
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 06 October 2022
Sec. Digital Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1029392
 Junqiang Zhao1,2,3†
Junqiang Zhao1,2,3† Xinxin Zhang2,3,4†
Xinxin Zhang2,3,4† Yi Lu2,3,4†
Yi Lu2,3,4† Xingyang Wu2,3,5
Xingyang Wu2,3,5 Fujun Zhou1
Fujun Zhou1 Shichang Yang6Luping Wang1
Shichang Yang6Luping Wang1 Xiaoyan Wu7*
Xiaoyan Wu7* Fangrong Fei8*
Fangrong Fei8*Objective: We aimed to explore the impact of using virtual reality technology to intervene in and encourage the developmental behavior areas of cognition, imitation, and social interaction in children with autism spectrum disorder.
Methods: Forty-four children with autism spectrum disorder were divided randomly into an intervention group and a control group, with each group consisting of 22 participants. Incorporating conventional rehabilitation strategies, virtual reality technology was used with the intervention group to conduct rehabilitation training in areas including cognition, imitation, and social interaction. The control group was provided conventional/routine clinical rehabilitation training. The children's cognitive development was evaluated before and 3 months after intervention.
Results: After intervention, the developmental abilities of both groups of children in the areas of cognition, imitation, and social interaction were improved over their abilities measured before the intervention (P < 0.05). However, post-intervention score differences between the two groups demonstrated that the intervention group levels were better than the control group levels only in the areas of cognition and social interaction (P < 0.05).
Conclusion: Combining virtual reality with conventional rehabilitation training improved the cognitive and social development of children with autism spectrum disorder and supported the goal of improving the rehabilitation effect.
Autism Spectrum Disorders (ASD), also known as autism, is a serious neurodevelopmental disorder that occurs in early childhood and affects five times as many boys as girls. Its clinical manifestations are characterized by unconventional social interaction, narrow interests, and rigid repetition (1). In 2018, 1 in every 59 children aged 4 years in the United States had ASD (2). In China, from 2014 to 2016, the incidence rate of children aged 6 to 12 years living in eight representative cities in China was estimated to be 0.7% (3). A common problem here is factors including the limited number of local and national rehabilitation facilities, a scarcity of practitioners, and different levels of rehabilitation training offered to children with ASD (4). Therapists must spend considerable time and energy creating rehabilitation training scenarios for children with ASD, and clinical treatment has the disadvantages of lengthy rehabilitation or therapy protocols and scenarios that cannot be replicated (5). Therefore, it is necessary to seek additional intervention methods that are more convenient and accessible. Virtual reality (VR) is capable of fusing the actual and virtual worlds, and can replicate various scenarios to produce an immersive experience. A growing number of studies have revealed that VR-based training can improve the outcomes of conventional therapy for patients with ASD (6), and many of these studies have been applied in psychology and development medical therapies (7, 8). VR technology can be utilized to create virtual rehabilitation scenarios and safe, controllable, and repeatable rehabilitation training modes that improve functional development in the social and cognitive abilities of children with ASD. In this study, VR technology was employed in rehabilitation therapies for children with ASD in the areas of cognition, imitation, and social interaction.
A total of 47 children diagnosed with ASD in the Pediatric Rehabilitation Department of a Grade A Hospital in Xinxiang from August 2020 to March 2021 were selected as the study's research participants. Patients participating in the intervention were selected according to their admission order. The researchers numbered the patients according to the time of admission. Patients with odd numbers were included in the intervention group, and patients with even numbers were included in the control group. Inclusion criteria included the following:
1. Caregivers with normal cognitive and reading abilities who agreed to participate in the study;
2. Caregivers who were relatives of the children and were aged 20–59 years;
3. Children aged 3–6 years who were stable and conscious patients;
4. Children diagnosed with ASD according to the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V).
Exclusion criteria included the following:
1. Children diagnosed with other serious organic diseases;
2. Children and caregiver who were participating in other investigations or interventions;
3. Participants or caregivers who refused to participate or withdrew at any stage of the study;
4. Other serious physical or mental diseases within the family.
The 47 children who met the inclusion criteria were divided into an intervention group and a control group. In the intervention group, 22 children finished the trial, while 3 dropped out for private reasons; 22 children from the control group finished the research. A total of 44 children with ASD finished the trial.
