 Zhonghui Zhao1,2
Zhonghui Zhao1,2 Jie Chu3,4
Jie Chu3,4 Xiaohui Xu3,4Yanwen Cao1,2
Xiaohui Xu3,4Yanwen Cao1,2 Tamara Schikowski5Mengjie Geng6
Tamara Schikowski5Mengjie Geng6 Gongbo Chen7
Gongbo Chen7 Guannan Bai8
Guannan Bai8 Kejia Hu9
Kejia Hu9 Jingjing Xia10
Jingjing Xia10 Wei Ma1,2
Wei Ma1,2 Qiyong Liu6Zilong Lu3,4Xiaolei Guo3,4*
Qiyong Liu6Zilong Lu3,4Xiaolei Guo3,4* Qi Zhao1,2,5*
Qi Zhao1,2,5*- 1Department of Epidemiology, School of Public Health, Shandong University, Jinan, China
- 2Shandong University Climate Change and Health Center, Jinan, China
- 3Shandong Center for Disease Control and Prevention, Jinan, China
- 4Academy of Preventive Medicine, Shandong University, Jinan, China
- 5Department of Epidemiology, Leibniz Institute for Environmental Medicine (IUF)-Leibniz Research Institute for Environmental Medicine, Düsseldorf, Germany
- 6Chinese Center for Disease Control and Prevention, Beijing, China
- 7Department of Occupational and Environmental Health, School of Public Health, Sun Yat-sen University, Guangzhou, Guangdong, China
- 8Department of Child Health Care, The Children's Hospital, National Clinical Research Center for Child Health, Zhejiang University School of Medicine, Hangzhou, China
- 9Department of Big Data in Health Science, School of Public Health, Zhejiang University, Hangzhou, China
- 10School of Life Sciences, Greater Bay Area Institute of Precision Medicine (Guangzhou), Fudan University, Guangzhou, China
Introduction: Numerous studies have reported the modification of particulate matters (PMs) on the association between cold temperature and health. However, it remains uncertain whether the modification effect may vary by size of PMs, especially in Shandong Province, China where the disease burdens associated with cold temperature and PMs are both substantial. This study aimed to examine various interactive effects of cold exposure and ambient PMs with diameters ≤1/2.5 μm (PM1 and PM2.5) on premature deaths in Shandong Province, China.
Methods: In the 2013-2018 cold seasons, data on daily mortality, PM1 and PM2.5, and weather conditions were collected from the 1822 sub-districts of Shandong Province. A time-stratified case-crossover study design was performed to quantify the cumulative association between ambient cold and mortality over lag 0-12 days, with a linear interactive term between temperature and PM1 and PM2.5 additionally added into the model.
Results: The mortality risk increased with temperature decline, with the cumulative OR of extreme cold (−16.9°C, the 1st percentile of temperature range) being 1.83 (95% CI: 1.66, 2.02), compared with the minimum mortality temperature. The cold-related mortality risk was 2.20 (95%CI: 1.83, 2.64) and 2.24 (95%CI: 1.78, 2.81) on high PM1 and PM2.5 days, which dropped to 1.60 (95%CI: 1.39, 1.84) and 1.60 (95%CI: 1.37, 1.88) on low PM1 and PM2.5 days. PM1 showed greater modification effect for per unit concentration increase than PM2.5. For example, for each 10?g/m3 increase in PM1 and PM2.5, the mortality risk associated with extreme cold temperature increased by 7.6% (95% CI: 1.3%, 14.2%) and 2.6% (95% CI: −0.7%, 5.9%), respectively.
Discussion: The increment of smaller PMs' modification effect varied by population subgroups, which was particularly strong in the elderly aged over 75 years and individuals with middle school education and below. Specific health promotion strategies should be developed towards the greater modification effect of smaller PMs on cold effect.
1. Introduction
Extreme temperature events are increasingly frequent in the context of climate change, becoming a major health challenge now and in the next decades (1). Numerous studies have reported that exposure to cold or high temperatures are both associated with adverse health outcomes. Despite the global warming trend, most temperature-related excess deaths are still attributable to exposure to cold temperatures (2, 3). For example, it is estimated that 9.43% of global premature deaths are associated with non-optimal temperature, with 8.52% explainable by cold exposure (4).
Particulate matter (PM) is another major environmental hazard, triggering a broad range of health outcomes such as cardiovascular disease, respiratory dysfunction and premature deaths (5–7). In 2019, exposure to PMs caused 6.4 million premature deaths, accounting for 18.4% of the global total mortality and therefore ranking the fifth top health risk factor (8). Moreover, PMs with smaller size may be more vulnerable than coarse PMs (9–11). For example, in Anhui Province, China between 2016 and 2018, the risk of hospitalization on childhood pneumonia increased by 10.28, 1.21, and 1.10% for each 10 μg/m3 increase in PMs with a diameter of ≤1.0, 2.5, and 10 μm (i.e., PM1, PM2.5, and PM10), respectively (9).
In recent years, increasing public concerns have focused on the combined effect of ambient cold and PMs. A study in Guangzhou, China has reported that the cold-related mortality risk may increase by 40.7 and 46.7% on days with PM10 concentrations at the 25th and 75th percentiles of concentration range during study period, respectively (12). Another European study has found that the cold-related risk of cardiovascular mortality may increase by 16.2 and 2.0% on days with high and low particle number concentrations (PNCs), respectively (13). However, it remains largely unclear how the modification effect of PMs on cold-related health risk may vary by the size of PMs. Clarifying this research issue can help us better understand the mixed disease burden of the two environmental factors, and thus develop more targeted health promotion strategies.
