 Bing Cao
Bing Cao Yuxiao Zhao1
Yuxiao Zhao1 Zhongyu Ren
Zhongyu Ren Roger S. McIntyre
Roger S. McIntyre Kayla M. Teopiz
Kayla M. Teopiz Xiao Gao
Xiao Gao- 1Key Laboratory of Cognition and Personality, Faculty of Psychology, Ministry of Education, Southwest University, Chongqing, China
- 2National Demonstration Center for Experimental Psychology Education, Southwest University, Chongqing, China
- 3College of Physical Education, Southwest University, Chongqing, China
- 4Mood Disorders Psychopharmacology Unit, University Health Network, Toronto, ON, Canada
- 5Pharmacy Department, The Central Hospital of Jiangjin, Chongqing, China
Psychological stress is a negative affective state. The association between physical activity and psychological stress was commonly reported in previous researches. Few published studies with large sample sizes have explored such an association in Chinese population. The current research aims to assess the association between perceived stress and physical activity preferences, as well as the association between risk of high perceived stress and physical activity behaviors (e.g., sports-, transport-, occupational-related physical activity, sedentary activities and time in bed). The data were collected from the China Health and Nutrition Survey (CHNS) in 2015. Generalized linear models and logistic regression models were used to explore the association between perceived stress and physical activity. In total, 11,066 participants were included in the current analysis. For physical activity preferences, we found that “like” preference of all six mentioned domains of activities contributed to lower perceived stress (i.e., lower perceived stress scale −14 score, all β < 0 and p < 0.05). For physical activity behaviors, the results indicated that none/low intensity physical activity behaviors (e.g., sports-, occupational- related, sedentary) were associated with risk of high perceived stress, except that low intensity of transport-related activities seemed to be protective from high stress. However, the association between intensity of physical activity behaviors and perceived stress was not simply the higher the better. High intensity of all these physical activity behaviors was also associated with high perceived stress. Our findings suggest that positive preferences and moderate physical activity behaviors were associated with low perceived stress. The findings herein highlight the effect of regulating physical activity on perceived stress, as well as inform potential strategies to reduce psychological stress.
Background
Psychological stress is a negative affective state, which is commonly associated with negative health outcomes, especially when it is chronic and unpredictable (1, 2). Accumulating evidence suggests that psychological stress is positively associated with some outcomes (e.g., smoking cigarettes, alcohol consumption) while negatively associated with other outcomes (e.g., physical activity) (3, 4). Several studies have reported that individuals may relieve or cope with stress via unhealthy yet rewarding behaviors, such as sedentary behavior and increased unhealthy eating behavior (5). In addition to changes in behaviors, chronic stress is also associated with disparate physiologic changes (e.g., increase in catecholamine release, cortisol dysregulation, and allosteric load) (6, 7). It is a highly replicated finding that chronic unpredictable stress predisposes and portends increased risk for obesity, metabolic syndrome, select forms of cancer, cardiovascular disease, mental disorders (e.g., major depressive disorder), as well as decreased quality of life and function (8, 9). The hazards posed by chronic, unpredictable stress provide the impetus for identifying potential risk factors for reduced health outcomes in stressed individuals.
Physical activity is defined as any movement of the body that results from skeletal muscles (10, 11). Epidemiological studies have reported on the bidirectional relationship between physical activity and stress, suggesting that daily physical activity may help to prevent, as well as improve, general physical and mental well-being in the context of stress (12, 13). Stults-Kolehmainen et al. reported that physical activity moderates the effect of excessive psychosocial stress and negative health outcomes. Additionally, they reported that the experience of stress attenuates efforts to be physically active (14). Extant literature also suggests that the interaction between physical activity and stress may be associated with several biological pathways, including but not limited to, aberrant brain connectivity, regulations in the hypothalamic-pituitary-adrenal axis, stimulation of a neurogenic processes, as well as alterations in the inflammatory system (15, 16). A recent publication pointed out that moderate level of physical activity is needed to retain a low level of stress during the COVID-19 pandemic lockdown (17). Physical activity interventions are also reported to tend to improve overall perceived stress mental health (18, 19). Numbers of previous basis found that higher physical activity levels are related to less perceived stress (20). Despite the overwhelming evidence suggesting an association between physical activity and mental health benefits (21, 22), whether there is a dose-response association between all the types of physical activities and mental health is still in debate. Some researchers argue that only leisure-time physical activity, but not transport-, occupational-, as well as sedentary activities are related to perceived stress and health (23). Moreover, the effect of physical activities on mental health seems not simply dose-response. Some researchers suggested that compared to highly vigorous physical activity, a moderate level would be more beneficial (24, 25). A recent study among preschool children reported that both low and high physical activity levels are related to unfavorable sleep characteristics. High physical activity is also found to be associated with increased post-traumatic stress disorder (PTSD) symptomatology among individuals aged 15 years and older in South Africa. Thus, the relationship between intensities of different types of physical activity and perceived psychological stress still needs further evaluation.