The intervention group included 19 males and 3 females. Participants were 3–5 years old, with an average age of 3.45 (3.00–4.00) years. Treatment duration was ≥12 months for 4 patients and <12 months for 18 patients. The control group included 16 males and 6 females. The average age of the participants, who ranged in age from 3 to 5 years old, was 3.50 (3.00–4.00). Treatment duration was ≥12 months for 5 patients and <12 months for 17 patients. There were no significant differences in age, gender, or treatment duration between the two groups (all P > 0.05). All children and caregivers provided written informed consent. The study was approved by the Ethics Committee of Xinxiang Medical University.
The intervention team was comprised of five members, one of whom was a pediatric clinician with the title of deputy chief physician. There were two clinical therapists and two nurses, one of whom was a nursing graduate student, who were responsible for data collection and the virtual intervention with the children. Another nurse who had received training from the Heep Hong Association performed the entire evaluation procedure, offered expert analysis of the results, and offered reliable conclusions. The study design for the project involved all team members. Pediatricians were largely in charge of disease diagnosis and providing a rehabilitation treatment plan, and therapists and nurses delivered rehabilitation training and advise in accordance with the pediatricians' recommendations.
The control group took part in conventional rehabilitation training, which included the following:
1. Collective class training (40–45 min): The therapist issued oral instructions to the children and waited for the children to respond. If a child responded correctly, reinforcement was given. If the child did not respond appropriately, the therapist paused and then re-issued the instruction, assisted the child, offered a reinforcement, paused again, and then re-issued the instruction once again. If the child did not respond, the therapist assisted the child as necessary.
2. Sensory integration training (40–45 min): This training utilized cylinders, a wooden balance table, push balls (to be used on the ground), horn balls (tactile exercise equipment), and other touchdown training tools. The children used the equipment to use gross motor skills for balance and defense training in which different parts of the body had to operate harmoniously and effectively. Classes were held each day, Monday through Friday, and two types of tools were used in each class. The instructor made adjustments according to each child's progress and current developmental level, which was assessed every week.
3. Fine motor training (40–45 min): This training included manual tasks based on the child's specific ASD diagnosis and abilities. Each week the children's training included picking up items, panel matching, and similar tasks. These manual tasks aided the developed the children's sensory organs, including their eyes and ears, helping to develop the functionality of their brains and body parts and the coordination of their physical and cognitive abilities.
In the intervention group, VR technology was added to the rehabilitation training offered to the control group. In the virtual scene, children were instructed to hold a cursor on a target or to answer questions according to the instructions given by virtual characters across different scenes to proceed to the next step. During the intervention, several children refused to wear head mounted VR displays. Considering the characteristics of patients with ASD, “desensitization therapy” was adopted 1 week before the intervention for children who resisted the rehabilitation training. Play time was increased as needed for each child until the child was able to accept and participate in the intervention program. In the intervention phase, each child received intervention training three times a week. Each training session totaled 15 min (3 instances of 5 min of training, with rest periods in between). The intervention period was a total of 12 weeks.
Researchers, clinicians, and therapists designed the VR training based on an accepted rehabilitation intervention method for the ASD population: applied behavior analysis (9). For example, if a child could not complete object identification after the virtual teacher had given instructions, the target object would flash to replace the teacher's assistance in real-world training. The virtual scene was designed considering the clinical characteristics of children with ASD, in that the advantages of picture communication, visual stimulation, and cartoon animation were combined. Unity3D was used to develop the VR training. The game was divided into six training scenes focused on the cognitive, social, imitation, gross motor, emotional expression, and language understanding of children with ASD, as shown in Table 1. Figure 1 shows a child participating in the VR training.