China has one of the greatest disease burdens from PMs and ambient suboptimal temperature (14). The lancet countdown report and the national environmental surveillance have further indicated that the PMs' concentration and extreme temperature events are more substantial in Shandong province than many other Chinese areas, considering its the second largest population size, unique location, and rapid population aging trend (15). Shandong has abundant industrial activities and a coal-based energy structure. In China, although the concentration of PM2.5 has declined in recent years, the PM pollution remain heavy in Shandong Province in comparison to most other regions (16). This leads Shandong Province to be an ideal area to evaluate the combined health risk of ambient cold and various sizes of PMs.
Using data from 1,822 sub-districts in Shandong Province, China, this study is designed to explore how PMs with various sizes (i.e. PM1 and PM2.5) may modify the strength of association between ambient cold temperature and mortality.
2. Materials and methods
2.1. Study area
Shandong Province is a coastal province in eastern China that locates between 34.382° N - 38.400° N and 114.792° E - 122.705° E, and covers an area of 155,800 km2. It has a monsoon climate of medium latitudes with four distinct seasons throughout the year. In 2021, the resident population in Shandong Province was 101.5 million, ranking it the second largest population size in China.
2.2. Data collection
We collected daily deaths in 1,822 sub-districts of Shandong province from 2013 to 2018 from Shandong Center for Disease Control and Prevention. Variables included each individual's date of death, age, gender, education level, cause of death (coded using the international classification of diseases code, ICD-10) and home address.
The daily concentrations of PM1 and PM2.5 were modeled at a spatial resolution of 0.01° × 0.01°, with the methods on modeling well described by our previous studies and the data quality validated (17, 18). Briefly, we collected daily data on PMs from monitoring sites of the China National Environmental Monitoring Center. A random forest model based on machine learning algorithm was combined with big data to generate data sets, including ground measurements, satellite remote sensing products, and atmospheric reanalysis. The daily meteorological data during the same period were collected from the China Meteorological Data Network (http://data.cma.cn/) at a spatial resolution of 0.01° × 0.01°, including daily average temperature, relative humidity and wind velocity. Meteorological data and pollution data were assigned to the sub-district where the individual lived.
2.3. Statistical analysis
Following previous studies (19–21), the cold season was defined as the four consecutive coldest months of the year in Shandong province. A time-stratified case-crossover study design was applied: Conditional logistic regression with the non-distributed lag model was used to fit the relationship between ambient temperature and risk of mortality in the cold season. Specifically, each case works as a stratum, and its controls were defined as the days of the same week of the same year and month (22). This self-matched case-control design can adjust for temporal variation and the effect of time-dependent variables such as age, sex and lifestyle (23). The bidirectional selection of controls can reduce long-term temporal trend, seasonality, and confounding effect caused by the “day-of-the-week effect.”
Our initial analysis indicated that the adverse effect of ambient temperature lasted for up to 12 days, which then were used in the formal analysis and justified in the sensitivity analysis below. The equation was as follows:
Logit (P) = αstratum(i) + cb (Tempi) + ns(RHi, df=3)+ PMi + cb (Tempi)*PMi.
Where P is the possibility of deaths. Each death case (i) with its controls works as a strata, and α1 to αs are stratum constants (assuming that the number of deaths is s). cb (Tempi) is the crossbasis function obtained by DLNM for the death case i to fit the nonlinear and lagged effect of temperature, with a natural cubic spline with three degrees of freedom (dfs) for the temperature dimension and a natural cubic spline with four dfs for the lag dimension. ns(RHi, df = 3) represents a natural spline function with 3 df for the moving average value of relative humidity (RH) over lag 0–12 days. PMi is the linear function of moving average value of PM1 or PM2.5 over lag 0–12 days. The cb (Tempi)*PMi is the interactive term between the crossbasis function of temperature and the linear function of PM1 or PM2.5.
Two model sets were used to examine the modification effects of PM1 and PM2.5 on temperature-mortality risk, respectively. For each model set, the interactive term was entered into the model by centering PM1 or PM2.5 at the low, median and high levels, respectively. Following previous studies (13, 24, 25), the low, median and high levels of PM1 and PM2.5 were defined using relative thresholds, i.e., the concentrations at the 10th, 50th and 90th percentile of the PM1 and PM2.5 concentration range during the study period. The extreme cold effect was defined as the cumulative OR (lag 0–12 days) with 95% confidence interval (CI) of mortality corresponding to the 1st percentile of the temperature range in the cold season, compared with the minimum mortality temperature (MMT).
To straightforwardly compare the modification effects of PM1 and PM2.5, the percentage changes in risk of mortality associated with extreme cold temperature for each 10 μg/m3 increase in PM1 and PM2.5 were calculated from the coefficient of the interactive term. Stratified analyses were performed by gender, age-groups (< 75 yr or ≥75 yr), educational level (middle school and below, or above middle school), and by cause of death [cardiorespiratory diseases (I00-J99) and others (A00-B99, C00-D48, D50-H95 and K00-Z99)].
2.4. Sensitivity analyses
We conducted a series of sensitivity analyses to verify the robustness of the model and parameters, including by changing the maximum lag of temperature from 10 to 18 days, and the positions and number of knots in the crossbasis function, the dfs in the natural cubic spline function of relative humidity from three to four, and by additionally adding the moving average value of ozone over lag 0–12 days into the model.
All analyses were conducted using R software (version 4.1.2). The “dlnm” package and “mvmeta” package were used to fit distributed lag non-linear model and multivariate meta-analysis, respectively.
