 Ayesha Mumtaz
Ayesha Mumtaz Erum Rehman
Erum Rehman Shazia Rehman4*
Shazia Rehman4* Iftikhar Hussain
Iftikhar Hussain
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 20 January 2022
Sec. Environmental Health and Exposome
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.812743
This article is part of the Research TopicPublic Health, Governance, Green Environment and EconomyView all 45 articles
Air pollution has emerged as a major global concern in recent decades as a result of rapid urbanization and industrialization, leading to a variety of adverse health outcomes. This research aims to investigate the influence of exposure to ambient and household particulate matter pollution (PM2.5), and ground-level ozone (O3) pollution on respiratory and cardiac mortality in Pakistan. We used grey incidence analysis (GIA) methodology to estimate the degree of proximity among selected variables and rank them based on mortality. Hurwicz's criterion is then adopted for further optimization by prioritizing the selected factors with the greatest influence on respiratory and cardiac mortality. The GIA findings revealed that asthma mortality is considerably impacted by exposure to ambient and household PM2.5 concentration while ischemic heart disease (IHD) mortality is potentially influenced by ground-level ozone exposure. Furthermore, results based on Hurwicz's analysis demonstrated that exposure to ambient PM2.5 concentration appeared as the most intensified factor of respiratory and cardiac mortality. This corroboration adds to the growing body of research demonstrating that exposure to ambient PM2.5 adversely leads to respiratory and cardiac risks, emphasizing the demand for further improvement of air quality in Pakistan. Besides, the suggested methodologies provide a valuable tool and additional practical knowledge for policymakers and decision-makers in drawing rational decisions.
Pakistan as a developing nation had the fifth-most polluted air in world in 2016, and positioned second in 2019 (1), owing to the same factors that plague much of South Asia: emanations from automobiles, industrial activities, such as block furnaces, industries, and power stations, and agricultural waste. This degree of air pollution is sabotaging well-being of Pakistanis, lowering down the median life expectancy by 2.7 years, comparative with what it would be if the WHO recommendation of 10 μg/m3 for long-term fine particulate matter (PM2.5) pollution was reached; and 2.2 years compared with the country's air quality benchmark of 15 μg/m3 (2). In 2016, 98% of population of Pakistan (nearly 200 million) resided in regions where yearly average PM2.5 pollution levels surpassed guidelines of the WHO. About 97% of the population inhabited regions where PM2.5 levels were higher than the threshold of country. PM2.5 concentrations have surged by 54% since 1998, leading to these high levels (3, 4).
The pathophysiologic effects of PM2.5 and O3 exposures in pulmonary systems have been widely studied, and it is evident that these particles can trigger and aggravate lungs infection in humans (5, 6). As the pulmonary and cardiac systems are complicatedly interconnected, it is conceivable that pulmonary oxidant stress characterized by PM2.5 and/or O3 exposure may cause downstream changes in the cardiovascular system. It is well-evidenced that particular environmental pollutants presented through the lungs can trigger and/or stimulate the development of cardiovascular disease (CVD) (7). However, many epidemiologic investigations have confirmed a strong link between PM2.5 and O3 and an increased risk of cardiac morbidity and mortality. In Pakistan, evidence comes from case studies revealing substantial variations in the outcomes, however, full-text original research articles are not more than a modest bunch (8–10).
Given its significance, a wealth of research and analytic methodologies are utilized to explore the relationship between disease mortality and exposure to air pollutants across the world. In the Pakistani setting, there is a paucity of evidence relating to air pollutant exposure and the risk of mortality from chronic respiratory disease (CRD) and CVD. The lack of evidence has made it very difficult to assess the real situation in the Pakistani population. In response, the present study attempts to bridge the existing literature gaps by exploring the tie between exposure to ambient PM2.5 concentration, ground-level ozone (O3) exposure, household PM2.5 concentration exposure, and mortality from asthma, chronic obstructive pulmonary disease (COPD), stroke, and ischemic heart disease (IHD) in the Pakistani nation. However, by addressing exposure to PM2.5 (ambient and household) concentration and ground-level ozone with a wide range of disease mortality, we may provide a more dynamic spectrum of the interactions. To explore this association, we deployed a mathematical grey incidence analysis (GIA) modeling of grey system theory (GST) which comprised of Deng degree of GIA (DD-GIA), absolute degree of GIA (AD-GIA), and the second synthetic degree of GIA (SSD-GIA). The GIA models provide many advantages when contrasted with standard statistical models. For instance, they exhibit greater precision and may yield reliable outcomes with small sample size. Second, traditional statistical approaches, such as logistic regression, are inefficient for depicting the relations between variables in the biomedical domain, because of its dependency restrictions (11, 12). The GIA models may overcome this shortcoming as they are devoid of such assumptions. In addition, this study used Hurwicz's criterion to conduct a comparative analysis of all the selected factors and mortality (CRD and CVD) to ascertain which air pollutant is contributing more to mortality. The proposed methodologies are more appropriate when contrasted with other techniques for convincing outcomes and assist with avoiding endogeneity issues. The suggested model provides a valuable tool and additional practical knowledge for policymakers and decision-makers in drawing rational decisions to reduce air pollution and mortality in the Pakistani region. More importantly, this investigation may facilitate researchers with multiple criteria decision-making roadmap to help them enhance the quality of their studies and their understanding of how to use multiple criteria decision analysis (MCDA) techniques to evaluate and prioritize the influencing factors of disease mortality in environmental healthcare research. The visual abstract of the study is presented in Figure 1.