To the best of our knowledge, few published studies with large sample sizes have explored the association between physical activity and perceived psychological stress in the Chinese population. In addition, the exploration of the relationship between physical activity preferences and perceived stress have not been extensively reported (26). Against this background, the objective of the study herein is to examine the association between physical activity and perceived stress in a largescale sample of the Chinese population. We used the data from the China Health and Nutrition Survey (CHNS) to assess (1) the associations between perceived stress and physical activity preferences; (2) the associations between risk of high perceived stress and different categories of physical activity behaviors (e.g., sports-, transport-, occupational-related physical activity, sedentary activities, and time in bed). It was hypothesized that (1) perceived stress would be negatively associated with physical activity preferences; (2) both low and high intensity physical activity behaviors would be associated with the risk of high perceived stress.
Methods
Data Resource and Study Participants
We used the publicly available de-identified data from CHNS, which is an international collaborative project conducted by the National Institute for Nutrition and Health of the Chinese Center for Disease Control and Prevention and the University of North Carolina at Chapel Hill in the United States. The CHNS is a population-based longitudinal household survey which drew a sample using a multistage, random cluster sampling method. From 1989 to 2015, individual-level information on health, socioeconomic status, and social and family networks was collected in 11 waves (1989, 1991, 1993, 1997, 2000, 2004, 2006, 2009, 2011, 2015, and 2018, respectively). The first survey to incorporate Perceived Stress Scale (PSS)-Chinese version was conducted in 2015, and the most recent database in 2018 has not been released. As a result, the current study used data from the recently released 2015 wave of survey data from the CHNS. More detailed information about the CHNS project is available from the following URL: https://www.cpc.unc.edu/projects/china.
Outcome Definition and Sample Selection Criteria
Perceived stress was measured with the Chinese version of the fourteen-item PSS (PSS-14). Accuracy of the Chinese version was ensured by translating the original PSS-14 from English to Chinese, and subsequently back into English (27). Each item was rated on a 5-point Likert-type scale, ranging from 0 = “never” to 4 = “very often.” The scale can be divided into two subscales: negative subscale (items 1, 2, 3, 8, 11, 12, and 14) and positive subscale (items 4, 5, 6, 7, 9, 10, and 13). The negative subscale asked frequency of negative incidents or feelings, such as “In the last month, how often have you felt that you were unable to control important things in your life?”. The positive subscale contained positively stated items, e.g., “In the last month, how often have you felt confident about your ability to handle your personal problems?”. Although the original PSS-14 contains a two-factor structure, this two-factor model did not fit well with the Chinese-validated version (27). Because of the weak correlation between these two factors (r = 0.2), scores of two subscales will be reported as a whole rather than separately to indicate the total perceived stress (28, 29), which ranges from 0 to 56. The one-factor structure showed satisfactory internal consistency (corresponding Cronbach's alpha = 0.83) (27). To obtain meaningful odds ratios (ORs), the variable was rescaled by the median of PSS-14 total score total as the unit of measure (i.e., low perceived stress and high perceived stress), which has also been used in previous studies [e.g., (30)].
In the CHNS questionnaire, the physical activity and inactivity preferences were assessed with the six activities listed as follows: Walking and Tai Chi, Sports (e.g., ping pong, badminton, tennis, soccer, basketball, volleyball), Body building, Watching TV, Computer/Video games, and Reading. The first three in the list are physical activity, and the other three are inactivity (31). For each activity and inactivity, the respondents were asked to rate their preference using the following responses: like very much, like somewhat, neutral, dislike somewhat, dislike very much, or does not participate. For physical activity participation, the respondents were asked to indicate whether they have participated in this activity selecting one of the options: “yes,” “no,” or, “unknown.” If respondents selected “yes” to a given item, they received a follow up question regarding participation time spent on that activity during a typical weekday or weekend day.
To create a measure of energy expenditure of physical activity behaviors, time spent in sport-related activities (i.e., martial arts; gymnastics, track and field; walking; soccer, basketball; badminton, volleyball), transport-related activities (i.e., by bus/subway; by bike; by foot; by car/taxi), and occupational-related activities (i.e., light activity; moderate activity; heavy activity) was multiplied by a specific metabolic equivalent of task (MET) intensity value. The final unit was MET-hours/week, which was the product of average number of hours spent per day participating in each physical activity and the MET score for that activity. The calculation method of MET was based on 2011 update of a major compendium of physical activities (32) and previous publication in Chinese population (33, 34). The MET value of each physical activity was listed in Supplementary Table 1. The sedentary activities (i.e., watching TV; VCR, VCDS, DVDS; video games; computer usage; reading, writing; surfing internet; joining chat rooms; playing computer games; watching videos/movies online; other sedentary activity) and time in bed were evaluated by the total time with the unit of hours/day.
