 Mailing Huang
Mailing Huang Yan Ma
Yan Ma Xinyu Ji
Xinyu Ji Hui Jiang
Hui Jiang Fangchao Liu
Fangchao Liu Naihui Chu
Naihui Chu Qi Li
Qi Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 January 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1040071
This article is part of the Research Topic Updates on Clinical and Molecular Epidemiology of Tuberculosis View all 18 articles
Purpose: The present study aimed to explore the risk factors for tuberculous meningitis (TBM) among patients with tuberculosis (TB).
Methods: This retrospective study was conducted on patients with TB who were hospitalized in Beijing Chest Hospital between January 2012 and December 2019. Demographic and clinical data of patients with TB were extracted from electronic medical records using a standardized data collection system. Logistic regression was used to analyze the risk factors associated with TBM.
Results: Of the total number of 22,988 cases enrolled, 3.1% were cases of TBM, which included 127 definite and 581 probable TBM, respectively. Multivariate analysis showed that definite TBM was significantly associated with patients aged < 30 years [adjusted odds ratio (aOR) = 3.015, 95% confidence interval (CI): (1.451–6.266)], who were farmers [aOR = 1.490, 95%CI: (1.020–2.177)], with miliary pulmonary TB [aOR = 105.842, 95%CI: (71.704–156.235)], and with malnutrition [aOR = 2.466, 95%CI: (1.110–5.479)]. Additionally, probable TBM was significantly associated with patients aged < 30 years [aOR = 2.174, 95% CI: (1.450–3.261)], aged 30–59 years [aOR = 1.670, 95% CI: (1.222–2.282)], who were farmers [aOR = 1.482, 95%CI: (1.203–1.825)], with miliary pulmonary TB [aOR = 108.696, 95%CI: (87.122–135.613)], and with a digestive system TB [aOR = 2.906, 95%CI: (1.762–4.793)].
Conclusion: An age of < 30 years, being a farmer, and having miliary pulmonary TB were risk factors for TBM among patients with TB. Further screening of patients with TB with aforementioned characteristics could facilitate clinicians to identify patients with TBM at an early stage.
Tuberculosis (TB) is ranked as the second leading cause of death from a single infectious agent after coronavirus 2019 (COVID-19) (1), and tuberculous meningitis (TBM) is the most severe form of TB (2). Despite 1-5% of TBM among cases of TB, it is universally fatal if left untreated (3, 4). Previous studies demonstrated that TBM had high mortality and morbidity, and the death rate reached up to 20-30% in TBM without HIV (human immunodeficiency virus) infection, but up to 50-60% in TBM with HIV infection (5–9). Moreover, nearly half of the survivors would have neurological sequelae, even if they are receiving treatment.
An early diagnosis of TBM can facilitate timely treatment and improve prognosis ultimately. However, it is difficult to diagnose TBM. Its symptoms and signs are variable and nonspecific. Existing diagnostic technologies still have some limitations. Elevated protein, lymphocytic pleocytosis, and low glucose with cerebrospinal fluid (CSF) cannot reliably distinguish TBM from other subacute meningitis types (cryptococcal meningitis, etc.) (10). Neuroimaging, especially cerebral magnetic resonance imaging (MRI), which is sensitive to the detection of the lesion, exhibits low specificity (11). Microbiological tests have good specificity but unfavorable sensitivity. Adenosine deaminase and T-SPOT.TB testing have different sensitivities and specificities and are expensive (12, 13). Notably, most of the aforementioned tests are unavailable in a resource-limited area. Risk factors for TBM should be identified, which could help clinicians to facilitate an early detection of TBM, especially in medical resource-limited areas.
Literature published demonstrated that being a farmer (14), having diabetes mellitus (15), having kidney failure (15–17), having HIV infection (1), having malnutrition (1), and having a rheumatic disease (18) are the risk factors for TB. Patients with the aforementioned characteristics are more likely to have TB, which can help clinicians identify TB early. Previous studies reported that TBM was the second stage of TB (19, 20), which was accompanied by the occurrence of any other TB. Up to 80% of miliary pulmonary TB is accompanied by TBM, and TBM was especially common in young children and people with untreated HIV infection (21, 22).
Early detection of TBM and targeted interventions are crucial for reducing the risk of TBM.
Thus, this study aimed to determine different factors associated with TBM in China.
Patients with TB who were hospitalized at Beijing Chest Hospital from 1 January 2012 to 31 December 2019 were enrolled in this retrospective study. Beijing Chest Hospital is a Class-3A level (the top level of hospital ranking in China) specialized hospital for treating TB infectious diseases in Beijing (north of China), equipped with 1,100 beds, and designated as a municipal-level hospital for treating patients with TB.
The participants were excluded, if they belonged to any of the following patient categories: (1) HIV-infected patients with TB; (2) possible cases of TBM according to the uniform case definition; and (3) suspected cases of TBM without results of cerebral imaging and lumbar puncture.
