 Yueyue You1,2
Yueyue You1,2 Hein Raat
Hein Raat- 1The Generation R Study Group, Erasmus Medical Center, Rotterdam, Netherlands
- 2Department of Public Health, Erasmus Medical Center, Rotterdam, Netherlands
- 3Department of Child and Adolescent Psychiatry/Psychology, Erasmus Medical Center, Rotterdam, Netherlands
Aim: To identify the factors associated with health-related quality of life (HRQOL) among early elementary age children (5–6 years) from a general population sample.
Methods: We analyzed data of 4,202 children from the Generation R Study, a population-based cohort study in the Netherlands. Children's physical and psychosocial HRQOL were measured using the Child Health Questionnaire Parent Form 28 (CHQ-PF28). Associations between socio-demographic characteristics (child age, sex, ethnic background, family situation, parental educational level, parental employment status, and net household income), health-related lifestyle behaviors (physical activity and screen time), health conditions (number of chronic conditions, emotional and behavioral problems, and family functioning) and children's physical and psychosocial HRQOL were assessed using multivariate regression analyses.
Results: Mean child age was 6.0 years (SD: 0.43); 63.6% had a majority (Dutch) ethnic background. Children with a non-western ethnic background, and children of unemployed mothers had a lower physical HRQOL (all p < 0.05). Older children, boys, and children from single-parent or low educated families had a lower psychosocial HRQOL (all p < 0.05). Children from a low income household family, children having chronic conditions or emotional and behavioral problems, or from families with relatively high “pathological family functioning” reported both lower physical and psychosocial HRQOL (all p < 0.05).
Conclusion: Indicators of adverse socioeconomic and family circumstances and indicators of child health problems were associated with lower HRQOL. Public health initiatives to improve HRQOL of children should prioritize children from a low socioeconomic status or with less favorable health conditions from early age onwards.
Introduction
Health-related quality of life (HRQOL) is a broad, multidimensional construct including not only disease states but also the person's physical, psychological, and social well-being (1). It is been increasingly used as an additional health outcome among children to assess their physical and social functioning, physical and mental health, and to evaluate the effect of both clinical and population-based interventions (2). Identifying the factors that affect child HRQOL may help develop effective prevention programs for children, and thereby promote positive physical and psychosocial health in the long term (3).
Several models have been proposed to study factors associated with HRQOL (4–6). For example, a general model from Wilson and Cleary (7) suggests five levels of factors related to HRQOL: biological, physiological, symptoms, functioning, and general health. Other researchers evaluating potential determinants of HRQOL have suggested that certain factors might have differential associations with HRQOL than other factors. For example, Sprangers et al. (4) proposed that socio-demographic characteristics (e.g., age, education, household income, etc.) are important factors that can affect individuals' HRQOL. Wendel-Vos et al. (5) suggested that health-related lifestyle behavior (e.g., physical activity, smoking, etc.) is an important predictor of HRQOL in both children and adults. In addition, Ware et al. (6) suggested that health conditions (e.g., overweight/obesity, asthma, infectious disease, etc.) have the most immediate direct impact on HRQOL. Thus, identifying whether and how the factors from these multiple domains have an impact on children's HRQOL is important to subgroups of children who are at risk of impaired HRQOL.
However, in the literature so far, the findings about associations between socio-demographic characteristics and HRQOL are not consistent (8, 9). For example, a study among U.S. school-aged children found that parental educational level was not related to child HRQOL, but household income was positively related to child overall HRQOL (10). Another study among European school-aged children reported that maternal educational level and household income were both positively related to child psychosocial HRQOL (11). Furthermore, previous studies mainly focused on one domain; research that studies simultaneously the associations of factors covering three domains (socio-demographic characteristics, health-related lifestyle behaviors, and health conditions) and HRQOL are lacking among young children. A comprehensive understanding of the potential factors associated with HRQOL provides support for intervention development and public health practitioners focusing on improving child HRQOL. Thus, in this study, we selected multiple factors covering the three domains relevant for HRQOL: socio-demographic characteristics, health-related lifestyle behaviors of the child, and indicators of health and well-being of the child and family.
The aim of the present study was to identify which factors were associated with both physical and psychosocial HRQOL at early elementary school age (5–6 years old). All factors were studied across three domains: socio-demographic characteristics (child age, sex, ethnic background, parental educational level, parental employment status, and net household income), health-related lifestyle behaviors (physical activity and screen time of the child), and indicators of health and well-being of the child and family (number of chronic conditions, emotional and behavioral problems, and family functioning). Based on previous studies (12–14), the hypothesis was that children with higher socio-demographic status; children with more favorable health-related behaviors; and children with more favorable health, well-being, and family functioning are more likely to have higher HRQOL than their counterparts.
Methods
Study Design and Population
This cross-sectional study was embedded in the Generation R Study, a multi-ethnic prospective cohort study of children born between 2002 and 2006 in the city of Rotterdam, the Netherlands, that has been described previously (15). In total, 8,305 children aged 6-years old still participated in the ongoing cohort study, and relevant data were collected from 2008 to 2012. Among participants of 8,305, parents of 5,298 joined the measurement of their child's HRQOL; parents did not finish the full questionnaire of measurement of HRQOL (n = 563) were excluded. To avoid clustering of data, second (n = 505) and third children (n = 12) from the same family were excluded. Then, children with missing data on all determinants (n = 16) were also excluded. Leaving a study population of 4,202 participants. The study was approved by the Medical Ethics Committee of the Erasmus University Medical Centre (MEC 217.595/2002/202). Written informed consent was obtained from all participants.
Independent Variables
Socio-demographic characteristics, health-related lifestyle behaviors, and indicators of health and well-being of the child and family were considered as the factors of HRQOL in this study. All related information was obtained via parental questionnaire when the child was 5 to 6 years old.
