 Eunsoo Kim
Eunsoo Kim Sujin Park
Sujin Park Soojin Kim
Soojin Kim Yeji Choi
Yeji Choi Jae Hyoung Cho
Jae Hyoung Cho Geonwoo Kim
Geonwoo Kim- Forest Human Service Division, Future Forest Strategy Department, National Institute of Forest Science, Seoul, South Korea
Introduction: Nature exposure is a widely accepted option for promoting public health owing to the recent surge of scientific evidence. However, the actual settings to facilitate this initiative is yet to be extensively reviewed. In this systematic review, we have aimed to provide an up-to-date summary of interventional studies investigating the psycho-physiological effects of forests and urban forests, including details on their physical settings, and investigate an effect-modifying role of altitude and summarize data on the magnitude and shape of the association.
Methods: A keyword search using five electronic academic databases (PubMed, Embase, PsycINFO, Web of Science, and Scopus) was conducted to identify relevant articles published in English from the inception year to the end of February 2022. The methodological quality was evaluated using the ROBINS-I or ROB2 tool, depending on the study design. Meta-regression and random effects model were jointly used to examine the relationship between altitude and health outcomes.
Results: We included 27 eligible studies and 31 cases extracted from 19 studies were used for the meta-analysis. In the meta-regression, we observed a non-linear association between altitude and psycho-physiological effects. Altitude had a positive quadratic association with anxiety (p < 0.000, adjusted R2 = 96.79%), depression (p < 0.000, adjusted R2 = 98.78%), and fatigue (p < 0.000, adjusted R2 = 64.74%) alleviating effects. Conversely, altitude demonstrated a negative non-linear association with the blood pressure-lowering effect (p = 0.009, adjusted R2 = 32.83%). Additionally, the thermal index (THI) and illuminance (lx) levels were significantly associated with effect sizes of psychological restoration.
Discussion: This review provides moderate-certainty evidence for an effect-modifying role of altitude. The meta-regression results suggested the optimal and minimal altitude ranges for psychological restoration and physiological relaxation, respectively. Despite some limitations, the study findings provide a significant basis for utilizing altitude, which is easily accessible and simple, to promote the health benefits of nature-based initiatives.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022310894, identifier: CRD42022310894.
Introduction
Historically, nature has empirically been used as a medium for psycho-physiological restoration. The commencement of earnest theoretical discussions in the 1980s have led to an active accumulation of scientific evidence on the restorative effects of nature (1, 2). Demands of daily life and stress may deplete psycho-physiological resources and result in heightened negative emotions, cognitive fatigue, and excessive physiological arousal (3–5). Persistent depletion can impair individuals' mental and physical health; hence, consistent restoration of psycho-physiological resources, analogous to the process of stress, is needed to remain healthy (6, 7). Nature exposure, which is rich in elements that can boost attention and restore cognitive resources without mental exertion, is a viable restoration process (8, 9). Furthermore, natural stimuli evoke moderate levels of interest and pleasure, which in turn elevate positive emotions, block negative thoughts, and enable a return to a moderate level of physiological arousal (10–12). Thus, nature exposure is linked to improved health via cognitive recovery, emotional restoration, stress reduction, and physiological relaxation.
A recent surge in scientific and clinical trials on nature and health has led to the social acceptance of nature-based interventions (13–16). Mounting evidence confirms the significant association between nature and health (1, 17–19); therefore, the World Health Organization and other health entities have emphasized nature as a health-promoting resource. Moreover, the recognition of nature as a non-pharmacological therapy in preventive and complementary medicine has penetrated the mainstream consciousness (20–22). Consequently, several countries have endeavored to quantitatively expand nature exposure (1, 23–26), and incorporated it into public health promotion practices (27–30). Notably, since the late 2000s, numerous forest-based initiatives have actively been implemented across East Asia, Europe, and North America to promote public health (28, 29, 31). Japan has introduced a forest certification system to maintain the quality of forest therapy, and emphasizes medical and scientific evidence (32). Korea has a license system for forest therapy, created healing forests, improved institutional framework, and trained therapists (33). Germany has promoted the use of forests for health promotion initiatives, including klimatherapie, terinkur, and kneipp; in 2019, a German state introduced legislation to ensure that forest therapy is covered by health insurance [(28), p. 321–336]. Additionally, forest-based interventions are officially employed across Europe and North America through green prescriptions, green exercise, and health tourism (34–37).
Several clinical trials concur that since all natural settings do not provide the same health benefits, the focus needs to shift from quantity to quality of nature (17, 38). Understanding the detailed characteristics of natural settings that determine the degree of health benefits is necessary to strengthen the evidence and systematize nature-based interventions (16, 21, 39, 40). Therefore, recent research is shifting from a simple dichotomous contrast between the natural and built environments to examining the variation in health effects according to the characteristics of natural settings. Previous studies have evaluated differences in health effects from an environmental psychological perspective using varied parameters, including the perceived amount of greenery (41–43), enclosure and openness of vegetation (44–48), and visual perception (49–59). Moreover, several studies have investigated the psychophysiological effects of different types of landscapes (60–69), and compared the health impacts of natural environments with varied ecological characteristics (64, 70–73) or silvicultural practices (2, 70–78). While recent research has predominantly focused on visual experience or ecological aspects, physical environments or non-visual experiences remain largely unexplored.
In recent studies, physical variables including altitude, temperature, humidity, and illuminance, are increasingly reported for comparing environmental conditions between study sites. Although these are readily available and crucial components of outdoor experiences, their impacts on outcomes have rarely been investigated. Few studies have investigated the relationship between the physical variables and outcomes of nature-based interventions (70, 79). An et al. (70) reported that changes in temperature, humidity, and light spectrum of forest settings can modify physiological outcomes of forest bathing. Similarly, Park et al. (79) indicated that physical variables of in-forest settings were responsible for psychological restoration. Thus, the physical factors may be crucial for nature-based interventions. However, to the best of our knowledge, comprehensive reviews or quantitatively synthesized evidence to investigate the effect-modifying role of physical variables remains limited. Previous reviews often focused on the association between vegetation levels and heat-related mortality (80, 81), which provided limited implications for selecting appropriate natural settings for nature-based interventions. Therefore, we have conducted a systematic review with meta-analysis to summarize the evidence across interventional studies investigating the psycho-physiological effects of nature exposure along with the descriptions of the physical variables.
Forests are a representative environment for nature-based interventions, and environmental changes according to altitude are particularly distinct and dramatic. Hence, we have focused on interventional studies conducted in forests or urban forests comprising “all woodlands, groups of trees, and individual trees located in urban and peri-urban areas” (82). Moreover, existing literature implies the link between forest-based intervention and physical factors of the forest. In several countries, definitions pertaining to the therapeutic use of forests frequently refer to the use of the atmospheric and topographic properties of forests. For example, shinrin-yoku—Japanese forest use for therapeutic purposes—is defined as “taking in the forest atmosphere or forest bathing.” (83). In Germany, kilmatherpie is refers to the use of microclimatic elements to deal with disease, and terrainkur is defined as an exercise method utilizing the terrain properties of forest trails [(29), p. 31]. In Korea, the government enacted a legislation defining forest healing as immune-strengthening and health-promoting activities utilizing the various forest elements (84). There are six distinctive forest healing practices; namely, climate, plant, water, diet, psycho-, and exercise therapies (85). The Korea Forest Service identified thermal comfort, scenery, and aromatic substances as essential properties for forest therapy (86). Furthermore, Shin et al. (33) highlighted the health advantages of forest-based interventions derived from experiencing the physical conditions of forest environments. Therefore, we have assumed that altitude and relevant physical variables are effect-modifiers that cause differences in the health effects of forest-based interventions.
Herein, we have provided an up-to-date summary of interventional studies examining the psycho-physiological effects of forest-based interventions, including descriptions of the physical variables of forests. In addition, using meta-analysis, we have statistically investigated whether altitude could modify the health benefits of forest exposures and the shape and magnitude of the associations by pooling the psychological and physiological outcomes with corresponding physical conditions. The research question conformed to the PICOS (Population, Intervention, Comparison, Outcomes, and Study) framework (39, 87): “In general populations, what is the effect of altitude of forest-based interventions on psycho-physiological effect—emotional restoration, cognitive restoration, stress reduction, physiological relaxation—from interventional studies?”
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 (88) and Cochrane Handbook for Systematic Reviews of Interventions (89) guidelines were followed. The PRISMA checklist is presented in Supplemental Table 1. This systematic review and meta-analysis were registered on PROSPERO (CRD42022310894) and OSF database (doi: https://doi.org/10.17605/OSF.IO/SG7TD) prior to commencement.
PICOS and eligibility criteria
Our research question was framed and refined using PICOS to address a clearly formulated review question: “In general populations, what is the effect of altitude of forest-based interventions on psycho-physiological aspects—emotional restoration, cognitive restoration, stress reduction, physiological relaxation—in interventional studies?” (87, 89). In addition, the eligibility criteria following the PICOS framework, is presented in Table 1.
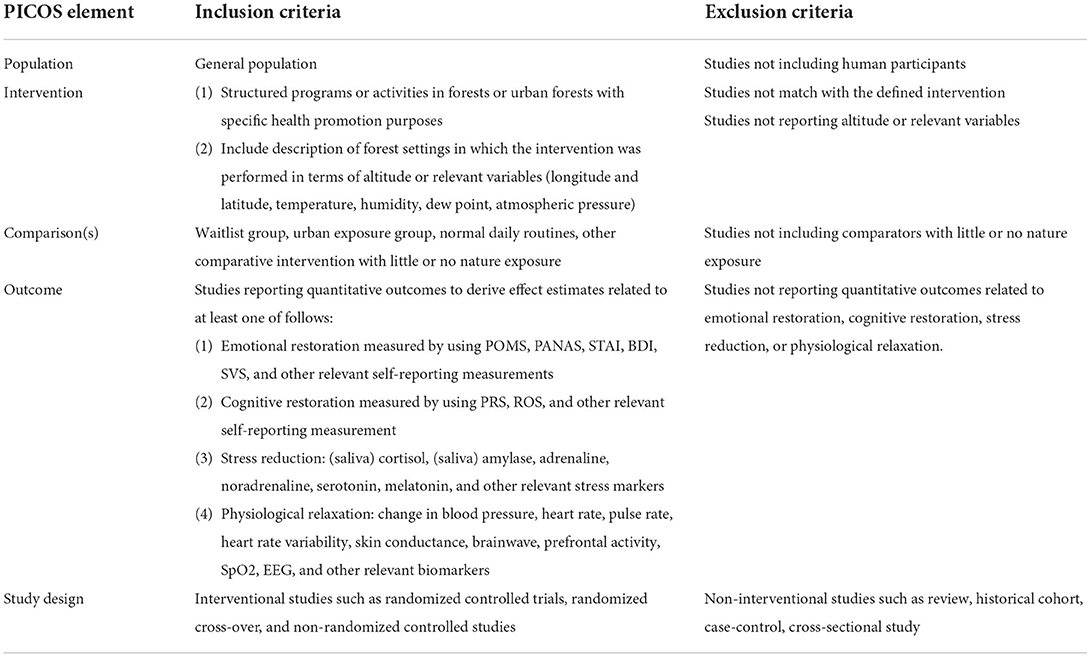
Table 1. Eligibility criteria for study selection.
Search strategy
A literature search using five electronic academic databases—PubMed, Embase, PsycINFO, Web of Science, and Scopus—was performed. Published articles in English, from the inception year to the end of February 2022, were searched using a combination of search terms related to environmental setting (21 terms), intervention (48 terms), altitude or location (71 terms), health outcomes (69 terms), and study designs (16 terms). Details on the search terms are presented in Supplemental Table 2 and are publicly available (DOI: https://www.crd.york.ac.uk/PROSPEROFILES/310894_STRATEGY_20220215.pdf).
Study selection process
The search results were exported to the EndNote Citation Manager software (Endnote 20.3, Clarivate Analytics, London, UK). After de-duplication, two investigators (EK and SK) independently screened the titles and abstracts to exclude explicitly irrelevant cases, and subsequently, conducted a full-text review based on the eligibility criteria. In case of discrepancies, both investigators conducted a second full-text review and consensus-based discussion to determine eligibility for inclusion. In case of conflicting views, two other investigators were consulted to resolve the discrepancies (GK and SP).
Data extraction
The data from the included studies were independently extracted by two investigators (GK and EK), using the same data extraction form, and were cross-checked. The extracted data included (a) study information (author, year of publication, country, city, study design, conducted date, and time of measurement); (b) sample (sample size, gender, and age); (c) forest variables [altitude, location, longitude, latitude, dominant tree species, height (m), diameter at breast height (cm), stand density (trees/ha), canopy density (%)]; (d) environmental variables [temperature (°C), relative humidity (%), radiant heat (°C), wind speed (m/s), illuminance (lx), and noise level (dB)]; (e) intervention (activities, activity duration, and frequency); (f) outcome measurement [measurement indices, pre-measurement (M ± SD), post-measurement (M ± SD), change in measurement (M ± SD), and inter-trial correlation]. In studies where only locations were reported, coordinates were used to estimate altitudes. In studies where altitudes were mentioned as ranges, median or midpoint value was chosen for each forest exposure, depending on data availability. In studies reporting both temperature and humidity, the temperature humidity index (THI) was calculated as an indicator of bioclimatic conditions reflecting heat and cold stress (90, 91).
Methodological quality
The latest version of the Risk of Bias 2 (RoB2) tool was used to evaluate the methodological quality of randomized parallel-group trials and randomized crossover trials (92). For non-randomized trials, the Risk of Bias in Non-randomized Studies Interventions (ROBINS-I) tool (93) was used. The risk of bias that may have occurred in the randomization process, trial design, dropouts and missing data, and outcome measurement were evaluated via the RoB2 tool. The risk of bias that may have arisen due to confounding factors, participant selection, classification of intervention, dropout and missing data, outcome measurement, and reporting were assessed via the ROBINS-I tool. The risk of bias was independently assessed by two investigators (EK and GK) based on the answers for the signaling questions in five, six, and domains for randomized parallel-group trials, randomized crossover trials, and non-randomized trials, respectively.