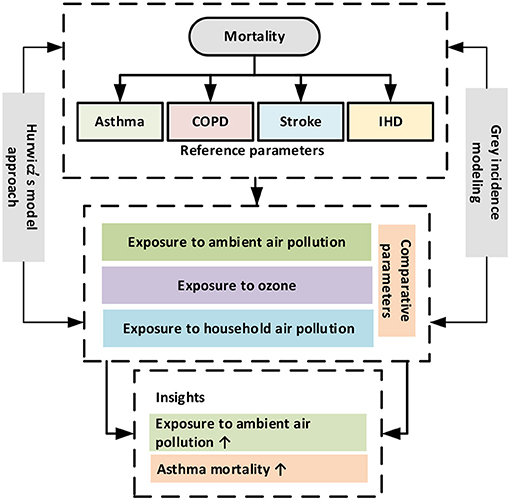
Figure 1. The visual abstract.
For the period 2010–2019, information on the mortality (asthma, COPD, stroke, and IHD) were extracted from the Global Burden of Disease (GBD) study, harmonized by the Institute for Health Metrics and Evaluation (IHME), and is publicly accessible online (13). In addition, population-weighted exposure to ambient PM2.5 concentration (μg/m3), ground-level ozone (O3 in ppb) exposure, and household PM2.5 concentration exposure (μg/m3) abstracted from the State of Global Air report (2010–2019) (14). These parameters are estimated as the average exposure levels of population of country (urban and rural regions) to mean annual concentrations of PM2.5 and O3, separately. To evaluate PM2.5 exposures, the GBD scientist combines the number of people living in a specific region and the PM2.5 concentrations to which they are exposed. To evaluate ozone exposures, they combined the number of people living in a specific region and the surface ozone concentration to which they are exposed. This method determines human exposure to air pollutants in terms of the population-weighted average seasonal 8-h daily maximum concentrations for a specific region.
The data are analyzed by employing GIA methods (DD-GIA, AD-GIA, and SSD-GIA) (15, 16). These models are designed using SPSS (v26, IBM, NY, USA). Additionally, Hurwicz's methodology is employed to hierarchize the risk factors (air pollutants) that have a greater impact on CRD and CVD-related mortality within the Pakistani nation. The present analyses and modeling methods are deployed for the first time in the study to quantify the strength of influence and degree of correlation between selected factors and mortality (asthma, COPD, stroke, and IHD) in a multi-dimensional way. Deng's GIA model was employed to measure the partial closeness (a measure of influence) of the selected variables (ambient and household PM2.5 concentration exposure, ground-level ozone exposure, mortality from CVDs, and CRDs), whereas the bidirectional absolute GIA model was used to evaluate the integral closeness (degree of correlation) of the selected variables. The second synthetic GIA model was performed to obtain an overall estimate (weight) of inclusive proximity by accompanying the methods outlined in. The algorithms involved with the grey methods are explained in the following section.
Let Yi = (yi(1), yi(2), ⋯ , yi(m)) be the basic/reference sequence addressing a dependent variable and Yj = (yj(1), yj(2), ⋯ , yj(m)) be the arrangement of comparative sequences addressing independent variables, in the wake of going through initialing operator then, at that point grey relational gradient (GRG), the real number degree addressing the output of GIA model is depicted as γij or γ(Yi, Yj) and can be accompanied by:
Where,
Here, ζ ϵ (0, 1) represent as a distinguishing coefficient, and its value is generally considered to be ζ = 0.5. The implementation of the Deng's GIA model for evaluating the effect of one parameter/variable on the other has been highlighted in the literature (17, 18).
If Yi = (yi(1), yi(2), ⋯ , yi(m)) and Yj = (yj(1), yj(2), ⋯ , yj(m)) are two data sequences representing two variables associated with a system, then the algorithm to calculate the bidirectional absolute GRG is listed below.
Where,
Next, compute the bidirectional absolute GRG (ϵ±), provided by (19).
Here, the –ve sign addresses an inverse grey relation (i.e., inversely proportional), while the +ve sign addresses a direct grey relation, and the magnitude to which either of these signs is appended indicates the intensities of the grey relation (i.e., degree of integral closeness/proximity).
The SS-GIA model is an approach to estimate SS-GRG and can be acquired by utilizing the accompanying equation.

where ′ ′ stands for the SS-GIA, ′ϵ′ for the absolute GIA, and ′γ′ for the Deng's GIA between the two grey datasets Yi and Yj. When a decision-maker desires a holistic assessment that evenly integrates the benefits of both ′ϵ′and ′γ′ without preferring one over the other and may keep ϑ at 0.5. In the case of preferring is fundamental, then, at that point, the value of ′ϑ′ can be adjusted (20). If one desire to prefer ′γ′, then ′ϑ′ can be diminished, and assuming one desires to prefer ′ϵ,′ then ′ϑ′ can be increased. In the present investigation, we thought of ϑ = 0.5. Furthermore, in the SS-GIA equation, the absolute GIA was substituted by the bidirectional absolute GIA (without taking signs). When the interactions within the frameworks/systems are ambiguous, it is likewise advised that the absolute GIA can be supplanted by the bidirectional absolute GIA. Deng's GIA is established on grey incidence/correlation/relational coefficients of specific points, while absolute GIA is based on an integral (generally far-reaching) perspective, however, the SS-GIA is based on specific points and integral perspectives and shows overall proximity (correlation/closeness) (21, 22).
