 Jessie Adams
Jessie Adams Alison Kennedy1,2
Alison Kennedy1,2 Jacquie Cotton
Jacquie Cotton Susan Brumby
Susan Brumby
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health, 09 December 2022
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1027426
This article is part of the Research TopicSafeguarding Youth from Agricultural Injury and Illness: International ExperiencesView all 29 articles
Children on farms are at increased risk of injury. In Australia, children under 15 years consistently represent ~15% of all farm-related fatalities. This study aimed to develop parent and child surveys to gain a greater understanding of children's (5–14 years) exposure to occupational risk on farms by exploring their exposure to farm hazards, risk-taking behavior, their use and attitudes toward safety measures, and experience of farm-related injury. As farming communities are heterogeneous, a modified Delphi method was undertaken to ensure input from a diverse group. Seventeen experts participated in a three round process—the first two rounds required rating of proposed survey questions in an online questionnaire and the final round was an online discussion. Consensus was defined as 75% agreement or higher. This process resulted in 155 parent questions and 124 child questions reaching consensus to include. The modified Delphi method developed surveys that provide insight into the behaviors and attitudes of children (individuals) and their parents on farms (family) and will assist in informing how community, organizations and policy frameworks can improve child safety on farms. It will assist in identifying and understanding common farming exposures/behaviors of children and their parents to inform the development of targeted and culturally appropriate injury prevention strategies. As farming groups are heterogeneous, these survey scan be used on varying farming cohorts to identify their unique farming hazards and challenges. Child farm-related injuries are a problem globally and must be addressed; children are dependent on adults and communities to create safe environments for them.
Globally, children on farms have been identified as vulnerable to injury. In Australia, children represent ~15% of farm-related fatalities; a rate that has remained consistent for over 20 years (1). The key hazards responsible for these deaths are; water bodies, quad bikes, tractors, utility vehicles and cars, motorbikes and horses (1).
While consistent rates of farming injury—and the hazards contributing to injury—are well identified, children's behavior on farms and how they engage with farming hazards is not well understood. Internationally, some research has explored the individual aspects of children's exposure to the farm, including their risk, use of safety measures or farm tasks completed (2–8). Research conducted in Australia has explored fatal injury associated with specific farming hazards, such as water bodies and quad bikes (9, 10). However, much of what is known about behaviors on Australian farms remains anecdotal. To our knowledge there has been no surveys previously developed that sought to investigate children's engagement with the farm, targeting known key hazards, use of safety measures, attitudes toward farm safety and role on the farm.
The farming workplace is frequently also a place of residence and an embedded part of farming family lifestyle, culture and values. As such, children will always be involved in agriculture to some degree. While agriculture remains one of the most dangerous industries in Australia (11), it is imperative to understand how children's engagement can be managed and integrated in the safest way possible.
Shifting culture and patterns of behavior that may have been established over multiple farming generations requires a “whole of community” approach (12, 13). The socio-ecological model (SEM) considers how factors influence individuals' behaviors. Specifically, it highlights the interaction between the individual (intrapersonal), relationships (interpersonal), community and societal factors (14). Understanding how these factors interact and influence the safety of children on farms is important to facilitate behavior, cultural and legislative changes.
Community engaged research has been identified as a tool able to empower communities through inclusion, collaboration and participation. Participatory research can occur on many levels from “inform” where stakeholders are informed on a certain topic, through to “empower” where the community leads the research project (15). There are many benefits to participatory research, including benefits for the community (capacity building and shared decision making) (16); greater relevance and cultural sensitivity of research; greater participant recruitment; and, improved reliability and validity of research outcomes and translation of research findings (17, 18). A valuable tool for community engaged research is the Delphi method (17). The Delphi method was developed by the Research and Development Corporation (RAND) in the 1950s (19, 20). Typically, the multistage technique focuses on gaining consensus from a group of experts on a particular subject (21, 22). While the process has evolved over time, it continues to be based on two fundamental characteristics: (i) a series of iterative rounds where expert panelists provide their opinion, and (ii) the results of each round being shared with panelists before they provide feedback in the next round (23). Based on these fundamental characteristics, the Delphi method allows for flexibility to ensure the process is suitable and appropriate for the aims of the study and the panel of experts recruited (21).
Most research to date that has explored children's engagement with the farm has gathered information from the perspective of the parent. Ehrlich and colleagues (24) matched parent and child surveys on their knowledge, habits and attitudes around safety behaviors, concluding it was inaccurate to rely on parents' responses on their children's use of safety measures, as they overestimated their use. The results also showed a strong association between parents' role-modeling positive safety behaviors and reduced risk-taking by children. This highlighted the need and benefits for injury prevention to be a whole family issue. Therefore, it was deemed important to develop two surveys to gain insight from both parents and children to develop a more holistic understanding of risk-taking behaviors and use of safety measures on farms.
The aim of this study was to utilize a modified Delphi method to develop community-informed parent and child surveys to measure children's exposure to farming hazards, their risk-taking behaviors and experience of farm-related injury, and their use of—and attitudes toward—safety measures. The purpose is to describe a method that can be used by others to develop surveys specific to their country.
The Delphi method was used in this study to develop a set of survey questions to explore children's exposure to farming hazards, risk-taking behaviors, use of safety measures and experience of farm-related injury, from the perspective of parents and their children (aged 5–14 years). As such, the following modifications to the traditional process were implemented.
1. Literature review: Traditionally, a single open-ended question would have been asked of panelists in the first round of the Delphi method. In this study, a review of the literature was undertaken to inform the development of a series of proposed closed-ended questions to undergo rating by the panel. This has become a widely accepted modification (25).
2. Rating scale: A five-or nine-point Likert scale is typically used in rating items via the Delphi method. In this study, the panel were asked to rate the proposed questions as either “yes” (to be included in the final survey), “no” (to be removed) or “unsure or needs further editing” (26, 27). This meant panelists had to make more definitive decisions with their rating of proposed questions.