We applied the sample selection from the dataset and merged the related files. Firstly, we merged the file of PSS, physical activity participation and preferences, and the basic demographic characteristics including: age, gender, education level, weight (kg), height (m), daily time in bed (hours), location, province, smoking status, alcohol consumption, and other necessary information. Then participants <18 years old who had indicated they do not know the level of their engagement in physical activities, or had missing data on stress outcomes, were excluded from analysis. Therefore, the final sample was comprised of 11, 066 (males = 5,870, females = 5,196).
Statistical Analysis
Body mass index (BMI) was calculated by the weight (kg) divided by the square of height (m). MET rate time was calculated as follows: MET rate time = (time spent on each workday*5 + time spent on each weekend day*2)/7. Descriptive statistics was performed for the basic characteristics analysis. The continuous variables were summarized by means and standard deviations (SD), and the categorical variables were summarized by frequencies and proportions, respectively. For continuous variables, the independent samples t-test or one-way ANOVA was used for comparisons between two or more than two independent groups.
For categorical variables, statistical significance between various groups was tested using the χ2-test. The generalized linear models were used to explore the associations between perceived stress and physical activity preferences. Logistic regression models were used to explore the associations between risk of high perceived stress and physical activity behaviors. ORs and their 95% confidence intervals (CIs) were estimated using maximum