Socio-demographic characteristics included child age (years), sex (boy, girl), ethnic background (Dutch, other western, non-western), family situation (two-parent family, one-parent family), parental educational level (high, middle, low), parental employment status (paid job, no paid job), and net household income (>€3,200, €2,000–3,200, < €2,000/month). Child ethnic background was based on the country of birth of the parents [according to the classification of Statistics Netherlands (16)]. Children were categorized into three groups regarding ethnic background: Dutch, other Western (American western, Asian western, European and Oceania), and non-Western (Indonesian, Cape Verdean, Moroccan, Dutch Antilles, Surinamese, Turkish, African, American non-western and Asian non-western). Both mother and father educational levels were defined according to Statistics Netherlands and categorized into three educational levels: high (bachelor's degree, higher vocational school or a university degree finished), middle (>4 years general secondary school, or intermediate vocational school), and low (no education, primary education, ≤ 4 years general secondary school, or lower vocational training) (17).
Indicators of health-related lifestyle behaviors included physical activity and screen time at child age 6 years. Child physical activity refers to sports participation and outdoor play. For sports participation, parents were asked the following question: “Does your child take part in sports (e.g., football, judo, tennis, etc.?).” Then, frequency (number of days) and duration (minutes) were asked for weekdays and weekend days separately. The average sports participation time per day of the child was calculated by the following formula: [(days per week) * (hours on a weekday) + (days per weekend) * (hours on a weekend day)]/7. The same set of questions was used to assess children's time spent on outdoor playing. Then, physical activity time per day was calculated by adding up children's sports participation and outdoor play. According to new WHO guidelines on physical activity for children, physical activity time was dichotomized into <1 hour per day and ≥1 hour per day (18). Child screen time refers to television viewing (including video/DVD) and computer game use (including video games). For both variables, frequency (number of days) and duration (minutes) were asked for weekdays and weekend days separately. Then, screen time per day was calculated by adding up children's television viewing and computer game use, and was dichotomized at <2 h per day and ≥2 h per day according to the recommendation from the American Academy of Pediatrics (19).
With regard to indicators of health and well-being of the child and family, we included the number of chronic conditions, the presence of emotional and behavioral problems, and the presence of “pathological family functioning.” Information of the chronic condition were measured by parents-reported questionnaire when the child aged 6-years old. Parents were asked whether their child had infectious disease (ear infection, urinary tract infection or bladder infection, sore throat, spurious croup, bronchitis, pneumonia, impetigo, stomach flu and/or diarrhea), wheezing attack, eczema, and pain in the past 12 months. Number of chronic conditions was counted based on parent's reply, and then categorized as 0, 1, 2, and 3 or more chronic conditions. Presence of emotional and behavioral problems (yes/no) were assessed with the Dutch version of Child Behavior Checklist (CBCL/1.5-5), a 99-item parents-reported questionnaire (20). The CBCL/1.5-5 has shown good concurrent validity and test-retest reliability in Dutch children (21). A borderline cut-off score [83rd percentile of a Dutch norm group (22)] of the CBCL total problem score was used to differentiate between children with and without emotional and behavioral problems (23). Family functioning (pathological/not pathological) was measured with the 12-item General Function scale of the McMasters Family Assessment Device (FAD) (24), a score >2.17 was defined as “pathological,” a score ≤ 2.17 was defined as “not pathological” (25). The McMaster FAD is a validated measure assessing overall health and pathology of a family (25).
Health-Related Quality of Life
With regard to HRQOL of their child, parents completed the Child Health Questionnaire Parent Form 28 items (CHQ-PF28), of which the validity and reliability had been documented (26). The questionnaire consists of 28 items with four, five or six response options across eight multi-item scales and five single-item concepts. The items from each of the scales were summed and transformed into 0 to 100 (0 indicating worst health and 100 best health). According to the CHQ Manual, these scores are used to calculate the Physical Summary Component Scale (PhS) and the Psychosocial Summary Component Scale (PsS); summary scores of 50 represent the mean in the US reference population children; 10 points above/below 50 reflect one standard deviation difference in either direction (26, 27).
Data Analyses
Descriptive analysis was applied to characterize the study population. Physical and psychosocial HRQOL across different factors were assessed using independent sample t-tests and one-way ANOVA (see Appendix Table 1). The normality of the data (the summary scores) was examined. Although score distributions were slightly negatively skewed, with the large number of respondents, parametric tests were performed (28). The multi-collinearity among all potential factors influencing HRQOL was assessed by examining the variance inflation factor (VIF) values. All the VIF values were <3, indicating acceptable collinearity between all indicators. Multivariate linear regressions were applied to assess the factors of physical and psychosocial HRQOL. In model 1, all socio-demographic characteristics were entered to model. In model 2, with additional inputs all indicators of health-related behaviors. In model 3, with additional inputs all indicators of health and well-being of the child and family. In Appendix Table 1, we calculated effect sizes (Cohen's d) to assess the relative differences between specific subgroups with regard to the PhS and PsS scores. The effect sizes (d) were calculated by dividing the difference in mean scores between subgroups by the largest SD (small difference: 0.2 ≤ d <0.5; moderate difference: 0.5 ≤ d <0.8; large difference: d ≥ 0.8) (29). Multiple imputation was applied to impute missing data in the determinants (30). Ten imputed datasets were generated using a fully conditional specified model, taking into account all the variables included in this study. Pooled estimates from these ten imputed datasets were used to report beta coefficients and 95% confidence intervals (95% CI). All analyses were conducted with Statistical Package for Social Sciences (SPSS) version 21.0 for Windows (IBM Corp., Armonk, NY, USA). Significance differences were indicated at the level of p < 0.05.
Non-response Analyses
Children with missing data on HRQOL (n = 563) were compared with children without missing data (n = 4,202) using Chi-square tests. Data were more often missing for children whose parents had a low educational level, parents without a paid job, a low household income, a single-parent family, from non-western ethnic background, and with screen time more than 2 h per day (all p < 0.05).