Quantitative synthesis
Statistical analysis was performed using R 4.20 and R Studio with “meta,” “metafor,” and other R packages (94, 95). First, the effect size of the individual studies and the overall effect size were calculated. Subsequently, a series of meta-regressions were performed to verify whether altitude and related physical variables influenced the effect size of studies and the magnitude and shape of the association were investigated. Finally, sensitivity and publication bias analyses were conducted to check the robustness of our results.
Estimating overall effect size
Standardized mean difference (SMD) was calculated using a random-effects model. The SMD is a representative measure of efficacy computed using the mean, standard deviation, and number of samples of both interventional and control groups. An SMD of zero indicates that there is no difference in effect between the intervention and control. If improvement is related to higher scores on outcome measures, an SMD > 0 reflects the extent to which the intervention is more effective than the control. Conversely, if improvement is related to lower scores on the outcome measure, an SMD <0 reflects the extent to which intervention is less effective than the control. According to Cohen's (96) guidelines, the result of SMD 0.20–0.49, 0.50–0.79, and ≥0.80 as “small,” “medium,” and “large” effect sizes, respectively.
Since the effect of forest exposure was hypothesized to vary by altitude and relevant physical variables, a random-effects model—which assumed that the true effect size varies by study and is distributed around the overall mean— was used to estimate effect size. A restricted maximum-likelihood estimation, recommended in a recent simulation study (97), was employed to estimate the between-study variance in the random-effects model. The overall effect size was weighted by the inverse variance method. Cochran's Q-test (p < 0.10 for statistical significance) and the I2 (I2 > 50% used as a threshold for significant heterogeneity) was used to investigate heterogeneity in the effect sizes. Cochran's Q test is a statistical test to determine whether interventions have an identical effect. I2 is an index reflecting variance across studies attributable to heterogeneity, with 25–50, 50–75, and 75–100% indicating low, medium, and large heterogeneity, respectively (98).
Meta-regression
Meta-regression, a sophisticated tool for exploring heterogeneity, aims to identify whether a significant association exists between an outcome measure and one or more study-level variables. In our study, we assumed that altitude and physical variables were effect modifiers and conducted a meta-regression to further explore heterogeneity. A series of meta-regression were performed using both linear and non-linear models; non-linear models reportedly reflect phenomena better than linear models (99–101). Log-likelihood and Akaike's Information Criterion (AIC) were used for model comparison and a suitable association model was selected. Data on the magnitude of the association was summarized using the following test statistics: QM (omnibus test statistics of model coefficients used in moderator analysis); R2 (the amount of heterogeneity accounted for); model outcomes (regression coefficients, standard error, and confidence limits); and difference between total heterogeneity and regression heterogeneity. The effect size trends by altitude are graphically represented using predicted curves and 95% confidence intervals (CI).
Sensitivity analysis and publication bias
Individual studies' influence on the effect estimation was checked through rstudent, diffits, Cook's D, covratio, τ2, Qresid, hat, and dfbetas values. The “leave-one-out” method was used for sensitivity analysis. Publication bias was graphically and quantitatively assessed using a funnel plot and Egger's regression test, respectively (102).
Certainty of evidence
The overall degree of certainty of evidence was evaluated using the GRADE method (103). Based on our research question, the certainty of altitudinal influence on psycho-physiological restoration provided by the meta-regression results was assessed. GRADEPro GDT (https://gradepro.org) was used to evaluate the certainty of evidence and create a Summary of Findings table (104).
Results
Study selection
The database search identified 7,024 studies, from which 2,052 duplicates and 4,840 studies were excluded after title and abstract screening. After a full-text assessment of the remaining 132 studies, 114 were excluded for the following reasons: without eligible health outcome (n = 27), without forest description (n = 25), without eligible intervention (n = 23), without eligible comparator (n = 24), reviews (n = 9), protocols (n = 5), and duplicated publication (n = 3). Ten studies and one study were added through backward citation and manual searches, respectively. Finally, 27 studies complied with the eligibility criteria, and 31 cases extracted from 19 studies were selected for the quantitative synthesis. The PRISMA flow diagram of the study selection is presented in Figure 1.
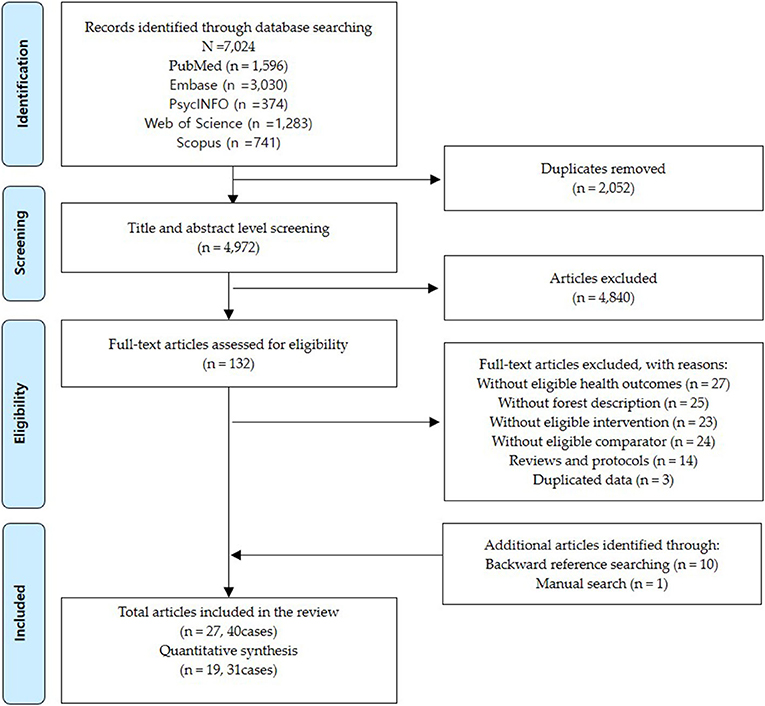
Figure 1. Flow diagram illustrating the selection process.
Study characteristics
Study characteristics of the 27 included studies are summarized in Table 2. The included studies performed nature-based interventions aimed at promoting health in urban forests and forests ranging in altitude from 11 to 1,324 m. The studies were published between 1995 and 2021; most were from East Asia (N = 16), followed by Northern Europe (N = 5), Central and Eastern Europe (N = 3), North America (N = 2), and Oceania (N = 1). The majority of studies (N=26) were conducted at latitudes between 28 and 60° N; the climate was typically temperate to humid continental, except one study (114) that was conducted at 19° S in semi-arid conditions. All the 26 study regions have distinct four-season patterns. The majority of studies conducted interventions between July and September [N = 11, temp 19.1–25.5°C, relative humidity (RH) 61.1–94.3%], followed by October–December (N = 5 temp 8–18°C, RH 52.3–79.0%), April–June (N = 4 temp 26.3–27.8°C, RH 39.9–44.3%), and January–March (N = 1, temp −0.5°C, RH 100.0%). Five studies did not indicate the precise period of the intervention, and one study carried out interventions throughout the year.
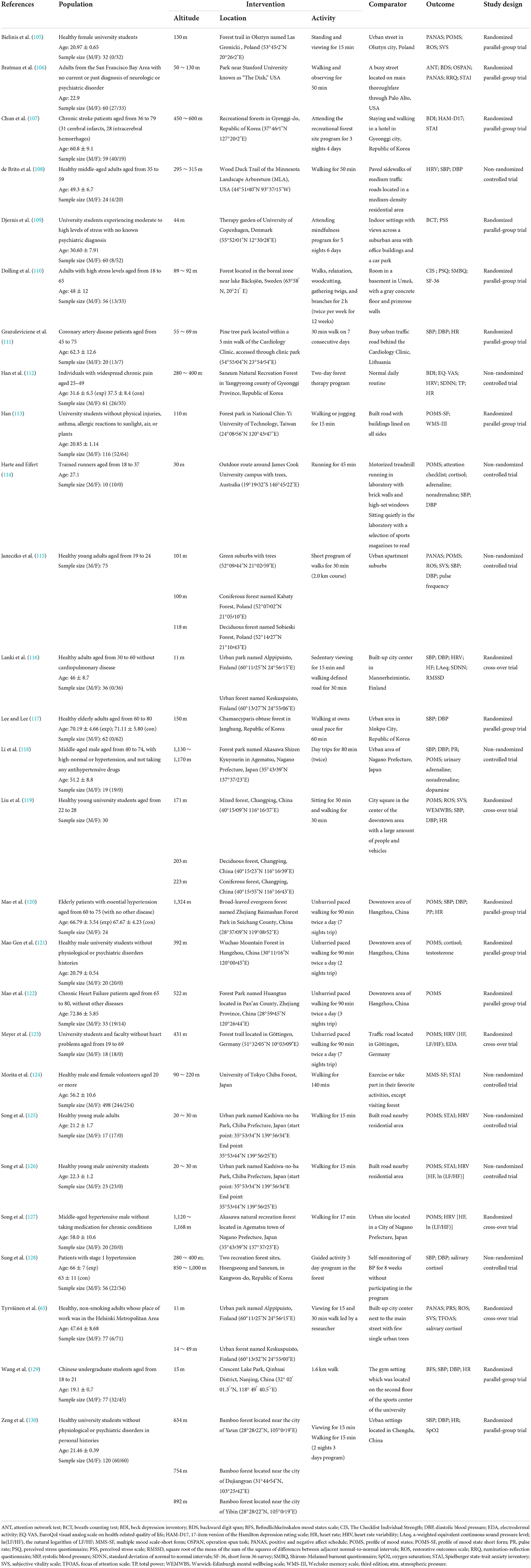
Table 2. Characteristics of the included studies ordered by first author's name and publication year.
Most of the included studies were randomized trials that employed either a randomized parallel-group design (N = 13) or a randomized cross-over design (N = 5), whereas the others were non-randomized controlled trials (N = 9). For studies with double or triple arms (65, 115, 116, 119), each arm was included as one independent case in comparison with the control. For studies reporting results separately by type or time of activity performed in both forest and control, each activity-specific case was included (116, 118, 119). Consequently, the studies will appear multiple times in the graphics and tables. The included studies cover a total of 1,668 participants, all of whom were adults. Participants totaled 436 below 100 m, 783 between 100 and 200 m, 153 between 200 and 500 m, 268 between 500 and 1,000 m, and 63 over 1,000 m. Most were healthy adults with no current or past diagnoses (N = 19). Hypertensive adults without medications for other conditions were recruited for four studies (118, 120, 127, 128). In addition, four included studies recruited patients with chronic heart failure (122), chronic stroke (107), coronary artery disease (111), and widespread chronic pain (112).
The included studies reported quantitative outcomes for emotional restoration (N = 19), physiological relaxation (N = 19), cognitive restoration (N = 7), and stress reduction (N = 7). Quantitative synthesis was performed on the results identified in more than ten cases. Mood states (including anxiety, depression, confusion, fatigue, hostility, and vitality) and blood pressure were investigated as an outcome in 20 and 12 studies, respectively. Cognitive restoration experience and heart rate or pulse rate were investigated in four and seven studies, respectively, although these reported in more than 10 cases. Affective state valance (65, 105, 106, 115), cognitive task score (65, 106, 113, 114), perceived stress level (109, 110) stress hormones (65, 114, 118, 121, 128), oxygen saturation (130), and time-domain measures or frequency-domain measures in heart rate variability (108, 112, 116, 123, 125–127) could not be analyzed owing to insufficient observations.
Prior to the quantitative synthesis, the investigators (EK, GK, SP, SK, and YC) reviewed several study-level variables to rule out possible confounding factors; namely, participant characteristics, geographical coordinates, climate classification, species compositions, physical environment of forest settings, time of measurement, duration, frequency, and activity intensity of interventions. Consequently, 31 cases from 19 studies were meta-analyzed. Seven studies were excluded because of unattainable data types (121, 125–127), rarely observed outcome (109), different species composition (130), and different climatic conditions (114).
Methodological quality
Results of the methodological quality assessment are presented in Tables 3, 4 for randomized trials and non-randomized trials, respectively. More than half of the included studies rated the risk of bias as “moderate” or “some concern.” Among the randomized trials, one study was deemed as “low” risk (129), 10 as being of “some concern” (38, 105, 106, 109, 111, 116, 117, 119, 120, 130), and seven as “high” risk of bias (65, 107, 110, 113, 121, 122, 127). Among the non-randomized trials, one study was deemed as “low” risk (108), five as “moderate” (112, 114, 118, 124, 128), and three as “serious” risk of bias (115, 125, 126).
