
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 07 December 2022
Sec. Aging and Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1048496
This article is part of the Research TopicActive and Healthy Aging and Quality of Life: Interventions and Outlook for the FutureView all 53 articles
 Antonina Tcymbal1*
Antonina Tcymbal1* Karim Abu-Omar1
Karim Abu-Omar1 Verena Hartung1
Verena Hartung1 Annalena Bußkamp2
Annalena Bußkamp2 Chiara Comito2Christin Rossmann2
Chiara Comito2Christin Rossmann2 Diana Meinzinger1
Diana Meinzinger1 Anne Kerstin Reimers1
Anne Kerstin Reimers1Background: In recent years, there has been a global trend toward an increase in life expectancy and the proportion of elderly people among the population. In this regard, it becomes important to promote active and healthy aging. Physical inactivity and social isolation are both risk factors of many chronic illnesses and highly prevalent in older adults. This challenges communities to develop interventions that reduce these risk factors among elderly populations. The main aims of this study were to summarize community-based interventions that aim to simultaneously promote social participation and physical activity in older adults and to examine their effects.
Methods: We performed a systematic review based on the PRISMA standards. Literature searches were conducted in six scientific databases in July 2021. Articles were included if they had an interventional design, focused on older adults living in the community and measured social participation and physical activity as an outcome. The data were summarized narratively due to the heterogeneity of studies and the variety of outcome measures.
Results: Overall, 46 articles published in English were included. The studies were grouped in (1) interventions with main focus on physical activity promotion; (2) social activities that included a physical activity component; (3) health behavior interventions/ health education interventions; (4) multicomponent interventions; (5) environmental interventions. The majority of the reviewed studies reported positive effects of interventions on physical activity and/or social participation. No study reported negative effects. Analysis of quantitative studies showed that multicomponent interventions have great positive effects on both outcomes. In qualitative studies positive effects were found regardless of intervention type.
Conclusion: This review summarizes the evidence about the effects of community-based interventions that aim to promote social participation and physical activity in older adults. Multicomponent interventions seem to be most suitable for simultaneous promotion of physical activity and social participation. However, high variability in measurement methods used to assess both social participation and physical activity in the included studies made it difficult to compare studies and to indicate the most effective.
Systematic review registration: www.crd.york.ac.uk, identifier: PROSPERO [CRD42021268270].
Physical activity and social participation are both vital components of healthy aging. However, many older adults are less physically active (1) and integrated in their social surroundings than adults younger than 65 years (2). Thus, improving our understanding of how to simultaneously increase both physical activity and social participation among adults is important for promoting health in old age. This is especially relevant when considering demographic shifts which will result in the world's population of older people to double by 2050 (3), and with it, the burden of disease among older adults (4).
Regarding physical activity, there are irrefutable health benefits for older people to stay active (5). Based on such evidence, the World Health Organization has issued guidelines on physical activity and sedentary behavior for older people in 2020 (6). These guidelines state that individuals over the age of 65 years should engage in 150–300 min of moderate or 75–150 min of vigorous physical activity. Despite these recommendations, more than 50% of older people (age 80 years and older) worldwide remain physically inactive, with progress in increasing physical activity having largely plateaued in recent years (7).
A review of reviews suggests that interventions conducted among community dwelling older people can result in increases in physical activity (8). Farrance et al. (9) demonstrated that community-based exercise programs can result in long-term adherence rates of 70%. There is also some, albeit limited, evidence that volunteer-lead physical activity interventions can result in positive health outcomes for older people (10). Furthermore, among the same population, eHealth interventions have also shown to be effective in increasing physical activity levels (11). For community dwelling older adults receiving home care, however, the results of interventions to increase physical activity remain inconclusive (12). Altogether, these findings indicate the potential of community-based interventions for increasing physical activity of older adults.
In addition to physical activity, social participation also plays an important role in the health of older individuals. Currently there are overlapping definitions and operationalizations for the concepts of social participation, social capital, social support. Levasseur et al. reviewed and analyzed definitions of social participation within aging literature and suggested defining social participation as a “person's involvement in activities that provide interaction with others in society or the community” (13). Based on this definition, social capital and social support can be considered as consequences of successful social participation, while the absence of social participation can lead to feelings of isolation and loneliness.
Studies have demonstrated that being less socially isolated (14) and belonging to social groups (15) results in important health benefits. In this regard, Steffens et al. reports the effects of a feeling of belonging on mortality as being similar to the effects of physically activity (15). Face-to-face interactions have also been positively linked to the mental health of older adults (16).
Regarding interventions aimed at decreasing feelings of loneliness and increasing social participation, several reviews have provided evidence of their effectiveness. Nevertheless, the results reported in these reviews are inconclusive: Dickens et al. (17) reported that most interventions targeted at reducing loneliness among older people report at least one positive outcome. In 2005, a review by Cattan et al. revealed that social and educational interventions are suitable to decrease feelings of loneliness among older people (18). A review of interventions to increase social capital by Coll-Planas et al. (19), however, concluded that similar interventions did not reduce feelings of loneliness among older people, although high-quality trials showed positive effects on mental health within this target group. In contrast, Franck et al. (20) reported that three out of five trials were able to reduce loneliness among older adults receiving home care.
Social participation and physical activity among older adults may mutually reinforce each other. A review performed by Lindsay Smith et al. (21), shows that older adults who report receiving more social support (from family members) report higher levels of leisure-time physical activity than their counterparts receiving less support. Pels and Kleinert (22) concluded from their review that physical activity can contribute to a reduction in feelings of loneliness among older adults.
However, ways to simultaneously promote social participation and physical activity among this population group are still unclear. Until now, no systematic review has summarized the literature on interventions aiming to promote both simultaneously. It is currently unclear which types of interventions would optimize the effects of increased social participation and physical activity among older people. In addition, it is uncertain what types of interventions communities should offer to optimize these effects among community-dwelling older adults.
This review therefore sets out to investigate the effects of interventions aiming to simultaneously promote physical activity and social participation among community dwelling older adults. It focuses on studies that have been conducted within real-world community settings, to investigate the effectiveness of these interventions, and thus increase the external validity of the review's findings.
This review was commissioned by the Federal Centre for Health Education (Bundeszentrale für gesundheitliche Aufklärung; BZgA), Germany. The results of the review are intended to support the participatory project “Aging in Balance” (“Älter werden in Balance”; https://www.aelter-werden-in-balance.de). In the project, researchers and project officers from communities collaborate to establish structures for health and physical activity promotion for older people. It is the intention of this project to improve service offers for citizens and exchange good practice in this field. The results of this review are meant to provide guidance to communities on which services they should offer to increase social participation and physical activity among older people. Methods used to conduct this review were aligned to reach this objective by focusing on trials that were able to investigate effectiveness (by conducting the trial in real-world settings) rather than efficacy (by doing randomized controlled trials conducted in laboratory or field setting) (23).
This review was conducted according to the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) statement guidelines (24). The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (www.crd.york.ac.uk) on August 18, 2021, with the registration number CRD42021268270.
Inclusion and exclusion criteria were formulated based on the PICO approach (25). Only articles from peer-reviewed journals published in English or German that fulfilled the criteria described in the Table 1 were eligible.
