 Régis Colin
Régis Colin Pascal Wild
Pascal Wild Christophe Paris2
Christophe Paris2 Stéphanie Boini
Stéphanie Boini- 1Department of Occupational Epidemiology, Occupational Health and Safety Institute (INRS), Vandoeuvre-les-Nancy, France
- 2INSERM U1085 Institut de Recherche en Santé, Environnement et Travail (IRSET), Rennes, France
Objective: The aim of this study was to analyze the effect of co-exposures to physical and psychosocial factors (PSF) regarding the incidence of workplace injuries (WI) among care workers. Additional objective was to identify the work factors associated with the co-exposure combinations leading to the highest rates of WI.
Methods: The study sample consisted of 4,418 care workers participating to the French Working Conditions Survey both in 2013 and 2016. WI were assessed during the 4-year follow-up by matching the databases of the National Health Insurance Funds' compensation system. We assessed exposure for physical factors and PSF using factorial analyses and hierarchical clustering. We implemented a Poisson regression model with the WI incidence as the outcome and the clusters as independent variables of interest. Logistic regression model allowed identifying the work factors that predicted co-exposure combinations with a WI rate > 40%.
Results: WI were highly related to both physical and psychosocial exposures. With low exposure to one or the other, there was no increased risk of WI. Physical factors and PSF potentiated each other and their co-exposure significantly increased the risk of WI, with model predicted rates per 1,000 persons-year for those most exposed to physical risk of 14.6 [4.5–24.8] with low PSF and 38.0 [29.8–46.3] with high PSF. Work factors that predicted co-exposure combinations with a rate > 40 WI% were: working as nursing assistant or hospital services officer, lack of predictability and flexibility of schedules, overtime, controlled schedules, work-family imbalance and insufficient preventive measures.
Conclusions: Our findings highlight the need to take into account psychosocial factors in addition of only considering physical factors when analyzing WI occurrence, as usually done. Prevention actions must be taken to reduce both physical and psychosocial exposure. These results provide keys points for the prevention of WI among care workers.
Introduction
Worldwide, the population of care workers is increasing, and they are victims of many workplace injuries (WI). For example, in United States, the rate of injury for emergency medical technicians and paramedics was about three times the national average for all occupations (1). Among care workers, the highest WI rates were observed among nursing professions (2). An Australian retrospective cohort analysis observed that health and social care workers had a significantly higher rate of WI than workers in other industries and found the highest rate of WI for ambulance officers and social workers (3). Similarly in France, the official statistics reported 3.5 million care workers (10% more than 10 years ago) in 2019. This year, 180,000 WI were recorded for this population. With a WI rate of 52.3 per 1,000 care workers, they rank first among injured workers, ahead of the construction industry and well above the national average (33.5 WI per 1,000 workers) (4). The rate of WI among care workers has increased by 12% in 5 years, while that of the other types of work activities has followed a downward trend.
The notion of “care work” covers the activities of care given to others, from the youngest to the oldest (medical care, dependence, meals, living space, wellbeing, etc.) and constitutes a concrete response to the needs of others. This occupational sector includes professions as varied as home care aide, nurse, laboratory technician, dental assistant, surgeon, etc., carried out in different contexts such as hospitals, the home, housing for elderly dependent persons, nursing homes, town practices, etc. They are subject to multiple occupational risks. Their function makes them particularly prone to musculoskeletal disorders (5–7) and low back pain (5, 8). All care workers have in common that they are exposed to a wide range of occupational risks related to physical activity mostly attributable to manual handling (9), falls and slips (10), and infectious (11), biological (12) and chemical risks [disinfectants (13), anesthetic gases (14), drugs (15)]. Because of the necessity of continuity of care, they are subject to a specific work organization that regularly requires shift work, night work (12, 16) and long and compressed work schedules (17). They are also particularly exposed to psychosocial risk factors (PSF) [stressful work organization (2), confrontation with illness, end of life, death (18), violence from colleagues (19, 20) or from patients and their relatives (21)].
Longitudinal studies that have observed the effect of PSF on the occurrence of WI for care workers are however scarce (22). In 2019, a prospective cohort study investigated the risk factors for back injury in the healthcare sector in Denmark and concluded that in addition to physical burden, poor collaboration between and support from colleagues increased the risk of back injury (23). A Dutch study found that low autonomy and exposure to harassment and violence inside and outside the organization were associated with WI for workers in the health and welfare sector (20).
Regarding the co-exposure between physical and psychosocial factors, a cross-sectional study found a higher prevalence of patient-handling injury when nursing personnel declared both high physical demand and low decision latitude (24). A recent longitudinal study found that the difference in WI rates between high and low psychosocial exposures seemed to increase with increasing physical exposure among workers from all sectors of activity, but not only care workers (25). To our knowledge, no prospective study has yet focused on the effects of joint exposure to physical factors and PSF on the occurrence of WI among care workers.
The literature, as described above, highlights the lack of prospective studies analyzing the effect of psychosocial factors on the occurrence of WI in care workers. Workers exposed to a single occupational risk factor are rare and are in fact most often exposed to several risk factors simultaneously. Multi-exposures between the risk factors for WI, and in particular between physical and psychosocial risk factors, have been scarcely explored. However, considering the synergetic effects between exposure to physical and psychosocial risks in the occurrence of WI seems to be a plausible hypothesis in order to identify the determinants for better-adapted prevention.
The objective of this study was, first, to analyse the effect of co-exposures to physical and psychosocial factors regarding the incidence of workplace injury among care workers. Secondly, our study aimed to identify the work factors associated with the co-exposure combinations leading to the highest rates of WI.
Methods
Study design
This observational study was designed as a prospective cohort study nested in the French Working Conditions Survey, with a follow-up period of 4 years. Participants of this study were workers interviewed in both 2013 and 2016.
Setting and participants
In the French Working Conditions Survey, trained interviewers questioned 33,673 workers face-to-face in 2013. In 2016, 22,852 of them were again interviewed. Data were collected from workers on working hours and the organization of working time, organization and the pace of work, risks, hardships and their prevention, psychosocial constraints, relations with the public and violence at work. Using the participants' social security ID (if available), the survey data were matched with data relative to WI, occupational diseases and the consumption of medical care or treatments, obtained from the databases of the National Health Insurance compensation system.
Study population consists of 17,831 workers interviewed in both 2013 and 2016. The exclusion criteria were: not providing a social security ID (n = 2,665); not being registered in the National Health Insurance compensation system (n = 2,337); and not having sufficient information about employment (n = 19).
The present paper focuses on care workers. We considered as a care worker the respondents reporting that their main function in their job was to care for people or that their main profession featured on a list of selected professional activities (nursing assistant, nurse, midwife, medical and paramedical profession, social workers, professional of cultural or sports activities, home care, nursery assistant and hospital services officer). Finally, our study sample consisted of 4,418 care workers.
