 Hye-Kyung Oh
Hye-Kyung Oh Cheol Yeung Jang
Cheol Yeung Jang Mi Suk Ko
Mi Suk Ko
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 09 December 2022
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1024284
Objectives: This study aims to identify critical incident trauma (CIT), social support, resilience, and post-traumatic stress disorder (PTSD) in Korean police officers and to determine factors related to PTSD to obtain basic data for developing a PTSD intervention.
Methods: A mixed-methods approach was adopted by administering structured questionnaires to Korean police officers and conducting semi-structured interviews with seven Korean police stakeholders. The structured questionnaires elicited information on CIT, social support, resilience, and PTSD. Data from 189 participants were analyzed using independent t-tests, Pearson's correlation coefficients, and multiple linear regression analysis. The interview data, which elicited information on difficulties and coping strategies after CIT, police organizational culture, current status of counseling programs, and suggestions for PTSD interventions, were analyzed using an inductive thematic analysis.
Results: Factors that are significantly related to PTSD (28.7% of variance) are very healthy subjective health status (B = −0.44, p = 0.013), CIT (B = 0.18, p ≤ 0.001), social support (B = −0.38, p ≤ 0.001), and resilience (B = −0.18, p = 0.044). The stakeholders revealed the following PTSD-related factors: the difficulties and limitations of overcoming traumatic experiences, coping strategies, police counseling program status, and opinions on PTSD-related programs.
Conclusion: Perceived health status, CIT, social support, and resilience had a strong relationship with PTSD. Therefore, the success of PTSD interventions for Korean police officers should be considered.
Police service is a risky and stressful occupation that involves frequent exposure to confrontation and violence, which are potentially harmful and can be a source of traumatic experiences for police personnel. Exposure to traumatic experiences can lead to various mental health complications, including post-traumatic stress disorder (PTSD) (1). Trauma may occur as a result of life-threatening events, such as car accidents, interpersonal violence, and manmade and natural disasters (2). Police officers are more often exposed to these situations than other occupational groups.
In a traumatic incident, a critical incident trauma (CIT) is any traumatic situation in which the service personnel experience unusually strong emotional reactions that interfere with their ability to exert control over the situation. It occurs when police officers face a crisis in the work environment that produces either immediate or delayed stress (3). Previous studies revealed that CIT plays an important role in the development of PTSD in police officers (1, 4). Currently, the suicide rate of police officers is approximately 20 deaths per 100,000 persons, which is approximately three times the suicide rate of public officials in South Korea (5, 6). Police officers face many challenges that affect their mental health, which may affect the important role they play in public policing; therefore, it is important to identify factors that influence police officers' PTSD.
One of the factors that may influence PTSD among police officers is social support. Social support is a multidimensional construct and refers to the various resources provided through interpersonal relationships (7). Even in high-risk situations, if appropriate social support is obtained, PTSD can be prevented and reduced among veterans and military service members (8). Among police officers, a lack of social support increases a sense of isolation and has been found to be correlated with a higher level of stress (3) and PTSD (9–11).
Similar to social support, resilience is a complex construct that encapsulates the process and outcomes of successful adaptation to difficult or adverse life events (12, 13). Resilience is a significant predictor of PTSD symptoms among paramedics (14). As for police officers, some foreign studies have shown that resilience significantly decreased PTSD symptoms (2, 10).
Several studies have identified the current status of PTSD and systemic coping strategies (9, 15), the relationships between CIT and PTSD (16), and resilience and PTSD (17) in police officers. However, in South Korea, few studies have been conducted on the factors affecting PTSD among police officers. In this study, we identified the factors that influence PTSD among police officers using questionnaires and interviews to develop a PTSD intervention for police officers in South Korea.
This study adopted a mixed-methods approach to identify the influencing factors of PTSD in police officers in South Korea. The quantitative design involved administering structured questionnaires to police officers, while the qualitative design involved conducting semi-structured video interviews with seven stakeholders (five police officers, one clinical psychologist, and one professor of police administration).
The participants were police officers who expressed a desire to voluntarily participate in the study. They were recruited using convenience sampling. Questionnaire surveys were conducted online from May to June 2022. For the quantitative part, the sample size was calculated using G*power 3.1.9.4, with a significant level of 0.05, medium effect size of 0.15, power of 0.95, and 13 independent variables. The minimum sample size was 189. After completing the questionnaire, the final sample size was 189. For the qualitative part, three nursing professors and two police officers prepared a list of relevant stakeholders through meetings. Semi-structured interviews were conducted from May to July 2022 using a video conferencing program.
This study was conducted after obtaining approval from the institutional review board (Approval no: 1040621-202111-HR-066) of Daegu University in Korea. We explained the purpose, methods, and procedure of the study; the confidentiality and anonymity of the data; and the possibility of withdrawing participation at any time for any reason. Written informed consent to participate in the study was obtained online.