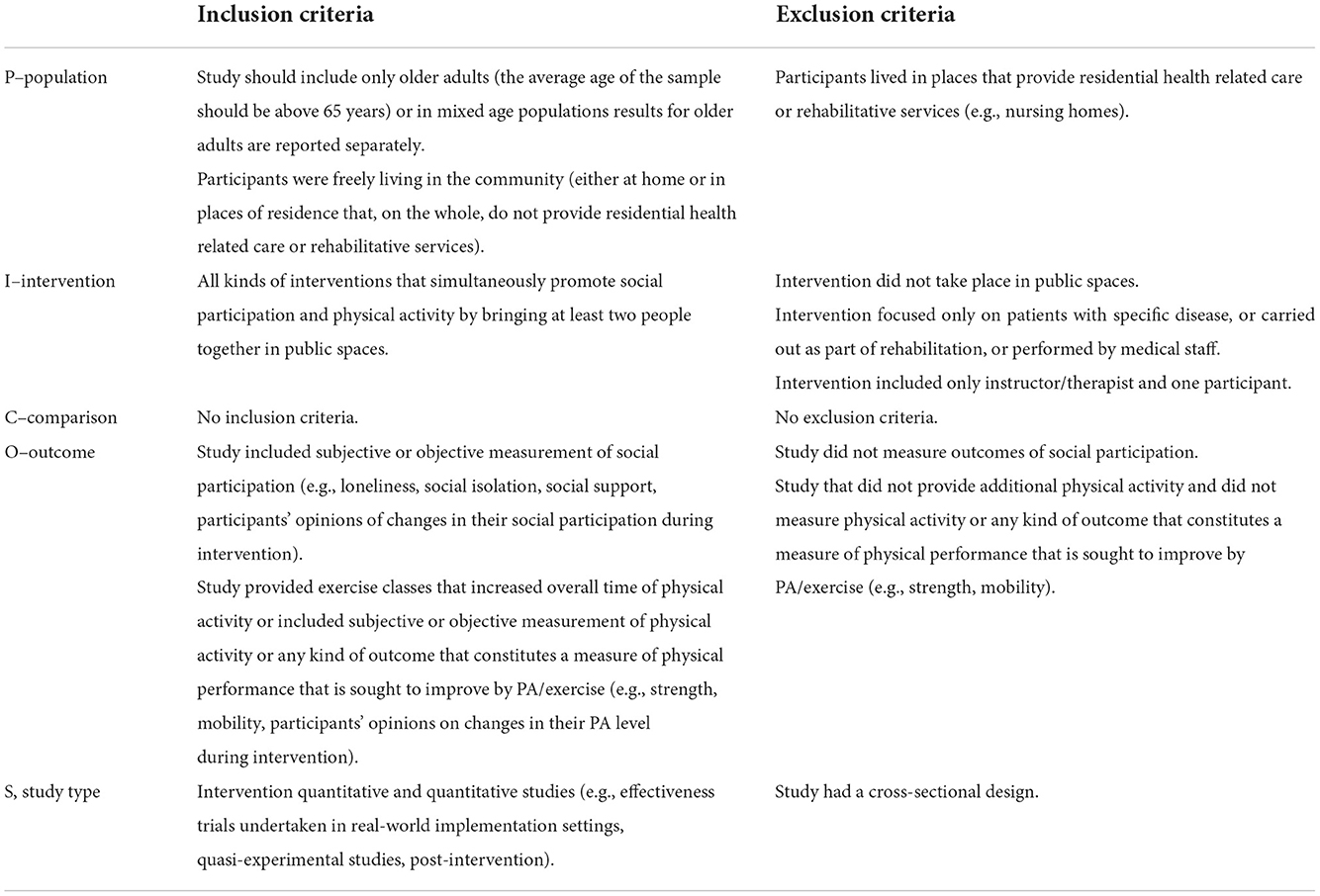
Table 1. Eligibility criteria.
A systematic search was performed on PubMed, CINAHL, SPORTDiscus, PsycINFO, Scopus, and Web of Knowledge in July 2021. By discussion with the research team members and project officers from communities of the project “Aging in Balance”, a comprehensive search strategy was developed using the PICO approach (25) with a combination of keywords in the categories study sample, intervention, and outcomes.
The search formula was as follows:
(“old people” OR “older people” OR elderly OR elders OR aging OR aging OR “old men” OR “old women” OR “older persons” OR “older adults” OR seniors)
AND (“physical activity” OR “physical activities” OR sport OR training OR exercise OR exercises OR fitness OR stretching OR flexibility OR strength OR resistance OR balance OR endurance OR aerobic OR mobility OR walking OR cycling OR yoga OR pilates OR dancing OR swimming OR jogging OR hiking OR “tai chi” OR taichi OR taijiquan OR gardening OR “qi gong” OR qigong)
AND (Intervention OR programme OR program OR trial)
AND (“social interaction” OR “social interactions” OR “social participation” OR “social support” OR “social network” OR “social networks” OR “social isolation” OR “social activity” OR “social activities” OR “social engagement” OR “social involvement” OR “social inclusion” OR “social life” OR loneliness OR “interpersonal communication” OR “interpersonal interaction” OR “interpersonal interactions” OR “interpersonal relationship” OR “interpersonal relationships” OR “community involvement” OR “community participation” OR “community life”).
Two reviewers independently screened and selected relevant articles using the Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia; www.covidence.org). The first stage consisted of screening titles and abstracts. Afterwards, full texts of potentially relevant articles were reviewed. If the title and/ or abstract indicated that the study fulfilled the eligibility criteria or did not provide sufficient information, both reviewers screened the full texts for eligibility. When necessary, Supplementary material were also assessed for additional information. Disagreements between the reviewers were discussed in the research team until a consensus was reached.
Data of included studies were extracted and summarized by one researcher, with verification by another reviewer, in order to reduce bias and error. Extraction included the following items: general study information (authors, year of publication, country), intervention description (name, type, duration, frequency, length of session, description of control conditions), sample characteristics (age, special conditions, functional status, activity status, language skills, sample size, mean age, proportion of females), type of collected data (quantitative, qualitative or mixed), quantitative (questionnaire, test, etc.) and/or qualitative (interview, focus groups) methods of measuring social participation and physical activity/fitness, results on effects of interventions on social participation and physical activity/fitness level.
The methodological quality of each study was assessed with the QualSyst tool- developed by the Alberta Heritage Foundation for Medical Research (26). This tool was chosen because it assists in the evaluation of intervention studies with different designs, including both qualitative and quantitative studies. Quantitative studies were evaluated according to the following 14 criteria: objective, study design, method of subject/comparison group selection, subject characteristics, intervention allocation, blinding, outcome measure definition, exposure measure definition, sample size, analytic methods, estimate of variance, control for confounding, reporting results and conclusions. For qualitative studies the tool provided the following ten criteria: objective, study design, context, connection to theoretical framework, sampling strategy, data collection, data analysis, verification procedure, conclusions, and reflexivity. Depending on the degree to which the specific criteria were met, each item was scored as “yes” = 2, “partial” = 1, or “no” = 0. If an item was not applicable to the study it was marked “N/A” and excluded from the summary score. The summary score (range: 0–1) indicates the risk of bias, with a higher score indicating higher quality and thus less risk of bias.
Before data analyses, the included interventions were grouped into five different intervention types that were defined based on a discussion with project officers from communities of the project “Aging in Balance”: (1) interventions which primarily focused on physical activity promotion; (2) social activities that included physical activity; (3) health education interventions; (4) environmental interventions; (5) multicomponent interventions. The criteria for classification are presented in Table 2. Associations between interventions and changes in social participation and physical activity/fitness level were analyzed for each type.
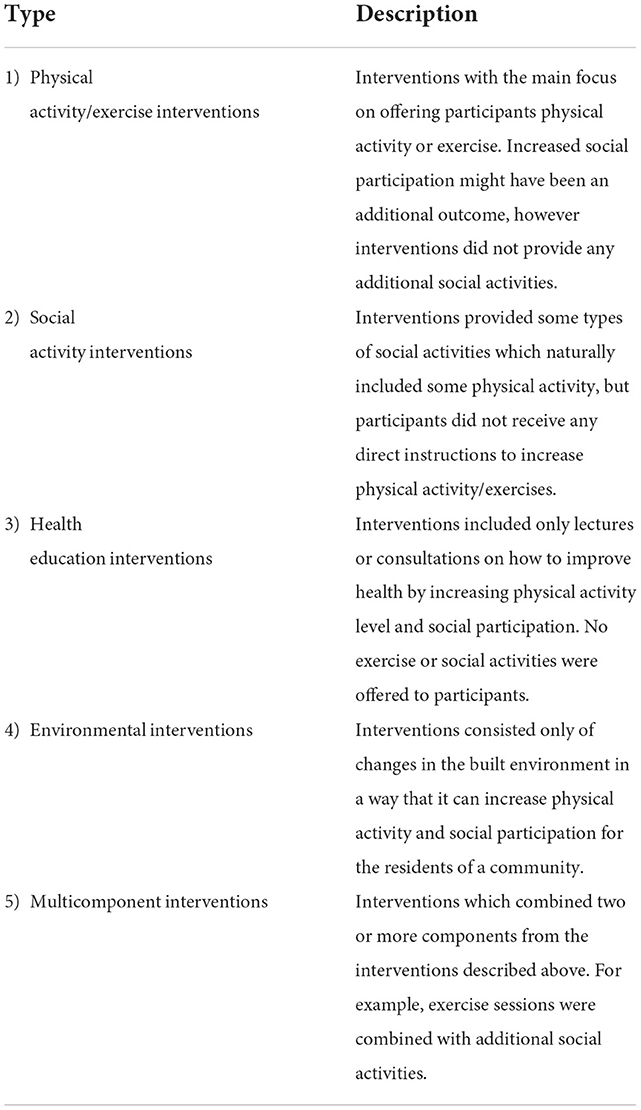
Table 2. Definition of intervention types.