3. Anonymity of the panel: Traditionally, Delphi panels remain anonymous to each other throughout the whole process. This is largely to avoid bias and potential influencing on decision-making. However, more recently, the combination of anonymous rounds and a subsequent face-to-face discussion have been successfully used (26, 27). The current three round study consisted of two rounds requiring panelists to complete online surveys (anonymous to other participants) and the final round held as an online discussion. This allowed all panelists to come together to discuss and clarify the remaining questions that were yet to reach consensus after the first two rounds. However, rating of the remaining questions was still completed anonymously.
There were benefits for utilizing a modified Delphi method to develop the two surveys. Previous research has described consensus as a reliable contingency and acceptable to achieve construct validity (28). Hutchings and colleagues (29) determined the Delphi method to be more reliable than nominal groups in using consensus in the development of clinical guidelines. Additionally, the use of the Delphi method allowed a group of experts and end-users from various geographical locations to assist and be involved in the development of the two surveys (30). This resulted in panelists being consulted and involved throughout the development of the surveys ensuring a participatory research process (15). The modest number of participants required allowed the study to be conducted with the limited resources available (31, 32). Utilizing the mixed methods of panelists rating questions on inclusion and providing qualitative responses allowed for thorough feedback and consideration of each proposed question. The online discussion of the remaining questions ensured all panelists could raise their uncertainties. Further, maintaining anonymity of individual panelists rating throughout the process ensured they could be comfortable providing their opinions and not be influenced by others which may have occurred if a focus group was utilized (e.g., dominating personalities or people they may identify as superior) (30). The providing of result reports following the first and second rounds allowed panelists to see how others were rating the proposed questions and the comments provided, this allowed them to reflect and potentially adjust their rating in the following rounds.
Ethics approval was obtained from Deakin University Research Ethics Committee (Ref: 2020-355).
There are no specific guidelines on who or how many participants to include in a Delphi panel. Each participant must be justified as a topic expert and the panel should represent variation in cognition, expertise and experience (21, 22, 26). Therefore, multidisciplinary experts with varied experience (agriculture, health, research, farming parents, and policy development) from varying geographic locations (across Australia and internationally) were invited to participate.
Potential panelists were identified through a combination of purposive and convenience sampling, drawing on the direct and extended networks of the National Center for Farmer Health (25). These included child farm safety specialists, injury data experts, child farm safety educators, farm safety researchers, farming parents, rural health researchers, agricultural industry and government representatives, and medical professionals. In total, 27 professionals were invited via email to participate, resulting in 17 consenting to participate in round one (see Table 1 for description of panel participants).
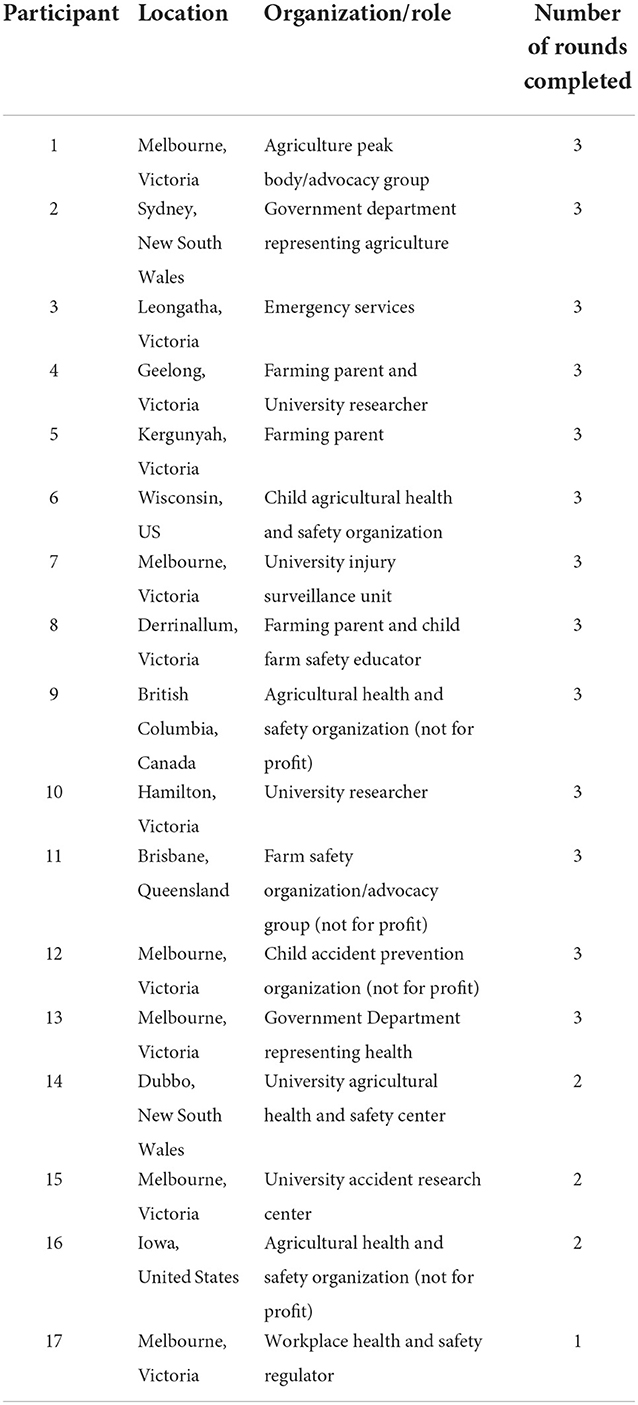
Table 1. Panel participants in the modified Delphi study.
Panel retention has been highlighted as a key aspect of a successful Delphi method (21). The research team encouraged panel retention by: (i) providing a brief description of the overall process so panelists were aware of the total commitment required, (ii) ensuring that those who were invited to participate had a demonstrated interest in the safety of children on farms, (iii) ensuring the process was undertaken in a short time frame, and (iv) encouraging a sense of panelist ownership over the survey development by creating each round from the results of the previous round (21, 26, 33).
