive effects.
In Brazil, the Federal Council of Dentistry (CFO) recognized treatment with ozone as a dental procedure in all areas of modern dentistry through CFO Resolution no. 166/2015. On October 18, 2017, the Federal Senate unanimously approved Bill No. 227, which authorizes the prescription of treatment with ozone throughout the national territory. This federal bill is currently being processed in the Chamber of Deputies under no. 9001/2017. During the 1st International Congress of Integrative Practices and Public Health (INTERCONGREPICS), the Ministry of Health of Brazil recognized and included treatment with ozone as an integrative and complementary practice of the SUS through the MS Ordinance No. March 2018. On December 9, 2021, the Constitution and Justice Committee (CCJ) of the Chamber of Deputies unanimously approved the opinion on Bill No. 9,001/17, which authorizes the use of treatment with ozone in health, in a complementary way, throughout the national territory.
The experience is considered a safe practice from the practical guidelines and the most developed practices from experiences and treatment protocols. The toxic effects by inhalation in high doses of ozone gas, for humans and animals, for the bronchi and lungs are well known. A review of the literature on ozone genotoxicity and cytogenetic studies administered intramuscularly, intraperitoneally, intratesticularly and rectally performed in vivo in laboratory animals has shown mainly good results. The absence of genotoxic effects in rats has also been documented in the bone marrow and sperm of animals treated with ozone at medicinal doses. The cases on safety issues of treatment with ozone discussed in international journals allow us to state that most safety problems are secondary to infections or traumatic infections due to malpractice. Commonly, the ozone molecule itself is not responsible for severe reactions (12, 43–48).
Treatment with ozone promotes stimulation of oxygen metabolism (49), modulation of the immune system (50), antimicrobial action (51), tissue repair (52) and hemorrheological improvement (52, 53).
In injured tissues, treatment with ozone favors cell recovery, contributing to the reduction of edema, inflammation, oxygenation of ischemic areas (54) and restoration of blood flow in collateral vessels (53). Also promoting the increase in the epithelialization process, increasing matrix deposition and cell proliferation. Lesions treated with the oxygen-ozone mixture demonstrate the formation of granulation tissue with fewer inflammatory cells, a greater number of myofibroblasts, greater collagen deposition and an increase in the number of blood vessels. Myofibroblasts and macrophages from ozone-treated skin lesions showed increased expression of Fibroblast Growth Factor (FGF). This increased expression of FGF results in differentiation, activation and proliferation of fibroblasts and myofibroblasts associated with angiogenesis. These findings corroborate the perception that treatment with ozone favors collagen production, neovascularization and tissue remodeling (52, 55).
It is also known that treatment with ozone, through reactive oxygen species, interacts with exudates from lesions, causing ozone degradation into peroxides, stimulating tissue repair and improving oxygenation in the affected area. It favors platelet aggregation in injured tissues, increasing the endogenous production and release of these growth factors (56, 57).
The antimicrobial properties of ozone have a broad spectrum, against viruses, bacteria, fungi, yeasts and protozoa, especially in aqueous media. The mechanism of antibacterial action of ozone is through the oxidation of unsaturated lipids constituting the cytoplasmic membrane. After exposure to ozone, the olefinic bonds are attacked to form an ozonide. This action initiates the destruction of the cell's functional capacity and may even be sufficient to cause the death of weaker cells (44). This ozonide has a high oxidation potential, is unstable and exerts its own disinfecting action by attacking enzymes, sulfhydryl groups, or aldehydes, releasing peroxyl compounds, which are also disinfectants. Finally, the cell is lysed and the cytoplasm is dispersed. Thus, the action of ozone is characterized by the increase of many other oxidizing substances that can compete or complement the action of ozone to destroy critical sites within the cell or generally to oxidize protoplasm. This ripple effect is unique to ozone and its decomposition products. Virus envelopes provide complex cell attachment, penetration, and egress strategies. Peplomers, fine-tuned to adjust to changing receptors on a variety of host cells, constantly assemble a new configuration of glycoproteins under the direction of parts of the viral genome, adapting to the host cell's defenses. Envelopes are fragile and can be broken by medical ozone and its derivatives (peroxides, aldehydes, hydroxyperoxides). Viruses involved with lipids in aqueous media are readily inactivated by ozone through the oxidation of their envelope lipoproteins and glycoproteins (51).