Results
Table 1 summarizes the general characteristics of the study population. Mean child age was 6.0 years (SD: 0.43); 2,090 (49.7%) were girls; 63.6% had a majority (Dutch) ethnic background. The average score (SD) for physical and psychosocial summary score were 56.98 (6.57) and 52.73 (7.07), respectively. The univariate analysis of physical and psychosocial summary score between subgroups according to socio-demographic characteristics, health-related lifestyle behaviors, and health and well-being of the child and family were presented in Appendix Table 1. The results showed that the following factors were associated with a higher physical and psychosocial summary score: two-parent household, high-educated fathers, employed mothers, a high income household, having physical activity more than 1 h per day, screen time <2 h per day, and no chronic disease (all p < 0.05).
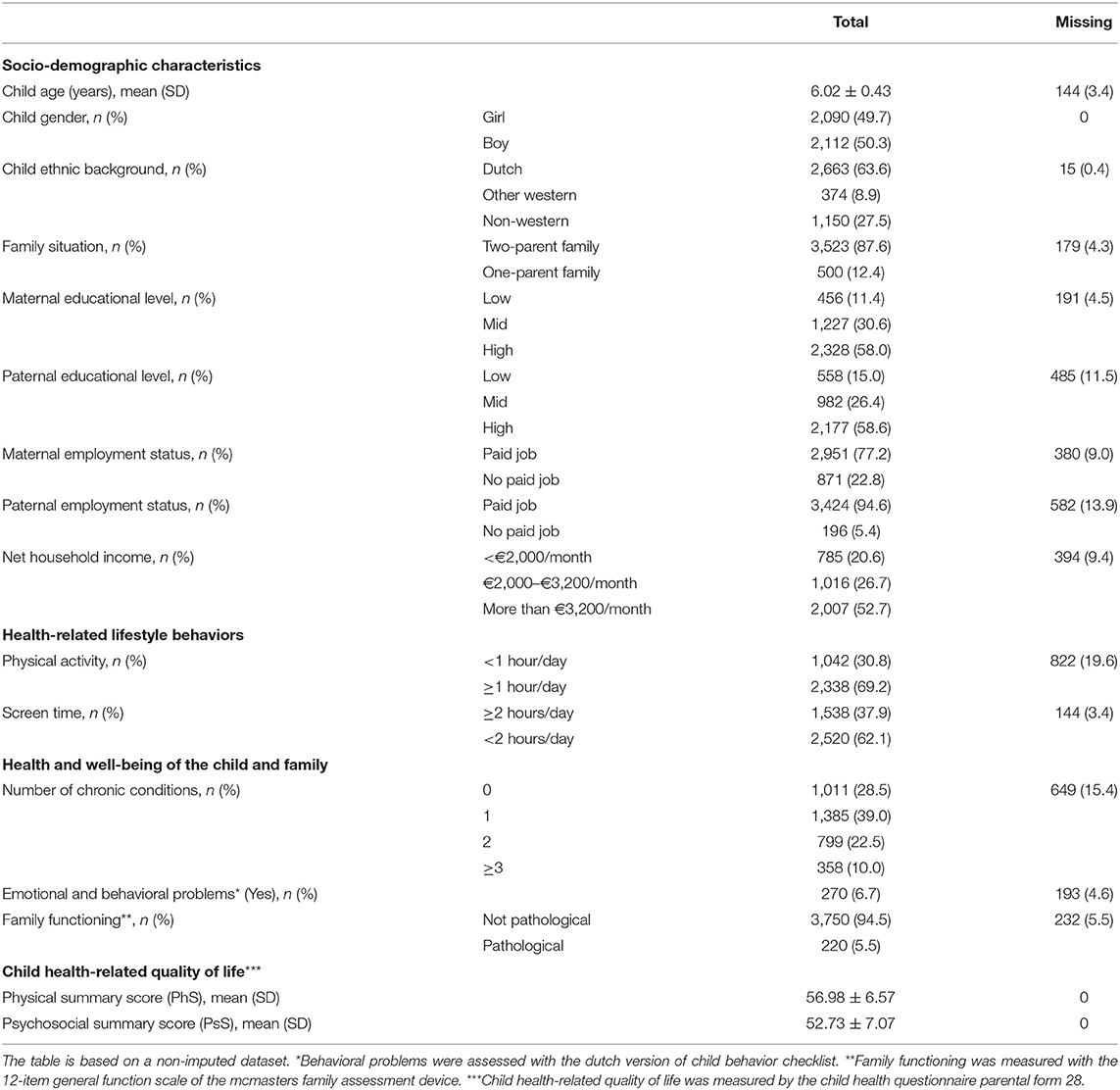
Table 1. General characteristics of the study population among 6-year-old children (n = 4,202).
Table 2 presents the factors associated with physical HRQOL. After including all three domains of factors into the model, non-western ethnic background, maternal unemployment status, and low household income were associated with lower physical HRQOL (all p < 0.05). In the domain of health and well-being of the child and family, all factors included were significantly associated with physical HRQOL (all p < 0.05). Emotional and behavioral problems, and pathological family functioning were associated with lower physical HRQOL. Having chronic conditions were also associated with lower physical HRQOL, of which having three or more chronic conditions showed the largest reduction in physical HRQOL (β = −4.59; 95%CI: −5.40, −3.77).