Outcome: Workplace injuries
The claims for recognition of WI are recorded by the National Health Insurance. WI were assessed during the 4-year follow-up. Detailed characteristics were collected on the date of occurrence, the nature and the site of the injury, and the duration of sick leave. The main outcome was the occurrence of a WI during the follow-up period, whatever the nature or duration of the sick leave as recorded by the National Health Insurance.
Risk factors
Numerous risk factors were investigated in this study. Given the large number of questions, we grouped them into broad categories or subgroups of physical factors and psychosocial factors identified by a group of French experts (26). The process to characterize physical and PSF exposures is detailed in Supplementary material 1.
Physical factors
We grouped the 20 items related to physical risk factors into six categories (Supplementary material 1):
- Awkward or uncomfortable postures (standing for long periods of time, staying in another awkward or tiring posture for a long time, performing painful or tiring movements, making long or frequent trips on foot);
- Carrying heavy loads (does your job require you to carry or move heavy loads?);
- Vibration or shaking (does your job cause you to shake or vibrate?);
- Loud noise (can you hear a person placed 2 or 3 meters away from you when they speak to you?);
- Concentration (keeping your eyes on the work, reading small, poorly printed, poorly written letters or numbers, examining very small objects, small details, reading and paying attention to brief, unpredictable, or hard-to-detect visual or audible signals);
- Unhealthy work environment (dirt, humidity, drafts, bad smells, high temperature, low temperature, lack or poor condition of sanitary facilities, no view of the external environment, lack of privacy).
Psychosocial factors
The following six groups were defined based on the 98 items (Supplementary material 1):
- Labor intensity and working time (three subgroups: excessive workload, time pressure, work complexity);
- Emotional demand (four subgroups: contact with suffering, poor relationship with the public, emotional dissonance, fear for safety during work);
- Lack of autonomy (five subgroups: monotony and boredom, lack of pleasure at work, skills not fully utilized or developed, unpredictability, no choice of how a job is done);
- Social relationships at work (10 subgroups: violence, poor cooperation between colleagues and integration in a team, poor team autonomy and work engagement, lack of support from superiors, lack of leadership, lack of organizational justice, lack of reward, lack of career prospects, insufficient salary, inadequate social recognition of the job);
- Conflict of values (two subgroups: ethical conflicts, no opportunity to perform high-quality jobs);
- Job insecurity (three subgroups: job instability, lack of work sustainability, occupational changes).
Other covariates
The questionnaire also collected items on socio-demographic characteristics: gender, age, educational level, family structure and monthly income per consumption unit. Furthermore, information about Health included sleep problems and the use of psychotropic drugs. Finally, occupational factors included the number of workers in the company, the type of work contract, seniority in the job, the type of workplace, and occupational category.
Statistical analysis
We calculated the mean rates of WI per 1,000 person-years (py) at work, taking into account part-time work.
We analyzed the occurrence of WI during the follow-up period as a function of the risk factors using multiple Poisson regression models accounting for the person-years at work. The models were fitted with covariates selected based on both scientific evidence and statistical considerations (stepwise selection). The results were presented in the form of a model predicted rate of WI per 1,000 py, with 95% confidence intervals and the p-value of the incidence rate ratio.
WI and exposures to each physical and each psychosocial factors
We fitted one model for each of the 6 physical exposures as well as for each of the 6 PSF exposures, as defined in Supplementary material 1; first step. The models were adjusted for gender, age class, educational level, work contract, seniority, sleep problem, and use of psychotropic drugs. In addition, we considered models with interaction between the risk factors and gender.
WI and co-exposures to physical and psychosocial factors
We used hierarchical clustering on the six categories of physical factors and the six categories of PSF, resulting in 3 levels of physical exposure and three levels of PSF exposure, respectively (Supplementary material 1, second step). We fitted the profiles of physical exposure and PSF exposure in interaction, adjusting for the previous covariates.
Work factors associated with the co-exposure combinations leading to the highest WI rates
Within each pairwise combination of the six physical categories and the six psychosocial categories, we computed model-based rates of WI according to the detailed exposure levels. We thus identified the pairwise combinations of physical and psychosocial factors with a rate higher than 40 WI per 1,000 py (subsequently called “high-rate group”). We modeled the probability of this high-rate group according to work activity, and sociodemographic and organization characteristics using logistic regression with a backward-stepwise selection.
In order to check the fit of the model, we first calculated the model-based area under the ROC curve. Secondly, we checked the relevance of the predicted probability to belong to this high-rate group by performing a logistic regression with the occurrence of WI as the outcome.
We performed the statistical analysis using Stata version 15.1 (StataCorp. LLC, Tx, USA), except for the clustering process, which was performed using R (27). The level of statistical significance was set at 0.05.
Results
Characteristics of the study population
The population of interest included 4,418 care workers (25% of the study population), mostly women (84%) with a mean age of 43 years in 2013 (Table 1). Sixty-three percent of them had an educational level higher than the secondary school certificate. Their family composition and income were not different from other workers. With regard to health, 34% reported having sleep problems and 11% were using psychotropic drugs. A majority of care workers worked in a company with more than 50 employees, and had more than 5 years' seniority at the time of inclusion (Table 1).