likelihood methods. The variables of age, gender, community category (urban or rural) were included as covariates in the above models. The association was considered to be statistically significant if the 2-sided p-value is <0.05. All analyses were performed using Stata 15.0 (Stata Corp LP, College Station, TX, USA).
Results
Basic Characteristics of Subjects
Table 1 shows descriptive statistics for the variables of basic characteristics in included participants. The results were illustrated according to gender (i.e., male or female), age group (i.e., 18–40, 41–59, 60 years old and above), and community category (i.e., urban, rural). In total, 11,066 participants were included in the current study. The participants had a mean age of 52.0 (SD of 15.4) years and a mean BMI of 24.3 (SD of 4.2). Female participants made up 53.1% of the sample (n = 5,870). Most of the participants (60.7%) were from rural communities.
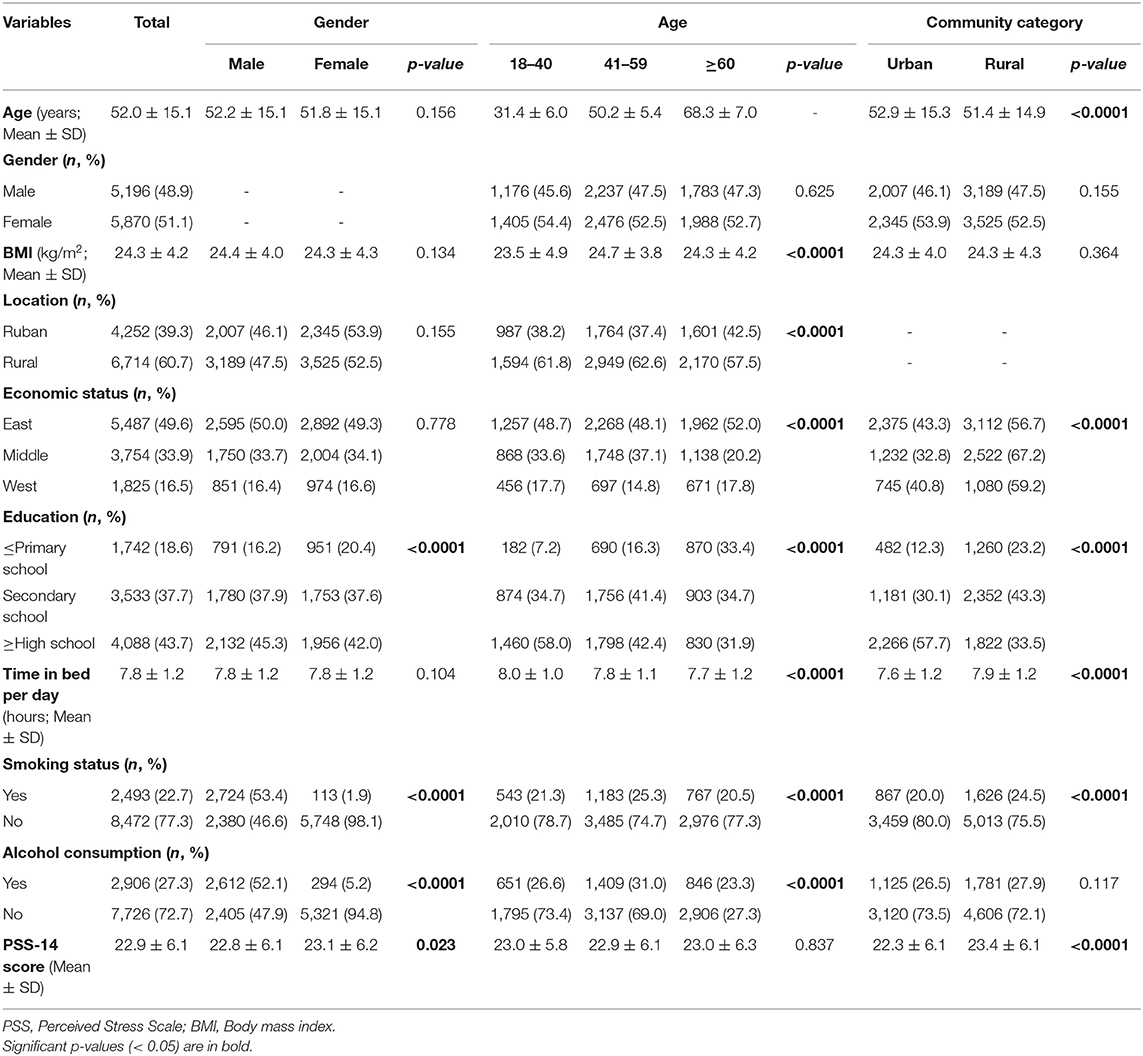
Table 1. Basic characteristics of included participants.
The average time in bed per day of the participants was 7.8 h (SD of 1.2). The differences of education levels were statistically significant in different gender, age group and community category (all p < 0.0001). Reports of smoking and alcohol consumption were significantly different between males and females, as well as different age groups (both p < 0.0001). No significant difference of reported smoking behavior was found between participants from urban and rural communities (p = 0.117). Female (p = 0.023) and participants from rural communities (p < 0.0001) reported higher perceived stress.
Association Between Perceived Stress and Physical Activity Preferences
