 Seo Yoon Lee
Seo Yoon Lee Jung Jae Lee2,3,4
Jung Jae Lee2,3,4
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 13 December 2022
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1024751
This article is part of the Research Topic Community Series in Mental Illness, Culture, and Society: Dealing with the COVID-19 Pandemic - Volume III View all 10 articles
Background: Individuals are at an increased risk of adverse mental health outcomes during the COVID-19 pandemic. To reduce the impact on mental health outcomes that were induced by national-level policies, which may influence an individual at the community level, exploring the comprehensive relations between individual and environmental factors are needed. The aim is to examine socio-ecological factors associated with mental health outcomes, including depressive and anxiety symptoms, with the perspective of support to provide interventions that help the community during future disease outbreaks.
Method: From 5 November to 20 November 2020, a cross-sectional and population-based study was conducted to assess the socio-ecological factors of mental health outcomes during the COVID-19 pandemic. A total of 1,000 participants, aged 20–69 years, in Chungnam Region, South Korea, were included in this study. Multiple linear regression models were used to examine the association between socio-ecological factors and mental health outcomes. The primary outcomes were individuals' mental health outcomes which are measured by PHQ-9 and GAD-7 scores.
Results: Of the 1,000 participants, the average PHQ-9 was 4.39, and GAD-7 was 3.21 during the COVID-19 pandemic. Specifically, the participants with moderate or severe levels of PHQ-9 and GAD-7 were 12.6 and 6.8%, respectively. Higher levels of depressive and anxiety symptoms were associated with participants who were single, reported a lower household income, had decreased support from friends or family, and increased stress from the workplace or home. In subgroup analyses by age, gender, and household income, a similar trend was reported in individual and interpersonal-level factors. There were significant associations between regional-level factors, including gross regional domestic product (GRDP), mental health institutions, psychiatrists, nurse-to-population ratios, and individuals' mental health outcomes.
Conclusion: The management of depressive and anxiety symptoms of individuals during the pandemic was better explained by individual and interpersonal characteristics rather than regional-level factors, highlighting the need for more policies aimed at these lower levels.
Due to the coronavirus disease 2019 (COVID-19) pandemic, countries have implemented various policies to prevent the spread, such as social distancing, multiple facility closures, and restrictions on travel. Such policies resulted in many changes in the lifestyles of people across the world. Before the COVID-19 pandemic, there was a case to be made for other infectious diseases (e.g., H1N1 and seasonal influenza) having an impact on public mental health (1, 2). There are multiple studies reporting the physical effects and sequelae, including myalgia, physical inactivity, cough, fever, breathing difficulty, and gastrointestinal symptoms caused by COVID-19 (3–6). Besides the physical effects, significant impacts on mental health including depression, anxiety, and suicidal ideation/behavior were reported around the world (7–17). In addition, unlike the physical effects, the impact on mental health not only affects individuals with direct virus contact but also the general public. In March 2020, in the US, the percentage of adults reporting the negative influence of COVID-19-related stress on their mental health was about 32% which increased to 53% by July 2020 (13). In South Korea, compared with the control group (i.e., matched individuals from the pre-pandemic period in 2019), individuals undergoing self-quarantine during the COVID-19 pandemic reported higher levels of depressive symptoms and a higher prevalence of major depression (14).
Among multiple methods to manage the population's mental health, enforcing a support system is one of the effective methods to implement for the public. There are multiple types of support defined (18). According to Cobb (19), although social support directly or indirectly affects mental health, depending on the type of support (i.e., instrumental, active, or material), the effect differs, and it is important to distinguish. Cobb's primary argument was that we should make a distinction between social support as perceived by an individual and social support as received in the form of resources or participation in supportive activities (18, 19). However, there was no study that investigated the effects of different types of support. Thus, in this study, individual- or interpersonal-level factors were focused on active support (i.e., marital status, support from friends and family, and stress from work and home) and regional-level factors were focused on instrumental or material support (i.e., mental health institution-to-population ratio and psychiatrist-to-population ratio).
Socio-ecological models were developed for a further understanding of the dynamic interrelations among various personal and environmental factors. Individual, interpersonal, and regional characteristics are likely to be connected to mental health outcomes among individuals in the community at various socio-ecological levels (20–22). To date, studies have provided evidence of the importance of factors at each level (22, 23). However, there is an existing gap confirming that, to our knowledge, no factors have been simultaneously examined at any socio-ecological level. Additional studies are needed to understand the range of socio-ecological factors contributing to mental health outcomes among community individuals in South Korea. Thus, this study aims to examine the association between socio-ecological factors (individual, interpersonal, and regional) and the individuals' mental health outcomes related to support in the general Korean population during the COVID-19 pandemic.
This study used data from a cross-sectional survey targeting adults aged 20–69 years in the Chungnam Region of South Korea and investigated their mental health, experiences, and perceptions of the COVID-19 pandemic, and the psychosocial effects of COVID-19. Data were collected via conventional face-to-face interviews or an online survey panel. Embrain Public® recruited the online survey panel through the random sampling of residential addresses throughout Korea at the end of October 2020. The participants answered the questionnaires anonymously via online survey or face-to-face interviews conducted from 5 November to 20 November 2020. Individuals voluntarily chose to participate by signing up on a panel platform. Online surveys or face-to-face interviews were conducted at the same time, and participants can be selected on how they would like to share their information. Of the 1,000 participants, 610 participated via online surveys, and 390 participated via face-to-face interviews. All participants provided informed consent prior to completing the study. The study included 16 Korean regional-level administrative districts, comprising seven cities (“Si”), seven counties (“Gun”), and two districts (“Gu”), to cover the Chungnam region.
The primary outcome variables were the participants' self-reported depression and anxiety levels. We used the Korean version of the Patient Health Questionnaire-9 (PHQ-9) to measure depressive status (24). The questionnaire consisted of nine items with a 4-point Likert scale ranging from 0 (never) to 3 (nearly every day) assessing the frequency of depressive symptoms over the past 2 weeks. The PHQ-9 score ranges from 0 to 27 points, and higher scores indicate more severe depression (25–27). The Korean version of the Generalized Anxiety Disorder-7 (GAD-7) scale was used to assess anxiety symptoms (28). The GAD-7 is composed of seven items assessing the frequency of anxiety over the past 2 weeks on a 4-point Likert scale ranging from 0 (never) to 3 (nearly every day). The total score of GAD-7 ranges from 0 to 21, and higher scores reflect greater severity of anxiety.
Socioeconomic and interpersonal factors were selected based on previous studies on individual levels (15). Socioeconomic factors included age, gender, job status, marital status, average monthly household income, and education level. Since the survey was conducted using two different methods (i.e., face-to-face interview and online survey), the data collection method was controlled. As for interpersonal factors, the researchers collected the variables that measure the negative changes and the self-role disruptions in the participant's life due to COVID-19 (i.e., in social life and home). Specifically, the negative changes depend on whether the support from friends and family members has decreased and the stress from the workplace and home has increased.