In the present study, patients were categorized as definite, probable, possible TBM, and non-TBM cases, based on a uniform case definition for use in clinical research on TBM (23). Briefly, three types of TBM, including definite, probable, and possible TBM of diagnostic criteria, are defined as follows: (1) definite TBM: microbiological identification or evidence from commercial nucleic acid amplification tests of the central nervous system (CNS) mycobacterium tuberculosis infection; (2) probable TBM: when imaging is available, a diagnostic score of 12 or above is required, and when imaging is not available, a diagnostic score of 10 or above is required; and (3) possible TBM: when imaging is available, a diagnostic score of 6–11 is required, and when imaging is not available, a diagnostic score of 6–9 is required.
The definition of miliary pulmonary TB included the presence of a miliary pattern on chest radiograph or computed tomography (CT), along with one or more of the following features: (1) clinical features compatible with pulmonary TB, including cough for a duration of 3 weeks or more, fever, weight loss, night sweats, loss of appetite, or hemoptysis; (2) microbiological and/or histopathological evidence of TB; and (3) response to antituberculosis treatment (24, 25).
Secondary pulmonary tuberculosis, also known as reactivated or adult pulmonary tuberculosis, refers to the reactivation of dormant tuberculosis lesions or re-exogenous infection.
Malnutrition was defined as the body mass index of patients (BMI) of < 18.5 kg/m2 according to the consensus statement of the European Society for Clinical Nutrition and Metabolism (ESPEN) (26). The BMI was calculated as weight in kilograms (kg) divided by height in meter square (kg/m2).
In this study, patients with TB included secondary pulmonary TB, miliary pulmonary TB, tuberculous pleuritis, tuberculous peritonitis, tuberculous pericarditis, lymph node TB, cutaneous and soft tissue TB, TB of the head and the neck, digestive system TB, genitourinary TB, vertebral TB, and osteoarticular TB, as seen in Table 1.
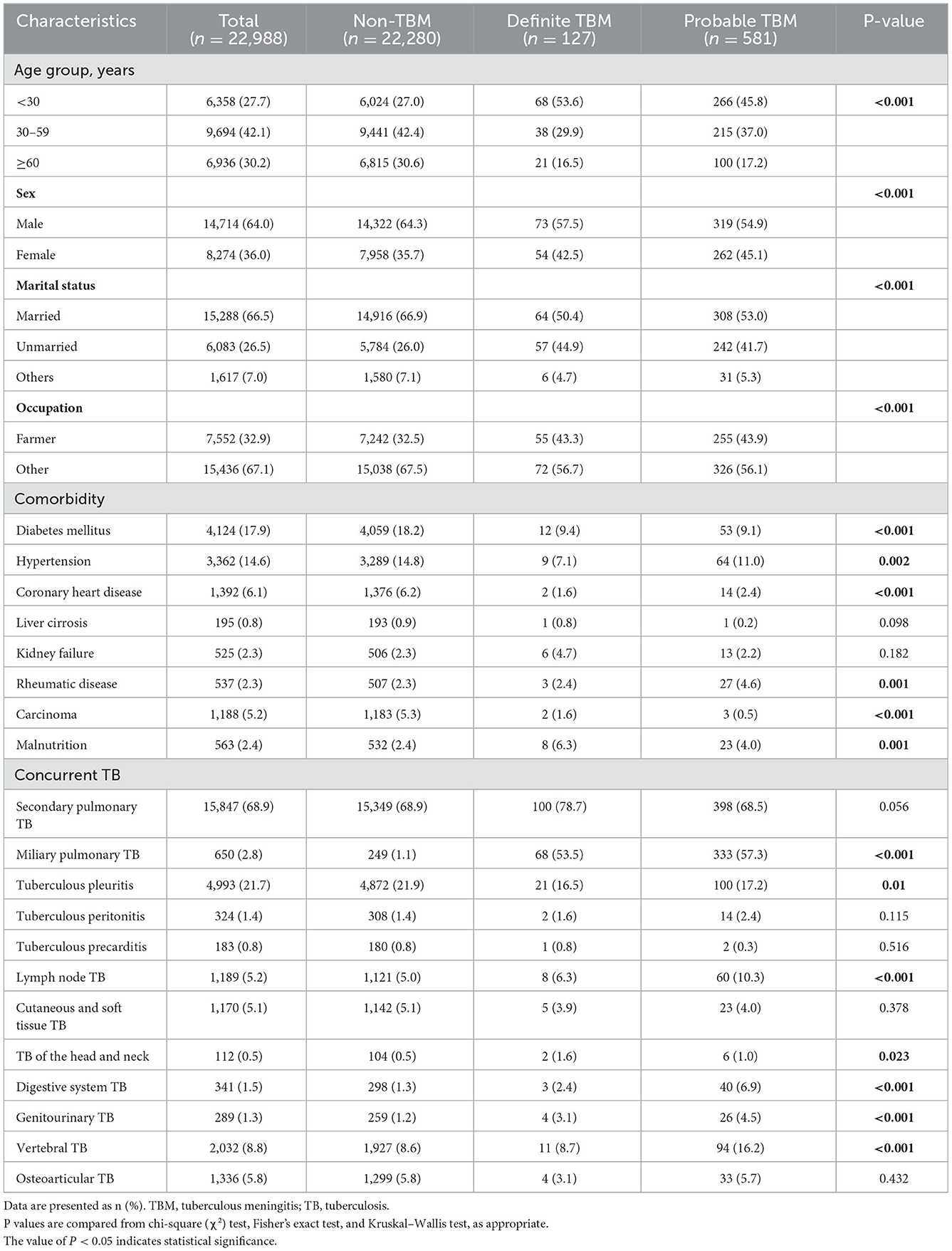
Table 1. Demographic and clinical characteristics of 22,988 cases from 2012 to 2019.