3. Results
3.1. Descriptive statistics
From 2013 to 2018, 1,473,300 deaths were recorded in the cold season (November to February) in all sub-districts of Shandong Province (Table 1). The median values of ambient temperature, PM1 and PM2.5 (with 25th and 75th percentile range) in the cold season were 1.17 (−1.49, 4.37)°C, 51.78 (42.63, 63.78) μg/m3, 81.34 (56.33, 111.05) μg/m3, respectively (Figure 1 and Supplementary Figure S1).
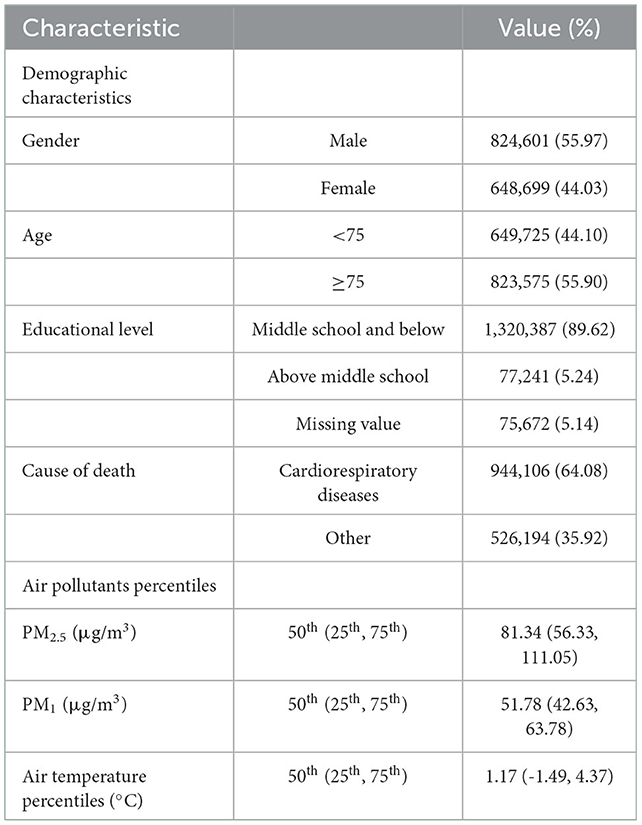
Table 1. Demographic and environmental characteristics of mortality in cold season in Shandong Province from 2013 to 2018.
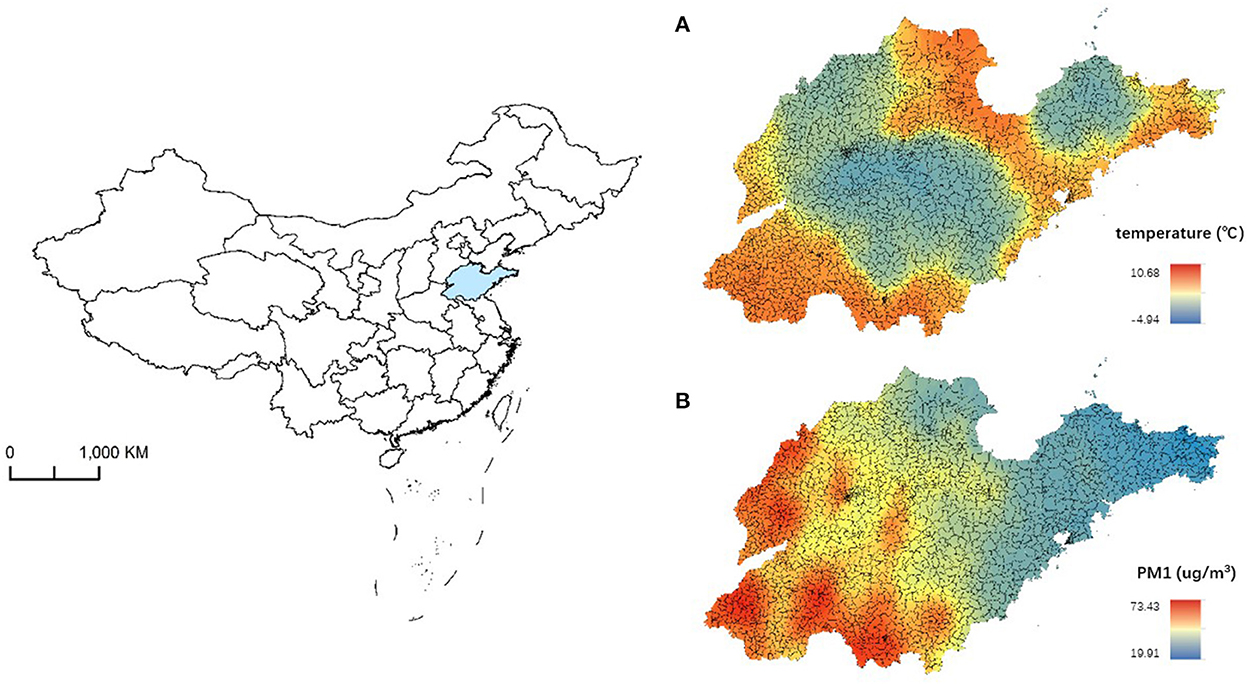
Figure 1. The distribution of temperature (A) and PM1 concentration (B) in cold season in Shandong Province during 2013–2018.