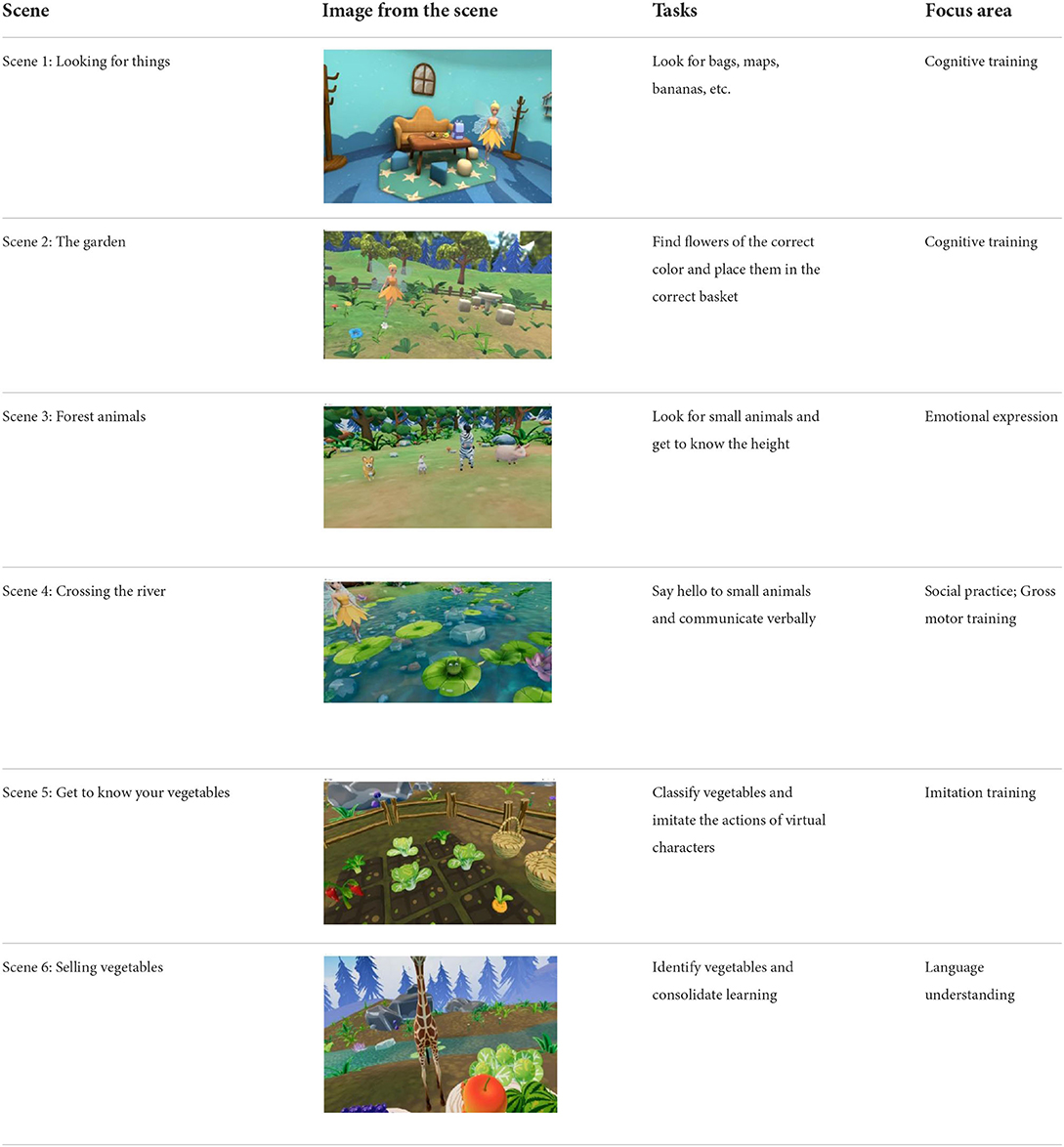
Table 1. Six virtual reality intervention training scenarios.

Figure 1. Children in the intervention group were trained with virtual reality technology.