The level of evidence within each type of interventions was summarized narratively due to the heterogeneity of studies and the variety of intervention contents and outcome measures, which prevented a quantitative meta-analysis. For the quantitative studies, we used an approach of summarizing results from studies with different designs that has been suggested by Sallis et al. (27) and also been used by Lindsay Smith et.al (21) in a systematic review with a similar topic. Using this approach, each study was rated as + or –, depending on if a statistically significant positive or negative effect of an intervention was found, and as 0 if no statistically significant associations were found. Ratings were assigned separately for effects on social participation and physical activity/fitness level. Overall ratings for quantitative studies in each category were calculated as “0” (No association; 0–33% of the findings supported the association), “?” (indeterminate association; 34–59% of the findings supported the positive or negative association), “+” or “–” (positive or negative association; 60–100% of the findings supported the association).
Electronic searches across the six databases identified 11,900 records, 7,935 remained after removing duplicates. The titles and abstracts were assessed for relevance based on eligibility criteria, resulting in 262 papers retrieved for full text review. After the full text screening, 56 papers met the inclusion criteria. Of these articles, 46 were written in English or German (languages spoken by at least two members of the research team) and included in the analysis. The selection process is presented in a PRISMA flow-diagram (see Figure 1). Characteristics of the included studies are shown as a structured table (see Table 3) and as a narrative summary (see Appendix 1).
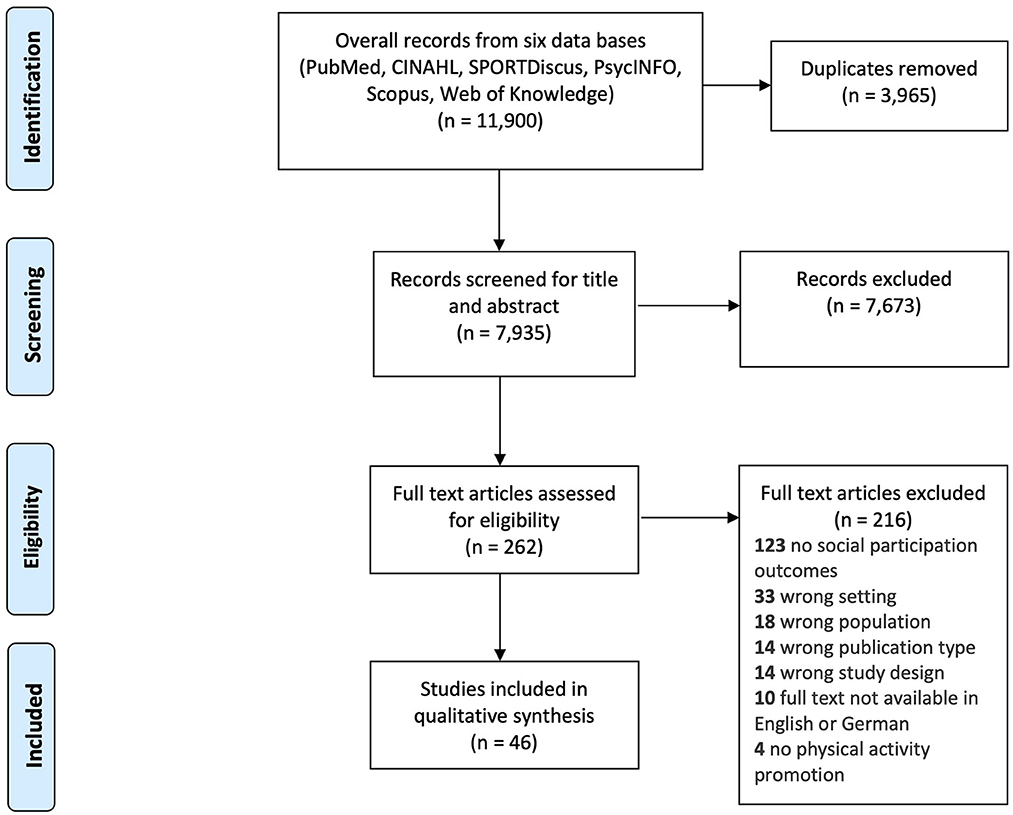
Figure 1. PRISMA flow-diagram of the study selection process.
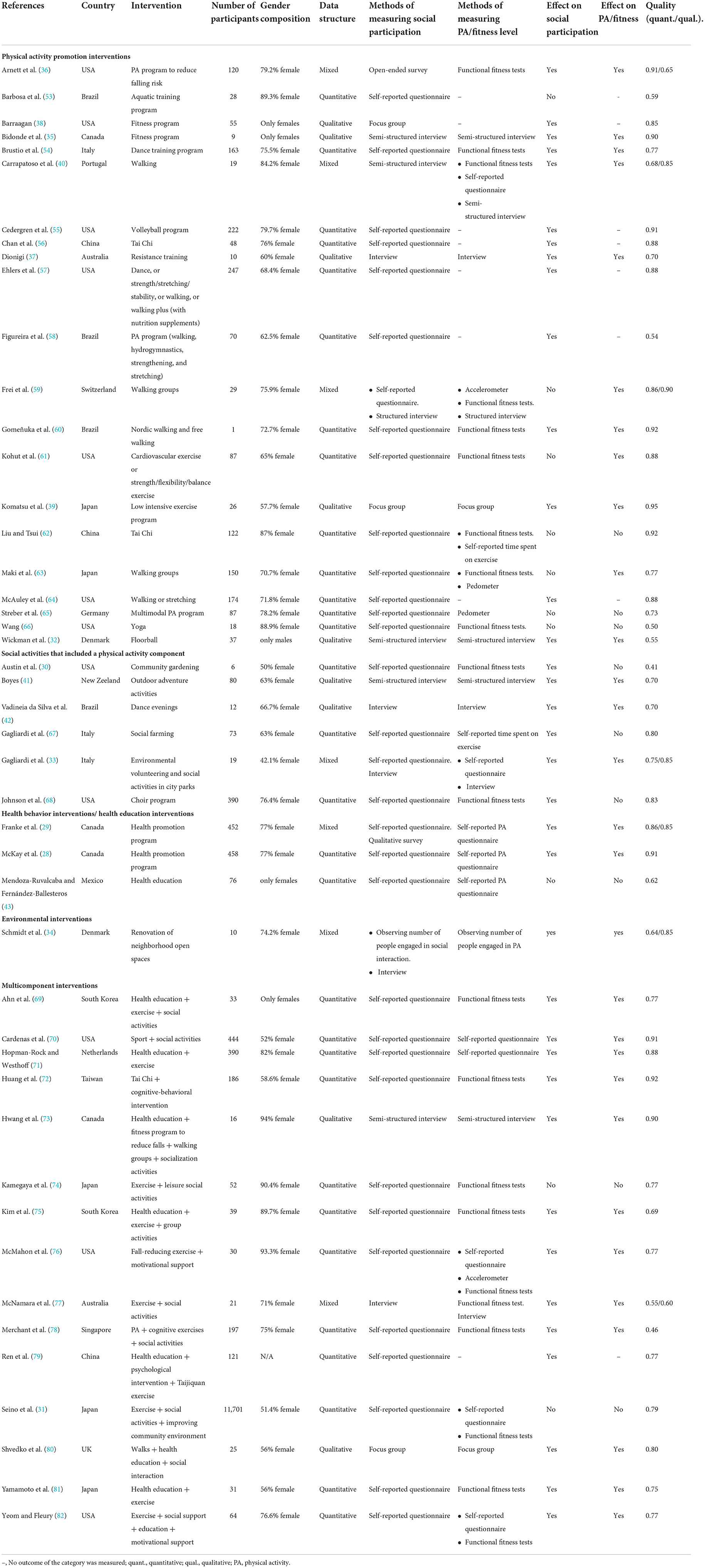
Table 3. Studies overview.