3.2. Cold death effect under different pollution levels
The risk of all-cause mortality increased with temperature cooling, with the MMT located at 18.5°C (Figure 2). The effect of extreme cold effect, i.e., the cumulative OR of mortality at the extreme low temperature (−16.9°C), was 1.83 (95% CI: 1.66, 2.02) over lag 0–12 days, in comparison to the MMT. In general, the cold-related risk of mortality was stronger at high levels of PM1 and PM2.5 (Figure 3). For example, the cumulative extreme cold effect was 2.20 (95%CI: 1.83, 2.64) and 2.24 (95%CI: 1.78, 2.81) on days with high PM1 and PM2.5 concentrations in the cold season. The extreme cold effect dropped to 1.60 (95%CI: 1.39, 1.84) and 1.60 (95%CI: 1.37, 1.88) on days with low PM1 and PM2.5 concentrations. Lag pattern analysis for PM1 and PM2.5 had similar results (Supplementary Figure S2): the extreme cold effect combined with high PMs appeared on the first day of cold exposure and diminished until lag 11 day, which commonly appeared on lag 2 day and disappeared until lag 10 day for the combination of cold temperature, and low PM1 and PM2.5 levels.
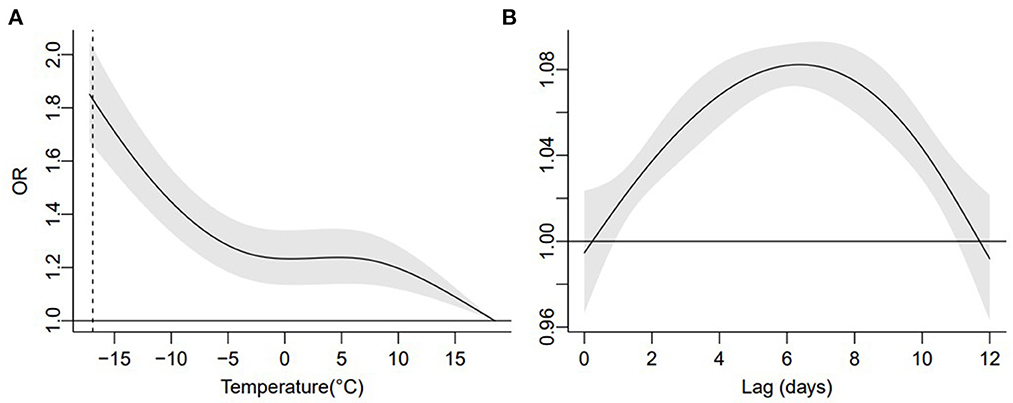
Figure 2. Overall cumulative relationship between ambient temperature and mortality (A) in the cold season, and the associated lag-response pattern (B). The dotted line indicates extreme low temperature.
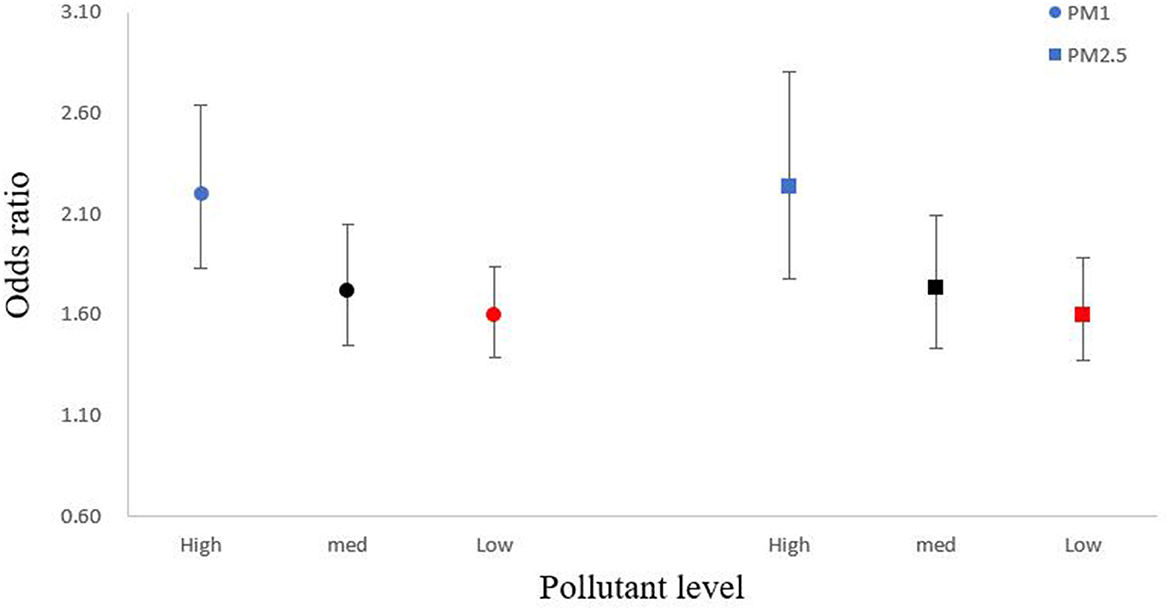
Figure 3. Modified overall cumulative air temperature-mortality associations at extreme low temperature by air pollution with 95% CIs. In the abscissa “pollution level,” the “high” represent for high air pollution level (concentration above 90th value), the “med” represent for medium air pollution level (concentration for 50th value), the “low” represent for low air pollution level (concentration below 10th value).
3.3. The modification effect of PMs and stratified analysis
Results indicated that the modification effect was slightly higher for smaller PMs size, such that for every 10 μg/m3 in PM1 and PM2.5, the mortality risk associated with extreme cold temperature increased by 7.6% (95% CI: 1.3%, 14.2%) and 2.6% (95% CI: −0.7%, 5.9%), respectively. The modification effect of smaller PMs on cold temperature-mortality association varied across population subgroups (Table 2). For example, for every 10 μg/m3 in PM2.5 and PM1, the increment of mortality risk associated with extreme cold temperature increased from 3.4% (95% CI: −1.2%, 8.1%) to 9.9% (95% CI: 0.9%, 19.8%) for the elderly aged over 75 years, which remained insignificant for younger adults. The variation was more obvious for subgroups with different educational levels: for every 10 μg/m3 in PM2.5 and PM1, the increment of mortality risk associated with extreme cold temperature increased from 3.4% (95% CI: −0.3%, 7.4%) to 8.3% (95% CI: 1.4%, 15.7%) for individuals with middle school education or below, which remained insignificant with the effect size also nearly unchanged for individuals with middle school educational level or higher.