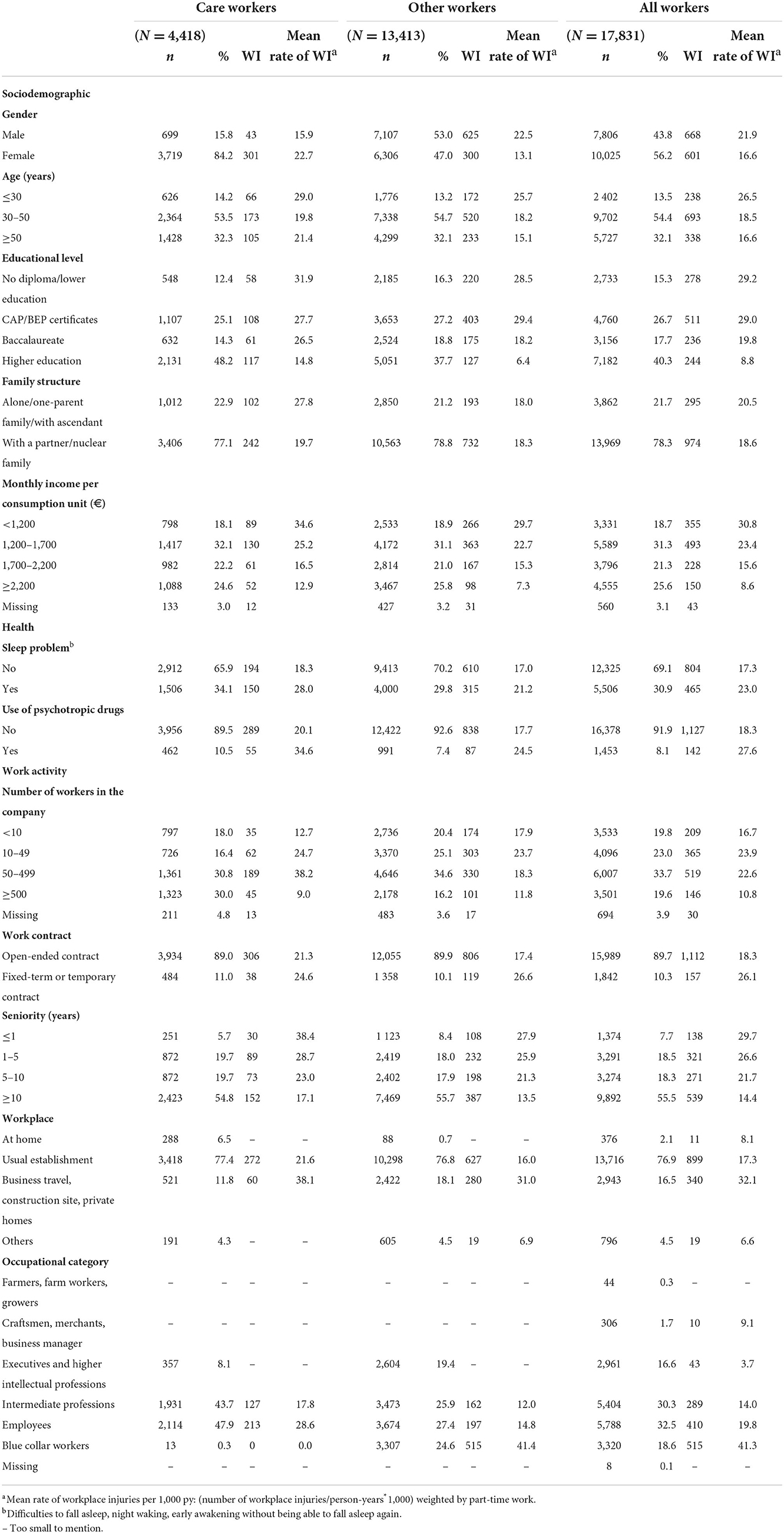
Table 1. Characteristics of participants at inclusion in 2013 and mean rate of workplace injuries (WI).
Workplace injuries
The National Health Insurance compensation system identified 344 care workers declaring at least one WI (8%) (Table 2). Sick leave for the occurrence of the first WI resulted in more than 1 day off work for 68% of them. The most frequent sites of WI were upper limb (30%), back (29%) and to a lesser extent lower limb (20%). Care workers were mainly victims of back pain, lumbago, neck pain, spine, sciatica, concussion and internal trauma (Table 2). The mean rates of WI were highest among women, the youngest, the least qualified, those with the lowest incomes, the least seniority, and precarious work contracts (Table 1—last column).
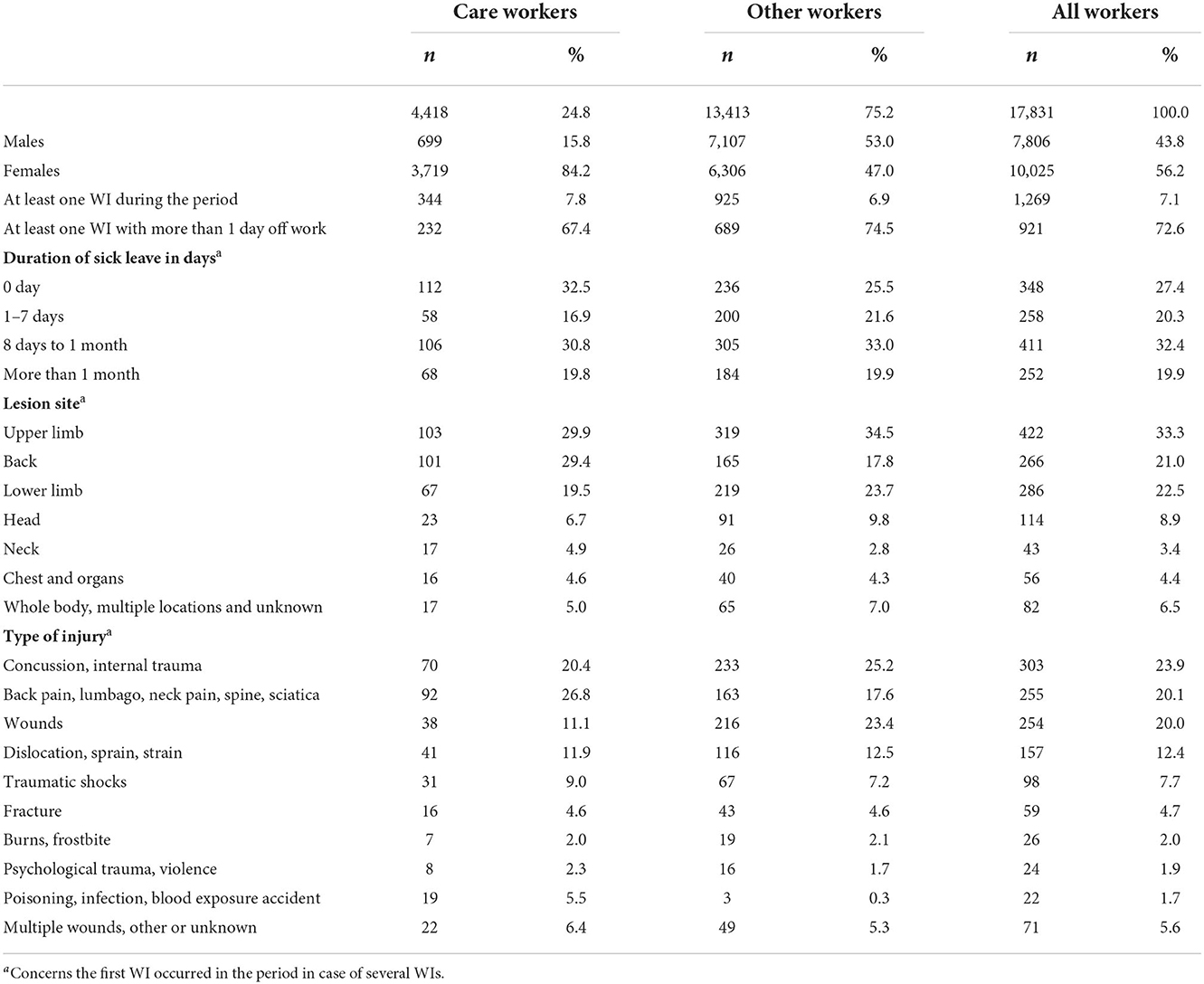
Table 2. Description of workplace injuries (WI) occurred in the follow up period for the entire study population and for care workers.