The 46 papers in this review included reports from 45 studies [McKay et al. and Franke et al. analyzed the same data with different methods (28, 29)]. The included articles were published between 2002 and 2021. Sixteen studies were conducted in North American countries, 12 in Asian countries, ten in European countries, four in Brazil, two in Australia, and one in New Zeeland. There was a total of 16,285 participants across 45 studies, ranging from six (30) to 11,701 (31) per study. The majority of participants were females. There were four studies which consisted solely of female participants, and in 18 studies females made up 75% or more of the sample. Meanwhile, just one intervention was designed exclusively for men (32) and only one further study consisted of more men than women (33). This review included 29 quantitative studies, nine qualitative studies, and seven mixed-methods studies. The way social participation and physical activity were measured and analyzed varied widely between studies.
Out of the studies which used quantitative methods, 32 applied different self-reported questionnaires to assess post-intervention changes in social participation. In one study, researchers counted the number of participants engaged in social interaction before and after changing the built environment (34). From studies using qualitative methods, nine performed interviews and three conducted focus groups to let participants describe their experiences and perceived changes in social participation during the interventions.
The most common methods of measuring a change in physical activity/fitness level, among the studies which employed quantitative methods, were functional fitness tests (21 studies) and self-reported physical activity questionaries (12 studies). Two studies used accelerometers to objectively assess time spent on physical activity and two studies used pedometers to objectively measure daily steps. Nine studies used interviews and two organized focus groups to gather participants experiences with changes in their physical activity/fitness level. Eight studies engaged participants in extra physical activity without measuring changes in physical activity levels.
The average quality score of included studies was 0.77 (0.76 for quantitative studies and 0.78 for qualitative studies) with a range of 0.41–0.95. In most of the quantitative studies, the research question, objective, analysis, and results were sufficiently described and the study design was appropriate. The main sources of bias were related to randomization, blinding of investigators, confounding, and subject selection. The quality of some quantitative studies suffered from poor sample representativeness or lack of a control group. In all qualitative studies, the context of study was well-described, and the conclusions were supported by results. The research question, design, and connection to a theoretical framework were also sufficiently presented in the majority of the studies. The main sources of bias for qualitative studies were related to sampling strategy and absence of reflexivity on how researcher's personal characteristics and methods could have impacted obtained data. Quality scores of the individual studies are reported in Table 3.
The majority of the reviewed quantitative studies reported interventions having a statistically significant positive effect on social participation (23 studies) and physical activity (18 studies). All qualitative studies showed positive effects on perceived social participation and on the physical activity/fitness levels of the participants. There were no studies which reported negative effects.
The studies were grouped as (1) interventions which primarily focused on physical activity promotion; (2) social activities that included physical activity; (3) health education interventions; (4) environmental interventions; (5) multicomponent interventions. The results of quantitative studies by intervention types are presented in the Table 4.
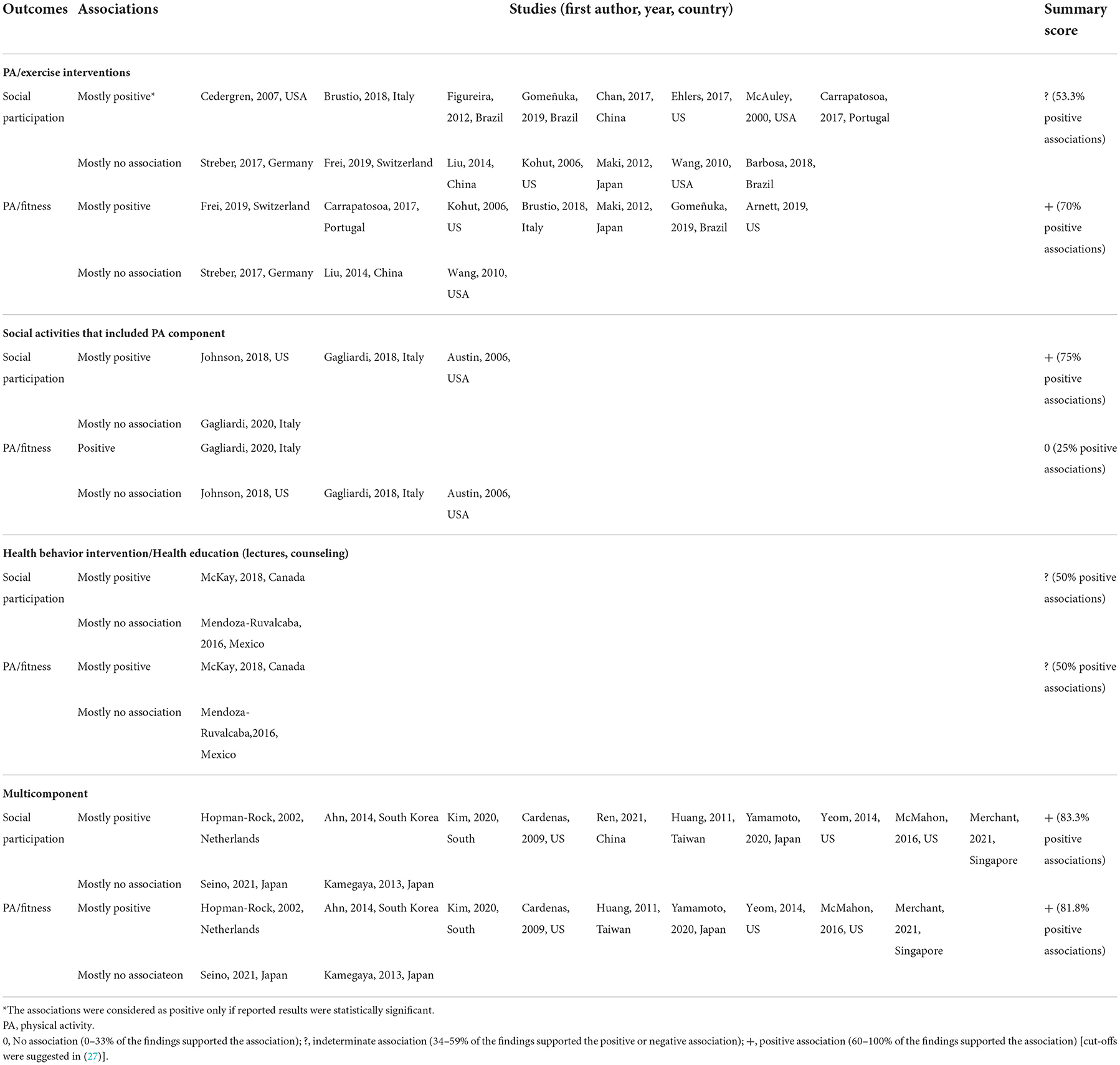
Table 4. Summary of quantitative studies results.
Of the included studies, 21 described interventions which focused primarily on providing different types of physical activity, and also measured intervention effects on social participation among older individuals. Studies included a total of 1,722 participants. Most of the studies (13 studies) used quantitative methods, five used qualitative methods, and three used mixed methods. During the interventions, participants performed different types of physical activity including walking, dancing, tai chi, fall prevention training, aquatic training, volleyball, and others (see Table 3).