′ stands for the SS-GIA, ′ϵ′ for the absolute GIA, and ′γ′ for the Deng's GIA between the two grey datasets Yi and Yj. When a decision-maker desires a holistic assessment that evenly integrates the benefits of both ′ϵ′and ′γ′ without preferring one over the other and may keep ϑ at 0.5. In the case of preferring is fundamental, then, at that point, the value of ′ϑ′ can be adjusted (20). If one desire to prefer ′γ′, then ′ϑ′ can be diminished, and assuming one desires to prefer ′ϵ,′ then ′ϑ′ can be increased. In the present investigation, we thought of ϑ = 0.5. Furthermore, in the SS-GIA equation, the absolute GIA was substituted by the bidirectional absolute GIA (without taking signs). When the interactions within the frameworks/systems are ambiguous, it is likewise advised that the absolute GIA can be supplanted by the bidirectional absolute GIA. Deng's GIA is established on grey incidence/correlation/relational coefficients of specific points, while absolute GIA is based on an integral (generally far-reaching) perspective, however, the SS-GIA is based on specific points and integral perspectives and shows overall proximity (correlation/closeness) (21, 22).
The issue of multiple objectives often exists in the problems within systems, increasing the ambiguity of decisions. In this setting, to minimize errors, it is significant to find techniques that include the greatest number of criteria in the decision-making process that direct influence decisions. However, most of the time this technique is not easy to execute, because in many cases the decision-making criteria vary, raising the degree of uncertainty of the final response. In the literature, there are multiple decision-making (MCDM) techniques that facilitate researchers to make decisions and analyze preferred alternatives. These techniques are regarded for a variety of reasons. Researchers believed that the procedure allows visibility, consistency, and precision toward a more reasonable priority setting from a methodological standpoint. In a broader sense, the MCDA application procedure is regarded as an efficient and successful in priority settings. In this regard, the Hurwicz's criterion is one of the most recognized techniques in the literature which integrates a measure of both by giving optimism a specific percentage weight and pessimism the remainder (23). For each action choice, a weighted average with an alpha-weight, known as the coefficient of realism, could be determined. The decision-maker chooses the α subjectively. Determining a value for α concurrently results in a pessimistic coefficient of (1–α), which indicates the sensitivity of decision-makers to risk (23). For each action alternative Bi in B, a Hurwicz's weighted average ‘H’ may now be computed as follows:
H (Bi) = α (row maximum) + (1–α) (row minimum)–for a maximization approach
H (Bi) = α (row minimum) + (1–α) (row maximum)–for a minimization approach
Hurwicz's decision rule is used in the following steps.
1. Determine the value of the optimism coefficient α. Take note that 0 ≤ α ≤ 1.
2. Calculate the Hurwicz weighted average H for each action alternative.
Select the action alternative with the highest H as the final decision (maximum for a maximization problem, and minimum for a minimization problem).
The present investigation is carried out using grey approaches to quantify the strength of association between asthma, COPD, stroke, and IHD mortality with associated risk factors (exposure to ambient PM2.5 concentration, exposure to ground-level ozone, and exposure to household PM2.5 concentration) for the years 2010–2019. Table 1 demonstrates the outcomes of grey models, namely, the Deng's GIA, absolute GIA, and the SS-GIA for respiratory and cardiac mortality with associated risk factors. The absolute GIA and the SS-GIA models have values ranging from 0 to 1, whereas, Deng's GIA has values ranging from 0.5 to 1. It is also considered highly associated if it is near to 1 and weak if it diverges from 1. The graphical representation of the comparative assessment based on GIA can be seen in Figures 2–4.
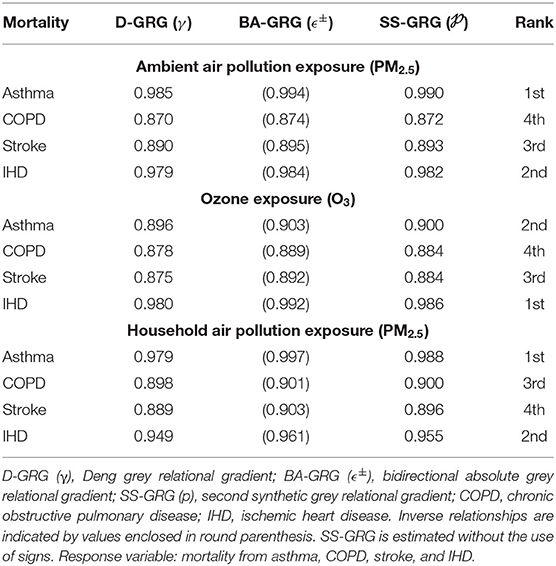
Table 1. Grey incidence assessment between mortality and associated factors.