In the present study, TBM included definite TBM and probable TBM. Non-TBM cases included all other cases of TB without TBM.
The present study collected demographic (including age, sex, marital status, and occupation) and clinical (comorbidities and concurrent TB) data for all hospitalized patients with TB from electronic medical records. In the hospital, all diseases are coded using the International Classification of Diseases, 10th Revision with Clinical Modification (ICD-10-CM). The information about patients was collected only during the first hospitalization, but not if the patient was hospitalized repeatedly. Moreover, to reclassify patients with TBM into definite, probable, and possible TBM according to the uniform case definition, the present study also collected symptoms and symptom duration, signs, history of recent (within the past 1 year) close contact with an individual with pulmonary TB, routine biochemistry and biochemical analysis of the cerebrospinal fluid (CSF), imaging (computed tomography (CT), magnetic resonance imaging (MRI), or ultrasound (US)) of the cereba and other organs, mycobacterial evidence by any of the smear microscopy, culture, polymerase chain reaction (PCR), Xpert from sputum, urine, and stool, pleural effusion, pericardial effusion, peritoneal effusion, pus, and bronchoalveolar lavage fluid from patients with TBM.
Categorical variables were described as frequency and percentages (%) and continuous variables as mean and standard deviation (SD) or median and interquartile range (IQR), as appropriate. The means for continuous variables were compared using the independent group variance analysis when the data were normally distributed; otherwise, the Kruskal–Wallis test was used. A comparison of categorical variables was done using the chi-square (χ2) test or the Fisher exact test if the cell counts were small. To investigate and identify the risk factors of TBM further, the present study generated multivariate logistic regression analyses. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to demonstrate the risk for TBM. Statistical analysis was conducted using SPSS software (version 19.0, IBM, Armonk, NY, USA), and a value of P of < 0.05 indicated statistical significance.
The study was approved by the Ethics Committee of Beijing Chest Hospital (20210113YJS-2021-007). In the present study, the retrospective collection and analysis of cases were patients' demographic characteristics and diagnostic information. All data were supplied and analyzed, without access to personal identifiable information (PII). No informed consent was required.
A total of 23,121 inpatient cases with TB were enrolled in this study between 2012 and 2019. Of these, 133 cases were excluded, including 102 possible cases of TBM diagnosed by the uniform case definition, 8 suspected cases of TBM who did not undergo lumbar puncture and cerebral imaging, and 23 HIV-positive cases. A total of 22,988 patients with TB were thus included in the present study (Figure 1).
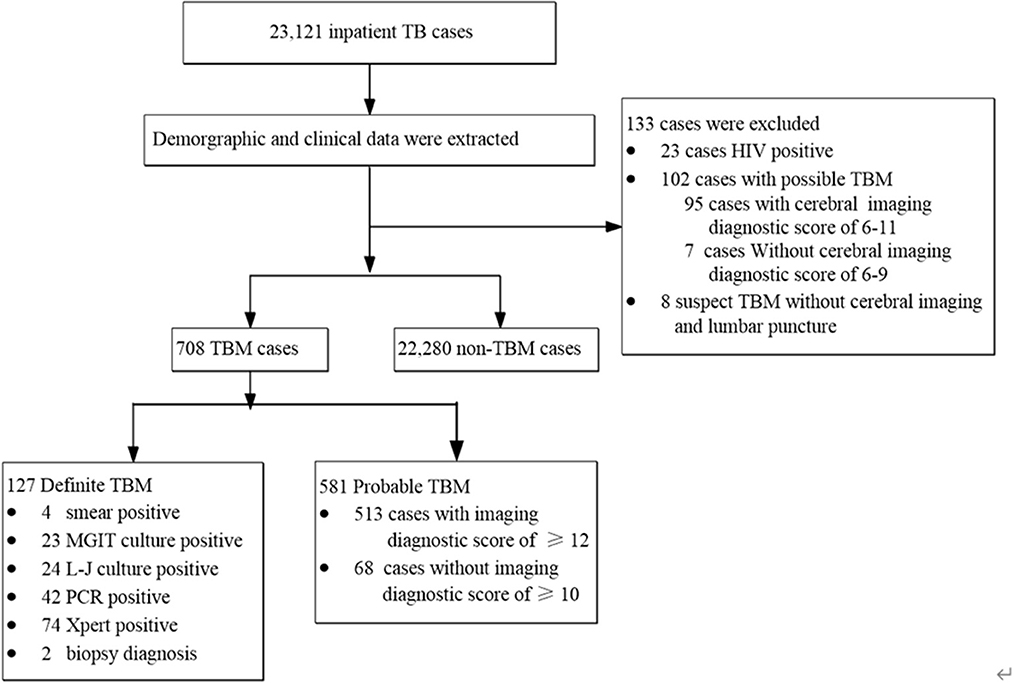
Figure 1. Flowchart of subjects enrolled in the study.