Positive effects of the physical activity interventions on physical activity and fitness outcomes were observed and reported in 70% of the quantitative studies (see Table 4). The effects of the interventions on social participation, however, were not as obvious (53.3% of quantitative studies reported positive associations). In the qualitative studies, participants reported that involvement in the programs gave them the opportunity to get out and be among other people with similar experiences (32, 35), feel more social engagement and social support (36, 37), be more socially connected (38, 39), and expand their communication beyond the group exercise (39). In the participants' opinion, physical activity programs also helped them to improve their physical performance in everyday life (e.g., strength, endurance, balance, coordination) (32, 35, 37, 39, 40).
Six of the reviewed studies, including 580 participants, presented the results of interventions which focused on performing different social activities with a physical activity component. These activities included social farming, community gardening, a choir program, dance evenings, outdoor adventure activities, environmental volunteering, and social activities in city parks.
From the four studies that used quantitative methods, three (75%) reported positive effects of the interventions on social participation outcomes; only one study, however, reported positive effects on physical activity/fitness outcomes (33). Qualitative analysis showed that participants noticed improvements in their social participation and felt that the interventions helped them to become more physically active (33, 41, 42).
Two studies, including a total of 534 participants, examined interventions that promoted physical activity and social participation solely through lectures or consultation. McKay et al. and Franke et al. reported the results of the health promotion program “Choose to Move”, which included consultations with active coaches, motivational meetings, and telephone support (28, 29). Mendoza-Ruvalcaba et al. described the results of “the Vital Aging” program to promote active aging through teaching basic knowledge about aging, and promoting healthy lifestyles (43). McKay et al. and Mendoza-Ruvalcaba et al. collected quantitative data and Franke et al. used a mixed methods approach. The results showed that the effects of health education interventions on social participation and physical activity/fitness outcomes are rather unclear. While the “Choose to Move” program showed positive effects on both social participation and physical activity, the “Vital Aging” program had no effect on either of these outcomes.
Schmidt et al. presented the results of the environmental intervention “Move the Neighborhood” a program based on a participatory research approach, which aimed to increase the use of neighborhood open spaces to promote active living through social interaction and physical activity (34). Together with landscape architects, local older adults explored and developed ideas on how to improve neighborhood open spaces. Renovations were later implemented based on the results of this collaboration. To evaluate the effects of renovations on older adults, authors used a mixed methods approach. They gathered data on the amount of older people engaged in social interaction and physical activity in renovated areas and conducted qualitative interviews with older people to see how these renovations affected social interaction. The environmental intervention study showed that renovating the neighborhood open spaces had some positive effects on social participation and physical activity.
Interventions which combined two or more different components from other approaches (physical activity/exercise, social activities, health education, environment changes) were classified as multicomponent: 15 such studies, with a total of 13,350 participants, were reviewed. All 15 included some form of exercise or physical activity. In addition, ten interventions included social group activities, six studies organized health education, five studies provided psychological or motivation support, and in one study improvements were made to the built environment.
Analysis of the quantitative studies showed that when compared to the other intervention groups, multicomponent interventions had a greater positive effect on both social participation outcomes (81.8% of studies) and physical activity/fitness outcomes (80% of studies). The results of the qualitative studies support this finding.
This review has summarized evidence on the effects of community-based interventions which aimed to promote social participation and physical activity in older adults. It focused on trials conducted within the communities. To the best of our knowledge, this is the first review that focused on investigating the effectiveness, rather than efficacy, of intervention studies. While this approach led to the inclusion of some studies with lower scientific evidence, it also describes the interventions used in real-world conditions, in as much as possible. Based on this, we are able to form recommendations for communities (see below).
This review summarized results from various intervention study designs including pre- and post-test, retrospective, controlled trials and randomized controlled trials. A variety of intervention types were identified and allocated to the physical activity interventions, social activities that included physical activity, health education intervention, environmental interventions, and multicomponent interventions.
The majority of quantitative studies reported positive effects of interventions on social participation (68% of studies) and physical activity (67% of studies). All included qualitative studies reported that participants believed the interventions had had positive effects on their physical activity and social participation. It could be argued that this is due to the fact that quantitative measures might often be less sensitive to change. However, it could also be disputed that qualitative inquiry is more prone to socially desirable answers.
Our findings that interventions promoting social participation and physical activity can have positive effects on older adults are in line with findings of other reviews on similar topics (8, 17, 44). The classification of interventions into different types made it possible to identify approaches that more often reported statistically significant positive changes in physical activity and social participation of participants. Interventions that provided only physical activity/exercise activities often showed more positive effects on physical activity/fitness outcomes, rather than on social participation, which is in line with the findings from another review (45). The majority of interventions which focused on social activities had positive effects on social participation outcomes and nearly no effect on physical activity/fitness levels. The effect of health education interventions is rather unclear. It was impossible to make a comparison regarding environmental interventions, since only one such study with a small number of participants (ten older adults) has been identified. Further research needs to be done on these types of interventions in the future. In agreement with the review from Zubala et al. (8), we found that in quantitative studies on multicomponent interventions, more than 80% reported statistically significant effects on both social participation and physical activity/fitness outcomes – the highest result among all intervention types. This is in line with principles of ecological perspectives on health behavior change (46).
We observed a high variability in measures on physical activity and social participation outcomes across trials. This finding is in line with previous reviews on similar topics (17, 44) and this fact prevents comparisons between studies and interventions. This heterogeneity allowed us to summarize data only narratively and prevented a quantitative meta-analysis.
The methodological quality of the studies was also very heterogeneous, which has previously been noted in other reviews on similar topics (18, 44). The methodological quality of the reviewed studies was limited due to a lack of appropriate control conditions, consideration of cofounders and poor sample representatives (small number of participants, high loss to follow-up). There were many trials that reported on a small number of participants. In quantitative studies, randomization, confounding, and subject selection were often poorly described. In qualitative studies, authors often did not reflect on how the personal characteristics of researchers and their methods could have impacted the obtained data. Blinding of the participants was often not implemented as it is in general complicated for physical activity interventions. From the 23 studies where blinding of investigators was potentially possible, less than half (ten studies) used this opportunity and at least partly described the process. It is recommended that future studies find a way to blind at least investigators when it is possible.
More than 70% of participants in the reviewed studies were female and there seemed to be few interventions that particularly target males. Consequently, women seem to be overrepresented in the studies, even when considering that with 55% of the global population aged 65 years or over women comprise a majority of older persons worldwide (47). This might also be due to the fact that older women are much more likely to attend health prevention programs and community-based health screening programs than older men (48, 49). In a study from Sims-Gould et al. male participants reported that knowing that other men are also participating in a program is an important and attractive feature (50). The development and evaluation of programs which are more geared toward men or which are of more interest to a male audience, such as the “Men's Sheds” (51), can be suggested as a direction for future research.
The included studies did not specifically address minorities and socially disadvantaged groups or report data regarding potential health disparities (52). Thus, it remains unclear whether these interventions are suitable to prevent health inequalities or, on the other hand, if they might potentially widen the health gap between advantaged and disadvantaged groups of older people.
Our main findings can be framed as recommendations to project officers working in communities to provide services to older people. Considering the findings of our review and the varied effectiveness of the different types of interventions to increase social participation and physical activity, certain (although preliminary) conclusions can be drawn:
• Health behavior and health education interventions that predominantly rely on lecturing and counseling do not work well. This type of interventions should only be conducted when there are special occasions that warrant this.
• Physical activity/exercise interventions increase physical activity, and social activities interventions increase social participation. Depending on the aim, one can choose which of the two to conduct accordingly.
• Physical activity/exercise interventions are more likely to increase social participation than social activity interventions are to increase physical activity. Due to the additional health benefits that come through physical activity/exercise interventions, these interventions might be a “best buy” for older people who are not too frail to participate in a physical activity program.
• Multicomponent interventions that combine social and physical activities had the highest rate of statistically positive results in comparison with other types of interventions. Services which are able to combine these different types of activities (e.g., health education, physical activity, and environmental measures) may be most beneficial.