Ten items on participants' characteristics (sex, age, education level, religion, affiliated working department, workplace, rank, work, field experience, and subjective health status) were constructed by the researchers based on previous studies. The Life Event Checklist for Diagnostic and Statistical Manual of Mental Disorder-5 (DSM-5) by the American National Center for PTSD was used to assess participants' CIT (18). The checklist assesses exposure to 17 events known to potentially result in PTSD or distress; however, we excluded 2 inappropriate questions such as those related to combat or exposure to a war zone in the military or as a civilian and severe human suffering. These ambiguous items were excluded because our study's participants were not military soldiers. The scoring was also modified from the existing 1–6 scale to a 1–5 scale (ranging from “doesn't apply” to “happened to me”). Because the survey was completed by police officers, the scale “Part of my job” was excluded. Social support was measured using the Korean version of the Interpersonal Support Evaluation list-12 (ISEL-12) (19). This scale comprises 12 questions, with each question rated on a 4-point Likert scale (ranging from “absolutely not true” to “absolutely true”). Resilience was measured using the resilience research center's adult resilience measure (RRC-ARM) developed by Liebenberg and Moore (20). It consists of eight elements (social/community inclusion, family attachment and support, spirituality, national and cultural identity, and personal competencies) and 28 items. Each question has a 5-point Likert scale ranging from 1 (“not at all”) to 5 (“extremely”). PTSD was assessed using the Korean version of the PTSD checklist-5 (PCL-5-K) developed by Kim et al. (21). It is a 20-item self-report measure that assesses the presence and severity of PTSD symptoms and corresponds with the Diagnostic and Statistical Manual of Mental Disorder-5 (DSM-5) criteria for PTSD. Severity was determined by adding the scores of each item to determine a total score (ranging from 0 to 80). A total score of 33 or higher suggests that the participants needed further assessment to confirm their diagnosis of PTSD. Each question uses a Likert scale ranging from 0 (“not at all”) to 4 (“extremely”).
All collected data were analyzed using SPSS Statistics 22.0 (IBM Corp., Armonk, MY, USA). We described participants' demographic characteristics, CIT, social support, resilience, and PTSD using real numbers, percentages, means, and standard deviations. Cronbach's α coefficient was used to verify the internal reliability of the measures. We analyzed the differences in the participants' CIT, social support, resilience, and PTSD according to their general characteristics using independent t-tests. Correlations among CIT, social support, resilience, and PTSD were analyzed using Pearson's correlation coefficients. Finally, factors that influence participants' PTSD were analyzed using multiple linear regression analyses. The dependent variable in these analyses was PTSD, and the independent variables were general characteristics, CIT, social support, and resilience. The interview data were analyzed using an inductive thematic analysis approach for thematic content analysis.
Table 1 presents the general characteristics of the 189 police officers who participated in this study. The majority are male (80.4%) and aged between 30 and 39 years (37.6%). Of the participants, 60.9% had completed a university degree, 19.0% had completed high school, 10.6% had completed a postgraduate degree, and 9.5% had completed a college degree. Approximately two-thirds of the participants are atheists. Additionally, approximately 21.7% of the police officers worked in the police precinct or police box, while 16.9, 11.1, 7.4, 7.4, 6.9, 6.3, 5.8, 4.8, 4.2, 2.7, and 2.1% worked in the investigation, detective, intelligence, women and juvenile affairs, police administration, community safety, public security, traffic division, emergency dispatching and operations command center, mobile police, and audit and inspection departments, respectively. As for rank, approximately half of the participants were assistant inspectors (22.2%) or inspectors (30.7%). Regarding work experience, the highest proportion (27.5%) had 5 to < 10 years of experience, while the smallest proportion (4.8%) had 25 to < 30 years of experience. As for the field experience of participants, the highest proportion (37.5%) had < 5 years, while the smallest proportion (5.3%) had over 25 years. Regarding subjective health status, the majority of participants perceived themselves to be generally healthy.
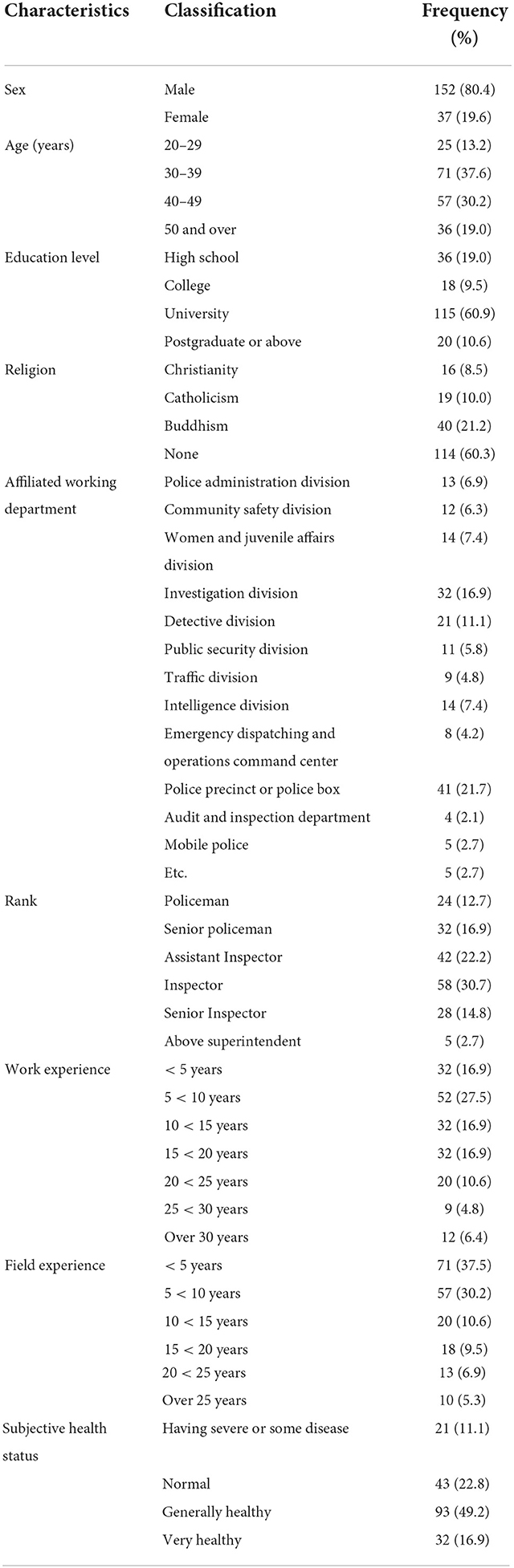
Table 1. Demographic characteristics of subjects (N = 189).
