 Ranran Zheng
Ranran Zheng Mingyang Yu2
Mingyang Yu2 Li Huang
Li Huang Guilin Liu
Guilin Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 03 October 2022
Sec. Aging and Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1009781
This article is part of the Research TopicHealthy Aging, Mental Health, and SexualityView all 16 articles
Background: As the population ages with fewer children, depression symptoms are increasing among the elderly who lack companionship. Intergenerational support is closely related to depression in the elderly; hence how the behavioral patterns and emotional quality of intergenerational support affect depressive symptoms in the elderly should be further explored.
Objective: To study the effects of intergenerational exchange patterns and intergenerational relationship quality on depressive symptoms in the elderly.
Methods: A total of 8,015 people over 60 years old in CHARLS in 2018 were selected as the object of this study. First, the correlation between demographics, economic conditions, health status, intergenerational support patterns, intergenerational relationship quality, and depressive symptoms in the elderly were analyzed. Three regression analysis models were established to analyze the relationship between control variables, intergenerational support patterns, intergenerational relationship quality, and depressive symptoms in the elderly. Results: Among the intergenerational economic, care, and emotional exchange modes, the risk of depressive symptoms in the elderly in the mutual support group was 31.8, 38.4, and 25.5% lower than that in the non-communication group. Compared with the elderly with very poor intergenerational relationship quality, the elderly with good, very good, and excellent intergenerational relationship quality had 74.5, 84.0, and 85.6% lower risk of depressive symptoms.
Discussion: Different cultural backgrounds also affect intergenerational exchange patterns and depression in the elderly. During the study of depressive symptoms, two aspects relating to intergenerational support should be considered behaviorally and emotionally: the intergenerational exchange model and the intergenerational relationship quality. As depression in the elderly is affected by multiple factors, the participation and joint efforts of the whole society are required to reduce depressive symptoms in the elderly and realize active aging.
Conclusion: The intergenerational exchange pattern of mutual support and the higher quality of the intergenerational relationship can significantly reduce the depressive symptoms of the elderly.
About 20% of people over 60 years old have varying degrees of depression worldwide (1). They have a significantly reduced quality of life, and severe ones have suicidal tendencies (2, 3). Among those who have committed suicide, 50–70% have suffered from depression (4). Depression and suicide in older adults have garnered much attention because of their vulnerability (5). China has entered an aging society, with the proportion of the elderly in the total population rising to 18.7% (6). According to the World Health Organization (WHO), the prevalence of depression among people aged 65 years and above exceeded 10% in 2018, suggesting that depression has become a significant disease that impairs the health of the elderly (7). The outbreak and continuous spread of Covid-19 in recent years have significantly challenged the mental health of the elderly (8, 9). How to release the depression of the elderly and achieve active aging has become a global social problem (10, 11).
Studies show that intergenerational support is closely related to depressive symptoms in the elderly (12–14). Intergenerational support refers to the economic, care, and emotional interactions between parents and their children within a family, including intergenerational resource exchange and intergenerational relationship quality.
According to the different combinations of the content and direction of intergenerational resource exchange, an intergenerational exchange can be divided into different patterns. Studies on the relationship between intergenerational support and elderly depressive symptoms mainly concentrate on two aspects. The first is the study on the relationship between the content of intergenerational resource exchange and depressive symptoms in the elderly. In terms of economic support, Marie et al. (15) showed that intergenerational economic support could meet the material needs of the elderly, thus increasing their life satisfaction by 14.4%. However, according to the research by Fingerman (16), excessive intergenerational economic support could damage the self-esteem of the elderly, making them feel powerless and thus damaging their mental health. Tang et al. (17) found that intergenerational care support could enable the elderly to get good care, alleviate diseases, and help maintain good health. Other studies have shown that the influence of intergenerational care support on the mental health of the elderly is not insignificant (18) and even harmful (19). In the field of intergenerational emotional support, Roh et al. (20) showed that compared with the above two factors, emotional support could more effectively maintain the mental health of the elderly and reduce the prevalence of depression. However, this effect was not as apparent for excessive or insufficient emotional support, according to research by Teixeira et al. (21). The second is the study on the relationship between the intergenerational support direction and depressive symptoms in the elderly. The intergenerational support direction can be divided into forwarding (parents provide support for children), backward (children provide support for parents), and mutual (children and parents provide support for each other) support. Bonsang et al. (22) found that care support from children hurt fathers' self-rated health and economic support for mothers' self-rated health. Guoping et al. (23) found that intergenerational support from the elderly with poor economic conditions in rural areas could increase children's life stress and the risk of depression in them. Abolfathi et al. (24) found that the elderly who could give feedback to their children for receiving intergenerational support was less depressed because they felt that they were “important” and “useful”.
Essentially, intergenerational support is a kind of purposeful interaction between generations. Beyond the essential characteristics of the two interacting parties, the expression form and result of interactive behavior in real life are also affected by the subjective emotion factor of both parties: the quality of intergenerational relationships. This is a critical factor to investigate (25). Most scholars measure it with such objective indicators as the intensity and frequency of intergenerational support. Huang et al. (26) measured the intergenerational relationship by using the intensity of intergenerational support, finding that older people who interacted with their children more closely were mentally healthier. Teixeira et al. (21) discovered a link between the frequency of intergenerational support and the mental health of the elderly. Yang et al. (27), using children's subjective evaluation to measure the intergenerational relationship, found that the intergenerational relationship had effects on the health and well-being of both generations. The content, direction, and quality of intergenerational support had specific effects on the level of depression in the elderly, but no uniform conclusion has been reached.
There are two limitations to current studies. First, most studies only analyze the relationship between the content or direction of intergenerational resource exchange and the depressive symptoms in the elderly separately, with few focusing on the combination of the content and direction. Second, both the content and direction of intergenerational support are closely related to depressive symptoms in the elderly. The results will inevitably be biased if we only study one of them. While there are few studies on the relationship between intergenerational relationship quality and depressive symptoms in the elderly, objective indicators such as the intensity and frequency of intergenerational support are often used as alternative variables of intergenerational relationship quality, which is indirect speculation that is not very accurate. Intergenerational relationship quality is more of a subjective feeling, and the elderly's subjective evaluation of the intergenerational relationship can better reflect its intergenerational relationship.
