 Alain-Claude Kouamen1†‖Helena Da Cruz2†Mohamed Hamidouche3†Anais Lamy4†Anna Lloyd5†
Alain-Claude Kouamen1†‖Helena Da Cruz2†Mohamed Hamidouche3†Anais Lamy4†Anna Lloyd5† Javier Castro Alvarez1Mathilde Roussel6
Javier Castro Alvarez1Mathilde Roussel6 Laurence Josset7Vincent Enouf8Charlotte Felici9
Laurence Josset7Vincent Enouf8Charlotte Felici9 Georges Dos Santos10Justine Schaeffer1‖
Georges Dos Santos10Justine Schaeffer1‖ Anna Maisa1*‖Regional COVID-19 Investigation Group‡Laboratory Group§
Anna Maisa1*‖Regional COVID-19 Investigation Group‡Laboratory Group§- 1Department of Infectious Diseases, Santé Publique France, Direction des maladies infectieuses, Saint-Maurice, France
- 2Bourgogne-Franche-Comté Regional Office, Santé publique France, Dijon, France
- 3Île-de-France Regional Office, Santé publique France, Paris, France
- 4Nouvelle-Aquitaine Regional Office, Santé publique France, Bordeaux, France
- 5Auvergne-Rhône-Alpes Regional Office, Santé publique France, Lyon, France
- 6Cerba, Cerba HealthCare, Saint-Ouen-l'Aumône, France
- 7National Reference Center for Respiratory Viruses, Hospices Civils de Lyon, CIRI, INSERM U1111, Université Claude Bernard Lyon 1, Lyon, France
- 8National Reference Center for Respiratory Viruses, Molecular Genetics of RNA Viruses, UMR 3569 CNRS, University of Paris, Institut Pasteur, Paris, France
- 9EspaceBio, Ouilab, Laxou, France
- 10Service de Virologie, CHU Martinique, Fort-de-France, Martinique
Aim: We aimed to describe the characteristics of individuals infected by BA.4 or BA.5 in France in comparison to BA.1, and analyze the factors associated with hospitalization among BA.4 and BA.5 cases.
Methods: A standardized questionnaire was used to collect information on confirmed and probable Omicron cases. Hospitalization risk factors among BA.4/BA.5 cases were analyzed using Poisson regression. Variables with a p-value below 0.2 in the univariate analysis and a priori confounders were included in the multivariable regression model.
Results: The median age of the 301 cases investigated was 47 years and 97% of cases were symptomatic. The most common clinical signs were asthenia/fatigue (75.7%), cough (58.3%), fever (58.3%), headache (52.1%) and rhinorrhea (50.7%). Twelve cases were hospitalized, and 27.1% reported risk factors. No admissions to intensive care and no deaths were reported. Vaccination status was available for 292 cases, 20.9% were unvaccinated, 1.4% had received one dose, 38.3% two doses and 39.4% three doses. Cases presenting at least one risk factor were almost seventeen times more likely to be hospitalized than those with no risk factors (aRR = 16.72 [95% CI2.59–326.86]).
Conclusion: Despite the longer duration of and the differences in symptoms and their possible immune escape, BA.4/BA.5 Omicron sub-lineages globally showed no severe clinical presentation. The presence of at least one risk factor for severe disease significantly increased the risk of hospitalization for those infected with BA.4 or BA.5.
Introduction
At the end of 2021, the SARS-CoV-2 Delta variant was replaced by Omicron (B.1.1.529), which was classified as a variant of concern by the World Health Organization (1). Omicron showed major differences compared to previous variants, including increased transmissibility, high immune escape, different clinical presentation (less anosmia and ageusia) and lower severity (2). Omicron's BA.1 sub-lineage became predominant in France in December 2021 and later gave way to new Omicron sub-lineages, such as BA.2, BA.4 and BA.5. Since April 2022, the number of BA.4 and BA.5 cases has been increasing, coinciding with an increased incidence rate, and by mid-June, these two sub-lineages combined represented more than half of all cases.
We aimed to describe the characteristics of individuals infected by BA.4 or BA.5 in France in comparison to BA.1, and analyze the factors associated with hospitalization among BA.4 and BA.5 cases. The purpose of these investigations was to produce early data that could inform public health decisions regarding these emerging variants.