The mean scores with corresponding SDs were 2.34 ± 1.02 (out of 5), 2.97 ± 0.49 (out of 4), 3.58 ± 0.56 (out of 5), and 1.05 ± 0.65 (out of 4) for CIT, social support, resilience score, and PTSD, respectively (Table 2).

Table 2. Critical incident trauma, social support, resilience, and post-traumatic stress disorder.
As shown in Table 3, we found significant differences in CIT scores based on sex (t = 5.12, p = 0.025), work experience (F = 2.20, p = 0.045), field experience (F = 2.66, p = 0.024), and subjective health status (F = 2.86, p = 0.038). An ex-post analysis revealed no significant differences between the groups. We also found differences in social support based on age (F = 4.28, p = 0.006), rank (F = 3.06, p = 0.011), work experience (F = 2.54, p = 0.022), and subjective health status (F = 12.24, p ≤ 0.001). The results of an ex-post analysis revealed that participants aged 20 years had higher social support scores than those aged 50 years and over. Among the rank levels, the policeman group (the lowest rank in South Korea) had higher social support scores than the senior inspector group. Regarding subjective health status, participants with a very healthy status showed significantly higher social support scores than those with other health statuses. Participants with a normal health status had significantly lower social support scores than those with a generally healthy status.
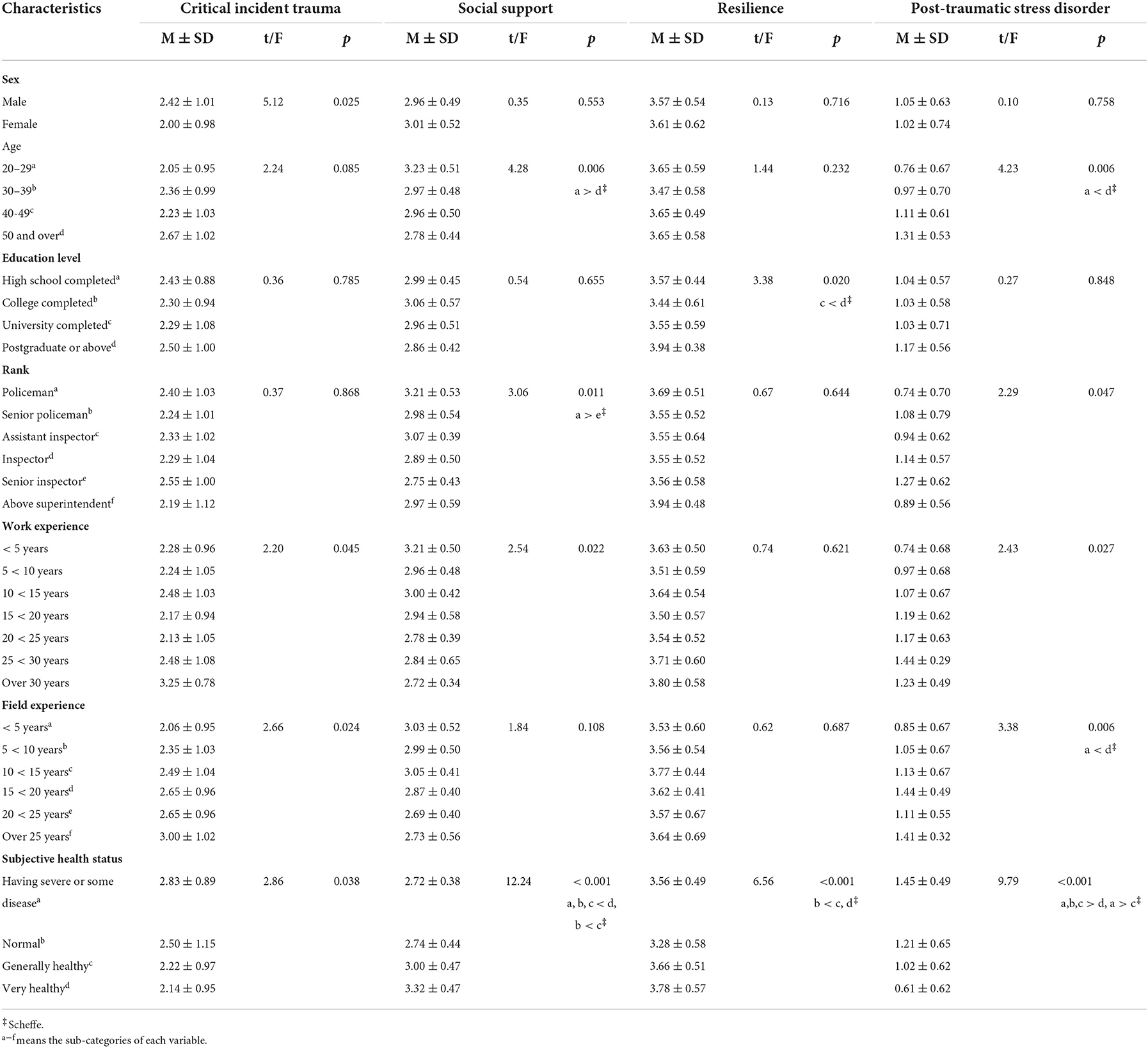
Table 3. Critical incident trauma, social support, resilience, and post-traumatic stress disorder according to general characteristics.
