 Eleanor L. S. Leavens1,2*
Eleanor L. S. Leavens1,2* Jordan Roberts3
Jordan Roberts3 Babalola Faseru1,2,3Mark Thompson4
Babalola Faseru1,2,3Mark Thompson4 Karin Denes-Collar5
Karin Denes-Collar5 Hina Shah6
Hina Shah6- 1Department of Population Health, School of Medicine, University of Kansas, Kansas City, KS, United States
- 2University of Kansas Cancer Center, Kansas City, KS, United States
- 3Kansas Department of Health and Environment, Topeka, KS, United States
- 4Kansas State Department of Education, Topeka, KS, United States
- 5Masonic Cancer Alliance, The University of Kansas Cancer Center, Kansas City, KS, United States
- 6Kansas Health Institute, Topeka, KS, United States
Introduction: Schools remain at the frontlines of addressing issues, such as e-cigarette use, that impact students. Despite e-cigarette use remaining a significant public health concern in the U.S., schools have limited resources (e.g., staff, capacity, programming) to address it, especially in rural and frontier areas. This ECHO Pilot Project aimed to build capacity and equip schools and school staff in the state of Kansas to address high rates of youth e-cigarette use by providing prevention support and information on best practices for e-cigarette cessation.
Methods and analysis: The pilot used the established Project ECHO model to disseminate evidence-based strategies for e-cigarette prevention and cessation among youth to schools across Kansas. The pilot selected 20 interdisciplinary school teams representing both rural and urban middle and high schools across the state to participate in seven ECHO sessions. ECHO sessions proceeded throughout Fall 2021, with the final session in Spring 2022. School participants completed pre-post surveys as well as component-specific surveys following each ECHO session. In addition, each school team created an individualized action plan to comprehensively address e-cigarette use at their school based on the information provided throughout the ECHO. Survey data, school tobacco/nicotine policies, and action plans will be analyzed to assess process and final outcomes.
Discussion: If successful, this pilot will demonstrate that the ECHO model is an effective platform for building school staff knowledge and skills to implement evidence-based strategies in both urban and rural settings. It is anticipated that the pilot will build capacity and equip schools and school staff to address high rates of youth e-cigarette use by providing support for school-based prevention programs and referrals for e-cigarette cessation which will lessen the burden of nicotine-related problems in Kansas schools and communities. Finally, the pilot will provide evidence that the ECHO model can be successfully and equitably applied in a school setting and may be a viable method for addressing other public health-related issues faced by schools.
Introduction
Electronic cigarettes (e-cigarettes) are battery-powered devices that heat and aerosolize nicotine-containing liquid which is inhaled and delivered to the user. While e-cigarettes are likely less harmful than combustible cigarettes (1), they are not without risk (2), particularly for youth and individuals that are otherwise naïve to tobacco (3, 4). For this reason, use of e-cigarettes among youth remains a significant public health concern. National data suggest that approximately 11% of high school students and 3% of middle school students report current (past 30-day) e-cigarette use (5) and in 2019, nearly a quarter (22.0%) of Kansas high school students reported current e-cigarette use (6). While overall use rates are plateauing or decreasing nationally, current users report more frequent use. Specifically, national surveys suggest that approximately 39% of high school and middle school e-cigarette users report e-cigarette use on at least 20 of the past 30 days (5), likely resulting in significant levels of nicotine dependence.
Schools play a critical role in promoting student health and are uniquely positioned to implement evidence-based tobacco prevention and cessation support for students. Evidence suggests that school-based prevention programs created to address youth tobacco use have proven to be effective in reducing initiation in the short term, and in some cases, achieve longer term cessation outcomes when programs implement sustainable policy, systems, and environmental changes (7). However, few comprehensive programs or resources are available to schools to implement such programs and address e-cigarette use, particularly in rural and frontier areas. For this reason, schools largely address e-cigarette use in a similar manner to other disciplinary issues. A study conducted by the Public Health Law Center that examined Kansas school disciplinary policies for e-cigarette use found that over 75% of middle and high schools used suspension at a first tobacco/nicotine offense while less than a quarter included offers of tobacco education or cessation support at a first offense (8). Unfortunately, discipline or even education alone have not been shown to be efficacious in achieving cessation (9). In fact, studies show that students who are suspended even once, are 44% less likely to graduate and almost 50% less likely to go on to college, highlighting the importance of implementing restorative practices in schools (10).