The median age of the patient was 47 years, and 64.0% of patients were men. Of these, 17.9% and 14.6% had diabetes mellitus and hypertension, respectively. Of 22,988 patients, 708 (3.1%) cases were patients with TBM, including 127 definite and 581 probable cases, and 22,280 (96.9%) cases were patients without TBM. Patients with definite and probable TBM were more likely to be younger, and nearly two-thirds of patients without TBM were women. Patients with definite and probable TBM were more likely to be male, to be less than aged 30 years, and to have rheumatic disease and malnutrition than patients without TBM. They were also more likely to have miliary pulmonary TB. The percentage of definite patients with TBM categorized as having miliary pulmonary TB (53.5%) was more than 48-fold greater than the percentage of patients without TBM (1.1%). Moreover, the percentage of probable TBM patients having miliary pulmonary TB (57.3%) was more than 52-fold greater than the percentage of patients without TBM (Table 1).
Among the 127 definite TBM cases, 4 (3.1%) of them were positive with smear microscopy, 23 (18.1%) for Mycobacteria Growth Indicator Tube (MGIT) culture, 24 (18.9%) for Lowenstein-Jenson culture, 42 (33.1%) for PCR, and 74 (58.3%) for Xpert, and two were pathologically diagnosed by biopsy from the brain (Figure 1). Additionally, although the hospitalized cases of TB increased gradually from 2,066 in 2012 to 3,475 in 2019, the proportion of TBM showed a decreasing trend from 4.4 to 2.4% during the same period (Figure 2). Miliary pulmonary TB (61.7%) with TBM was the highest, followed by digestive system TB (12.6%) and genitourinary TB (10.4%) (Figure 3).
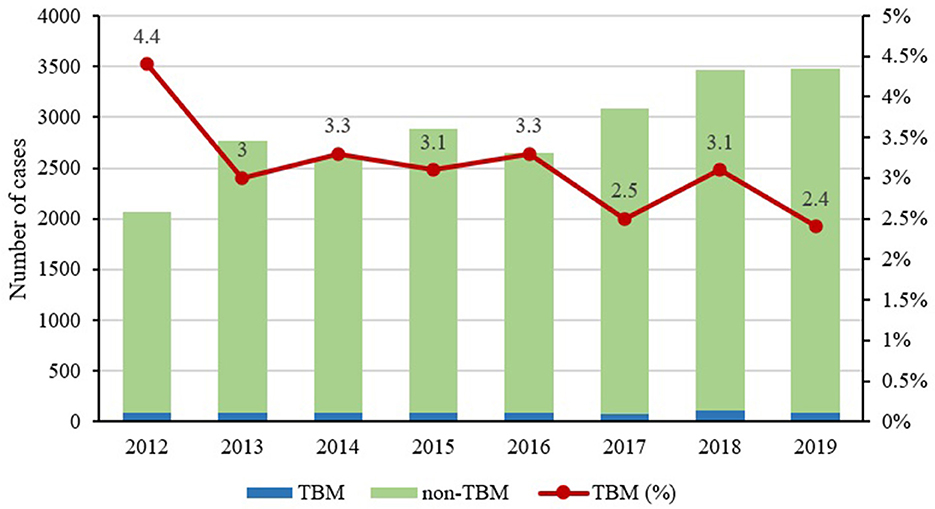
Figure 2. Proportion of tuberculosis (TB) and tuberculous meningitis (TBM) from 2012 to 2019.

Figure 3. The proportion of TBM in different types of tuberculosis.
When comparing patients with TB to patients without TBM, the univariate analysis showed that age, sex, marriage, occupation, comorbidities (including diabetes mellitus, hypertension, coronary heart disease, rheumatic disease, carcinoma, and malnutrition), and concurrent TB (miliary pulmonary TB, tuberculous pleuritis, lymph node TB, TB of the head and neck, digestive system TB, genitourinary TB, and vertebral TB) were significantly different among the three groups (p < 0.05), as reported in Table 1.