The model predicted rates of WI per 1,000 py for each adjustment variable selected after a stepwise selection (sociodemographic, health, activity) are presented in Supplementary material 2.
Physical risk factors and workplace injuries
Four out of six physical factors were significantly associated with the incidence of WI: awkward or uncomfortable postures, carrying heavy loads, having disturbed concentration, and working in an unhealthy work environment (Table 3).
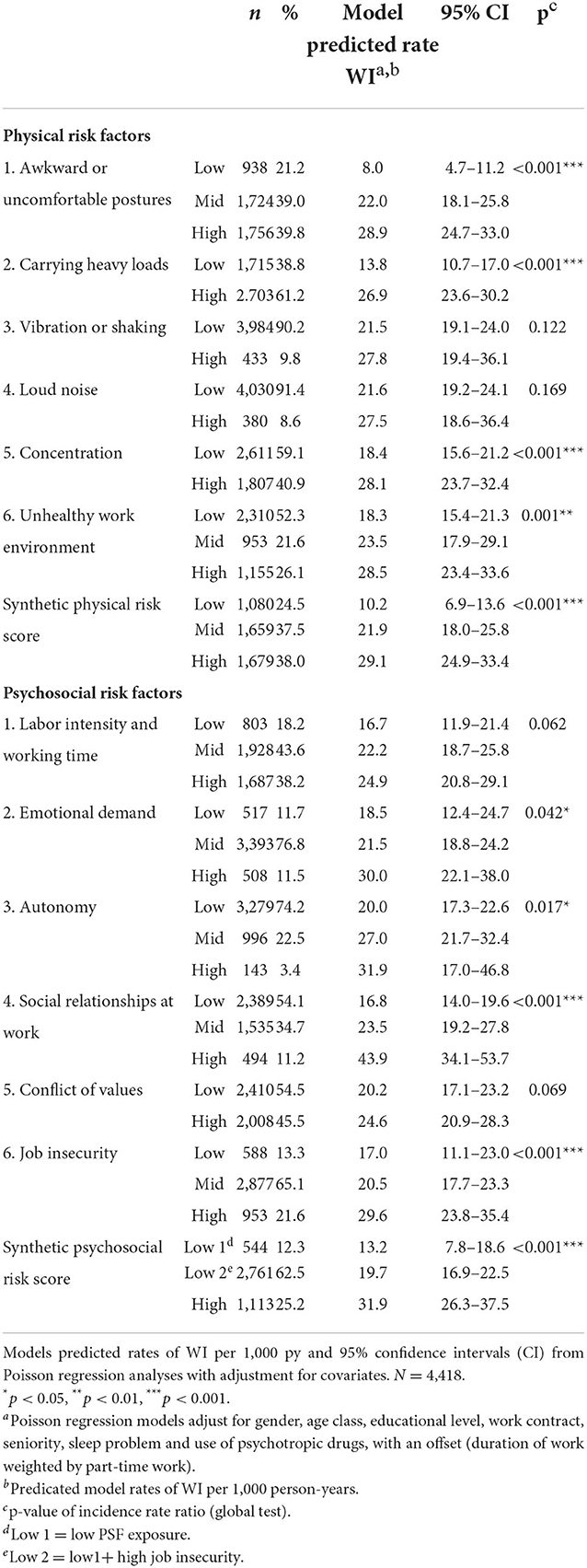
Table 3. Association between occurrence of workplace injuries (WI) during the period of follow-up and exposures to each physical and each psychosocial risk factors (PSF) among care workers.
We characterized as low, middle and high physical exposure the three groups (synthetic physical score) obtained using the hierarchical classification carried out on the physical factors (Supplementary material 1, second step). The higher this score, the higher the model predicted rate of WI (Table 3). Rates of WI according to gender are presented in Supplementary material 3.
Psychosocial risk factors and workplace injuries
Poor social relationships at work, job insecurity, lack of autonomy, and emotional demand were statistically associated with the incidence of WI among care workers (Table 3).
Regarding the synthetic PSF risk score, the cluster analysis of the PSF led to the identification of three groups of psychosocial exposure: low PSF exposure, low PSF exposure but high job insecurity, and multiple high PSF exposures (Supplementary material 1, second step). The lowest model predicted rate was for low PSF exposure [low 1: 13.2 WI per 1,000 py (7.8–18.6)]. The rate was higher for low PSF exposure but high job insecurity [low 2: 19.7 WI per 1,000 py (16.9–22.5)]. Finally, the rate was the highest in the case of multiple high exposures to PSF risk factors [31.9 WI per 1,000 py (26.3–37.5)].
Rates of WI according to gender are presented in Supplementary material 4.
Co-exposures to physical and psychosocial work factors
WI were closely related to both the synthetic physical score (p < 0.001) and the synthetic PSF risk score (p < 0.001) (Figure 1). With low physical exposure, there was no increased risk of WI whatever the level of PSF (p = 0.867). Model predicted rates of WI did not differ significantly for the lowest PSF exposed, regardless of the physical exposure. There was a significant increase in predicted injury rates as PSF exposure increased for both middle and high exposure to physical factors (p = 0.029 and p = 0.005, respectively).
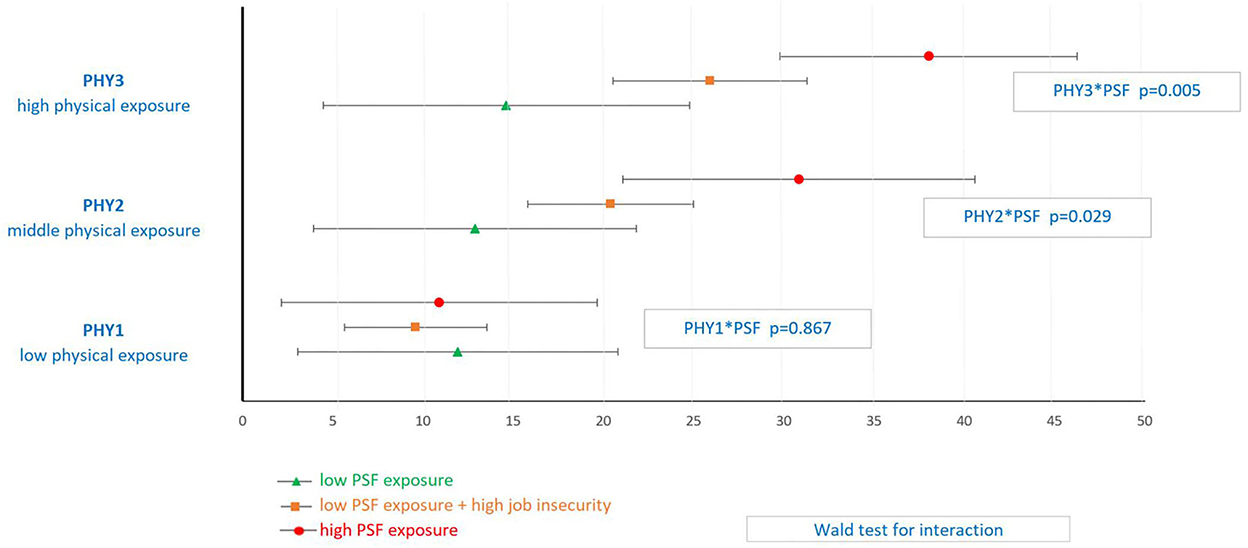
Figure 1. Model predicted rate of workplace injuries for each level of physical (PHY) and psychosocial (PSF) exposure among Care workersa. aPoisson regression model with adjustment for covariates: gender, age class, educational level, work contract, seniority, sleep problem and use of psychotropic drugs, with an offset (duration of work weighted by part-time work).
