 Tewodros Yosef
Tewodros Yosef Enawgaw Sineshaw2
Enawgaw Sineshaw2 Nigusie Shifera
Nigusie Shifera
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 11 January 2023
Sec. Occupational Health and Safety
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1060755
This article is part of the Research TopicInsights in Occupational Health and Safety: 2022View all 16 articles
Background: Construction business is currently the second greatest source of injuries in Ethiopia after automotive accidents, with a risk of fatality that is five times higher than that of other industrial sectors. To establish measures for injury prevention, it is crucial to assess the severity of occupational injuries and identify the variables that contribute to them. Therefore, this study aimed to assess the magnitude and factors associated with occupational injuries among Bure Industrial Park construction workers, Northwest Ethiopia.
Methods: An institutional-based cross-sectional study was conducted among 372 construction workers at Bure Industrial Park. The study participants were selected using a simple random sampling method. The data were collected using interviewer-administered structured questionnaire and work environment observation using structured checklist. In the descriptive statistic, frequencies, proportion, and mean were calculated and the results of the analysis were presented in text and tables. The bi-variable and multivariable logistic regression analyses were carried out to identify independent factors having associations with the occurrence of occupational injury.
Results: The overall prevalence of occupational injuries among Bure industrial park construction workers was 39.4%, 95%C.I (34.4%-44.4%). Factors such as sex (being male) [AOR = 1.74, 95%CI (1.02–2.97)], being married [AOR = 2.79, 95%CI (1.50–5.17)], no use of personal protective equipment [AOR = 1.67, 95%CI (1.12–2.85)], no training on occupational safety [AOR = 1.45, 95%CI (1.06–2.98)], and not satisfied with the job [AOR = 5.97, 95%CI (3.48–10.2)] were the factors associated with occupational injuries.
Conclusion and recommendation: The finding shows the public health importance of occupational injury among construction workers in the study area. Numerous factors have been linked to workplace injuries, including sex, marital status, the usage of personal protection equipment, training in occupational safety, and job satisfaction. As a result, in order to lower the rate of occupational injury, employers should prioritize offering safety training, encouraging the use of personal protective equipment while working, conducting routine workplace inspections, and ensuring that their staff members are happy at work by providing comfortable workspaces.
Any accidental physical hurt or harm to body tissue resulting from work exposure is referred to as an occupational injury (1). The construction sector is home to about a quarter of all work-related fatalities, in addition to a large number of other injuries (2). Safety in the workplace is described as preventing incidents that could cause bodily harm to people (3, 4). Safety on construction sites lowers the danger of work-related accidents and injuries as well as harm to the general public (2).
Worldwide, hundreds of millions of individuals are working in unsafe circumstances (5). In both industrialized and developing countries, work injuries have been identified as one of the most important factors that contribute to poor health and life-threatening illnesses (6). Globally, there are approximately 270 million occupational injuries and two million fatalities per year in all productive sectors (6, 7). Occupational illnesses or accidents claim the lives of 6,300 people per day (8). Annually, 55,000 fatal injuries are caused by the construction sector (9). According to estimates, occupational accidents cost the global economy 4% of its GDP (USD 1.25 trillion) (10, 11). The annual projected direct and indirect costs of fatal and nonfatal construction injury are above $10 billion USD (12).
Construction industry is one of the riskiest and most accident-prone industries (6, 13). People working on construction sites are more likely to suffer traumatic injuries, illnesses, and fatalities than people in other occupations in both developed and developing countries (12, 14–16). Compared to manufacturing industry, peoples working in construction have 2.5 and 5 times higher risk of serious injury and death respectively (17).
Construction workers in poor countries experience occupational health and safety risks that are between 10 and 20 times more severe than those in industrialized countries (18). Construction workers have greater occupational health and safety injuries in developing countries than in developed ones; this is more common in Sub-Saharan Africa. This could be because there are less laws and regulations governing workplace health and safety (19).
The magnitude of work injuries among construction employees in Egypt was reported to be 46.2% (20), 74% in Kenya (21), and the magnitude range from 38.3 and 84.7% in Ethiopia (10, 22). Although unsafe work environments are frequently the cause of workplace injuries, other factors are also mentioned as contributing to occupational injuries, including sex, age, workload, lack of safety training, job stress, the absence of safety signs, sleep issues, alcohol consumption, cigarette smoking, chewing khat, and poor exercise habits (10, 13, 21–23).
Construction business is currently the second greatest source of injuries in Ethiopia after automotive accidents, with a risk of fatality that is five times higher than that of other industrial sectors (7). Although evidence-based work health and safety services are essential, studies showing the prevalence and factors of occupational injuries in the Construction Park are scarce in Ethiopia, particularly no study conducted in the study area so far. Accident prevention starts with having a firm awareness of the contributing factors because accident causalities in the construction sector are complicated and multidimensional (24). To establish measures for injury prevention, it is crucial to assess the severity of occupational injuries and identify the variables that contribute to them. Therefore, this study aimed to assess the magnitude and factors associated with occupational injuries among Bure Industrial Park construction workers, Northwest Ethiopia.