Table 2 shows the results of the logistic regression model for factors related to definite TBM and probable TBM. In the present multivariable logistic regression model, compared with patients without TBM, patients aged < 30 years were associated with a greater likelihood of definite TBM compared with patients aged >59 years [aOR = 3.015, 95% CI: (1.451–6.266)]. Farmers were more likely to have definite TBM [aOR = 1.490, 95%CI: (1.020–2.177)]. Compared with patients without miliary pulmonary TB, patients with miliary pulmonary TB increased the risk of definite TBM [aOR = 105.842, 95%CI: (71.704–156.235)]. Malnutrition also increased the risk of definite TBM [aOR = 2.466, 95%CI: (1.110–5.479)]. Additionally, probable TBM was significantly associated with patients aged < 30 years [aOR = 2.174, 95% CI: (1.450–3.261)], aged 30–59 years [aOR = 1.670, 95%CI: (1.222–2.282)], who are farmers [aOR = 1.482, 95%CI: (1.203–1.825)], with miliary pulmonary TB [aOR = 108.696, 95%CI: (87.122–135.613)], and with digestive system TB [aOR = 2.906, 95%CI: (1.762–4.793)] (Table 2).
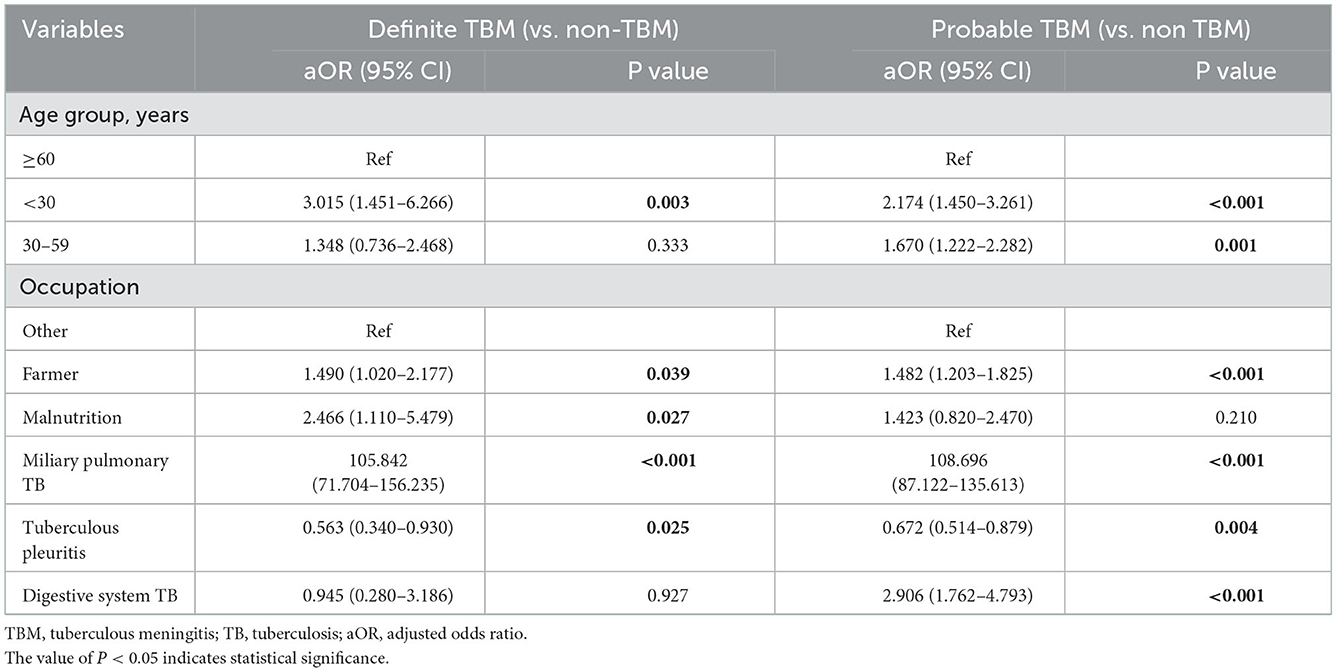
Table 2. Associated factors for definite TBM and probable TBM.
The present study found that 3.1% of TBM was prevalent among patients with TB, which was consistent with those given in previous studies (2, 3, 27). The present study also found that patients aged < 30 years, being farmers, and having miliary pulmonary TB were associated with a higher risk of definite and probable TBM. Additionally, malnutrition increased the probability of definite TBM, while digestive system TB increased the probability of probable TBM. Meanwhile, tuberculous pleuritis was associated with decreased probability.
Our study reported patients with TB who were < 30 years of age were two to three times more likely to have TBM, and compared with patients aged > 59 years, younger patients were more susceptible to TBM. Previous studies observed that TBM affected young children most commonly, and the peak was 2–4 years old, while the progression from latent tuberculosis infection (LTBI) to more severe forms of TB disease was faster in younger children (~1–4 months for TBM) (28–30). However, there is no report about patients aged < 30 years who are more prone to suffer from TBM. A retrospective cohort study from China found that patients aged > 20 years had a significantly lower risk for treatment delay (31). The possible reason was that younger patients are more likely to come to the hospital to seek health care, once they have suspected symptoms of TB. Additionally, the present study also observed that farmer was associated with an increased probability of TBM, while the results on farmers had not been reported in previous studies. Wang et al. reported that the farmer increased the risk of TB (14). Possible reasons were that farmers have a relatively low income, live in a relatively crowded poor environment, and are malnourished, thus making them vulnerable to TB. Second, farmers have low education level and poor knowledge of TB, which are the other reasons why they do not seek medical care when they are suspected symptoms of TB (32–34). However, TB progresses without treatment, which increases the probability of TBM. Therefore, increasing income and improving living conditions are helpful to prevent TBM from affecting farmers. Moreover, an appropriate way of promoting health education is to propagate the knowledge of TB among farmers, especially among illiterate farmers, which in turn promotes them to seek timely healthcare, which plays a more important role in reducing the incidence of TBM.