Physical and psychosocial exposures potentiated each other and their co-exposure significantly increased the risk of WI. Model predicted rates of WI per 1,000 py for those most exposed to physical factors was 14.6 WI per 1,000 py [4.5–24.8] when low PSF, 25.9 WI per 1,000 py [20.5–31.3] when low PSF and high job insecurity, and 38.0 [29.8–46.3] when high PSF (p < 0.001) (Figure 1).
Profile of the care workers with the highest rate of WI
Among care workers, 709 workers (16%) were exposed to combinations of physical and psychosocial risk factors with model predicted rates higher than 40 WI per 1,000 py (high-rate group). Their co-exposure consisted mainly of poor social relationships at work and, to a lesser extent, a lack of autonomy, high job insecurity and high labor intensity (Supplementary material 5). Socio-demographic characteristics did not differ between the high-rate group and the other care workers (data not shown).
According to the results of the logistic regression shown in Table 4 (Model 2), work factors that predicted belonging to the high-rate group were as follows: working as nursing assistant or hospital services officer, difficulty of organization in scheduling, overtime, work-family imbalance, and insufficient preventive measures.
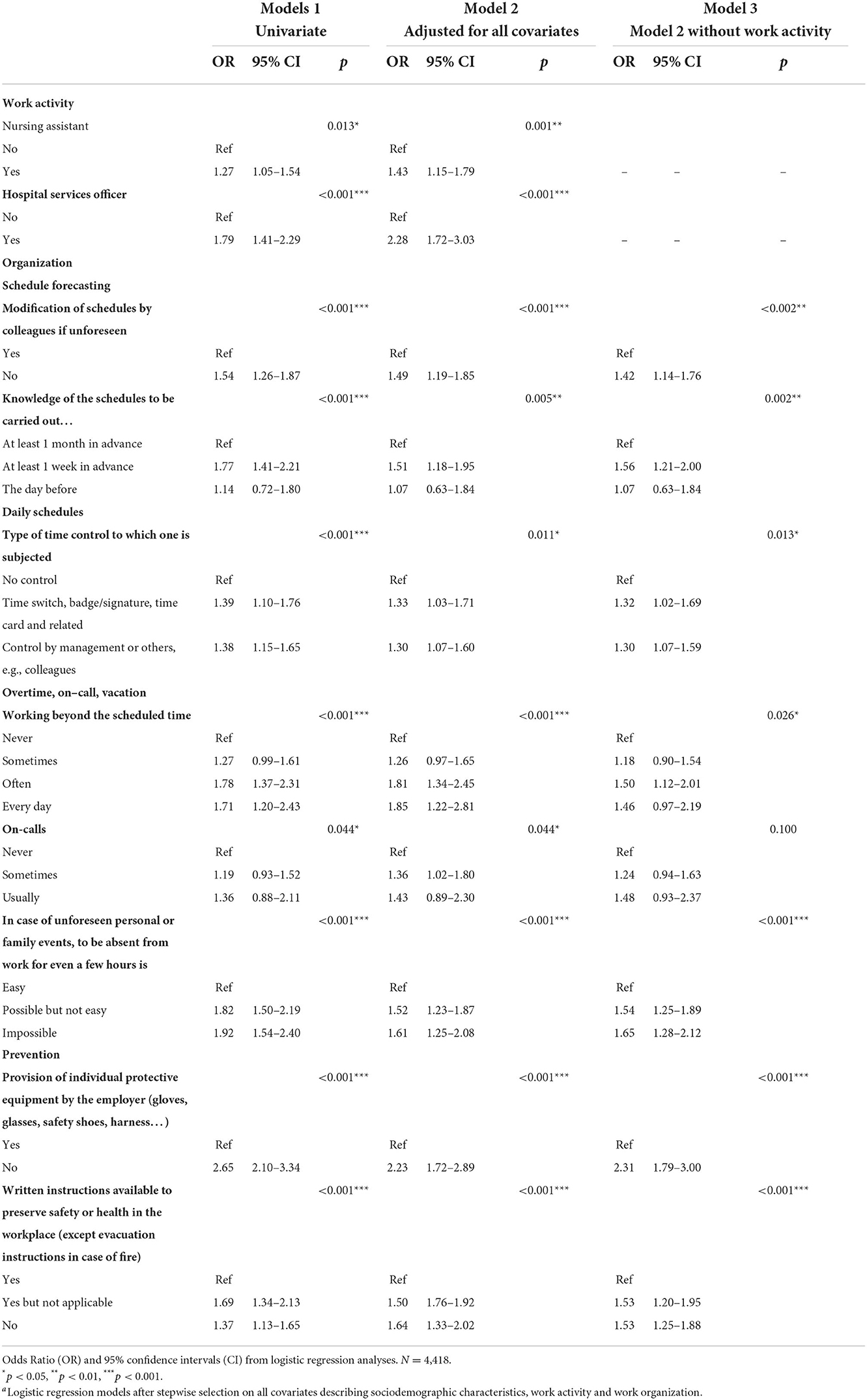
Table 4. Work activity and work organization characteristicsa associated with belonging to care workers exposed to combinations of physical and psychosocial exposures with workplace injuries rates >40 per 1,000 py (n = 709).
The area under the curve was 0.67. Finally, the higher the probability of belonging to the high-rate group, the higher the risk of WI [OR = 1.05 (1.00–1.09) with p = 0.031].