An institutional-based cross-sectional study was in Bure industrial park construction workers from January to February 2022. Bure town administration Industry Park is found in the Amhara region, 411 km Northwest of Addis Ababa, the capital city of Ethiopia. The park has created job opportunities for thousands of people in the area. The number of workers fluctuates from time to time from a minimum of 1,500 to a maximum of 2,000. These construction projects cover range of activities such as site clearance, the demolition or dismantling of building structures or plants and equipment, excavations, reinforcement-bar works, concrete works, HCB (Hollow Concrete block) other material fabrication, decoration, cleaning, installation, and the removal and maintenance of services (electricity, water, and telecommunications). It also includes the use of woodworking, painting, and decorating and the use of heavy machinery for site landscaping.
All Bure industry park workers were the source population. The study populations were all randomly selected Bure industry park, construction workers. All Bure industrial park construction workers were eligible and included regardless of their job categories whether they working as daily labor, plasterer, carpenter, mason, welder/electrician, painter, driver/operator, and office/site engineers under construction Enterprise. Construction workers who were unable to respond due to illness and workers with hearing or speaking difficulties were excluded.
The sample size was calculated using a single population proportion formula by assuming 32.6% the prevalence rate of occupational injuries among construction workers in Dessie town (11), with a 95% confidence level, 5% desired precision, and adding 10% for non-response rate, the total calculated sample size was 372. First, a list of building construction works with their respective job category was obtained from Bure Industrial park administration. Then, a simple random sampling technique was employed to select the study participants. If the selected participant is not available at the time of data collection, the next participant was considered.
The presence of occupational injuries among construction workers was the outcome variable. The independent variables were socio-demographic and economic factors (age, residence, marital status, economic status, educational level, medical condition, pattern of employment, salary), occupational factors (working section/job category, total work hours/day, availability of safe tools, availability safe machinery, occupational safety training, availability PPE (personal protective equipment's) and behavioral factors (use of PPE (personal protective equipment's), job satisfaction, sleeping disturbance problem, usage of substances).
Occupational injuries are any physical injuries sustained by a worker in connection with the performance of his or her work (25). Personal Protective Equipment (PPE) was defined as specialized clothing or equipment worn by employees for protection against health and safety hazards. Workers were classified as those who used PPE when they responded to use PPE that was necessary to be worn during a particular activity (10). Substance use was defined as a person who used at least one of the following substances such as cigarette, khat and alcohol in the past 30 days (26).
The data were collected using a pretested structured questionnaire, which was developed after reviewing relevant literature (11, 14). After preparing the English version it was translated first into Amharic and then back to English to keep its consistency. The local language Amharic was used to collect the data. A face-to-face interview was used to collect the data. The questionnaire was composed of the following variables; socio-demographic and economic factors (age, residence, marital status, economic status, educational level, medical condition, pattern of employment, and salary), occupational factors (working section/job category, total work hours/day, availability of safe tools, availability safe machinery, occupational safety training, availability PPE (personal protective equipment's), behavioral factors [use of PPE (personal protective equipment's), job satisfaction, sleeping disturbance problem, usage of substances], and occupational injury-related variables (the occurrence of injuries, and their types, time of injury happen and causes of injury). The outcome variable was occupational injury. It was measured by asking respondents a question stated as, “Have you encountered any injuries in the past 12 months?” Responses that were “yes” were coded as “1” while responses that were “no” were categorized as “0”. In addition to participant self-reports, we confirm the existence and type of injury by looking at the respondent's damaged body part. The health center record also used to confirm such injuries which are documented when an individual's sustain injury and visit for treatment. The availability and use of personal protective equipment (PPE) as well as different workplace hazards (such as whether respondents worked with machines or not and whether they worked in an environment that made them vulnerable to injury) were also determined using a work environment observation checklist. The questionnaire's face validity was examined by professionals in occupational health. In terms of instrument reliability, a test of reliability was conducted on the questionnaire status, and a satisfactory reliability status was obtained (in this study, a Cronbach's alpha of 0.79 was obtained). A pretest of the tool was conducted on 5% of the sample size (not actually part of the study, but had similar characteristics) among construction workers in Finote Selam town before the actual data collection commenced and necessary correction was done. The data collection was done by three BSc nurses, who had previous experience in data collection. The overall data collection process was supervised by two BSc public health officers. Two days of training was given for data collectors along with their supervisors about the questionnaire and data collection procedures.
The data were coded and entered into Epi Data version 3.1 and then exported to SPSS version 20 for statistical analysis. In the descriptive statistic, frequencies, proportion, and mean were calculated and the results of the analysis were presented in text and tables. Binary logistic regression analysis was carried out to assess the association of different independent variables with the dependent variable. Independent variables having P < 0.25 on the binary logistic regression analysis were considered as candidates for the final multivariable logistic regression analysis. The level of significance was declared at a p < 0.05.
Ethical approval was obtained from Mizan-Tepi University Ethical Review Committee. Confidentiality and privacy were maintained; only the ID number was used during data collection, analysis, and reporting in which the information obtained from the respondents will not be shared with anyone other than the data collectors and principal investigator. The data collectors provide health education related to occupational injuries to study participants a long side of the data collection process. Taking the current COVID-19 pandemic into account, preventive measures such as the use of personal protective materials and physical distancing were applied during the data collection. First aid kit and other necessary materials were prepared in advance to provide first aid service for the participants if occupation accidents occur at the time of data collection. Written informed consent was obtained from participants who participated in the study.