Regional-level variables included the district's gross regional domestic product (GRDP), the community's mental health utilization indicators (i.e., mental health institution-to-population ratio, psychiatrist-to-population ratio, and nurse-to-population ratio), and the rates of unmet healthcare needs. GRDP is the sum of the market prices of all final goods and services produced within an administrative district for a certain period and is used to determine the economic structure or size. According to the European Parliament, an unmet healthcare need is defined as a state in which there is no existing satisfactory method of prevention, diagnosis, and treatment (29).
One-way ANOVA was conducted to determine whether there were any differences between the PHQ-9 and GAD-7 among districts (Figure 1). Although individuals were nested within region-level administrative districts of Chungnam Region, since there were no statistically significant differences between the districts, the generalized linear model was not employed. Descriptive statistics were conducted for all variables in the analysis (Table 1), and independent t-tests, one-way ANOVA, and chi-square tests were examined for differences between participants in the sample. Multicollinearity was tested, and the highest variance inflation factor (VIF) was 2.8, which is less than 4, meaning there was no excessive multicollinearity reported (30). We theorize that individual, interpersonal, and region-level factors predict changes in the individual's PHQ-9 and GAD-7. Each dependent variable (i.e., PHQ-9 and GAD-7) was modeled as a continuously distributed variable. Multiple linear regression was conducted to investigate the association between socio-ecological factors and mental health outcomes (Table 2). All socio-ecological factors were included simultaneously in adjusted models. Additionally, to investigate the differences in particular populations such as income, gender, and lifespan age, subgroup analyses were conducted (Tables 1–5, respectively). All statistical analyses were conducted in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). We considered a p-value of less than 0.05 to be statistically significant.
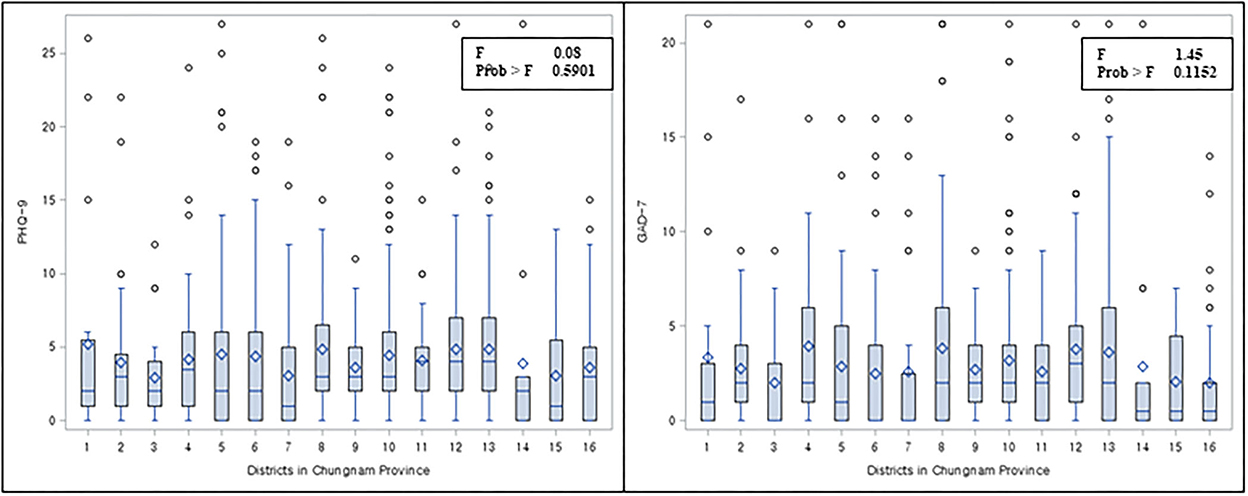
Figure 1. Distribution of PHQ-9 and GAD-7 by regional-level districts.
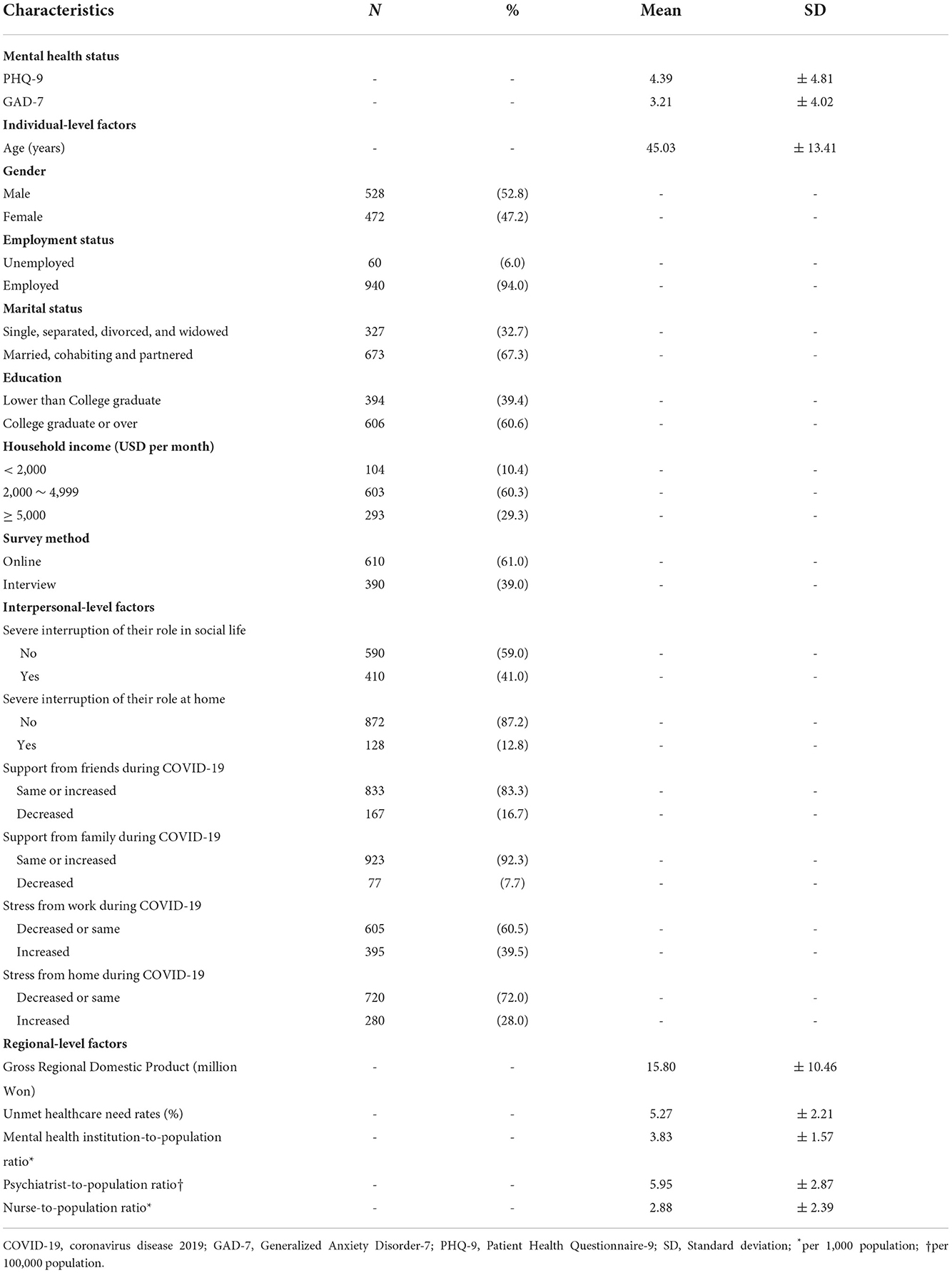
Table 1. Descriptive statistics of all variables in the analysis (N = 1,000).