Discussion
Among the 4,418 care workers, workplace injuries were closely linked to both reported physical and psychosocial exposures. Physical and PSF exposures potentiated each other and their co-exposure increased the risk of occurrence of WI. The highest rate of predicted rate of WI concerned care workers with the highest co-exposure to psychosocial and physical factors: 38 WI per 1,000 py. Moreover, with low exposure to physical risk factors, there was no increased risk of the occurrence of WI, whatever the level of PSF exposure. Similarly, with low PSF exposure, the predicted rates of WI were not different according to the level of exposure to physical factors.
These results are in line with the findings of our previous study on a population of workers from all sectors of activity: the risk of WI was highest among workers with high physical exposures regardless of the psychosocial exposures. Indeed, the difference in rates of WI between high and low PSF exposures seemed to increase with increasing physical exposure, but not significantly (25).
When focusing on the high WI rate group, the PSF mainly involved consisted of poor social relationships at work, whatever the type of physical factors and, to a lesser extent, low autonomy, high job insecurity and high labor intensity. Our results are consistent with the literature. Studies found that nursing assistant WI rates were higher in case of low supervisor support (28), nurses who reported higher social support from co-workers had lower WI rates (29) and workers in the health and welfare sector exposed to violence and harassment from supervisors, colleagues or others were associated with a high WI rate (20). In this population, low autonomy was also associated with WI (20) as well as high workload (30, 31) and precarious employment resulting in high job insecurity (32).
We identified two main types of occupations in our high-rate group: nursing assistants and hospital services officer. Similarly, higher WI rates among nursing assistants, relative to nurses, were previously reported in 4 studies (24, 33–35). Moreover, emergency medical technicians and paramedics had a WI rate about three times the United States average for all occupations (1). Among hospital workers, emergency medical technicians had the highest rate of WI (33). A recent Australian study provided evidence of a high WI rate among health and social care workers. However, they found the highest rates of WI for social workers and ambulance officers, which was not the case in our study (3). Contrary to nursing assistants and hospital services officers, being a nurse was not associated with exposures leading to the highest WI rates. A previous study, focusing on the risk perception of musculoskeletal injury, found that most critical care nurses were concerned about their ergonomic job risks (36), which may be one explanation for lowest WI rate that we observed in nurses. Moreover, Rodriguez-Acosta et al. (34) observed that most of the WI for health care workers were related to the process of delivering direct patient care, nurses performing fewer tasks compared to assistant nurses and having a lower risk of lifting injuries than assistant nurses.
We identified some organizational factors that predicted belonging to the high-rate group. These care workers had in common: schedule inflexibility, work duration, mandatory overtime, impossibility or difficulty to be absent in the case of unforeseen personal or family events and inadequate safety prevention policy (i.e., provision of individual protective equipment and availability of written instructions). In the literature on nursing assistants, the frequency of working mandatory overtime (37), as well as not having sufficient time to complete patient activities of daily living (37, 38), were strongly associated with the occurrence of WI. The absence or unavailability of mechanical lifting equipment when needed increased the risk of WI among nursing assistants (33, 38). When nursing assistants declared available facilities training to reduce injuries, the risk of WI was lower (38). Finally, nurses who reported better safety leadership, greater safety diligence or better ergonomic practices, had lower WI rates (29).
Our results were in line with previous literature on most of the factors known to influence the occurrence of WI. WI rates were statistically higher among the youngest workers (39–41), those with a lower educational level (39, 41), subject to precarious contracts (42), or with poor seniority (43), sleep problems (44) or using psychotropic drugs (45). While the literature highlighted higher rates of WI among men than women in other sectors of activity (39, 40), the rate of WI among care workers was highest for women in our study. These results were in line with other studies (1, 12). Within the same occupations, men were globally more likely to be exposed to physical hazards compared to women, but women in healthcare occupations were more exposed to prolonged standing, kneeling, lifting, and other material handling than men, increasing the likelihood of WI (46).
To the best of our knowledge, this is the first epidemiological study to analyse the impact of multiple exposure to physical and psychosocial factors on the occurrence of WI among care workers. The most striking result in our study is the significant interaction between physical and PSF exposures in the occurrence of WI among care workers. Moreover, no potentiation of exposures was observed in either low physical or low PSF exposure. In comparison to the care workers, model predicted rates of WI for all workers were not significantly different between two low PSF exposure categories (data not shown). More specifically, same analyses in blue collar workers seems to report different patterns of interaction between physical factors and PSF (data not shown). The levels of exposure to physical factors, mainly awkward, uncomfortable postures and carrying heavy loads, were high among both blue collar and care workers. Both had high levels of psychosocial exposure but blue-collar workers reported low autonomy, lack of reward and low job insecurity more frequently, while care workers mainly reported high emotional demand, poor social support, high conflicts of values, excessive workload and work complexity (data not shown). These results lead us to assume that the potentiation of physical and psychosocial factors differs according to the type of FPS and should be investigated in depth.
Our study have several strengths. This survey covered workers who were representative of the French working population. The large number of participants allowed us to focus on specific occupational sectors. Matching with the databases of the National Health Insurance Funds' compensation system provided independent and systematic data on WI with detailed information on the nature, circumstances and duration of any sick leave. Moreover, the detailed questionnaires obtained before the incidence of WI allowed the accurate characterization of physical and psychosocial exposures, eliminating any information bias inherent to retrospective information collection.
In order to estimate potential selection bias, we compared our sample with those lost to follow-up (not interviewed in 2016) and those excluded due to absence of national insurance ID. Globally, there were no differences between these groups in terms of overall health and reported number of WI in the year before 2013.
A final issue might be underreporting of WI to the employer in small companies due to the lack of a reference person to pass on the information or the difficulty/impossibility of replacement when absent (47). Regarding our care workers, the raw WI rate was higher in small companies than in the largest companies. Therefore, underreporting in small companies does not seem to be a major issue in our study.
Conclusion
Our findings highlight the need to take into account psychosocial factors in addition of only considering physical factors when analyzing WI occurrence, as usually done.
From a theoretical perspective, future research should focus on identifying the most deleterious combinations of risks from multiple exposures to physical and psychosocial risk factors in the occurrence of occupational injuries.
These results provide practical keys points for the prevention of WI among care workers. Prevention actions must be taken to reduce both physical and psychosocial exposure. More specifically, interventions targeted at reducing the handling of loads or people and promoting an organization more centered on the management of human resources could jointly reduce the physical and psychosocial risks that cause many WI in the field of care.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
All the subjects gave their free and informed consent for participation in the Working Conditions survey. Access to certain confidential data for this work was made possible within a secure environment offered by CASD—Centre d'accès sécurisé aux données (Ref. 10.34724/CASD). Our study was performed in accordance with the ethical standards in force and received the necessary regulatory approvals (Visa Comité du secret statistique-ME463 and CNIL-2215533).