Of the 377 total sample size, 368 study participants have completed the interview, giving a response rate of 97.6%. The mean age of the participants was 27.2 (±8.4 SD) ranging from 16 to 47 years old. Almost all of the respondents, 348 (94.5%) and 348 (94.8) were orthodox religion followers and Amhara by ethnicity respectively (Table 1). The mean monthly salary of the participants was 3,444 (±1,449 SD) ranging from 1,800 to 6,000 Ethiopian birr.
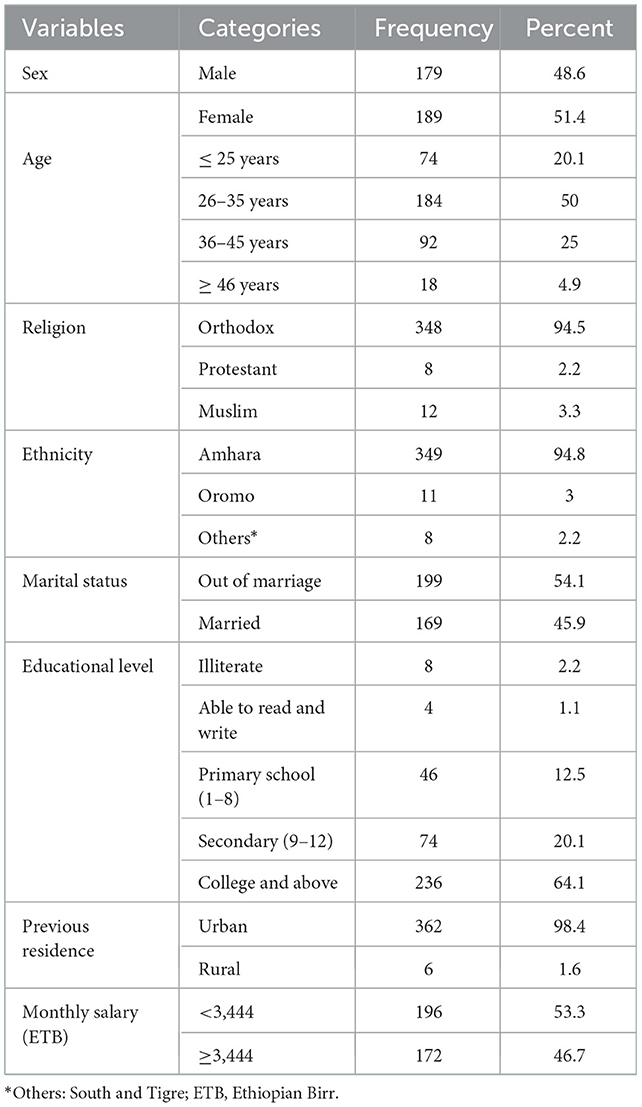
Table 1. Socio-demographic characteristics of the Bure industry park construction workersin Northwest Ethiopia.
Of the 368 study participants, 41.8% were daily laborers, followed by 29.9% masons and 9.8 carpenters (Figure 1). The commonest type of injury mentioned was laceration (42%) followed by 23.5%. One hundred seventy-six (47.8%) used personal protective equipment (Table 2). The overall prevalence of occupational injuries among workers of Bure industrial park was 39.4%, 95% C.I (34.4–44.4%).
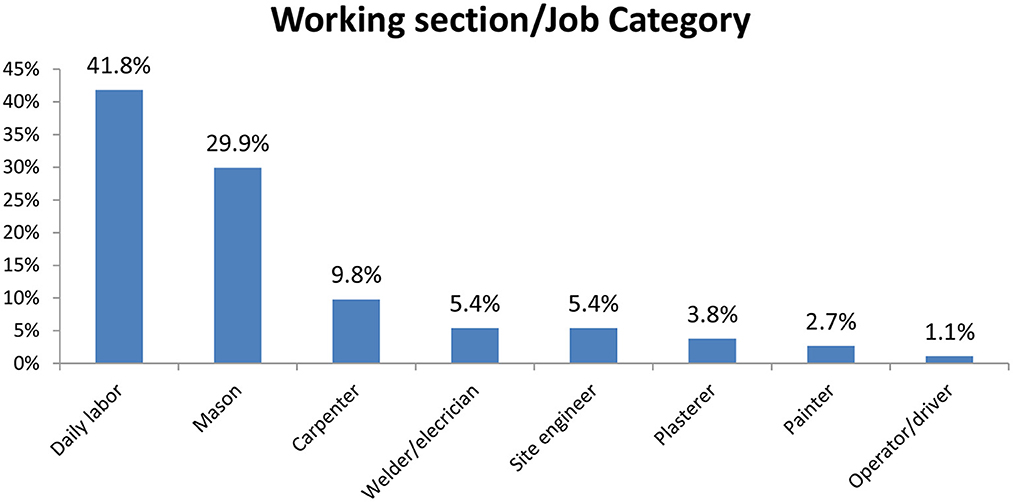
Figure 1. The working section/job category of the Bure industry park construction workers in Northwest Ethiopia.