Table 2. Percentage change in cold-related mortality per 10 μg/m3 increase in PM1 and PM2.5 in Shandong Province from 2013 to 2018.
3.4. Sensitivity analysis
Sensitivity analysis indicated the results were reliable by changing lags of temperature, and positions and number of knots in the crossbasis function, and by additionally adding ozone into the model (Supplementary Figures S3–S5).
4. Discussion
Our study in Shandong Province of China indicated a strong association between ambient cold temperature and risk of mortality. The strength of association was strongly intensified by high PMs concentrations, with smaller size of PMs showing greater modification effect. Subgroup analysis indicated that the stronger modification effect of smaller PMs on cold-mortality association varied across population subgroups, which was particularly obvious for the elderly aged 75 years and above, and for individuals educated middle school and below.
Previously, numerous studies have reported the modification of PMs on adverse effect of suboptimal temperature while most of them focused on heat exposure. For example, in France, every 10 μg/m3 increase in PM10 was associated with a 14.2% increase in mortality during heat waves (26). In comparison, less evidence is available on the combined impact of PMs and cold temperature. Our study observed a strong association between ambient temperature in the cold season and mortality risk in Shandong Province, with the strength of association greater on days with high PMs concentrations. Similar findings were reported in Europe, where cold temperature was observed to have a greater impact on total mortality and cardiovascular mortality on days with high PMs levels (13). Another Chinese study also showed that the death risk of PM2.5 at low temperature was higher than that at medium temperature (27). Cold temperatures can lead to vasoconstriction and the release of inflammatory markers in the blood, which may increase blood pressure and vascular resistance, and finally trigger cardiovascular events (28). In comparison to previous explorations, our analysis provides details of the changing cold effect by PMs levels over lag days. The extreme cold effect combined with high PMs appeared immediately rather than appeared on lag 2 day with low PMs levels, and diminished until lag 11 day. This may indicate that the PM level has a specific modification on the extreme cold effect. In the case of high particulate pollution, the extreme cold effect would appear directly after cold exposure. It is speculated that low temperature and PM exposures may share certain pathways toward adverse health outcomes, such as reducing the clearance rate of respiratory mucosa cilia (29). This may partly explain the immediate cold effect on days with high PM concentration. Further research is encouraged to clarify the underpinning mechanism.
Some studies have evaluated whether the health impact of PM may vary by its physical size. For example, a study has pointed out that the global risk of all-cause mortality may increase by 0.44 and 0.68% per 10 μg/m3 increase in PM10 and PM2.5, respectively (30). A study in Guangzhou, China has indicated that PM1 may be a more important risk factor for cardiovascular death (31). Another Chinese study in Zhejiang Province has also shown that PM1 have slightly higher impacts on all-cause, cardiovascular and respiratory mortality than PM2.5 (10). In addition, a mice experiment has observed that the toxic effect of PM2.5 on lung tissue cells increases with exposure to higher PM2.5 mass concentration, and PM1 may explain the major effect size of PM2.5 in damaging mouse cells (32). In comparison, the modification of PMs size on cold effect remains largely unclear. Our study found that smaller size of PMs might have greater modification effect on the association between ambient cold and mortality.
Without more clinical and molecular information, it is difficult to explain the underpinning mechanisms of the observed higher modification effect of PM1 than PM2.5. However, compared with PM2.5, PM1 has small size and large active surface area, allowing it to penetrate the deepest part of the respiratory system and then travel to other physiological organs via the circulatory system in an easier way (33). As a result, the health risk is expected to be greater under the same exposure concentration of PM1 than for PM2.5 (34). A study shows that cold temperature can impair the antiviral response that induced by interferon (35). Both PMs and cold temperature are reported to cause inflammation: PMs exposure induces mucus metaplasia and increases mucus production (36). Meanwhile, cold temperature can induce airway inflammation and excess mucus production through cold-inducible RNA-binding protein mediated increase in mRNA stability and protein translation (37). Another study has indicated that low ambient temperature and PM may increase the level of respiratory inflammation (38). The evidence aforementioned may explain the interactive effect between cold temperature and PM exposure, and the higher modification effect of smaller size of PM. However, more supportive findings are still necessary to clarify the mechanism.
Stratified analysis showed that the greater modification effect of PM1 than PM2.5 on cold-related mortality risk was more obvious for certain population subgroups such as the elderly aged over 75 years and individuals with middle school education and below. There is no substantial difference in the modification effect of PMs between males and females. Few studies have explored the differences between men and women in the modification effect of PMs. However, a study in Hong Kong found that although the cold-related mortality risk for both males and males was significantly higher, the gender difference in cold effect is the smallest (39). In addition, although the mortality risk of PM2.5 in females was slightly stronger than males, the differences were not statistically significant (40). Consistent with our study, previous research found that with the rise of particulate matter levels, the elderly are more vulnerable to low temperature than the young (12). In addition, we found that the modification effect of PMs on cold-related mortality risk was higher for other diseases than cardiorespiratory disease. The mechanism remains unclear without more details about the study population at the individual level. However, a considerable proportion of patients in “Other” group were due to tumors, whose physiological systems were extremely susceptible to cold temperature and air pollution because many studies showed that low temperature and PMs are risk factors for tumors (41–44).