We conducted an analysis to explore the associations between perceived stress and physical activity and inactivity preferences. The means and SDs were also calculated in each group of each activity preference. The “Neutral” activity preference option was considered as a reference value. It was observed from the models that the PSS-14 score was negatively correlated with “like somewhat,” “like very much” in all six investigated domains of physical activity and inactivity preferences both before and after adjusting the potential confounders of age, gender and community category (all β < 0 and p < 0.05). Positive correlations were also found between PSS-14 scores with “does not participate” in walking/Tai Chi, watching TV, computer/video games and reading (all β > 0 and p < 0.05). Additionally, the results indicated that PSS-14 score was negatively correlated with “dislike” of walking/Tai Chi, computer/video games and reading. The details are shown in Table 2.
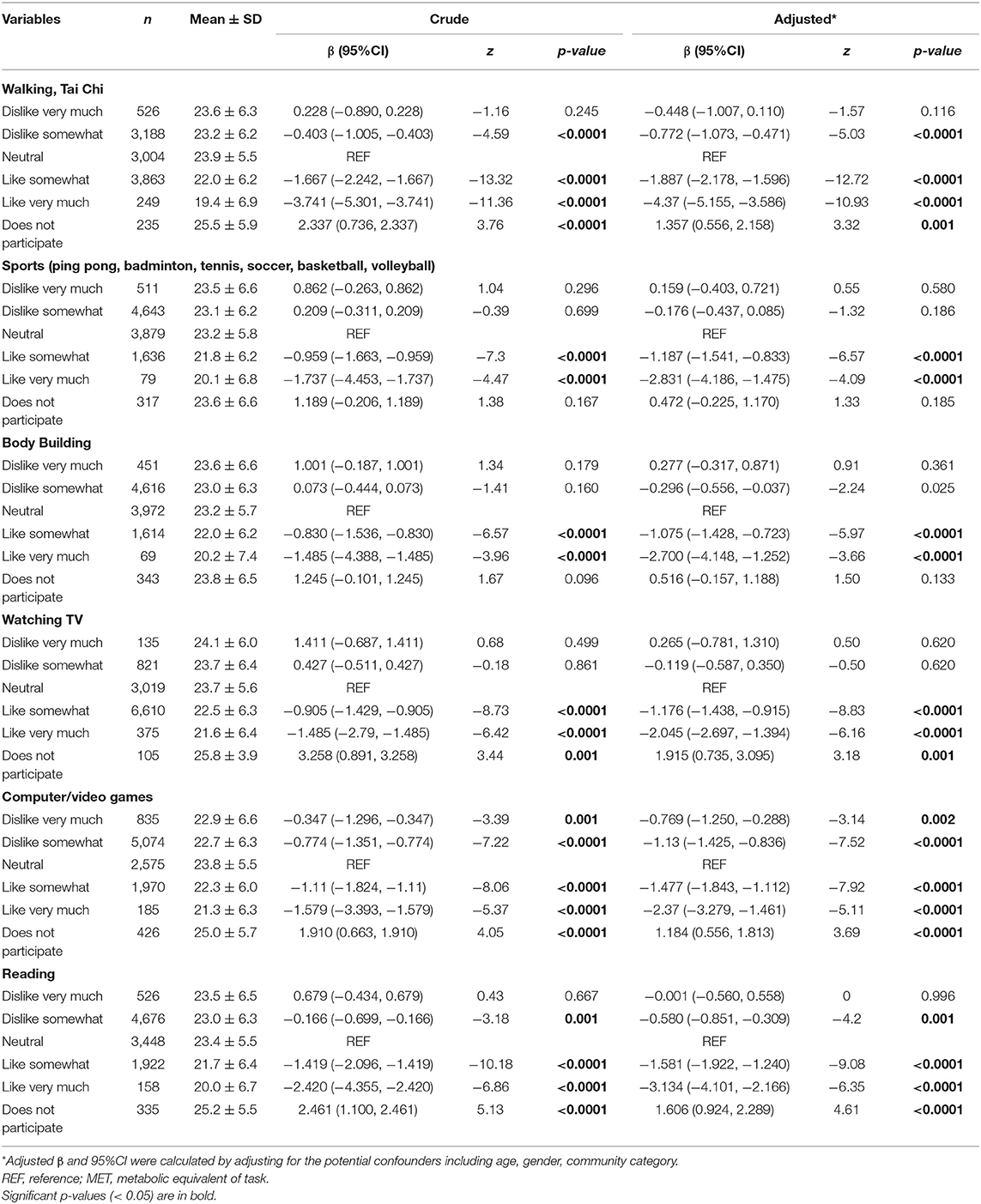
Table 2. Association between perceived stress and physical activity preferences.
The Association Between Risk of High Perceived Stress and Physical Activity Behavior
We rescaled the variable of PSS-14 total scores into low and high perceived stress by the median of their values. Table 3 shows the logistic regressions assessing the associations between risk of high perceived stress and physical activity behaviors. For sports-related physical activity, both none and high (>28) MET-hours/week were associated with risk of high perceived stress (AOR = 1.381, 95%CI: 1.124, 1.696; p = 0.002; AOR = 1.255, 95%CI: 1.095, 1.438; p = 0.001, respectively).
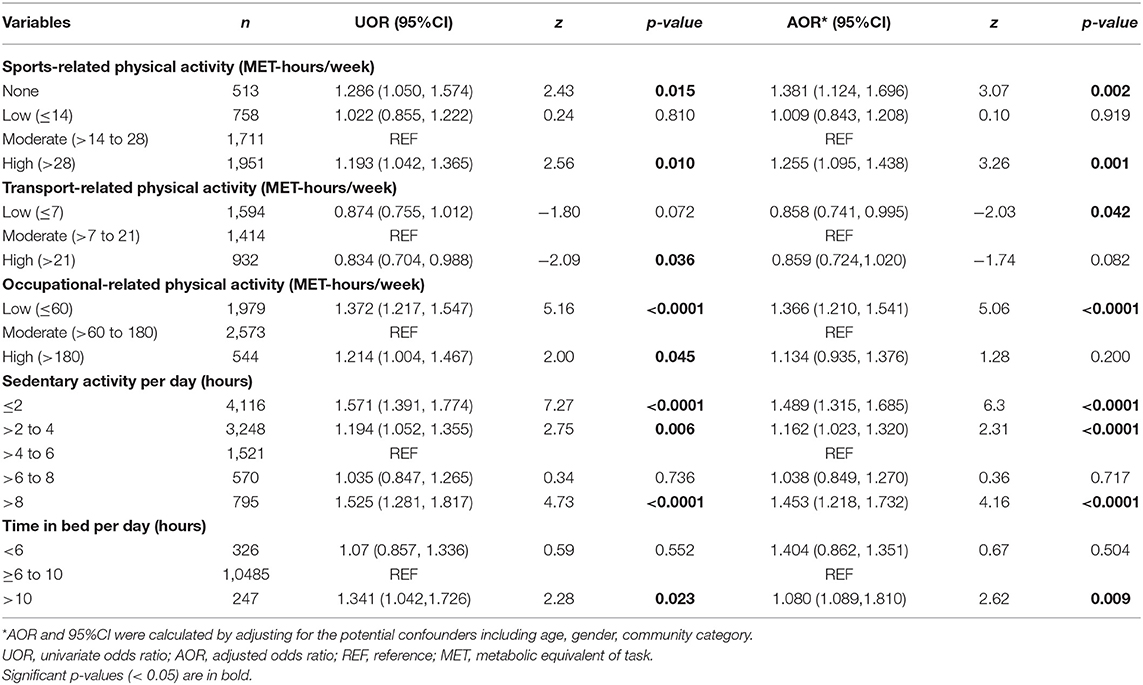
Table 3. The association between risk of high perceived stress and physical activity.