The innovations of this study mainly include two aspects. First, the content and direction of intergenerational support are integrated and conceptualized as intergenerational exchange patterns to comprehensively study the relationship between different intergenerational exchange patterns and depressive symptoms in the elderly. Second, the elderly's subjective evaluation of the intergenerational relationship is taken as an indicator to measure the intergenerational relationship quality, and the relationship between the intergenerational relationship quality and intergenerational exchange patterns and the depressive symptoms in the elderly is investigated.
Data for this study were obtained from the China Health and Retirement Longitudinal Study (CHARLS) in 2018. The CHARLS began in 2008 and was followed up every 2–3 years, with samples collected through stratified random sampling from 150 county-level and 450 village-level units nationwide. In 2018, 19,744 samples were obtained from CHARLS. Respondents aged 60 years and above as of December 31, 2018, were selected as participants of this study, from which those with missing data were eliminated, and finally, 8,015 valid samples were obtained. All the respondents signed informed consent at the time of participation, and this study was approved by the Institutional Review Board of Peking University (IRB00001052-11014).
In this paper, whether the elderly have depressive symptoms was regarded as the dependent variable. In the CHARLS, Andresen's 1994 revision of the Center for Epidemiologic Studies Depression Scale of the 10-item short table (CES-D-10) was used to measure the degree of depression in respondents. The scale consists of ten questions with four answer options assigned to 0, 1, 2, and 3, from positive to negative, respectively. Respondents were asked to rate the ten questions based on their feelings and behaviors in the previous week, and the total score was the final score, ranging from 0 to 30. The questionnaire is listed in Table 1. Those with a final score ≥10 were determined to have depressive symptoms (28), and the answer was assigned 1; those with a final score < 10 were determined to have no depressive symptoms, and the answer was assigned 0. The study showed that the CES-D-10 scale has sufficient reliability and validity (29). Besides, studies based on CHARLS have confirmed that the CES-D-10 can effectively measure the depression level of the elderly population in China (30). With a short response time and high recovery rate, the scale has greater application potential in ample survey research. However, it is primarily used to assess the severity of depressive symptoms rather than as a diagnostic tool.
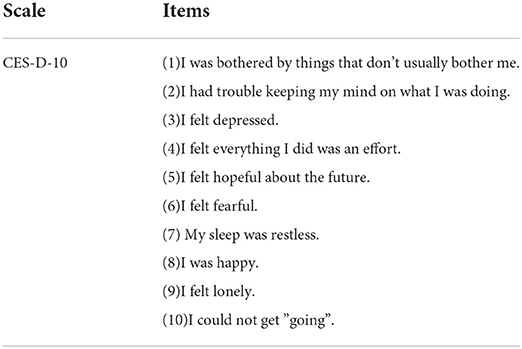
Table 1. CES-D-10 Scale items.
In this study, three types of intergenerational support were explored: the economic ties between participants and their children (economic support), mutual care between participants and their children (care support), and regular meetings or contact between participants and their children (emotional support). To measure whether the elderly received or provided intergenerational support, participants were asked questions about it. See Table 2 for specific questionnaires.
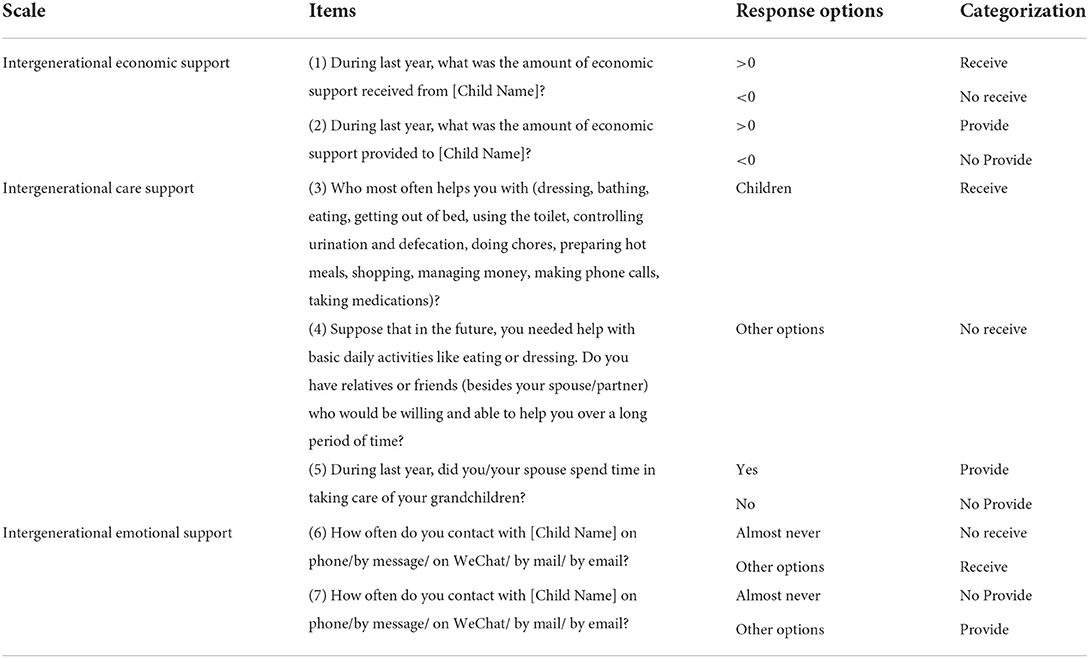
Table 2. Questionnaire of intergenerational support.
Based on the responses of receiving and providing intergenerational support, the exchange modes were divided into four types: no exchange, only provide, only receive, and mutual support. The first type of “no exchange” means that the respondent has neither provided nor received any support for a year. The second “only receive” means that the respondent only received support without providing any support. The third “Only provide” means that the respondent only provided support without receiving any support for 1 year. The last “mutual support” means that the respondent received and provided support simultaneously. Because effective support is bidirectional, there are two types of intergenerational emotion exchange modes: no exchange and mutual support.
The subjective evaluation of the respondents was used in this paper to measure the quality of intergenerational relationships. CHARLS asked respondents to answer, “Are you satisfied with your relationship with your children?”, and the answers were “extremely satisfied,” “very satisfied,” “relatively satisfied,” “not very satisfied,” and “very dissatisfied.” These answers represented five grades of intergenerational relationship quality: “excellent,” “very good,” “good,” “not good,” and “extremely poor”.