There are also several studies on the effectiveness of ozone in general (58) and specific viral infections: herpes (59), hepatitis B and C (60), HIV (50), poliovirus (61), hepatitis A and norovirus (62), rotavirus (63). Ozone can inactivate viruses by direct oxidation of its components in vitro. However, virucidal activity in vivo becomes uncertain when viruses are in biological fluids or when they are intracellular (pneumocytes, hepatocytes, epithelia, CD4+ lymphocytes, monocytes, glial and neuronal cells), because the powerful antioxidant system protects viral integrity (64).
Medical ozone modulates the Nrf2 system (65, 66) producing three effects. First, it normalizes the redox balance through the increase of antioxidants in the cytoplasm, mitochondria and finally in the plasma, mainly glutathione peroxidase, but also glutathione reductase, NADPH and Superoxide Dismutase (SOD). Second, it induces the production of HemeOxygenase-1 (HO-1), a protective enzyme, together with heat shock proteins such as HSP-60, HSP-70 and HSP-90 (66). Third, it activates the NF-κB system, which modulates the production of pro-inflammatory interleukins in injured tissues (67). These effects contribute to restoring the normal functioning of inflamed tissues and decreasing the amount of plasma interleukins.
The treatment with ozone is also capable of inducing an adaptation to oxidative stress or promoting oxidative preconditioning by increasing and preserving antioxidant systems (68–70). The adaptation is developed after multiple exposures to treatment with ozone (71). Prolonged exposure to treatment with ozone in elderly individuals causes an increase in both ATP and 2,3-DPG in red blood cells (72). The oxygen-ozone mixture has the function of restoring and improving the metabolism of oxygen, sugars and fats to produce energy, through the normal metabolic pathways of controlled combustion: improvement of glycolysis, the respiratory chain, the fatty acid cycle, glucose 6-phosphate dehydrogenase, pyruvic acid decarboxylation (49) and increased intraerythrocytic glutathione levels (73, 74).
EGMs is created and published to include graphically presenting the best evidence found, analyzed and classified, and linking it to bibliography and full research text to make the information more accessible (14). In wounds the treatment with ozone improves wound healing and reduces treatment time but does not seem to be superior to conventional treatments. In chronic treatments, it can lead to healing in a shorter time, but additional studies are needed. In knee joints, ozone is effective in reducing pain up to 3 months with effects reducing after 3 months. Adverse effects are rarely reported. However, further studies are needed regarding the standardization of protocols for clinical practice. In herniated discs, ozone is effective and present low risk mainly via paravertebral. The intradiscal route has also been shown to be effective whether administered with or without steroids. There is evidence of long-term superiority of treatment with ozone compared to steroid injection, radiofrequency and open surgery.
Among the strengths of this study, we highlight that it was the first evidence map for the use of treatment with ozone in general therapeutic areas of our knowledge, including a comprehensive search of eligible SR, with explicit inclusion and exclusion criteria. The study provides readers with an overview, as well as detailed information, of evidence and gaps in medical ozone treatment, as well as access to primary studies.
As limitations we mention that we do not calculate the effect sizes as in a meta-analysis, nor do we provide risk assessments of bias, but we overcome these limitations by relying on the author's skills in conducting and evaluating the quality of the studies, choosing the results, analyzing the results effects and susceptibility to publication and results report bias. We suggest that in future studies, health and economic impact assessments for health services should be adopted, as well as robust methodologies for evaluating clinical trials.
5. Conclusions
This treatment with ozone EGMs proved that ozone can be effective in controlling pain, infections, inflammation and wound healing, as well as increasing the quality of life with high evidence level. No serious adverse effects were observed. The parenteral application of the oxygen-ozone gas mixture was the administration route more effective, followed by local and topical routes. Therefore, treatment with ozone can be offered as another option in the treatment of several clinical conditions, as an integrative treatment, considering its low cost, efficiency and safety. The EGMs brought confidence and credibility to the prescription and use of treatment with ozone.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
Author contributions
MS, ML, and AA: conceptualization. CM: methodology, software, and formal analysis. MS and AA: validation. MS, JB-N, CB, and AA: investigation and writing–review and editing. MS, CB, and AA: resources and writing–original draft. MS, CM, CB, and AA: data curation. MS, JB-N, ML, CM, CB, and AA: visualization. CB and AA: supervision. MS: project administration and funding acquisition. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1112296/full#supplementary-material
References
1. Ministry of Health. Maior sistema público de saúde do mundo, SUS completa 31 anos. UNA-SUS. (2021). Available online at: https://www.unasus.gov.br/noticia/maior-sistema-publico-de-saude-do-mundo-sus-completa-31-anos#:~:text=Garantidonoartigo196da,paraqualqueratendimentodesaúde (accessed November 01, 2022).