Methods
Between 6 April and 10 June 2022, 277 confirmed cases (by sequencing) and 24 possible cases (linked to a confirmed case) of BA.4 or BA.5 (designated BA.4/BA.5 for the following text) were investigated by epidemiologists from the regional offices of Santé publique France in collaboration with the Regional Health Agencies. A standardized questionnaire was used as for the previously investigated 468 Omicron cases between November 2021 and January 2022 (>99% BA.1) (3). Hospitalization risk factors among BA.4/BA.5 cases were analyzed using Poisson regression. Predictors with a p-value below 0.2 in the univariate analysis (Table 2) and age and sex as a priori confounders were included in the multivariable regression model.
Results
Characteristics of BA.4/BA.5 cases compared to BA.1
The 301 cases of BA.4/BA.5 were distributed within 16 out of 18 regions of France (including three overseas regions). Median age was 47 years (interquartile range (IQR) 30–58, range 1–97; Figure 1, left panel), compared to 35 for BA.1 cases. Moreover, the proportion of BA.4/BA.5 cases over 70 years old (15.5%) was significantly higher than that of BA.1 cases (2.7%, p < 0.001). The sex ratio was 0.7 (Table 1).
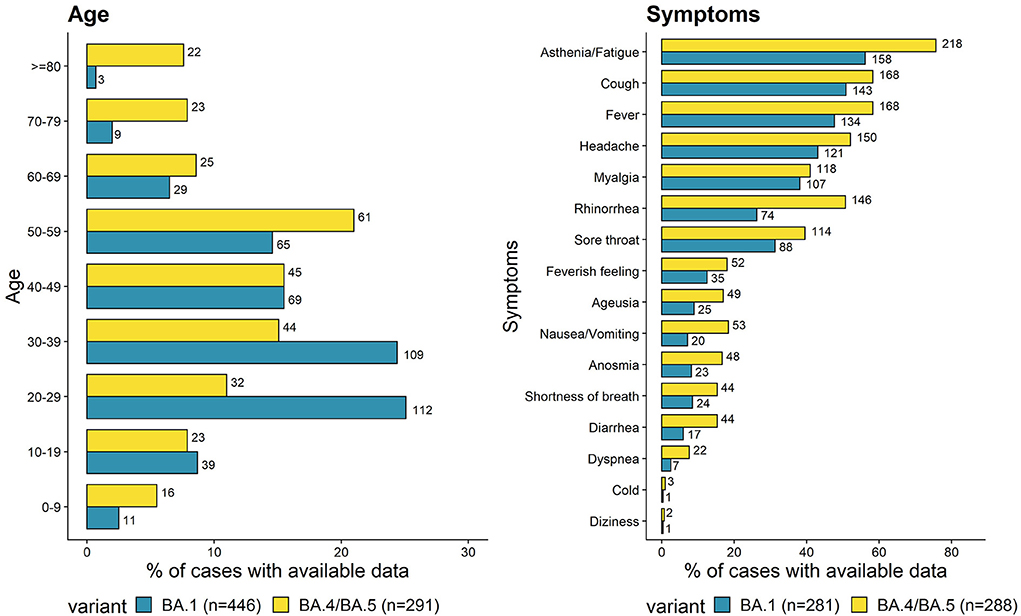
Figure 1. Proportion of age groups (left panel) and symptoms (right panel) of BA.4/BA.5 cases compared to previously investigated BA.1 cases. Absolute numbers of cases are shown beside the bars.