Other control factors, including demographics, economic conditions, and health status, also affect the presence of depressive symptoms in the elderly (31, 32). In this paper, the three types of control variables were introduced, among which demographic variables included age, gender, and marital status; economic condition variables included working status, education, residence, and medical insurance status; and health status variables included the presence of chronic diseases and disabilities.
First, CHARLS database indicators were screened, grouped, and assigned. Variables and assignments are shown in Table 3. Second, a descriptive analysis of the participants' variables was carried out, including their demographics, financial and health status, intergenerational exchange patterns, and the quality of their intergenerational relationships. Third, a one-way ANOVA was conducted to determine whether there was a significant correlation between control variables, intergenerational support patterns, intergenerational relationship quality, and depressive symptoms in the elderly. Fourth, three binary logistic regression models were established to study the effects of control variables, intergenerational support patterns, and intergenerational relationship quality on depressive symptoms in the elderly.
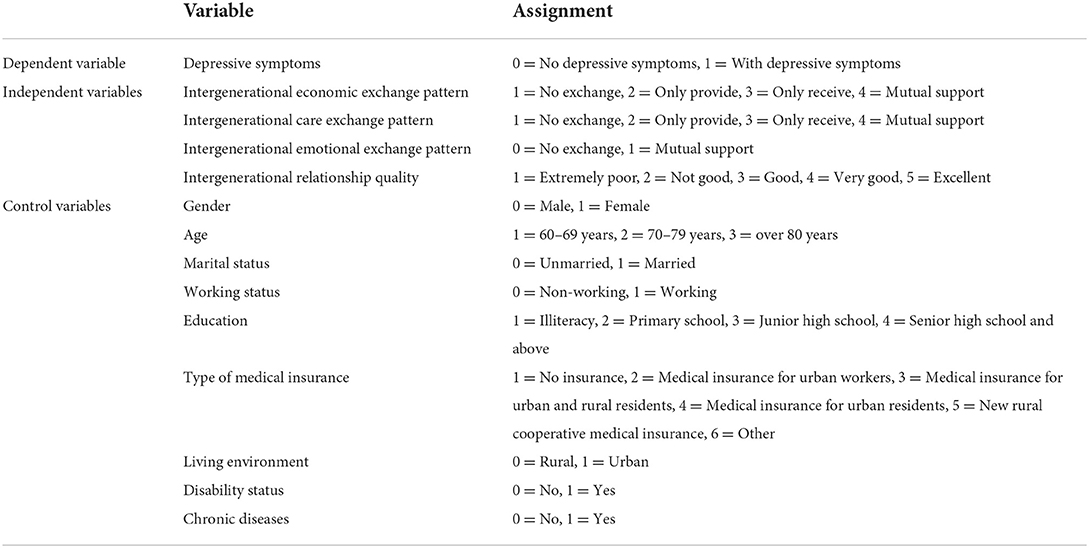
Table 3. Variables and assignments.
Table 4 describes the investigation samples. Depressive symptoms were found in 37.8% of the sample. The quality of intergenerational relationships was relatively good (39.1%) or very good (49.1%). In terms of the mode of intergenerational exchange, more than half (54%) of the elderly said they had no intergenerational economic exchange with their children. In the intergenerational care exchange mode, the elderly in the only receiving group accounted for the largest proportion (45.7%); more than half (59.3%) had no emotional exchange with their children.
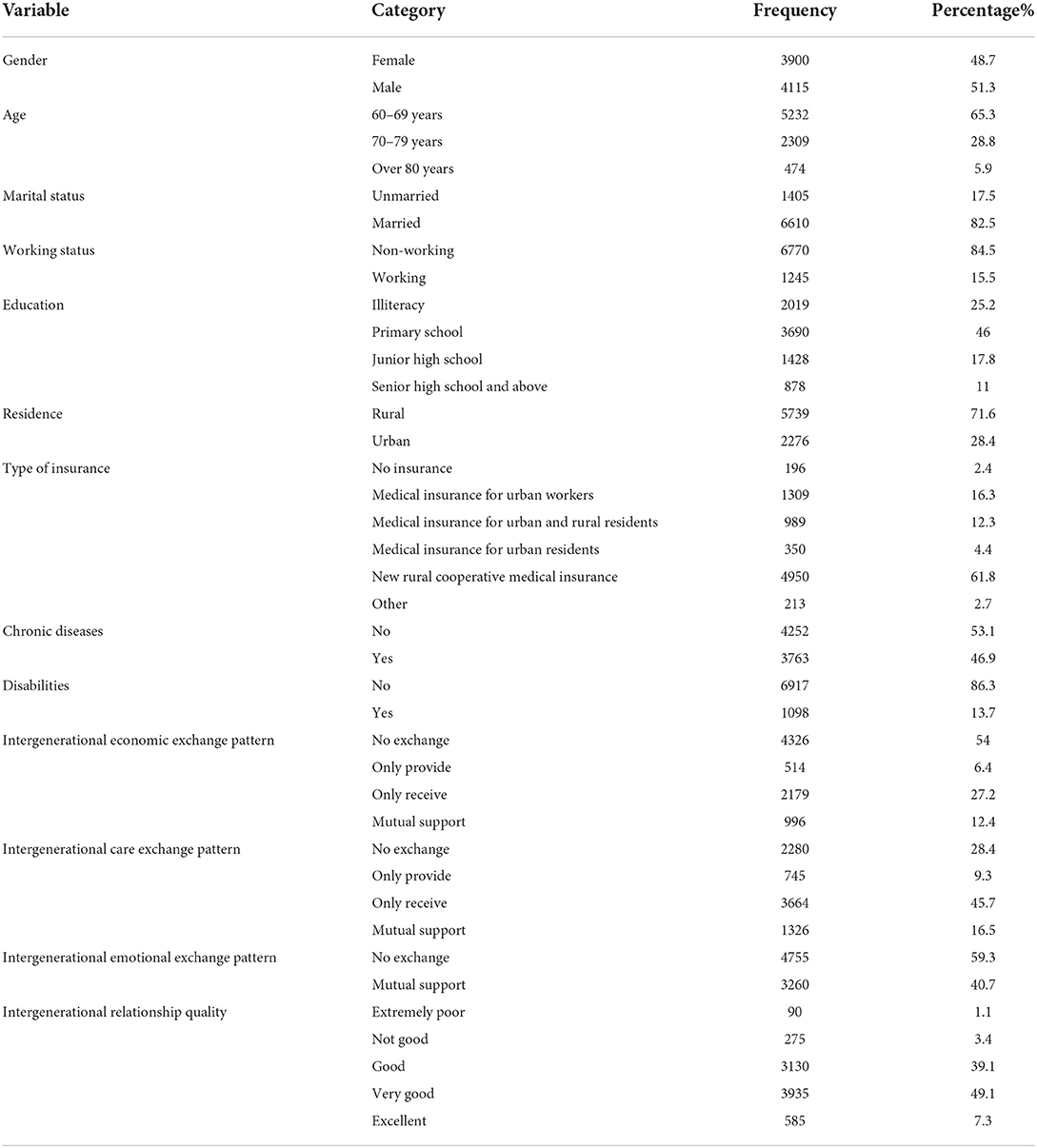
Table 4. Basic characteristics of survey samples (n = 8,015).