Author contributions
RC designed the study, reviewed the literature, performed data management and statistical analyses, and drafted the manuscript. SB designed the study, reviewed the literature, oversaw statistical analyses, and drafted the manuscript. PW participated in study design, oversaw statistical analyses, and drafted the manuscript. CP participated in study design and drafted the manuscript. All authors collaborated interactively, read, and approved the final manuscript.
Funding
This research was financed by the core funding of the INRS.
Acknowledgments
We wish to express our gratitude to the Research, Studies and Statistics Coordination Department (Direction de l'Animation de la Recherche, des Études et des Statistiques –DARES), affiliated with the French Ministry of Labor, which produces data on labor and work conditions.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1055846/full#supplementary-material
References
1. Maguire BJ, Smith S. Injuries and fatalities among emergency medical technicians and paramedics in the United States. Prehosp Disaster Med. (2013) 28:376–82. doi: 10.1017/S1049023X13003555
2. Lee SJ, Lee JH. Associations of organizational safety practices and culture with physical workload, perceptions about work, and work-related injury and symptoms among hospital nurses. J Nurs Administr. (2017) 47:404–11. doi: 10.1097/NNA.0000000000000504
3. Xia T, Collie A. Work-related injury and illness in the Victorian healthcare sector: a retrospective analysis of workers' compensation claim records. Austral Health Rev. (2020) 44:24–30. doi: 10.1071/AH18017
4. CNAM DdRP. Statistiques de sinistralité 2019 tous CTN et par CTN 2021(2021). 62 p. (Direction des Risques Professionnels). 2020-281-CTN.
5. Gilchrist A, Pokorná A. Prevalence of musculoskeletal low back pain among registered nurses: results of an online survey. J Clin Nurs. (2021) 30:1675–83. doi: 10.1111/jocn.15722
6. Lin SC, Lin LL, Liu CJ, Fang CK, Lin MH. Exploring the factors affecting musculoskeletal disorders risk among hospital nurses. PLoS ONE. (2020) 15:e0231319. doi: 10.1371/journal.pone.0231319
7. Du J, Zhang L, Xu C, Qiao J. Relationship between the exposure to occupation-related psychosocial and physical exertion and upper body musculoskeletal diseases in hospital nurses: a systematic review and meta-analysis. Asian Nurs Res. (2021) 15:163–73. doi: 10.1016/j.anr.2021.03.003
8. Sun W, Zhang H, Tang L, He Y, Tian S. The factors of non-specific chronic low back pain in nurses: a meta-analysis. J Back Musculoskel Rehabil. (2021) 34:343–53. doi: 10.3233/BMR-200161
9. Bernardes JM, Monteiro-Pereira PE, Gómez-Salgado J, Ruiz-Frutos C, Dias A. Healthcare workers' knowledge for safe handling and moving of the patient. Int J Occup Saf Ergon JOSE. (2021) 5:1–7. doi: 10.1080/10803548.2021.1955484
10. Demaria J, Valent F, Danielis M, Bellomo F, Farneti F, Bressan V, et al. Do falls and other safety issues occur more often during handovers when nurses are away from patients? findings from a retrospective study design. J Nurs Care Qual. (2021) 36:202–9. doi: 10.1097/NCQ.0000000000000526
11. Shin Y, Kim UJ, Lee HA, Choi EJ, Park HJ, Ahn HS, et al. Health and mortality in Korean healthcare workers. J Korean Med Sci. (2022) 37:1–14. doi: 10.3346/jkms.2022.37.e22
12. Cofini V, Capodacqua A, Calisse S, Galassi I, Cipollone L, Necozione S. Trend analysis and factors associated with biological injuries among health care workers in Southern Italy. Med Lavoro. (2018) 109:308–15. doi: 10.23749/mdl.v109i4.7245
13. Dumas O, Varraso R, Boggs KM, Quinot C, Zock J-P, Henneberger PK, et al. Association of occupational exposure to disinfectants with incidence of chronic obstructive pulmonary disease among US female nurses. JAMA Network Open. (2019) 2:e1913563. doi: 10.1001/jamanetworkopen.2019.13563
14. González-Rodríguez R, Muñoz Martínez A, Galan Serrano J, Moral García MV. Health worker exposure risk during inhalation sedation with sevoflurane using the (AnaConDa®) anaesthetic conserving device. Rev Espanola Anestesiol Reanim. (2014) 61:133–9. doi: 10.1016/j.redar.2013.11.011
15. Gianfredi V, Salvatori T, Nucci D, Villarini M, Moretti M. [Genotoxic risk in nurses handling antiblastic drugs: systematic review of literature and meta-analysis]. Recenti Progr Med. (2017) 108:511–20. doi: 10.1701/2829.28583
16. Vedaa Ø, Harris A, Erevik EK, Waage S, Bjorvatn B, Sivertsen B, et al. Short rest between shifts (quick returns) and night work is associated with work-related accidents. Int Arch Occup Environ Health. (2019) 92:829–35. doi: 10.1007/s00420-019-01421-8
17. Thompson BJ. Does work-induced fatigue accumulate across three compressed 12 hour shifts in hospital nurses and aides? PLoS ONE. (2019) 14:e0211715. doi: 10.1371/journal.pone.0211715
18. Leuter C, Petrucci C, La Cerra C, Dante A, Franconi I, Caponnetto V, et al. Nurses' and physicians' opinions on end-of-life: a secondary analysis from an Italian cross-sectional study. Ann Igiene. (2020) 32:274–84. doi: 10.7416/ai.2020.2350
19. Crawford CL, Chu F, Judson LH, Cuenca E, Jadalla AA, Tze-Polo L, et al. An integrative review of nurse-to-nurse incivility, hostility, and workplace violence: a GPS for nurse leaders. Nurs Administr Quart. (2019) 43:138–56. doi: 10.1097/NAQ.0000000000000338
20. van der Klauw M, Hengel KO, Roozeboom MB, Koppes LL, Venema A. Occupational accidents in the Netherlands: incidence, mental harm, and their relationship with psychosocial factors at work. Int J Injury Control Saf Promot. (2016) 23:79–84. doi: 10.1080/17457300.2014.966119
21. Babiarczyk B, Turbiarz A, Tomagová M, Zeleníková R, Önler E, Sancho Cantus D. Reporting of workplace violence towards nurses in 5 European countries - a cross-sectional study. Int J Occup Med Environ Health. (2020) 33:325–38. doi: 10.13075/ijomeh.1896.01475
22. Taibi Y, Metzler YA, Bellingrath S, Müller A. A systematic overview on the risk effects of psychosocial work characteristics on musculoskeletal disorders, absenteeism, and workplace accidents. Appl Ergon. (2021) 95:103434. doi: 10.1016/j.apergo.2021.103434
23. Andersen LL, Vinstrup J, Villadsen E, Jay K, Jakobsen MD. Physical and psychosocial work environmental risk factors for back injury among healthcare workers: prospective cohort study. Int J Environ Res Public Health. (2019) 16:4528. doi: 10.3390/ijerph16224528
24. Schoenfisch AL, Lipscomb HJ. Job characteristics and work organization factors associated with patient-handling injury among nursing personnel. Work. (2009) 33:117–28. doi: 10.3233/WOR-2009-0847
25. Colin R, Wild P, Paris C, Boini S. Effect of joint exposure to psychosocial and physical work factors on the incidence of workplace injuries: results from a longitudinal survey. J Occup Environ Med. (2021) 63:921–30. doi: 10.1097/JOM.0000000000002313