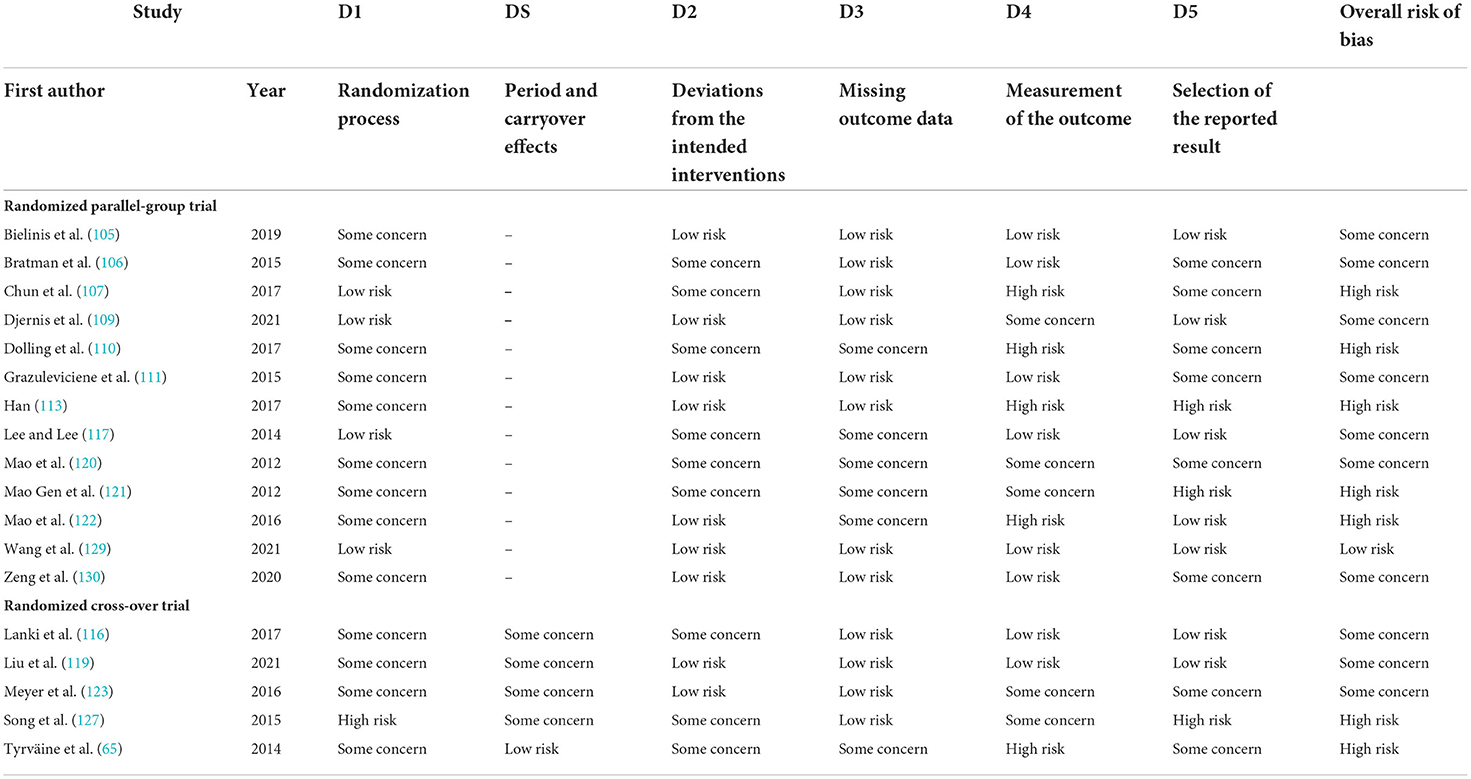
Table 3. Methodological quality assessment of randomized studies using RoB2 tool.
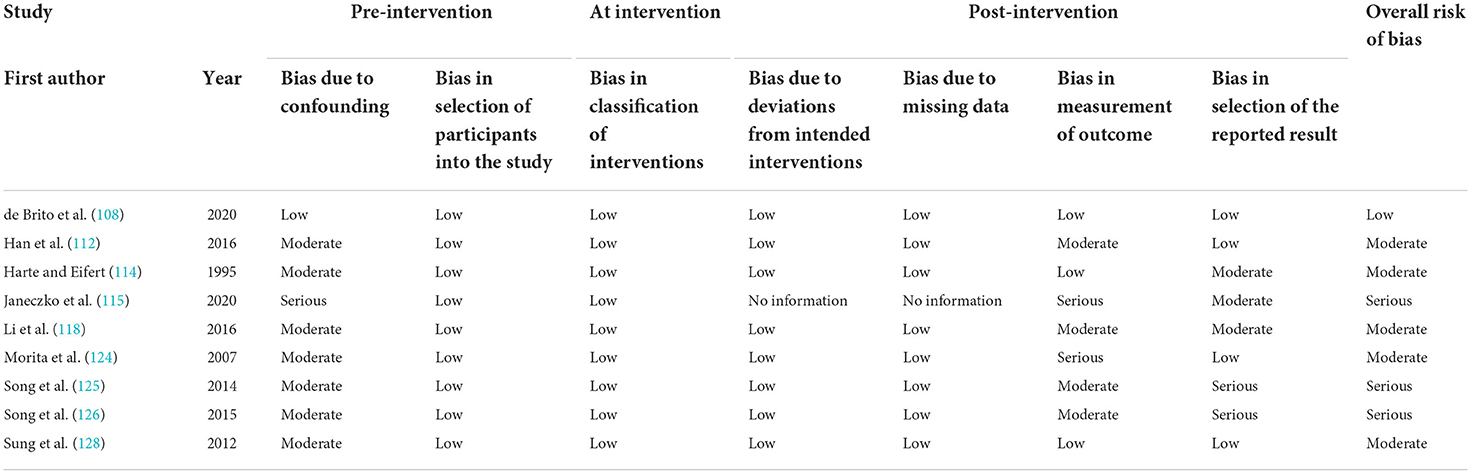
Table 4. Methodological quality assessment of non-randomized studies using ROBINS-I tool.
In randomized trials, the randomization process (D1), measurement of the outcome (D4), and selection of reported result (D5) were principally responsible for raising overall risk of bias. Only four studies described a detailed randomization process and allocation concealment (107, 109, 117, 129); however, the remaining studies were not sufficiently detailed. The majority of studies identified baseline differences for assignments, with one exception (127). Since 10 studies used self-reported measures without adequate participant blinding, the risk of bias in measurement was rated as “some concern” or “high risk” (65, 107, 109, 110, 113, 120–123, 127). Regarding reporting, 15 studies fully disclosed the results of multiple outcome measures and multiple analyses; seven studies were rated as having “low” risk of bias as they had pre-specified plans (105, 109, 116, 117, 119, 122, 129), whereas eight were rated as having “some concerns” owing to the lack of evidence to justify their analytical methods (65, 106, 107, 110, 111, 120, 123, 130).
In non-randomized trials, confounding bias and bias in the measurement of outcomes and selection of reported results were generally responsible for increasing overall risk of bias. Most studies were adequately measured or controlled for significant confounding factors; however, these were not comparable to well-performed randomizations, and therefore, were rated as “moderate” risk of bias. Eight studies using self-reported measures without adequate participant blinding were rated as “moderate” to “high” risk of bias, because knowledge of the intervention could lead to errors in measurement (112, 114, 115, 118, 124–126, 128). With the exception of two studies (125, 126), the majority provided complete disclosure of the measures and analyses (114, 115, 118), and four studies even offered pre-specified plans supporting their analytical methods (108, 112, 124, 128).
Quantitative synthesis
Overall effects of forest exposure
Compared with non-nature exposure, forest exposure revealed significant alleviating effects on symptoms of anxiety, depression, confusion, fatigue, and hostility with effect size (SMD) as follows: SMD = −1.20 (95% CI: −1.50–−0.89, 18 cases); SMD = −1.01 (95% CI: −1.34–−0.67, 17 cases); SMD = −1.05 (95% CI: −1.34–−0.75, 14 cases), −0.77(95% CI: −1.05–−0.49, 17 cases); and SMD = −0.77 (95% CI: −1.05–−0.49, 14 cases), respectively. Similarly, significant lowering in diastolic blood pressure (SMD = −0.32, 95% CI: −0.55–−0.10, 21 cases), systolic blood pressure (SMD = −0.50, 95% CI: −0.77–−0.23, 21 cases), and heart rate (SMD = −0.80, 95% CI: −1.09–−0.51, 23 cases) were observed. Additionally, Significant improvements in vitality (SMD = 1.04, 95% CI: 0.58–1.50, 14 cases) and restorative experience (SMD = 1.38, 95% CI: 0.95–1.80, 14 cases) were observed. Overall effect size and heterogeneity are reported in Table 5. Forest plots are reported in the Supplemental Figures 1–10.
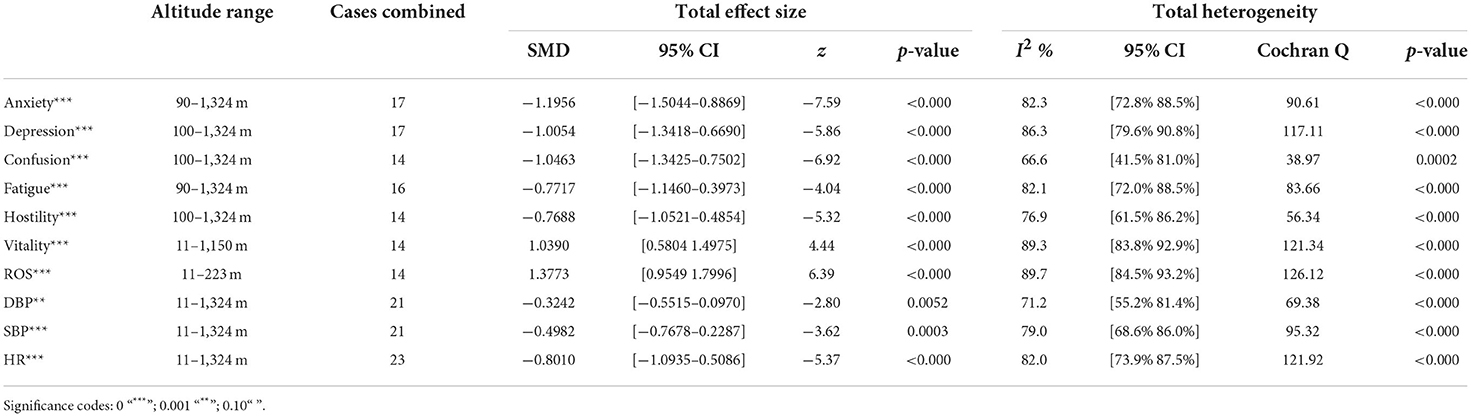
Table 5. Overall effect size and test of heterogeneity (random effects model).
Meta-regression
A series of meta-regressions detected a non-linear association between altitude studies and effect sizes. The model comparison results are presented in Table 6. In the log-likelihood ratio test, the quadratic model offered a significantly better fit for anxiety (Chi2 = 5.753, p = 0.016), depression (Chi2 = 9.040, p = 0.003), and confusion (Chi2 = 4.180, p = 0.041). Similarly, in AIC model selection, quadratic models for anxiety, depression, and confusion carried 62, 83, and 47%, respectively, of predictive power provided by the full set of models. Regarding physiological relaxation, a cubic association was noted for diastolic blood pressure (Chi2 = 6.447, p = 0.011, AICc weight = 44%), systolic blood pressure (Chi2 = 3.731, p = 0.005, AICc weight = 17%), and heart rate (Chi2 = 7.239, p = 0.007, AICc weight = 65%). Fitted meta-regression plots and test statistics are presented in Table 7.
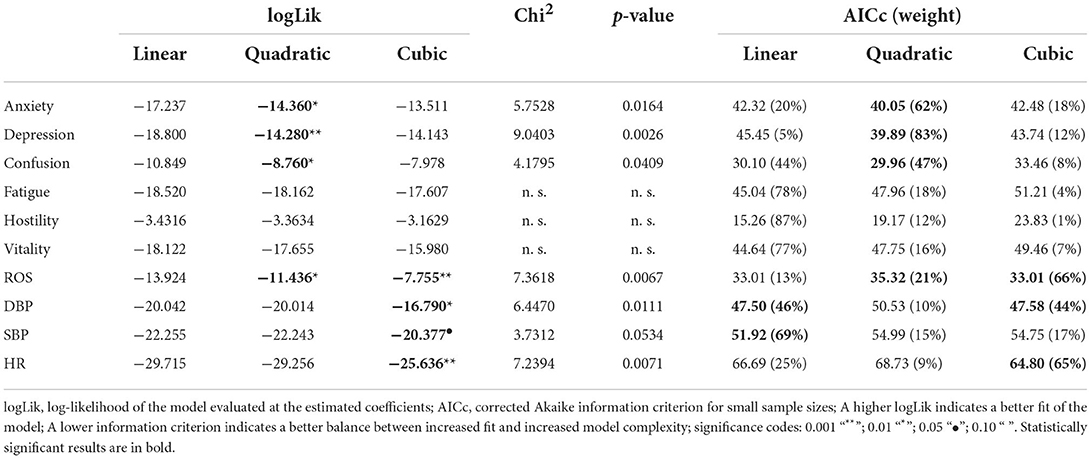
Table 6. Comparison of the models in terms of log likelihoods and information criteria.

Table 7. Fitted meta-regression plots for three different models.
We identified the influence of altitude on the effect size of studies captured by the QM index. Regarding emotional restoration, a significant quadratic association between altitude and alleviation of negative emotion was observed. Effect size (SMD) for anxiety (R2 = 31.41%, QM = 6.851, p = 0.033), depression (R2 = 39.41%, QM = 9.732, p = 0.008), and confusion (R2 = 31.10%, QM = 4.925, p = 0.085) had a significant positive quadratic association with altitude. The model estimated the regression weights of quadratic terms to be 0.0004, 0.0004, and 0.0003 for anxiety, depression, and confusion, respectively, which are highly significant (p < 0.001). Moreover, estimates of regression weight for linear terms of altitude were significant [p < 0.01 (Table 7)]. According to the equation model and its graphical depiction, the amount of alleviation of negative emotions generally increased with altitude, till an altitude of ~600–900 m. After this point, altitude increase predicted a decrease in alleviation efficacy. In the quadratic equation, altitude clarifies ~31–39% of the variance in effect size. The effect size of ROS– an indicator of restorative experience–revealed a significant positive linear association (R2 = 31.10%, QM = 4.925, p = 0.085), although with a limited altitude ranging from 11 to 223 m. Regarding physiological relaxation, a cubic association was found to be significant in diastolic blood pressure (R2 = 48.90%, QM = 12.250, p = 0.007) and heart rate (R2 = 23.58%, QM = 9.715, p = 0.021).