Nearly half (45.8%) of Kansas middle and high school students who currently use tobacco products tried to quit in the past year (6) and national data suggest that approximately 4% of youth e-cigarette users have experienced an unsuccessful quit attempt (11), supporting the need for comprehensive cessation support in schools. By equipping school staff with best practice information on prevention and intervention of e-cigarette use, students will have the support and resources necessary to increase the likelihood of cessation. However, because youth e-cigarette use is an emerging public health concern, there is limited data and best-practice recommendations specific to these products. Tobacco control programs that include a range of complementary and coordinated strategies such as school-based tobacco prevention programs can reduce prevalence of tobacco use among school-aged youth.
The Extension for Community Healthcare Outcomes (ECHO) Project is a model for global dissemination of expert-level education to medical providers and patients (12, 13). In recent years, and with COVID-19 as a catalyst, the ECHO model has been used to broadly disseminate information to educators and school personnel. The current pilot initiative aimed to build capacity and equip schools and school staff to address high rates of youth e-cigarette use by providing support for school-based prevention programs and referrals for e-cigarette cessation.
The goal of this pilot program was to apply the Whole School, Whole Community, Whole Child Model (WSCC) (14) and use a collaborative blended learning approach to equip critical personnel with e-cigarette cessation resources, tools, and techniques. The WSCC model is a student-centered framework developed by the Centers for Disease Control and Prevention for addressing health in schools, which calls for greater alignment between the public health and education sectors and emphasizes the importance of evidence-based school policies and practices. The WSCC model emphasizes the importance of building a network of community support around schools and youth to improve student health. The Kansas State Department of Education (KSDE) has applied the WSCC model to several initiatives to improve student learning and health, including work undertaken by Child Nutrition and Wellness, Social-Emotional Learning, and Health and Physical Education curriculum guidance, among others. This model and resulting work was consistent with KSDE's vision, “Kansas leads the world in the success of each student.” As a pioneer in the field, the pilot program aims: (1) To develop a network of stakeholders to help design, tailor, implement and evaluate strategies and interventions to reduce vaping in schools. (2) To build capacity to increase the confidence of schools and school personnel to address e-cigarette cessation. (3) To develop skills of school health professionals to provide support and referrals for e-cigarette cessation. (4) To evaluate the quality, effectiveness, and impact of the program within Kansas schools.
Methods
Pilot program description
The pilot program was a fully online experience. The pilot program included four structured learning components: (1) a summit to kick off the program, understand the issue, and share experiences; (2) a toolkit to develop and strengthen participants' knowledge and skills and provide resources for implementation in a school setting; (3) a specialized training experience based on the tele-mentoring approach of Project ECHO focused on implementing tobacco and nicotine prevention and cessation practices in middle and high schools in Kansas and (4) an action plan developed by each team to address e-cigarette use in their school.
Partners
The pilot leveraged longstanding relationships with Kansas State Department of Education, the Kansas Department of Health and Environment, the University of Kansas Medical Center, the University of Kansas Cancer Center, Children's Mercy Kansas City, the Kansas Health Institute, Kansas Association of School Boards, Kansas Nursing Association, DCCCA, Kansas Attorney General's office, and youth programs such as Kansas RESIST, and other stakeholders to reduce e-cigarette use in middle and high schools.
Target audience
School teams included up to five members and were comprised of teachers, school nurses, counselors, social workers, athletic trainers, health teachers, coaches, administrators, and student resource officers. This target audience was selected because of their role in the school and their potential influence among students.
Recruitment and application
The ECHO hub team elicited applications from middle and high schools statewide with the goal of selecting 20 schools with two representing each of the 10 Kansas State Board of Education (KBOE) members' districts and a total of approximately 100 participants. A total of 49 schools submitted completed applications to participate in the pilot. Not all the KBOE districts were represented by the applicants, though the applicants did represent a geographical spread throughout the state.