Table 5 shows the analysis of the correlation between various factors and depressive symptoms in the elderly. Results showed that in addition to age, other control variables, including gender, marital status, working status, education, residence, medical insurance status, chronic diseases, and disabilities, were significantly correlated with the depressive symptoms in the elderly; intergenerational economic, care and emotional exchange patterns had a significant impact on the presence or absence of depressive symptoms in the elderly; intergenerational relationship quality was significantly correlated with depressive symptoms in the elderly.
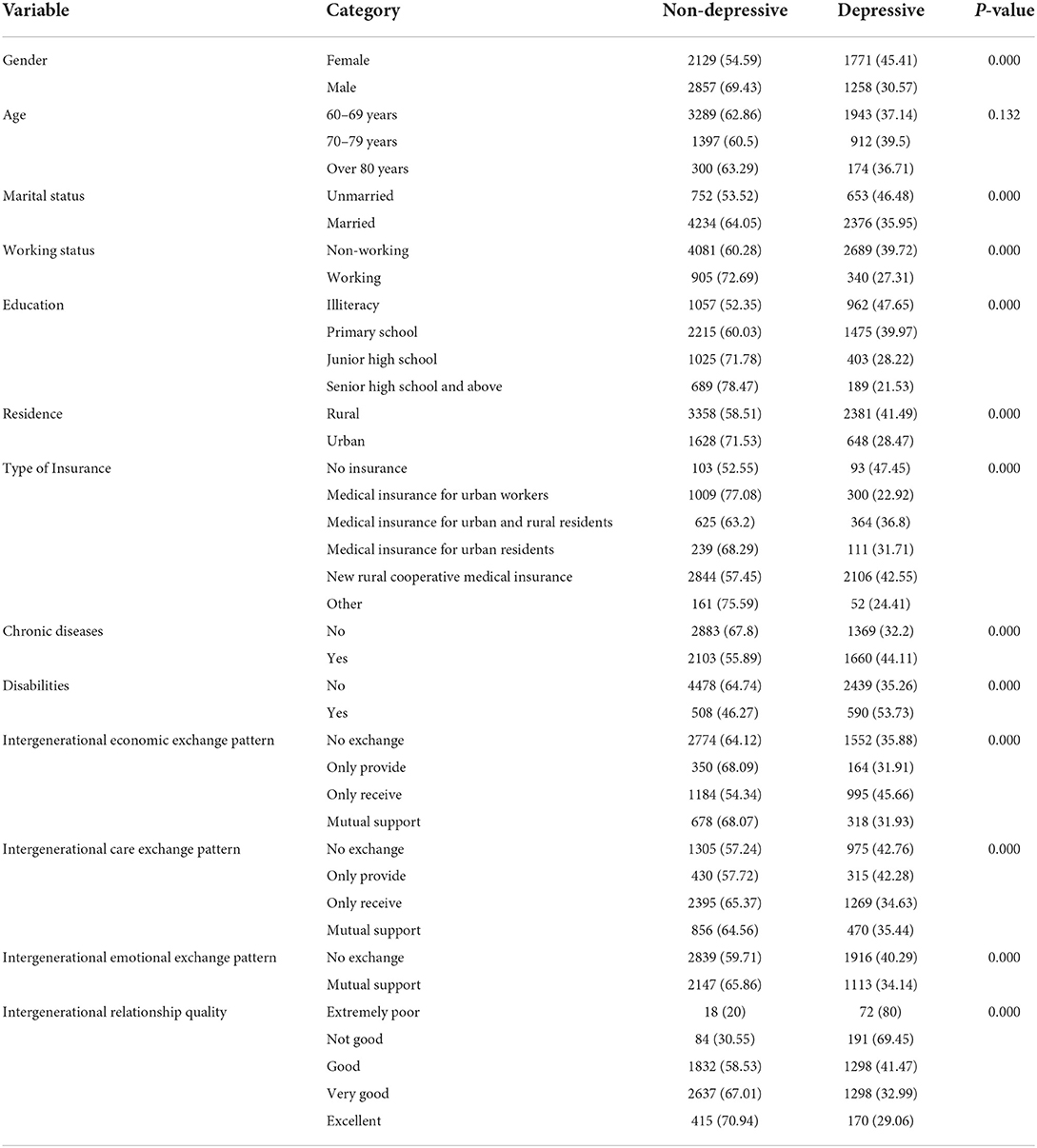
Table 5. Correlation analysis on the influencing factors of depressive symptoms (n = 8,015, n/%).
Table 6 shows three binary logistic regression models. Model 1 studied the effect of control variables on depressive symptoms in the elderly. Model 2, based on Model 1, included intergenerational exchange pattern variables in regression models to study the effect of intergenerational exchange patterns on depressive symptoms in the elderly after controlling control variables. Model 3, based on Model 2, included intergenerational relationship quality variables in regression models to study the effect of intergenerational relationship quality on depressive symptoms in the elderly after controlling control variables and intergenerational exchange pattern variables. Collinearity analysis was performed on three models before the inclusion of variables, and the results showed that VIF (Variance Inflation Factor) < 10 and no collinearity problems occurred (33). Meanwhile, the Hosmer test results showed P > 0.05, suggesting that the models fit well (34).