The Psychoeducational Profile, Third Edition (PEP-3) was used to evaluate the rehabilitation impact on children with ASD before and after intervention. The Chinese version of the PEP-3 assessment is divided into three parts: developmental and behavioral side tests, child caregiver reports, and composite scores. The developmental and behavioral side tests include 34 assessments of cognitive behaviors, 25 assessments of verbal expression, 19 assessments of verbal comprehension, 20 assessments of fine motor skills, 15 assessments of gross motor skills, 10 motor imitation tests, 11 emotional expression tests, 12 social interaction tests, 15 non-verbal behavior tests, and 11 verbal ability tests. The child caregiver report includes 10 queries about problem behaviors, 13 queries about self-care behaviors, and 15 queries about adaptive behaviors. This study used six development areas in the development and behavioral subtest: cognitive, language comparison, cross motor, mimicry, social interaction, and emotional expression.
The PEP-3 can be used to evaluate the strength and development/adaptation of children with ASD. Individual scores for each development and behavioral side test are expressed as 0 (fail), 1 (intermediate response), or 2 (pass) points. The corresponding age and percentage progression of children's development parts can be found through the original score. A percentage progression >89 indicates appropriate degree of development/adaptation; 75–89 indicates a slight degree of development/adaptation; 25–74 indicates moderate degree of development adaptation; and <25 indicates a severe degree of development/adaptation. The Cronbach'α coefficient of the scale is 0.84.
All participants were evaluated before intervention and 3 months after intervention. After obtaining the consent of guardians, nurse evaluators assessed the children and completed the evaluation questionnaire, which was collected immediately. A total of 47 questionnaires were issued; 44 questionnaires were recovered effectively, with a questionnaire recovery rate of 94%.
SPSS 25.0 software was used for statistical analysis of the data. If the data followed normal distribution, a two-sample/independent t-test would be used for inter-group comparison. A paired t-test was used to compare results before and after intervention. Non-normal distribution data were tested by a non-parametric rank-sum test, with a test level α = 0.05. For the data followed normal distribution, we display mean ± SD, for the data not followed normal distribution, we display quartile.
Before the intervention, there was no statistical difference between the cognitive development scores of the two groups (P > 0.05), as shown in Table 2.
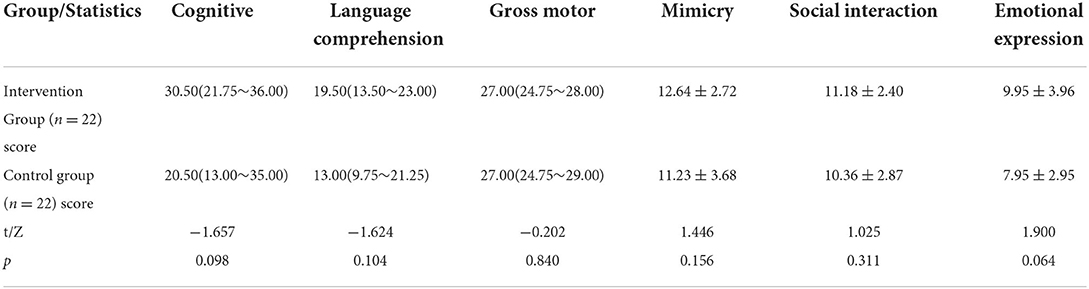
Table 2. Score comparison of the two groups before intervention.
In both groups, the post-intervention developmental ability scores in the areas of cognition, imitation, and social interaction were significantly better than the pre-intervention scores (P < 0.05; see Table 3). This result indicates that the intervention program was effective in improving the ability of children with ASD.

Table 3. Score comparison of the two groups before and after intervention.
After the intervention, the cognitive ability and social communication ability of the children in the intervention group were significantly higher than in the control group (P < 0.05; see Table 4). These results indicate that VR-assisted intervention technology can promote the development of these abilities in children with ASD.