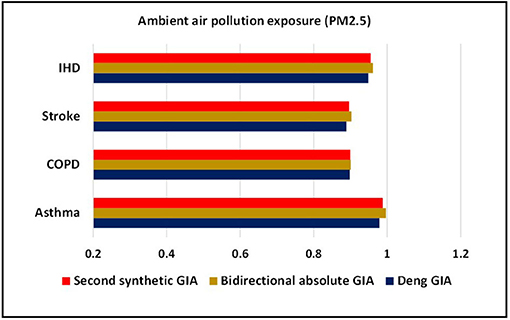
Figure 2. Comparative assessment of ambient air pollution exposure based on grey incidence analysis (GIA).
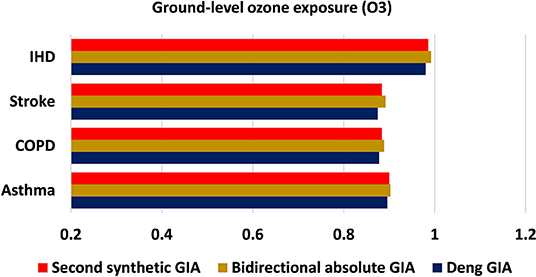
Figure 3. Comparative assessment of ground-level ozone exposure based on GIA.
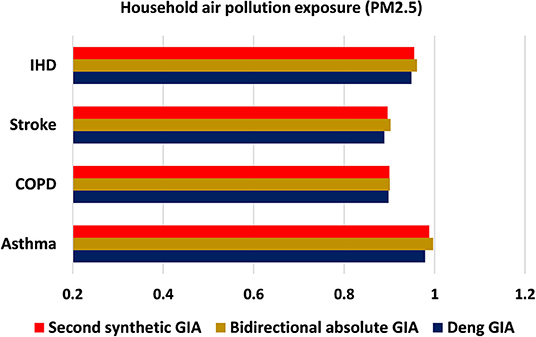
Figure 4. Comparative assessment of household air pollution exposure based on GIA.
Ambient PM2.5 exposure is regarded among the most significant risk factors for CRD and CVD-related comorbidity and mortality, both of which are serious public health concerns (24). In the present analyses, as indicated by Deng's GIA model findings, a more grounded measure of influence between ambient PM2.5 exposure and asthma mortality in the Pakistani populace (0.985: first) is observed whereas, a most fragile level of influence is seen for COPD (0.870: fourth). The higher impact measure of asthma mortality portrays that the factors are unequivocally interconnected with one another. Then again, the same succession showed up from the findings of the bidirectional absolute GIA model. The degree of correlation is found much higher for mortality from asthma against ambient PM2.5 exposure with an estimated grey weight of 0.994. At a more aggregate level, as per SS-GIA findings, exposure to ambient PM2.5 is distinguished as the major contributor in accelerating mortality from asthma when compared with COPD, stroke, and IHD and ranked top. After asthma, IHD appeared to be more affected from exposure to ambient PM2.5 with an estimated weight of 0.982 and ranked second, trailed by stroke and COPD with an estimated degree of 0.893 and 0.872, respectively. When compared with COPD and CVD mortality, the greater degree of correlation between asthma mortality and ambient air pollution exposure portrays that those variables are significantly associated with each other (Table 1). These findings are aligned with the findings by Ilyas et al. (9) and Yamamoto et al. (25).
Exposure to the ground-level ozone potentially exacerbates a multitude of health complications, particularly respiratory and cardiovascular illnesses. Ozone levels are expected to rise in many regions of the world, resulting in an upsurge in ozone-related deaths and morbidities (26). Considering the impact of ground-level ozone exposure on mortality from CVD and CRD in Pakistan, asthma, COPD, stroke, and IHD all sustained their ranking order across all grey incidence models; however, the strength of influence and correlation was determined to be greater for IHD mortality. As per Deng's GIA estimates, mortality from IHD (0.980: first) tends to be more strongly influenced by ground-level ozone exposure when compared with asthma, COPD, and stroke, though the least fortunate influence is seen with stroke mortality (0.875: fourth). Nonetheless, as per bidirectional absolute GIA model findings, mortality from IHD (0.889: first) gave off an impression of being significantly associated with exposure to ozone concentration and situated top among the rest of the disease mortality. In general, mortality from stroke and COPD was shown to have the least association from ground-level ozone exposure by acquiring grey incidence (relational/association) weights of 0.884 (rank: third) and 0.884 (rank: fourth), respectively. Broadly speaking, exposure to ozone concentration had all the earmarks of being a potential risk factor in assessing and anticipating mortality from IHD in the population of Pakistan when compared with stroke and CRDs. These findings back-up prior investigations substantiating the adverse impact of ground-level ozone exposure in the development and progression of respiratory and cardiac disorders (27, 28).