The Delphi method relies on agreement between participants. This “consensus” is defined as the minimum acceptable percentage of agreement between panelists. Literature suggests it is crucial to predefine the level of consensus for a study (21, 26, 33, 34). However, there are no consistent guidelines for determining consensus. Previous literature has suggested varying levels of consensus. Nair et al. (33) recommended between 70 and 80% agreement is appropriate, Niederberger and Spranger (22) endorsed over 60% consensus. Jimenez-Garcia et al. (35), Woodcock et al. (36) and Keeney and colleagues (37) all suggested 75% agreement as appropriate in determining consensus. In the current study, consensus was set at 75% or higher agreement.
Figure 1 demonstrates the process undertaken in this modified Delphi method. Round one required the 17 panelists to rate proposed questions developed from a review of the literature exploring injury and safety of children on Australian farms (38). The questions developed were a combination constructed by the research team aiming to target the themes and gaps in knowledge identified in the literature review. Where possible, questions that had been used in previous research were utilized (6, 7, 39–45). During question development, all levels of the SEM model were considered including individual (e.g., child demographics); relationships (e.g., the behaviors of those closest to the child including parents); community (e.g., the physical and social environment including the safety measures in place on the farm); and, societal (e.g., cultural norms/influences including what factors influence where children are allowed on the farm) (14). Exploring how these factors interact and influence the safety of children on farms is important to understand behavior and consequently how to influence behavior change.
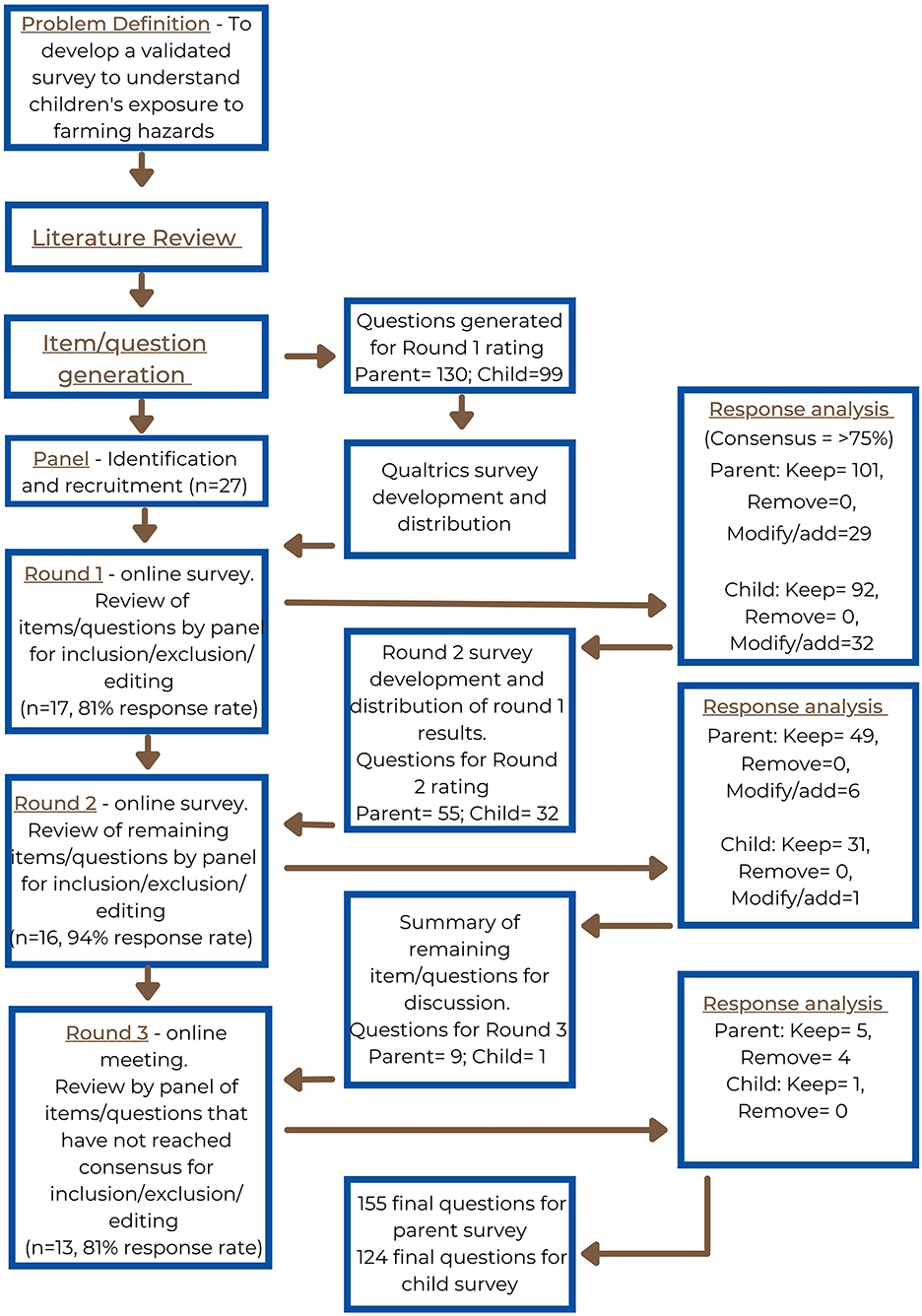
Figure 1. The modified Delphi method utilized in this study (25).
Questions underwent a pre-Delphi piloting process where a selection of parents (n = 7) and their children (within the survey age range of 5–14 years) were asked to provide feedback on question comprehension, wording and overall survey. This ensured the questions presented to the Delphi panel in round one were suitable for the study's target audience. The proposed questions were formatted as an online survey using Qualtrics with questions split into those targeting parents and those for children. Panelists were asked to rate each proposed question using a three-point scale; “yes” (to be included in the final survey), “no” (to be removed), or “unsure or needs further editing”. They were able to provide comments on their decisions, which were then themed and utilized in round two of the process. The three-point scale meant panelists had to make more definitive selections, therefore, assisting in more immediate consensus (33).