2. Nascimento CM, Tesser CD, Sousa MC. Traditional, complementary and integrative medicines in the Brazilian health primary care. Int J Complement Altern Med. (2019) 12:248–248. doi: 10.15406/ijcam.2019.12.00481
3. Ministry of Health. PORTARIA N° 702, DE 21 DE MARÇO DE 2018 - Altera a Portaria de Consolidação no 2/GM/MS, de 28 de setembro de 2017, para incluir novas práticas na Política Nacional de Práticas Integrativas e Complementares - PNPIC. (2018). Available online at: https://bvsms.saude.gov.br/bvs/saudelegis/gm/2018/prt0702_22_03_2018.html (accessed November 01, 2022).
4. Bocci V, Di Paolo N. Oxygen-ozone therapy in medicine: an update. Blood Purif. (2009) 28:373–6. doi: 10.1159/000236365
5. Viebahn-Hänsler R, León Fernández OS, Fahmy Z. Ozone in medicine: the low-dose ozone concept-guidelines and treatment strategies. Ozone Sci Eng. (2012) 34:408–24. doi: 10.1080/01919512.2012.717847
6. Duymus TM, Mutlu S, Dernek B, Komur B, Aydogmus S, Kesiktas FN. Choice of intra-articular injection in treatment of knee osteoarthritis: platelet-rich plasma, hyaluronic acid or ozone options. Knee Surg Sport Traumatol Arthrosc. (2017) 25:485–92. doi: 10.1007/s00167-016-4110-5
7. Mishra SK, Pramanik R, Das P, Das PP, Palit AK, Roy J, et al. Role of intra-articular ozone in osteo-arthritis of knee for functional and symptomatic improvement. Ind J Phys Med Rehabil. (2011) 22:65–9. Available online at: http://www.iapmr.net/ijpmr/ijpmr201102/ozone.pdf
8. Kim HS, Noh SU, Han YW, Kim KM, Kang H, Kim HO, et al. Therapeutic effects of topical application of ozone on acute cutaneous wound healing. J Korean Med Sci. (2009) 24:368–74. doi: 10.3346/jkms.2009.24.3.368
9. Indurkar MS, Verma R. Effect of ozonated oil and chlorhexidine gel on plaque induced gingivitis: a randomized control clinical trial. J Indian Soc Periodontol. (2016) 20:32–5. doi: 10.4103/0972-124X.170806
10. Patel PV, Kumar S, Vidya GD, Patel A, Holmes JC, Kumar V. Cytological assessment of healing palatal donor site wounds and grafted gingival wounds after application of ozonated oil: an eighteen-month randomized controlled clinical trial. Acta Cytol. (2012) 56:277–84. doi: 10.1159/000336889
11. Vaillant JD, Fraga A, Diaz MT, Mallok A, Viebahn-Hansler R, Fahmy Z, et al. Ozone oxidative postconditioning ameliorates joint damage and decreases pro-inflammatory cytokine levels and oxidative stress in PG/PS-induced arthritis in rats. Eur J Pharmacol. (2013) 714:318–24. doi: 10.1016/j.ejphar.2013.07.034
12. Steppan J, Meaders T, Muto M, Murphy KJ. A Metaanalysis of the effectiveness and safety of ozone treatments for herniated lumbar discs. J Vasc Interv Radiol. (2010) 21:534–48. doi: 10.1016/j.jvir.2009.12.393
13. Miake-Lye IM, Hempel S, Shanman R SP. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst Rev. (2016) 5:28. doi: 10.1186/s13643-016-0204-x
14. Portella CFS, Ghelman R, Abdala CVM, Schveitzer MC. Evidence map on the contributions of traditional, complementary and integrative medicines for health care in times of COVID-19. Integr Med Res. (2020) 9:100473. doi: 10.1016/j.imr.2020.100473
15. Schveitzer MC, Abdala CVM, Portella CFS, Ghelman R. Traditional, complementary, and integrative medicine evidence map: a methodology to an overflowing field of data and noise. Rev Panam Salud Publica. (2021) 45:1–5. doi: 10.26633/RPSP.2021.48
16. Schlechta Portella CF, Ghelman R, Abdala V, Schveitzer MC, Afonso RF. Meditation: evidence map of systematic reviews. Front Public Health. (2021) 9:1–11. doi: 10.3389/fpubh.2021.742715
17. International Initiative for Impact Evaluation. Evidence Gap Maps. (2022). Available online at: https://www.3ieimpact.org/evidence-hub/evidence-gap-maps (accessed October 12, 2022).