Table 1 shows a review of the relationship between household PM2.5 exposure and mortality from CVD and CRD in the Pakistani populace using grey incidence models. Given the weights determined by Deng's GIA model findings, the highest influence measure is observed in the case of asthma mortality (0.979: rank: first) due to household PM2.5 exposure, whereas the most fragile measure is seen in the case of stroke (0.889: rank: fourth). The assessment based on bidirectional absolute GIA outcomes revealed the same sequence of ranking depicting asthma mortality (0.997: rank: first) is highly significant with exposure to household PM2.5 concentration. As a general view, based on the outcomes of the SS-GIA model, mortality from asthma and IHD is shown to be strongly associated with exposure to household PM2.5, whereas COPD and stroke are determined to be less associated. In general, exposure to household PM2.5 is determined to be potentially impacting asthma and IHD mortality in the Pakistani population with an estimated degree of association of 0.988 and 0.955, respectively. The scope of epidemiological investigations is steady with the findings of the current study depicting a strong association between household PM2.5 pollution and a variety of respiratory and cardiac disorders and associated mortality (25, 29, 30). The ranking order based on grey modeling analysis is as follows.
Exposure to ambient PM2.5 concentration
Asthma > IHD > Stroke > COPD
Exposure to ground-level ozone (O3) pollution
IHD > Asthma > Stroke > COPD
Exposure to household PM2.5 concentration
Asthma > IHD > COPD > Stroke
To distinguish the potential risk factor in raising mortality from CRD (asthma, COPD) and CVD (stroke, IHD) in the Pakistani populace, Hurwicz's criterion was applied. Before applying it, one needs to create a decision scheme as shown in Table 2. Let, p = 4, k = 3, and outcome = v (Pk, Dp), whereas k = 1, 2, 3 and p = 1, 2, 3, 4. Let P1, P2, and P3 represent risk factors of mortality, and D1, D2, D3, and D4 represent mortality from asthma, COPD, stroke, and IHD, respectively. Table 3 represents the SS-GIA based matrix between the decision criteria (D1-D4) and decision actions (P1-P3).

Table 2. Defining the decision variables/parameters.

Table 3. Grey decision matrix.
Among the chosen variables (P1-P3), to identify the potential risk factor of mortality (asthma, COPD, stroke, and IHD), Hurwicz's approach is employed. For the present investigation, we need to minimize the mortality, so the decision of Hurwicz's criterion would be characterized as follows by keeping alpha-weight at 0.3 for an optimistic approach, whereas 0.7 for a pessimistic approach.
The calculated weighted average by Hurwicz's criterion is presented in Table 4.
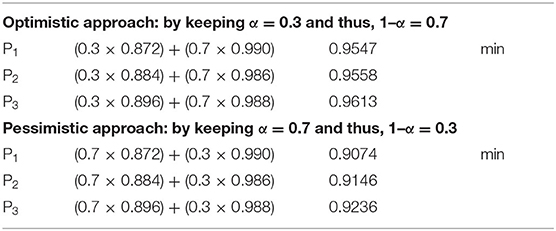
Table 4. Hurwicz's evaluations.
Given Hurwicz's criterion outcomes for both optimistic and pessimistic approaches, exposure to ambient PM2.5 concentration gave off an impression of being a more intense risk factor in accelerating mortality (asthma, COPD, stroke, and IHD) among the selected risk factors. At a more aggregate level, the findings revealed that exposure to ambient PM2.5 concentration is a potential contributor to mortality from CVD (stroke and IHD) and CRD (asthma and COPD) in the populace of Pakistan. As per the WHO recommendations, air quality in Pakistan is unhealthy; the most current statistics show that the annual mean concentration of country of PM2.5 is 58 g/m3, which exceeds the recommended level of 10 g/m3. The most significant contributors to these air pollutants in metropolitan areas are inadequate energy consumption, a spike in the number of vehicles driven regularly, an increase in uncontrolled industrial emissions, and the combustion of waste and plastic (31, 32). Thus, for the synergistic reduction of air pollutants, a holistic management framework integrating health, energy, climate, and environment sectors should be designed.
The considerable loss of life and comorbidities synonymous with non-communicable diseases (NCDs) in developing countries, such as Pakistan, entails a rigorous assessment of all the relevant factors, from an individual up to the public level. Addressing this subject can make a significant impact on overall general public health improvement. Nonetheless, relatively few investigations have emphasized the assessment of air pollutant exposure and mortality from CVD and CRD in Pakistani settings via an MCDA approach. To the best of the authors' knowledge, the study is the first of its kind to measure the intensity and nature of the relationship between exposure to air pollutants specifically PM2.5 and O3, and mortality from asthma, COPD, stroke, and IHD in the Pakistani setting by employing grey modeling. Consideration of endogeneity concerns in the acquisition of mortality-related variables is one contribution to this type of study. MCDA methods could be beneficial in facilitating appropriate policy solutions. Such investigations could assist improve our capacity to acquire valuable insights into the multifaceted nature of the variables in a system.
Given the GIA findings, exposure to ambient and household PM2.5 concentration had all the earmarks of being profoundly associated with mortality from asthma, while ground-level ozone exposure seemed, by all accounts, to be exceptionally associated with IHD mortality among the chosen variables. In the outcomes of Hurwicz's analysis, exposure to ambient PM2.5 demonstrated to be a more heightened factor in influencing mortality from CRD and CVD among the chosen factors. To be more specific, our findings emphasize the importance of planned urbanization, sustainable population growth, energy-efficient local transportation frameworks, adaptation of clean and renewable energy sources, and city-wide tree planting to avoid further environmental and population health deterioration.