Resilience scores differed significantly across education levels (F = 3.38, p = 0.020) and subjective health status (F = 6.56, p < 0.001). An ex-post analysis revealed that, for education level, participants with a university degree had higher resilience scores than those with a postgraduate degree. In terms of subjective health status, participants with normal health status had lower resilience scores than those in the general and very healthy status groups. We also found differences in PTSD according to age (F = 4.23, p = 0.006), rank (F = 2.29, p = 0.047), work experience (F = 2.43, p = 0.027), field experience (F = 3.38, p = 0.006), and subjective health status (F = 9.79, p ≤ 0.001). The results also revealed that participants aged 20–29 years had lower PTSD scores than those aged 50 years and over. As for field experience, participants who had <5 years of experience had lower PTSD scores than those who had 15 to <20 years of experience. For subjective health status, participants who had a very healthy status had lower PTSD scores than those who had other health statuses. Participants who had severe or some diseases had higher PTSD scores than those who were generally healthy.
The correlations between the major variables are listed in Table 4. CIT had a significant positive correlation with resilience (r = 0.19, p = 0.009) and PTSD (r = 0.30, p #x02264; 0.001). Social support showed a significant positive correlation with resilience (r = 0.48, p < 0.001) and a significant negative correlation with PTSD (r = −0.40, p < 0.001). Resilience had a negative correlation with PTSD (r = −0.23, p < 0.001).

Table 4. Correlations between critical incident trauma, social support, resilience, and post-traumatic stress disorder.
Multiple regression analyses were conducted to identify factors that are independently related to PTSD. Variance inflation factors (VIFs) and tolerance values were confirmed for multicollinearity. There were no multicollinearity issues. The VIFs were 1.241–5.152 (and therefore, smaller than the reference value of 10), and the range of tolerance values was 0.194–0.806 (and thus, larger than 0.1 but did not exceed 10). The independence of the residuals was checked using the Durbin-Watson statistic, which was 2.082, and there was no problem with autocorrelation. Cook's distance for outliers was 0.061 or smaller, and thus, were all smaller than the reference value of 1.0, and the assumptions for the multiple regression analyses were satisfied.
Table 5 shows the results of the regression analysis. The model was found to be significant (F = 6.41, p ≤ 0.001), and the adjusted coefficient of determination (Adj R2), which indicates the explanatory power of the model, was 0.287. Significant factors related to PTSD included having a very healthy status (B = −0.44, p = 0.013), CIT (B = 0.18, p ≤ 0.001), social support (B = −0.38, p ≤ 0.001), and resilience (B = −0.18, p = 0.044). These factors explained 28.7% of the variance in PTSD.