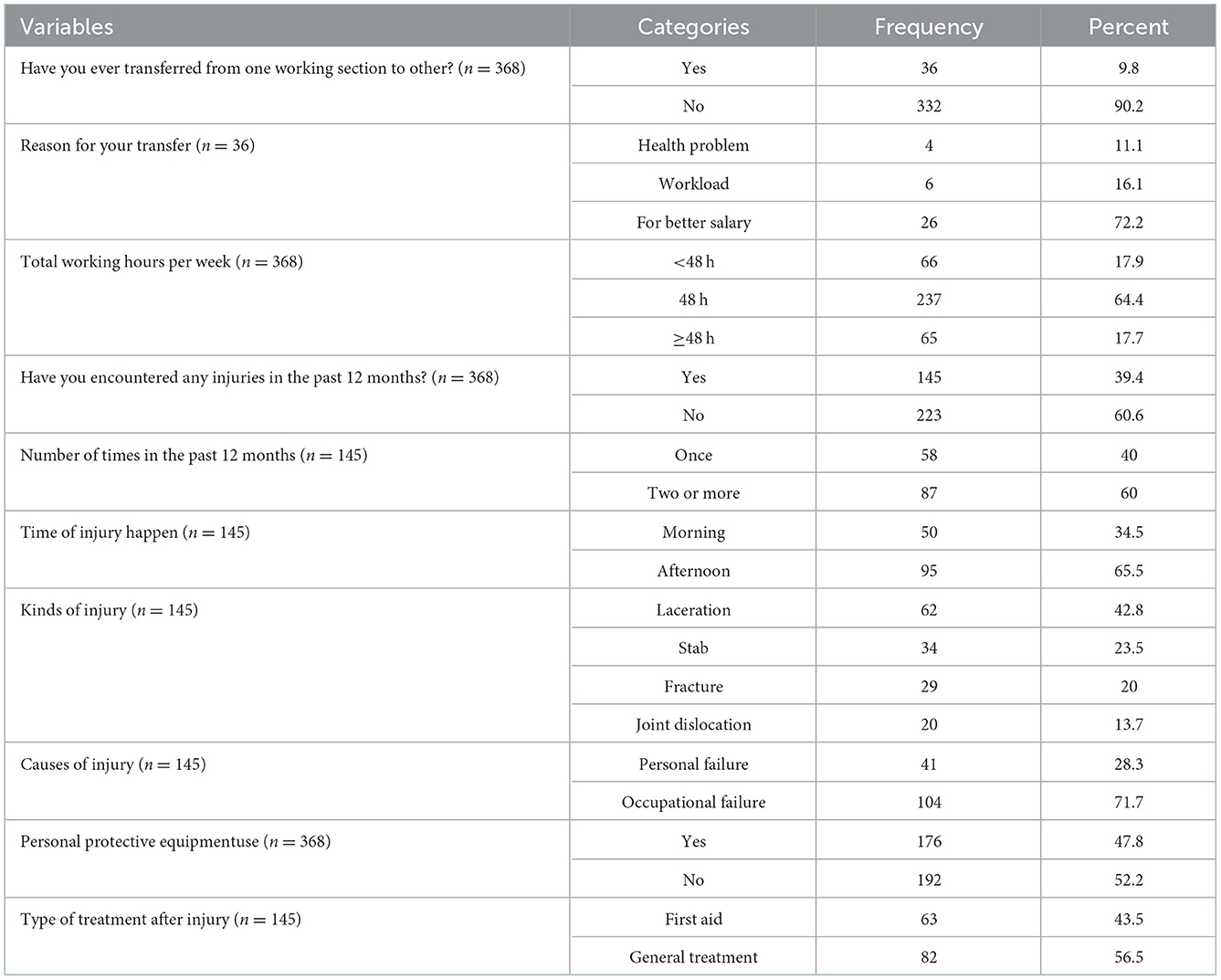
Table 2. Description of the occupational injury-related characteristics among Bure industry park construction workers in Northwest Ethiopia.
Fifty-four (14.7%) of the participants had occupational safety training at work. More than three-fourths (80.4%) of the participants had regular workplace supervision. Slightly above half (47.8%) and 36 (9.8%) of the participants were alcohol drinkers and had sleep disturbance, respectively (Table 3).
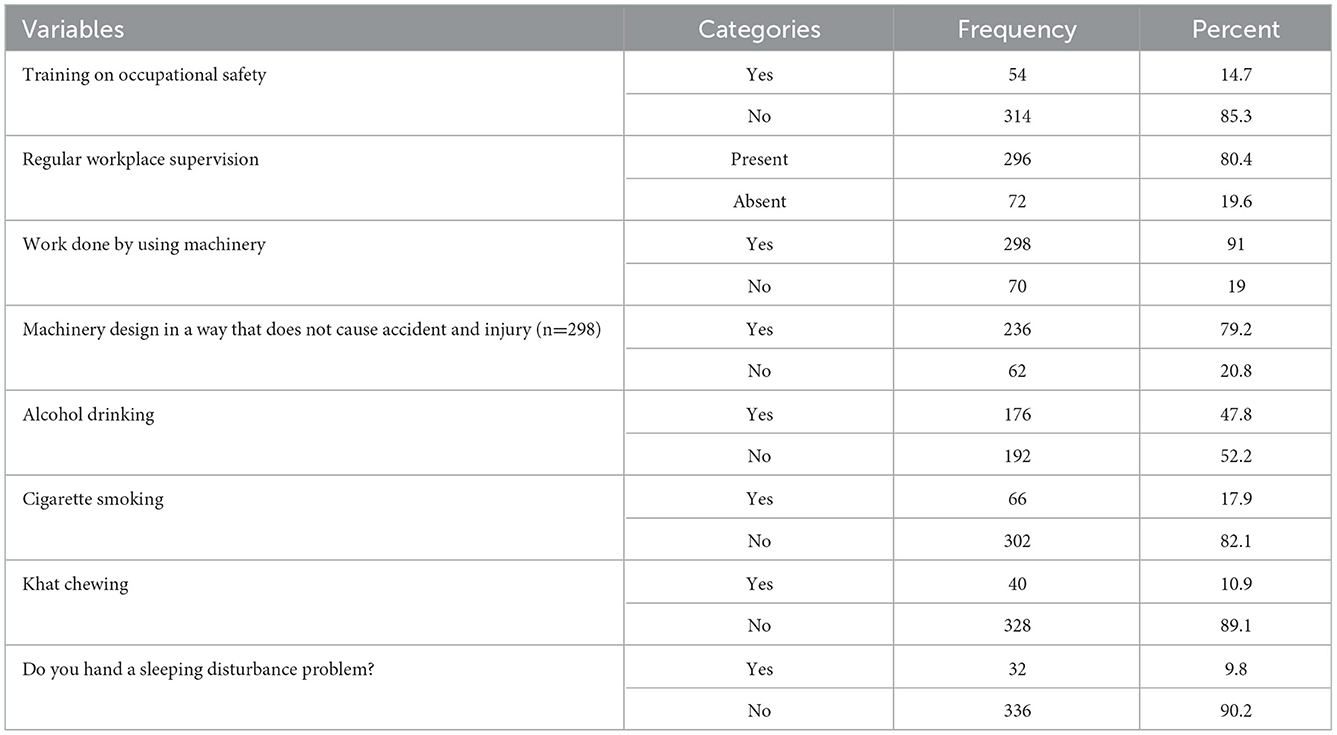
Table 3. Common occupational and behavioral factors of injuries among Bure industry park construction workers in Northwest Ethiopia.
After reviewing the records, 112 (30.4%) of the respondents visited the health center for treatment after sustained injury. Of 112 participants visited health center, the majority, 35 (31.3%) for laceration followed by 34 (30.4%), 29 (25.9%) and 14 (12.5%) were for stab, fracture and dislocation injuries