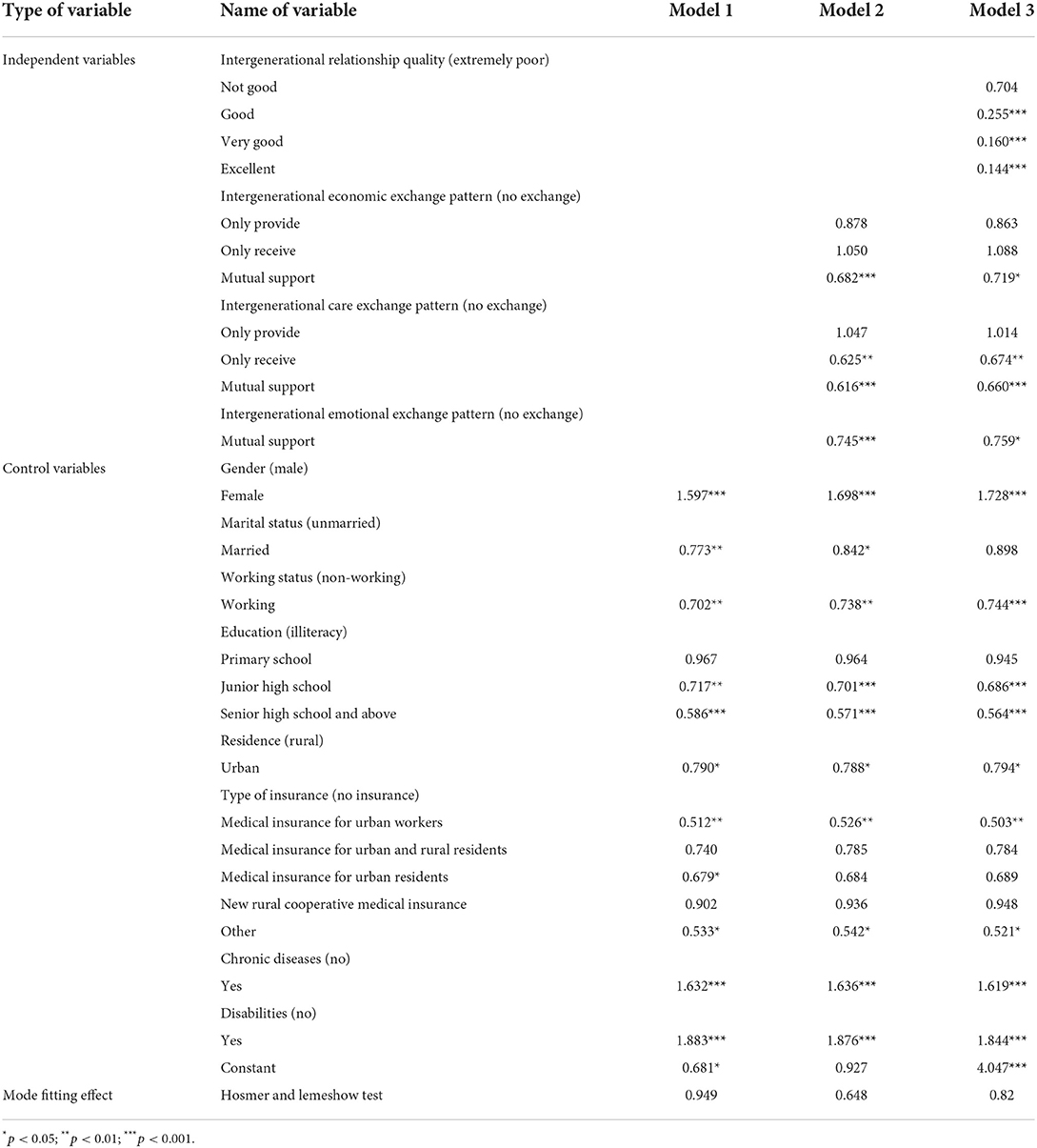
Table 6. Analysis of the relationship between intergenerational relationship quality and intergenerational exchange patterns and the depressive symptoms in the elderly (n = 8,015).
Model 1 studied the effects of 8 control variables, including gender, marital status, working status, education, residence, medical insurance status, chronic diseases, and disabilities, on depressive symptoms of the elderly. Among them, gender is a risk factor for depressive symptoms; the risk of depressive symptoms in older women was significantly higher (1.597 times) than in older men. Being working and married are protective factors for depressive symptoms in the elderly; the risk of depressive symptoms in the working elderly was 29.8% lower than in non-working ones, and that in the married was 22.7% lower than the unmarried. With the improvement of educational levels, the elderly's depressive symptoms were somewhat reduced. Compared with illiterate older people, there was no significant difference in the risk of depressive symptoms in older people with primary school education, while there were significant differences in those with junior high school education and those with senior high school education and above (the risk of depressive symptoms decreased by 28.3 and 41.4%, respectively). Compared with the elderly without medical insurance, there was no significant difference in the risk of depressive symptoms in those with new rural cooperative medical insurance and medical insurance for urban and rural residents, while there were significant differences in those with basic medical insurance for urban workers, medical insurance for urban residents, and other medical insurance (the risk of depressive symptoms decreased by 48.8, 31.2, and 46.7%). Diseases are a risk factor for depressive symptoms in the elderly; older people with chronic diseases and disabilities had a significantly increased risk of depressive symptoms, which was 1.632 and 1.883 times that of healthy people.
After controlling control variables, Model 2 studied the effects of different intergenerational exchange patterns on the risk of depressive symptoms in the elderly. In the economic exchange pattern, compared with the group having no exchange, there were significant differences in the risk of depressive symptoms in the elderly in the mutual support group (the risk in the mutual support group was 31.8% lower than the group having no exchange), while there was no significant difference in the group only providing support and the group receiving support. In the care exchange pattern, compared with the group having no exchange, there were significant differences in the risk of depressive symptoms in the elderly in the group receiving support and the mutual support group (the risks in the two groups were 37.5 and 38.4% lower than the group having no exchange, respectively), while there was no significant difference in the group only providing support. In the emotional exchange pattern, there were significant differences in the risk of depressive symptoms in the elderly between the group having no support and the mutual support group (the risk in the latter was 25.5% lower than in the former). To sum up, the risks of depressive symptoms in the elderly in the mutual support group were significantly lower than those in the group having no exchange in the economic, care, and emotional exchange patterns.