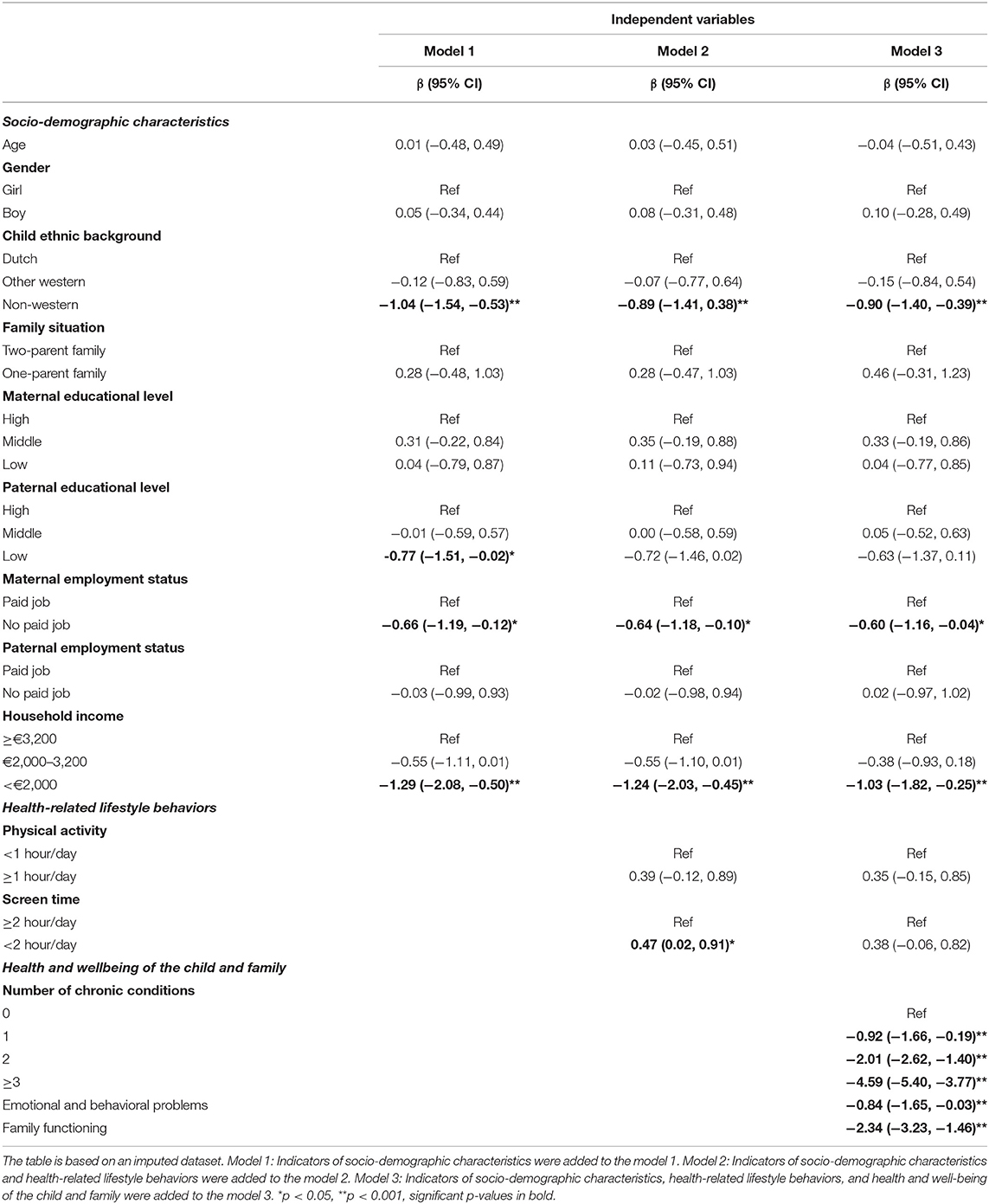
Table 2. Multivariate analyses of socio-demographic characteristics, health-related lifestyle behaviors, and health and well-being of the child and family with physical summary score (PhS).
Table 3 presents the factors associated with psychosocial HRQOL. After including all three domains of factors into the model, child age, being a boy, one-parent family, low maternal education level, and low household income were associated with lower psychosocial HRQOL. All factors from health and well-being of the child and family were significantly associated with psychosocial HRQOL. Emotional and behavioral problems, pathological family functioning, and having three or more chronic conditions were associated with lower psychosocial HRQOL (all p < 0.05).
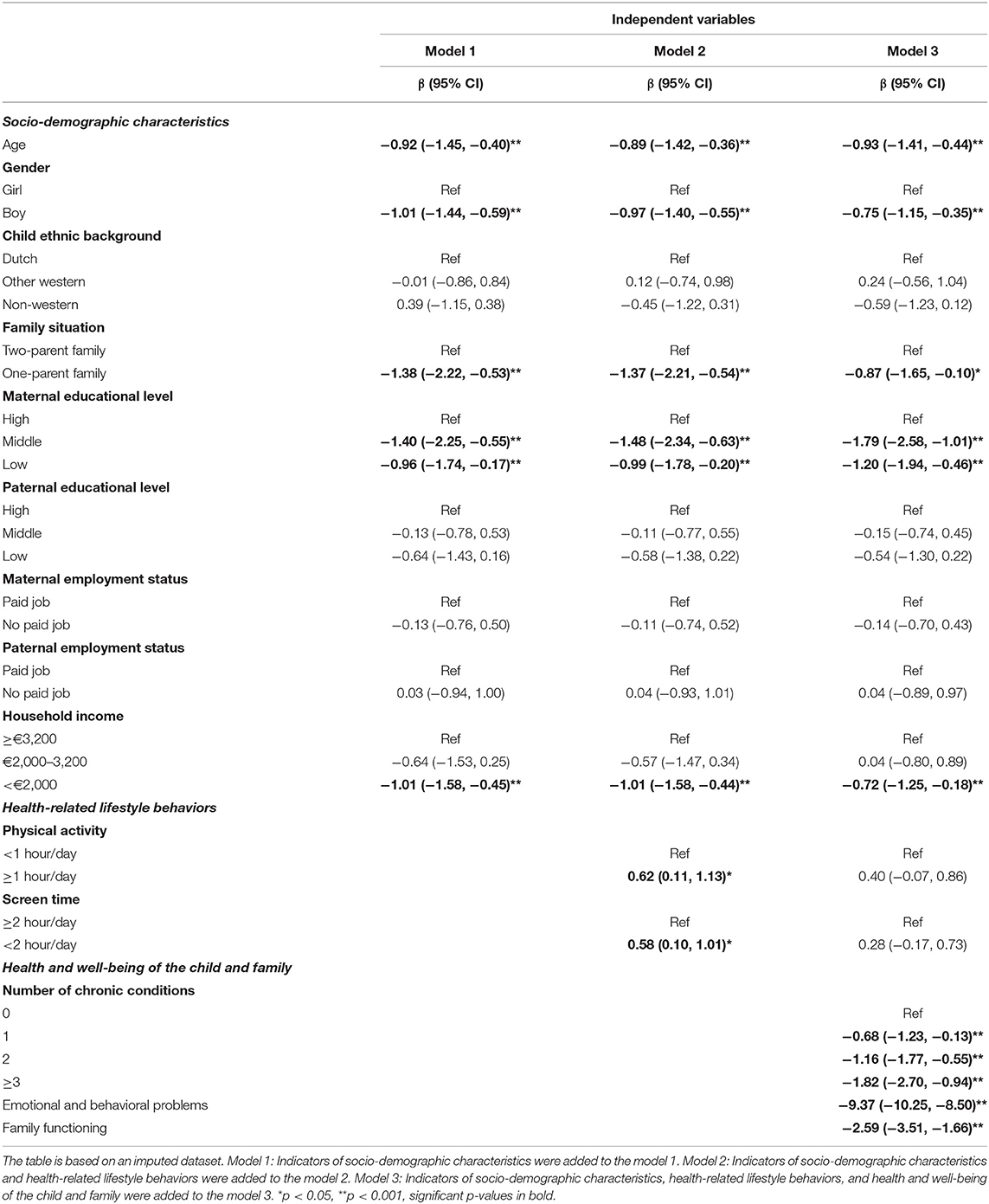
Table 3. Multivariate analyses of socio-demographic characteristics, health-related lifestyle behaviors, and health and well-being of the child and family with psychosocial summary score (PhS).