Miliary pulmonary TB results from the hematogenous spread of mycobacterium tuberculosis (Mtb) in the pulmonary. The present study found that 61.7% of patients with miliary pulmonary TB had TBM, which was similar to those mentioned in previous studies (11, 21). On the other hand, more than one-half (56.6%) of the patients with TBM had miliary pulmonary TB and only 1.1% of patients without TBM had miliary pulmonary TB. Miliary pulmonary TB was the most common hematogenous TB, followed by digestive system TB (30). In the present study, patients with miliary pulmonary TB had more than 100 times increased risk of both definite and probable TBM compared with TB patients without miliary pulmonary TB, and digestive system TB was also associated with increased risk for probable TBM. Lymph node TB, vertebral TB, and TB of the head and the neck were not associated with the risk for TBM, and the results indicated from the TBM pathogenesis mentioned previously that TBM was secondary to hematogenous spread, other than lymphangitic or contiguous spread. The results also suggested that, when physicians encounter such patients they consider performing cerebral imaging and lumbar puncture to exclude TBM for TB patients with miliary pulmonary TB in clinical practice.
The results of the present study observed that malnutrition increased the risk of definite TBM. The cellular immunity plays a critical role in immune responses to Mtb infection. Malnutrition could impair T-cell function, particularly the production of T-helper-1 cytokines and functions of the macrophage antimycobacterial effector (35). A previous study demonstrated that malnutrition increased the incidence and exacerbated clinical manifestations of TB (36). Patients with TB have an increased metabolism and a decreased appetite that compounds the already present malnutrition. Thus, a merciless vicious circle between TB and malnutrition continues (37). Previous studies revealed that malnutrition increased the risk of death for TB (38) and TBM (30). Improving the living conditions and reducing malnutrition can not only reduce the occurrence of TB and TBM but also improve the prognosis.
Our results found that tuberculous pleuritis was related to decreased risk for definite and probable TBM. The reason can be given that most patients with tuberculous pleuritis have fever, chest pain, shortness of breath, etc. Urgently, these types of discomfort promote patients to seek healthcare, while the diagnosis and treatment of tuberculous pleuritis reduce its progression to TBM. In addition, tuberculous pleuritis decreases the probability of TBM that may relate to their pathogenesis, but the pathogenesis of these two diseases is not so clear; hence, further studies need to be conducted in the future.
There are some limitations to our study. First, the study included inpatients only from a single center in China. Second, patients with HIV infection had not been analyzed further based on a small sample with 23 cases. In addition, the present study did not collect information about smoking and drinking, which is likely to correlate with TBM.
In summary, the present data reported on the proportion of TBM, including definite and probable TBM among patients with TB from a large sample study, and revealed risk factors including patients aged < 30 years, being farmers, and having miliary pulmonary TB affecting patients with TBM. The results of the present study suggested screening patients with TB having the aforementioned characteristics that could facilitate clinicians to identify patients with TBM at an early stage and improve the prognosis of patients with TBM further. Further studies should be conducted to confirm the findings of the present study.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
The study was approved by the Ethics Committee of Beijing Chest Hospital. In our study, the retrospective collection and analysis of case were patients' demographic characteristics and diagnosis information. All data were supplied and analyzed, without access to personal identifying information. No informed consent was required.
MH, YM, QL, and NC were involved in the conception and design of the project. MH and YM carried out the analysis and wrote the first draft of the manuscript. MH, YM, XJ, HJ, and FL conducted the literature search, data acquisition, and input data. QL had full access to all the data in the study and had final responsibility for the decision to submit for publication. All authors read and contributed to the final manuscript.
This study was supported by Tongzhou Yunhe Project under Grant (YH201906), the Scientific and Technological Innovation project of CACMS (CI2021B003, CI2021A01314, and CI2021A00704), and the China Tuberculosis Clinical Trial Consortium (CTCTC) research funding under Grant (2017KYJJ004).