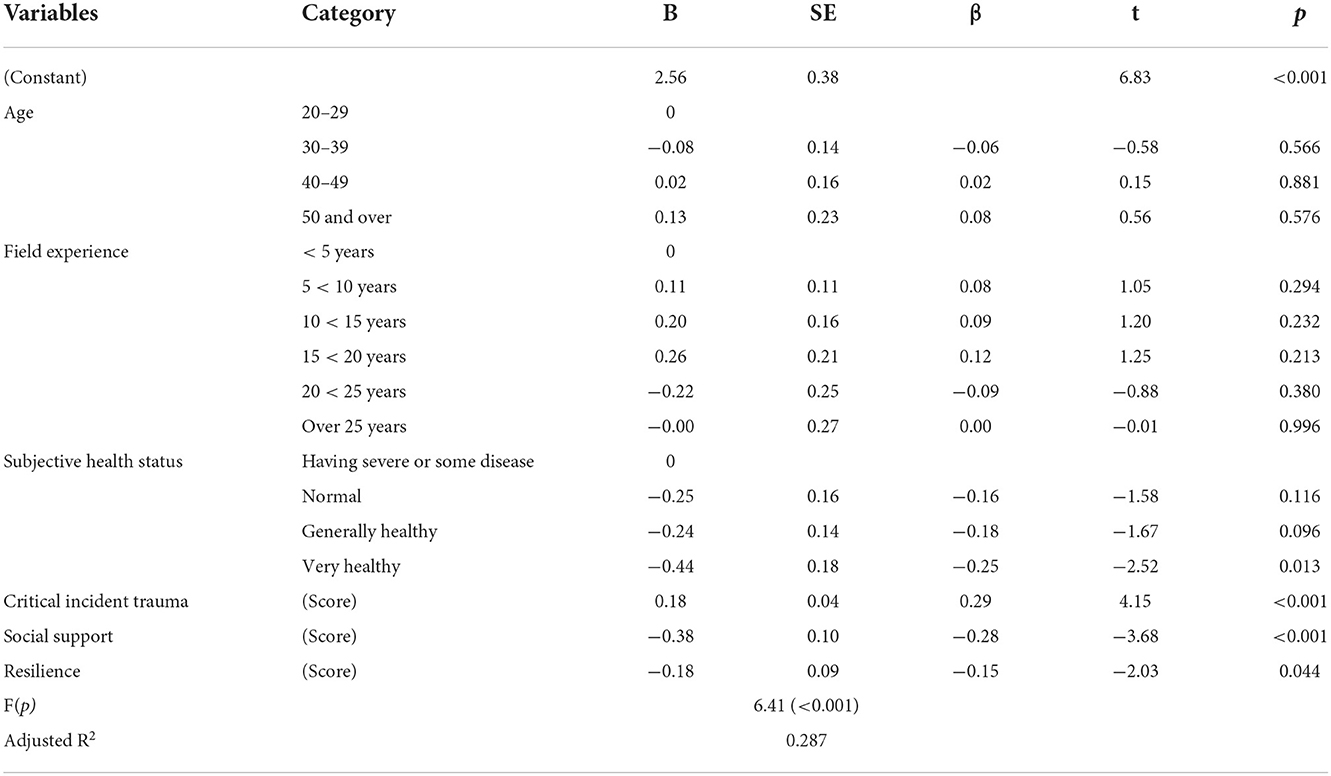
Table 5. Factors influencing post–traumatic stress disorder of police officers.
For the semi-structured interviews with stakeholders, all stakeholders responded that police officials suffer psychological difficulties after traumatic experiences (Table 6). The limitations of overcoming traumatic experiences were classified into five obstructive factors: social prejudice as a police official, fear of stigma and medical history of PTSD treatment, difficulty in receiving social support, fear and doubts about self-disclosure, and closed working environments. Coping strategies with traumatic experiences were divided into five categories, namely, individual response (failure), using external support, conscious separation, emotional purification, and response at the department level. The issues of anonymity, accessibility, and target selection should be considered when operating counseling programs for PTSD police officials.
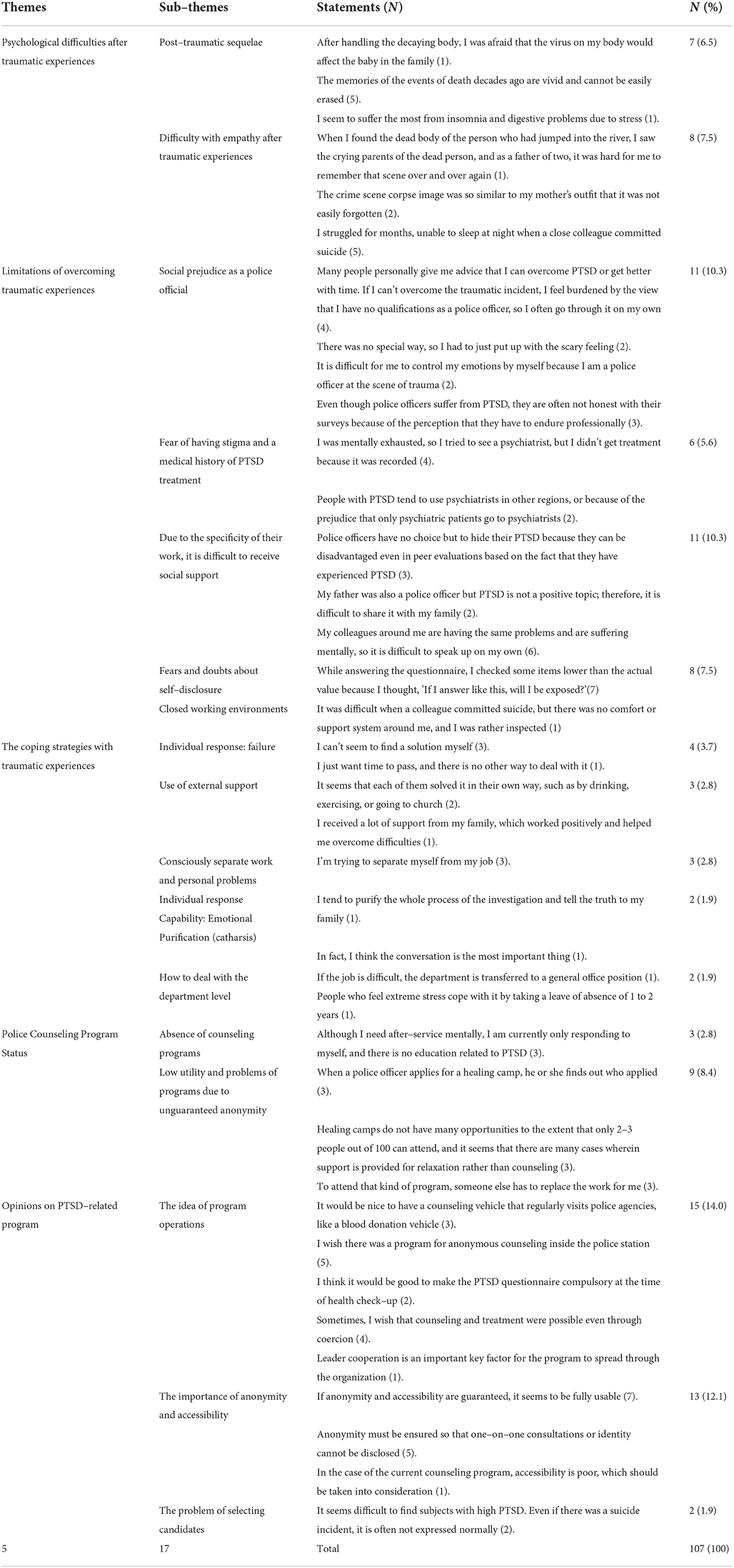
Table 6. Content analysis of semi–structured interviews with stakeholders.
We aimed to investigate the factors affecting PTSD among Korean police officers.
In analyzing the differences in CIT, social support, resilience, and PTSD according to participants' general characteristics, we found that male police officers have higher CIT scores. This is confirmed by the fact that male officers have more field experience than female officers. Therefore, male police officers are more likely to encounter traumatic incidents than female police officers. We found that participants aged between 20 and 29 years had higher social support scores than those aged 50 years and over. Participants aged 50 years and over had higher PTSD scores than those aged 20–29 years. These findings are consistent with previous findings (22, 23). Therefore, it is necessary to implement PTSD intervention programs for the group aged 50 years and over with low social support and high PTSD levels. We found that participants with university education had lower resilience than those with postgraduate education or higher. However, a previous study found no differences between educational level and resilience (24). Therefore, a follow-up study is needed.
Regarding rank, we also found that lower-ranked policemen had higher social support than senior inspectors. Although this result cannot be easily interpreted because there are no existing studies on this topic, Luceno-Moreno et al. (25) revealed that lower-ranked policemen had higher organizational support than higher-ranked policemen. In addition, this result is consistent with social support results based on age. As for field experience, participants with 15 to < 20 years of field experience had higher PTSD scores than those with < 5 years of experience. This result is consistent with that of Kim (26), indicating that long exposure to trauma is associated with higher PTSD scores; therefore, these participants should be selected as a high-risk group.