18. Centro Cochrane do Brasil. Ozone Therapy in the Treatment of Chronic Lower Limb Ulcer: Systematic Literature Review. (2013). Available online at: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-1024062
19. Wen Q, Liu D, Wang X, Zhang Y, Fang S, Qiu X, et al. A systematic review of ozone therapy for treating chronically refractory wounds and ulcers. Int Wound J. (2022) 19:853–70. doi: 10.1111/iwj.13687
20. Liu J, Zhang P, Tian J, Li L, Li J, Tian JH, et al. Ozone therapy for treating foot ulcers in people with diabetes. Cochrane Database Syst Rev. (2015) 2015:CD008474. doi: 10.1002/14651858.CD008474.pub2
21. Fitzpatrick E, Holland OJ, Vanderlelie JJ. Ozone therapy for the treatment of chronic wounds: a systematic review. Int Wound J. (2018) 15:633–44. doi: 10.1111/iwj.12907
22. Leon BR, Romary DJ, Landsberger SA, Bradner KN, Ramirez M, Lubitz RM. Risks of ozonated oil and ozonated water on human skin: A systematic review. Int Wound J. (2022) 19:1901–10. doi: 10.1111/iwj.13760
23. Costa T, Rodrigues-Manica S, Lopes C, Gomes J, Marona J, Falcao S, et al. Ozone therapy in knee osteoarthritis: a systematic review. Acta Med Port. (2018) 31:576–80. doi: 10.20344/amp.10330
24. Raeissadat SA, Tabibian E, Rayegani SM, Rahimi-Dehgolan S, Babaei-Ghazani A. An investigation into the efficacy of intra-articular ozone (O2/O3) injection in patients with knee osteoarthritis: a systematic review and meta-analysis. J Pain Res. (2018) 11:2537–50. doi: 10.2147/JPR.S175441
25. Arias-Vázquez PI, Tovilla-Zárate CA, Hernández-Díaz Y, González-Castro TB, Juárez-Rojop IE, López-Narváez ML, et al. Short-term therapeutic effects of ozone in the management of pain in knee osteoarthritis: a meta-analysis. PM R. (2019) 11:879–87. doi: 10.1002/pmrj.12088
26. Noori-Zadeh A, Bakhtiyari S, Khooz R, Haghani K, Darabi S. Intra-articular ozone therapy efficiently attenuates pain in knee osteoarthritic subjects: a systematic review and meta-analysis. Complement Ther Med. (2019) 42:240–7. doi: 10.1016/j.ctim.2018.11.023
27. Sconza C, Respizzi S, Virelli L, Vandenbulcke F, Iacono F, Kon E, et al. Oxygen–ozone therapy for the treatment of knee osteoarthritis: a systematic review of randomized controlled trials. Arthrosc J Arthrosc Relat Surg. (2020) 36:277–86. doi: 10.1016/j.arthro.2019.05.043
28. Arias-Vázquez PI, Tovilla-Zárate CA, Bermudez-Ocaña DY, Legorreta-Ramírez BG, López-Narváez ML. Efficacy of ozone infiltrations in the treatment of knee osteoarthritis vs. other interventional treatments: a systematic review of clinical trials. Rehabilitacion. (2019) 53:43–55. doi: 10.1016/j.rh.2018.11.001
29. Oliviero A, Giordano L, Maffulli N. The temporal effect of intra-articular ozone injections on pain in knee osteoarthritis. Br Med Bull. (2019) 132:33–44. doi: 10.1093/bmb/ldz028
30. Hedayatabad JJ, Kachooei AR, Taher Chaharjouy N, Vaziri N, Mehrad-Majd H, Emadzadeh M, et al. The Effect of ozone (O3) versus hyaluronic acid on pain and function in patients with knee osteoarthritis: A systematic review and meta-analysis. Arch Bone Jt Surg. (2020) 8:343–54. doi: 10.22038/abjs.2020.46925.2292
31. Li Q, Qi X, Zhang Z. Intra-articular oxygen-ozone versus hyaluronic acid in knee osteoarthritis: a meta-analysis of randomized controlled trials. Int J Surg. (2018) 58:3–10. doi: 10.1016/j.ijsu.2018.08.007
32. Carmona L. Ozone therapy in rheumatic diseases: a systematic review. Reumatol Clin. (2006) 2:119–23. doi: 10.1016/S1699-258X(06)73032-7
33. Magalhaes FN, Dotta L, Sasse A, Teixera MJ, Fonoff ET. Ozone therapy as a treatment for low back pain secondary to herniated disc: a systematic review and meta-analysis of randomized controlled trials. Pain Physician. (2012) 15:E115–29.