Selection criteria
Selection criteria were designed to enroll schools and school teams that were representative of Kansas students. Specific criteria included diversity of geography between schools, rural/urban setting, socioeconomic status (SES; percent free and reduced lunch), and racial and ethnic make-up of the student body. In addition, pilot school applicants were evaluated on their motivation to impact student e-cigarette use as evidenced by previous efforts taken toward e-cigarette prevention and/or intervention. Applicants were also asked to assure their willingness to fully participate in the Project ECHO sessions. This assurance was listed as a pre-requisite for applying. Further, applicants were asked to show evidence of a group of stakeholders who would form a comprehensive team that, at a minimum, included a school health champion (e.g., school nurse, counselor) and a school administrator. To accomplish this, the application included a requirement that schools list their team members and their role. The application is included in the Supplementary Figure 1.
Selected schools
A total of 20 interdisciplinary school teams were selected, representing 21 schools. One team consisted of staff, including administrators, from two high schools in the same town. Of the 20 school teams, four were classified as urban, four were semi-urban, five densely settled rural, four rural, and three frontier. Eleven were high schools, five were junior/senior high schools, and four were middle schools. In terms of district size classification (1A being the smallest and 6A being the largest), two were 1A, four were 2A, four were 3A, two were 4A, five were 5A, and four were 6A.
Deliverables
School teams were required to submit an individualized action plan at the end of the ECHO. Schools were instructed to use a SMART (specific, measurable, achievable, realistic, timely) goal approach when creating their action plans. Under this general model, action plans included a vision, goals, objectives, accountability log, and timeline. School teams were also provided an example action plan for reference and office hours for pre-submission feedback and brainstorming with a hub team member. The action plan instructions and template are included in the Supplementary Figure 2.
Procedures
Table 1 includes an outline of specific topics covered during orientation, summit, and core ECHO sessions.
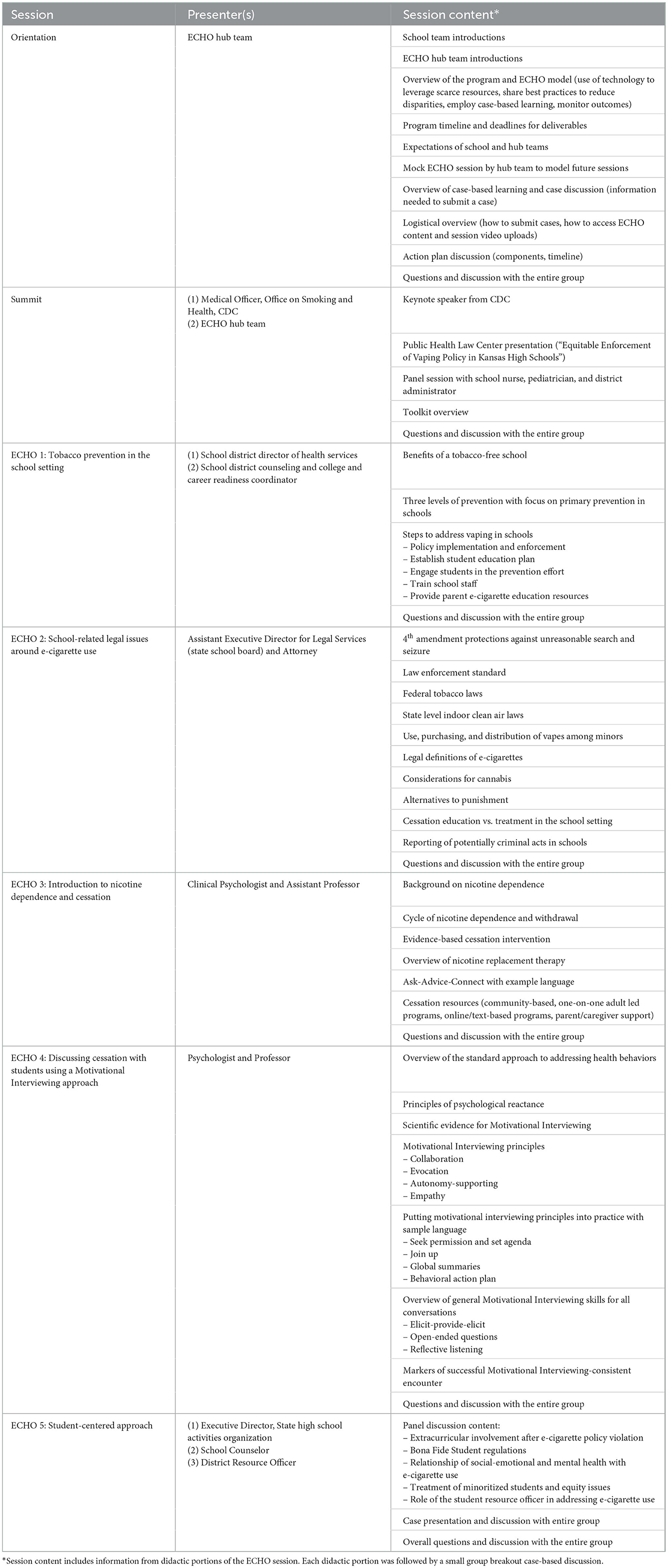
Table 1. Session overviews and content.