We found that individuals of low educational level were more susceptible to low temperatures, and the risk of death increased with the rise of PMs concentration. Many studies have reached similar conclusion (45, 46). Compared with well-educated people, less educated people are more vulnerable to extreme temperature events (47). Socioeconomic factors such as educational attainment may modify the health effects of air pollution in several pathways (48). For example, it is speculated that individuals of low educational level are often at a lower socioeconomic status, which may lead to poor living standards and nutritional conditions.
Our study has several strengths. First, we used a time stratified case-crossover design to explore the various interactive effects of cold exposure and ambient PMs on premature deaths, which can control both seasonal effect and day-of-the-week effect. The self-control method has well balanced the impact of many individual factors on the outcome. Second, compared with other studies, we focused on exploring the effects of different size particles on the cold temperature-death relationship, which help better understand the combined effects of air pollution and extreme temperature events. Finally, most studies exploring the individual or combined effect of air pollutants and ambient temperature using data at the city or county level. In this study, the assignment of pollution and weather exposure at a sub-district level improved the accuracy of exposure assessment. There are several limitations to this study. We were unable to consider the impact of PM components on the cold-mortality association. In addition, the environmental exposure assessment still needs improvement in the future, such as at the individual level.
5. Conclusions
Our study finds that the risk of cold temperature on mortality increased on days with higher PMs concentrations, and the modification effect increased for smaller size of PMs. The findings suggest that more consideration should be given to the combined effect of smaller air pollution particles and ambient cold when developing healthcare strategies. Specific subgroups, such as individuals aged 75 years and above, and those with low educational level should be considered with public health priority.
Data availability statement
The datasets presented in this article are not readily available because data is confidential. Requests to access the datasets should be directed to QZ, cWkuemhhb0BzZHUuZWR1LmNu.
Author contributions
ZZ: conceptualization, methodology, formal analysis, data curation, and writing–original draft. JC, XX, TS, MG, GC, GB, KH, and JX: writing–review and editing. YC: methodology and formal analysis. WM and QL: conceptualization, supervision, and writing–review and editing. ZL: data curation. XG: data curation and writing–review and editing. QZ: conceptualization, methodology, writing–review and editing, supervision, project administration, and funding acquisition. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Natural Science Foundation of Shandong Province in China (ZR2021QH318) and the Shandong Excellent Young Scientists Fund Program (Overseas) (2022HWYQ-055).
Acknowledgments
We thank the Shandong Center for Disease Control and Prevention for providing daily counts of death data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1093588/full#supplementary-material
References
1. Maibach EW, Sarfaty M, Mitchell M, Gould R. Limiting global warming to 15 to 20°C-A unique and necessary role for health professionals. PLoS Med. (2019) 16:e1002804. doi: 10.1371/journal.pmed.1002804
2. Cheng J, Xu Z, Bambrick H, Su H, Tong S, Hu W. Impacts of heat, cold, and temperature variability on mortality in Australia, 2000-2009. Sci Total Environ. (2019) 651(Pt 2):2558–65. doi: 10.1016/j.scitotenv.2018.10.186
3. Choi HM, Chen C, Son JY, Bell ML. Temperature-mortality relationship in North Carolina, USA: regional and urban-rural differences. Sci Total Environ. (2021) 787:147672. doi: 10.1016/j.scitotenv.2021.147672
4. Zhao Q, Guo Y, Ye T, Gasparrini A, Tong S, Overcenco A, et al. Global, regional, and national burden of mortality associated with non-optimal ambient temperatures from 2000 to 2019: a three-stage modelling study. Lancet Planet Health. (2021) 5:e415–25. doi: 10.1016/S2542-5196(21)00081-4
5. Chen J, Hoek G. Long-term exposure to PM and all-cause and cause-specific mortality: a systematic review and meta-analysis. Environ Int. (2020) 143:105974. doi: 10.1016/j.envint.2020.105974
6. Saini P, Sharma M. Cause and Age-specific premature mortality attributable to PM(25) exposure: an analysis for Million-Plus Indian cities. Sci Total Environ. (2020) 710:135230. doi: 10.1016/j.scitotenv.2019.135230
7. Li T, Guo Y, Liu Y, Wang J, Wang Q, Sun Z, et al. Estimating mortality burden attributable to short-term PM(25) exposure: a national observational study in China. Environ Int. (2019) 125:245–51. doi: 10.1016/j.envint.2019.01.073
8. Explore results from the 2019 Global Burden of Disease (GBD) study. Available online at: https://vizhub.healthdata.org/gbd-results/ (accessed November 01, 2022).