respectively. Despite not being full, all participants had at least one PPE. One hundred seventy-six (47.8%) of the participants used personal protective equipment at work (Table 2). Two hundred ninety-eight (91%) of the participants were work with machineries. Of those who work with machineries, 62 (20.8%) were work under risky machineries (Table 3).
After A multi variable logistic regression four variables namely; sex (being male) [AOR = 1.74, 95%CI (1.02–2.97)] being married [AOR = 2.79, 95%CI (1.50–5.17)], no use of personal protective equipment [AOR = 1.67, 95%CI (1.12–2.85)], no training on occupational safety [AOR = 1.45, 95%CI (1.06–2.98)], and not satisfied with the job [AOR = 5.97, 95%CI (3.48–10.2)] were the factors associated with occupational injury (Table 4).
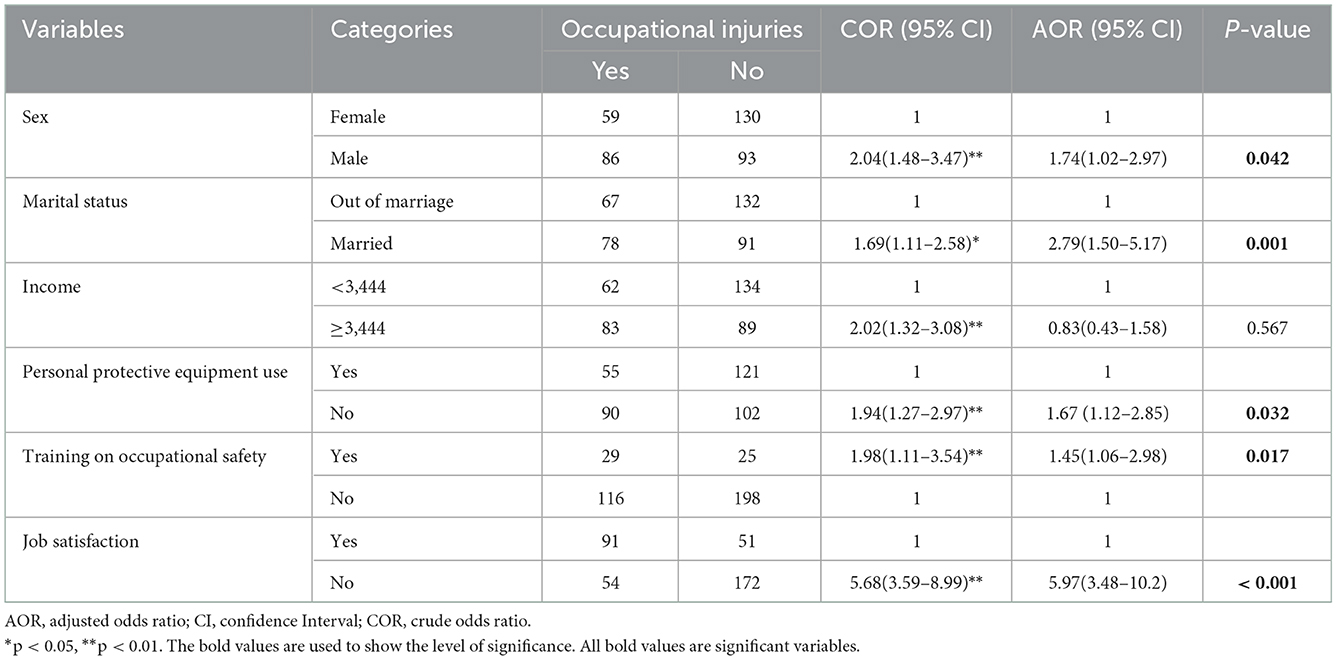
Table 4. Factors associated with occupational injuries among Bure industry park construction workers in Northwest Ethiopia (n = 368).