Orientation
Every school team member was required to attend one of two orientation sessions. The objectives of the orientation were to share (1) the uniqueness of the ECHO, (2) the importance of the ECHO, and (3) the overarching and procedural goals of the ECHO with all participants and other stakeholders. The orientation lasted 1 h and 20 min and covered the timeline and expectations (e.g., expectation for participation by all individual team members, utilization of the toolkit, and responsiveness of the ECHO hub team) for the current ECHO program, background and origin of the broad ECHO model, tailoring of the current pilot to address e-cigarette use, procedures, timeline, and expectations (e.g., ECHO sessions, deliverables, assessments). During the orientation, the hub team introduced the topics for the five core ECHO sessions and corresponding content experts. Throughout the orientation, a strong emphasis was placed on the use of case-based learning. The hub team modeled case presentation and discussion.
Summit
Each school team attended a 3-h kickoff summit that aimed to provide a basic understanding of e-cigarettes, nicotine dependence, harms of e-cigarette use among youth, an overview of available resources, current challenges experienced by schools in addressing student health issues, and legal challenges in addressing e-cigarette use in schools. In addition, the summit included a keynote address and panel discussion. During the panel, an associate superintendent, pediatrician, and school nurse discussed challenges and barriers to addressing e-cigarette use in schools and strategies for success in implementing prevention and cessation strategies.
Toolkit
A web-based toolkit housed resources for implementation of e-cigarette prevention and cessation in the school setting. Toolkit chapters corresponded directly with the core ECHO sessions and were released the week preceding the ECHO session. Toolkit chapters included a brief introduction to the topic, resources for implementation of strategies in a school setting, and an introductory video. Toolkit chapters were developed in collaboration with a team of content experts who provided recommendations for content, feedback on content, and final approval.
Core ECHO sessions
The core ECHO sessions consisted of five learning sessions with specialized training using the ECHO model and two additional sessions dedicated for sharing action plans and implementation progress. The five specialized training sessions covered (1) tobacco prevention in the school setting, (2) school-related legal issues around e-cigarette use, (3) introduction to nicotine dependence and cessation, (4) discussing cessation with students using a Motivational Interviewing approach, and (5) using a student-centered approach. Consistent with the ECHO model, each training session began with a didactic and question/answer period followed by a case presentation and discussion. Didactics were provided to the whole group and case presentations and discussions were conducted in breakout rooms with 4–5 school teams, a trained facilitator, and a content expert. School teams were grouped in breakout rooms based on geographic area due to the likelihood of access to shared resources. The breakout room groups remained consistent each session with only the content expert changing based on the topic.
Pilot evaluation
An evaluation of the pilot was designed to understand how well the program worked to achieve the intended goals, to improve its effectiveness, and to inform programming decisions. A logic model that guided program development and will guide evaluation is presented in Table 2.