Second, the negative correlations between social support and PTSD as well as resilience and PTSD showed that higher social support and resilience had positive effects on PTSD, which is consistent with the results of previous studies (27, 28). Additionally, the positive correlation between social support and resilience was also reported by Mesidor and Sly (28). A positive correlation between CIT and resilience was confirmed. This is in line with the findings of Vincent (29), who showed that providing police officers with greater resilience after serious critical incidents can prevent serious mental health problems. The positive correlation between CIT and PTSD is the same as the results of Ntatamala and Adams (30) and also supports the argument that the more critical incidents police officers are exposed to, the more severe their PTSD (31).
The factors that influence PTSD include health status (very healthy), CIT, social support, and resilience. A subjective health status (very healthy) results in a lower degree of PTSD, as confirmed by previous studies (32, 33). Thormar et al. (33) found high levels of PTSD symptoms and subjective health complaints at 18 months post-disaster. In other words, PTSD also forms an area of mental health, and perceived subjective health status (very healthy) is related to lower PTSD symptoms. This study revealed that CIT influences PTSD, which confirms the findings of Bogaerts et al. (34) study, in which security workers with critical incidents suffered more PTSD symptoms and were significantly more unstable than those with no or indirect critical incidents. Similarly, Ménard and Arter (4) reported that critical incidents were positively associated with PTSD symptoms among police officers. Therefore, preventive programs related to PTSD are needed for police officers who are frequently exposed to CIT. In this study, social support and resilience were found to lower PTSD symptoms. Studies have also found that social support (10, 28) and resilience (10, 17, 28) are protective factors against PTSD. Therefore, future programs should include these components to overcome and prevent PTSD.
The results of the semi-structured interviews with stakeholders revealed that police officers are unable to easily express their mental stress due to social prejudice. Despite experiencing PTSD, it is difficult for police officers to receive social support from colleagues and families. In addition, they cannot receive appropriate psychiatric treatment because of their personal evaluations as police officers. Therefore, PTSD programs with enhanced anonymity and accessibility are necessary.