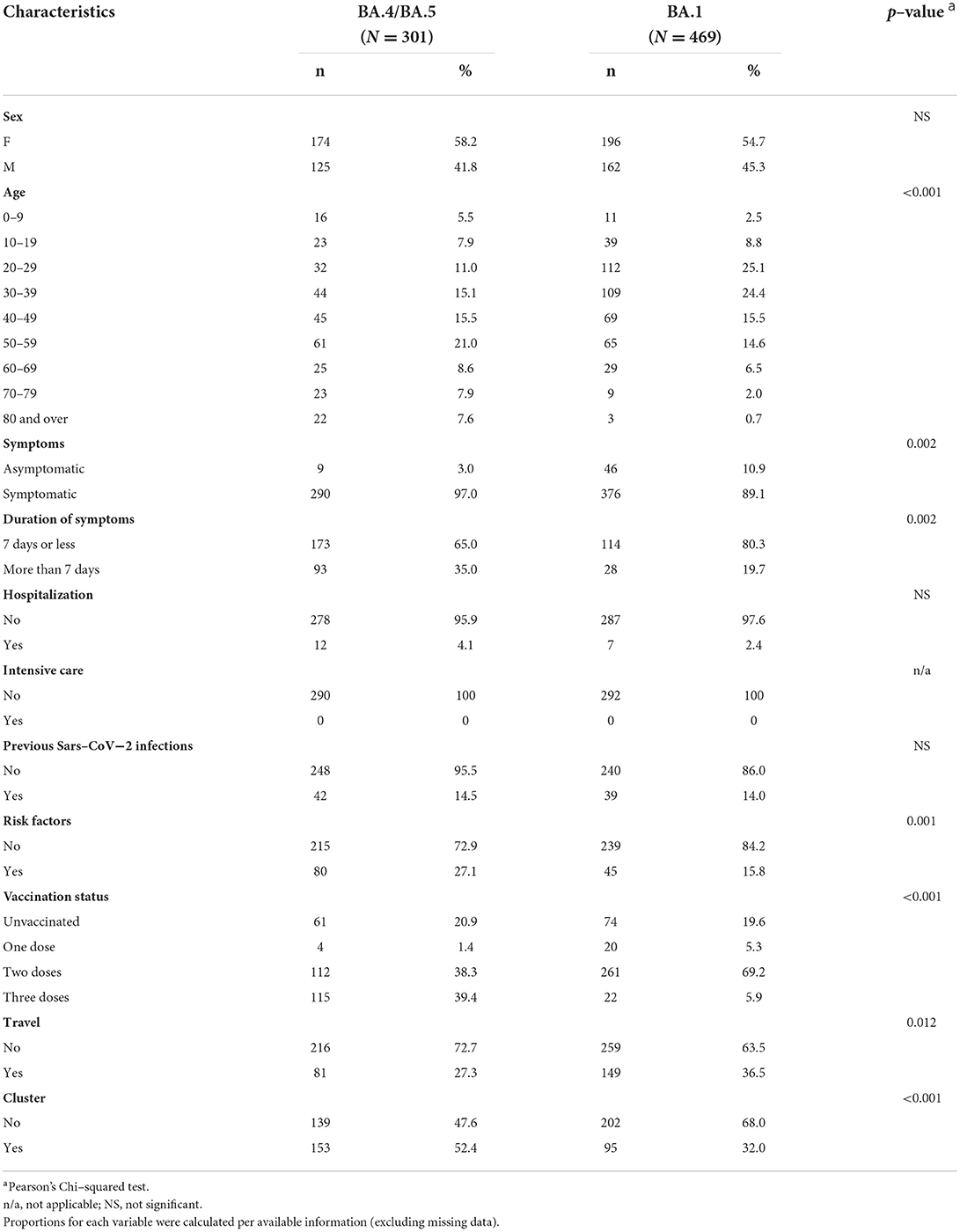
Table 1. Characteristics of confirmed (by sequencing) or possible (linked to a confirmed case) cases of infection by BA.4/BA.5 and comparison with BA.1 cases.
Almost all BA.4/BA.5 cases were symptomatic (97%), which was significantly higher than for BA.1 cases (89.1%, p < 0.001) and may be explained by changes in testing policies and behavior. The most common clinical signs were asthenia/fatigue (75.7%), cough (58.3%), fever (58.3%), headache (52.1%) and rhinorrhea (50.7%, Figure 1, right panel). BA.4/BA.5 cases were more likely to report rhinorrhea (odds ratio (OR) = 1.79, [confidence interval at 95% (95% CI) 1.22–2.63]), nausea/vomiting (OR = 2.39, [95% CI 1.36–4.34]), diarrhea (OR = 2.33, [95% CI 1.27–2.43]), ageusia (OR = 1.77, [95% CI 1.02–3.10]), and anosmia (OR = 1.88, [95% CI 1.08–3.36]) than BA.1 cases. The median duration of symptoms was 7 days (IQR 3–10 days), which was longer than for BA.1 cases [4 days (IQR 2–7 days)].