Alongside altitude, other study-level factors were dummy-coded, and an independent meta-ANOVA or meta-regression was performed. Accordingly, seasonal covariates were identified and included as control variables (Table 8). Subsequently, a substantial quadratic association was found between altitude and alleviating effect on anxiety (adjusted R2 = 96.79%, QM = 70.414, p < 0.000), depression (adjusted R2 = 98.78%, QM = 95.348, p < 0.000), fatigue (adjusted R2 = 64.74%, QM = 29.251, p < 0.000). The quadratic terms were found to be significant predictors of effect size on alleviation of anxiety (β = 0.0004, p = 0.001), depression (β = 0.0006, p < 0.000), fatigue (β = 0.0009, p = 0.014). Additionally, the linear quadratic terms were found to be significant predictors of effect size on alleviation of anxiety (β = −0.0589, p < 0.000), depression (β = −0.0980, p < 0.000), and fatigue (β = −0.1682, p = 0.007). The linear association between altitude and ROS was more substantial after inclusion of seasonal covariates (adjusted R2 = 70.67%, QM = 37.416, p < 0.000) and the linear term of altitude with a regression weight 0.0106 (p = 0.013). Additionally, diastolic blood pressure demonstrated significant quadratic association with altitude after the inclusion of seasonal covariates (adjusted R2 = 32.83%, QM = 15.245, p = 0.009), and regression weights on quadratic (β = −0.0003, p = 0.016) and linear (β = 0.0432, p = 0.0012) terms were significant.
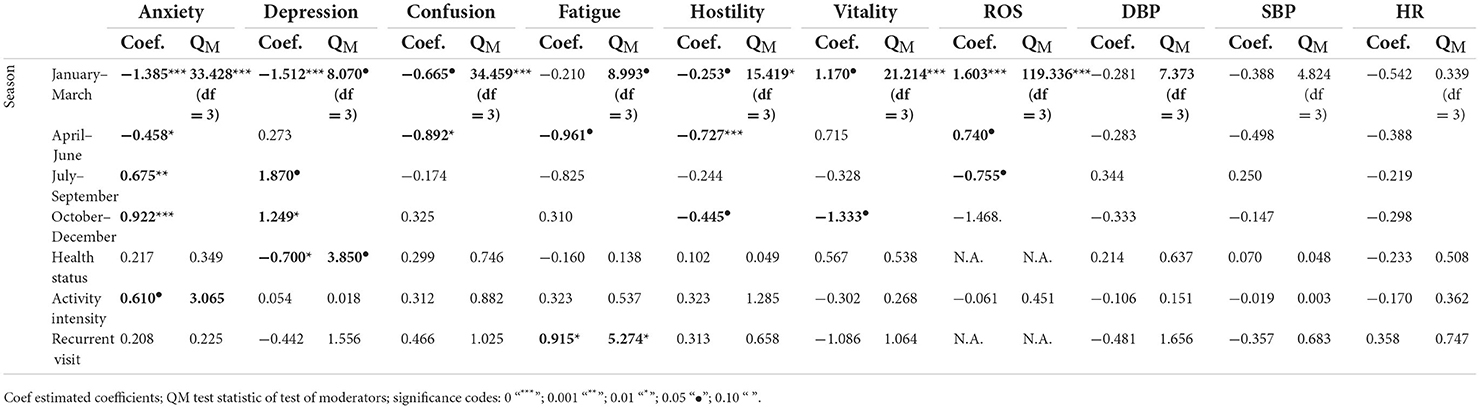
Table 8. Meta-regression results for binary covariates.
Furthermore, we conducted an additional analysis for studies reporting physical variables possibly related to the altitudinal condition. Table 9 reveals that the thermal index (THI) and illuminance (lx) levels were significantly associated with the effect size of psychological restoration, suggesting that heat and light conditions are potential effect modifiers. Additionally, we found that the intensity of physical activity was significantly associated with the effect size of anxiety relief.

Table 9. Meta-regression results for physical variable.
Sensitivity analysis and publication bias assessment
We investigated the influence of individual observations on effect estimation using rstudent, diffits, Cook's D, covratio, τ2, qresid, hat, and dfbetas values. Accordingly, except for hostility and heart rate, for which influential observations were found, most psycho-physiological effect domains were considered to not include influential observations that significantly altered the effect estimate (Supplemental Figures 11–20). Funnel plots indicated the risk of publication bias for the studies investigating depression, hostility, vitality, restorative experience, systolic blood pressure, and heart rate, with significant results of Egger's test (Supplemental Figure 21). Publication bias for studies examining anxiety (t = −1.54, p = 0.145) and fatigue (t = −0.34, p = 0.736) were almost negligible. Moderate publication bias was identified for studies on confusion (t = 2.05, p = 0.063) and diastolic blood pressure (t = −2.11, p = 0.078). The magnitude of Egger's test was consistent or declined after excluding studies at “high” risk of bias from the analysis of anxiety, fatigue, and diastolic and systolic blood pressure. For depression and heart rate, the publication bias persisted even after the elimination of studies with a “high” risk of bias (Supplemental Figure 22).
Certainty of evidence
The result of the GRADE assessment and summary of the findings are presented in Table 10. Overall, when all studies were considered, the evidence for an association between altitude and anxiety relief was at moderate-certainty, whereas the evidence for depression, fatigue, and diastolic blood pressure was at low-certainty. After excluding studies at “high” risk of bias, we found evidence of moderate- to high-certainty suggesting altitudinal influence on alleviation of anxiety, fatigue, and diastolic blood pressure. We assessed the certainty of evidence by considering five criteria: risk of bias, inconsistency, indirectness, imprecision, and publication bias. The risk of bias was of concern in analyses of all studies for anxiety, depression, fatigue, and diastolic blood pressure owing to studies rated at high risk of bias. Inconsistency was of concern for anxiety, depression, and fatigue owing to large heterogeneity across studies. However, concerns of inconsistency decreased for fatigue after the elimination of studies with a “high” risk of bias. There were no major issues due to indirectness, except for diastolic blood pressure. Since samples in the high-altitude settings were typically obtained from populations with cardiovascular issues, the physiological impacts may have been overestimated. Therefore, we assessed the serious indirectness for diastolic blood pressure, which may not accurately reflect the physiological outcomes of the general population at high altitude settings. Imprecision was assessed as of concern in analyses of all studies for anxiety, depression, fatigue, and diastolic blood pressure owing to few cases or small sample sizes. In all scenarios, we upgraded the evidence because of the presence of altitude-effect size association. Similarly, we upgraded the evidence level in case of large effects.
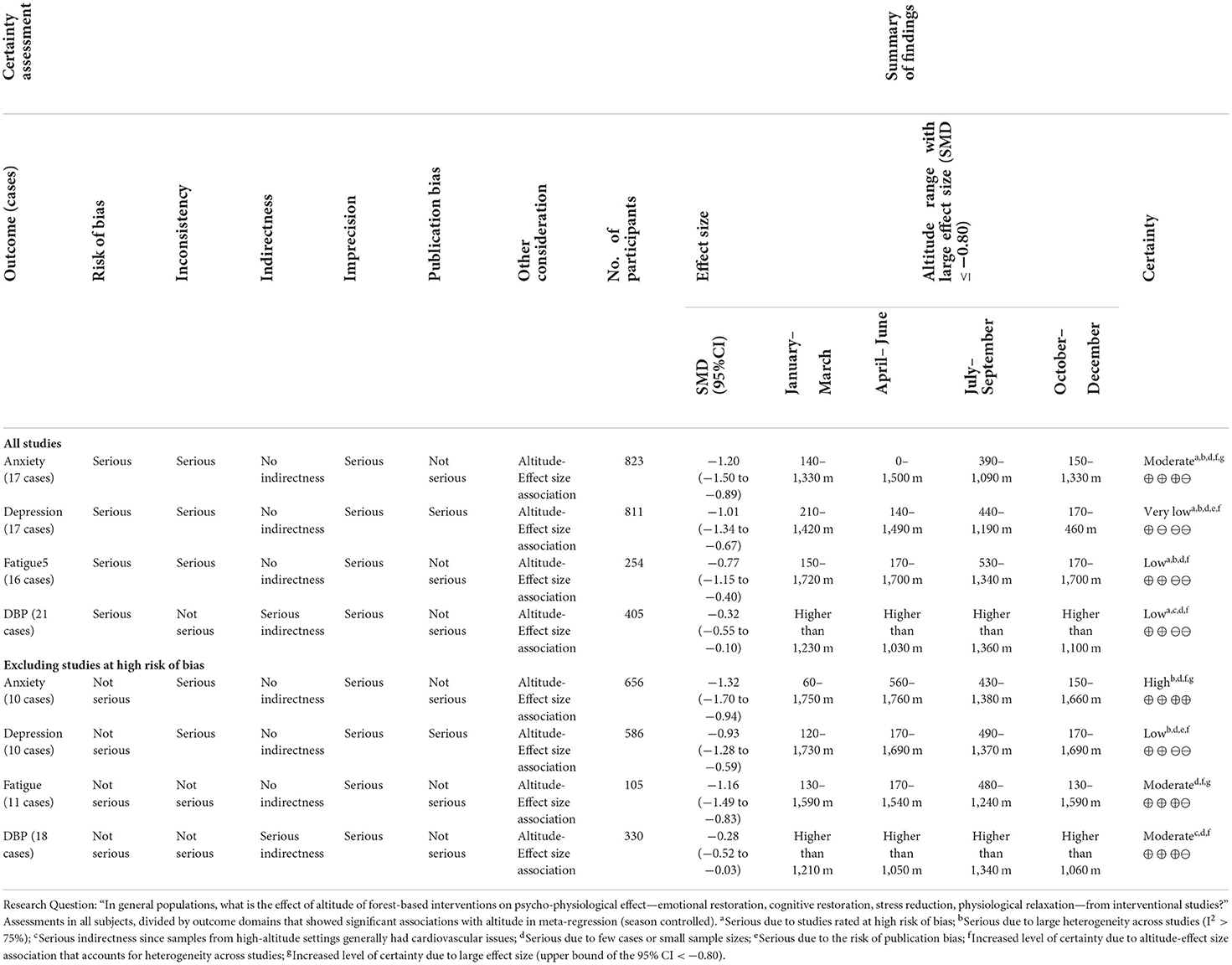
Table 10. Summary of findings table.
Discussion
Recently, forest-based interventions are recognized as an alternative therapy for disease prevention and public health improvement in several countries. It is critical to identify and describe the potentially effective candidate environments for improving health outcomes for forest-based interventions to be a reliable upstream healthcare approach. Therefore, our review began with the aforementioned PICO question. Accordingly, we aimed to provide an up-to-date summary of evidence that would benefit forest managers, practitioners, and planners who wish to choose suitable forest environments with the appropriate conditions to promote visitor health.
Overall, we found that altitude was significantly associated with alleviation of negative emotions and increase in physiological relaxation. Regarding negative emotions, anxiety, depression, confusion, and fatigue had a significant positive quadratic association with altitude, which implied that the alleviation of negative emotion concurrently increased with altitude up to a certain point, and subsequently, the efficacy declined as the altitude increased thereafter. After summing up a series of meta-regression results, we found that the peak of the regression curve was generally between 600 and 900 m. Conversely, regarding physiological relaxation, diastolic blood pressure demonstrated a significant negative non-linear association with altitude, which suggested that blood pressure-lowering effects tend to become apparent when the altitude of forest settings is high. Moreover, these associations were significant even after controlling for seasonal covariates and became apparent after excluding studies of low methodological quality. Consequently, we calculated the altitude range for large effect sizes based on the evidence in this review with moderate to high certainty. The effect size of anxiety relief and fatigue relief was estimated to be large enough between 560–1,380 and 490–1,240 m, respectively, for all seasons. Additionally, the diastolic blood pressure-lowering effect was predicted to be large enough when the forest-based intervention took place at an altitude of at least 1,050 m.
One intriguing aspect of our findings was that different association patterns emerged between psychological and physiological outcomes. Psychological benefits in environments with natural factors are widely reported from lowland greenspaces to highlands (131–135), and several studies have suggested a altitudinal effect on mood, emotion, cognitive function and behavior (136–140). Spending time at high altitudes reportedly has physiological benefits (141–150) and previous studies adopted outdoor settings >1,500 m to observe apparent changes in pulmonary, cardiac, circulatory, metabolic, and inflammatory outcomes (141, 145, 151, 152). There are multiple potential mechanisms linking altitude with psychophysiological responses, and the observed difference is possibly consequence of the varied altitude-related mechanisms involved in psychological and physiological restoration. Increases in altitude are associated with lower atmospheric pressure, oxygen partial pressure, humidity, and temperature, which could alter metabolic and neuronal activity as a compensatory response of body (153–156). Regarding psychological responses, high altitude exposure is associated with hypobaric hypoxia which alters neurotransmitter function (157, 158), modifies brain bioenergetics (156, 159–161), and changes efficiency of serotonin production (139, 162), all of which have an impact on mood (140, 163–165) and other psychiatric problems (137–139, 166). Regarding the physiological responses, high altitude exposure is also associated with distinctive mountain climate that induces adaptive changes in an individual's metabolic processes (167–173). Short-term intermittent exposure to high altitude has been reported to lower the risk of cardiovascular disease (167, 174), hypertension (168, 174, 175), and metabolic syndrome (155, 175, 176). Relatively extensive studies have been conducted on the molecular mechanisms underlying cellular and organ responses to high-altitude environments. Individual-level psychophysiological reactions, on the other hand, are more complicated and involve interactions between divergent pathways. Therefore, further investigation is needed on the psycho-physiological mechanisms of individuals in natural settings at various altitudes.
Moreover, several recent studies suggest a synergistic interaction between physical activity and the environment at various altitudes (166, 177–179). Physical activity is well-recognized as an effective health-promoting tool, and several studies have shown that physical activity in a natural environment provides a more consistent and powerful effect in improving mood and alleviating psychological stress (22, 177, 180–183). Recently, research on the optimal dose for the intensity and duration of physical activity (184), environmental factors (177, 185), and the optimal combination of physical activity and altitude (166, 178, 179) has been conducted.
Another remarkable finding was the seasonal variation in the altitude range, which is expected to have large effect sizes. Previous studies have outlined the meteorological changes in physiological altitude, and physiological responses at various altitudes are often simulated by adjusting atmospheric pressure and oxygen partial pressure (163, 168, 171–174, 178, 186). According to Millet and Devec (187), physiological altitude varies by up to 250 m per day and up to 500 m per year due to potential changes in barometric pressure even at the same point. In the future, formulating more comprehensive guidelines that account for seasonal variations by repeatedly evaluating the efficacy of forest-based interventions for different seasons may be possible. Recently, a investigations along similar lines have already been initiated (105, 188–190).