Analysis was conducted after each round using the Statistical Package for the Social Sciences (SPSS) (version 27). The percentage agreement on each question was calculated. Agreement of 75% or higher for “yes” or “no” was deemed consensus and the question was removed from future rounds (25, 34, 36). The qualitative comments were grouped per question; the comments on the proposed questions that had not reached consensus to keep were analyzed and alterations were made accordingly. Additionally, new questions were developed from suggestions by the panelists. The altered and new questions were then rated in round two. Result reports were developed for each panel member outlining their individual response per question, the overall panel results and the qualitative feedback (25). Following each round, the result reports were sent to each panelist to allow them to compare their decisions to the overall panel and to see how the survey was being developed from their feedback (21, 22, 30, 33).
Round two followed the same process as the first round with 16 panelists completing the rating of proposed questions. The Qualtrics survey for this round was developed from the results of the first round. This resulted in panelists re-rating questions that had not yet reached consensus (parent survey n = 29, child survey n = 7) as well as rating additional questions developed from the qualitative feedback provided (parent survey n = 26, child survey n = 25) (25, 26, 33, 36). In round one, panelists provided qualitative comments after each question category. During analysis, qualitative comments were themed—this included collating comments about each proposed round one question and any additional comments/question suggestions for each question category group. Where deemed appropriate by the research team (i.e., where there was a gap in the proposed questions and where this was considered within the scope of the study), the proposed new questions were then added to the next round of rating, or the wording of previously proposed questions was altered, or multiple choice options were added in previously developed questions. An example of a new question added to round two for rating was “does your child engage with other farming hazards?” This question was developed following panelist feedback on the need to explore other possible hazards. An example of an amended question seeking a more specific understanding was “are there factors you take into consideration when deciding what areas of the farm your child is allowed to go to?” This was amended from “what contributes to your decision to allow your child into the farm workplace?” Rating was completed using the same three-point scale as the previous round. Analysis was conducted in the same way and result reports were disseminated to panelists.
The final round was held as an online face-to-face Zoom discussion with the aim of reaching efficient consensus on the remaining questions. Until this point, the panel had been anonymous to each other. This modification to the traditional Delphi method has become more common with Boulkedid and colleagues (26) suggesting more than half of all Delphi studies in their systematic review had at least one meeting of panelists. Thirteen panelists attended the online meeting. Each of the remaining questions were presented to the panel (parent survey n = 6, child survey n = 1) as well as three additional questions for the parent survey, these were all discussed and then rated. The rating of questions was altered slightly from the previous two rounds—panelists were asked to rate questions at the time as either “yes” or “no”—the “unsure” option was removed as panelists could raise their uncertainties and discussion could take place, this was to ensure consensus was achieved by the end of the round. The online program Mentimeter was used for live voting as it ensured rating was still anonymous. If consensus was not reached, further discussion was held and amendments to the question were made before rating was completed again until consensus was reached. Questions that reached consensus to be removed in this round were the disclaimer statements (e.g., “certain authorities” state that children under 16 are not to ride on or operate quad bikes) added in to round two following feedback from some panelists. However, comments provided by other panelists and discussion within the research team highlighted the influence these statements could have on parents answering the survey, resulting in bias. Following discussion in this round, it was agreed that these would be removed.
Following the final Delphi round, the two final surveys were developed in Qualtrics with all questions that had reached consensus to be included. A final review was then conducted by the research team to assess the questions and survey flow/logic, minor alterations and removal of redundant questions was completed.
Table 2 demonstrates the results by each round of the Delphi method to develop the parent survey. In the first round, the 17 panelists rated 130 proposed questions, 78% (n = 101) of which reached consensus to include in the final survey and 22% (n = 29) did not reach agreement. No questions were removed.
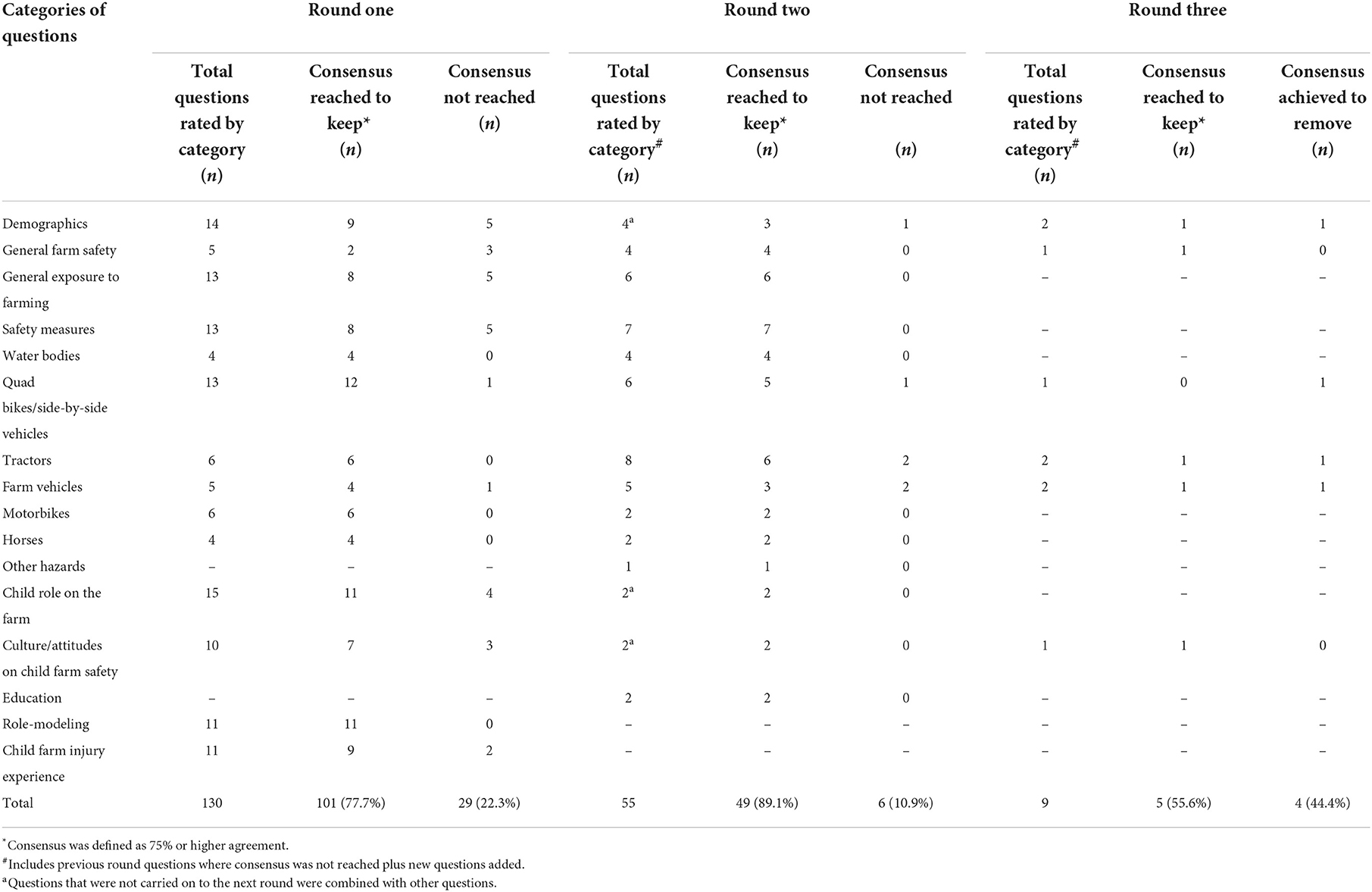
Table 2. Results of the Delphi method consensus process for the parent survey by round and question category.