26. Gollac M, Bodier M. Mesurer les facteurs psychosociaux de risque au travail pour les maîtriser. (2011). p. 223.
27. R Core Team,. R: A language environment for statistical computing. Vienna: R Foundation for Statistical Computing (2021). Available online at: https://www.R-project.org/
28. McCaughey D, McGhan G, Walsh EM, Rathert C, Belue R. The relationship of positive work environments and workplace injury: evidence from the National Nursing Assistant Survey. Health Care Manag Rev. (2014) 39:75–88. doi: 10.1097/HMR.0b013e3182860919
29. Tveito TH, Sembajwe G, Boden LI, Dennerlein JT, Wagner GR, Kenwood C, et al. Impact of organizational policies and practices on workplace injuries in a hospital setting. J Occup Environ Med. (2014) 56:802–8. doi: 10.1097/JOM.0000000000000189
30. Bagheri Hosseinabadi M, Khanjani N, Etemadinezhad S, Samaei SE, Raadabadi M, Mostafaee M. The associations of workload, individual and organisational factors on nurses' occupational injuries. J Clin Nurs. (2019) 28:902–11. doi: 10.1111/jocn.14699
31. Çelikkalp Ü, Dilek F. Factors affecting the occupational accident rates among nurses. Rev Escola Enfermagem U S P. (2019) 53:e03524. doi: 10.1590/s1980-220x2018049703524
32. Inoue M, Nishikitani M, Tsurugano S, Yano E. [The health of permanent workers and workers with precarious employment: a literature review]. Sangyo Eiseigaku Zasshi. (2011) 53:117–39. doi: 10.1539/sangyoeisei.A11002
33. Pompeii LA, Lipscomb HJ, Schoenfisch AL, Dement JM. Musculoskeletal injuries resulting from patient handling tasks among hospital workers. Am J Ind Med. (2009) 52:571–8. doi: 10.1002/ajim.20704
34. Rodríguez-Acosta RL, Richardson DB, Lipscomb HJ, Chen JC, Dement JM, Myers DJ, et al. Occupational injuries among aides and nurses in acute care. Am J Ind Med. (2009) 52:953–64. doi: 10.1002/ajim.20762
35. Rey-Merchán MDC, López-Arquillos A, Rey-Merchán AM. Characteristics of occupational injuries among spanish nursing workers. Healthcare. (2022) 10:220. doi: 10.3390/healthcare10020220
36. Lee SJ, Faucett J, Gillen M, Krause N, Landry L. Risk perception of musculoskeletal injury among critical care nurses. Nurs Res. (2013) 62:36–44. doi: 10.1097/NNR.0b013e31827334d6
37. Tak S, Sweeney MH, Alterman T, Baron S, Calvert GM. Workplace assaults on nursing assistants in US nursing homes: a multilevel analysis. Am J Public Health. (2010) 100:1938–45. doi: 10.2105/AJPH.2009.185421
38. D'Arcy LP, Sasai Y, Stearns SC. Do assistive devices, training, and workload affect injury incidence? Prevention efforts by nursing homes and back injuries among nursing assistants. J Adv Nurs. (2012) 68:836–45. doi: 10.1111/j.1365-2648.2011.05785.x
39. Julia M, Catalina-Romero C, Calvo-Bonacho E, Benavides FG. Exposure to psychosocial risk factors at work and the incidence of occupational injuries: a cohort study in Spain. J Occup Environ Med. (2016) 58:282–6. doi: 10.1097/JOM.0000000000000614
40. Rommel A, Varnaccia G, Lahmann N, Kottner J, Kroll LE. Occupational injuries in Germany: population-wide national survey data emphasize the importance of work-related factors [Research Support, Non-U S Gov't]. PLoS ONE. (2016) 11:e0148798. doi: 10.1371/journal.pone.0148798
41. Hanvold TN, Kines P, Nykänen M, Thomée S, Holte KA, Vuori J, et al. Occupational safety and health among young workers in the nordic countries: a systematic literature review. Saf Health Work. (2019) 10:3–20. doi: 10.1016/j.shaw.2018.12.003
42. Koranyi I, Jonsson J, Rönnblad T, Stockfelt L, Bodin T. Precarious employment and occupational accidents and injuries – a systematic review. Scand J Work Environ Health. (2018) 44:341–50. doi: 10.5271/sjweh.3720
43. Breslin FC, Dollack J, Mahood Q, Maas ET, Laberge M, Smith PM. Are new workers at elevated risk for work injury? A systematic review. Occupat Environ Med. (2019) 76:694–701. doi: 10.1136/oemed-2018-105639
44. Tucker P, Albrecht S, Kecklund G, Beckers DG, Leineweber C. Work time control, sleep & accident risk: a prospective cohort study. Chronobiol Int. (2016) 33:619–29. doi: 10.3109/07420528.2016.1167723
45. Seppala LJ, van de Glind EMM, Daams JG, Ploegmakers KJ, de Vries M, Wermelink A, et al. Fall-risk-increasing drugs: a systematic review and meta-analysis: III. others. J Am Med Direct Assoc. (2018) 19:372.e1–8. doi: 10.1016/j.jamda.2017.12.099
46. Biswas A, Harbin S, Irvin E, Johnston H, Begum M, Tiong M, et al. Sex and gender differences in occupational hazard exposures: a scoping review of the recent literature. Curr Environ Health Rep. (2021) 8:267–80. doi: 10.1007/s40572-021-00330-8
Keywords: workplace injuries, physical factors, psychosocial factors, co-exposure, care workers
Citation: Colin R, Wild P, Paris C and Boini S (2022) Co-exposures to physical and psychosocial work factors increase the occurrence of workplace injuries among French care workers. Front. Public Health 10:1055846. doi: 10.3389/fpubh.2022.1055846
Received: 28 September 2022; Accepted: 21 November 2022;
Published: 13 December 2022.
Edited by:
Kun-Shan Wu, Tamkang University, TaiwanCopyright © 2022 Colin, Wild, Paris and Boini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Régis Colin, cmVnaXMuY29saW5AaW5ycy5mcg==