Among the investigated BA.4/BA.5 cases, 12 hospitalizations and no critical care admissions or deaths were reported. The hospitalization rate was not significantly higher for BA.4/BA.5 compared to BA.1. A significantly higher proportion of BA.4/BA.5 cases had at least one risk factor for severe COVID-19, such as hypertension, diabetes, heart disease, kidney disease, respiratory illness, immunosuppression, obesity, cancer, neuromuscular disease, and/or pregnancy (27.1% vs. 15.8% of BA.1, p = 0.001). The median length of hospitalization was 5 days (IQR 2–16 days).
Travel history or contact with a person having traveled within 14 days preceding their positive SARS-CoV-2 test was reported for 81 BA.4/BA.5 cases (27.3%). Among them, 37 were linked to Portugal and 6 to South Africa. More than half of the investigated cases were associated with clusters (epidemiologically linked SARS-CoV-2 cases).
In addition, 42 cases of BA.4/BA.5 reported a previous SARS-CoV-2 infection (14.5%, Table 1), similar to BA.1 (14.0%, p = 0.96). The median time between previous infection and date of BA.4/BA.5 positive test was 257 days (IQR 117–569 days). Vaccination status was available for 292 cases: 20.9% were unvaccinated (30% of those were <12 years old), 1.4% had received one dose, 38.3% two doses and 39.4% three doses. The proportion of triple vaccinated individuals infected by BA.4/BA.5 was significantly higher compared to BA.1 cases (39.4% vs. 5.9%, p < 0.001), which may reflect the different investigation periods (April-May 2022 for BA.4/BA.5, November 2021-January 2022 for BA.1) and the increased vaccine uptake in the population for the third dose after September 2021. The median time between date of the administration of the last dose and positive test was 167 days (IQR 126–310 days).
Risk factors for hospitalization due to BA.4/BA.5
Hospitalization risk factors among BA.4/BA.5 cases were analyzed using Poisson regression. After adjusting for age, sex and vaccination status, patients presenting at least one risk factor were almost seventeen times more likely to be hospitalized than those with no risk factors (aRR = 16.72 [95% CI 2.59–326.86]; Table 2).
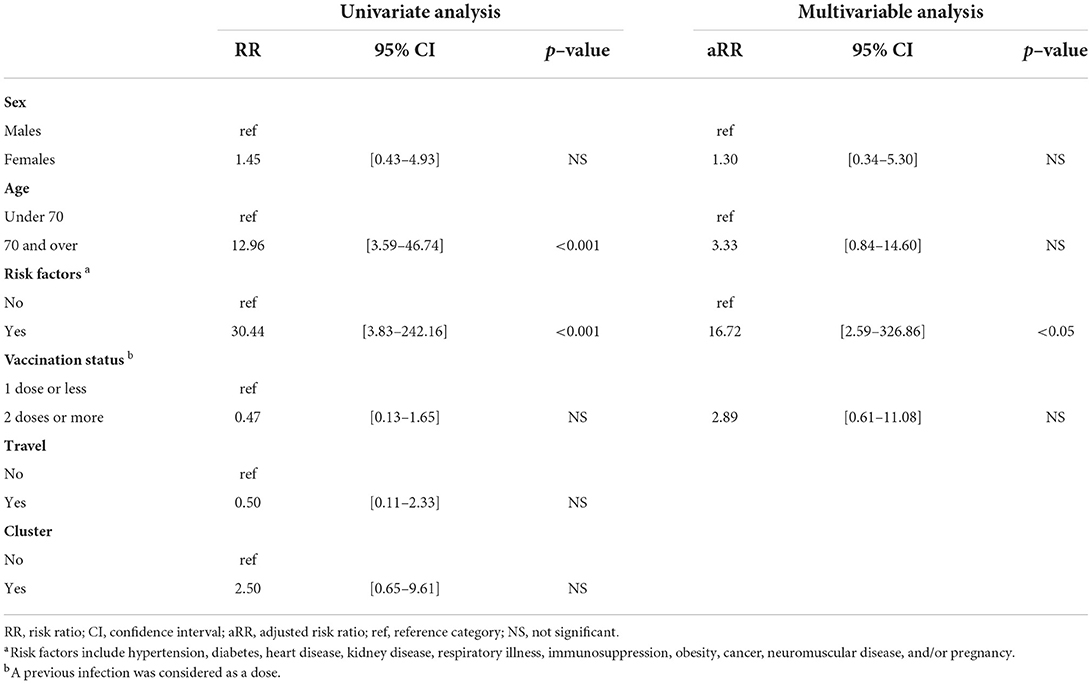
Table 2. Univariate and multivariate analysis for risk of hospitalization among BA.4 and BA.5 cases.