34. Costa T, Linhares D, Ribeiro da Silva M, Neves N. Ozone therapy for low back pain. A systematic review. Acta Reumatol Port. (2018) 43:172–181.
35. Sampaio N da R, Cruz LRO, Medrado AP. A utilização da Ozonioterapia no tratamento da lombalgia associada à hérnia de disco lombar – Uma Revisão Sistemática TT - Ozonetherapy in the treatment of Low Back Pain associated to Lumbar Disk Herniation – a systematic review. Rev Pesqui Fisioter. (2018) 8:579–87. doi: 10.17267/2238-2704rpf.v8i4.2107
36. de Andrade RR, de Oliveira-Neto OB, Barbosa LT, Santos IO, de Sousa-Rodrigues CF, Barbosa FT. Effectiveness of ozone therapy compared to other therapies for low back pain: a systematic review with meta-analysis of randomized clinical trials. Brazilian J Anesthesiol. (2019) 69:493–501. doi: 10.1016/j.bjane.2019.06.007
37. Rimeika G, Saba L, Arthimulam G, Della Gatta L, Davidovic K, Bonetti M, et al. Metanalysis on the effectiveness of low back pain treatment with oxygen-ozone mixture: Comparison between image-guided and non-image-guided injection techniques. Eur J Radiol Open. (2021) 8:100389. doi: 10.1016/j.ejro.2021.100389
38. Sconza C, Leonardi G, Kon E, Respizzi S, Massazza G, Marcacci M, et al. Oxygen-ozone therapy for the treatment of low back pain: a systematic review of randomized controlled trials. Eur Rev Med Pharmacol Sci. (2021) 25:6034–46. doi: 10.26355/eurrev_202110_26881
39. Najadir Cristina De Faria GC, Victor Gualberto VC, Sergio Bruzadelli M, Fayez Bahmad JR. Efficacy of ozone therapy in the treatment of tinnitus: a systematic review. Int Tinnitus J. (2021) 25:149–53. doi: 10.5935/0946-5448.20210027
40. Radvar S., Karkon-shayan S, Motamed-Sanaye A, Majidi M, Hajebrahimi S, Taleschian-Tabrizi N, et al. Using ozone therapy as an option for treatment of COVID-19 patients: a scoping review. Adv Exp Med Biol. (2021) 1327:151–60. doi: 10.1007/978-3-030-71697-4_12
41. Baeza-Noci J, Pinto-Bonilla R. Systemic review: ozone: a potential new chemotherapy. Int J Mol Sci. (2021) 22:11796. doi: 10.3390/ijms222111796
42. Centro Cochrane do Brasil. Ozonioterapia no tratamento da dor lombar. (2013). Available online at: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-1024059
43. Hu B, Zheng J, Liu Q, Yang Y, Zhang Y. The effect and safety of ozone autohemotherapy combined with pharmacological therapy in postherpetic neuralgia. J Pain Res. (2018) 11:1637–43. doi: 10.2147/JPR.S154154
44. Fisher CW, Lee D, Dodge BA, Hamman KM, Robbins JB, Martin SE. Influence of catalase and superoxide dismutase on ozone inactivation of Listeria monocytogenes. Appl Environ Microbiol. (2000) 66:1405–9. doi: 10.1128/AEM.66.4.1405-1409.2000
45. Bocci V, Zanardi I, Travagli VR. Reply to “The irrationality of a non-specific immunomodulation therapy used in cardiovascular diseases deserves a critical comment”. Atherosclerosis. (2010) 211:40. doi: 10.1016/j.atherosclerosis.2010.04.016
46. Bocci V. Ozone: A New Medical Drug. (2011). Available online at: https://link.springer.com/book/10.1007/978-90-481-9234-2