The second round consisted of questions that had not reached consensus in the first round, along with additional questions/altered questions following analysis of the qualitative comments. The main themes arising from panelist comments included (i) the need to remove open ended questions and provide multiple choice options, (ii) alterations in question construction and wording, and (iii) the need to focus questions on the key hazards causing child injury.
Of the 55 questions rated, the 16 panelists reached consensus to keep 89% (n = 49) of the questions and 11% (n = 6) remained unresolved.
The online discussion resulted in 13 panelists coming together to discuss the remaining questions. Five (56%) were kept and four (44%) were removed from the final parent survey.
Table 3 demonstrates the results per round of the Delphi method for the development of the child survey. Panel consensus was very high in the development of the child survey questions. Panelists rated 99 proposed questions for the development of the child survey; 93% (n = 92) reached consensus to be included in the final child survey and 7% (n = 7) remained unresolved. The qualitative comments provided by panelists on the child survey was consistent with comments on the parent survey. Panelists did highlight some questions were too complex for children so small changes were made to make it simpler for children to answer.
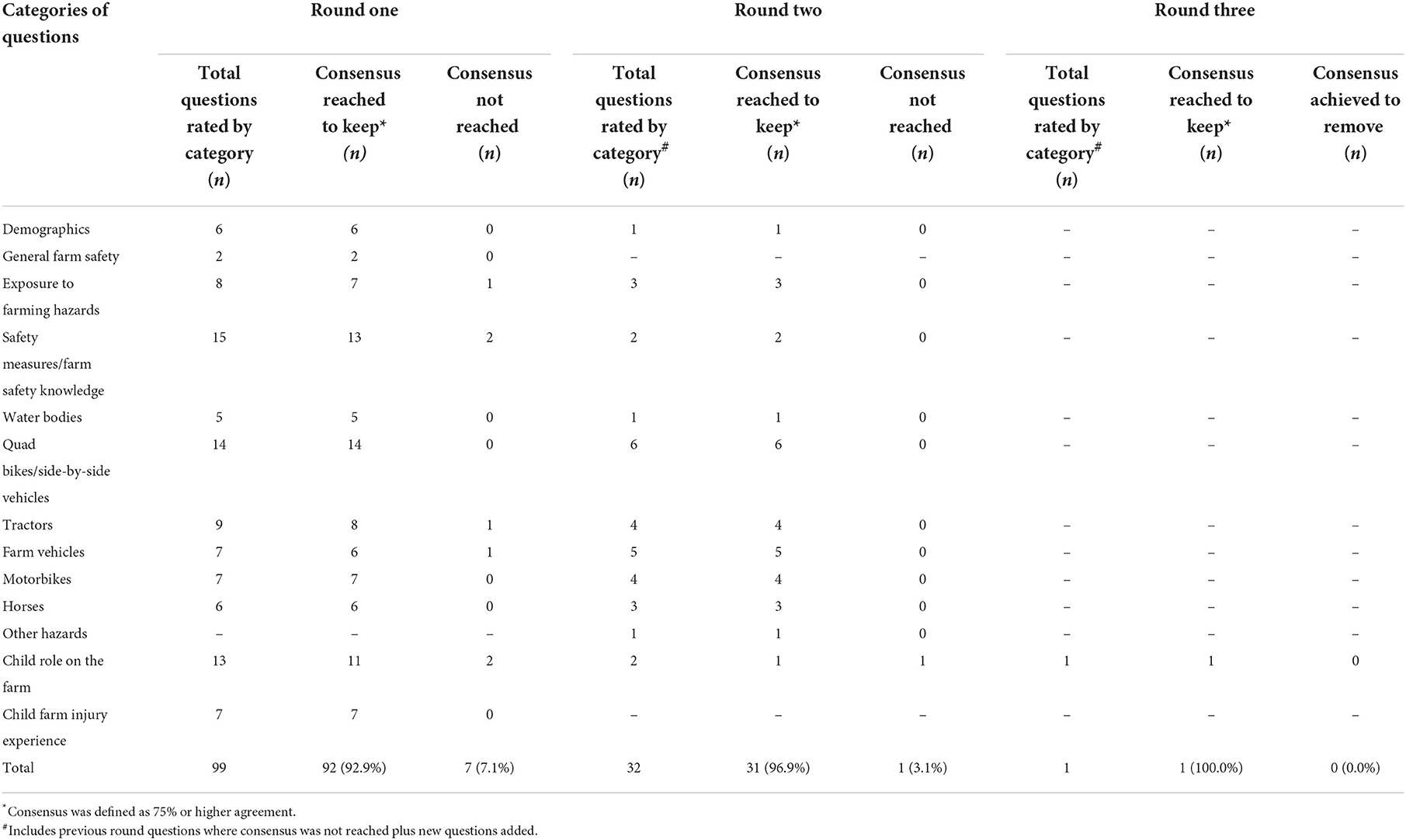
Table 3. Results of the Delphi method consensus process for the child survey by round and question category.