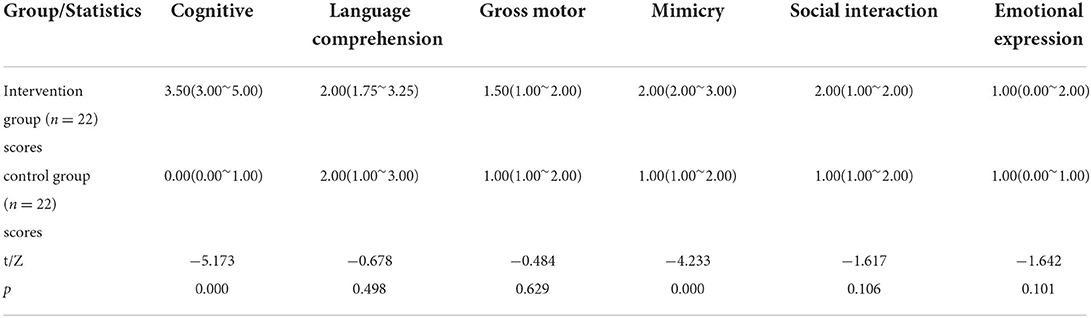
Table 4. Score comparison of the two groups before and after intervention.
The results of this study demonstrated that there was no significant differences in the developmental ability scores of the children in the control and intervention groups before the intervention across gender, age, treatment time, and cognition variables (P > 0.05). After 3 months of rehabilitation, the intervention group's developmental ability scores for cognition, imitation, and social interactions were significantly higher than before the intervention (P < 0.05). The scores of the children in the intervention group were also significantly better than the scores of the children in the control group for cognition and social interaction abilities (P < 0.05). The study results suggest that both conventional clinical rehabilitation training and conventional rehabilitation training with VR training can affect the developmental ability of children with ASD (10–12). These results confirm results from previous studies (13).
Patients with ASD often have anxiety and fear about unfamiliar environments (14–17). Frequent staffing changes occur within rehabilitation teams, and children with ASD often do not cooperate, which can lead to potential delays in the rehabilitation process and increasing difficulty for medical personnel (18–20). A VR environment has the advantages of safety, controllability, and repeated operation. Its immersive picture makes children with ASD receptive to visual stimulation, which is conducive to cognitive learning (21–25). Moreover, social stories are presented in the form of virtual animation, and it tends to be simple to interest and immerse children in animation and to maintain their attention for a long time (26, 27). With these advantages, the use of virtual training can help further improve children's cognitive ability.
One core issue in ASD is that social communication is very difficult (28–30). The results of this study show that the rehabilitation effect in terms of social interaction improved for the children in the intervention group. Some nonverbal communication skills, such as greeting, were included in the study's VR training. Additionally, in the virtual scenes, the tasks presented to the children had them face and learn about emotional reactions in social interaction. Under the supervision of nurses, social skills learned by children in the training environment (including facial expression recognition, happy tone of voice, and body language based on the actions of virtual characters) can be generalized into daily life gradually. This integration mobilizes overall mental state, which can increase the enthusiasm of children in rehabilitation training (31). Adopting multi-level and multi-channel VR social training can further improve children's social ability.
One limitation of this study was its small sample size. The sample size should be increased in future studies to track and record the developmental ability of children with ASD to further confirm the applicability and value of this study.
For abilities other than cognitive development and social communication, although VR technology can produce dynamic interaction, skill levels and the development obtained in specific training contexts must be further tested and trained in actual social situations (32–34). The timeframe of this study was short, with only 3 months of intervention. Moreover, whether the training described in this study can build on rehabilitation effects in other fields is a research question deserving further discussion and investigation.
In the virtual environment, it is difficult for children to control their behavior and explain the reasoning or purpose behind their choice of behavior. In this study, the nurses could not enter the virtual environment to help the children understand the situation and guide them to make appropriate responses (35). This restriction may also limit children's use of VR technology for rehabilitation training of related skills. If the nurse and the child could appear together in the scene and perform task decomposition through voice instructions, the rehabilitation effect may be better. However, current technology levels make it difficult to solve this problem.
Children with ASD typically demonstrate social withdrawal, anxiety, and fear in unfamiliar environments. Training with VR requires long periods of concentration, which is a challenge for these, and many, children. In this study, it was feasible for the nurses to use items of interest to the children (i.e., “reinforcement”) to increase the children's compliance during the training. The question of how to optimize the volume, pictures, scene-switching mode, and more within VR to produce more positive effects for the children must be considered.