We acknowledge the work and contribution of all participants in the present study for their hard work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization. Global tuberculosis report 2022. Geneva. Available online at: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022
2. Torok ME. Tuberculous meningitis: advances in diagnosis and treatment. Brit Med Bull. (2015) 113:117–31. doi: 10.1093/bmb/ldv003
3. Lincoln EM. Tuberculous meningitis in children; with special reference to serous meningitis; tuberculous meningitis. Am Rev Tuberc. (1947) 56:75–94. doi: 10.1164/art.1947.56.2.75
4. Seddon JA, Wilkinson R, van Crevel R, Figaji A, Thwaites GE, Tuberculous MIRC. Knowledge gaps and research priorities in tuberculous meningitis. Wellcome Open Res. (2019) 4:188. doi: 10.12688/wellcomeopenres.15573.1
5. Thao LTP, Heemskerk AD, Geskus RB, Mai NTH, Ha DTM, Chau TTH, et al. Prognostic models for 9-month mortality in tuberculous meningitis. Clin Infect Dis. (2018) 66:523–32. doi: 10.1093/cid/cix849
6. Wen L, Li M, Xu T, Yu X, Wang L, Li K. Clinical features, outcomes and prognostic factors of tuberculous meningitis in adults worldwide: systematic review and meta-analysis. J Neurol. (2019) 266:3009–21. doi: 10.1007/s00415-019-09523-6
7. Wang M, Luo L, Zhang Y, Liu X, Liu L, He J. Treatment outcomes of tuberculous meningitis in adults: a systematic review and meta-analysis. BMC Pulm Med. (2019) 19:1. doi: 10.1186/s12890-019-0966-8
8. Thwaites GE, Duc Bang N, Huy Dung N, Thi Quy H, Thi Tuong Oanh D, Thi Cam Thoa N, et al. The influence of HIV infection on clinical presentation, response to treatment, and outcome in adults with tuberculous meningitis. (2005) 192:2134–41. doi: 10.1086/498220
9. Heemskerk AD, Bang ND, Mai NTH, Chau TTH, Chau NVV, Phu NH, et al. Intensified antituberculosis therapy in adults with tuberculous meningitis. N Engl J Med. (2016) 374:124–34. doi: 10.1056/NEJMoa1507062
10. Bahr NC, Boulware DR. Methods of rapid diagnosis for the etiology of meningitis in adults. Biomark Med. (2014) 8:1085–103. doi: 10.2217/bmm.14.67
11. Venkatraman N, King T, Bell D, Woltmann G, Wiselka M, Abubakar I, et al. High levels of neurological involvement but low mortality in miliary tuberculosis: a 6-year case-series from the UK. Eur Respir J. (2016) 47:1578–81. doi: 10.1183/13993003.01958-2015
12. Li XL, Xie N, Wang SW, Wu QH, Ma Y, Shu W, et al. Diagnostic value of cerebrospinal fluid T-SPOTTB for tuberculousis meningitis in China. Biomed Environ Sci. (2017) 30:681–4. doi: 10.3967/bes2017.091
13. Gupta BK, Bharat A, Debapriya B, Baruah H. Adenosine deaminase levels in CSF of tuberculous meningitis patients. J Clin Med Res. (2010) 2:220–4. doi: 10.4021/jocmr429w
14. Wang X, Yin S, Li Y, Wang W, Du M, Guo W, et al. Spatiotemporal epidemiology of, and factors associated with, the tuberculosis prevalence in northern China, 2010-2014. BMC Infect Dis. (2019) 19:365. doi: 10.1186/s12879-019-3910-x
15. Dooley KE, Chaisson RE. Tuberculosis and diabetes mellitus: convergence of two epidemics. Lancet Infect Dis. (2009) 9:737–46. doi: 10.1016/S1473-3099(09)70282-8
16. Shu C, Wei Y, Yeh Y, Lin H, Chen C, Wang P, et al. The impact on incident tuberculosis by kidney function impairment status: analysis of severity relationship. Resp Res. (2020) 21:51. doi: 10.1186/s12931-020-1294-5
17. Cho PJ, Wu C, Johnston J, Wu M, Shu C, Lin H. Progression of chronic kidney disease and the risk of tuberculosis: an observational cohort study. Int J Tuberc Lung Dis. (2019) 23:555–62. doi: 10.5588/ijtld.18.0225
18. Vuorela M, Mars NJ, Salonen J, Kauppi MJ. Tuberculosis in people with rheumatic disease in Finland 1995-2007: a nationwide retrospective register study. Rheumatol Adv Pract. (2019) 3:z20. doi: 10.1093/rap/rkz020
19. Davis AG, Rohlwink UK, Proust A, Figaji AA, Wilkinson RJ. The pathogenesis of tuberculous meningitis. J Leukocyte Biol. (2019) 105:267–80. doi: 10.1002/JLB.MR0318-102R
20. Donald P, Schaaf H, Schoeman J. Tuberculous meningitis and miliary tuberculosis: the Rich focus revisited. J Infection. (2005) 50:193–5. doi: 10.1016/j.jinf.2004.02.010