Construction business is one of the most dangerous workplaces (15). It is currently the second greatest source of injuries in Ethiopia after automotive accidents, with a risk of fatality that is five times higher than that of other industrial sectors (7). Although evidence-based work health and safety services are essential, studies showing the prevalence and factors of occupational injuries in the Construction Park are scarce in Ethiopia, particularly no study conducted in the study area so far. Therefore, this study aimed to assess the magnitude and factors associated with occupational injuries among Bure Industrial Park construction workers in Northwest Ethiopia.
The prevalence of occupational injury in the last year among Bure industry park construction workers was 39.4%, 95% C.I (34.4–44.4%). The prevalence stated above was consistent with 39% in Gonder (15), 39.2% in Robe town (27), 38.3% in Addis Ababa (10) studies in Ethiopia, and 39.3% in Nigeria (15). The result of this study is lower than 84.7 and 67.7% in Addis Ababa, Ethiopia (20, 22), 79.8% in Iran (28), and 46.2% in Egypt (20). The result of this study is also higher than 15% in Gondar, Ethiopia (29), 32.4% in Uganda (30), and 34.8% in China (31). The possible discrepancy may be due to study setting differences, working conditions, level of accident prevention strategies, and socio-cultural and regulatory factors (15). Besides, the difference in the level of regular workplace supervision, PPEs utilization, and working hours per day, as well as week, may create a considerable variation across different studies. There was also a discrepancy between the self-reported and observation of the health center records. This could be due to the participants' avoidance of seeking care for laceration by considering it as a mild. Besides, the preference and attendance of traditional healers for joint dislocation also another thing for the variation observed. The incompleteness of documentation due to the above reasons, the discrepancy between self-report and record observation was observed.
Male construction workers were more vulnerable to occupational injury than female construction workers. In this study, the risk of occupational injury was 1.74 times higher among male workers as compared to female workers. This finding was consistent with a studies conducted in Ethiopia (31–33), Ghana (34), and China (35) which reported that male workers are more prone to occupational injury than female workers. The possible explanation for this report is due to the difference in tasks and males are high in risk-taking behavior (36).
The occurrences of occupational injury among married were 2.8 times higher as compared to their counterparts. The finding of this study is supported by another similar study conducted in Gonder, Ethiopia (15) and Iran (37). This may be due to married workers may more engage in works without taking adequate rest to cover a family expenses. Stress and fatigue can be higher among married workers than single ones because of higher responsibilities in life to secure family needs. It may be led to more unsafe acts resulting in an accident (32).
The odds of work-related injuries among workers who did not receive occupational safety training were 1.45 times more likely compared to those who received occupational safety training. This finding was supported by a study done in Bahirdar (1), Dessie (11), and a systematic analysis in Ethiopia (32), which reported that workers who attend safety training programs were less likely to experience work-related injuries. This might be due to training that provides knowledge about the presence of different safety hazards in construction and helps workers how to protect them. In addition, training may have an impact on changing the behaviors of workers to follow the safety precautions.
Personal protective equipment use was another factor significantly associated with the occurrence of occupational injuries. Accordingly, workers who did not engage in the work by wearing personal protective equipment were 1.67 times less likely to develop occupational injuries than those workers who did use PPE. This finding was supported by studies done in Bahrdar, Ethiopia (11), and Addis Ababa, Ethiopia (20), Uganda (30), which indicated that the use of PPE in a working environment reduces the occurrence of occupational injuries. This could be due to personal protective equipment protecting the worker against the hazards to which the worker may be exposed. Worker protection equipment (PPE) shields workers against a range of dangers, including chemical, physical, biological, electrical, mechanical, and radiological dangers (38).
Workers who had no job satisfaction were a 5.6 times higher risk of developing occupational injuries compared to their counterparts. This finding was supported by a study conducted in Addis Ababa, Ethiopia (20), and Nigeria (15). This might be because those workers who had no satisfaction with work did not comply with standard work procedures, and safety precautions including proper use of PPEs. Evidence suggests that there is a link between accidents and Job satisfaction (39). Job satisfaction can result in improved performance and a decrease in occupational accidents (40). This means that job dissatisfaction might lead to an increase unsafe acts and result in occupational accidents (41).
One-year prevalence may be underestimated or overestimated due to recall and social desirability bias although much effort was taken to minimize it. Furthermore, the study's cross-sectional design makes it difficult to demonstrate cause-and-effect linkages between the dependent and independent variables. Therefore, future studies should be consider with better study designs (cohort study) to minimize recall bias and to determine the cause-and-effect relationship between the dependent and independent variables.