• Specific efforts are required to reach minority or socially disadvantaged populations to prevent health inequalities and pursue health equity. Additionally, interventions specifically addressing the needs and interests of men are needed to attract this target group.
The decisive factors in choosing the type of intervention are undoubtedly the resources existing in the community and the characteristics of the population living in it. However, we recommend that communities take other factors into account that may generally contribute to or, conversely, hinder the implementation and promotion of such interventions. Organizers should consider in advance: the strategies for attracting participants to the program, the availability of the program venue, and the number and the necessary number of staff to conduct regular classes (50).
To the best of our knowledge, this is the first review focused on the effectiveness of interventions aiming to simultaneously promote physical activity and social participation among community-dwelling older people. The systematic search of relevant studies, with various study designs, was conducted in six electronic databases, and the methodological quality (risk of bias) was evaluated for all included studies. We see it as a strength of our study, that we were able to include 45 trials and draw some, although limited, conclusions regarding the effectiveness of different types of interventions.
We faced certain difficulties when conducting the review. From the outset, it was decided that an effectiveness review would need to be conducted, rather than an efficacy review (23). We were thus interested in trials that had been conducted in real-world settings, with free-living populations. This turned out to be difficult to determine for some studies, since the contexts within which trials were conducted and the recruitment of participants were sometimes ambiguously described.
Distinguishing between physical activity/exercise, social activities including physical activity, health education, and multicomponent interventions in the analysis was challenging, and for some interventions might have resulted in classifications that could be disputed. This was partially due to the fact that, like in other health behavior reviews, interventions were sometimes described only cursorily. This type of classification can also be regarded as being somewhat arbitrary. A dance class for example could, depending on one's perspective, be classified as an exercise intervention, a social activity, or a multicomponent intervention. We attempted, however, to describe the content of the intervention since it was our intention to provide project officers with some guidance on what to do. Additionally, most trials did not focus on minority or socially disadvantaged populations. This limits the generalizability of our findings.
This systematic review focused only on the effects of the interventions and did not provide information on the implementation process, such as how participants were recruited, drop-off rates, or protentional challenges. It could be recommended to focus on implementation effectiveness in further research.
This systematic review sheds light on the effectiveness of community-based programs promoting physical activity and social participation for older people. Notwithstanding the large variability in study designs and measurements, overall, the findings from this review show that among the existing interventions there are some that can simultaneously increase physical activity and improve social participation among older people. The evidence also highlights multicomponent interventions' higher probability to show positive effects. The analyzed studies allowed for the formulation of some recommendations for communities who aim to promote physical activity and social participation in older adults. Further research on the effectiveness of interventions is recommended, especially in the field of rarely studied interventions, such as environmental interventions.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
AT and VH conducted the literature search. AT, KA-O, and VH performed abstract/title screening, full-text selection, and data extraction. DM participated in the quality assessment. AT and KA-O analyzed data and summarized results. AT and KA-O with support from DM prepared a first draft of the manuscript. VH, AB, CC, CR, and AR critically revised the draft. AR supervised this work. All authors contributed to conceptualization of the study and approved the final manuscript.
This research was financed by the Federal Centre for Health Education (BZgA), which had no influence on the content of this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1048496/full#supplementary-material
1. Macera CA, Cavanaugh A, Bellettiere J. State of the art review: physical activity and older adults. Am J Lifestyle Med. (2017) 11:42–57. doi: 10.1177/1559827615571897
2. Coyle CE, Dugan E. Social isolation, loneliness and health among older adults. J Aging Health. (2012) 24:1346–63. doi: 10.1177/0898264312460275
3. World Health Organization. Ageing and Health (2021). Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed July 15, 2021).
4. Sleeman KE, de Brito M, Etkind S, Nkhoma K, Guo P, Higginson IJ, et al. The escalating global burden of serious health-related suffering: projections to 2060 by world regions, age groups, and health conditions. Lancet Glob Health. (2019) 7:e883–e92. doi: 10.1016/S2214-109X(19)30172-X
5. McPhee JS, French DP, Jackson D, Nazroo J, Pendleton N, Degens H. Physical activity in older age: perspectives for healthy ageing and frailty. Biogerontology. (2016) 17:567–80. doi: 10.1007/s10522-016-9641-0
6. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
7. Sallis JF, Bull F, Guthold R, Heath GW, Inoue S, Kelly P, et al. Progress in physical activity over the Olympic quadrennium. Lancet. (2016) 388:1325–36. doi: 10.1016/S0140-6736(16)30581-5
8. Zubala A, MacGillivray S, Frost H, Kroll T, Skelton DA, Gavine A, et al. Promotion of physical activity interventions for community dwelling older adults: a systematic review of reviews. PLoS ONE. (2017) 12:e0180902. doi: 10.1371/journal.pone.0180902
9. Farrance C, Tsofliou F, Clark C. Adherence to community based group exercise interventions for older people: a mixed-methods systematic review. Prev Med. (2016) 87:155–66. doi: 10.1016/j.ypmed.2016.02.037
10. Lim SER, Cox NJ, Tan QY, Ibrahim K, Roberts HC. Volunteer-led physical activity interventions to improve health outcomes for community-dwelling older people: a systematic review. Aging Clin Exp Res. (2021) 33:843–53. doi: 10.1007/s40520-020-01556-6
11. Jonkman NH, van Schooten KS, Maier AB, Pijnappels M. eHealth interventions to promote objectively measured physical activity in community-dwelling older people. Maturitas. (2018) 113:32–9. doi: 10.1016/j.maturitas.2018.04.010
12. Burton E, Farrier K, Galvin R, Johnson S, Horgan NF, Warters A, et al. Physical activity programs for older people in the community receiving home care services: systematic review and meta-analysis. Clin Interv Aging. (2019) 14:1045–64. doi: 10.2147/CIA.S205019
13. Levasseur M, Richard L, Gauvin L, Raymond E. Inventory and analysis of definitions of social participation found in the aging literature: proposed taxonomy of social activities. Soc Sci Med (1982). (2010) 71:2141–9. doi: 10.1016/j.socscimed.2010.09.041
14. Gale CR, Westbury L, Cooper C. Social isolation and loneliness as risk factors for the progression of frailty: the English Longitudinal Study of Ageing. Age Ageing. (2018) 47:392–7. doi: 10.1093/ageing/afx188
15. Steffens NK, Cruwys T, Haslam C, Jetten J, Haslam SA. Social group memberships in retirement are associated with reduced risk of premature death: evidence from a longitudinal cohort study. BMJ Open. (2016) 6:e010164. doi: 10.1136/bmjopen-2015-010164
16. Teo AR, Choi H, Andrea SB, Valenstein M, Newsom JT, Dobscha SK, et al. Does mode of contact with different types of social relationships predict depression in older Adults? Evidence from a Nationally Representative Survey. J Am Geriatr Soc. (2015) 63:2014–22. doi: 10.1111/jgs.13667
17. Dickens AP, Richards SH, Greaves CJ, Campbell JL. Interventions targeting social isolation in older people: a systematic review. BMC Public Health. (2011) 11:647. doi: 10.1186/1471-2458-11-647
18. Cattan M, White M, Bond J, Learmouth A. Preventing social isolation and loneliness among older people: a systematic review of health promotion interventions. Ageing Soc. (2005) 25:41–67. doi: 10.1017/S0144686X04002594
19. Coll-Planas L, Del Valle Gómez G, Bonilla P, Masat T, Puig T, Monteserin R. Promoting social capital to alleviate loneliness and improve health among older people in Spain. Health Soc Care Community. (2017) 25:145–57. doi: 10.1111/hsc.12284
20. Franck L, Molyneux N, Parkinson L. Systematic review of interventions addressing social isolation and depression in aged care clients. Qual Life Res. (2016) 25:1395–407. doi: 10.1007/s11136-015-1197-y
21. Lindsay Smith G, Banting L, Eime R, O'Sullivan G, van Uffelen JGZ. The association between social support and physical activity in older adults: a systematic review. Int J Behav Nutr Phys Act. (2017) 14:56. doi: 10.1186/s12966-017-0509-8
22. Pels F, Kleinert J. Loneliness and physical activity: a systematic review. Int Rev Sport Exerc Psychol. (2016) 9:231–60. doi: 10.1080/1750984X.2016.1177849
23. Flay BR. Efficacy and effectiveness trials (and other phases of research) in the development of health promotion programs. Prev Med. (1986) 15:451–74. doi: 10.1016/0091-7435(86)90024-1
24. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
25. Aslam S, Emmanuel P. Formulating a researchable question: a critical step for facilitating good clinical research. Indian J Sex Transm Dis AIDS. (2010) 31:47–50. doi: 10.4103/0253-7184.69003
26. Kmet LM, Lee RC, Cook LS. Standard Quality Assessment Criteria for Evaluating Primary Research Papers From a Variety of Fields. Edmonton: Alberta Heritage Foundation for Medical Research (AHFMR) (2004).