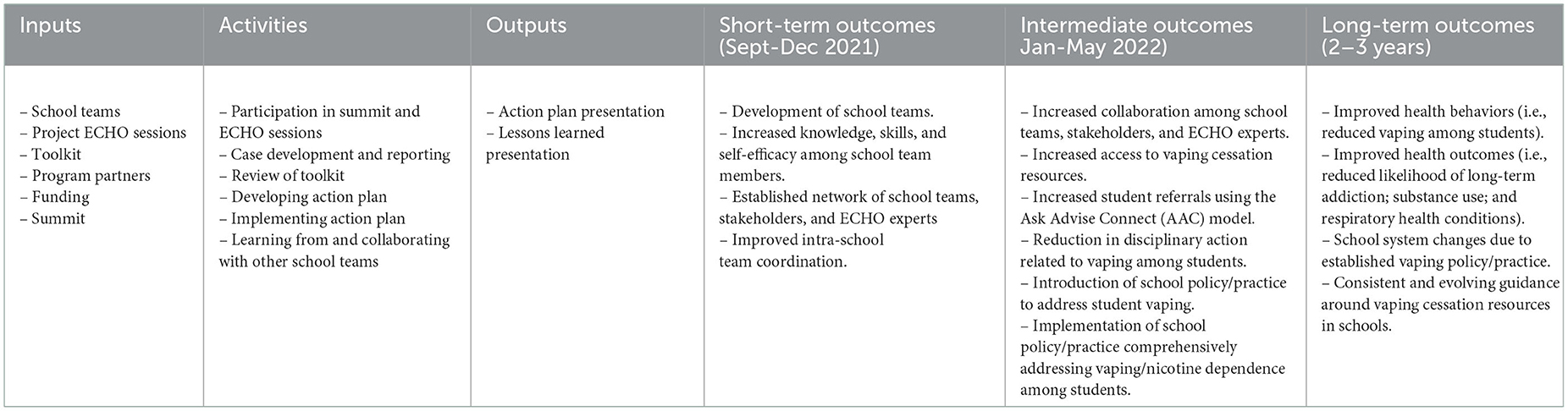
Table 2. Logic model for pilot evaluation.
The goals of the evaluation of the Vaping ECHO for Education pilot program are to:
• Assess pilot management and implementation.
• Assess level and quality of support provided to program participants by the Project ECHO team.
• Assess the extent to which the goals of the pilot program are being achieved.
• Assess how effectively school teams can develop an individualized action plan to address e-cigarette use.
The evaluation will include two components: process and outcome. The process evaluation component will assess (1) project management (how well the initiative is being managed and implemented); (2) technical assistance (the degree to which school teams have adequate support and resources to successfully implement the pilot); and (3) team-specific goals (the degree to which school teams can develop an action plan).
The outcome evaluation will assess (1) participant perceptions of capacity and skills to execute vaping cessation referrals and support for students in need; (2) the participant confidence in making policy, practice, and system changes that address e-cigarette use; and (3) school team referrals and actions specifically addressing e-cigarette use.
Evaluation outcomes were collected via self-report surveys and school action plans. The timing of surveys is depicted in Table 3. Evaluation question were set for each process and outcome component and will be addressed with a mix of quantitative and qualitative data, through descriptive analysis using mid-ECHO evaluations and pre-post comparisons.
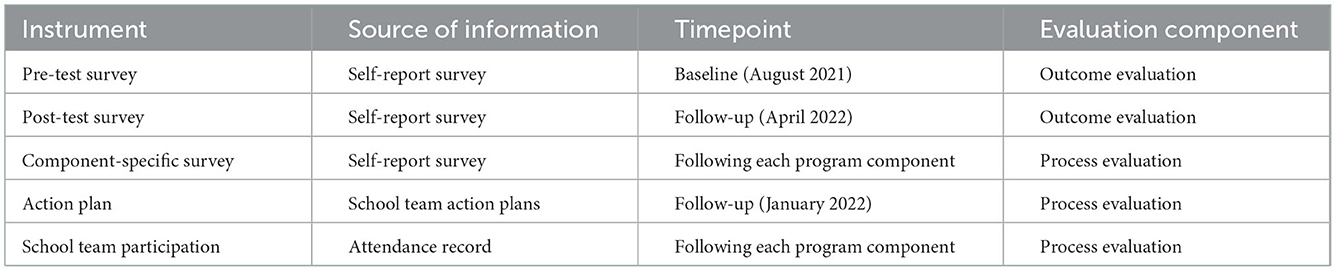
Table 3. Assessment data source and timing.