After adjusting age, gender and community category, low transport-related physical activity was associated with low perceived stress (AOR = 0.858, 95%CI: 0.741, 0.995; p = 0.042). Low occupation-related physical activity was associated with risk of high perceived stress. Significant associations between both low and high sedentary activity per day and risk of high perceived stress were also reported. Additionally, time in bed >10 h/day was associated with risk of high perceived stress (AOR = 1.404, 95%CI: 1.089, 1.81; p = 0.009).
Discussion
The overarching goal of the study herein was to characterize the association between perceived stress and physical activity preferences and behaviors. By using publicly available data from CHNS in this analysis, we evaluated the association between perceived stress and six physical activity and inactivity preferences, as well as the association between risk of high perceived stress and physical activity behaviors in 11,066 participants from the Chinese population. For the physical activity preferences, we found that “like” preference of all six mentioned domains of activities is associated with lower perceived stress (i.e., higher PSS-14 score). Moreover, the preferences of “dislike” and/or “does not participate” in some activities (e.g., walking/Tai Chi, computer/video games and reading) were associated with higher perceived stress.
For the physical activity behaviors, the results indicated that both no physical activity and low intensity of physical activities (such as sports-, occupational- related, sedentary, time in bed) were associated with risk of high perceived stress. However, low intensity of transport—related activities were protective from high stress. Our results herein suggest that greater intensity of physical activities may be beneficial in the prevention of high psychological stress.
To our knowledge, relatively few prior studies have explored the relationship between physical activity as well as inactivity preferences and psychological stress in a largescale sample of the Chinese population. In general, the individuals who “like” all six domains of activities in the preference questionnaire have lower perceived stress than those who “does not participate in” or “dislike.” Moreover, reports of analyses conducted on CHNS data indicated that leisure time physical activity preference was a significant predictor of actual leisure time physical activity behavior (26).
A separate study of patients with lung cancer revealed that physical activity preferences were associated with social support and self-efficacy (35). According to our existing evidence, positive activity preferences are associated with low perceived stress, especially in activities related to sports (i.e., walking, Tai Chi, sports, body building). However, potential underlying psychological mechanisms require further investigation.
Previous studies have assessed the effect of physical activity participation on psychological stress, and have reported that high-intensity physical activity is better for stress prevention and management than low-intensity leisure time physical activity (20, 36). One possible explanation is that prior physical activity before a stressful situation can reduce cortisol concentrations during psychosocial stress and furtherly reduce the impact of stress on health (37). However, from our current analysis, we found that excessive high-intensity sports-related physical activities were not correlated with lower perceived stress. In fact, too much exercise may backfire and lead to higher level of stress. Since it can be observed in our study that both none participation as well as high MET-hours/week sports-related physical activity increased the risk of high perceived stress when compared with moderate intensity of physical activities, our findings supported the U-shaped relationship between exercise intensity and psychological stress.
We also observed that low intensity of transport-related physical activity had a protective effect on perceived stress. Additionally, our results suggest that low intensity MET-hours/week of occupational-related activities were related to increased risk of high perceived stress when compared with the moderate intensity. This is in accordance with additional reports of physical activity as a protective factor for psychological stress (38).
It has been reported that psychosocial stress is one risk factor for sedentary behavior in pregnant women (39); however, additional studies have reported that not all forms of sedentary activities are linked to perceived stress (40). Moreover, it has been reported that sleep deprivation may be a risk factor for psychological stress (41, 42), although we did not find the association between lack of sleep (i.e., <6 h/day) and high perceived stress in our sample. From our findings, we also determined that spending too much time in bed (i.e., >10 h/day) may be a risk factor for perceived stress. Although there are few studies focusing on the relationship between excessive sleep or hypersomnia and psychological stress, previous studies have found that a longer time spent in bed is associated with negative mental health outcomes, including but not limited to, depressed mood and suicidality (27, 43, 44). It was separately reported in a group of civil servants in Japan that that a U-shaped association exists between time in bed with poor sleep and psychosocial stress (45).