27. Sallis JF, Prochaska JJ, Taylor WC, A. review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. (2000) 32:963–75. doi: 10.1097/00005768-200005000-00014
28. McKay H, Nettlefold L, Bauman A, Hoy C, Gray SM, Lau E, et al. Implementation of a co-designed physical activity program for older adults: positive impact when delivered at scale. BMC Public Health. (2018) 18. doi: 10.1186/s12889-018-6210-2
29. Franke T, Sims-Gould J, Nettlefold L, Ottoni C, McKay HA. “It makes me feel not so alone”: features of the Choose to Move physical activity intervention that reduce loneliness in older adults. BMC Public Health. (2021) 21:312. doi: 10.1186/s12889-021-10363-1
30. Austin EN, Johnston YAM, Morgan LL. Community gardening in a senior center: a therapeutic intervention to improve the health of older adults. Ther Recreat J. (2006) 40:48–56.
31. Seino S, Tomine Y, Nishi M, Hata T, Fujiwara Y, Shinkai S, et al. Effectiveness of a community-wide intervention for population-level frailty and functional health in older adults: a 2-year cluster nonrandomized controlled trial. Prev Med. (2021) 149:106620. doi: 10.1016/j.ypmed.2021.106620
32. Wikman JM, Nistrup A, Vorup J, Pedersen MT, Melchor PS, Bangsbo J, et al. The effect of floorball training on health status, psychological health and social capital in older men. AIMS Public Health. (2017) 4:364–82. doi: 10.3934/publichealth.2017.4.364
33. Gagliardi C, Pillemer K, Gambella E, Piccinini F, Fabbietti P. Benefits for older people engaged in environmental volunteering and socializing activities in city parks: preliminary results of a program in Italy. Int J Environ Res Public Health. (2020) 17. doi: 10.3390/ijerph17113772
34. Schmidt T, Pawlowski CS, Kerr J, Schipperijn J. Investigating the WHAT and WHY on older adults' use of neighborhood open spaces following an environmental intervention. Transl Behav Med. (2021) 11:582–96. doi: 10.1093/tbm/ibaa004
35. Bidonde Mj, Goodwin DL, Drinkwater DT. Older women's experiences of a fitness program: the importance of social networks. J Appl Sport Psychol. (2009) 21(Suppl. 1):S86–101. doi: 10.1080/10413200802595963
36. Arnett M, Toevs SE, Bond L, Hannah E. Outcomes of participation in a community-based physical activity program. Front Public Health. (2019) 7:225. doi: 10.3389/fpubh.2019.00225
37. Dionigi R. Resistance training and older adults' beliefs about psychological benefits: the importance of self-efficacy and social interaction. J Sport Exerc Psychol. (2007) 29:723–46. doi: 10.1123/jsep.29.6.723
38. Barragan C. Social relationships and the importance of community-based fitness programs (cbfp). J Women Aging. (2021) 33:428–41. doi: 10.1080/08952841.2021.1915685
39. Komatsu H, Yagasaki K, Saito Y, Oguma Y. Regular group exercise contributes to balanced health in older adults in Japan: a qualitative study. BMC Geriatr. (2017) 17. doi: 10.1186/s12877-017-0584-3
40. Carrapatoso S, Silva P, Purakom A, Novais C, Colaço P, Carvalho J. The experience of older adults in a walking program at individual, interpersonal, and environmental levels. Act Adapt Aging. (2017) 41:72–86. doi: 10.1080/01924788.2016.1272393
41. Boyes M. Outdoor adventure and successful ageing. Ageing Soc. (2013) 33:644–65. doi: 10.1017/S0144686X12000165
42. Vadineia da Silva M, Alves Lima D, da Conceição Silva TM, de Carvalho Melo TMT, Pereira da Cunha V, Pessoa da Silva MN. Dance: a therapeutic resource in the third age. J Nurs UFPE. 10:232–8. doi: 10.5205/reuol.7901-80479-1-SP.1001sup201606
43. Mendoza-Ruvalcaba NM, Fernández-Ballesteros R. Effectiveness of the vital aging program to promote active aging in Mexican older adults. Clin Interv Aging. (2016) 11:1631–44. doi: 10.2147/CIA.S102930
44. Gardiner C, Geldenhuys G, Gott M. Interventions to reduce social isolation and loneliness among older people: an integrative review. Health Soc Care Commun. (2018) 26:147–57. doi: 10.1111/hsc.12367
45. Shvedko A, Whittaker AC, Thompson JL, Greig CA. Physical activity interventions for treatment of social isolation, loneliness or low social support in older adults: a systematic review and meta-analysis of randomised controlled trials. Psychol Sport Exerc. (2018) 34:128–37. doi: 10.1016/j.psychsport.2017.10.003
46. Sallis JF, Owen N, Fisher E. Ecological models of health behavior. In:Glanz K, Rimer BK, Viswanath K, , editors, Health Behavior: Theory, Research, and Practice. San Francisco, CA: Jossey-Bass (2015). p. 43–64.
47. United Nations. World Population Ageing 2020 Highlights. (2020). Available from: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/files/documents/2020/Sep/un_pop_2020_pf_ageing_10_key_messages.pdf (accessed July 15, 2021).
48. Dryden R, Williams B, McCowan C, Themessl-Huber M. What do we know about who does and does not attend general health checks? Findings from a narrative scoping review. BMC Public Health. (2012) 12:723. doi: 10.1186/1471-2458-12-723
49. Jordan S, Lippe Evd. Teilnahme an Verhaltenspräventiven Maßnahmen. Robert Koch-Institut, Epidemiologie und Gesundheitsberichterstattung, Berlin (2013).
50. Sims-Gould J, Franke T, Lusina-Furst S, McKay HA. Community health promotion programs for older adults: what helps and hinders implementation. Health Sci Rep. (2020) 3:e144. doi: 10.1002/hsr2.144
51. Age UK. Help The Shed. (2021). Available from: https://www.ageuk.org.uk/exeter/our-services/men-in-sheds/help-the-shed/ (accessed December 10, 2021).