Discussion
Anticipated benefits
This pilot Vaping ECHO for Education aims to address a school-based need to address nicotine use in Kansas middle and high schools in order to maximize student health. We anticipate that, if successful, the pilot will result in both short- and long-term benefits to the schools, staff, and students. Specifically, in the short-term, it is anticipated that schools will build high functioning, skilled teams to address e-cigarette use. Teams will exhibit increased knowledge and competency, experience increased collaboration among school teams, greater referrals to cessation resources using evidence-based models such as Ask, Advise, Connect, and changes in policies to reduce punishment-based discipline for e-cigarette use. The following longer-term outcomes are anticipated two to three years following the pilot: (1) reductions in student vaping, (2) resultant improvements in student health, (3) system level changes in vaping-related policies and practice, and (4) cultural changes such that school or district norms do not support use of e-cigarettes.
Unique features
The program included unique features that set it apart from many other ECHOs. First, the ECHO included a summit kick-off with nationally recognized speakers which functioned to align participants' goals and energize the school teams. Second, a toolkit of resources was provided ahead of each corresponding session and school teams were encouraged to review them and refer to them as they created their individualized plan for addressing e-cigarette use at their school. Third, component specific assessments were reviewed immediately following the sessions and allowed for real-time correction and response to learner feedback. Finally, schools created and submitted individualized action plans that were entirely school team-directed based on the provided training and were shared between school teams to encourage inter-team collaboration and work toward building a community of practice.
Potential barriers or limitations
While we anticipate numerous benefits, the pilot is not without limitations. First, the ECHO ran during the second school year of the COVID-19 pandemic during two significant surges. As such, school teams' time was particularly limited and there were numerous competing priorities. It is unknown how this might impact the pilot outcomes. Second, the Vaping ECHO for Education was highly intensive and resulted in at least 12 h of in-session training and additional time spent devising and implementing action plans. While this resulted in a high-quality training experience, the time commitment may be seen as a barrier. Lastly, the program was piloted in 20 interdisciplinary schools across the state, each with unique approaches and implementation strategies, various degrees of access to resources, and each having different starting points in addressing vaping cessation in schools. It is unknown to what extent these differences will function as barriers to peer learning and collaboration.
Dissemination plan
The findings from this pilot ECHO will be compiled by the evaluation team and published in peer-reviewed journals and presented at professional conferences. In addition, we will present methods and findings to state and regional tobacco control groups. Of note, we plan to include pilot participants in these presentations to ensure that the network of schools is represented in all dissemination efforts.
Conclusions
If successful, the pilot findings would suggest that the ECHO model is an effective platform for disseminating evidence-based strategies to school staff. Moreover, the pilot will reach urban, rural, small, and large schools in the state of Kansas and, if successful, result in evidence-based policy changes and student and staff engagement in e-cigarette prevention and cessation. Moreover, the pilot could pave the way to implement the ECHO model to address other health-related issues faced by schools, providing access to high quality training in urban and rural areas of the state.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
EL, JR, BF, MT, KD-C, and HS contributed to the conceptualization of the project, methods, and investigation. HS oversaw data analysis. KD-C served as project administrator. EL wrote the original draft of the paper. All authors provided critical feedback, reviewed, and approved the final manuscript.
Funding
This work was supported by Developing Caring Communities Committed to Action (DCCCA) and the Kansas Department of Health and Environment.