Notably, the minimum altitude for large effects tended to be higher from July to September compared with the other months. This may be because the areas where the studies were conducted typically experience summer between July and September. Based on the Köppen-Geiger climate classification for each study site (191), all regions have a distinct four-season pattern with the highest temperatures between June and September. In this context, meteorological factors (186, 192) possibly have contributed to the higher elevation range from July to September. It can also be influenced by other potential variables in the ambient environment.
Several published studies have demonstrated that physiological, biochemical, and perceptual changes with altitude were mainly due to the ambient environment (122, 144, 148, 193–195). There have been suggestions on altitude-related elements and their physiological effects; namely, atmospheric pressure (143, 144, 147, 149, 152, 195, 196), air oxygen concentration (143, 146, 149, 194), negative ions (122, 143, 144, 147, 149, 152, 193, 194, 196–198), absence of pollutants or allergens (144, 149, 152), solar radiation and UVB intensity (143, 144, 149, 199), temperature (143, 144, 149, 196), and relative humidity (143, 149, 196). Several factors, which may vary with altitude, have been reported as mediators of psychological restoration; namely, visually perceivable natural components (2, 43, 54, 55, 58, 59, 68, 71, 133), forest structure and understory vegetation (2, 45, 55, 68–71, 75), microclimate and thermal comforts (55, 79, 83, 131, 132, 135, 200), in-forest light conditions (54, 201, 202), airborne substances (28, 203–205), and pollutant concentrations (131, 132, 135). Thus, future studies should perform multi-faceted environmental measurements in conjunction with forest-based interventions to elucidate the underlying mechanisms or causal variables of the altitudinal effects. This will provide robust and credible evidence of the ideal delivery mechanisms to decision-makers in charge of forest-based initiatives.
To the best of our knowledge, the effects of altitude and physical factors remain largely unexplored in the literature on nature-based interventions. In this review, we have primarily focused on altitude because it is a simple and accessible indicator of the in-forest ambient environment. We have assumed altitude to be an effect modifier of the psychophysiological effects of forest-based intervention and summarized data on the magnitude and shape of the association. Our findings are significant because they clarify the link between altitude and health benefits of forest exposure. The identified associations may be considered to maximize the health advantages of forest-based interventions.
Our study has some limitations. First, our findings are observational. We have provided a quantitative summary of all available evidence via meta-analysis; however, we have not provided additional data to test the capability of the regression models in predicting unseen data. Nevertheless, our findings can identify potentially significant predictors and be used to generate hypotheses for future verification studies. Second, there is a risk of overestimating physiological effects in high-altitude conditions. Regarding interventions which investigated physiological effects, most interventions in low-altitude settings have carried out in urban park or urban forest. Moreover, most interventions in high-altitude settings have involved participants with cardiovascular disease or symptoms. Previous studies have noted that these participants frequently exhibited a greater physiological reaction to a given intervention (206, 207). Further investigations of other representative populations in high-altitude environments to derive accurate estimates are needed. Third, stress-related results and other biomarkers could not be analyzed owing to the limited number of studies. Therefore, further studies examining the stress-reducing effects of forest-based interventions, along with descriptions of the forest environment are necessary. Fourth, most of the included studies were rated as “moderate” to “high” risk of bias owing to the absence of concealment of random allocation and lack of participant blinding. Forest-based interventions are may inevitably have a higher risk of bias regarding random assignment and outcome measurement. These essentially require participants to visit a forest environment or participate in a directed program; thus, assignment concealment and participant blinding are rendered more difficult and increase the risk of bias during randomization. Regarding self-reported measurements, lack of participant blinding may be a major contributor to a higher risk of bias in outcome measures. To manage this, Bratman et al. (106) assigned an unrelated task (i.e., taking pictures) to disguise the purpose of the intervention, and Bielinis et al. (105) explained the study intent after the experiment. Additionally, more than half of the included studies did not provide a detailed randomization process and pre-registered analysis plan. Thus, future investigations should utilize trial registry platforms and sophisticated randomization methods to improve the quality of evidence (15, 208).
Conclusion
This review and meta-analysis explored the effect of altitude on the health benefits of forest exposures. Overall, we found significant non-linear associations between altitude and the magnitude of health effects. Based on the meta-regression results, we have approximated altitude ranges for psychological and physiological restoration with large effect sizes. We observed the different association patterns between altitude and psychological and physiological effects. We also identified the seasonal variation in altitude range for large effect sizes. We discussed the potential mechanisms involves in altitudinal effects shown in our findings. Recent research in nature-based interventions and preventive medicine has taken a more systematic approach, including examining environmental and activity conditions to estimate the optimal dose of nature to maximize therapeutic effectiveness. Despite some limitations, these findings supplement the available evidence on selecting nature environment for health improvement initiatives. Further investigative studies examining the multi-faceted aspects of environmental factors are needed to advance and implement forest-based interventions beyond research contexts.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
EK: conceptualization, formal analysis, investigation, methodology, project administration, supervision, visualization, writing—original draft, and writing—review and editing. SP: formal analysis, methodology, visualization, writing—original draft, and writing—review and editing. SK: investigation, writing—original draft, and writing—review and editing. YC: investigation, writing—original draft, writing—review and editing, and methodology. JC: conceptualization, project administration, supervision, writing—original draft, writing—review and editing, and methodology. GK: formal analysis, investigation, methodology, writing—original draft, and writing—review and editing. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1021618/full#supplementary-material
References
1. Zupancic T, Kingsley M, Jason T, Macfarlane R. Green City: Why Nature Matters to Health: An Evidence Review. Toronto, ON: Toronto Public Health (2013). Available online at: http://www.toronto.ca/legdocs/mmis/2015/hl/bgrd/backgroundfile-83421.pdf (accessed March 27, 2022).
2. Kim E, Park S, Kim S, Choi Y, Cho J, Cho S-i, et al. Can different forest structures lead to different levels of therapeutic effects? A systematic review and meta-analysis. Healthcare. (2021) 9:1427. doi: 10.3390/healthcare9111427
3. Ulrich RS, Simons RF, Losito BD, Fiorito E, Miles MA, Zelson M. Stress recovery during exposure to natural and urban environments. J Environ Psychol. (1991) 11:201–30. doi: 10.1016/S0272-4944(05)80184-7
4. Parsons R. The potential influences of environmental perception on human health. J Environ Psychol. (1991) 11:1–23. doi: 10.1016/S0272-4944(05)80002-7
5. Brannon L, Feist J, Updegraff JA. Health Psychology: An Introduction to Behavior and Health. Boston, MA: Cengage Learning (2013). p. 544.
6. Meijman TF, Mulder G. Psychological aspects of workload. In: A Handbook of Work and Organizational Psychology. London: Psychology Press (2013). p. 15–44.
7. Hartig T. Three steps to understanding restorative environments as health resources. In: Open Space: People Space. London: Taylor & Francis (2007).
8. Kaplan S. The restorative benefits of nature: toward an integrative framework. J Environ Psychol. (1995) 15:169–82. doi: 10.1016/0272-4944(95)90001-2
9. Kaplan R, Kaplan S. The Experience of Nature: A Psychological Perspective. Cambridge: Cambridge University Press (1989).
10. Ulrich RS. Aesthetic and affective response to natural environment. In: Behavior and the Natural Environment. Boston, MA: Springer (1983). p. 85–125. doi: 10.1007/978-1-4613-3539-9_4
11. McEwen BS. Stress, adaptation, and disease: allostasis and allostatic load. Ann N Y Acad Sci. (1998) 840:33–44. doi: 10.1111/j.1749-6632.1998.tb09546.x
12. Hartig T, Böök A, Garvill J, Olsson T, Gärling T. Environmental influences on psychological restoration. Scand J Psychol. (1996) 37:378–93. doi: 10.1111/j.1467-9450.1996.tb00670.x
13. Astell-Burt T, Mitchell R, Hartig T. The association between green space and mental health varies across the lifecourse. A longitudinal study. J Epidemiol Community Health. (2014) 68:578–83. doi: 10.1136/jech-2013-203767
14. Corazon SS, Sidenius U, Poulsen DV, Gramkow MC, Stigsdotter UK. Psycho-physiological stress recovery in outdoor nature-based interventions: a systematic review of the past eight years of research. Int J Environ Res Public Health. (2019) 16:1711. doi: 10.3390/ijerph16101711
15. Park S, Kim E, Kim G, Kim S, Choi Y, Paek D. What activities in forests are beneficial for human health? A systematic review. Int J Environ Res Public Health. (2022) 19:2692. doi: 10.3390/ijerph19052692
16. Nilsson K, Sangster M, Konijnendijk CC. Forests, trees and human health and well-being: introduction. In: Forests, Trees and Human Health. Berlin: Springer (2011). p. 1–19. doi: 10.1007/978-90-481-9806-1_1
17. van den Berg M, Wendel-Vos W, van Poppel M, Kemper H, van Mechelen W, Maas J. Health benefits of green spaces in the living environment: a systematic review of epidemiological studies. Urban For Urban Green. (2015) 14:806–16. doi: 10.1016/j.ufug.2015.07.008
18. Gascon M, Triguero-Mas M, Martínez D, Dadvand P, Forns J, Plasència A, et al. Mental health benefits of long-term exposure to residential green and blue spaces: a systematic review. Int J Environ Res Public Health. (2015) 12:4354–79. doi: 10.3390/ijerph120404354
19. White MP, Alcock I, Wheeler BW, Depledge MH. Would you be happier living in a greener urban area? A fixed-effects analysis of panel data. Psychol Sci. (2013) 24:920–8. doi: 10.1177/0956797612464659
20. Stigsdotter UK, Palsdottir AM, Burls A, Chermaz A, Ferrini F, Grahn P. Nature-Based therapeutic interventions. In:Nilsson K, Sangster M, Gallis C, Hartig T, de Vries S, Seeland K, et al., editors. Forests, Trees and Human Health. Dordrecht: Springer (2011). p. 309–42. doi: 10.1007/978-90-481-9806-1_11
21. Shanahan DF, Astell–Burt T, Barber EA, Brymer E, Cox DTC, Dean J, et al. Nature–Based interventions for improving health and wellbeing: the purpose, the people and the outcomes. Sports. (2019) 7:141. doi: 10.3390/sports7060141
22. Koselka EPD, Weidner LC, Minasov A, Berman MG, Leonard WR, Santoso MV, et al. Walking green: developing an evidence base for nature prescriptions. Int J Environ Res Public Health. (2019) 16:4338. doi: 10.3390/ijerph16224338
23. WHO. Urban Green Space Interventions and Health: A Review of Impacts and Effectiveness. Copenhagen: WHO Regional Office for Europe (2017).
24. WHO. Control of Noncommunicable Diseases in the European Region: A Progress Report. Copenhagen: World Health Organization (2014).
25. Croucher K, Myers L, Bretherton J. The Links between Greenspace and Health: A Critical Literature Review. York: University of York (2007).
26. Van den Berg M, van Poppel M, van Kamp I, Andrusaityte S, Balseviciene B, Cirach M, et al. Visiting green space is associated with mental health and vitality: a cross-sectional study in four European cities. Health Place. (2016) 38:8–15. doi: 10.1016/j.healthplace.2016.01.003
27. Marušáková L, Sallmannshofer M, Kašpar J, Schwarz M, Tyrväinen L, Bauer N. Human health and sustainable forest management. In:Marusakova L, Sallmanshofer M, editors. Zvolen: FOREST EUROPE - Liaison Unit Bratislava (2019). p. 170.
28. Kotte D, Li Q, Shin WS, Michalsen A. International Handbook of Forest Therapy. Newcastle upon Tyne: Cambridge Scholars Publishing (2019).
29. FAO. Forests for Human Health and Well-Being – Strengthening the Forest–Health–Nutrition Nexus. Rome: Forestry Working Paper No 18 (2020). 84 p.
30. Bricker KS, Brownlee MTJ, Dustin DL. Healthy parks, healthy people. J Park Recreat Admin. (2016) 34:1–4. Available online at: https://www.proquest.com/scholarly-journals/introduction-healthy-parks-people-special-issue/docview/1795755123/se-2 (accessed July 24, 2022).
31. Kotera Y, Richardson M, Sheffield D. Effects of shinrin-yoku (forest bathing) and nature therapy on mental health: a systematic review and meta-analysis. Int J Ment Health Addict. (2022) 20:337–61. doi: 10.1007/s11469-020-00363-4
32. Hansen MM, Jones R, Tocchini K. Shinrin-Yoku (forest bathing) and nature therapy: a state-of-the-art review. Int J Environ Res Public Health. (2017) 14:851. doi: 10.3390/ijerph14080851
33. Shin WS, Yeoun PS, Yoo RW, Shin CS. Forest experience and psychological health benefits: the state of the art and future prospect in Korea. Environ Health Prev Med. (2010) 15:38–47. doi: 10.1007/s12199-009-0114-9
34. Pyky R, Neuvonen M, Kangas K, Ojala A, Lanki T, Borodulin K, et al. Individual and environmental factors associated with green exercise in urban and suburban areas. Health Place. (2019) 55:20–8. doi: 10.1016/j.healthplace.2018.11.001
35. Polku M. Liiku Ja Huilaa Keski-Suomessa 2017–2047 [Move and Rest in Central Finland 2017–2047]. (2020). Available online at: www.meijanpolku.fi (accessed July 10, 2022).
36. ten Brink P, Mutafoglu K, Schweitzer J-P, Kettunen M, Twigger-Ross C, Baker J, et al. The Health and Social Benefits of Nature and Biodiversity Protection. A Report for the European Commission (ENV B 3/ETU/2014/0039). London; Brussels: Institute for European Environmental Policy (2016).
37. Maller C, Townsend M, Leger L, Henderson-Wilson C, Pryor A, Prosser L, et al. Healthy Parks, Healthy People: The Health Benefits of Contact with Nature in a Park Context-a Review of Relevant Literature, 2nd Edn. Melbourne, VIC: Parks Victoria (2008).