Overall, our study revealed that the relationship between perceived stress and physical activity preferences as well as behaviors were not linear associations. There should be a suitable reference range for each activity to reduce the perceived stress. Our findings herein provide preliminary evidence for formulating a reasonable reference range to regulate physical activity. Further longitudinal researches are needed to clarify the influence of specific physical activity on alteration of perceived stress.
Limitations
Several methodological aspects of our study may affect inferences and interpretations of our findings. Firstly, as this analysis was cross-sectional, the results can only be concluded as associations with no implication of causality or directionality of the effect. Secondly, the CHNS delimited its assessment of perceived stress levels one time with PSS-14, which is a self-reported scale. Thirdly, because some important variables (e.g., the frequency of physical activity behaviors) were not available and some data of individuals were missing in our download version, our current analysis was limited to the accessible data. Notwithstanding the limitations, the results of our study provide an important basis for future intervention to reduce perceived stress and improve quality of life and well-being in a large-scale population.
Conclusion
In summary, our results indicated that positive attitudinal preferences to select activities as well as moderate physical activity were associated with low perceived stress in a large-scale sample of the Chinese population. The findings herein also provide an empirical basis for prescribing exercise intensity at a population level and provide impetus to explore protective biological factors mediating the health outcomes observed.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://www.cpc.unc.edu/projects/china.
Ethics Statement
The studies involving human participants were reviewed and approved by University of North Carolina at Chapel Hill. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
LD and BC conceived and designed the study. BC and ZR performed the statistical analysis. BC, LD, and XG contributed to the discussion. YZ, RM, KT, LD, and ZR revised the paper. All authors have read and approved the final version of this article.
Funding
This work was supported by the Startup Foundation for Talents from Southwest University (SWU019039).
Conflict of Interest
RM has received research grant support from CIHR/GACD/Chinese National Natural Research Foundation; speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Abbvie. RM is the CEO of Braxia Scientific Corp. KT has received personal fees from Braxia Scientific Corp.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
This research uses data from the China Health and Nutrition Survey (CHNS). We thank the National Institute of Nutrition and Food Safety (China Center for Disease Control and Prevention), Carolina Population Center (University of North Carolina at Chapel Hill) for providing analysis files.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.697484/full#supplementary-material
References
1. Roderigo T, Benson S, Schols M, Hetkamp M, Schedlowski M, Enck P, et al. Effects of acute psychological stress on placebo and nocebo responses in a clinically relevant model of visceroception. Pain. (2017) 158:1489–98. doi: 10.1097/j.pain.0000000000000940
2. Michels N. Biological underpinnings from psychosocial stress towards appetite and obesity during youth: research implications towards metagenomics, epigenomics and metabolomics. Nutr Res Rev. (2019) 32:282–93. doi: 10.1017/S0954422419000143
3. Tavolacci MP, Ladner J, Grigioni S, Richard L, Villet H, Dechelotte P. Prevalence and association of perceived stress, substance use and behavioral addictions: a cross-sectional study among university students in France, 2009-2011. BMC Public Health. (2013) 13:724. doi: 10.1186/1471-2458-13-724
4. Slavich GM. Social safety theory: a biologically based evolutionary perspective on life stress, health, and behavior. Annu Rev Clin Psychol. (2020) 16:265–95. doi: 10.1146/annurev-clinpsy-032816-045159
5. Krueger PM, Chang VW. Being poor and coping with stress: health behaviors and the risk of death. Am J Public Health. (2008) 98:889–96. doi: 10.2105/AJPH.2007.114454
6. Brietzke E, Mansur RB, Soczynska J, Powell AM, McIntyre RS A. theoretical framework informing research about the role of stress in the pathophysiology of bipolar disorder. Prog Neuropsychopharmacol Biol Psychiatry. (2012) 39:1–8. doi: 10.1016/j.pnpbp.2012.05.004