Round 2 saw similar results with 97% (n = 31) reaching consensus to include and 3% (n = 1) remained. The panel reached consensus to keep the remaining proposed question during the online discussion round.
Table 4 provides a summary of results of the Delphi method showing 155 questions reached consensus to be included in the parent survey and 124 for the child survey.
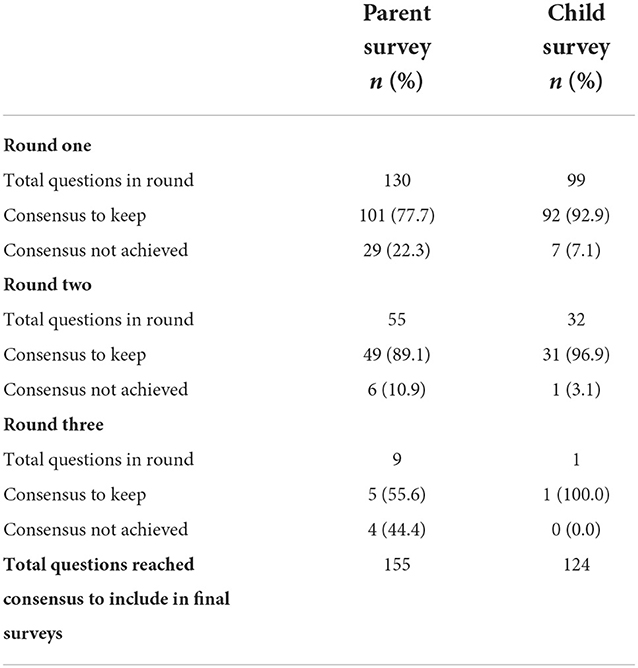
Table 4. Summary table of the Delphi method for each round.
The modified Delphi method utilized in this study was effective in developing two surveys to explore children's exposure to farming hazards, risk-taking behaviors, attitudes and use of safety measures, and experience of injury. The mixed method nature of the modified Delphi (including rating and qualitative data) allowed for a more thorough identification of appropriate questions, as well as a greater understanding of panelist reasoning behind the rating choices and the subsequent amending or adding new questions. Furthermore, holding the final (3rd) round as a live online discussion with anonymous ratings, encouraged varying opinions to be shared and allowed all panelists to feel comfortable providing their individual opinions.
The results of the Delphi method highlighted the value and importance of collaboration and participatory research. Although there was >70% agreement in the parent and 90% in the child proposed questions after the first round of rating, uncertainty still remained in 20% and 7% of proposed questions, respectively. This collaborative/participatory method enabled improvements in the relevance and cultural sensitivity of the surveys (17, 18). The comments and level of disagreement on some proposed questions demonstrates the process rigor. This resulted in improved use of language, additional collaboratively-agreed-upon questions, inclusion of appropriate examples and multiple choice options. While efforts were made to ensure a diverse representation of experts involved in the Delphi, the overall number of participants (n = 17) was not large. Consideration for inclusion in the panel included organizational affiliation, experience, academic qualification, geographical location and recommendation by others (22, 31). In a Delphi method, group size does not rely on statistical power and there is no agreed upon minimum number of panelists recommended (31). Rather, the focus is on multidisciplinary representation, differences in cognition, expertise and experiences as well as potential group dynamics (22, 26, 46).
A potential limitation to this study was the high consensus between the panel members in regard to the child survey. It is suggested this may be due to the child survey questions being presented after the adult questions in every round (47). It is not believed this influenced the development of validity of the final child survey as the additional questions introduced in round two were aligned to the results of the parent survey to ensure the two surveys would be comparable. It is recommended in future research that the order of the proposed questions for a survey be changed between rounds, as panelists may fatigue toward the end of each round.
The Delphi method relies on group consensus, and while the panelists that participated in this study were deemed “experts” in the field, there is the potential that the results are not necessarily the most correct, as they are still based on opinion (23). However, when there is no other evidence available, the reliance on group opinion is believed to be a better basis and superior than the dependence on an individual judgement (48, 49). As child farm-related injury rates have remained consistent over an extended period, a new approach is required.
The consensus between panelists to “keep” questions was high, resulting in a large number of questions to be included in the final surveys. As described above, following the completion of the three Delphi rounds, the research team assessed the questions and removed any questions that had become redundant throughout the rounds. Further, survey logic was added to ensure participants were not asked to answer any questions that were not relevant to them, reducing completion time.
Following the development of the two surveys, the parent survey will be promoted throughout rural/regional Victoria for completion. Once a parent completes the survey, they will be emailed a link for their child to complete the survey. It is aimed 100 surveys will be completed in this study.
The survey age range (5–14 years) will facilitate a greater understanding of the different safety attitudes and farm activities that children—of varying ages—are undertaking on farms. Previous international research has described children's engagement on the farm as varying—depending on factors such as age and developmental level (3, 4, 8). Future analysis of survey results, will enable comparisons between different age cohorts to see trends in children's behaviors on the farm as they develop. This should assist in the identification and improvement of age appropriate interventions.
This modified Delphi method supported the development of surveys that can assess the behaviors and attitudes of children (individuals), and their parents (relationships) on farms. This will provide insight on how community, organizations and policy frameworks can interact to assist in the development of effective and appropriate interventions to improve child safety on farms. As farming communities are heterogeneous, these surveys will be able to be used across varying farming cohorts (e.g., geographic or industry) to identify specific challenges/behaviors, and assist in developing targeted and appropriate responses to child safety. The resulting surveys may be used longitudinally—with the ability to track change in industry behaviors and attitudes overtime and evaluate the effect of any interventions and parental awareness of safety for children on farms.