Discussion
The present study was designed to assess which factors were related with physical and psychosocial HRQOL among early elementary school age children (5–6 years). The factors covered three domains: socio-demographic characteristics, health-related lifestyle behaviors, and health and well-being of the child and family. Several socio-demographic characteristics (age, sex, ethnic background, family situation, paternal educational level, maternal employment status, and household income) were associated with lower physical or psychosocial HRQOL; indicators of health and well-being of the child and family (number of chronic conditions, emotional and behavioral problem, and family functioning) were associated with lower physical and psychosocial HRQOL. No associations were observed between health-related lifestyle behaviors and HRQOL.
Our findings showed that children with a low family socioeconomic status, as indicated by low maternal education level, maternal unemployment, and low income household have a relatively lower physical or psychosocial HRQOL score. The findings are consistent with previous studies (31–33). Currently, several mechanisms are suggested explaining the associations between the family socioeconomic status and HRQOL of children (34–36). For example, Adler et al. (34) indicated that one pathway from family socioeconomic status to HRQOL is through exposure to different environments and adaptations to these environments. Children with low socioeconomic status may live in relatively poor neighborhoods, where they may be more likely to be victimized, and may experience peer aggression, and community violence (37). This may explain that they are more likely to have lower physical or psychosocial HRQOL. Another mechanism refers to the smaller access to material and social resources among children in families with a low socioeconomic status (36). Children from families with low socioeconomic status may have access to fewer social resources (i.e., services, goods, and social connections) than their counterparts, which may put them at risk for developmental problems, which may affect children's physical and psychosocial well-being (38). Therefore, the current findings support that health professionals should pay attention to children with low socioeconomic status backgrounds and good social support might help to improve these children's HRQOL.
Previous researchers have reported that, among children aged 9 and older, child with older age and living in a one-parent family were associated with lower psychosocial HRQOL (32, 39). Our study observed the same finding in a younger age group (6-year-old). However, our results showed that compared to girls, boys were more likely to have lower scores of psychosocial HRQOL. This finding is inconsistent with previous studies that reported lower HRQOL for girls, which was measured by KIDSCREEN (32, 39). Currently, gender differences in the HRQOL of children are even less clear, or are not found at all, more studies of this topic among younger children are needed in the future.
Regarding health-related lifestyle behaviors, previous researchers observed an association between health-related lifestyle behavior, such as physical activity (40) and screen time (41), and children's HRQOL. For example, Wu et al. (13) in a systematic review, reported that among generational population of children and adolescents aged 8 or older, a higher frequency of physical activity or less screen time, were both related to higher overall HRQOL. However, differently as expected, in the current study, no associations were observed between physical activity, screen time, and HRQOL. It could be possible that at the age of the children in this study (6-year-old), health behaviors do not yet show an association with HRQOL (42). The beneficial effects of physical activity or non-sedentary behavior on HRQOL might need to be assessed over a longer period of time (43).
This study found that health and well-being of the child and family (number of chronic conditions, emotional and behavior problems, and family environment) were negatively associated with children's physical and psychosocial HRQOL. Our results add to the evidence that chronic conditions in childhood may function as a stressor that affect the physical and psychological well-being of individuals (44). Thus, it is important for pediatric practitioners to pay attention to not only the development of the chronic conditions of the children, but also on their physical and psychological well-being.
Overall, socio-demographic characteristics, health-related lifestyle behaviors, and health and well-being of the child and family were studied in relation to both physical and psychosocial HRQOL. When studying the finding it appears that some factors might be specifically affecting HRQOL of early elementary school age children. For example, socioeconomic status was only associated with lower psychosocial HRQOL. Also, all indicators of health and well-being of the child and family were associated with both lower physical and psychosocial HRQOL. Therefore, priority might be given to children from a low socioeconomic status or with less favorable health conditions.