Model 3 studied the effect of intergenerational relationship quality on depressive symptoms in the elderly after optimizing control variables and intergenerational exchange pattern variables. There were significant differences in the risk of depressive symptoms in the elderly with extremely poor intergenerational relationships and other groups, and the risks in the elderly with good, very good, and excellent intergenerational relationships were 74.5, 84.0, and 85.6% lower than those with extremely poor intergenerational relationships. The results are shown in Figure 1. This shows that intergenerational relationship quality is a protective factor toward depressive symptoms in the elderly, and the risk of depressive symptoms in the elderly gradually decreases as intergenerational relationship quality improves.
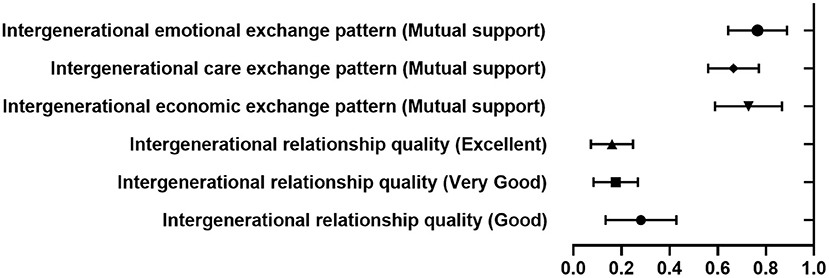
Figure 1. Forest diagram of factors influencing depressive symptoms in the elderly.
In different exchange patterns, the elderly have the lowest risk of depressive symptoms when there is mutual economic, care, and emotional support between generations, which is consistent with several conclusions based on Chinese data. For example, Dura et al. (35) found that intergenerational exchange with children could directly enhance parents' well-being; Huang et al. (26) found that intergenerational exchange was conducive to the elderly's self-rated health, and the closer the intergenerational exchanges, the better for the elderly's physical and mental health. Nevertheless, most studies based on non-Chinese data have not supported this conclusion. Lowenstein et al. (26) found that older people were more likely to be the “givers” in intergenerational exchange, in which they could realize their self-value while receiving support from their children could only hurt their self-esteem and thus affect their mental health. Cultural differences may be the root cause of the differences in research results. In western countries where freedom and independence are advocated, parents are responsible for bringing up their children, but children have no obligation to support their parents (36). In this case, parents play the role of a “giver.” On the contrary, in China and even East Asia, the norm of filial piety still significantly affects family relations. Exchange is sustainable only through reciprocity and balance between generations (37). We can see from family relationships that the elderly feel depressed when they are unable to support their children, thus hurting their mental health. They perceive themselves as responding to their children's support and recognize that they are needed. This move can improve their self-esteem and thus reduce the risk of depression (24). This is in line with the results of this study, which showed that the mutually supportive intergenerational exchange model could greatly reduce the risk of depression in the elderly.
As the intergenerational relationship quality enhances, the risk of depressive symptoms in the elderly significantly decreases. Compared with the results obtained using the intensity of intergenerational exchange to expect intergenerational relationship quality, this study directly measured intergenerational relationship quality with the elderly's subjective evaluation, which was more significantly correlated with the level of depressive symptoms in the elderly (27, 28). The reason may be that the high intensity of intergenerational exchange does not inevitably mean good intergenerational relationships, and negative intergenerational exchange (such as quarrels and frequently asking for money) may cause trouble for older people and thus increase the risk of depressive symptoms. The quality of intergenerational relationships is a cross-cultural concept, and good intergenerational relationships are an important determinant of older adults' well-being wherever and whenever they occur (27, 38). In China, home-based care, as the most traditional form of old-age care, still has a major position (39), while the quality of the intergenerational relationship, the core social relationship in the elderly's life, has a greater impact on the elderly. According to Amato and Booth, intergenerational support should be influenced not only by demographics but also by prospects for intergenerational interaction such as the number and availability of relatives (40). This means that the study of intergenerational support should be performed not only at the behavioral level, such as frequency of contact, giving, and receiving of support, but also at the emotional level, such as the feelings, values, and perspectives of intimacy and connection. In addition, intergenerational support is affected not only by the measurable exchange but also by normative issues such as the amount of support given and received between members, the importance of filial duty, and values in the parent-child relationship (41). This study suggests that improving the quality of intergenerational relationships can effectively reduce the risk of depressive symptoms in the elderly.
The depressive symptoms in the studied elderly were high, with significant internal heterogeneity. According to the WHO report in 2017, the prevalence of depressive symptoms was 7.5% in women and over 5.5% in men aged 55–74 years (42). In the sample in this paper, up to 37.80% of the elderly had depressive symptoms, including 30.57% of men and 45.41% of women, much higher than the world average, suggesting that the depressive symptoms in the elderly are serious in China. There were significant differences in the degree of depressive symptoms in the elderly of different genders, marriage, urban and rural areas, education level, type of insurance, and health status. Compared with the urban elderly, the rural elderly suffered from a significantly higher risk of depression. Perhaps, due to the impact of urbanization and population aging, young people in rural areas flooding into cities for better development, and the increase of empty-nested elderly, these factors exacerbate the aging degree in rural areas. The elderly living alone have difficulties communicating with their children without intergenerational emotional support and intergenerational care support, thus creating an unrelieved depression in the elderly in rural areas. In parallel, studies have shown that rural areas are provided with scarce health care resources and low availability of medical professionals (43). These negative factors lead to deeper depression in the elderly who cannot get help in time.
Under the background of increasing aging, it is necessary to improve the quality of intergenerational relationships and establish a positive intergenerational exchange mode to reduce the level of depression in the elderly. Firstly, the government should encourage intergenerational communication by providing more adequate family leave and more time for intergenerational communication. Secondly, society should provide daily care services for the elderly, including routine physical examination, psychological consultation, and daily activity places, to meet the needs of the elderly in time. Thirdly, family members should take the initiative to communicate with the elderly; children should actively meet or call them, and teachers should learn to use communication tools to help the elderly keep up with the pace of society as much as possible. Lastly, the elderly should also learn to change their mindset, seek help from their children, and strengthen mutual support between generations.