Child farm injury and fatalities have been consistent and an ongoing global shame for centuries. Children are reliant on the adults around them to provide them with a safe environment. Therefore, more needs to be done to understand the farming life/behaviors of children. This study utilized a modified Delphi method that resulted in the development of parent and child surveys to explore children's exposure to farming hazards, risk-taking behaviors, attitudes and use of safety measures and experience of farm-related injury. The consideration of each of the SEM levels within this study will ensure factors influencing behaviors are identified to assist in developing effective, appropriate and targeted “whole of community” initiatives to address child farm-related injury.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Deakin University Research Ethics Committee (Ref: 2020-355). The patients/participants provided their written informed consent to participate in this study.
JA conducted the data collection, data analysis, and drafting of the manuscript. AK, SB, and JC provided guidance and supervision throughout the study. All authors contributed to the study design, reviewing and editing of the manuscript, and approved the final manuscript.
JA is supported through an Australian Government Research Training Program Scholarship.
The authors would like to acknowledge the contributions of the Delphi panel members that provided their time and expertise to develop these two surveys.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Peachey K, Lower T, Rolfe M. Protecting the future: fatal incidents on Australian farms involving children (2001–2019). Aust J Rural Health. (2020) 28:1–9. doi: 10.1111/ajr.12650
2. Browning S, Westneat S, Reed D. Farm work injuries among a cohort of children in Kentucky. USA Ann Agric Environ Med. (2016) 23:604–11. doi: 10.5604/12321966.1226854
3. Nilsson K. Parents' attitudes to risk and injury to children and young people on farms. PLoS ONE. (2016) 11:e0158368. doi: 10.1371/journal.pone.0158368
4. Summers P, Quandt S, Spears Johnson C, Arcury T. Child work safety on the farms of local agricultural market producers: parent and child perspectives. J Agromed. (2018) 23:52–9. doi: 10.1080/1059924X.2017.1387635
5. Becot F, Bendixsen C, Barnes K, Rudolphi J. Broadening our understanding of farm children's risk exposure by considering their parents' farming background. IJERPH. (2021) 18:5218. doi: 10.3390/ijerph18105218
6. McCurdy SA, Kwan JA. Ethnic and gender differences in farm tasks and safety practices among rural california farm youth. J Occup Environ Hyg. (2012) 9:362–70. doi: 10.1080/15459624.2012.679584
7. Reed DB, Browning SR, Westneat SC, Kidd PS. Personal protective equipment use and safety behaviors among farm adolescents: gender differences and predictors of work practices. J Rural Health. (2006) 22:314–20. doi: 10.1111/j.1748-0361.2006.00052.x
8. Lachowski S, Lachowska BH. Adolescent work on family farms in Poland: an assessment of hazards. Ann Agric Environ Med. (2020) 27:672–9. doi: 10.26444/aaem/130924
9. McIntosh AS, Patton DA, Rechnitzer G, Grzebieta R. Injury mechanisms in fatal Australian quad bike incidents. Traffic Inj Prev. (2016) 17:386–90. doi: 10.1080/15389588.2015.1091073
10. Wallis BA, Watt K, Franklin RC, Nixon JW, Kimble RM. Where children and adolescents drown in Queensland: a population-based study. BMJ Open. (2015) 5:e008959-e. doi: 10.1136/bmjopen-2015-008959
11. Safe Work Australia. Work-related Traumatic Injury Fatalities. Canberra: Safe Work Australia (2019).
12. Rose DC, Keating C, Morris C. Understanding How to Influence Farmers' Decision-Making Behaviour: A Social Science Literature Review. Nottingham: University of Nottingham: Agriculture and Horticulture Development Board (2018).
13. Orozco FA, Cole DC, Ibrahim S, Wanigaratne S. Health promotion outcomes associated with a community-based program to reduce pesticide-related risks among small farm households. Health Promot Int. (2011) 26:432–46. doi: 10.1093/heapro/dar006
14. Centres for Disease Control Prevention. The Socio-Ecological Model: A Framework for Prevention. Atlanta: Centres for Disease Control and Prevention (2022). Available online at: https://www.cdc.gov/violenceprevention/about/social-ecologicalmodel.html (accessed June 20, 2022).
15. Vaughn LM, Jacquez F. Participatory research methods-choice points in the research process. J Particip Res Methods. (2020) 1:13244. doi: 10.35844/001c.13244
16. Mikesell L, Bromley E, Khodyakov D. Ethical community-engaged research: a literature review. Am J Public Health. (2013) 103:7–14. doi: 10.2105/AJPH.2013.301605
17. Brady SR. Utilizing and adapting the Delphi method for use in qualitative research. Int J Qual Methods. (2015) 14:1–6. doi: 10.1177/1609406915621381
18. Anderst A, Conroy K, Fairbrother G, Hallam L, Taylor V. Engaging consumers in health research: a narrative review. Health Serv Res. (2020) 44:806–13. doi: 10.1071/AH19202
19. Fitch K, Bernstein SJ, Aguilar MD, Burnand B, LaCalle JR, Lazaro PvhL M, et al. The RAND/UCLA Appropriateness Method User's Manual. Santa Monica: RAND (2001).
20. Research Development Corporation (RAND). Delphi Method. Santa Monica: RAND (2021). Available online at: https://www.rand.org/topics/delphi-method.html (accessed March 20, 2022).