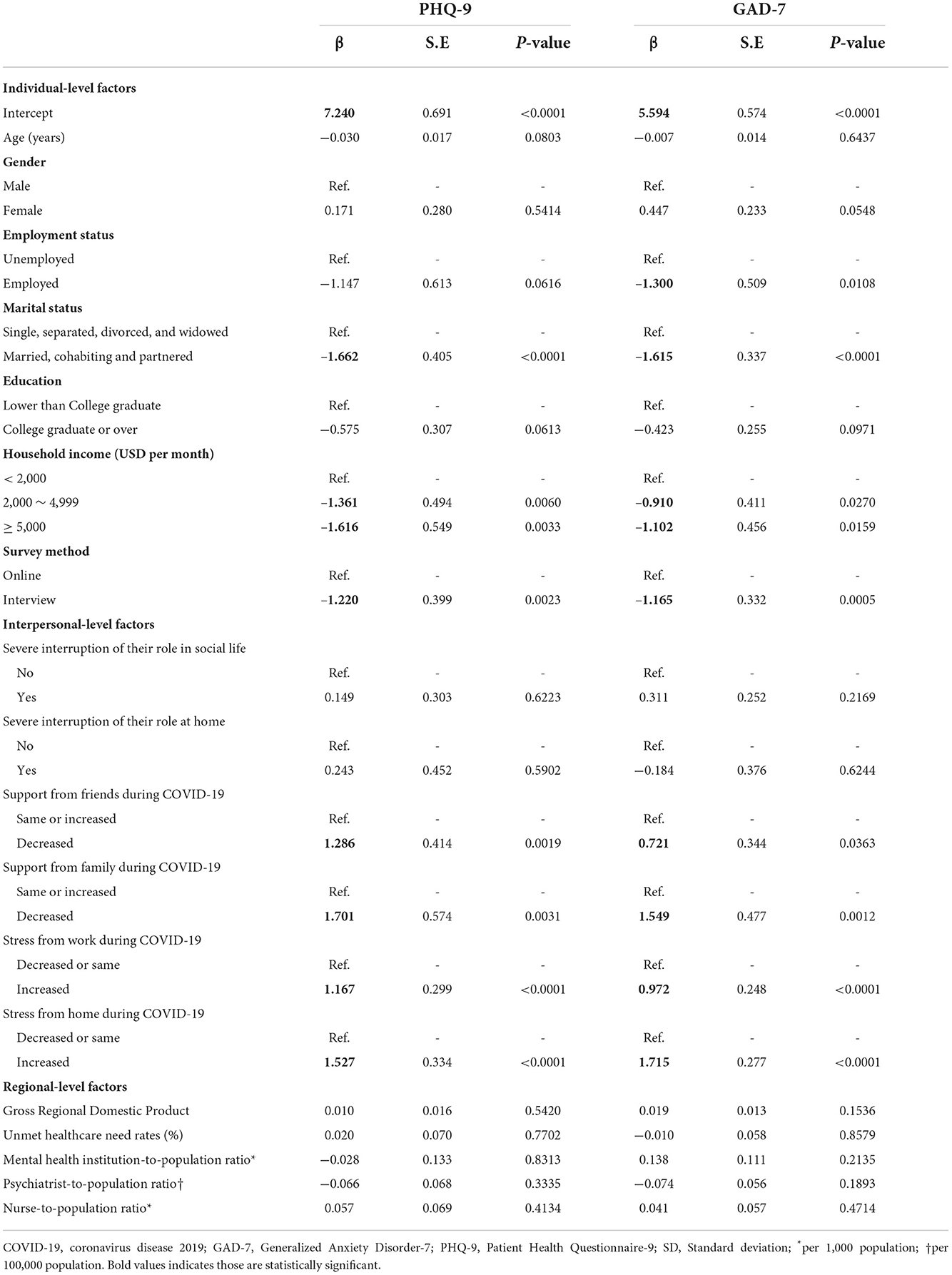
Table 2. Multiple linear regression for the effect of individual and community factors on individual's mental health status.
The demographic characteristics of the study participants are provided in Table 1. The average age of the study participants was 45.03 years. Among 1,000 participants, 47.2% of them were women, 94% were employed, and 97% were college graduates. During COVID-19, 16.7% of the participants reported a decrease in support from friends, and 7.7% reported a decrease in family support. In addition, 39.5 and 28% of the participants reported that their stress from work and home increased, respectively. For regional-level variables, the average mental health institution-to-population ratio was 3.83 per 1,000 population, the psychiatrist-to-population ratio was 5.95 per 100,000 population, and the nurse-to-population ratio was 2.88 per 1,000 population. The mean of PHQ-9 and GAD-7 scores were 4.39 and 3.21, indicating a low level of depressive and anxiety symptoms, respectively. Each score distribution by each district is presented as a boxplot in Figure 1. No significant differences were identified between the districts (PHQ: F = 0.88, p = 0.5901; GAD-7: F = 1.45, p = 0.1152).
The result of the adjusted multiple linear regression analysis is presented in Table 2. The intercept of PHQ-9 and GAD-7 was 7.240 and 5.594, respectively. Among individual factors, those who were married, had an income over 2,000 USD, and who completed the survey face-to-face reported less depressive symptoms (PHQ-9) and anxiety (GAD-7). Participants who were employed showed fewer anxiety symptoms, but there was no statistically significant association reported with depressive symptoms. In addition, participants who reported a decrease in family and friend support and an increase in stress from work and home during COVID-19 reported higher depressive and anxiety symptoms. However, there was no statistically significant association shown between regional-level factors and both PHQ-9 and GAD-7 scores (Table 2).