To prevent prevalence of PTSD in Korean police officers, even if they experience frequent traumatic events, it is necessary for police organizations to make efforts to strengthen their social support and resilience. In particular, there is an urgent need to prepare practical and policy measures to provide direct assistance to police officers in their work performance and to provide more active interventions for police officers who experience trauma.
The critical results obtained in this study are as follows:
First, subjective health status (very healthy), CIT, social support, and resilience appeared to have strong effects on PTSD.
Second, it is important to identify the difficulties faced after post-traumatic experiences, the uniqueness of the police organization, coping strategies, and the current status of support programs for police officers in South Korea.
However, this study has some limitations that must be addressed in future studies. First, the participants were recruited through convenience sampling. Nonetheless, the results are meaningful. The vulnerability of quantitative research results was strengthened through the semi-structured interviews. In particular, mixed-methods research should be applied because of the closeness and specificity of the police organization.
Third, our findings are subject to the limitations inherent in the cross-sectional data. Therefore, in future studies, causal relationships among variables should be analyzed using longitudinal study designs.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of Daegu University. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. The patients/participants provided their written informed consent to participate in this study.
H-KO and MK designed the study. H-KO, MK, and CJ conducted the study and collected the data. H-KO coordinated and supervised the data collection, analyzed the data, and drafted the manuscript. H-KO and CJ reviewed and revised the manuscript. All authors read and approved the final manuscript.
This study was supported by a research grant from the National Research Foundation of Korea in 2022. This funder had no role in the study design, data collection, analysis, interpretation, writing of the manuscript, or decision to submit the article for publication.
The authors are grateful to the police officers for their participation in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Maguen S, Metzler TJ, McCaslin SE, Inslicht SS, Henn-Haase C, Neylan TC, et al. Routine work environment stress and PTSD symptoms in police officers. J Nerv Ment Dis. (2009) 197:754–60. doi: 10.1097/NMD.0b013e3181b975f8
2. McCanlies EC, Mnatsakanova A, Andrew ME, Burchfiel CM, Violanti JM. Positive psychological factors are associated with lower PTSD symptoms among police officers: post Hurricane Katrina. Stress Health. (2014) 30:405–15. doi: 10.1002/smi.2615
3. Clark R, Distelrath C, Vaquera G, Winterich D, Dezolt E. Critical-incident trauma and crime scene investigation: a review of police organizational challenges and interventions. J Foren Identification. (2015) 65:929–51.
4. Ménard KS, Arter ML. Police officer alcohol use and trauma symptoms: Associations with critical incidents, coping, and social stressors. Int J Stress Manag. (2013) 20:37–56. doi: 10.1037/a0031434
5. Korea Government National Action Plan for Suicide Prevention. Available online at: https://www.opm.go.kr/flexer/view.do?ftype=hwp&attachNo=94247 (accessed August 10, 2022).
6. Maeil Business Newspaper. 21 Police Officers Committed Suicide this Year and one Counselor is Consulting 427 Police Officers. Seoul: Maeil Business Newspaper.
7. Cohen S, Hoberman HM. Positive events and social supports as buffers of life change stress. J Appl Soc Psychol. (1983) 13:99–125. doi: 10.1111/j.1559-1816.1983.tb02325.x
8. Blais RK, Tirone V., Orlowska D, Lofgreen A, Klassen B, Held P., et al. Self-reported PTSD symptoms and social support in U.S. military service members and veterans: a meta-analysis. Europ J Psychotraumatol. (2021) 12:1851078. doi: 10.1080/20008198.2020.1851078
9. Kwak D-G, Kim D-W, Kim, MG. A study on the post-traumatic stress disorder in police office. Korean Assoc Criminal Psychol. (2011) 7:23–46.
10. McCanlies EC, Gu JK, Andrew ME, Burchfiel CM, Violanti JM. Resilience mediates the relationship between social support and post-traumatic stress symptoms in police officers. J Emerg Manag. (2017) 15:107–116. doi: 10.5055/jem.2017.0319
11. Olff M, Koch SBJ, Nawijn L, Frijling JL, Van Zuiden M, Veltman DJ, et al. Social support, oxytocin, and PTSD. Eur J Psychotraumatol. (2014) 5:26513. doi: 10.3402/ejpt.v5.26513
12. Horn SR, Charney DS, Feder A. Understanding resilience: new approaches for preventing and treating PTSD. Exp Neurol. (2016) 284:119–32. doi: 10.1016/j.expneurol.2016.07.002
13. Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatol. (2014) 5:25338. doi: 10.3402/ejpt.v5.25338
14. Streb M, Häller P, Michael TPTSD. in paramedics: resilience and sense of coherence. Behav Cogn Psychother. (2014) 42:452–63. doi: 10.1017/S1352465813000337
15. Kim BH, Park JP. A study on the survey of post-traumatic stress disorder of Korea police officers and systematic counter-measures. Korean J Public Safety Criminal Justice. (2016) 64:109–38. doi: 10.21181/KJPC.2016.25.3.109
16. Kim BH. Effect of police office's trauma aase experience on post-traumatic stress disorder [the analysis of casual effects among traumatic events, PTSD in the police officers–focused on the police officers in Busan Metropolitan. Korean J Public Safety Criminal Justice. (2016) 25:119–44. doi: 10.21181/KJPC.2016.25.4.119
17. Kim SH. Effects of resilience on the post-traumatic stress disorder of police officers. Korean J Public Safety Criminal Justice. (2018) 27:69–90. doi: 10.21181/KJPC.27.2.69
18. National Center for PTSD (2018). Life Events Checklist for DSM-5. Available online at: https://www.ptsd.va.gov/professional/assessment/te-measures/life_events_checklist.asp (accessed August 10, 2022).