Many studies have found that VR training helps children with ASD and patients with adjacent neurological diseases to build various skills, such as language function, attention, and executive function (36, 37). Our study found that rehabilitation training based on VR technology can effectively promote the cognitive and social communication abilities of children with ASD. This study's results offer a new and meaningful rehabilitation method for the ongoing clinical rehabilitation of children with ASD. However, no significant differences were seen between the children in the control and intervention groups for areas of development other than cognition and social communication.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of Xinxiang Medical University. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
JZ, XZ, and YL analyzed the data and drafted the manuscript. XinW, FZ, SY, and LW analyzed the data and designed the VR environment. XiaW and FF designed the research and revised the manuscript. All authors agreed to be accountable for the content of the work.
The work was financially supported the Key R&D and Promotion Projects in Henan Province (222102310615), Henan Province Medical Science and Technology Key Project Jointly Constructed by Province and Ministry (SBGJ202102189), and Research on Visualization Construction of TAVR Therapy Based on Virtual Reality Technology (XZZX2022011).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. De Luca R, Leonardi S, Portaro S, Le Cause M, De Domenico C, Colucci PV, et al. Innovative use of virtual reality in autism spectrum disorder: a case-study. Appl Neuropsychol Child. (2021) 10:90–100. doi: 10.1080/21622965.2019.1610964
2. Shaw KA, Maenner MJ, Bakian AV, Bilder DA, Durkin MS, Furnier SM, et al. Early identification of autism spectrum disorder among children aged 4 years - autism and developmental disabilities monitoring network, 11 sites, United States, 2018. Morbidity Mortal Wkly Rep Surveil Summaries. (2021) 70:1–14. doi: 10.15585/mmwr.ss7010a1
3. Zhou H, Xu X, Yan W, Zou X, Wu L, Luo X, et al. Prevalence of autism spectrum disorder in china: a nationwide multi-center population-based study among children aged 6 to 12 years. Neurosci Bull. (2020) 36:961–71. doi: 10.1007/s12264-020-00530-6
4. Wan G-B, Deng F-H, Jiang Z-J, Lin S-Z, Zhao C-L, Liu B-X, et al. Attention shifting during child—Robot interaction: a preliminary clinical study for children with autism spectrum disorder. Front Inf Technol Electron Eng. (2019) 20:374–87. doi: 10.1631/FITEE.1800555
5. Dyson MW, Chlebowski C, Brookman-Frazee L. Therapists' adaptations to an intervention to reduce challenging behaviors in children with Autism spectrum disorder in publicly funded mental health services. J Autism Dev Disord. (2019) 49:924–34. doi: 10.1007/s10803-018-3795-3
6. Maskey M, Rodgers J, Grahame V, Glod M, Honey E, Kinnear J, et al. A randomised controlled feasibility trial of immersive virtual reality treatment with cognitive behaviour therapy for specific phobias in young people with autism spectrum disorder. J Autism Dev Disord. (2019) 49:1912–27. doi: 10.1007/s10803-018-3861-x
7. Meindl JN, Saba S, Gray M, Stuebing L, Jarvis A. Reducing blood draw phobia in an adult with autism spectrum disorder using low-cost virtual reality exposure therapy. J Appl Res Intellect Disabil. (2019) 32:1446–52. doi: 10.1111/jar.12637
8. Mccleery JP, Zitter A, Solorzano R, Turnacioglu S, Miller JS, Ravindran V, et al. Safety and feasibility of an immersive virtual reality intervention program for teaching police interaction skills to adolescents and adults with autism. Autism Res. (2020) 13:1418–24. doi: 10.1002/aur.2352