Table 3 shows the subgroup analysis by lifespan age group. In the age group between 20 and 45, the association with PHQ-9, two individual factors, and three interpersonal factors were statistically significant, showing a similar trend. Two major factors, namely marital status and decreased support from friends, showed a bigger effect size. The association with GAD-7, two individual factors, and three interpersonal factors were statistically significant and showed a similar trend. Female participants reported more anxiety, which differed from the results of multiple linear regression. In the age group over 45, the association with PHQ-9, four individual factors, five interpersonal factors, and one regional-level factor were statistically significant. In the same age group, GAD-7 also showed similar significant associations except for four regional-level factors, including GRDP and healthcare utilization factors, which showed statistical significance. GRDP, the mental health institution-to-population ratio, and the nurse-to-population ratio showed a positive association, while the psychiatrists-to-population ratio showed a negative association.
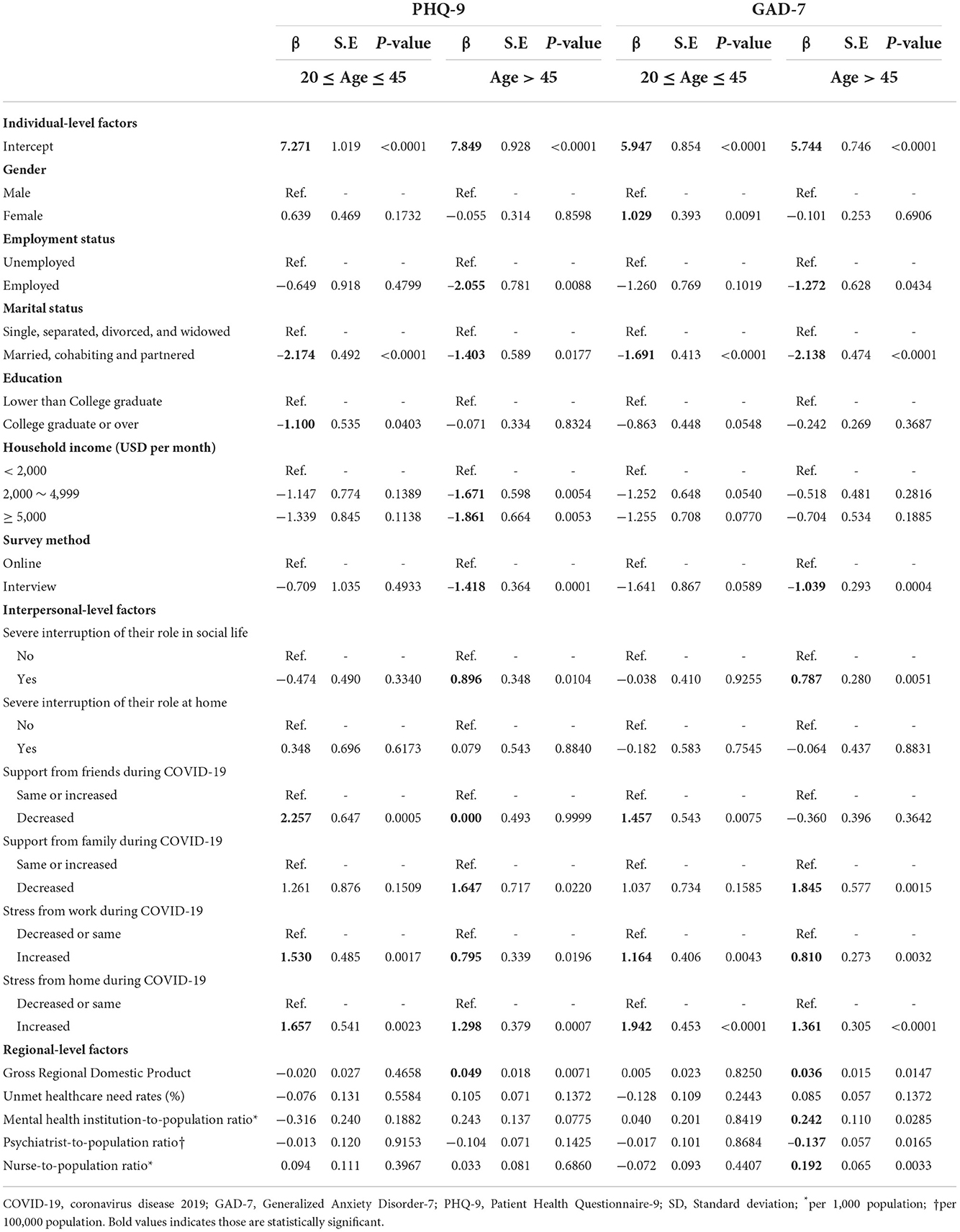
Table 3. Subgroup analysis of multiple linear regression for the effect of individual and community factors on mental health status by lifespan age group.
From Table 4, among the men, marital status, support from friends or family, and stress gained from home during COVID-19 were the main factors with a high impact on PHQ-9 and GAD-7. On the contrary, among the women, monthly household income and stress from home during COVID-19 showed significant associations with PHQ-9 and GAD-7. However, none of the regional-level factors showed a statistically significant association.