47. González VM, Figueras JT, Cepero SM, Díaz HA. Ozonoterapia y laserpuntura en el tratamiento de la sordera súbita TT - Ozonetherapy and the laser puncture in the treatment of sudden deafness. Rev Cuba cir. (2004) 43. Available online at: https://pesquisa.bvsalud.org/portal/resource/pt/lil-628196
48. Re L, Rutledge DK, Erario A, Baeza-Noci J, Travagli V, Menendez S, et al. Mollica Correcting misinformation about the science and practice of evidence-based, safe and effective ozone therapy. J Emerg Med. (2021) 17:1–2. doi: 10.1016/j.jemermed.2021.08.001
49. Aydogan S, Seda A. How Ozone Treatment Affects Erythrocytes. Hemodynamics. (2012). doi: 10.5772/36876
50. Cespedes-Suarez J, Martin-Serrano Y, Carballosa-Peña MR, Dager-Carballosa DR. The immune response behavior in HIV-AIDS patients treated with Ozone therapy for two years. J Ozone Ther. (2018) 2:1–9. doi: 10.7203/jo3t.2.3.2018.11458
51. Wells KH, Latino J, Gavalchin J, Poiesz BJ. Inactivation of human immunodeficiency virus type 1 by ozone in vitro. Blood. (1991) 78:1882–90. doi: 10.1182/blood.V78.7.1882.1882
52. Svystonyuk DA, Ngu JMC, Mewhort HEM, Lipon BD, Teng G, Guzzardi DG, et al. Fibroblast growth factor-2 regulates human cardiac myofibroblast-mediated extracellular matrix remodeling. J Transl Med. (2015) 13:1–11. doi: 10.1186/s12967-015-0510-4
53. Abyshov NS, Abdullayev AG, Zakirdzhaev ED, Guliyev RA, Akhmedov MB, Tagizade GT, et al. The results of combined surgical treatment of thromboangiitis obliterans and critical lower limb ischemia using prolonged epidural analgesia and autohemotherapy with ozone. Khirurgiia (Sofiia). (2016) 9:45–50. doi: 10.17116/hirurgia2016945-50
54. Clavo B, Catala L, Perez JL, Rodriguez V, Robaina F. Ozone therapy on cerebral blood flow: a preliminary report. Evid Based Complement Alternat Med. (2004) 1:315–9. doi: 10.1093/ecam/neh039
55. Soares CD, Morais TML, Araújo RMFG, Meyer PF, Oliveira EAF, Silva RMV, et al. Effects of subcutaneous injection of ozone during wound healing in rats. Growth Factors. (2019) 37:95–103. doi: 10.1080/08977194.2019.1643339
56. Zhang J, Guan M, Xie C, Luo X, Zhang Q, Xue Y. Increased growth factors play a role in wound healing promoted by noninvasive oxygen-ozone therapy in diabetic patients with foot ulcers. Oxid Med Cell Longev. (2014) 2014:273475. doi: 10.1155/2014/273475
57. Wang Y, Tan M, Ouyang H, Deng L. Effects of ozone stimulation of bronchial epithelial cells on proliferation and collagen synthesis of co-cultured lung fibroblasts. Exp Ther Med. (2018) 15:5314–22.
58. Di Paolo N, Bocci V, Gaggiotti E. Ozone therapy. Int J Artif Organs. (2004) 27:168–75. doi: 10.1177/039139880402700303
59. Huang J, Huang J, Xiang Y, Gao L, Pan Y, Lu J. [Topical ozone therapy: An innovative solution to patients with herpes zoster]. Zhong Nan Da Xue Xue Bao Yi Xue Ban. (2018) 43:168–72. doi: 10.11817/j.issn.1672-7347.2018.02.011
60. Neronov VA. [Experience with the use of ozone for the treatment of chronic viral hepatitis]. Vopr Kurortol Fizioter Lech Fiz Kult. (2009) 6:14–7.