9. Wang X, Xu Z, Su H, Ho HC, Song Y, Zheng H, et al. Ambient particulate matter (PM(1), PM(25), PM(10)) and childhood pneumonia: the smaller particle, the greater short-term impact? Sci Total Environ. (2021) 772:145509. doi: 10.1016/j.scitotenv.2021.145509
10. Hu K, Guo Y, Hu D, Du R, Yang X, Zhong J, et al. Mortality burden attributable to PM(1) in Zhejiang province, China. Environ Int. (2018) 121(Pt 1):515–22. doi: 10.1016/j.envint.2018.09.033
11. Liu W, Wei J, Cai M, Qian Z, Long Z, Wang L, et al. Particulate matter pollution and asthma mortality in China: a nationwide time-stratified case-crossover study from 2015 to 2020. Chemosphere. (2022) 308(Pt 2):136316. doi: 10.1016/j.chemosphere.2022.136316
12. Li L, Yang J, Guo C, Chen PY, Ou CQ, Guo Y. Particulate matter modifies the magnitude and time course of the non-linear temperature-mortality association. Environ Pollut. (2015) 196:423–30. doi: 10.1016/j.envpol.2014.11.005
13. Chen K, Wolf K, Breitner S, Gasparrini A, Stafoggia M, Samoli E, et al. Two-way effect modifications of air pollution and air temperature on total natural and cardiovascular mortality in eight European urban areas. Environ Int. (2018) 116:186–96. doi: 10.1016/j.envint.2018.04.021
14. Xu J, Yao M, Wu W, Qiao X, Zhang H, Wang P, et al. Estimation of ambient PM(2.5)-related mortality burden in China by 2030 under climate and population change scenarios: a modeling study. Environ Int. (2021) 156:106733. doi: 10.1016/j.envint.2021.106733
15. Watts N, Amann M, Arnell N, Ayeb-Karlsson S, Beagley J, Belesova K, et al. The 2020 report of The Lancet Countdown on health and climate change: responding to converging crises. Lancet. (2021) 397:129–70. doi: 10.1016/s0140-6736(20)32290-x
16. Li J, Liu H, Lv Z, Zhao R, Deng F, Wang C, et al. Estimation of PM(2.5) mortality burden in China with new exposure estimation and local concentration-response function. Environ Pollut. (2018) 243(Pt B):1710–8. doi: 10.1016/j.envpol.2018.09.089
17. Chen G, Li S, Knibbs LD, Hamm NAS, Cao W, Li T, et al. A machine learning method to estimate PM(25) concentrations across China with remote sensing, meteorological and land use information. Sci Total Environ. (2018) 636:52–60. doi: 10.1016/j.scitotenv.2018.04.251
18. Chen G, Knibbs LD, Zhang W, Li S, Cao W, Guo J, et al. Estimating spatiotemporal distribution of PM(1) concentrations in China with satellite remote sensing, meteorology, and land use information. Environ Pollut. (2018) 233:1086–94. doi: 10.1016/j.envpol.2017.10.011
19. Ma C, Yang J, Nakayama SF, Iwai-Shimada M, Jung CR, Sun XL, et al. Cold spells and cause-specific mortality in 47 Japanese prefectures: a systematic evaluation. Environ Health Perspect. (2021) 129:67001. doi: 10.1289/EHP7109
20. Zhao Q, Li S, Coelho M, Saldiva PHN, Hu K, Abramson MJ, et al. Assessment of intraseasonal variation in hospitalization associated with heat exposure in Brazil. JAMA Netw Open. (2019) 2:e187901. doi: 10.1001/jamanetworkopen.2018.7901
21. Gasparrini A, Guo Y, Hashizume M, Lavigne E, Tobias A, Zanobetti A, et al. Changes in susceptibility to heat during the summer: a multicountry analysis. Am J Epidemiol. (2016) 183:1027–36. doi: 10.1093/aje/kwv260
22. Levy D, Sheppard L, Checkoway H, Kaufman J, Lumley T, Koenig J, et al. A case-crossover analysis of particulate matter air pollution and out-of-hospital primary cardiac arrest. Epidemiology. (2001) 12:193–9. doi: 10.1097/00001648-200103000-00011
23. Zhao Q, Li S, Coelho M, Saldiva PHN, Xu R, Huxley RR, et al. Ambient heat and hospitalisation for COPD in Brazil: a nationwide case-crossover study. Thorax. (2019) 74:1031–6. doi: 10.1136/thoraxjnl-2019-213486
24. Luo K, Li R, Wang Z, Zhang R, Xu Q. Effect modification of the association between temperature variability and daily cardiovascular mortality by air pollutants in three Chinese cities. Environ Pollut. (2017) 230:989–99. doi: 10.1016/j.envpol.2017.07.045
25. Li YC, Chiou JY, Lin CL, Wei JC, Yeh MH. The association between air pollution level and breast cancer risk in Taiwan. Medicine (Baltimore). (2021) 100:e25637. doi: 10.1097/MD.0000000000025637
26. Pascal M, Wagner V, Alari A, Corso M, Le Tertre A. Extreme heat and acute air pollution episodes: A need for joint public health warnings? Atmos Environ. (2021) 249:118249. doi: 10.1016/j.atmosenv.2021.118249
27. Chen S, Dong H, Li M, Huang L, Lin G, Liu Q, et al. Interactive effects between temperature and PM(2.5) on mortality: a study of varying coefficient distributed lag model - Guangzhou, Guangdong Province, China, 2013-2020. China CDC Wkly. (2022) 4:570–6. doi: 10.46234/ccdcw2022.124
28. Silveira IH, Cortes TR, Oliveira BFA, Junger WL. Temperature and cardiovascular mortality in Rio de Janeiro, Brazil: effect modification by individual-level and neighbourhood-level factors. J Epidemiol Community Health. (2021) 75:69–75. doi: 10.1136/jech-2020-215002
29. Eccles R. An explanation for the seasonality of acute upper respiratory tract viral infections. Acta Otolaryngol. (2002) 122:183–91. doi: 10.1080/00016480252814207