In light of the outcomes, this investigation suggested that ambient concentration of PM2.5 might be the key influencing factor of mortality from asthma followed by IHD, stroke, and COPD within the Pakistani nation. Pakistan has experienced swift urban growth since its foundation, and the pace has intensified in recent decades. Presently, ~50% populace of Pakistan lives in metropolitan regions. Individuals commute to metropolitan regions for better job prospects and significant ventures are arranged nearby urban areas. Furthermore, rural regions have inadequate medical and educational facilities, and land ownership among rural residents is diminishing. These are different components instigating rural residents to relocate to metropolitan regions (33, 34). In Pakistan, the industry has grown at an exponential rate; thus, urbanization degrades the environmental quality indirectly via industrialization. Furthermore, due to the poor public transit infrastructure in the urban regions of Pakistan, inhabitants opt for private transportation, which has led to massive automobiles emissions that contribute to environmental deterioration. Consequently, urbanization in Pakistan causes pollution and worsens population health over the long haul (35, 36).
Pakistan has insufficient energy sources. As per Demographic Health Survey, 62% of Pakistani households cook with biomass fuels (e.g., wood, coal, and agricultural, and animal wastes) (37). PM2.5 concentrations emitted by biomass fuel use have a significant impact on cardiac morbidity and mortality worldwide. Individually, the amount of fuel burned in a household might be significantly less than the amount used in industries. However, its influence on population health is far stronger because of its pervasive and continuous existence in the internal environment and the maximum time spent inside by humans (38, 39). This issue is quite possibly the most ignored area of the disease burden in the Pakistani region. It is indeed not hard to establish a tight connection between household PM2.5 concentrations exposure and health risks in humans. To minimize indoor air pollution during culinary activities, a variety of treatments are available. Changes in energy technology and boosting public awareness about the severity of household air pollution caused by cooking are required at individual levels. Appropriate measures tending to a wide variety of issues related to cooking through awareness, economic development, and renewable energy resources can be extremely beneficial in reducing the possible CV health concerns produced by biomass fuel smoke.
In recent years, China has made significant progress in terms of improving air quality. In 2014, the government proclaimed a battle against air pollution and enacted a national plan to combat it. Since the announcement was made, air pollution levels in the cities of China have dropped by ~32% on average, as per estimates from ground-level sensors. Although these reductions are usually greater than those identified with the satellite-derived pollution information utilized in the AQLI, they would increase life expectancy by 2.3 years if confirmed and sustained over time. India has proclaimed its war against pollution in January 2019, would be on a comparable way if it prevails with regards to meeting its expressed pollution mitigation objective of 20–30%. Pakistan has the potential to encounter similar strides. If Pakistan somehow happened to accomplish a similar 32% pollution reduction experienced in China and to maintain it, its inhabitants would survive 1.2 years longer by and large. This would put the country 52% of the best approach to accomplishing its air quality norm and 43% closer to achieve the WHO recommendation (1, 40).
Our findings have significant ramifications for policymakers and decision-makers in terms of the sustainable environment and health infrastructure. We must realize that the health sector is simply one of many factors to a healthy life expectancy to achieve a health objective with a CRD or CVD focus. Agriculture, environmental, transportation, and economic policies, along with international trade pacts, will influence diet, physical inactivity, environmental sustainability, and access to better health facilities. We must work together and collaborate within regions and disciplines to promote and assert a significant return of interest in respiratory and cardiac health; only then, we will be able to persuade economies and businesses to contribute critical resources to our mutual goals, which is fundamental to population health and wellness in the populace of Pakistan. Eventually, the Government and private organizations in Pakistan should unanimously collaborate, encourage, and concentrate on strategies that can minimize the regional burden of diseases through planned urbanization, sustainable population growth, adoption of clean and renewable energy sources, raising the educational level, enhancing living standards, improving access to quality health services, and investment in public health expenditure to mitigate the risk of air pollution and related mortality.
Besides, researchers have agreed that the MCDA paradigm is productive in environmental healthcare domains and a beneficial decision-making tool since it enables transparency, robustness, and consistency in the context of diverse and contradictory parameters (41, 42). The study outcomes recommend that when confronted with various alternatives of equivalent worth in decision-making situations, researchers should employ MCDA methodologies and tools. This investigation may facilitate researchers with multiple criteria decision-making roadmap to help them enhance the quality of their studies and their understanding of how to use MCDA techniques to evaluate and prioritize the influencing factors of disease mortality in environmental healthcare research. Further, the suggested methodologies provide a valuable tool and additional practical knowledge for policymakers and decision-makers in drawing rational decisions. However, further investigations are necessary to contrast the particularities of MCDA approaches (e.g., preferred inferencing approaches) and enable researchers in selecting the appropriate tool, as there is no rationale for why one MCDA technique is adopted over the other.
This corroboration adds to the growing body of research demonstrating that exposure to ambient PM2.5 adversely leads to respiratory and cardiac risks, emphasizing the demand for further air quality improvement in Pakistan. Besides, the suggested methodologies provide a valuable tool and additional practical knowledge for policymakers and decision-makers in drawing rational decisions.
The data used to support the findings of this study are included within the article.