21. Garg RK, Sharma R, Kar AM, Kushwaha RAS, Singh MK, Shukla R, et al. Neurological complications of miliary tuberculosis. Clin Neurol Neurosur. (2010) 112:188–92. doi: 10.1016/j.clineuro.2009.11.013
22. Thwaites GED, van Toorn RM, Schoeman JP. Tuberculous meningitis: more questions, still too few answers. Lancet Neurology. (2013) 12:999–1010. doi: 10.1016/S1474-4422(13)70168-6
23. Marais S, Thwaites G, Schoeman JF, Torok ME, Misra UK, Prasad K, et al. Tuberculous meningitis: a uniform case definition for use in clinical research. Lancet Infect Dis. (2010) 10:803–12. doi: 10.1016/S1473-3099(10)70138-9
24. Hussain SF, Irfan M, Abbasi M, Anwer SS, Davidson S, Haqqee R, et al. Clinical characteristics of 110 miliary tuberculosis patients from a low HIV prevalence country. Int J Tuberc Lung Dis. (2004) 8:493
25. Sharma SK, Mohan A, Sharma A, Mitra DK. Miliary tuberculosis: new insights into an old disease. Lancet Infect Dis. (2005) 5:415–30. doi: 10.1016/S1473-3099(05)70163-8
26. Cederholm T, Bosaeus I, Barazzoni R, Bauer J, Van Gossum A, Klek S, et al. Diagnostic criteria for malnutrition - an ESPEN consensus statement. Clini Nutr. (Edinburgh, Scotland). (2015) 34:335–40. doi: 10.1016/j.clnu.2015.03.001
27. Seddon JA, Tugume L, Solomons R, Prasad K, Bahr NC. Tuberculous MIRC. The current global situation for tuberculous meningitis: epidemiology, diagnostics, treatment and outcomes. Wellcome Open Res. (2019) 4:167. doi: 10.12688/wellcomeopenres.15535.1
28. Duque-Silva A, Robsky K, Flood J, Barry PM. Risk factors for central nervous system tuberculosis. Pediatrics. (2015) 136:e1276–84. doi: 10.1542/peds.2014-3958
29. Donovan J, Thwaites GE, Huynh J. Tuberculous meningitis: where to from here? Curr Opin Infect Dis. (2020) 33:259–66. doi: 10.1097/QCO.0000000000000648
30. Starke JR. Tuberculosis in children. Semin Resp Crit Care. (2004) 25:353–64. doi: 10.1055/s-2004-829507
31. He Y, Han C, Chang K, Wang M, Huang T. Total delay in treatment among tuberculous meningitis patients in China: a retrospective cohort study. BMC Infect Dis. (2017) 17:341. doi: 10.1186/s12879-017-2447-0
32. Asres M, Gedefaw M, Kahsay A, Weldu Y. Patients' delay in seeking health care for tuberculosis diagnosis in East Gojjam zone, Northwest Ethiopia. Am J Trop Med Hyg. (2017) 96:1071–5. doi: 10.4269/ajtmh.16-0892
33. Luba TR, Tang S, Liu Q, Gebremedhin SA, Kisasi MD, Feng Z. Knowledge, attitude and associated factors towards tuberculosis in Lesotho: a population based study. BMC Infect Dis. (2019) 19:96. doi: 10.1186/s12879-019-3688-x
34. Ali Warsi SM, Danish SH, Ahmad F, Khan AI, Khan MP, Bano S, et al. Tuberculosis knowledge and health seeking behaviour: a tale of two districts of Sindh, Pakistan. JPMA. (2016) 66:1120–6
35. Boelaert JR, Gordeuk VR. Protein energy malnutrition and risk of tuberculosis infection. Lancet. (2002) 360:1102. doi: 10.1016/S0140-6736(02)11169-X
36. Macallan DC. Malnutrition in tuberculosis. Diagn Micr Infec Dis. (1999) 34:153–7. doi: 10.1016/s0732-8893(99)00007-3
37. Martin SJ, Sabina EP. Malnutrition and associated disorders in tuberculosis and its therapy. J Diet Suppl. (2019) 16:602–10. doi: 10.1080/19390211.2018.1472165
Keywords: tuberculosis, tuberculous meningitis, miliary pulmonary tuberculosis, risk factors, malnutrition
Citation: Huang M, Ma Y, Ji X, Jiang H, Liu F, Chu N and Li Q (2023) A study of risk factors for tuberculous meningitis among patients with tuberculosis in China: An analysis of data between 2012 and 2019. Front. Public Health 10:1040071. doi: 10.3389/fpubh.2022.1040071
Received: 08 September 2022; Accepted: 21 December 2022;
Published: 27 January 2023.
Edited by:
Amit Singh, Central University of Punjab, IndiaReviewed by:
Masaraf Hussain, All India Institute of Medical Sciences, Guwahati, IndiaCopyright © 2023 Huang, Ma, Ji, Jiang, Liu, Chu and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qi Li,  bHEwNzAzQGhvdG1haWwuY29t; Naihui Chu, ZG9uZ2NodTE5OTRAc2luYS5jb20=
bHEwNzAzQGhvdG1haWwuY29t; Naihui Chu, ZG9uZ2NodTE5OTRAc2luYS5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.