The finding shows the public health importance of occupational injury among construction workers in the study area. Numerous factors have been linked to workplace injuries, including sex, marital status, the usage of personal protection equipment, training in occupational safety, and job satisfaction. As a result, in order to lower the rate of occupational injury, employers should prioritize offering safety training, encouraging the use of personal protective equipment while working, conducting routine workplace inspections, and ensuring that their staff members are happy at work by providing comfortable workspaces.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Mizan-Tepi University Ethical Review Committee. The patients/participants provided their written informed consent to participate in this study.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
First, we would like to thank all study participants for their participation. Second, our thank goes to the Bure Industry Park management bodies for providing valuable information.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hunegnaw B, Molla M, Mulugeta Y, Meseret M. Assessment of occupational injury among industrial workers in the Bahir Dar city of northwest ethiopia : institution-based cross-sectional study. J Environ Public Health. (2021) 2021:2793053. doi: 10.1155/2021/2793053
2. Ambegaonkar R. The Importance of Safety on Construction Sites. Miami, FL: NearBy Engineers (2020).
3. Huang Z, Chen W. Occupational injuries among construction workers in Hong Kong. Zhonghua Liu Xing Bing Xue Za Zhi. (2002) 23:57–9.
4. WHO/ILO. Occupational Health and safety in Africa. Meeting report. In: World Health Organization with input of WHO/ILO Joint Effort Taskforce. Geneva: WHO (2001).
5. Hämäläinen P, Takala J, Kiat TB. Global Estimates of Occupational Accidents and Work-Related Illnesses 2014. Tampere: Tampere University of Technology (2014).
6. Majori S, Bonizzato G, Signorelli D, Lacquaniti S, Andreeta L, Baldo V. Epidemiology and prevention of domestic injuries among children in the Verona area (north – east italy). Ann Ig. (2002) 14:495–502.
7. Mekkodathil A. Ei-Menyar, AI-Thani H. Occupational injuries in workers from different ethnicities. Int J Crit III Injury Sci. (2016) 6:25–32. doi: 10.4103/2229-5151.177365
8. International Labour Organization (ILO). Business, Occupational Safety and Health. Geneva: ILO (2022).
9. ElSafty A, ElSafty A MM. Construction safety and occupational health education in Egypt, the EU, and US firms. Open J Civ Eng. (2012) 2:174–82. doi: 10.4236/ojce.2012.23023
10. Tadesse S, Israel D. Occupational injuries among building construction workers in Addis Ababa, Ethiopia. J Occup MedToxicol. (2016) 11:16. doi: 10.1186/s12995-016-0107-8
11. Gebremeskel T, Yimer T. Prevalence of occupational injury and associated factors among building construction workers in Dessie town, North East Ethiopia; 2018. BMC Res Notes. (2019) 12:481. doi: 10.1186/s13104-019-4436-4
12. Gittleman JL, Gardner PC, Haile E, Sampson JM, Cigularov KP, Ermann ED, et al. [case study] City Center and cosmopolitan construction projects, Las Vegas, Nevada: lessons learned from the use of multiple sources and mixed methods in a safety needs assessment. J Saf Res. (2010) 41:263–81. doi: 10.1016/j.jsr.2010.04.004
13. Jackson SA, Loomis D. Fatal occupational injuries in the North Carolina construction industry, 1978-1994. Appl Occup Environ Hyg. (2002) 17:27–33. doi: 10.1080/104732202753306122
14. Probst TM, Brubaker TL, Barsotti A. Organizational injury rate underreporting: the moderating effect of organizational safety climate. J Appl Psychol. (2008) 93:1147–54. doi: 10.1037/0021-9010.93.5.1147
15. Berhanu F, Gebrehiwot M, Gizaw Z. Workplace injury and associated factors among construction workers in Gondar town, Northwest Ethiopia. BMC Musculoskelet Disord. (2019) 20:523. doi: 10.1186/s12891-019-2917-1
16. MoUDC (Ministry of Urban Development and Construction). Directives for the Registration of Construction Professionals and Contractors. Directive No 19. Addis Ababa: Ministry of Urban Development and Construction (2013).
17. Sawacha E, Naoum S, Fong D. Factors affecting safety performance on construction sites. Int J Project Manag. 17:309–15. doi: 10.1016/S0263-7863(98)00042-8
18. Kiwekete HM. Job safety analysis: a practical tool for ensuring safety of the workplace African Newsletter on occupational health and safety. Geneva, Switzerland: International Labour Organisation. (2008).
19. Kjestveit K, Tharaldsen J, Holte K. Young and strong: what influences injury rates within building and construction? Saf Sci Monit. (2011) 15(2):15.