A major strength of this study is the large number of children being studied with detailed information on a broad range of potential determinants. However, several limitations should be considered. First, the cross-sectional of the present study did not allow to establish the causal relationship between all factors and HRQOL. Future work should examine the associations longitudinally. Second, child HRQOL was measured by the CHQ-PF28, which is a parent proxy measure. Thus, data presented in our study are from the parent's perspective. Nevertheless, previous work supports the validity of the CHQ-PF28 (26). We recommend future studies among children over 10 years to adopt the child self-report HRQOL questionnaire (CHQ-CF87). This could be used as an addition to the parent report HRQOL of the child. Taking both assessment would allow a comparison of parent perceived child HRQOL and HRQOL reported by the child him/herself. Third, the population in this study is on average 6 years old. Previous literature on determinants of HRQOL among younger children showed inconsistent results. Although the related data of current study was collected from 2008 to 2012, an ongoing birth cohort study offers good opportunity to generate an overall understanding of potential determinants of HRQOL in large general child population. Also, the factors included in this study cover all three domains. We recommend future studies to confirm our findings in more recent dataset.
Conclusion
Our study investigated a wide range of factors covering three domains (socio-demographic characteristics, health-related lifestyle behaviors, and health and well-being of the child and family) related to child HRQOL. Public health initiatives to improve HRQOL of children should prioritize children from a low socioeconomic status or with less favorable health conditions from early age onward.
Data Availability Statement
The datasets presented in this article are not readily available because the Generation R Study is subject to the Dutch law on medical research among humans (Wet Medisch-Wetenschappelijk Onderzoek met mensen, WMO). This law prescribes data analyses to be restricted to the topics defined in the information form and informed consent forms. It is not allowed by the WMO law that de-identified data are provided to others without restriction. The Medical Ethical Committee at Erasmus University Medical Center Rotterdam has approved the Generation R Study and supervises research leaders to conduct accordingly. Only after a written agreement about the use of the data made via the Technology Transfer Office of Erasmus MC, datasets can be requested by means of contacting the data managers (Claudia J. Kruithof, Yy5rcnVpdGhvZkBlcmFzbXVzbWMubmw= or ZGF0YW1hbmFnZW1lbnRnZW5yQGVyYXNtdXNtYy5ubA==) and the Director of the Generation R Study (Vincent Jaddoe, di5qYWRkb2VAZXJhc211c21jLm5s). Requests to access the datasets should be directed to Claudia J. Kruithof, Yy5rcnVpdGhvZkBlcmFzbXVzbWMubmw= and Vincent Jaddoe, di5qYWRkb2VAZXJhc211c21jLm5s.
Ethics Statement
The study was approved by the Medical Ethics Committee of the Erasmus University Medical Centre (MEC 217.595/2002/202). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
YY, JY-H, AG, FE-L, and HR conceptualized and designed the study. YY performed the statistical analyses and drafted the manuscript. AG and HR supervised the data analyses. JY-H and AG contributed to methodology considerations. JY-H, AG, FE-L, and HR reviewed the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
Funding
FE-L received funding from the European Union's Horizon 2020 research and innovation programme under the Marie Sklodowska-Curie (Grant No. 707404).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The Generation R Study is conducted by the Erasmus Medical Center in close collaboration with the School of Law and Faculty of Social Sciences of the Erasmus University Rotterdam, the Municipal Health Service Rotterdam area, Rotterdam, the Rotterdam Homecare Foundation, Rotterdam, and the Stichting Trombosedienst and Artsenlaboratorium Rijnmond (STAR-MDC), Rotterdam. The authors wish to thank the study participants for their contribution to the study, as well as current and past investigators and staff.
References
1. Gothwal VK, Bharani S, Mandal AK. Parent-child agreement on health-related quality of life in congenital glaucoma. Transl Vis Sci Technol. (2018) 7:15. doi: 10.1167/tvst.7.4.15
2. Solans M, Pane S, Estrada MD, Serra-Sutton V, Berra S, Herdman M, et al. Health-related quality of life measurement in children and adolescents: a systematic review of generic and disease-specific instruments. Value Health. (2008) 11:742–64. doi: 10.1111/j.1524-4733.2007.00293.x
3. Lane DC, Pala Ö, Barlas Y. Health, demographic change and well-being: the European Union's Horizon 2020 programme and system dynamics. Syst Res Behav Sci. (2015) 32:407–13. doi: 10.1002/sres.2333
4. Sprangers MAG, Schwartz CE. Integrating response shift into health-related quality of life research: a theoretical model. Soc Sci Med. (1999) 48:1507–15. doi: 10.1016/S0277-9536(99)00045-3
5. Wendel-Vos GCW, Schuit AJ, Tijhuis MAR, Kromhout D. Leisure time physical activity and health-related quality of life: cross-sectional and longitudinal associations. Qual Life Res. (2004) 13:667–77. doi: 10.1023/B:QURE.0000021313.51397.33
6. Ware Jr JE. Conceptualizing disease impact and treatment outcomes. Cancer. (1984) 53:2316–23. doi: 10.1002/cncr.1984.53.s10.2316
7. Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life: a conceptual model of patient outcomes. JAMA. (1995) 273:59–65. doi: 10.1001/jama.273.1.59
8. Varni JW, Limbers CA, Burwinkle TM. How young can children reliably and validly self-report their health-related quality of life?: an analysis of 8,591 children across age subgroups with the PedsQL™ 4.0 Generic Core Scales. Health Qual Life Outcomes. (2007) 5:1–13. doi: 10.1186/1477-7525-5-1
9. Bevans KB, Riley AW, Moon J, Forrest CB. Conceptual and methodological advances in child-reported outcomes measurement. Expert Rev Pharmacoecon Outcomes Res. (2010) 10:385–96. doi: 10.1586/erp.10.52
10. Mansour ME, Kotagal U, Rose B, Ho M, Brewer D, Roy-Chaudhury A, et al. Health-related quality of life in urban elementary schoolchildren. Pediatrics. (2003) 111:1372–81. doi: 10.1542/peds.111.6.1372
11. Erhart M, Ottova V, Gaspar T, Jericek H, Schnohr C, Alikasifoglu M, et al. Measuring mental health and well-being of school-children in 15 European countries using the KIDSCREEN-10 Index. Int J Public Health. (2009) 54:160–6. doi: 10.1007/s00038-009-5407-7
12. Houben-van Herten M, Bai G, Hafkamp E, Landgraf JM, Raat H. Determinants of health-related quality of life in school-aged children: a general population study in the Netherlands. PLoS ONE. (2015) 10:e0125083. doi: 10.1371/journal.pone.0125083
13. Wu XY, Han LH, Zhang JH, Luo S, Hu JW, Sun K. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: a systematic review. PLoS ONE. (2017) 12:e0187668. doi: 10.1371/journal.pone.0187668
14. Oppenheimer S, Krispin O, Levy S, Ozeri M, Apter A. The impact of coping patterns and chronic health conditions on health-related quality of life among children and adolescents. Eur J Pediatr. (2018) 177:935–43. doi: 10.1007/s00431-018-3146-6
15. Kooijman MN, Kruithof CJ, van Duijn CM, Duijts L, Franco OH, van Ijzendoorn MH, et al. The generation R study: design and cohort update 2017. Eur J Epidemiol. (2016) 31:1243–64. doi: 10.1007/s10654-016-0224-9
16. Netherlands S: Immigrants in the Netherlands 2004 (Allochtonen in Nederland 2004). Den Haag/Heerlen: Statistics Netherlands (Centraal Bureau voor de Statistiek) 2004.