61. Herbold K, Flehmig B, Botzenhart K. Comparison of ozone inactivation, in flowing water, of hepatitis A virus, poliovirus 1, and indicator organisms. Appl Environ Microbiol. (1989) 55:2949–53. doi: 10.1128/aem.55.11.2949-2953.1989
62. Brié A, Boudaud N, Mssihid A, Loutreul J, Bertrand I, Gantzer C. Inactivation of murine norovirus and hepatitis a virus on fresh raspberries by gaseous ozone treatment. Food Microbiol. (2018) 70:1–6. doi: 10.1016/j.fm.2017.08.010
63. Khadre MA, Yousef AE. Susceptibility of human rotavirus to ozone, high pressure, and pulsed electric field. J Food Prot. (2002) 65:1441–6. doi: 10.4315/0362-028X-65.9.1441
64. Zaky S, Kamel SE, Hassan MS, Sallam NA, Shahata MA, Helal SR, et al. Preliminary results of ozone therapy as a possible treatment for patients with chronic hepatitis C. J Altern Complement Med. (2011) 17:259–63. doi: 10.1089/acm.2010.0016
65. Galiè M, Covi V, Tabaracci G, Malatesta M. The role of Nrf2 in the antioxidant cellular response to medical ozone exposure. Int J Mol Sci. (2019) 20:1–15. doi: 10.3390/ijms20164009
66. Sagai M, Bocci V. Mechanisms of action involved in ozone therapy: Is healing induced via a mild oxidative stress? Med Gas Res. (2011) 1:29. doi: 10.1186/2045-9912-1-29
67. Viebahn-Häensler R, León Fernández OS. Ozone in medicine. The low-dose ozone concept and its basic biochemical mechanisms of action in chronic inflammatory diseases. Int J Mole Sci. (2021) 22:7890. doi: 10.3390/ijms22157890
68. Bocci VA. Scientific and medical aspects of ozone therapy. State of the art. Arch Med Res. (2006) 37:425–35. doi: 10.1016/j.arcmed.2005.08.006
69. Tylicki L, Nieweglowski T, Biedunkiewicz B, Chamienia A, Debska-Slizien A, Aleksandrowicz E, et al. The influence of ozonated autohemotherapy on oxidative stress in hemodialyzed patients with atherosclerotic ischemia of lower limbs. Int J Artif Organs. (2003) 26:297–303. doi: 10.1177/039139880302600404
70. Martinez G, Al-Dalain SM, Menendez S, Guiliani A, León OS. Ozone treatment reduces blood oxidative stress and pancreas damage in a streptozotocin-induced diabetes model in rats. Acta Farm Bonaer. (2005) 24:491–7.
71. Ajamieh H, Merino N, Candelario-Jalil E, Menéndez S, Martinez-Sanchez G, Re L, et al. Similar protective effect of ischaemic and ozone oxidative preconditionings in liver ischaemia/reperfusion injury. Pharmacol Res. (2002) 45:333–9. doi: 10.1006/phrs.2002.0952
72. du Plessis LH, van der Westhuizen FH, Kotze HF. The effect of blood ozonation on mitochondrial function and apoptosis of peripheral blood mononuclear cells in the presence and absence of plasma antioxidants. Afr J Biotechnol. (2007) 6:1763–9. doi: 10.5897/AJB2007.000-2259
73. Bocci V, Luzzi E, Corradeschi F, Paulesu L. Studies on the biological effects of ozone: 5. Evaluation of immunological parameters and tolerability in normal volunteers receiving ambulatory autohaemotherapy. Biotherapy. (1993) 7:83–90. doi: 10.1007/BF01877731
Keywords: systematic reviews, Ozone Therapy, Medical Ozone Therapy, evidence gap map, complementary therapies
Citation: Serra MEG, Baeza-Noci J, Mendes Abdala CV, Luvisotto MM, Bertol CD and Anzolin AP (2023) The role of ozone treatment as integrative medicine. An evidence and gap map. Front. Public Health 10:1112296. doi: 10.3389/fpubh.2022.1112296
Received: 30 November 2022; Accepted: 28 December 2022;
Published: 16 January 2023.
Edited by:
Bernardino Clavo, University Hospital of Gran Canaria Dr. Negrín, SpainCopyright © 2023 Serra, Baeza-Noci, Mendes Abdala, Luvisotto, Bertol and Anzolin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Paula Anzolin,  YW5hcGF1bGFzb3JkaWFuem9saW5AZ21haWwuY29t
YW5hcGF1bGFzb3JkaWFuem9saW5AZ21haWwuY29t