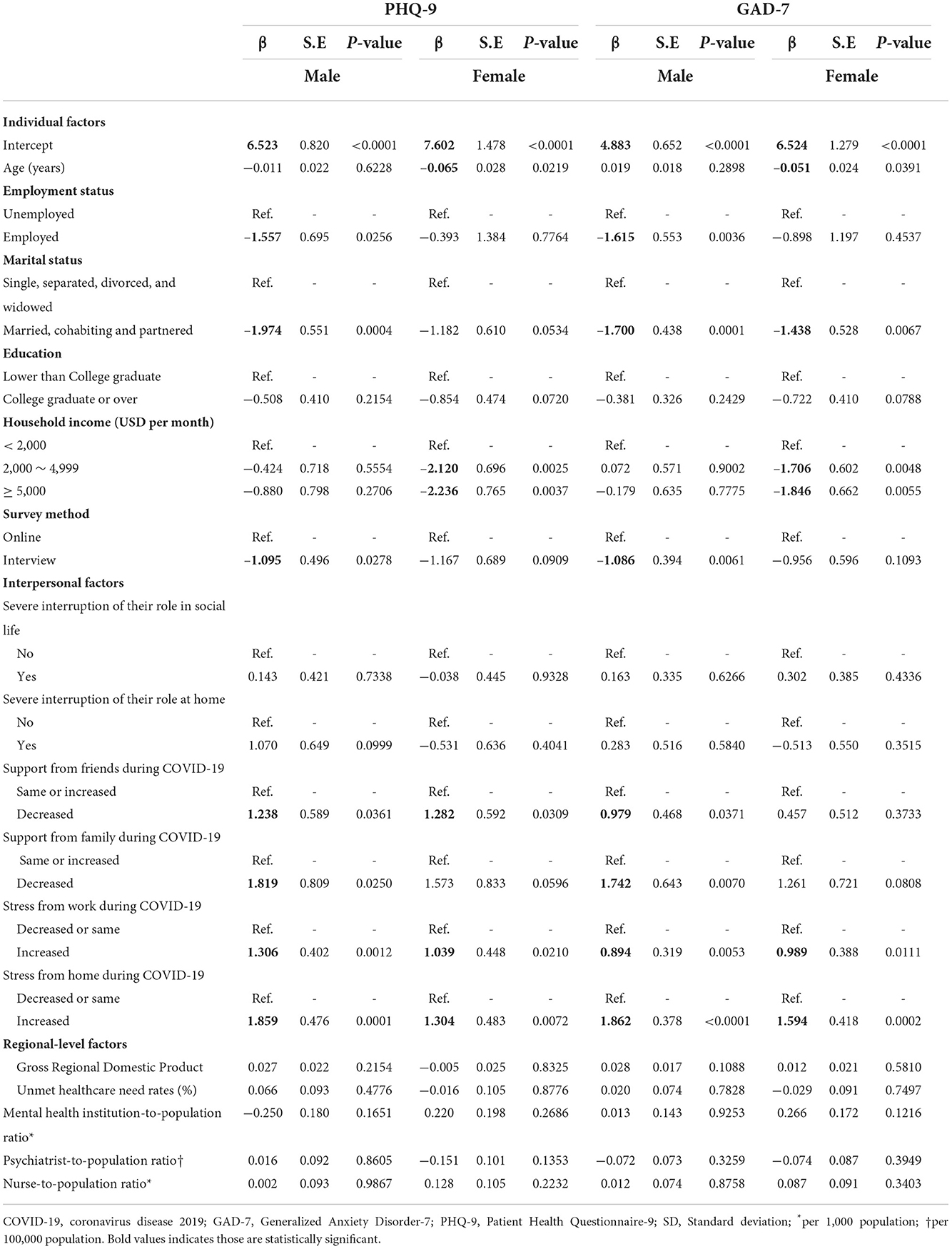
Table 4. Subgroup analysis of multiple linear regression for the effect of individual and community factors on mental health status by gender.
Finally, Table 5 shows subgroup analysis by monthly household incomes. Among the participants with incomes less than USD 2,000, decreased support from friends, and increased stress from home were significant factors of depressive symptoms (PHQ-9). On the other hand, individual characteristics such as marital and education statuses contributed to lowering anxiety levels (GAD-7). Finally, participants with more mental health resources in the region (i.e., the mental health institution-to-population ratio) reported fewer depressive symptoms and anxiety. The income of USD 2,000–4,999, employment status, survey method, decreased family support during COVID-19, and increased stress from work and home were statistically significant factors of PHQ-9 and GAD-7 among the groups. Factors particularly related to family or home were found to be significant among the participants with a household income of over USD 5,000.
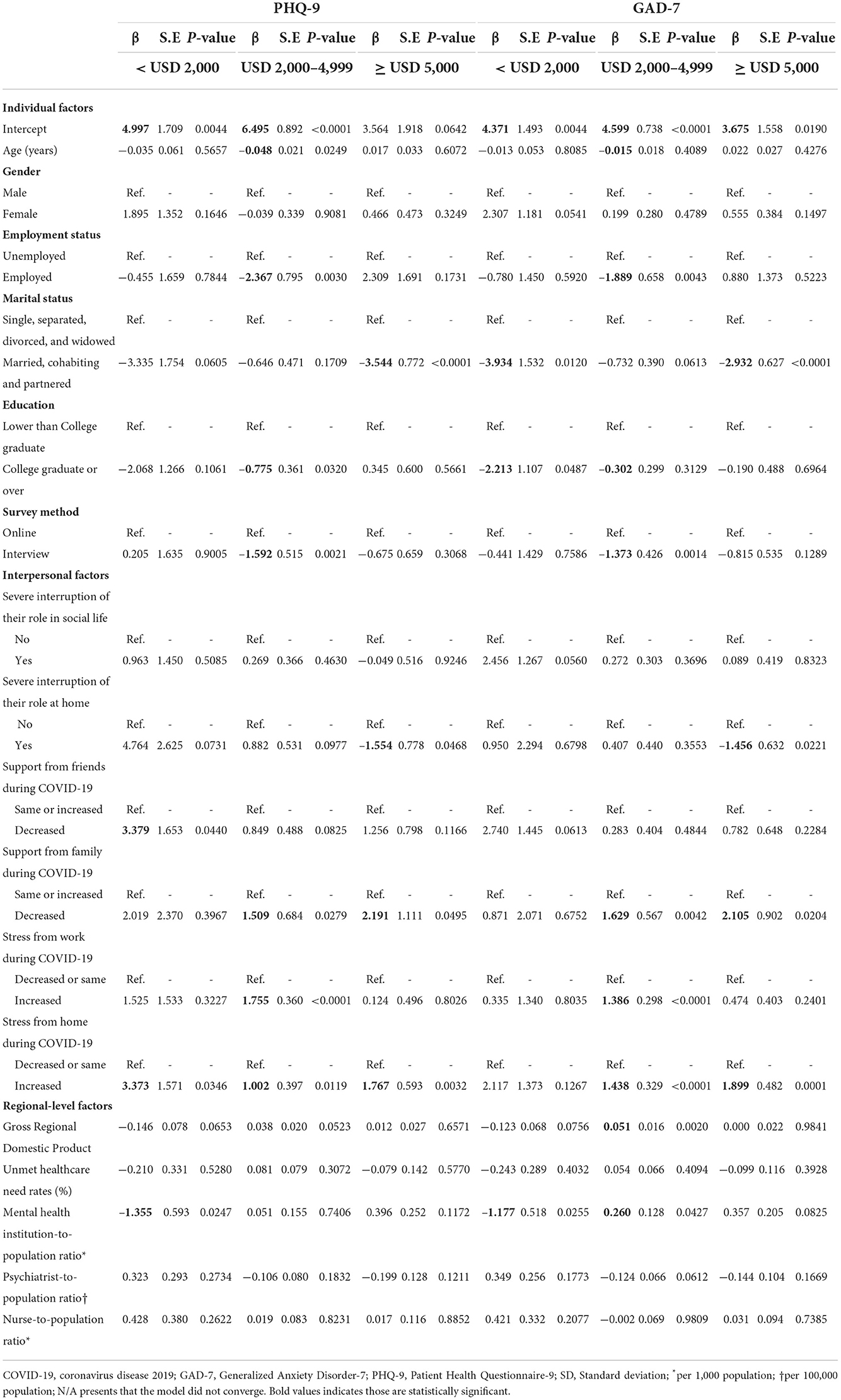
Table 5. Subgroup analysis of multiple linear regression for the effect of individual and community factors on mental health status by monthly household income.