Discussion
In comparison to BA.1, our investigation shows that the first BA.4/BA.5 cases in France were significantly older, less likely to have traveled during the 14 days preceding the positive test, more likely to be related to a cluster, and more likely to have risk factors. BA.4/BA.5 cases had significantly longer median duration of symptoms, and were significantly more likely to develop rhinorrhea, nausea/vomiting, diarrhea, ageusia and anosmia. The hospitalization rate was not significantly different compared to BA.1.
The current increase of cases in France coincides with a spread of mostly BA.5 (4), as previously observed in other countries (5). The replacement of BA.2 by BA.4/BA.5 illustrates a growth advantage, which could be due to higher transmissibility and/or immune evasion (6). Increased case numbers might have been due to BA.4/BA.5, as well as changes in population behavior, waning immunity (7, 8) and relaxation of prevention measures (9). In addition, elderly have been vaccinated earlier with a third dose than younger individuals, hence waning immunity in this population is expected (10) and may have contributed to more infections in higher age groups during the BA.4/BA.5 wave.
The investigation periods for BA.1 and BA.4/BA.5 differ by the increase of vaccination coverage for the third dose and an easing of preventive measures, which may have led to different infection patterns regarding clusters and vaccinated individuals.
The hospitalization rate among BA.4/BA.5 cases was only significantly related to risk factors for severe COVID-19, as reported previously (5, 11). A higher proportion of BA.4/BA.5 cases were symptomatic with different clinical signs and a longer median duration of symptoms than observed for BA.1.
Most cases investigated were symptomatic, which could be due to changes in testing behaviors (lower adherence to testing recommendations); hence, the proportion of hospitalizations for BA.4/BA.5 infections might be overestimated compared to hospitalizations for BA.1. Small numbers of hospitalized cases in both groups also lowered the statistical power of the analysis. Nevertheless, our study found similar disease severity between BA.4/BA.5 and BA.1 as reported recently from South Africa (12). These investigations included as a reference only individuals infected by BA.1 and not BA.2, which had followed and overtaken BA.1. However, while Omicron sub-lineages have shown varying competitiveness, no major differences in vaccine effectiveness, severity and clinical presentation have been identified so far.
Conclusion
Despite the longer duration of and the differences in symptoms and their possible immune escape, BA.4/BA.5 Omicron sub-lineages globally showed no severe clinical presentation. This is similar to other Omicron sub-lineages, and their impact on public health could remain limited. However, an increase in case numbers of these more transmissible sub-lineages may still lead to a high burden of absenteeism and hospitalizations.