20. Thewodros Bekele Tolera. occupational hazards in construction industry: case studies from housing and construction workers at Addis Ababa, Ethiopia. Int J Res -GRANTHAALAYAH. (2016) 4:84–96. doi: 10.29121/granthaalayah.v4.i9.2016.2539
21. Kemei R, Kaluli JW KC. Common construction site hazards in Nairobi County, Kenya. Am J Const Build Mater. (2017) 2:70–7. doi: 10.11648/j.ajcbm.20170101.14
22. Mersha H, Mereta ST DL. Prevalence of occupational injuries and associated factors among construction workers in Addis Ababa, Ethiopia. J Public Heal Epidemiol. (2017) 9:1–8. doi: 10.5897/JPHE2016.0883
23. Macdonald D, Sanati K, Macdonald E. The costs and characteristics of occupational injuries admitted to a trauma unit. Int J Occup Saf Ergon. (2012) 18:587–90. doi: 10.1080/10803548.2012.11076961
24. Gambatese JA, Behm M RS. Design's role in construction accident causality and prevention: perspectives from an expert panel. Saf Sci. (2008) 46:675–91. doi: 10.1016/j.ssci.2007.06.010
25. Osman Y, Kumie A. Assessment of occupational injuries in tendaho agricultural development S.C, Afar regional state Ethiopia. Ethiop J Heal Dev. (2010) 24:167–74. doi: 10.4314/ejhd.v24i3.68380
26. Yosef T, Getachew D, Bogale B, Wondimu W, Shifera N, Negesse Y, et al. Psychoactive substance use and its associated factors among truck drivers in Ethiopia. Biomed Res Int. (2021) 2021:1–7. doi: 10.1155/2021/1604245
27. Lette A, Kumbi M, Hussen A, Nuriye S. Determinants of occupational injury among building construction employees in Southeastern Ethiopia. Int J Trop Dis Heal. (2019) 34:1–11. doi: 10.9734/ijtdh/2018/v34i430103
28. Moradinazar M, Kurd N, Farhadi R, Amee V, Najafi F. Epidemiology of work-related injuries among construction workers of Ilam (Western Iran) during 2006–2009. Iran Red Crescent Med J. (2013) 15:e8011. doi: 10.5812/ircmj.8011
29. Tadesse T, Kumie A. Prevalence and factors affecting work-related injury among workers engaged in Small and Medium-Scale Industries in Gondar wereda, north Gondar zone, Amhara Regional State, Ethiopia. EthiopJHealth Dev. (2001) 21:25–34. doi: 10.4314/ejhd.v21i1.10028
30. Kiconco A, Ruhinda N, Kyobutungi V, Watya S, Bazeyo W. Determinants of occupational injuries among building construction workers in Kampala City, Uganda. Ann Glob Heal. (2017) 83:86. doi: 10.1016/j.aogh.2017.03.189
31. Zheng L, Xiang H, Song XZ. Nonfatal unintentional injuries and related factors among male construction workers in central China. Am J Ind Med. (2010) 52–4. doi: 10.1002/ajim.20833
32. Ashuro Z, Zele YT, Kabthymer RH, Diriba K, Tesfaw A, Alamneh AA. Prevalence of work-related injury and its determinants among construction workers in ethiopia : a systematic review and meta-analysis. J Environ Public Health. (2021) 2021:1–7. doi: 10.1155/2021/9954084
33. Tesfaw A, Eshetu M, Teshome F, Fenta E, Gelaw M, Mihret G, et al. Prevalence of head injury among trauma patients at debre tabor comprehensive specialized hospital, North Central Ethiopia. Open Access Surg. (2021) 14:47–54. doi: 10.2147/OAS.S321404
34. Amissah J, Badu E, Baffour PA, Nakua EK, Mensah I. Predisposing factors influencing occupational injury among frontline building construction workers in Ghana. BMC Res Notes. (2019) 8–15. doi: 10.21203/rs.2.13542/v1
35. Shalaw FA, Hamedon TR. Proportion of work-related injuries and its characteristics among the staff of a public university in Malaysia. Int J Public Heal Clin Sci. (2016) 3:69–82. doi: 10.9790/0853-15136977
36. Chou P, Huang S, Chung R, Huang Y, Chung C. Gender differences in the epidemiological characteristics and long-term trends of injuries in taiwan from 1998 to 2015 : a cross-sectional study. Int J Environ Res Public Health. (2022) 19:2531. doi: 10.3390/ijerph19052531
37. Alizadeh SS, Mortazavi SB, Sepehri MM. Analysis of occupational accident fatalities and injuries among male group in Iran between 2008 and 2012. Iran Red Crescent Med J. (2015) 17:e18976. doi: 10.5812/ircmj.18976
38. What hazards do PPE protect from? Creative Safety Supply. (2022). Available online at: https://www.creativesafetysupply.com/qa/ppe/hazards-ppe-protects-from (accessed December 5, 2022)
39. Simpson SA, Wadsworth EJK, Moss SC, Smith AP. Minor injuries, cognitive failures and accidents at work : incidence and associated features. Occup Med (Chic Ill). (2005) 55:99–108. doi: 10.1093/occmed/kqi035
40. Jahani F, Mosavian Asl Z, Kouhnavard B, Shamsaddini S. Association between Job satisfaction and occupational accidents among operating staff at a cement factory, 2018. J Occup Heal Epidemiol. (2020) 9:189–93. doi: 10.29252/johe.9.3.189
Keywords: occupational injuries, construction workers, Bure, Amhara region, Ethiopia
Citation: Yosef T, Sineshaw E and Shifera N (2023) Occupational injuries and contributing factors among industry park construction workers in Northwest Ethiopia. Front. Public Health 10:1060755. doi: 10.3389/fpubh.2022.1060755
Received: 03 October 2022; Accepted: 29 December 2022;
Published: 11 January 2023.
Edited by:
Luigi De Maria, University of Bari Aldo Moro, ItalyReviewed by:
Federica Caffaro, Roma Tre University, ItalyCopyright © 2023 Yosef, Sineshaw and Shifera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tewodros Yosef,  dGV3b2Ryb3N5b3NlZjQ3QG10dS5lZHUuZXQ=; Nigusie Shifera, bmlndXNpZXNoaWZlcmFAZ21haWwuY29t
dGV3b2Ryb3N5b3NlZjQ3QG10dS5lZHUuZXQ=; Nigusie Shifera, bmlndXNpZXNoaWZlcmFAZ21haWwuY29t
†ORCID: Tewodros Yosef orcid.org/0000-0002-3173-6753
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.