This study aimed to examine the effects of individual, interpersonal, and regional factors at different socio-ecological levels on individuals' mental health status. The mean score of the depression level was 4.29, and the anxiety level was 3.29, indicating, in general, a very mild level of depression and anxiety (31). The average score of PHQ-9 in this study was reported higher compared to the reported results from previous studies (32), and the mean score of GAD-7 was also slightly higher compared to individuals with no mental disorder (28). With all the factors controlled, the intercept of predicted PHQ-9 and GAD-7 were mild-to-moderate levels of depression and anxiety. This difference might be attributable to the unique era of the pandemic and the situation of national-level lockdown and downsizing due to the COVID-19 case burden as compared to another era.
In addition to government measures, South Korea may have been able to effectively regulate COVID-19 because of public support. The current study found that factors at each level of the social-ecological model predicted the individual's depressive and anxiety symptoms during the pandemic in South Korea, confirming previous findings about the applicability of the social-ecological model to various issues (22, 33, 34). Our study results suggest that different efforts in multiple factors are needed to promote the management of mental health, in general. Moreover, although regional factors were identified as non-significant factors in general, for particular groups, such as groups by age and household income, regional factors, including GRDP and healthcare utilization variables, were revealed as significant factors. The factors significantly associated with anticipating the individual's mental health outcomes across the three levels were common in terms of support.
In this study, among intrapersonal factors, four of them were shown as significant factors in the associations with mental health outcomes throughout the analyses. Specifically, compared to the pre-pandemic era, the participants receiving less support from their family or friends or more stress from their workplace or home showed significant prediction with increased PHQ-9 and GAD-7 scores, which reflect a more severe level of depression and anxiety. Social bonds and supportive interactions with others are important for mental health; also, social support can buffer one from the negative consequences of stress (18). In addition, this study revealed the fact that among social support, family or home-related factors (i.e., marital status, support from family, and stress from home) have greater impacts on the individuals' depression and anxiety levels. These features were especially highlighted in several certain groups, including groups over 45 years old, or men, or with household incomes less than USD 2,000 or more than USD 5,000, whereas participants under 45 or with a household income less than USD 2,000 showed that support from friends was a significant factor.
An economic perspective can also be considered as one kind of social support, specifically material support. In general, participants with higher income levels showed lower levels of depressive and anxiety symptoms. Additionally, participants over 45 showed better depressive and anxiety levels in case of a secured financial status (i.e., employed or higher household income) (35–37). Among the women, household income status seemed to be the most significant predictor for their depressive and anxiety levels, whereas, among men, active support factors were significant. This finding may reflect cultural norms present in South Korea. In South Korea, wives are the main decision makers in the household and, therefore, may have been more affected by financial issues (38). In the subgroup analyses of the household incomes, each group highlighted different factors associated with the mental health outcomes of each group member. For example, the high-impact factors on mental health outcomes in low-income groups were related to financial support sources, whereas in middle-income groups, they were related to the security of the income sources (i.e., job status), and in high-income groups, they were associated with the family relationship. Based on the result interpretation of this study, active support has the main overall effect. However, the effect size may differ depending on the individual's income status since the material supports that affect the individuals' livelihood are different. Therefore, the support policy that considers people's SES is different, and its implementation is a matter to be considered.
Some subgroup analyses showed significant regional factors associated with mental health outcomes; however, those results were mixed. To understand the positive associations of regional factors with mental health status, we conducted an additional correlation analysis between socio-ecological factors and population as a proxy of urbanness and mental health outcomes (Supplementary Figure 1). The correlation result showed that population and mental health outcomes were associated with a higher GRDP and a higher ratio of healthcare personnel to the population. Among participants aged over 45, both PHQ-9 and GAD-7 showed positive associations with GRDP. GRDP measures the economic performance of a region which is an indicator of macro-economic performance in the local economy (39). Moreover, higher GRDP is most likely to be observed in metropolitan areas with large populations (39). In a previous study, participants living in metropolitan areas had lower perceived social support than those in rural areas (40). This is likely to be interpreted as urban communities tend to be more isolating or individualistic. The culture of familism may have decreased more in urban populations than in rural populations, as South Korea rapidly industrializes as a developing nation (40).
Among regional factors, healthcare utilization factors were the ones that showed mixed results; in other words, both positive and negative associations were shown. Specifically, those with a household income of less than 2,000 USD lived in areas with lower healthcare to an institution-to-population ratio and reported higher scores on the PHQ-9 and GAD-7. In South Korea, mental health promotion programs are planned and implemented in “Si,” “Gun,” and “Gu” to manage community mental health levels via community primary mental health clinics. Those programs are mandatory projects conducted in the clinics. According to our study, low household-income individuals are likely to benefit from resources such as greater numbers of mental health institutions provided in their community. Thus, a large supply of local mental health institutions can help provide mental illness prevention services and distribute and apply them prophylactically among low-income individuals (41). On the other hand, the psychiatrist-to-population ratio or nurse-to-population ratio was positively associated with mental health outcomes among participants aged over 45 and household income between 2,000 and 4,999. From the result of the correlation analysis, the psychiatrist-to-population ratio, nurse-to-population ratio, and household income showed positive correlations with the population. Considering those results, the beta coefficients showed in multiple regression analyses may reflect the characteristics of large populations.
This study is the first that examined the association of individual-, interpersonal-, and regional-level factors on the individuals' mental health outcomes in the general Korean population during the COVID-19 pandemic with the perspective of a socio-ecological model. There are some limitations that should be noted. First, this is a representative sample of one region, but not of the entire country or analyzing other regional differences, which threatens generalizability. Second, the main focus of this survey is on the individual and interpersonal factors impacting mental health status; however, the regional-level variables have not been developed with the purpose of the study in mind. Thus, we may omit key community factors with a significant impact on the individuals' depressive symptom management, including satisfaction with community mental health management programs. Third, the study measured mental symptoms using self-reported questionnaires rather than making clinical diagnoses. There may have also been response bias, with nervous individuals stressed by the epidemic and more inclined to engage in the survey. To minimize the response bias, the study survey was designed by a professional survey company with a psychiatrist consultant, and the interview was conducted by trained personnel, to avoid the leading questions. Fourth, since the survey's primary objective was to examine the general depressive mood and anxiety symptoms experienced by the community's residents as a result of COVID-19 during the pandemic, it is vital to evaluate for any pre-existing conditions that might have an impact on mental health or account for them in the analysis. However, the survey was more focused on environmental factors or general sociodemographic factors. The authors strongly suggest that in the next term of the survey, they should collect related pre-conditions that may influence mental health. Finally, due to the different survey methods, participants may have responded differently. There may be a possible social desirability bias (42). Social desirability bias is one of the response biases, the tendency of respondents to answer questions in a way that will be deemed positive by others. It is particularly observed in the questions that require socially desirable responses, which include personality, sexual behavior, and drug usage (42). To reduce the effect of bias, we confounded the survey method as a variable and conducted subgroup analysis by survey method to investigate different tendencies with beta coefficients that were not shown (Supplementary Table 1).