AM, SR, ER, and IH are responsible for conceptualizing the research theme, data collection, and analysis, interpretation of the results, and drafting earlier versions of the manuscript. SR is in charge of project administration and supervision of the overall manuscript. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. IQAir. Air Quality Index (AQI) and PM2.5 Air Pollution in Pakistan (2021). Available online at: https://www.iqair.com/pakistan (accessed August 8, 2021).
2. World Bank. Air Pollution Deaths Cost Global Economy US$225 Billion (2016). Available online at: https://www.worldbank.org/en/news/press-release/2016/09/08/air-pollution-deaths-cost-global-economy-225-billion (accessed August 12, 2021).
4. Rehman S, Li X, Wang C, Ikram M, Rehman E, Liu M. Quality of care for patients with acute myocardial infarction (AMI) in Pakistan: a retrospective study. Int J Environ Res Public Health. (2019) 16:3890. doi: 10.3390/ijerph16203890
5. Farraj AK, Walsh L, Haykal-Coates N, Malik F, McGee J, Winsett D, et al. Cardiac effects of seasonal ambient particulate matter and ozone co-exposure in rats. Part Fibre Toxicol. (2015) 12:1–20. doi: 10.1186/s12989-015-0087-3
6. Shahzad U, Fareed Z, Shahzad F, Shahzad K. Investigating the nexus between economic complexity, energy consumption and ecological footprint for the United States: new insights from quantile methods. J Clean Prod. (2021) 279:123806. doi: 10.1016/j.jclepro.2020.123806
7. Huang J, Song Y, Chu M, Dong W, Miller MR, Loh M, et al. Cardiorespiratory responses to low-level ozone exposure: the indoor ozone study in childrEn (DOSE). Environ Int. (2019) 131:105021. doi: 10.1016/j.envint.2019.105021
8. Nasir ZA, Murtaza F, Colbeck I. Role of poverty in fuel choice and exposure to indoor air pollution in Pakistan. J Integr Environ Sci. (2015) 12:107–17. doi: 10.1080/1943815X.2015.1005105
9. Ilyas SZ, Khattak AI, Nasir SM, Qurashi T, Durrani R. Air pollution assessment in urban areas and its impact on human health in the city of Quetta, Pakistan. Clean Technol Environ Policy. (2010) 12:291–9. doi: 10.1007/s10098-009-0209-4
10. Sahibzada UF, Xu Y, Afshan G, Khalid R. Knowledge-oriented leadership towards organizational performance: symmetrical asymmetrical approach. Bus Process Manag J. (2021) 27:1720–46. doi: 10.1108/BPMJ-03-2021-0125
11. Zhang Z, Zhang J, Wei Z, Ren H, Song W, Pan J, et al. Application of tabu search-based Bayesian networks in exploring related factors of liver cirrhosis complicated with hepatic encephalopathy and disease identification. Sci Rep. (2019) 9:6251. doi: 10.1038/s41598-019-42791-w
12. Pan J, Ren Z, Li W, Wei Z, Rao H, Ren H, et al. Prevalence of hyperlipidemia in Shanxi Province, China and application of Bayesian networks to analyse its related factors. Sci Rep. (2018) 8:14101. doi: 10.1038/s41598-018-22167-2
13. Ritchie HMR. OurWorldinData. (2018). Available online at: https://ourworldindata.org/causes-of-death#what-do-people-die-from (accessed March 19, 2021).
14. StateofGlobalAir. State of Global Air (2019). Available online at: https://www.stateofglobalair.org (accessed June 18, 2021).
17. Liu S, Xie N, Forrest J. Novel models of grey relational analysis based on visual angle of similarity and nearness. Grey Syst Theory Appl. (2011) 1:8–18. doi: 10.1108/20439371111106696
18. Ng DKW, Deng J. Contrasting grey system theory to probability and fuzzy. ACM Sigice Bull. (1995) 20:3–9. doi: 10.1145/202081.202082
19. Javed SA, Liu S. Bidirectional absolute GRA/GIA model for uncertain systems: application in project management. IEEE Access. (2019) 7:60885–96. doi: 10.1109/ACCESS.2019.2904632
20. Liu S, Lin C, Tao L, Javed SA, Fang Z, Yang Y. On Spectral Analysis New Research Directions in Grey System Theory. Burnham: Research Information Ltd. (2020). Available Online at: https://dora.dmu.ac.uk/bitstream/handle/2086/19945/On%20Spectral%20Analysis%20And%20New%20Research%20Directions%20In%20Grey%20System%20Theory%20%281%29.pdf?sequence=1&isAllowed=n