9. Rafiee S, Ani ZK. The effectiveness of applied behavior analysis therapy on eye contact enhancement, stereotypical behaviors and reduction of behavioral problems in children with autism spectrum. Revista Gestao Tecnol. (2020) 20:98–122. doi: 10.20397/2177-6652/2020.v20i2.1651
10. Xu WX, Yao JW, Liu WY. Intervention effect of sensory integration training on the behaviors and quality of life of children with Autism. Psychiatria Danubina. (2019) 31:340–6. doi: 10.24869/psyd.2019.340
11. Malinverni L, Mora-Guiard J, Padillo V, Valero L, Hervas A, Pares N. An inclusive design approach for developing video games for children with Autism spectrum disorder. Comput Hum Behav. (2017) 71:535–49. doi: 10.1016/j.chb.2016.01.018
12. Yang YJD, Allen T, Abdullahi SM, Pelphrey KA, Volkmar FR, Chapman SB. Brain responses to biological motion predict treatment outcome in young adults with autism receiving virtual reality social cognition training: preliminary findings. Behav Res Therapy. (2017) 93:55–66. doi: 10.1016/j.brat.2017.03.014
13. De Moraes ÍAP, Monteiro CBDM, Silva TDD, Massetti T, Crocetta TB, De Menezes LDC, et al. Motor learning and transfer between real and virtual environments in young people with autism spectrum disorder: a prospective randomized cross over controlled trial. Autism Res. (2020) 13:307–19. doi: 10.1002/aur.2208
14. Capriola-Hall NN, Mcfayden T, Ollendick TH, White SW Caution when screening for autism among socially anxious youth. J Autism Dev Disord. (2021) 51:1540–9. doi: 10.1007/s10803-020-04642-w
15. Iandolo G, Lopez-Florit L, Venuti P, Neoh MJY, Bornstein MH, Esposito G. Story contents and intensity of the anxious symptomatology in children and adolescents with Autism Spectrum Disorder. Int J Adolesc Youth. (2020) 25:725–40. doi: 10.1080/02673843.2020.1737156
16. Van Steensel FJA, Bogels SM, Dirksen CD. Anxiety and quality of life: clinically anxious children with and without autism spectrum disorders compared. J Clin Child Adolescent Psychol. (2012) 41:731–8. doi: 10.1080/15374416.2012.698725
17. White SW, Ollendick T, Scahill L, Oswald D, Albano AM. Preliminary efficacy of a cognitive-behavioral treatment program for anxious youth with autism spectrum disorders. J Autism Dev Disord. (2009) 39:1652–62. doi: 10.1007/s10803-009-0801-9
18. Kohenraz R, Volkmar FR, Cohen DJ. Postural control in children with autism. J Autism Dev Disord. (1992) 22:419–32. doi: 10.1007/BF01048244
19. Alvares GA, Balleine BW, Whittle L, Guastella AJ. Reduced goal-directed action control in autism spectrum disorder. Autism Res. (2016) 9:1285–93. doi: 10.1002/aur.1613
20. Olaff HS, Vandbakk M, Holth P. Blocking of stimulus control in children with autism. Psychol Rec. (2022) 72:305–17. doi: 10.1007/s40732-020-00454-7
21. Campbell K, Carpenter KLH, Hashemi J, Espinosa S, Marsan S, Borg JS. Computer vision analysis captures atypical attention in toddlers with autism. Autism. (2019) 23:619–28. doi: 10.1177/1362361318766247
22. Khan NA, Sawand MA, Qadeer M, Owais A, Junaid S, Shahnawaz P. Autism detection using computer vision. Int J Comput Sci Network Security. (2017) 17:256–62. Available online at: http://cloud.politala.ac.id/politala/1.%20Jurusan/Teknik%20Informatika/19.%20e-journal/Jurnal%20Internasional%20TI/IJCSNS/2017%20Vol.%2017%20No.%2004/20170435%20Autism%20Detection%20using%20Computer%20Vision.pdf
23. Marothi R, Csigo K, Keri S. Early-stage vision and perceptual imagery in autism spectrum conditions. Front Hum Neurosci. (2019) 13:337. doi: 10.3389/fnhum.2019.00337
24. Bossenbroek R, Wols A, Weerdmeester J, Lichtwarck-Aschoff A, Granic I, Van Rooij MMJJMH. Efficacy of a virtual reality biofeedback game (DEEP) to reduce anxiety and disruptive classroom behavior: single-case study. JMIR Ment Health. (2020) 7:e16066. doi: 10.2196/16066