30. Liu C, Chen R, Sera F, Vicedo-Cabrera AM, Guo Y, Tong S, et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N Engl J Med. (2019) 381:705–15. doi: 10.1056/NEJMc1913285
31. Lin H, Tao J, Du Y, Liu T, Qian Z, Tian L, et al. Particle size and chemical constituents of ambient particulate pollution associated with cardiovascular mortality in Guangzhou, China. Environ Pollut. (2016) 208(Pt B):758–66. doi: 10.1016/j.envpol.2015.10.056
32. Wang G, Xu Y, Huang L, Wang K, Shen H, Li Z. Pollution characteristics and toxic effects of PM(10) and PM(25) in Harbin, China. Environ Sci Pollut Res Int. (2021) 28:13229–42. doi: 10.1007/s11356-020-11510-8
33. Arias-Pérez RD, Taborda NA, Gómez DM, Narvaez JF, Porras J, Hernandez JC. Inflammatory effects of particulate matter air pollution. Environ Sci Pollut Res Int. (2020) 27:42390–404. doi: 10.1007/s11356-020-10574-w
34. Filep Á, Fodor GH, Kun-Szabó F, Tiszlavicz L, Rázga Z, Bozsó G, et al. Exposure to urban PM1 in rats: development of bronchial inflammation and airway hyperresponsiveness. Respir Res. (2016) 17:26. doi: 10.1186/s12931-016-0332-9
35. Boonarkart C, Suptawiwat O, Sakorn K, Puthavathana P, Auewarakul P. Exposure to cold impairs interferon-induced antiviral defense. Arch Virol. (2017) 162:2231–7. doi: 10.1007/s00705-017-3334-0
36. He F, Liao B, Pu J, Li C, Zheng M, Huang L, et al. Exposure to ambient particulate matter induced COPD in a rat model and a description of the underlying mechanism. Sci Rep. (2017) 7:45666. doi: 10.1038/srep45666
37. Juan Y, Haiqiao W, Xie W, Huaping H, Zhong H, Xiangdong Z, et al. Cold-inducible RNA-binding protein mediates airway inflammation and mucus hypersecretion through a post-transcriptional regulatory mechanism under cold stress. Int J Biochem Cell Biol. (2016) 78:335–48. doi: 10.1016/j.biocel.2016.07.029
38. Li H, Bai H, Yang C, Chen R, Wang C, Zhao Z, et al. Acute effects of ambient temperature and particulate air pollution on fractional exhaled nitric oxide: a panel study among diabetic patients in Shanghai, China. J Epidemiol. (2017) 27:584–9. doi: 10.1016/j.je.2017.01.002
39. Liu S, Chan EYY, Goggins WB, Huang Z. The mortality risk and socioeconomic vulnerability associated with high and low temperature in Hong Kong. Int J Environ Res Public Health. (2020) 17:7326. doi: 10.3390/ijerph17197326
40. Chen R, Yin P, Meng X, Liu C, Wang L, Xu X, et al. Fine particulate air pollution and daily mortality. A nationwide analysis in 272 Chinese cities. Am J Respir Crit Care Med. (2017) 196:73–81. doi: 10.1164/rccm.201609-1862OC
41. Ethan CJ, Mokoena KK, Yu Y, Shale K, Fan Y, Rong J, et al. Association between PM(25) and mortality of stomach and colorectal cancer in Xi'an: a time-series study. Environ Sci Pollut Res Int. (2020) 27:22353–63. doi: 10.1007/s11356-020-08628-0
42. Bandyopadhayaya S, Ford B, Mandal CC. Cold-hearted: A case for cold stress in cancer risk. J Therm Biol. (2020) 91:102608. doi: 10.1016/j.jtherbio.2020.102608
43. Sharma A, Verma HK, Joshi S, Panwar MS, Mandal CC. A link between cold environment and cancer. Tumour Biol. (2015) 36:5953–64. doi: 10.1007/s13277-015-3270-0
44. Sharma A, Sharma T, Panwar MS, Sharma D, Bundel R, Hamilton RT, et al. Colder environments are associated with a greater cancer incidence in the female population of the United States. Tumour Biol. (2017) 39:1010428317724784. doi: 10.1177/1010428317724784
45. Wang L, Liu T, Hu M, Zeng W, Zhang Y, Rutherford S, et al. The impact of cold spells on mortality and effect modification by cold spell characteristics. Sci Rep. (2016) 6:38380. doi: 10.1038/srep38380
46. Chen J, Yang J, Zhou M, Yin P, Wang B, Liu J, et al. Cold spell and mortality in 31 Chinese capital cities: definitions, vulnerability and implications. Environ Int. (2019) 128:271–8. doi: 10.1016/j.envint.2019.04.049
47. Yang Z, Yang J, Zhou M, Yin P, Chen Z, Zhao Q, et al. Hourly temperature variability and mortality in 31 major Chinese cities: Effect modification by individual characteristics, season and temperature zone. Environ Int. (2021) 156:106746. doi: 10.1016/j.envint.2021.106746
48. Kan H, London SJ, Chen G, Zhang Y, Song G, Zhao N, et al. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environ Health Perspect. (2008) 116:1183–8. doi: 10.1289/ehp.10851
Keywords: particulate matter, ambient cold, modification effect, mortality, air pollution
Citation: Zhao Z, Chu J, Xu X, Cao Y, Schikowski T, Geng M, Chen G, Bai G, Hu K, Xia J, Ma W, Liu Q, Lu Z, Guo X and Zhao Q (2023) Association between ambient cold exposure and mortality risk in Shandong Province, China: Modification effect of particulate matter size. Front. Public Health 10:1093588. doi: 10.3389/fpubh.2022.1093588
Received: 09 November 2022; Accepted: 06 December 2022;
Published: 05 January 2023.
Edited by:
Shengzhi Sun, Boston University, United StatesReviewed by:
Jun Yang, Guangzhou Medical University, ChinaJian Cheng, Anhui Medical University, China
Copyright © 2023 Zhao, Chu, Xu, Cao, Schikowski, Geng, Chen, Bai, Hu, Xia, Ma, Liu, Lu, Guo and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qi Zhao,  cWkuemhhb0BzZHUuZWR1LmNu; Xiaolei Guo, Z3VveGlhb2xlaUAxMjYuY29t
cWkuemhhb0BzZHUuZWR1LmNu; Xiaolei Guo, Z3VveGlhb2xlaUAxMjYuY29t