21. Liu S, Forrest J. The current developing status on grey system theory. J Grey Syst. (2007) 19:111–23.
22. Liu S, Yang Y, Xie N, Forrest J. New progress of grey system theory in the new millennium. Grey Syst Theory Appl. (2016) 6:2–31. doi: 10.1108/GS-09-2015-0054
23. Zeng XT, Li YP, Huang W, Chen X, Bao AM. Two-stage credibility-constrained programming with hurwicz criterion (TCP-CH) for planning water resources management. Eng Appl Artif Intell. (2014) 35:164–75. doi: 10.1016/j.engappai.2014.06.021
24. Rehman S, Rehman E, Ikram M, Jianglin Z. Cardiovascular disease (CVD): assessment, prediction and policy implications. BMC Public Health. (2021) 21:1299. doi: 10.1186/s12889-021-11334-2
25. Yamamoto SS, Phalkey R, Malik AA. A systematic review of air pollution as a risk factor for cardiovascular disease in South Asia: limited evidence from India and Pakistan. Int J Hyg Environ Health. (2014) 217:133–44. doi: 10.1016/j.ijheh.2013.08.003
26. Zhang JJ, Wei Y, Fang Z. Ozone pollution: a major health hazard worldwide. Front Immunol. (2019) 10:2518. doi: 10.3389/fimmu.2019.02518
27. Sarfraz Z. The social and economic burden of smog in Pakistan. Pak J Med Sci. (2020) 1:5–7. doi: 10.37978/pjsm.v1i1.92
28. Raza W, Saeed S, Saulat H, Gul H, Sarfraz M, Sonne C, et al. A review on the deteriorating situation of smog and its preventive measures in Pakistan. J Clean Prod. (2020) 279:123676. doi: 10.1016/j.jclepro.2020.123676
29. Clark ML, Peel JL, Balakrishnan K, Breysse PN, Chillrud SN, Naeher LP, et al. Health and household air pollution from solid fuel use: the need for improved exposure assessment. Environ Health Perspect. (2013) 121:1120–8. doi: 10.1289/ehp.1206429
30. Iqbal N, Fareed Z, Shahzad F, He X, Shahzad U, Lina M. The nexus between COVID-19, temperature and exchange rate in Wuhan city: new findings from partial and multiple wavelet coherence. Sci Total Environ. (2020) 729:138916. doi: 10.1016/j.scitotenv.2020.138916
31. IAMAT. International Association for Medical Assisstance to Travellers (2020). Available online at: https://www.iamat.org/country/pakistan/risk/air-pollution (accessed July 4, 2021).
32. Fareed Z, Meo MS, Zulfiqar B, Shahzad F, Wang N. Nexus of tourism, terrorism, and economic growth in Thailand: new evidence from asymmetric ARDL cointegration approach. Asia Pac J Tour Res. (2018) 23:1129–41. doi: 10.1080/10941665.2018.1528289
33. Imran M, Bakhsh K, Hassan S. Rural to urban migration and crop productivity: evidence from Pakistani Punjab. Mediterr Agric Sci. (2016) 29:17–9.
34. Li X, Wang C, Rehman S, Wang X, Zhang W, Su S, et al. Setting performance benchmarks for stroke care delivery: which quality indicators should be prioritized in quality improvement; an analysis in 500,331 stroke admissions. Int J Stroke. (2020) 16:737–37. doi: 10.1177/1747493020958608
35. Ali R, Bakhsh K, Yasin MA. Impact of urbanization on CO2 emissions in emerging economy: evidence from Pakistan. Sustain Cities Soc. (2019) 48:101553. doi: 10.1016/j.scs.2019.101553
36. Iqbal N, Fareed Z, Wan G, Shahzad F. Asymmetric nexus between COVID-19 outbreak in the world and cryptocurrency market. Int Rev Financ Anal. (2021) 73:101613. doi: 10.1016/j.irfa.2020.101613
37. Khan MSB, Lohano HD. Household air pollution from cooking fuel and respiratory health risks for children in Pakistan. Environ Sci Pollut Res. (2018) 25:24778–86. doi: 10.1007/s11356-018-2513-1
38. Hadley MB, Vedanthan R, Fuster V. Air pollution and cardiovascular disease: a window of opportunity. Nat Rev Cardiol. (2018) 15:193–4. doi: 10.1038/nrcardio.2017.207
39. Fareed Z, Ali Z, Shahzad F, Nazir MI, Ullah A. Determinants of profitability: evidence from power and energy sector. Stud Univ Babe Bolyai. (2016) 61:59. doi: 10.1515/subboec-2016-0005
40. Fareed Z, Iqbal N, Shahzad F, Shah SG, Zulfiqar B, Shahzad K, et al. Co-variance nexus between COVID-19 mortality, humidity, and air quality index in Wuhan, China: new insights from partial and multiple wavelet coherence. Air Qual Atmos Health. (2020) 13:673–82. doi: 10.1007/s11869-020-00847-1
41. Glaize, Duenas A, Di Martinelly C, Fagnot I. Healthcare decision-making applications using multicriteria decision analysis: a scoping review. J Multi Criteria Decis Anal. (2019) 26:62–83. doi: 10.1002/mcda.1659
Keywords: environmental pollution, public health, cardiac mortality, respiratory mortality, particulate matter, ground-level ozone, MCDA
Citation: Mumtaz A, Rehman E, Rehman S and Hussain I (2022) Impact of Environmental Degradation on Human Health: An Assessment Using Multicriteria Decision Making. Front. Public Health 9:812743. doi: 10.3389/fpubh.2021.812743
Received: 10 November 2021; Accepted: 02 December 2021;
Published: 20 January 2022.
Edited by:
Suleman Sarwar, Jeddah University, Saudi ArabiaReviewed by:
Umar Farooq, Northwestern Polytechnical University, ChinaCopyright © 2022 Mumtaz, Rehman, Rehman and Hussain. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shazia Rehman, cmVobWFuc2hhemlhLm1hbGlrQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.