17. voor de Statistiek CB. Standaard Onderwijsindeling 2006. The Dutch Standard Classification of Education.
18. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
19. Carlson SA, Fulton JE, Lee SM, Foley JT, Heitzler C, Huhman M. Influence of limit-setting and participation in physical activity on youth screen time. Pediatrics. (2010) 126:e89–96. doi: 10.1542/peds.2009-3374
20. Achenbach TM, Rescorla L. Manual for the ASEBA Preschool Forms And Profiles. Vol. 30. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families (2000).
21. Achenbach TM, Rescorla LA. Reliability, cross-informant agreement, and stability. Manual ASEBA Preschool Forms Profiles. (2000) 30:74–100.
22. Tick NT, Koot HM, Verhulst FC. 14-year changes in emotional and behavioral problems of very young Dutch children. J Am Acad Child Adolesc Psychiatry. (2007) 46:1333–40. doi: 10.1097/chi.0b013e3181337532
23. Fang X, Bai G, Windhorst DA, Feeny D, Saigal S, Duijts L, et al. Feasibility and validity of the health status classification system-preschool (HSCS-PS) in a large community sample: the Generation R study. BMJ Open. (2018) 8:e022449. doi: 10.1136/bmjopen-2018-022449
24. Epstein NB, Baldwin LM, Bishop DS. The McMaster family assessment device. J Marital Fam Ther. (1983) 9:171–80. doi: 10.1111/j.1752-0606.1983.tb01497.x
25. Byles J, Byrne C, Boyle MH, Offord DR. Ontario child health study: reliability and validity of the general functioning subscale of the mcmaster family assessment device. Fam Process. (1988) 27:97–104. doi: 10.1111/j.1545-5300.1988.00097.x
26. Raat H, Botterweck AM, Landgraf JM, Hoogeveen WC, Essink-Bot M-L. Reliability and validity of the short form of the child health questionnaire for parents (CHQ-PF28) in large random school based and general population samples. J Epidemiol Commun Health. (2005) 59:75–82. doi: 10.1136/jech.2003.012914
27. Raat H, Bonsel GJ, Essink-Bot M-L, Landgraf JM, Gemke RJBJ. Reliability and validity of comprehensive health status measures in children: the Child Health questionnaire in relation to the health utilities index. J Clin Epidemiol. (2002) 55:67–76. doi: 10.1016/S0895-4356(01)00411-5
28. Fagerland MW. T-tests, non-parametric tests, and large studies—a paradox of statistical practice? BMC Med Res Methodol. (2012) 12:1–7. doi: 10.1186/1471-2288-12-78
29. Cohen J. Statistical Power Analysis For The Behavioral Sciences. Academic press (2013). doi: 10.4324/9780203771587
30. Greenland S, Finkle WD. A critical look at methods for handling missing covariates in epidemiologic regression analyses. Am J Epidemiol. (1995) 142:1255–64. doi: 10.1093/oxfordjournals.aje.a117592
31. Ravens-Sieberer U, Erhart M, Wille N, Bullinger M. Health-related quality of life in children and adolescents in Germany: results of the BELLA study. Eur Child Adolesc Psychiatry. (2008) 17:148–56. doi: 10.1007/s00787-008-1016-x
32. Michel G, Bisegger C, Fuhr DC, Abel T. Age and gender differences in health-related quality of life of children and adolescents in Europe: a multilevel analysis. Qual Life Res. (2009) 18:1147–57. doi: 10.1007/s11136-009-9538-3
33. Björkqvist K, Lagerspetz KMJ, Kaukiainen A. Do girls manipulate and boys fight? Developmental trends in regard to direct and indirect aggression. Aggress Behav. (1992) 18:117–27. doi: 10.1002/1098-2337(1992)18:2%3C117::AID-AB2480180205%3E3.0.CO;2-3
34. Adler NE, Ostrove JM. Socioeconomic status and health: what we know and what we don't. Ann N Y Acad Sci. (1999) 896:3–15. doi: 10.1111/j.1749-6632.1999.tb08101.x
35. Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. (1986) 51:1173. doi: 10.1037/0022-3514.51.6.1173
36. Bradley RH, Corwyn RF. Socioeconomic status and child development. Annu Rev Psychol. (2002) 53:371–99. doi: 10.1146/annurev.psych.53.100901.135233
38. Brooks-Gunn J, Duncan GJ. The effects of poverty on children. Future Child. (1997) 7:55–71. doi: 10.2307/1602387
39. Gaspar T, Matos MG, Pais R, Jose L, Leal I, Ferreira A. Health-related quality of life in children and adolscents and associated factors. J Cognitive Behav Psychother. (2009) 9:33–48.