Caution is required and continued vaccination efforts and adhesion to prevention measures are necessary to reduce the spread and impact of these variants. The French public health system through the EMERGEN Consortium, local, regional and national authorities, maintains its ability to quickly detect, react and adapt to the emergence of a new variant.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Collaborators
Members of the Regional COVID-19 Investigation Group: Gwenola Picard (Santé publique France, Rennes); Michée Géraud Vikpognon (Santé publique France, Orléans); Alice Brembilla (Santé publique France, Nancy); Ellen Dahl (Santé publique France, Cayenne); Souhaila Chent (Santé publique France, Lille); Alizé Mercier (Santé publique France, Saint-Denis, La Réunion); Gwladys Nadia Gbaguidi (Santé publique France, Fort-de-France, Martinique); Carine Grenier (Santé publique France, Rouen); Adeline Riondel (Santé publique France, Montpellier); Caroline Huchet-Kervella (Santé publique France, Nantes); Leila Bekheira (Santé publique France, Marseille)
Members of the Laboratory group—Stephan Kemeny (Inovie Gen-Bio); Claire Vignault (Laborizon Center-Biogroup); Pauline Trémeaux (CHU Toulouse); Pierre-Edouard Fournier (APHM); Sophie Vallet (CHU Brest); Vincent Thibault (CHU Rennes); Diane Descamps (APHP-Bichat); Lionel Chollet (CHI Toulon); Nefert Dossou (CHU Caen); Alice Moisan (CHU Rouen); Anais Soares (Eurofins Biomnis); Marie Christine Jaffar Bandjee (CHU Réunion); Alexis de Rougemont (CHU Dijon); Cécile Henquell (CHU Clermont Ferrand); Anne Lavergne (CNR Virus des infections respiratoires, laboratoire associé, Institut Pasteur de la Guyane, Cayenne)
Author contributions
A-CK, HD, MH, ALa, and ALl wrote the manuscript. A-CK, JS, and AM were involved in the study design, coordination and interpretation. HD, MH, ALa, ALl, and the COVID-19 Investigation Group investigated BA.4/BA.5 and Omicron cases. A-CK, HD, MH, ALa, ALl, JS, and AM participated in data analysis and interpretation. MR, LJ, VE, CF, and GD critically reviewed the manuscript and participated in data interpretation. MR, GD, and authors from the Laboratory group provided sequencing results for this study. JS and AM coordinated this work. All authors reviewed this manuscript.
Funding
This work was funded by Santé publique France, the French national public health agency; the Caisse nationale d'assurance maladie (Cnam), the national health insurance funds; and the Enhancing Whole Genome Sequencing (WGS) and/or Reverse Transcription Polymerase Chain Reaction (RT-PCR) national infrastructures and capacities to respond to the COVID-19 pandemic in the European Union and European Economic Area Grant Agreement ECDC/HERA/2021/007 ECD. 12221.
Acknowledgments
We would like to thank all EMERGEN partners for their efficient monitoring of SARS-CoV-2 variants in France. We would like to acknowledge especially Bruno Coignard and Anne Bozorgan for their daily work in coordinating this network and their valuable input on this study; and Jeanne Sudour and Maël Pretet for their support concerning data analysis. Genomic surveillance would not be possible without the involvement of diagnostic laboratories who voluntarily select and send their samples for sequencing. We are also immensely grateful to the French Bioinformatics Institute (Institut Français de Bioinformatique, IFB) for the construction, maintenance and continuous improvement of the EMERGEN database.
We would like to acknowledge the tireless work of the regional health authorities and the clinicians, who have contributed to the sample and data collection, as well as the individuals interviewed for this investigation. We also thank Guillaume Spaccaferri for his help in developing the questionnaire and coordinating case investigations, and Joël Deniau for the efficient data collection tools he designed.
Our final thanks go to our partners at the National Reference Center for Respiratory Viruses, especially Sylvie van der Werf and Bruno Lina, for their immense expertise and their precious support in all of our activities.
This data has been previously published in French in the monthly variants risk analysis on 17 June 2022 by Santé publique France and the National Reference Center for Respiratory Viruses (https://www.santepubliquefrance.fr/dossiers/coronavirus-covid-19/coronavirus-circulation-des-variants-du-SARS-CoV-2).
Conflict of interest
Author MR was employed by Cerba HealthCare.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. WHO. Tracking SARS-CoV-2 Variants. (2022). Available online at: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed July 11, 2022).
2. Nyberg T, Ferguson NM, Nash SG, Webster HH, Flaxman S, Andrews N, et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B. 11529) and delta (B16172) variants in England: a cohort study. Lancet. (2022) 399:1303–12. doi: 10.1016/S0140-6736(22)00462-7
3. Maisa A, Spaccaferri G, Fournier L, Schaeffer J, Deniau J, Rolland P, et al. First cases of Omicron in France are exhibiting mild symptoms, November 2021-January 2022. Infect Dis Now. (2022) 52:160–4. doi: 10.1016/j.idnow.2022.02.003
4. Santé, publique France. COVID-19: point épidémiologique du 30 juin 2022. Available online at: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/infection-a-coronavirus/documents/bulletin-national/covid-19-point-epidemiologique-du-30-juin-2022 (accessed July 13, 2022).