38. Meyer K, Bürger-Arndt R. How forests foster human health–present state of research-based knowledge (in the field of forests and human health). Int For Rev. (2014) 16:421–46. doi: 10.1505/146554814813484103
39. Stigsdotter UK, Sidenius U, Grahn P. From research to practice: operationalisation of the eight perceived sensory dimensions into a health-promoting design tool. Alam Cipta. (2020) 13:57–70.
40. Markevych I, Schoierer J, Hartig T, Chudnovsky A, Hystad P, Dzhambov AM, et al. Exploring pathways linking greenspace to health: theoretical and methodological guidance. Environ Res. (2017) 158:301–17. doi: 10.1016/j.envres.2017.06.028
41. Kuo FE, Sullivan WC. Environment and crime in the inner city: does vegetation reduce crime? Environ Behav. (2001) 33:343–67. doi: 10.1177/00139160121973025
42. Kuo FE, Sullivan WC, Coley RL, Brunson L. Fertile ground for community: inner-city neighborhood common spaces. Am J Commun Psychol. (1998) 26:823–51. doi: 10.1023/A:1022294028903
43. Jiang B, Chang C-Y, Sullivan WC. A dose of nature: tree cover, stress reduction, and gender differences. Landsc Urban Plan. (2014) 132:26–36. doi: 10.1016/j.landurbplan.2014.08.005
44. Lis A, Iwankowski P. Why is dense vegetation in city parks unpopular? The mediative role of sense of privacy and safety. Urban For Urban Green. (2021) 59:126988. doi: 10.1016/j.ufug.2021.126988
45. Staats H, Gatersleben B, Hartig T. Change in mood as a function of environmental design: arousal and pleasure on a simulated forest hike. J Environ Psychol. (1997) 17:283–300. doi: 10.1006/jevp.1997.0069
46. Herzog TR, Chernick KK. Tranquility and danger in urban and natural settings. J Environ Psychol. (2000) 20:29–39. doi: 10.1006/jevp.1999.0151
47. Gao T, Zhang T, Zhu L, Gao Y, Qiu L. Exploring psychophysiological restoration and individual preference in the different environments based on virtual reality. Int J Environ Res Public Health. (2019) 16:3102. doi: 10.3390/ijerph16173102
48. Tabrizian P, Baran PK, Smith WR, Meentemeyer RK. Exploring perceived restoration potential of urban green enclosure through immersive virtual environments. J Environ Psychol. (2018) 55:99–109. doi: 10.1016/j.jenvp.2018.01.001
49. Hofmann M, Gerstenberg T, Gillner S. Predicting tree preferences from visible tree characteristics. Euro J For Res. (2017) 136:421–32. doi: 10.1007/s10342-017-1042-7
50. Milligan C, Bingley A. Restorative places or scary spaces? The impact of woodland on the mental well-being of young adults. Health Place. (2007) 13:799–811. doi: 10.1016/j.healthplace.2007.01.005
51. Gundersen VS, Frivold LH. Public preferences for forest structures: a review of quantitative surveys from Finland, Norway and Sweden. Urban For Urban Green. (2008) 7:241–58. doi: 10.1016/j.ufug.2008.05.001
52. Van der Jagt APN, Craig T, Anable J, Brewer MJ, Pearson DG. Unearthing the picturesque: the validity of the preference matrix as a measure of landscape aesthetics. Landsc Urban Plan. (2014) 124:1–13. doi: 10.1016/j.landurbplan.2013.12.006
53. Nielsen AB, Heyman E, Richnau G. Liked, disliked and unseen forest attributes: relation to modes of viewing and cognitive constructs. J Environ Manage. (2012) 113:456–66. doi: 10.1016/j.jenvman.2012.10.014
54. Gao Y, Zhang T, Sasaki K, Uehara M, Jin Y, Qin L. The spatial cognition of a forest landscape and its relationship with tourist viewing intention in different walking passage stages. Urban For Urban Green. (2021) 58:126975. doi: 10.1016/j.ufug.2020.126975
55. Ebenberger M, Arnberger A. Exploring visual preferences for structural attributes of urban forest stands for restoration and heat relief. Urban For Urban Green. (2019) 41:272–82. doi: 10.1016/j.ufug.2019.04.011
56. Kuper R. Restorative potential, fascination, and extent for designed digital landscape models. Urban For Urban Green. (2017) 28:118–30. doi: 10.1016/j.ufug.2017.10.002
57. Stamps AE. Mystery, complexity, legibility and coherence: a meta-analysis. J Environ Psychol. (2004) 24:1–16. doi: 10.1016/S0272-4944(03)00023-9
58. Gao Y, Zhang T, Zhang W, Meng H, Zhang Z. Research on visual behavior characteristics and cognitive evaluation of different types of forest landscape spaces. Urban For Urban Green. (2020) 54:126788. doi: 10.1016/j.ufug.2020.126788
59. Deng L, Li X, Luo H, Fu E-K, Ma J, Sun L-X, et al. Empirical study of landscape types, landscape elements and landscape components of the urban park promoting physiological and psychological restoration. Urban For Urban Green. (2020) 48:126488. doi: 10.1016/j.ufug.2019.126488
60. Lee KJ, Hur J, Yang K-S, Lee M-K, Lee S-J. Acute biophysical responses and psychological effects of different types of forests in patients with metabolic syndrome. Environ Behav. (2018) 50:298–323. doi: 10.1177/0013916517700957
61. Sonntag-Öström E, Nordin M, Lundell Y, Dolling A, Wiklund U, Karlsson M, et al. Restorative effects of visits to urban and forest environments in patients with exhaustion disorder. Urban For Urban Green. (2014) 13:344–54. doi: 10.1016/j.ufug.2013.12.007
62. Sonntag-Ostrom E, Stenlund T, Nordin M, Lundell Y, Ahlgren C, Fjellman-Wiklund A, et al. “Nature's effect on my mind” - patients' qualitative experiences of a forest-based rehabilitation programme. Urban For Urban Green. (2015) 14:607–14. doi: 10.1016/j.ufug.2015.06.002
63. Zhou C, Yan L, Yu L, Wei H, Guan H, Shang C, et al. Effect of short-term forest bathing in urban parks on perceived anxiety of young-adults: a pilot study in Guiyang, southwest China. Chin Geograp Sci. (2019) 29:139–50. doi: 10.1007/s11769-018-0987-x
64. Simkin J, Ojala A, Tyrväinen L. Restorative effects of mature and young commercial forests, pristine old-growth forest and urban recreation forest-a field experiment. Urban For Urban Green. (2020) 48:126567. doi: 10.1016/j.ufug.2019.126567
65. Tyrväinen L, Ojala A, Korpela K, Lanki T, Tsunetsugu Y, Kagawa T. The influence of urban green environments on stress relief measures: a field experiment. J Environ Psychol. (2014) 38:1–9. doi: 10.1016/j.jenvp.2013.12.005
66. Wilkie S, Clouston L. Environment preference and environment type congruence: effects on perceived restoration potential and restoration outcomes. Urban For Urban Green. (2015) 14:368–76. doi: 10.1016/j.ufug.2015.03.002
67. Huang Q, Yang M, Jane H-a, Li S, Bauer N. Trees, grass, or concrete? The effects of different types of environments on stress reduction. Landsc Urban Plan. (2020) 193:103654. doi: 10.1016/j.landurbplan.2019.103654
68. Arnberger A, Eder R, Allex B, Ebenberger M, Hutter H-P, Wallner P, et al. Health-Related effects of short stays at mountain meadows, a river and an urban site—results from a field experiment. Int J Environ Res Public Health. (2018) 15:2647. doi: 10.3390/ijerph15122647
69. Lin W, Chen Q, Zhang X, Tao J, Liu Z, Lyu B, et al. Effects of different bamboo forest spaces on psychophysiological stress and spatial scale evaluation. Forests. (2020) 11:616. doi: 10.3390/f11060616
70. An B-Y, Wang D, Liu X-J, Guan H-M, Wei H-X, Ren Z-B. The effect of environmental factors in urban forests on blood pressure and heart rate in university students. J For Res. (2019) 24:27–34. doi: 10.1080/13416979.2018.1540144
71. Guan H, Wei H, He X, Ren Z, An B. The tree-species-specific effect of forest bathing on perceived anxiety alleviation of young-adults in urban forests. Ann For Res. (2017) 60:327–41. doi: 10.15287/afr.2017.897
72. Hussain RI, Walcher R, Eder R, Allex B, Wallner P, Hutter H-P, et al. Management of mountainous meadows associated with biodiversity attributes, perceived health benefits and cultural ecosystem services. Sci Rep. (2019) 9:14977. doi: 10.1038/s41598-019-51571-5
73. Lopez-Pousa S, Bassets Pages G, Monserrat-Vila S, de Gracia Blanco M, Hidalgo Colome J, Garre-Olmo J. Sense of well-being in patients with fibromyalgia: aerobic exercise program in a mature forest-a pilot study. Evid Based Complement Altern Med. (2015) 2015:61483. doi: 10.1155/2015/614783
74. Saito H, Horiuchi M, Takayama N, Fujiwara A. Effects of managed forest versus unmanaged forest on physiological restoration from a stress stimulus, and the relationship with individual traits. J For Res. (2019) 24:77–85. doi: 10.1080/13416979.2019.1586300
75. An KW, Kim EI, Joen KS, Setsu T. Effects of Forest Stand Density on Human's Physiophychological Changes. J Agri Syushu Univ. (2004) 49:283–91. doi: 10.5109/4588
76. Takayama N, Saito H, Fujiwara A, Horiuchi M. The effect of slight thinning of managed coniferous forest on landscape appreciation and psychological restoration. Prog Earth Planet Sci. (2017) 4:1–15. doi: 10.1186/s40645-017-0129-6
77. Takayama N, Fujiwara A, Saito H, Horiuchi M. Management effectiveness of a secondary coniferous forest for landscape appreciation and psychological restoration. Int J Environ Res Public Health. (2017) 14:800. doi: 10.3390/ijerph14070800
78. Martens D, Gutscher H, Bauer N. Walking in “wild” and “tended” urban forests: the impact on psychological well-being. J Environ Psychol. (2011) 31:36–44. doi: 10.1016/j.jenvp.2010.11.001
79. Park B-J, Furuya K, Kasetani T, Takayama N, Kagawa T, Miyazaki Y. Relationship between psychological responses and physical environments in forest settings. Landsc Urban Plan. (2011) 102:24–32. doi: 10.1016/j.landurbplan.2011.03.005
80. Son J-Y, Lane KJ, Lee J-T, Bell ML. Urban vegetation and heat-related mortality in seoul, Korea. Environ Res. (2016) 151:728–33. doi: 10.1016/j.envres.2016.09.001
81. Burkart K, Meier F, Schneider A, Breitner S, Canário P, Alcoforado MJ, et al. Modification of heat-related mortality in an elderly urban population by vegetation (urban green) and proximity to water (urban blue): evidence from Lisbon, Portugal. Environ Health Perspect. (2016) 124:927–34. doi: 10.1289/ehp.1409529
82. Salbitano F, Borelli S, Conigliaro M, Chen Y. Guidelines on Urban Peri-Urban Forestry. FAO Forestry Paper No. 178. Food Agriculture Organization of the United Nations (2016). Available online at: https://www.fao.org/3/i6210e/i6210e.pdf (accessed July 24, 2022).
83. Park BJ, Tsunetsugu Y, Kasetani T, Kagawa T, Miyazaki Y. The physiological effects of shinrin-yoku (taking in the forest atmosphere or forest bathing): evidence from field experiments in 24 forests across Japan. Environ Health Prev Med. (2010) 15:18–26. doi: 10.1007/s12199-009-0086-9
84. Forestry Culture and Recreation Act. Act No. 17421, 09, Jun, 2020, Partial Amendment. (2010). Available online at: https://Elaw.Klri.Re.Kr/Kor_Service/Lawview.Do?Lang=Eng&Hseq=54797 (accessed July 22, 2022).
85. Kim KW. A study on conceptual method for forest trail planning. J Korean Inst Forest Recreat. (2009) 13:11–24. doi: 10.34272/forest.2009.13.2.003
86. Park S. Characteristics and Health Effects of Forest Healing Properties, Vol. 15. Seoul: Korea Forest Service (2015). p. 1–81.