21. Trevelyan EG, Robinson N. Delphi methodology in health research: how to do it? Eur J Integr Med. (2015) 7:423–8. doi: 10.1016/j.eujim.2015.07.002
22. Niederberger M, Spranger J. Delphi technique in health sciences: a map. Public Health Front. (2020) 8:457. doi: 10.3389/fpubh.2020.00457
23. Barrett D, Heale R. What are Delphi studies? Evid Based Nurs. (2020) 23:68–9. doi: 10.1136/ebnurs-2020-103303
24. Ehrlich P, Helmkamp J, Williams J, Haque A, Furbee P. Matched analysis of parent's and children's attitudes and practices towards motor vehicle and bicycle safety: an important information gap. Inj Control Saf Promot. (2004) 11:23–38. doi: 10.1076/icsp.11.1.23.26307
25. Taylor E. We agree, don't we? The Delphi method for health environments research. HERD J. (2020) 13:11–23. doi: 10.1177/1937586719887709
26. Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS ONE. (2011) 6:e20476. doi: 10.1371/journal.pone.0020476
27. Hernan AL, Giles SJ, O'Hara JK, Fuller J, Johnson JK, Dunbar JA. Developing a primary care patient measure of safety (PC PMOS): a modified Delphi process and face validity testing. BMJ Qual Saf. (2016) 25:273–80. doi: 10.1136/bmjqs-2015-004268
28. Cross H. Consensus methods: a bridge between clinical reasoning and clinical research? Int J Lepr Other Mycobact Dis. (2005) 73:28–32. doi: 10.1489/1544-581X(2005)7328:CMABBC2.0.CO;2
29. Hutchings A, Raine R, Sanderson C, Black N. A comparison of formal consensus methods used for developing clinical guidelines. J health Serv Res Policy. (2006) 11:218–24. doi: 10.1258/135581906778476553
30. MacLennan S, Kirkham J, Lam TBL, Williamson PR. A randomized trial comparing three Delphi feedback strategies found no evidence of a difference in a setting with high initial agreement. J Clin Epidemiol. (2018) 93:1–8. doi: 10.1016/j.jclinepi.2017.09.024
31. Okoli C, Pawlowski SD. The Delphi method as a research tool: an example, design considerations and applications. Inf Manag. (2004) 42:15–29. doi: 10.1016/j.im.2003.11.002
32. Roney L, McKenna C. Determining the education and research priorities in pediatric trauma nursing: a Delphi study. J Trauma Nurs. (2018) 25:290–7. doi: 10.1097/JTN.0000000000000390
33. Nair R, Aggarwal R, Khanna D. Methods of formal consensus in classification/diagnostic criteria and guidleline development. Sem Arth Rheum. (2011) 41:95–105. doi: 10.1016/j.semarthrit.2010.12.001
34. Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, et al. Defining consensus: a systemative review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. (2014) 67:401–9. doi: 10.1016/j.jclinepi.2013.12.002
35. Jimenez-Garcia JA, Hong AK, Miller MA, DeMont R. The child focused injury risk screening tool (ChildFIRST) for 8–12-year-old children: a validation study using a modified Delphi method. Measur Phys Educ Exer Sci. (2020) 24:235–46. doi: 10.1080/1091367X.2020.1793344
36. Woodcock T, Adeleke Y, Goeschel C, Pronovost P, Dixon-Woods M. A modified Delphi study to identify the features of high quality measurement plans for healthcare improvements projects. BMC Med Res Methodol. (2020) 20:1–9. doi: 10.1186/s12874-019-0886-6
37. Keeney S, Hasson F, McKenna H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J Adv Nurs. (2006) 53:205–12. doi: 10.1111/j.1365-2648.2006.03716.x
38. Adams J, Kennedy A, Cotton J, Brumby S. Child farm-related injury in australia: a review of the literature. IJERPH. (2021) 18:1–16. doi: 10.3390/ijerph18116063
39. Stiller L, Depczynski J, Fragar L, Franklin R. An evidence-consultation base for developing child injury prevention priorities for Australian farms. Health Promot J Aust. (2008) 19:91–6. doi: 10.1071/HE08091
40. Depczynski J, Fragar L, Hawkins A, Stiller L. Safe play areas for prevention of young children drowning in farm dams. AJEC. (2009) 34:50–7. doi: 10.1177/183693910903400307
41. Bailey J, Dutton T, Payne K, Wilson R, Brew BK. Farm safety practices and farm size in New South Wales. J Agromed. (2017) 22:229–34. doi: 10.1080/1059924X.2017.1318101
42. Zentner L, Berg R, Pickett W, Marlenga B. Do parents' perceptions of risks protect children engaged in farm work? Prev Med. (2005) 40:860–6. doi: 10.1016/j.ypmed.2004.10.007
43. Browning S, Westneat S, Donnelly C, Reed D. Agricultural tasks and injuries among kentucky farm children: results of the farm family health and hazard surveillance project. South Med J. (2003) 96:1203–12. doi: 10.1097/01.SMJ.0000082014.94642.06
44. Lachowski S. Health consequences of work in childhood in opinions of respondents from agricultural families. Ann Agric Environ Med. (2013) 20:624–30. doi: 10.13075/mp.5893.2013.0032
45. Lachowski S, Zagorski J. Child labour for the benefit of the family in rural Poland. Ann Agric Environ Med. (2011) 18:386–92.
46. Willems J, Sutton K, Maybery D. Using a Delphi process to extend a rural mental health workforce recruitment initative. J Ment Health Train Educ Pract. (2015) 10:91–9. doi: 10.1108/JMHTEP-10-2014-0033
47. Brookes ST, Chalmers KA, Avery KNL, Coulman K, Blazeby JM. Impact of question order on priositisation of outcomes in the development of a core outcome set: a randomised controlled trial. Trials. (2018) 19:1–11. doi: 10.1186/s13063-017-2405-6
48. Sniezek JA, Henry RA. Accuracy and confidence in group judgment. Organ Behav Hum Decis Process. (1989) 43:1–28.
Keywords: Delphi technique, child, parent, risk-taking, agriculture, farms, Australia, attitude
Citation: Adams J, Kennedy A, Cotton J and Brumby S (2022) Utilizing the Delphi method to develop parent and child surveys to understand exposure to farming hazards and attitudes toward farm safety. Front. Public Health 10:1027426. doi: 10.3389/fpubh.2022.1027426
Received: 25 August 2022; Accepted: 22 November 2022;
Published: 09 December 2022.
Edited by:
Richard Franklin, James Cook University, AustraliaReviewed by:
Jacques Oosthuizen, Edith Cowan University, AustraliaCopyright © 2022 Adams, Kennedy, Cotton and Brumby. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessie Adams, amVzc2llLmFkYW1zQHdkaHMubmV0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.