40. Gopinath B, Hardy LL, Baur LA, Burlutsky G, Mitchell P. Physical activity and sedentary behaviors and health-related quality of life in adolescents. Pediatrics. (2012) 130:e167–74. doi: 10.1542/peds.2011-3637
41. Lacy KE, Allender SE, Kremer PJ, de Silva-Sanigorski AM, Millar LM, Moodie ML, et al. Screen time and physical activity behaviours are associated with health-related quality of life in Australian adolescents. Qual Life Res. (2012) 21:1085–99. doi: 10.1007/s11136-011-0014-5
42. Vuillemin A, Boini S, Bertrais S, Tessier S, Oppert J-M, Hercberg S, et al. Leisure time physical activity and health-related quality of life. Prev Med. (2005) 41:562–9. doi: 10.1016/j.ypmed.2005.01.006
43. Boyle SE, Jones GL, Walters SJ. Physical activity, quality of life, weight status and diet in adolescents. Qual Life Res. (2010) 19:943–54. doi: 10.1007/s11136-010-9659-8
44. Wallander JL. Psychosocial adjustment of children with chronic physical condition. Pediatr Psychol. (2003) 141–58.
Appendix
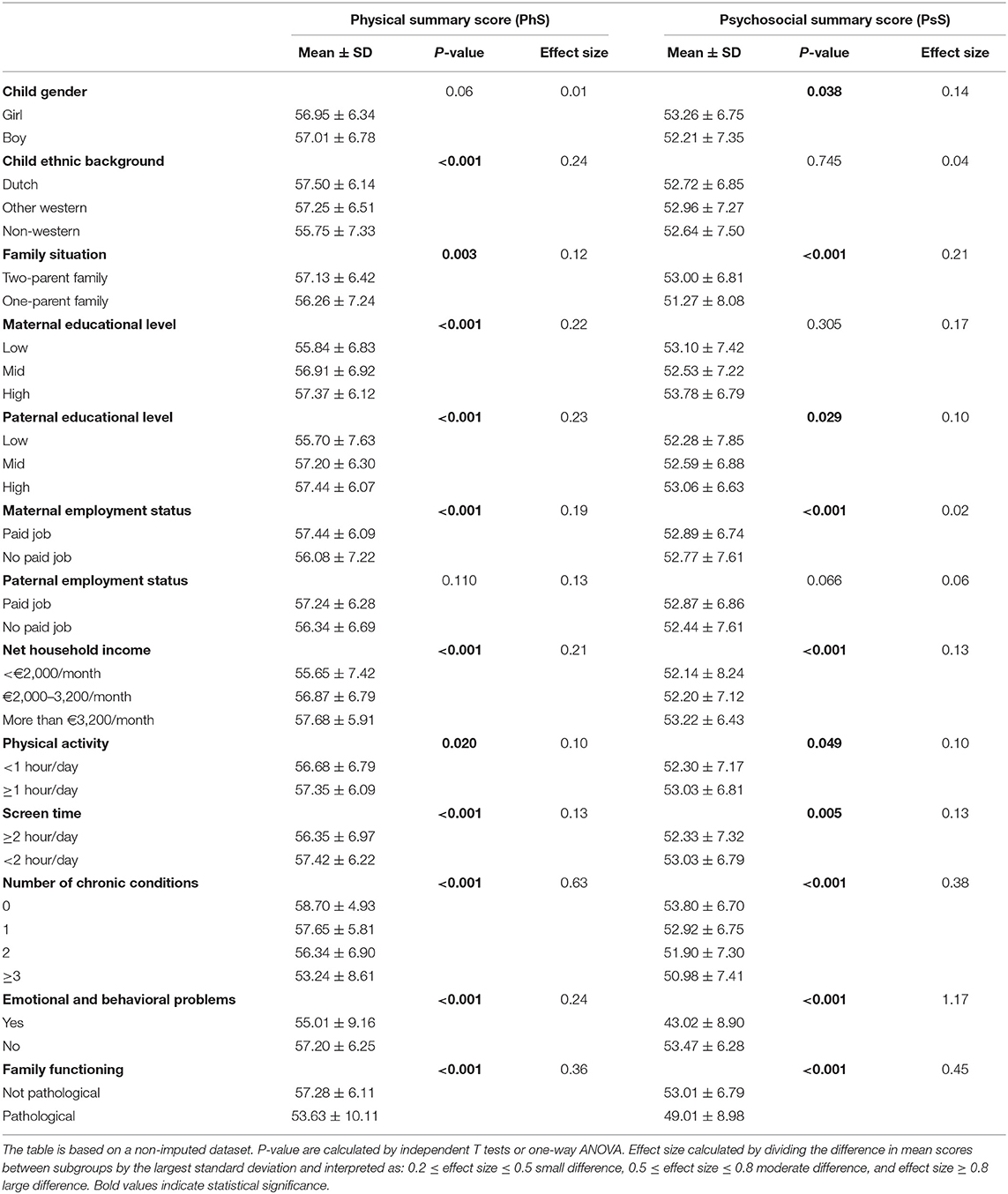
Appendix Table 1. Univariate analysis of physical and psychosocial summary score between subgroups according to socio-demographic characteristics, health-related lifestyle behaviors and health and well-being of the child and family (n = 4,202).
Keywords: socio-demographic characteristics, socioeconomic status, health-related lifestyle behaviors, chronic conditions, HRQOL, early elementary school age children
Citation: You Y, van Grieken A, Estévez-López F, Yang-Huang J and Raat H (2022) Factors Associated With Early Elementary Child Health-Related Quality of Life: The Generation R Study. Front. Public Health 9:785054. doi: 10.3389/fpubh.2021.785054
Received: 28 September 2021; Accepted: 22 December 2021;
Published: 27 January 2022.
Edited by:
Steven Hirschfeld, Uniformed Services University of the Health Sciences, United StatesReviewed by:
Si-Tong Chen, Victoria University, AustraliaLarry Kenith Olsen, Logan University, United States
Copyright © 2022 You, van Grieken, Estévez-López, Yang-Huang and Raat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hein Raat, aC5yYWF0QGVyYXNtdXNtYy5ubA==