87. Santos CMdC, Pimenta CAdM, Nobre MRC. The pico strategy for the research question construction and evidence search. Rev Latino Am Enfermagem. (2007) 15:508–11. doi: 10.1590/S0104-11692007000300023
88. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The prisma 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
89. Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions. Chichester: John Wiley & Sons (2019). doi: 10.1002/9781119536604
90. Unger J. Comparisons of urban and rural bioclimatological conditions in the case of a central-European city. Int J Biometeorol. (1999) 43:139–44. doi: 10.1007/s004840050129
91. Morakinyo TE, Adegun OB, Balogun AA. The effect of vegetation on indoor and outdoor thermal comfort conditions: evidence from a microscale study of two similar urban buildings in akure, Nigeria. Indoor Built Environ. (2016) 25:603–17. doi: 10.1177/1420326X14562455
92. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:14898. doi: 10.1136/bmj.l4898
93. Sterne JAC, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. Robins-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. (2016) 355:i4919. doi: 10.1136/bmj.i4919
94. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. (2019) 22:153–60. doi: 10.1136/ebmental-2019-300117
95. Viechtbauer W. Conducting meta-analyses in r with the metafor package. J Stat Softw. (2010) 36:1–48. doi: 10.18637/jss.v036.i03
96. Cohen J. Statistical Power Analysis for the Behavioral Sciences New York, NY: Routledge (2013). doi: 10.4324/9780203771587
97. Langan D, Higgins JPT, Jackson D, Bowden J, Veroniki AA, Kontopantelis E, et al. A comparison of heterogeneity variance estimators in simulated random-effects meta-analyses. Res Synthes Methods. (2019) 10:83–98. doi: 10.1002/jrsm.1316
98. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
99. Desquilbet L, Mariotti F. Dose-Response analyses using restricted cubic spline functions in public health research. Stat Med. (2010) 29:1037–57. doi: 10.1002/sim.3841
100. Liu Q, Cook NR, Bergström A, Hsieh C-C. A two-stage hierarchical regression model for meta-analysis of epidemiologic nonlinear dose–response data. Comput Stat Data Anal. (2009) 53:4157–67. doi: 10.1016/j.csda.2009.05.001
101. Shim SR, Lee J. Dose-Response meta-analysis: application and practice using the R software. Epidemiol Health. (2019) 41:e2019006. doi: 10.4178/epih.e2019006
102. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
103. Atkins D, Eccles M, Flottorp S, Guyatt GH, Henry D, Hill S, et al. Systems for grading the quality of evidence and the strength of recommendations I: critical appraisal of existing approaches the grade working group. BMC Health Serv Res. (2004) 4:1–7. doi: 10.1186/1472-6963-4-38
104. Schünemann HJ, Higgins JPT, Vist GE, Glasziou P, Akl EA, Skoetz N, et al. Completing summary of findings' tables and grading the certainty of the evidence. Cochrane Handbook Syst Rev Intervent. (2019) 2:375–402. doi: 10.1002/9781119536604.ch14
105. Bielinis E, Łukowski A, Omelan A, Boiko S, Takayama N, Grebner DL. The effect of recreation in a snow-covered forest environment on the psychological wellbeing of young adults: Randomized controlled study. Forests. (2019) 10:827. doi: 10.3390/f10100827
106. Bratman GN, Daily GC, Levy BJ, Gross JJ. The benefits of nature experience: improved affect and cognition. Landsc Urban Plan. (2015) 138:41–50. doi: 10.1016/j.landurbplan.2015.02.005
107. Chun MH, Chang MC, Lee S-J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int J Neurosci. (2017) 127:199–203. doi: 10.3109/00207454.2016.1170015
108. de Brito JN, Pope ZC, Mitchell NR, Schneider IE, Larson JM, Horton TH, et al. The effect of green walking on heart rate variability: a pilot crossover study. Environ Res. (2020) 185:109408. doi: 10.1016/j.envres.2020.109408
109. Djernis D, O'Toole MS, Fjorback LO, Svenningsen H, Mehlsen MY, Stigsdotter UK, et al. A short mindfulness retreat for students to reduce stress and promote self-compassion: pilot randomised controlled trial exploring both an indoor and a natural outdoor retreat setting. Healthcare. (2021) 9:910. doi: 10.3390/healthcare9070910
110. Dolling A, Nilsson H, Lundell Y. Stress recovery in forest or handicraft environments – an intervention study. Urban For Urban Green. (2017) 27:162–72. doi: 10.1016/j.ufug.2017.07.006
111. Grazuleviciene R, Vencloviene J, Kubilius R, Grizas V, Dedele A, Grazulevicius T, et al. The effect of park and urban environments on coronary artery disease patients: a randomized trial. Biomed Res Int. (2015) 2015:403012. doi: 10.1155/2015/403012
112. Han J-W, Choi H, Jeon Y-H, Yoon C-H, Woo J-M, Kim W. The effects of forest therapy on coping with chronic widespread pain: physiological and psychological differences between participants in a forest therapy program and a control group. Int J Environ Res Public Health. (2016) 13:255. doi: 10.3390/ijerph13030255
113. Han K-T. The effect of nature and physical activity on emotions and attention while engaging in green exercise. Urban For Urban Green. (2017) 24:5–13. doi: 10.1016/j.ufug.2017.03.012
114. Harte JL, Eifert GH. The effects of running, environment, and attentional focus on athletes' catecholamine and cortisol levels and mood. Psychophysiology. (1995) 32:49–54. doi: 10.1111/j.1469-8986.1995.tb03405.x
115. Janeczko E, Bielinis E, Wójcik R, Woznicka M, Kedziora W, Lukowski A, et al. When urban environment is restorative: the effect of walking in suburbs and forests on psychological and physiological relaxation of young polish adults. Forests. (2020) 11:591. doi: 10.3390/f11050591
116. Lanki T, Siponen T, Ojala A, Korpela K, Pennanen A, Tiittanen P, et al. Acute effects of visits to urban green environments on cardiovascular physiology in women: a field experiment. Environ Res. (2017) 159:176–85. doi: 10.1016/j.envres.2017.07.039
117. Lee J-Y, Lee D-C. Cardiac and pulmonary benefits of forest walking versus city walking in elderly women: a randomised, controlled, open-label trial. Euro J Integrat Med. (2014) 6:5–11. doi: 10.1016/j.eujim.2013.10.006
118. Li Q, Kobayashi M, Kumeda S, Ochiai T, Miura T, Kagawa T, et al. Effects of forest bathing on cardiovascular and metabolic parameters in middle-aged males. Evid Based Complement Altern Med. (2016) 2016:2587381. doi: 10.1155/2016/2587381
119. Liu Q, Wang X, Liu J, An C, Liu Y, Fan X, et al. Physiological and psychological effects of nature experiences in different forests on young people. Forests. (2021) 12:1391. doi: 10.3390/f12101391
120. Mao G-X, Cao Y-B, Lan X-G, He Z-H, Chen Z-M, Wang Y-Z, et al. Therapeutic effect of forest bathing on human hypertension in the elderly. J Cardiol. (2012) 60:495–502. doi: 10.1016/j.jjcc.2012.08.003
121. Mao Gen X, Lan Xiao G, Cao Yong B, Chen Zhuo M, He Zhi H, Lv Yuan D, et al. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang province, China. Biomed Environ Sci. (2012) 25:317–24. doi: 10.3967/0895-3988.2012.03.010
122. Mao GX, Lan XG, Chen ZM, Chen SS, Wang JR, Wang SY, et al. The salutary influence of forest bathing on elderly patients with chronic heart failure. Int J Environ Res Public Health. (2017) 14:368. doi: 10.3390/ijerph14040368
123. Meyer K, Hey S, Buerger-Arndt R. Effects of walking through a forest on stress level physical and psychological measurements of well-being during a walk in a german mixed forest stand. Allgemeine Forst Und Jagdzeitung. (2016) 187:69–80. Available online at: http://www.jstor.org/stable/24310694
124. Morita E, Fukuda S, Nagano J, Hamajima N, Yamamoto H, Iwai Y, et al. Psychological effects of forest environments on healthy adults: shinrin-yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health. (2007) 121:54–63. doi: 10.1016/j.puhe.2006.05.024
125. Song C, Ikei H, Igarashi M, Miwa M, Takagaki M, Miyazaki Y. Physiological and psychological responses of young males during spring-time walks in urban parks. J Physiol Anthropol. (2014) 33:8. doi: 10.1186/1880-6805-33-8
126. Song C, Ikei H, Igarashi M, Takagaki M, Miyazaki Y. Physiological and psychological effects of a walk in urban parks in fall. Int J Environ Res Public Health. (2015) 12:14216–28. doi: 10.3390/ijerph121114216
127. Song C, Ikei H, Kobayashi M, Miura T, Taue M, Kagawa T, et al. Effect of forest walking on autonomic nervous system activity in middle-aged hypertensive individuals: a pilot study. Int J Environ Res Public Health. (2015) 12:2687–99. doi: 10.3390/ijerph120302687
128. Sung J, Woo J-M, Kim W, Lim S-K, Chung E-J. The effect of cognitive behavior therapy-based “forest therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin Exp Hypertens. (2012) 34:1–7. doi: 10.3109/10641963.2011.618195
129. Wang X, Zhou Q, Zhang M, Zhang Q. Exercise in the park or gym? The physiological and mental responses of obese people walking in different settings at different speeds: a parallel group randomized trial. Front Psychol. (2021) 12:728826. doi: 10.3389/fpsyg.2021.728826
130. Zeng C, Lyu B, Deng S, Yu Y, Li N, Lin W, et al. Benefits of a three-day bamboo forest therapy session on the physiological responses of university students. Int J Environ Res Public Health. (2020) 17:3238. doi: 10.3390/ijerph17093238
131. Hartig T, Mitchell R, De Vries S, Frumkin H. Nature and health. Ann Rev Public Health. (2014) 35:207–28. doi: 10.1146/annurev-publhealth-032013-182443
132. James P, Banay RF, Hart JE, Laden F. A review of the health benefits of greenness. Curr Epidemiol Rep. (2015) 2:131–42. doi: 10.1007/s40471-015-0043-7
133. Nguyen P-Y, Astell-Burt T, Rahimi-Ardabili H, Feng X. Green space quality and health: a systematic review. Int J Environ Res Public Health. (2021) 18:11028. doi: 10.3390/ijerph182111028
134. Stier-Jarmer M, Throner V, Kirschneck M, Immich G, Frisch D, Schuh A. The psychological and physical effects of forests on human health: a systematic review of systematic reviews and meta-analyses. Int J Environ Res Public Health. (2021) 18:1770. doi: 10.3390/ijerph18041770
135. Wolf KL, Lam ST, McKeen JK, Richardson GRA, van den Bosch M, Bardekjian AC. Urban trees and human health: a scoping review. Int J Environ Res Public Health. (2020) 17:4371. doi: 10.3390/ijerph17124371
136. Bahrke MS, Shukitt-Hale B. Effects of altitude on mood, behaviour and cognitive functioning. Sports Med. (1993) 16:97–125. doi: 10.2165/00007256-199316020-00003
137. Kious BM, Bakian A, Zhao J, Mickey B, Guille C, Renshaw P, et al. Altitude and risk of depression and anxiety: findings from the intern health study. Int Rev Psychiatry. (2019) 31:637–45. doi: 10.1080/09540261.2019.1586324
138. Ishikawa M, Yamanaka G, Yamamoto N, Nakaoka T, Okumiya K, Matsubayashi K, et al. Depression and altitude: cross-sectional community-based study among elderly high-altitude residents in the himalayan regions. Cult Med Psychiatry. (2016) 40:1–11. doi: 10.1007/s11013-015-9462-7
139. Wang F, Liu S, Zhang Q, Ng CH, Cui X, Zhang D, et al. Prevalence of depression in older nursing home residents in high and low altitude regions: a comparative study. Front Psychiatry. (2021) 12:669234. doi: 10.3389/fpsyt.2021.669234
140. Wang J, Zhou Y, Liang Y, Liu Z. A large sample survey of tibetan people on the qinghai–tibet plateau: current situation of depression and risk factors. Int J Environ Res Public Health. (2020) 17:289. doi: 10.3390/ijerph17010289
141. Schultze-Werninghaus G. Effects of high altitude on bronchial asthma. Pneumologie. (2008) 62:170–6. doi: 10.1055/s-2007-1016442
142. Schultze-Werninghaus G. Should asthma management include sojourns at high altitude? Allergy Asthma Mod Soc Sci Approach. (2006) 91:16–29. doi: 10.1159/000090227
143. Schuh A, Immich G. Forest Therapy-the Potential of the Forest for Your Health. Berlin: Springer (2022). doi: 10.1007/978-3-662-64280-1
144. Schuh A. Die evidenz der klima-und thalassotherapie. Ein Rev. (2009) 21:96–104. doi: 10.1159/000287219
145. Schobersberger W, Leichtfried V, Mueck-Weymann M, Humpeler E. Austrian moderate altitude studies (amas): benefits of exposure to moderate altitudes (1,500–2,500 M). Sleep Breath. (2010) 14:201–7. doi: 10.1007/s11325-009-0286-y
146. Saretta F, Pizziment C, Poser S, Toller I, Guerra M, Zanor S, et al. Variation of Oxygen Uptake in Asthmatic Children During Summer Holiday Camp in High Mountain. Vienna: European Respiratory Society Annual Congress Vienna; Clinical Advances in Childhood Asthma (2009).