52. Braveman P. What are health disparities and health equity? We need to be clear. Public Health Rep. (2014) 129(1_suppl2):5–8. doi: 10.1177/00333549141291S203
53. Barbosa BT, Da Silva RLS, De Meneses ABC, Brindeiro-Neto W, Bacurau TP, De Souza Rocha AIS, et al. Self-related quality of life of elderly submitted to a 12-week aquatic training program. J Hum Sport Exerc. (2019) 14:281–91. doi: 10.14198/jhse.2019.142.03
54. Brustio PR, Liubicich ME, Chiabrero M, Rabaglietti E. Dancing in the golden age: a study on physical function, quality of life, and social engagement. Geriatr Nurs. (2018) 39:635–9. doi: 10.1016/j.gerinurse.2018.04.013
55. Cedergren A, King KA, Wagner DI, Wegley S. Perceived social health benefits among participants in a countrywide senior chair volleyball program. Act Adapt Aging. (2007) 31:23–36. doi: 10.1300/J016v31n04_02
56. Chan AW Yu DS, Choi KC. Effects of tai chi qigong on psychosocial well-being among hidden elderly, using elderly neighborhood volunteer approach: a pilot randomized controlled trial. Clin Interv Aging. (2017) 12:85–96. doi: 10.2147/CIA.S124604
57. Ehlers DK, Daugherty AM, Burzynska AZ, Fanning J, Awick EA, Chaddock-Heyman L, et al. Regional brain volumes moderate, but do not mediate, the effects of group-based exercise training on reductions in loneliness in older adults. Front Aging Neurosci. (2017) 9:110. doi: 10.3389/fnagi.2017.00110
58. Figueira HA, Figueira AA, Cader SA, Guimarães AC, De Oliveira RJ, Figueira JA, et al. Effects of a physical activity governmental health programme on the quality of life of elderly people. Scand J Public Health. (2012) 40:418–22. doi: 10.1177/1403494812453885
59. Frei A, Dalla Lana K, Radtke T, Stone E, Knöpfli N, Puhan MA, et al. novel approach to increase physical activity in older adults in the community using citizen science: a mixed-methods study. Int J Public Health. (2019) 64:669–78. doi: 10.1007/s00038-019-01230-3
60. Gomeñuka NA, Oliveira HB, Silva ES, Costa RR, Kanitz AC, Liedtke GV, et al. Effects of Nordic walking training on quality of life, balance and functional mobility in elderly: a randomized clinical trial. PLoS ONE. (2019) 14:e0211472. doi: 10.1371/journal.pone.0211472
61. Kohut ML, McCann DA, Russell DW, Konopka DN, Cunnick JE, Franke WD, et al. Aerobic exercise, but not flexibility/resistance exercise, reduces serum IL-18, CRP, and IL-6 independent of β-blockers, BMI, and psychosocial factors in older adults. Brain Behav Immun. (2006) 20:201–9. doi: 10.1016/j.bbi.2005.12.002
62. Liu YWJ, Tsui CM. A randomized trial comparing Tai Chi with and without cognitive-behavioral intervention (CBI) to reduce fear of falling in community-dwelling elderly people. Arch Gerontol Geriatr. (2013) 59:317–25. doi: 10.1016/j.archger.2014.05.008
63. Maki Y, Ura C, Yamaguchi T, Murai T, Isahai M, Kaiho A, et al. Effects of intervention using a community-based walking program for prevention of mental decline: a randomized controlled trial. J Am Geriatr Soc. (2012) 60:505–10. doi: 10.1111/j.1532-5415.2011.03838.x
64. McAuley E, Blissmer B, Marquez DX, Jerome GJ, Kramer AF, Katula J. Social relations, physical activity, and well-being in older adults. Prev Med. (2000) 31:608–17. doi: 10.1006/pmed.2000.0740
65. Streber A, Abu-Omar K, Hentschke C, Rütten A, A. multicenter controlled study for dementia prevention through physical, cognitive and social activities - GESTALT-kompakt. Clin Interv Aging. (2017) 12:2109–21. doi: 10.2147/CIA.S141163
66. Wang DS. Feasibility of a yoga intervention for enhancing the mental well-being and physical functioning of older adults living in the community. Act Adapt Aging. (2010) 34:85–97. doi: 10.1080/01924781003773559
67. Gagliardi C, Santini S, Piccinini F, Fabbietti P, di Rosa M, A. pilot programme evaluation of social farming horticultural and occupational activities for older people in Italy. Health Soc Care Commun. (2019) 27:207–14. doi: 10.1111/hsc.12641
68. Johnson JK, Stewart AL, Acree M, Nápoles AM, Flatt JD, Max WB, et al. A community choir intervention to promote well-being among diverse older adults: results from the Community of Voices Trial. J Gerontol. (2020) 75:549–59. doi: 10.1093/geronb/gby132
69. Ahn O, Cha HG, Chang SJ, Cho HC, Kim HS. Effect of an integrated health management program based on successful aging in Korean women. Public Health Nurs. (2015) 32:307–15. doi: 10.1111/phn.12177
70. Cardenas D, Henderson KA, Wilson BE. Experiences of participation in senior games among older adults. J Leis Res. (2009) 41:41–56. doi: 10.1080/00222216.2009.11950158
71. Hopman-Rock M, Westhoff MH. Health education and exercise stimulation for older people: development and evaluation of “Healthy & Vital”. Tijdschr Gerontol Geriatr. (2002) 33:56–63.
72. Huang TT, Yang LH, Liu CY. Reducing the fear of falling among community-dwelling elderly adults through cognitive-behavioural strategies and intense Tai Chi exercise: a randomized controlled trial. J Adv Nurs. (2011) 67:961–71. doi: 10.1111/j.1365-2648.2010.05553.x
73. Hwang J, Wang L, Siever J, Medico TD, Jones CA. Loneliness and social isolation among older adults in a community exercise program: a qualitative study. Aging Ment Health. (2019) 23:736–42. doi: 10.1080/13607863.2018.1450835
74. Kamegaya T, Araki Y, Kigure H, Yamaguchi H. Twelve-week physical and leisure activity programme improved cognitive function in community-dwelling elderly subjects: a randomized controlled trial. Psychogeriatrics. (2014) 14:47–54. doi: 10.1111/psyg.12038
75. Kim HJ, Kim HY, Yang Y, Ko E. Effect of an integrated healthcare program for korean rural older adults: a quasi-experimental study. Healthcare. (2020) 8. doi: 10.3390/healthcare8030244
76. McMahon SK, Wyman JF, Belyea MJ, Shearer N, Hekler EB, Fleury J. Combining motivational and physical intervention components to promote fall-reducing physical activity among community-dwelling older adults: a feasibility study. Am J Health Promot. (2016) 30:638–44. doi: 10.4278/ajhp.130522-ARB-265
77. McNamara B, Rosenwax L, Lee EA, Same A. Evaluation of a healthy ageing intervention for frail older people living in the community. Australas J Ageing. (2016) 35:30–5. doi: 10.1111/ajag.12196
78. Merchant RA, Tsoi CT, Tan WM, Lau W, Sandrasageran S, Arai H. Community-based peer-led intervention for healthy ageing and evaluation of the 'HAPPY' program. J Nutr Health Aging. (2021) 25:520–7. doi: 10.1007/s12603-021-1606-6
79. Ren Y, Tang R, Sun H, Li X. Intervention effect of group reminiscence therapy in combination with physical exercise in improving spiritual well-being of the elderly. Iran J Public Health. (2021) 50:531–9. doi: 10.18502/ijph.v50i3.5594
80. Shvedko AV, Whittaker AC, Greig CA, Thompson JL. Physical activity intervention for loneliness (PAIL) in community-dwelling older adults: a randomised feasibility study. Psychosomat Med. (2019) 81:A86. doi: 10.1186/s40814-020-00587-0
81. Yamamoto S, Ishii D, Noguchi A, Tanamachi K, Okamoto Y, Takasaki Y, et al. A short-duration combined exercise and education program to improve physical function and social engagement in community-dwelling elderly adults. Int Q Community Health Educ. (2020) 40:281–7. doi: 10.1177/0272684X19896732
Keywords: older adults, community-based intervention(s), physical activity, social participation, physical activity promotion
Citation: Tcymbal A, Abu-Omar K, Hartung V, Bußkamp A, Comito C, Rossmann C, Meinzinger D and Reimers AK (2022) Interventions simultaneously promoting social participation and physical activity in community living older adults: A systematic review. Front. Public Health 10:1048496. doi: 10.3389/fpubh.2022.1048496
Received: 19 September 2022; Accepted: 10 November 2022;
Published: 07 December 2022.
Edited by:
Mila Nu Nu Htay, Manipal University College Malaysia, MalaysiaReviewed by:
Joseph Kwon, University of Oxford, United KingdomCopyright © 2022 Tcymbal, Abu-Omar, Hartung, Bußkamp, Comito, Rossmann, Meinzinger and Reimers. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonina Tcymbal, YW50b25pbmEudGN5bWJhbEBmYXUuZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.