19. Kim DH, Lee HK, Kim JW, Lee K. Reliability and validity of the Korean version of interpersonal support evaluation and List-12 (ISEL-12). Korean Neuropsychiatr Assoc. (2012) 51:416–21. doi: 10.4306/jknpa.2012.51.6.416
20. Liebenberg L, Moore JCA. social ecological measure of resilience for adults: The RRC-ARM. Soc Indicators Res. (2018) 136:1–19. doi: 10.1007/s11205-016-1523-y
21. Kim J, Chung H, Choi J, So H, Kang S, Kim DS, et al. Psychometric properties of the korean version of the PTSD Checklist-5 in Elderly Korean Veterans of the Vietnam War. J Anxiety Mood. (2017) 13:123–31. doi: 10.24986/anxmod.2017.13.2.123
22. Lee JH, Kim I, Won J-U, Roh J. Post-traumatic stress disorder and occupational characteristics of police officers in Republic of Korea: a cross-sectional study. BMJ Open. (2016) 6:e009937. doi: 10.1136/bmjopen-2015-009937
23. Lee S, Jeong S, Choi Y. Factors affecting social support and resilience on police officer. Int J Curr Res Rev. (2021) 13:4–10. doi: 10.31782/IJCRR.2021.13528
24. Talavera-Velasco B, Luceño-Moreno L, García-Albuerne Y, Martín-García J. Perception of health, resilience, and engagement in spanish police officers during the COVID-19 pandemic. Psicothema. (2021) 33:556–63.
25. Luceno-Moreno L, Garcia-Albuerne Y, Talavera-Velasco B, Martin-Garcia J. Stress in Spanish police force depending on occupational rank, sex, age and work-shift. Psicothema. (2016) 28:389–93. doi: 10.7334/psicothema2015.310
26. Kim JKA. Study on the post traumatic stress disorder of police officer. Korean Assoc Police Sci Rev. (2012) 36:31.
27. Lee JK, Choi HG, Kim JY, Nam J, Kang HT, Koh SB, et al. Self-resilience as a protective factor against development of post-traumatic stress disorder symptoms in police officers. Ann Occup Environ Med. (2016) 28:58. doi: 10.1186/s40557-016-0145-9
28. Mesidor JK, Sly KF. Religious coping, general coping strategies, perceived social support, PTSD symptoms, resilience, and posttraumatic growth among survivors of the 2010 earthquake in Haiti. Ment Health Relig Cult. (2019) 22:130–43. doi: 10.1080/13674676.2019.1580254
29. Vincent M. The Relationship Between Programming After Critical Incidents, Shootings, and Resilience in Police. ProQuest Dissertations Publishing
30. Ntatamala I, Adams S. The correlates of post-traumatic stress disorder in ambulance personnel and barriers faced in accessing care for work-related stress. Int J Environ Res Public Health. (2022) 19:2046. doi: 10.3390/ijerph19042046
31. Clair ME. The Relationship Between Critical Incidents, Hostility and PTSD Symptoms in Police Officers. ProQuest Dissertations Publishing.
32. Kim SY. An analysis of factors influencing post-traumatic stress disorder (PTSD) - difference by disaster information. Crisisonomy. (2020) 16:65–78. doi: 10.14251/crisisonomy.2020.16.5.65
33. Thormar SB, Gersons BPR, Juen B, Djakababa MN, Karlsson T, Olff M, et al. The impact of disaster work on community volunteers: the role of peri-traumatic distress, level of personal affectedness, sleep quality and resource loss, on post-traumatic stress disorder symptoms and subjective health. J Anxiety Dis. (2014) 28:971–77. doi: 10.1016/j.janxdis.2014.10.006
Keywords: post-traumatic stress disorder, Korean police officers, critical incident trauma, social support, resilience
Citation: Oh H-K, Jang CY and Ko MS (2022) Factors influencing post-traumatic stress disorder among police officers in South Korea. Front. Public Health 10:1024284. doi: 10.3389/fpubh.2022.1024284
Received: 21 August 2022; Accepted: 11 November 2022;
Published: 09 December 2022.
Edited by:
Wulf Rössler, Charité Universitätsmedizin Berlin, GermanyReviewed by:
Gabriele d'Ettorre, ASL Lecce, ItalyCopyright © 2022 Oh, Jang and Ko. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cheol Yeung Jang, aGV5Zm9yMUB0ay5hYy5rcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.