Acknowledgments
The authors would like to thank Tatiana Lin for her critical review of the final manuscript and Wen-Chieh Lin for his critical feedback at the manuscript planning phase. In addition, the authors would like to thank the school teams, facilitators, content experts, and notetakers without whom, the project would not have been possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1057600/full#supplementary-material
References
1. Wilson N, Summers JA, Ait Ouakrim D, Hoek J, Edwards R, Blakely T. Improving on estimates of the potential relative harm to health from using modern ENDS (vaping) compared to tobacco smoking. BMC Public Health. (2021) 21:1–10. doi: 10.1186/s12889-021-12103-x
2. National National Academies of Sciences Engineering and Medicine. Public Health Consequences of E-Cigarettes. Washington, DC: The National Academies Press (2018). doi: 10.17226/24952
3. Walley SC, Wilson KM, Winickoff JP, Groner J. A public health crisis: Electronic cigarettes, vape, and JUUL. Pediatrics. (2019) 143:e20182741. doi: 10.1542/peds.2018-2741
4. Krishnan-Sarin S, Jackson A, Morean M, Kong G, Bold KW, Camenga DR, et al. E-cigarette devices used by high-school youth. Drug Alcohol Depend. (2019) 194:395–400. doi: 10.1016/j.drugalcdep.2018.10.022
5. Gentzke AS, Wang TW, Cornelius M, Park-Lee E, Ren C, Sawdey MD, et al. Tobacco product use and associated factors among middle and high school students—national youth tobacco survey, United States, 2021. MMWR Surveill Summ. (2022) 71:1. doi: 10.15585/mmwr.ss7105a1
6. Centers for Disease Control Prevention. 1991-2019 High School Youth Risk Behavior Survey Data. (2022). Available online at: http://yrbs-explorer.services.cdc.gov/ (accessed June 27, 2022).
7. Thomas RE, McLellan J, Perera R. Effectiveness of school-based smoking prevention curricula: systematic review and meta-analysis. BMJ Open. (2015) 5:e006976. doi: 10.1136/bmjopen-2014-006976
8. Public Health Law Center. Equitable Enforcement of Vaping Policy in Kansas High Schools. (2021). Available online at: https://www.publichealthlawcenter.org/sites/default/files/resources/Equitable-Enforcement-Vaping-Policy-KS-High-Schools.pdf (accessed August 5, 2022).
9. Hemphill SA, Heerde JA, Herrenkohl TI, Toumbourou JW, Catalano RF. The impact of school suspension on student tobacco use: a longitudinal study in Victoria, Australia, and Washington State, United States. Health Educ Behav. (2012) 39:45–56. doi: 10.1177/1090198111406724
10. Darling-Hammond S, Fronius TA, Sutherland H, Guckenburg S, Petrosino A, Hurley N. Effectiveness of restorative justice in US K-12 schools: a review of quantitative research. Contemp Sch Psychol. (2020) 24:295–308. doi: 10.1007/s40688-020-00290-0
11. Miech R, Leventhal AM, O'Malley PM, Johnston LD, Barrington-Trimis JL. Failed attempts to quit combustible cigarettes and e-cigarettes among US adolescents. JAMA. (2022) 327:1179–81. doi: 10.1001/jama.2022.1692
12. Arora S, Geppert CM, Kalishman S, Dion D, Pullara F, Bjeletich B, et al. Academic health center management of chronic diseases through knowledge networks: project ECHO. Acad Med. (2007) 82:154–60. doi: 10.1097/ACM.0b013e31802d8f68
13. Komaromy M, Duhigg D, Metcalf A, Carlson C, Kalishman S, Hayes L, et al. Project ECHO (Extension for Community Healthcare Outcomes): a new model for educating primary care providers about treatment of substance use disorders. Subs Abus. (2016) 37:20–4. doi: 10.1080/08897077.2015.1129388
14. Centers for Disease Control Prevention. Whole School, Whole Community, Whole Child (WSCC). Available online at: https://www.cdc.gov/healthyschools/wscc/index.htm (accessed July 22, 2022).
Keywords: tobacco, electronic cigarette, school, prevention, cessation, ECHO
Citation: Leavens ELS, Roberts J, Faseru B, Thompson M, Denes-Collar K and Shah H (2023) Development and implementation of the ECHO model in a school setting to address youth electronic cigarette use in Kansas: A protocol. Front. Public Health 10:1057600. doi: 10.3389/fpubh.2022.1057600
Received: 30 September 2022; Accepted: 23 December 2022;
Published: 12 January 2023.
Edited by:
Kristine C-Y McGrath, University of Technology Sydney, AustraliaReviewed by:
Suchitra Krishnan-Sarin, Yale University, United StatesLinda Neff, Centers for Disease Control and Prevention (CDC), United States
Copyright © 2023 Leavens, Roberts, Faseru, Thompson, Denes-Collar and Shah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eleanor L. S. Leavens,  ZWxlYXZlbnNAa3VtYy5lZHU=
ZWxlYXZlbnNAa3VtYy5lZHU=