147. Ohno H, Kuno S, Saito T, Kida M, Nakahara N. The effects of hypobaric conditions on man's thermal responses. Energy Build. (1991) 16:755–63. doi: 10.1016/0378-7788(91)90048-8
148. Massimo T, Blank C, Strasser B, Schobersberger W. Does climate therapy at moderate altitudes improve pulmonary function in asthma patients? A systematic review. Sleep Breath. (2014) 18:195–206. doi: 10.1007/s11325-013-0870-z
149. Immich G, Schuh A. A conceptual framework of forest therapy as an innovative health approach combined with local health resort medicine in alpine regions to increase mental health and well– being. Phys Med Rehabil Int. (2021) 8:1179. doi: 10.26420/physmedrehabilint.2021.1179
150. Dodev Y, Zhiyanski M, Glushkova M, Borisova B, Semerdzhieva L, Ihtimanski I, et al. An integrated approach to assess the potential of forest areas for therapy services. Land. (2021) 10:1354. doi: 10.3390/land10121354
151. Schuh A, Nowak D. Evidence-Based acute and long-lasting effects of climatotherapy in moderate altitudes and on the seaside. Deutsche Medizinische Wochenschrift. (2011) 136:135–9. doi: 10.1055/s-0031-1272496
152. Grafetstätter C, Prossegger J, Braunschmid H, Sanovic R, Hahne P, Pichler C, et al. No concentration decrease of house dust mite allergens with rising altitude in alpine regions. Allergy Asthma Immunol Res. (2016) 8:312–8. doi: 10.4168/aair.2016.8.4.312
153. Rahn H, Otis AB. Man's respiratory response during and after acclimatization to high altitude. Am J Physiol. (1949) 157:445–62. doi: 10.1152/ajplegacy.1949.157.3.445
154. Taylor L, Watkins SL, Marshall H, Dascombe BJ, Foster J. The impact of different environmental conditions on cognitive function: a focused review. Front Physiol. (2016) 6:372. doi: 10.3389/fphys.2015.00372
155. Lopez-Pascual A, Bes-Rastrollo M, Sayón-Orea C, Perez-Cornago A, Díaz-Gutiérrez J, Pons JJ, et al. Living at a geographically higher elevation is associated with lower risk of metabolic syndrome: prospective analysis of the sun cohort. Front Physiol. (2017) 7:658. doi: 10.3389/fphys.2016.00658
156. Qiang Q, Manalo JM, Sun H, Zhang Y, Song A, Wen AQ, et al. Erythrocyte adenosine A2b receptor prevents cognitive and auditory dysfunction by promoting hypoxic and metabolic reprogramming. PLoS Biol. (2021) 19:e3001239. doi: 10.1371/journal.pbio.3001239
157. Kumar GK. Hypoxia. 3. Hypoxia and neurotransmitter synthesis. Am J Physiol Cell Physiol. (2011) 300:C743–51. doi: 10.1152/ajpcell.00019.2011
158. Joseph V, Pequignot J-M. Breathing at high altitude. Cell Mol Life Sci. (2009) 66:3565–73. doi: 10.1007/s00018-009-0143-y
159. Kondo DG, Forrest LN, Shi X, Sung Y-H, Hellem TL, Huber RS, et al. Creatine target engagement with brain bioenergetics: a dose-ranging phosphorus-31 magnetic resonance spectroscopy study of adolescent females with ssri-resistant depression. Amino Acids. (2016) 48:1941–54. doi: 10.1007/s00726-016-2194-3
160. Jain K, Prasad D, Singh SB, Kohli E. Hypobaric hypoxia imbalances mitochondrial dynamics in rat brain hippocampus. Neurol Res Int. (2015) 2015:742059. doi: 10.1155/2015/742059
161. Shi X-F, Carlson PJ, Kim T-S, Sung Y-H, Hellem TL, Fiedler KK, et al. Effect of altitude on brain intracellular ph and inorganic phosphate levels. Psychiatry Res Neuroimaging. (2014) 222:149–56. doi: 10.1016/j.pscychresns.2014.04.002
162. Ray K, Dutta A, Panjwani U, Thakur L, Anand JP, Kumar S. Hypobaric hypoxia modulates brain biogenic amines and disturbs sleep architecture. Neurochem Int. (2011) 58:112–8. doi: 10.1016/j.neuint.2010.11.003
163. Mukandala G, Tynan R, Lanigan S, O'Connor JJ. The effects of hypoxia and inflammation on synaptic signaling in the Cns. Brain Sci. (2016) 6:6. doi: 10.3390/brainsci6010006
164. Matte DL, Pizzichini MMM, Hoepers ATC, Diaz AP, Karloh M, Dias M, et al. Prevalence of depression in copd: a systematic review and meta-analysis of controlled studies. Respir Med. (2016) 117:154–61. doi: 10.1016/j.rmed.2016.06.006
165. Li X-Y, Wu X-Y, Fu C, Shen X-F, Wu Y-H, Wang T. Effects of acute mild and moderate hypoxia on human mood state. Space Medicine Med Engg. (2000) 13:1–5.
166. Burtscher J, Niedermeier M, Hüfner K, van den Burg E, Kopp M, Stoop R, et al. The interplay of hypoxic and mental stress: implications for anxiety and depressive disorders. Neurosci Biobehav Rev. (2022) 138:104718. doi: 10.1016/j.neubiorev.2022.104718
167. Faeh D, Moser A, Panczak R, Bopp M, Röösli M, Spoerri A, et al. Independent at heart: persistent association of altitude with ischaemic heart disease mortality after consideration of climate, topography and built environment. J Epidemiol Community Health. (2016) 70:798–806. doi: 10.1136/jech-2015-206210
168. Serebrovskaya TV, Manukhina EB, Smith ML, Downey HF, Mallet RT. Intermittent hypoxia: cause of or therapy for systemic hypertension? Exp Biol Med. (2008) 233:627–50. doi: 10.3181/0710-MR-267
169. Stock MJ, Norgan NG, Ferro-Luzzi A, Evans E. Effect of altitude on dietary-induced thermogenesis at rest and during light exercise in man. J Appl Physiol. (1978) 45:345–9. doi: 10.1152/jappl.1978.45.3.345
170. Hannon JP, Sudman DM. Basal metabolic and cardiovascular function of women during altitude acclimatization. J Appl Physiol. (1973) 34:471–7. doi: 10.1152/jappl.1973.34.4.471
171. Cable NT, Drust B, Gregson WA. The impact of altered climatic conditions and altitude on circadian physiology. Physiol Behav. (2007) 90:267–73. doi: 10.1016/j.physbeh.2006.09.002
172. Shannon OM, Duckworth L, Barlow MJ, Deighton K, Matu J, Williams EL, et al. Effects of dietary nitrate supplementation on physiological responses, cognitive function, and exercise performance at moderate and very-high simulated altitude. Front Physiol. (2017) 8:401. doi: 10.3389/fphys.2017.00401
173. Viscor G, Torrella JR, Corral L, Ricart A, Javierre C, Pages T, et al. Physiological and biological responses to short-term intermittent hypobaric hypoxia exposure: from sports and mountain medicine to new biomedical applications. Front Physiol. (2018) 9:814. doi: 10.3389/fphys.2018.00814
174. Aleshin IA, IaI K, Tverdokhlib VP, Galiautdinov GS, Vdovenko LG, Zabirov MR, et al. The nondrug treatment of hypertension patients by their adaptation to periodic hypoxia in a barochamber. Terapevticheskii Arkhiv. (1993) 65:23–9.
175. Lin Q, Liu J, Xu S, Ning X, Tu J, Yang Q, et al. Epidemiological features of glycemic levels and relative determinants at different altitudes among tibetans in china: a cross-sectional population-based study. Front Public Health. (2020) 8:472. doi: 10.3389/fpubh.2020.00472
176. Woolcott OO, Castillo OA, Gutierrez C, Elashoff RM, Stefanovski D, Bergman RN. Inverse association between diabetes and altitude: a cross-sectional study in the adult population of the United States. Obesity. (2014) 22:2080–90. doi: 10.1002/oby.20800
177. Legrand FD, Jeandet P, Beaumont F, Polidori G. Effects of outdoor walking on positive and negative affect: nature contact makes a big difference. Front Behav Neurosci. (2022) 16:901491. doi: 10.3389/fnbeh.2022.901491
178. Millet GP, Debevec T, Brocherie F, Malatesta D, Girard O. Therapeutic use of exercising in hypoxia: promises and limitations. Frontiers Media SA. (2016) 7:224. doi: 10.3389/fphys.2016.00224
179. Ando S, Komiyama T, Sudo M, Higaki Y, Ishida K, Costello JT, et al. The interactive effects of acute exercise and hypoxia on cognitive performance: a narrative review. Scand J Med Sci Sports. (2020) 30:384–98. doi: 10.1111/sms.13573
180. Daley AJ, Huffen C. The effects of low and moderate intensity exercise on subjective experiences in a naturalistic health and fitness club setting. J Health Psychol. (2003) 8:685–91. doi: 10.1177/13591053030086003
181. Thompson Coon J, Boddy K, Stein K, Whear R, Barton J, Depledge MH. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ Sci Technol. (2011) 45:1761–72. doi: 10.1021/es102947t
182. Lu Z-C, Tseng C-H, Lin H-H, Perng Y-S, Tseng Y-H. Suggestions on relieving physical anxiety of medical workers and improving physical and mental health under the covid-19 epidemic—a case study of Meizhou City. Front Public Health. (2022) 10:919049. doi: 10.3389/fpubh.2022.919049
183. Gierc M, Riazi NA, Fagan MJ, Di Sebastiano KM, Kandola M, Priebe CS, et al. Strange days: adult physical activity and mental health in the first two months of the Covid-19 pandemic. Front Public Health. (2021) 9:567552. doi: 10.3389/fpubh.2021.567552
184. Chan JSY, Liu G, Liang D, Deng K, Wu J, Yan JH. Special issue–therapeutic benefits of physical activity for mood: a systematic review on the effects of exercise intensity, duration, and modality. J Psychol. (2019) 153:102–25. doi: 10.1080/00223980.2018.1470487
185. Zhai Y, Li D, Wang D, Shi C. Seniors' physical activity in neighborhood parks and park design characteristics. Front Public Health. (2020) 8:322. doi: 10.3389/fpubh.2020.00322
186. Gallagher SA, Hackett PH. High-Altitude illness. Emerg Med Clin. (2004) 22:329–55. doi: 10.1016/j.emc.2004.02.001
187. Millet GP, Debevec T. Crosstalk proposal: barometric pressure, independent of Po2, is the forgotten parameter in altitude physiology and mountain medicine. J Physiol. (2020) 598:893–6. doi: 10.1113/JP278673
188. de Bloom J, Sianoja M, Korpela K, Tuomisto M, Lilja A, Geurts S, et al. Effects of park walks and relaxation exercises during lunch breaks on recovery from job stress: two randomized controlled trials. J Environ Psychol. (2017) 51:14–30. doi: 10.1016/j.jenvp.2017.03.006
189. Peterfalvi A, Meggyes M, Makszin L, Farkas N, Miko E, Miseta A, et al. Forest bathing always makes sense: blood pressure-lowering and immune system-balancing effects in late spring and winter in central Europe. Int J Environ Res Public Health. (2021) 18:2067. doi: 10.3390/ijerph18042067
190. Bielinis E, Jaroszewska A, Lukowski A, Takayama N. The effects of a forest therapy programme on mental hospital patients with affective and psychotic disorders. Int J Environ Res Public Health. (2020) 17:118. doi: 10.3390/ijerph17010118
191. Beck HE, Zimmermann NE, McVicar TR, Vergopolan N, Berg A, Wood EF. Present and future köppen-geiger climate classification maps at 1-Km resolution. Sci Data. (2018) 5:1–12. doi: 10.1038/sdata.2018.214
192. Dhillon S. Environmental hazards, hot, cold, altitude, and sun. Infect Dis Clin. (2012) 26:707–23. doi: 10.1016/j.idc.2012.07.001
193. Hu Z, Wu J, Yang L, Gu Y, Ren H. Physiological and perceptual responses of exposure to different altitudes in extremely cold environment. Energy Build. (2021) 242:110844. doi: 10.1016/j.enbuild.2021.110844
194. Zhu S-x, Hu F-f, He S-y, Qiu Q, Su Y, He Q, et al. Comprehensive evaluation of healthcare benefits of different forest types: a case study in shimen national forest park, China. Forests. (2021) 12:207. doi: 10.3390/f12020207
195. Wang H, Hu S, Liu G, Li A. Experimental study of human thermal sensation under hypobaric conditions in winter clothes. Energy Build. (2010) 42:2044–8. doi: 10.1016/j.enbuild.2010.06.013
196. Ou CQ, Jun Y, Ou QQ, Liu HZ, Lin GZ, Chen PY, et al. The impact of relative humidity and atmospheric pressure on mortality in Guangzhou, China. Biomed Environ Sci. (2014) 27:917–25. doi: 10.3967/bes2014.132
197. Wang R, Chen Q, Wang D. Effects of altitude, plant communities, and canopies on the thermal comfort, negative air ions, and airborne particles of mountain forests in summer. Sustainability. (2022) 14:3882. doi: 10.3390/su14073882
198. Pino O, La Ragione F. There's something in the air: empirical evidence for the effects of negative air ions (Nai) on psychophysiological state and performance. Res Psychol Behav Sci. (2013) 1:48–53. doi: 10.12691/rpbs-1-4-1
199. Sandhu MS, Casale TB. The role of vitamin D in asthma. Ann Allergy Asthma Immunol. (2010) 105:191–9. doi: 10.1016/j.anai.2010.01.013
200. Lyu B, Zeng C, Deng S, Liu S, Jiang M, Li N, et al. Bamboo forest therapy contributes to the regulation of psychological responses. J For Res. (2019) 24:61–70. doi: 10.1080/13416979.2018.1538492
201. Keeling HC, Phillips OL. A calibration method for the crown illumination index for assessing forest light environments. For Ecol Manage. (2007) 242:431–7. doi: 10.1016/j.foreco.2007.01.060
202. Farkic J, Isailovic G, Taylor S. Forest bathing as a mindful tourism practice. Ann Tour Res Emp Insights. (2021) 2:100028. doi: 10.1016/j.annale.2021.100028
203. Bach A, Maneja R, Zaldo-Aubanell Q, Romanillos T, Llusià J, Eustaquio A, et al. Human absorption of monoterpenes after a 2-H forest exposure: a field experiment in a mediterranean holm oak forest. J Pharm Biomed Anal. (2021) 200:114080. doi: 10.1016/j.jpba.2021.114080
204. Tsunetsugu Y, Park BJ, Miyazaki Y. Trends in research related to “shinrin-yoku” (taking in the forest atmosphere or forest bathing) in Japan. Environ Health Prev Med. (2010) 15:27–37. doi: 10.1007/s12199-009-0091-z
205. Antonelli M, Donelli D, Barbieri G, Valussi M, Maggini V, Firenzuoli F. Forest volatile organic compounds and their effects on human health: a state-of-the-art review. Int J Environ Res Public Health. (2020) 17:6506. doi: 10.3390/ijerph17186506
206. Song C, Ikei H, Miyazaki Y. Elucidation of a physiological adjustment effect in a forest environment: a pilot study. Int J Environ Res Public Health. (2015) 12:4247–55. doi: 10.3390/ijerph120404247
207. Ideno Y, Hayashi K, Abe Y, Ueda K, Iso H, Noda M, et al. Blood pressure-lowering effect of shinrin-yoku (forest bathing): a systematic review and meta-analysis. BMC Complement Alternat Med. (2017) 17:409. doi: 10.1186/s12906-017-1912-z
Keywords: nature-based intervention, forest therapy, psychological restoration, physiological relaxation, meta-regression
Citation: Kim E, Park S, Kim S, Choi Y, Cho JH and Kim G (2022) Is altitude a determinant of the health benefits of nature exposure? A systematic review and meta-analysis. Front. Public Health 10:1021618. doi: 10.3389/fpubh.2022.1021618
Received: 18 August 2022; Accepted: 11 November 2022;
Published: 25 November 2022.
Edited by:
Linchuan Yang, Southwest Jiaotong University, ChinaReviewed by:
Gregoire P. Millet, Université de Lausanne, SwitzerlandDong Wei, Southwest Jiaotong University, China
Copyright © 2022 Kim, Park, Kim, Choi, Cho and Kim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Geonwoo Kim, YmtpbTUwMjBAa29yZWEua3I=