25. Babu PRK, Oza P, Lahiri U. Gaze-Sensitive virtual reality based social communication platform for individuals with autism. IEEE Trans Affect Comput. (2018) 9:450–62. doi: 10.1109/TAFFC.2016.2641422
26. Zhao H, Swanson AR, Weitlauf AS, Warren ZE, Sarkar NJITOH-MS. Hand-in-hand: a communication-enhancement collaborative virtual reality system for promoting social interaction in children with autism spectrum disorders. IEEE Trans Hum Mach Syst. (2018) 48:136–48. doi: 10.1109/THMS.2018.2791562
27. Herrero JF, Lorenzo G. An immersive virtual reality educational intervention on people with autism spectrum disorders (ASD) for the development of communication skills and problem solving. Educ Inf Technol. (2020) 25:1689–722. doi: 10.1007/s10639-019-10050-0
28. Lo YC, Chen YJ, Hsu YC, Tseng WYI, Gau SSF. Reduced tract integrity of the model for social communication is a neural substrate of social communication deficits in autism spectrum disorder. J Child Psychol Psychiatry. (2017) 58:576–85. doi: 10.1111/jcpp.12641
29. Robertson JM, Tanguay PE, L'ecuyer S, Sims A, Waltrip C. Domains of social communication handicap in autism spectrum disorder. J Am Acad Child Adolesc Psychiatry. (1999) 38:738–45. doi: 10.1097/00004583-199906000-00022
30. Santhanam SP, Hewitt LE. Perspectives of adults with autism on social communication intervention. Commun Disord Q. (2021) 42:156–65. doi: 10.1177/1525740120905501
31. Russo-Ponsaran N, Mckown C, Johnson J, Russo J, Crossman J, Reife I. Virtual environment for social information processing: assessment of children with and without autism spectrum disorders. Autism Res. (2018) 11:305–17. doi: 10.1002/aur.1889
32. Smith MJ, Pinto RM, Dawalt L, Smith JD, Sherwood K, Miles R, et al. Using community-engaged methods to adapt virtual reality job-interview training for transition-age youth on the autism spectrum. Res Autism Spectr Disord. (2020) 71:101498. doi: 10.1016/j.rasd.2019.101498
33. Didehbani N, Allen T, Kandalaft M, Krawczyk D, Chapman S. Virtual reality social cognition training for children with high functioning autism. Comput Hum Behav. (2016) 62:703–11. doi: 10.1016/j.chb.2016.04.033
34. Schmidt MM, Glaser N. Piloting an adaptive skills virtual reality intervention for adults with autism: findings from user-centered formative design and evaluation. J Enabling Technol. (2021) 15:137–58. doi: 10.1108/JET-09-2020-0037
35. Fitzgerald E, Yap HK, Ashton C, Moore DW, Furlonger B, Anderson A, et al. Comparing the effectiveness of virtual reality and video modelling as an intervention strategy for individuals with autism spectrum disorder: brief report. Dev Neurorehabil. (2018) 21:197–201. doi: 10.1080/17518423.2018.1432713
36. Bian D, Wade J, Swanson A, Weitlauf A, Warren Z, Sarkar N. Design of a physiology-based adaptive virtual reality driving platform for individuals with ASD. ACM Trans Accessible Comput. (2019) 12:3301498. doi: 10.1145/3301498
Keywords: autism spectrum disorder, virtual reality, cognition, social communication, developmental ability, nursing information
Citation: Zhao J, Zhang X, Lu Y, Wu X, Zhou F, Yang S, Wang L, Wu X and Fei F (2022) Virtual reality technology enhances the cognitive and social communication of children with autism spectrum disorder. Front. Public Health 10:1029392. doi: 10.3389/fpubh.2022.1029392
Received: 27 August 2022; Accepted: 15 September 2022;
Published: 06 October 2022.
Edited by:
Yanwu Xu, Baidu, ChinaReviewed by:
Jiangmei Liu, Chinese Center for Disease Control and Prevention, ChinaCopyright © 2022 Zhao, Zhang, Lu, Wu, Zhou, Yang, Wang, Wu and Fei. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoyan Wu, d3V4aWFveWFuMDcwNEAxMzkuY29t; Fangrong Fei, ZnJmZWlAY2RjLnpqLmNu
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.