Despite these limitations, our findings have implications for psychological therapies aiming at lowering psychological distress and enhancing mental health and psychological resilience in the face of public health crises. To give evidence-based recommendations on responding to future pandemics in Korea, population-based research considering complex relations of the individual-, interpersonal-, and regional-level factors on mental health and COVID-19 should be established.
In summary, we conducted a cross-sectional survey study to investigate socio-ecological factors associated with mental health outcomes, PHQ-9 and GAD-7, among 1,000 individuals during the COVID-19 pandemic in South Korea. From the adjusted multiple linear regression model, the study result revealed that the only different significant factor of PHQ-9 and GAD-7 was an individual-level factor which is employment status. Other than the employment status factor, three individual factors (i.e., marital status, monthly household income, and survey method) and four interpersonal factors (i.e., support from friends and family, stress from work and home) had significant associations, but no mental outcomes had significant associations with regional factors. All those factors are related to the economic status and support system of the individual and community. However, as shown in the previous study, individual and interpersonal factors were more adapted to explain the individuals' depressive and anxiety symptoms management during the COVID-19 pandemic than upper-level factors, suggesting the need for additional policies targeting these lower levels (22).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Institutional Review Board of Dankook University (DKU 2021-05-038). The patients/participants provided their written informed consent to participate in this study.
SL has made substantial contributions to the conception, design of the work, interpretation of data, drafted the work, substantively revised it, final approval of the version to be published, and agreed to be accountable for the integrity of any part of the work are appropriately investigated and resolved. JL has made substantial contributions to the acquisition and interpretation of data for the work, revising it critically for important intellectual content, final approval of the version to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy. HL has made substantial contributions to the design of the work, the acquisition, analysis, and interpretation of data, substantively revised the work, final approval of the version to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy and integrity of any part of the work are appropriately investigated and resolved. All authors have approved the submitted version and have agreed to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
The authors wish to acknowledge the financial support of the Catholic Medical Center Research Foundation made in the program year of 2022 (Grant number: 5-2022-B0001-00207).
The authors gratefully acknowledge the assistance of professor Eileen Collins, Ph.D., RN, FAAN, ATSF of the University of Illinois at Chicago (UIC) and academic specialist Bahar Baniasad MA of UIC Academic Center for Excellence with the check and edit of the English in this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1024751/full#supplementary-material
1. Pfefferbaum B, Schonfeld D, Flynn BW, Norwood AE, Dodgen D, Kaul RE, et al. The H1N1 crisis: a case study of the integration of mental and behavioral health in public health crises. Disaster Med Public Health Prep. (2012) 6:67–71. doi: 10.1001/dmp.2012.2
2. Douglas PK, Douglas DB, Harrigan DC, Douglas KM. Preparing for pandemic influenza and its aftermath: mental health issues considered. Int J Emerg Ment Health. (2009) 11:137.
3. Wang C, Tee M, Roy AE, Fardin MA, Srichokchatchawan W, Habib HA, et al. The impact of COVID-19 pandemic on physical and mental health of Asians: a study of seven middle-income countries in Asia. PLoS ONE. (2021) 16:e0246824. doi: 10.1371/journal.pone.0246824
4. Wang C, Tripp C, Sears SF, Xu L, Tan Y, Zhou D, et al. The impact of the COVID-19 pandemic on physical and mental health in the two largest economies in the world: a comparison between the United States and China. J Behav Med. (2021) 44:741–759. doi: 10.1007/s10865-021-00237-7
5. Sassone B, Mandini S, Grazzi G, Mazzoni G, Myers J, Pasanisi G. Impact of COVID-19 pandemic on physical activity in patients with implantable cardioverter-defibrillators. J Cardiopulm Rehabil Prev. (2020) 40:285. doi: 10.1097/HCR.0000000000000539
6. Alonzi S, La Torre A, Silverstein MW. The psychological impact of preexisting mental and physical health conditions during the COVID-19 pandemic. Psychol Trauma. (2020) 12:S236. doi: 10.1037/tra0000840
7. Sade S, Sheiner E, Wainstock T, Hermon N, Yaniv Salem S, Kosef T, et al. Risk for depressive symptoms among hospitalized women in high-risk pregnancy units during the COVID-19 pandemic. J Clin Med. (2020) 9:2449. doi: 10.3390/jcm9082449
8. Patabendige M, Gamage MM, Weerasinghe M, Jayawardane A. Psychological impact of the COVID-19 pandemic among pregnant women in Sri Lanka. Int J Gynaecol Obstetr. (2020) 151:150. doi: 10.1002/ijgo.13335
9. Durankuş F, Aksu E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: a preliminary study. J Mater Fetal Neonatal Med. (2022) 35:205–11. doi: 10.1080/14767058.2020.1763946
10. Thayer ZM, Gildner TE. COVID-19-related financial stress associated with higher likelihood of depression among pregnant women living in the United States. Am J Hum Biol. (2021) 33:e23508. doi: 10.1002/ajhb.23508
11. Silverman ME, Medeiros C, Burgos L. Early pregnancy mood before and during COVID-19 community restrictions among women of low socioeconomic status in New York City: a preliminary study. Arch Womens Mental Health. (2020) 23:779–782. doi: 10.1007/s00737-020-01061-9
12. Li W, Yang Y, Liu Z-H, Zhao Y-J, Zhang Q, Zhang L, et al. Progression of mental health services during the COVID-19 outbreak in China. Int J Biol Sci. (2020) 16:1732. doi: 10.7150/ijbs.45120
13. Kearney A, Hamel L, Brodie M. Mental Health Impact of the COVID-19 Pandemic: An Update. San Franciso, CA: Kaiser Family Foundation (2021).
14. Kim Y, Kwon H-Y, Lee S, Kim C-B. Depression during COVID-19 quarantine in South Korea: a propensity score-matched analysis. Front Public Health. (2021) 9:743625. doi: 10.3389/fpubh.2021.743625
15. Lee H, Choi D, Lee JJ. Depression, anxiety, and stress in Korean general population during the COVID-19 pandemic. Epidemiol Health. (2022) 44:e2022018. doi: 10.4178/epih.e2022018
16. Yao H, Chen J-H, Xu Y-F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry. (2020) 7:e21. doi: 10.1016/S2215-0366(20)30090-0
17. Canet-Juric L, Andrés ML, Del Valle M, López-Morales H, Poó F, Galli JI, et al. A longitudinal study on the emotional impact cause by the COVID-19 pandemic quarantine on general population. Front Psychol. (2020) 2431:565688. doi: 10.3389/fpsyg.2020.565688
18. Turner RJ, Brown RL. Social support and mental health. In:Scheid T, Brown T, , editors. A Handbook for the Study of Mental Health: Social Contexts, Theories, and Systems. Cambridge: Cambridge University Press (2010). p. 200–12.