5. ECDC. Implications of the emergence and spread of the SARS-CoV-2 variants of concern BA.4 and BA.5 for the EU/EEA. 14 June 2022. ECDC: Stockholm.(2022).
6. UKHSA. SARS-CoV-2 variants of concern and variants under investigation in England, Technical Briefing 43–28/06/2022. 2022. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1086494/Technical-Briefing-43-28.06.22.pdf (accessed July 6, 2022).
7. Goldberg Y, Mandel M, Bar-On Bar-On YM, Bodenheimer O, Freedman LS, Ash N, et al. Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. New Eng J Med. (2022) 386:2201–12. doi: 10.1056/NEJMoa2118946
8. Tegally H, Moir M, Everatt J, Giovanetti M, Scheepers C, Wilkinson E, et al. Emergence of SARS-CoV-2 Omicron lineages BA.4 and BA.5 in South Africa. Nat Med. (2022). doi: 10.1038/s41591-022-01911-2. [Epub ahead of print].
9. Service publique français. COVID 19 Obligation de port du masque: quelles sont les règles ?; 2022. Available online at: https://www.service-public.fr/particuliers/vosdroits/F35351 (accessed July 13, 2022).
10. Santé publique France. COVID-19: point épidémiologique du 9 décembre 2021. 2022 09/12/2021. Available online at: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/infection-a-coronavirus/documents/bulletin-national/covid-19-point-epidemiologique-du-9-decembre-2021 (accessed July 13, 2022).
11. WHO. Weekly epidemiological update on COVID-19–29 June 2022. (2022). Available online at: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19———29-june-2022 (accessed July 13, 2022).
12. Davies M-A, Morden E, Rosseau P, Arendse J, Bam J-L, Boloko L, et al. Outcomes of laboratory-confirmed SARS-CoV-2 infection during resurgence driven by Omicron lineages BA.4 and BA.5 compared with previous waves in the Western Cape Province, South Africa. medRxiv. 2022:2022.06.28.22276983. doi: 10.1101/2022.06.28.22276983
Keywords: SARS-CoV-2, variant, Omicron, hospitalization, symptoms, BA.4, BA.5
Citation: Kouamen A-C, Da Cruz H, Hamidouche M, Lamy A, Lloyd A, Castro Alvarez J, Roussel M, Josset L, Enouf V, Felici C, Dos Santos G, Schaeffer J, Maisa A, Regional COVID-19 Investigation Group and Laboratory Group (2022) Rapid investigation of BA.4/BA.5 cases in France. Front. Public Health 10:1006631. doi: 10.3389/fpubh.2022.1006631
Received: 29 July 2022; Accepted: 16 September 2022;
Published: 10 October 2022.
Edited by:
Eduardo Rodriguez-Noriega, Civil Hospital of Guadalajara, MexicoReviewed by:
Pamela Davis, Case Western Reserve University, United StatesAbraham Campos-Romero, Salud Digna A.C., Mexico
Raghda Eldesouki, Johns Hopkins Medicine, United States
Cathrine Scheepers, National Institute of Communicable Diseases (NICD), South Africa
Copyright © 2022 Kouamen, Da Cruz, Hamidouche, Lamy, Lloyd, Castro Alvarez, Roussel, Josset, Enouf, Felici, Dos Santos, Schaeffer, Maisa, Regional COVID-19 Investigation Group and Laboratory Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna Maisa, YW5uYS5tYWlzYUBzYW50ZXB1YmxpcXVlZnJhbmNlLmZy
†These authors have contributed equally to this work and share first authorship
‡The members of the regional COVID-19 Investigation Group are listed under Collaborators
§The members of the Laboratory Group are listed under Collaborators
‖ORCID: Alain-Claude Kouamen orcid.org/0000-0003-1433-5947
Justine Schaeffer orcid.org/0000-0003-4311-3294
Anna Maisa orcid.org/0000-0002-8372-7525