There are several limitations to this study. First, intergenerational relationship quality is a dimensionally rich concept, and it is inadequate to measure it using a single subjective indicator. Emotional evaluation is somewhat subjective and unstable; therefore, the results should be interpreted more carefully. Second, the causal relationship should also be determined carefully in cross-sectional studies, and if conditions permit, targeted follow-up can be carried out to verify the conclusions of this study. In the future, the panel data can be used to further verify the conclusions of this paper. Alternatively, targeted follow-up surveys can be performed focusing on the measurement indicators of intergenerational relationship quality to further explore the relationship between intergenerational relationship quality and depression in the elderly. Additionally, we look forward to continuing exploring the gender and urban-rural differences in the influence of intergenerational relationships on depression in the elderly to reduce their level of depression and provide more targeted suggestions for active aging.
In conclusion, intergenerational relationship quality and intergenerational exchange patterns significantly affect depressive symptoms in the elderly, and high-quality intergenerational relationships and the intergenerational exchange pattern of mutual support can greatly reduce the risk of depressive symptoms in the elderly. This study not only added to the theories of related studies but also pointed in the right direction for reducing the severity of depressive symptoms in the elderly. The quality of intergenerational relationships can be improved by encouraging closer economic, care, and mutual emotional support between generations.
Publicly available datasets were analyzed in this study. This data can be found here: https://charls.pku.edu.cn.
All the respondents signed informed consent at the time of participation, and this study was approved by the Institutional Review Board of Peking University (IRB00001052-11014).
RZ took responsibility for the integrity of the data and the accuracy of the data analysis. RZ, MY, and GL study design. JZ, LH, BG, FW, and DF contributed to the writing of the manuscript and statistical analysis. JZ and GL study supervision. All authors contributed to this article and approved the submitted version.
The authors would like to acknowledge all participants of the National School of Development workshop at Peking University, as well as those who contributed to the 2018 China Health and Retirement Longitudinal Study (CHARLS).
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Li N, Chen G, Zeng P, Pang J, Gong H, Han Y, et al. Prevalence of depression and its associated factors among Chinese elderly people: a comparison study between community-based population and hospitalized population. Psychiatry Res. (2016) 243:87–91. doi: 10.1016/j.psychres.2016.05.030
2. Chollet F, Cramer SC, Stinear C, Kappelle LJ, Baron JC, Weiller C, et al. Pharmacological therapies in post stroke recovery: recommendations for future clinical trials. J Neurol. (2014) 261:1461–8. doi: 10.1007/s00415-013-7172-z
3. Jorn C, Ute L. Adapted psychotherapy for suicidal geriatric patients with depression. BMC Psychiatry. (2018) 18:203. doi: 10.1186/s12888-018-1775-y
4. Qin BY Dai LL, Zheng Y. Efficacy of repetitive transcranial magnetic stimulation for alleviating clinical symptoms and suicidal ideation in elderly depressive patients: a randomized controlled trial. Nan Fang Yi Ke Da Xue Xue Bao. (2017) 37:97–101. doi: 10.3969/j.issn.1673-4254.2017.01.18
5. Chan ASW, Lo IPY, Yan E. Health and social inclusion: the impact of psychological well-being and suicide attempts among older men who have sex with men. Am J Men's Health. (2022) 16:15579883221120985. doi: 10.1177/15579883221120985
6. National Bureau of Statistics of People's Republic of China. China Population Census Yearbook. Beijing: China Statistics Press (2020).
7. World Health Statistics. Monitoring Health for the SDGs. Boston, MA: World Health Statistics (2018).
8. Chan ASW, Ho JMC, Tam HL, Hsu WL, Tang PMK. COVID-19, SARS, and MERS: the risk factor associated with depression and its impact on psychological well-being among sexual moralities. J Psychiatry Behav Sci. (2022) 5:1073.
9. Chan A, Ho J, Li J, Tam HL, Tang P. Impacts of COVID-19 pandemic on psychological well-being of older chronic kidney disease patients. Front Med. (2021) 8:666973. doi: 10.3389/fmed.2021.666973
10. Chan ASW, Ho JMC, Tam HL, Tang PMK. Book review: successful aging: a neuroscientist explores the power and potential of our lives. Front Psychol. (2021) 2234:705368. doi: 10.3389/fpsyg.2021.705368
11. Ho JMC, Chan ASW, Luk CY, Tang PMK. Book review: the body keeps the score: brain, mind, and body in the healing of trauma. Front Psychol. (2021) 2021:2383. doi: 10.3389/fpsyg.2021.704974
12. Schwarzbach M, Luppa M, Forstmeier S, König HH, Riedel-Heller SG. Social relations and depression in late life-a systematic review. Int J Geriatr Psychiatry. (2014) 29:1–21. doi: 10.1002/gps.3971
13. Gariépy G, Honkaniemi H, Quesnel-Vallée A. Social support and protection from depression: a systematic review of current findings in Western countries. Br J Psychiatry J Mental Sci. (2016) 209:284–93. doi: 10.1192/bjp.bp.115.169094
14. Werner-Seidler A, Afzali MH, Chapman C, Sunderland M, Slade T. The relationship between social support networks and depression in the 2007 national survey of mental health and well-being. Soc Psychiatry Psychiatr Epidemiol. (2017) 52:1463–73. doi: 10.1007/s00127-017-1440-7
15. Marie YS, Montgomery RJ, Kosloski K. A dimensional analysis of caregiver burden among spouses and adult children. Gerontologist. (2011) 51:321–31. doi: 10.1093/geront/gnq102
16. Fingerman KL, Sechrist J, Birditt K. Changing views on intergenerational ties. Gerontology. (2013) 59:64–70. doi: 10.1159/000342211
17. Tang S, Yang T, Ye C, Liu M, Gong Y, Yao L, et al. Research on grandchild care and depression of Chinese older adults based on CHARLS2018: the mediating role of intergenerational support from children. BMC Public Health. (2022) 22:137. doi: 10.1186/s12889-022-12553-x