19. Cobb S. Social support and health through life course. In:Riley MW, , editor. Aging From Birth to Death Interdisciplinary Perspective. Washington, DC: American Association for the Advancement of Science (1979). p. 93–106.
20. Lee JH, Lee H, Kim JE, Moon SJ, Nam EW. Analysis of personal and national factors that influence depression in individuals during the COVID-19 pandemic: a web-based cross-sectional survey. Global Health. (2021) 17:1–12. doi: 10.1186/s12992-020-00650-8
21. Ruiz-Pérez I, Bermúdez-Tamayo C, Rodríguez-Barranco M. Socio-economic factors linked with mental health during the recession: a multilevel analysis. Int J Equity Health. (2017) 16:1–8. doi: 10.1186/s12939-017-0518-x
22. Hennein R, Mew EJ, Lowe SR. Socio-ecological predictors of mental health outcomes among healthcare workers during the COVID-19 pandemic in the United States. PLoS ONE. (2021) 16:e0246602. doi: 10.1371/journal.pone.0246602
23. Jang SH. Social-ecological factors related to preventive behaviors during the COVID-19 pandemic in South Korea. PLoS ONE. (2022) 17:e0266264. doi: 10.1371/journal.pone.0266264
24. Shin C, Ko Y-H, An H, Yoon H-K, Han C. Normative data and psychometric properties of the Patient Health Questionnaire-9 in a nationally representative Korean population. BMC Psychiatry. (2020) 20:1–10. doi: 10.1186/s12888-020-02613-0
25. McMillan D, Gilbody S, Richards D. Defining successful treatment outcome in depression using the PHQ-9: a comparison of methods. J Affect Disord. (2010) 127:122–9. doi: 10.1016/j.jad.2010.04.030
26. Cassin S, Sockalingam S, Hawa R, Wnuk S, Royal S, Taube-Schiff M, et al. Psychometric properties of the Patient Health Questionnaire (PHQ-9) as a depression screening tool for bariatric surgery candidates. Psychosomatics. (2013) 54:352–8. doi: 10.1016/j.psym.2012.08.010
27. Ko M, Cho HM, Park J, Chi S, Han C, Yi HS, et al. Impact of the coronavirus disease pandemic on mental health among local residents in Korea: a cross sectional study. J Korean Med Sci. (2021) 36:e322. doi: 10.3346/jkms.2021.36.e322
28. Ahn J-K, Kim Y, Choi K-H. The psychometric properties and clinical utility of the Korean version of GAD-7 and GAD-2. Front Psychiatry. (2019) 10:127. doi: 10.3389/fpsyt.2019.00127
29. Sandman L, Hofmann B. Why we don't need “Unmet Needs”! on the concepts of unmet need and severity in health-care priority setting. Health Care Anal. (2019) 27:26–44. doi: 10.1007/s10728-018-0361-2
30. O'brien RM. A caution regarding rules of thumb for variance inflation factors. Qual Quant. (2007) 41:673–90. doi: 10.1007/s11135-006-9018-6
31. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
32. Kim SY, Yoo DM, Min C, Choi HG. Assessment of the difference in depressive symptoms of the Korean adult population before and during the COVID-19 pandemic using a community health survey. J Affect Disord. (2022) 300:130–6. doi: 10.1016/j.jad.2021.12.107
33. Dryhurst S, Schneider CR, Kerr J, Freeman AL, Recchia G, Van Der Bles AM, et al. Risk perceptions of COVID-19 around the world. J Risk Res. (2020) 23:994–1006. doi: 10.1080/13669877.2020.1758193
34. Capraro V, Barcelo H. The effect of messaging and gender on intentions to wear a face covering to slow down COVID-19 transmission. arXiv preprint arXiv:200505467. (2020) doi: 10.31234/osf.io/tg7vz
35. Samuelsson G, McCamish-Svensson C, Hagberg B, Sundström G, Dehlin O. Incidence and risk factors for depression and anxiety disorders: results from a 34-year longitudinal Swedish cohort study. Aging Ment Health. (2005) 9:571–5. doi: 10.1080/13607860500193591
36. Yaka E, Keskinoglu P, Ucku R, Yener GG, Tunca Z. Prevalence and risk factors of depression among community dwelling elderly. Arch Gerontol Geriatr. (2014) 59:150–4. doi: 10.1016/j.archger.2014.03.014
37. MacEwen KE, Barling J, Kelloway EK, Higginbottom SF. Predicting retirement anxiety: the roles of parental socialization and personal planning. J Soc Psychol. (1995) 135:203–13. doi: 10.1080/00224545.1995.9711424
38. Lee KJ, Um CC, Kim S. Multiple roles of married Korean women: effect on depression. Sex Roles. (2004) 51:469–78. doi: 10.1023/B:SERS.0000049235.60839.ef
39. Feriyanto N. Determinant of gross regional domestic product (GRDP) in Yogyakarta special province. Econ J Emerg Mark. (2014) 2014:131–40. doi: 10.20885/ejem.vol6.iss2.art6
40. Eom CS, Shin DW, Kim SY, Yang HK, Jo HS, Kweon SS, et al. Impact of perceived social support on the mental health and health-related quality of life in cancer patients: results from a nationwide, multicenter survey in South Korea. Psychooncol. (2013) 22:1283–90. doi: 10.1002/pon.3133
41. Fleury M-J, Ngamini Ngui A, Bamvita J-M, Grenier G, Caron J. Predictors of healthcare service utilization for mental health reasons. Int J Environ Res Public Health. (2014) 11:10559–86. doi: 10.3390/ijerph111010559
Keywords: COVID-19, pandemics, depression, anxiety, GAD-7 scale, PHQ-9, socio-ecological model of health, support system
Citation: Lee SY, Lee JJ and Lee H (2022) Socio-economic factors associated with mental health outcomes during the COVID-19 pandemic in South Korea. Front. Public Health 10:1024751. doi: 10.3389/fpubh.2022.1024751
Received: 22 August 2022; Accepted: 10 November 2022;
Published: 13 December 2022.
Edited by:
Samer El Hayek, Erada Center for Treatment and Rehab, United Arab EmiratesReviewed by:
Miguel Vasconcelos Da Silva, King's College London, United KingdomCopyright © 2022 Lee, Lee and Lee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hooyeon Lee, aHlsZWVAY2F0aG9saWMuYWMua3I=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.