18. Åhlin J, Hallgren M, Öjehagen A, Källmén H, Forsell Y. Adults with mild to moderate depression exhibit more alcohol related problems compared to the general adult population: a cross sectional study. BMC Public Health. (2015) 15:542. doi: 10.1186/s12889-015-1837-8
19. Van de Velde S, Bracke P, Levecque K. Gender differences in depression in 23 European countries. Cross-national variation in the gender gap in depression. Soc Sci Med. (2010) 71:305–13. doi: 10.1016/j.socscimed.2010.03.035
20. Roh HW, Lee Y, Lee KS, Chang KJ, Kim J, Lee SJ, et al. Frequency of contact with non-cohabitating adult children and risk of depression in elderly: a community-based 3-year longitudinal study in Korea. Arch Gerontol Geriatr. (2015) 60:183–9. doi: 10.1016/j.archger.2014.09.007
21. Teixeira AR, Wender MH, Gonçalves AK, Freitas C, Santos AM, Soldera CL. Dizziness, physical exercise, falls, and depression in adults and the elderly. Int Arch Otorhinolaryngol. (2016) 20:124–31. doi: 10.1055/s-0035-1566304
22. Bonsang E, Bordone V. The effect of informal care from children on cognitive functioning of older parents. Develop Utilisat Hum Resour Semin Ser. (2013) 8:1–35. doi: 10.2139/ssrn.2251784
23. He G, Xie JF, Zhou J-D, Zhong Z-Q, Qin C-X, Ding S-Q. Depression in left-behind elderly in rural China: prevalence and associated factors. Geriatr Gerontol Int. (2016) 16:638–43. doi: 10.1111/ggi.12518
24. Abolfathi Momtaz Y, Ibrahim R, Hamid TA. The impact of giving support to others on older adults' perceived health status. Psychogeriat Off J Jpn Psychogeriat Soc. (2014) 14:31–7. doi: 10.1111/psyg.12036
25. Xiong B, Shi R. How intergenerational relationship influences intergenerational support in Chinese family: based on the perspective of the elderly parents. Populat J. (2016) 5:102–11. doi: 10.16405/j.cnki.1004-129X.2016.05.011
26. Huang Q, Hu Y, Chen G. Effects of intergenerational support on health among elderly: a study based on the perspective of social exchange theory. Populat Develop. (2017) 23:43–5. doi: 10.3969/j.issn.1674-1668.2017.01.005
27. Yang J, Ariela L, Todd J, Yong Z. Intergenerational latent solidarity class and relationship quality among Chinese: implications for self-reported health and well-being. Acta Psychol Sin. (2013) 45:811–24. doi: 10.3724/SP.J.1041.2013.00811
28. Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D. Am J Prev Med. (1994) 10:77–84. doi: 10.1016/S0749-3797(18)30622-6
29. Liu Y-G, Wang C-C, Huang Q, Zhang L, Liu Y. Association of vision and hearing status with depressive symptoms among middle-aged and older Chinese adults [Original Research]. Front Public Health. (2022) 10:857307. doi: 10.3389/fpubh.2022.857307
30. Qingbo H, Xiaohua W, Gong C. Reliability and validity of 10-item CES-D among middle aged and older adults in China. China J Health Psychol. (2015) 7:1036–41. doi: 10.13342/j.cnki.cjhp.2015.07.023
31. Köhler CA, Evangelou E, Stubbs B, Solmi M, Veronese N, Belbasis L, et al. Mapping risk factors for depression across the lifespan: an umbrella review of evidence from meta-analyses and Mendelian randomization studies. J Psychiatr Res. (2018) 103:189–207. doi: 10.1016/j.jpsychires.2018.05.020
32. Fernandez-Rodrigues V, Sanchez-Carro Y, Lagunas LN, Rico-Uribe LA, Pemau A, Diaz-Carracedo P, et al. Risk factors for suicidal behavior in late-life depression: a systematic review. World J Psychiatry. (2022) 12:187–203. v12.i1.187. doi: 10.5498/wjp.v12.i1.187
33. O'Brien RM. A caution regarding rules of thumb for variance inflation factors. Qual Quant. (2007) 41:673–90. doi: 10.1007/s11135-006-9018-6
34. Hosmer DW, Hosmer T, Le Cessie S, Lemeshow S. A comparison of goodness-of-fit tests for the logistic regression model. Stat Med. (1997) 16:965–80. doi: 10.1002/(SICI)1097-0258(19970515)16:9<965::AID-SIM509>3.0.CO;2-O
35. Li C, Jiang S, Zhang X. Intergenerational relationship, family social support, and depression among Chinese elderly: a structural equation modeling analysis. J Affect Disord. (2019) 248:73–80. doi: 10.1016/j.jad.2019.01.032
36. Lowenstein A, Katz R, Gur-Yaish N. Reciprocity in parent-child exchange and life satisfaction among the elderly: a cross-national perspective. J Soc Issues. (2007) 63:865–83. doi: 10.1111/j.1540-4560.2007.00541.x
37. Antonucci TC, Ajrouch KJ, Manalel JA. Social relations and technology: continuity, context, and change. Innovat Aging. (2017) 1:igx029. doi: 10.1093/geroni/igx029
38. Antonucci TC, Ajrouch KJ, Birditt KS. The convoy model: explaining social relations from a multidisciplinary perspective. Gerontologist. (2014) 54:82–92. doi: 10.1093/geront/gnt118
39. Huang H, Zhang L. Present situation and thinking of various pension modes and service technologies. Chin J Gerontol. (2021) 41:203–7. doi: 10.3969/j.issn.1005-9202.2021.01.057
40. Amato P, Booth A. A generation at risk: growing up in an era of family upheaval. By Paul R Amato Alan Booth Soc Forces. (1999) 78:396–7. doi: 10.2307/3005818
42. World Health Statistics. Depression and Other Common Mental Disorders, Global Health Estimates. Boston, MA: World Health Statistics (2017).
Keywords: intergenerational exchange pattern, intergenerational relationship quality, active aging, the elderly, depressive symptoms
Citation: Zheng R, Yu M, Huang L, Wang F, Gao B, Fu D, Zhu J and Liu G (2022) Effect of intergenerational exchange patterns and intergenerational relationship quality on depressive symptoms in the elderly: An empirical study on CHARLS data. Front. Public Health 10:1009781. doi: 10.3389/fpubh.2022.1009781
Received: 02 August 2022; Accepted: 16 September 2022;
Published: 03 October 2022.
Edited by:
Alex Siu-Wing Chan, Hong Kong Polytechnic University, Hong Kong SAR, ChinaReviewed by:
Mei Chi Jacqueline Ho, Hong Kong Polytechnic University, Hong Kong SAR, ChinaCopyright © 2022 Zheng, Yu, Huang, Wang, Gao, Fu, Zhu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinghui Zhu, emh1amhAd211LmVkdS5jbg==; Guilin Liu, Z3VpbGlubGl1ODhAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.