7. Martinez de Toda I, Miguelez L, Siboni L, Vida C, De la Fuente M. High perceived stress in women is linked to oxidation, inflammation and immunosenescence. Biogerontology. (2019) 20:823–35. doi: 10.1007/s10522-019-09829-y
8. Myers B, Scheimann JR, Franco-Villanueva A, Herman JP. Ascending mechanisms of stress integration: implications for brainstem regulation of neuroendocrine and behavioral stress responses. Neurosci Biobehav Rev. (2017) 74:366–75. doi: 10.1016/j.neubiorev.2016.05.011
9. Tomiyama AJ. Stress and obesity. Annu Rev Psychol. (2019) 70:703–18. doi: 10.1146/annurev-psych-010418-102936
10. Higueras-Fresnillo S, Cabanas-Sanchez V, Garcia-Esquinas E, Rodriguez-Artalejo F, Martinez-Gomez D. Physical activity attenuates the impact of poor physical, mental, and social health on total and cardiovascular mortality in older adults: a population-based prospective cohort study. Qual Life Res. (2018) 27:3293–302. doi: 10.1007/s11136-018-1974-5
11. Powell KE, King AC, Buchner DM, Campbell WW, DiPietro L, Erickson KI, et al. The scientific foundation for the physical activity guidelines for Americans, 2nd edition. J Phys Act Health. (2018) 16:1–11. doi: 10.1123/jpah.2018-0618
12. Cowley J, Kiely J, Collins D. Is there a link between self-perceived stress and physical activity levels in Scottish adolescents? Int J Adolesc Med Health. (2017) 31. doi: 10.1515/ijamh-2016-0104
13. Brockmann AN, Ross KM. Bidirectional association between stress and physical activity in adults with overweight and obesity. J Behav Med. (2020) 43:246–53. doi: 10.1007/s10865-020-00145-2
14. Stults-Kolehmainen MA, Sinha R. The effects of stress on physical activity and exercise. Sports Med. (2014) 44:81–121. doi: 10.1007/s40279-013-0090-5
15. Moylan S, Eyre HA, Maes M, Baune BT, Jacka FN, Berk M. Exercising the worry away: how inflammation, oxidative and nitrogen stress mediates the beneficial effect of physical activity on anxiety disorder symptoms and behaviours. Neurosci Biobehav Rev. (2013) 37:573–84. doi: 10.1016/j.neubiorev.2013.02.003
16. Mury P, Chirico EN, Mura M, Millon A, Canet-Soulas E, Pialoux V. Oxidative stress and inflammation, key targets of atherosclerotic plaque progression and vulnerability: potential impact of physical activity. Sports Med. (2018) 48:2725–41. doi: 10.1007/s40279-018-0996-z
17. Lipert A, Kozlowski R, Timler D, Marczak M, Musial K, Rasmus P, et al. Physical activity as a predictor of the level of stress and quality of sleep during COVID-19 lockdown. Int J Environ Res Public Health. (2021) 18:5811. doi: 10.3390/ijerph18115811
18. Kroll LS, Hammarlund CS, Westergaard ML, Nielsen T, Sloth LB, Jensen RH, et al. Level of physical activity, well-being, stress and self-rated health in persons with migraine and co-existing tension-type headache and neck pain. J Headache Pain. (2017) 18:46. doi: 10.1186/s10194-017-0753-y
19. Gilbert L, Gross J, Lanzi S, Quansah DY, Puder J, Horsch A. How diet, physical activity and psychosocial well-being interact in women with gestational diabetes mellitus: an integrative review. BMC Pregnancy Child. (2019) 19:60. doi: 10.1186/s12884-019-2185-y
20. Schultchen D, Reichenberger J, Mittl T, Weh TRM, Smyth JM, Blechert J, et al. Bidirectional relationship of stress and affect with physical activity and healthy eating. Br J Health Psychol. (2019) 24:315–33. doi: 10.1111/bjhp.12355
21. Joseph RP, Royse KE, Benitez TJ, Pekmezi DW. Physical activity and quality of life among university students: exploring self-efficacy, self-esteem, and affect as potential mediators. Qual Life Res. (2014) 23:659–67. doi: 10.1007/s11136-013-0492-8
22. Lopez-Bueno R, Andersen LL, Smith L, Lopez-Sanchez GF, Mompel J, Casedas L, et al. Physical activity and perceived stress at work in university workers: a cross-sectional study. J Sports Med Phys Fitness. (2020) 60:314–9. doi: 10.23736/S0022-4707.19.10259-9
23. Bogaert I, De Martelaer K, Deforche B, Clarys P, Zinzen E. Associations between different types of physical activity and teachers' perceived mental, physical, and work-related health. BMC Public Health. (2014) 14:534. doi: 10.1186/1471-2458-14-534
24. Holmes MD, Chen WY, Feskanich D, Kroenke CH, Colditz GA. Physical activity and survival after breast cancer diagnosis. JAMA. (2005) 293:2479–86. doi: 10.1001/jama.293.20.2479
25. Kang KD, Bae S, Kim HJ, Hwang IG, Kim SM, Han DH. The relationship between physical activity intensity and mental health status in patients with breast cancer. J Korean Med Sci. (2017) 32:1345–50. doi: 10.3346/jkms.2017.32.8.1345
26. Zhou J, Britigan DH, Rajaram SS, Wang H, Su D. Association between leisure time physical activity preference and behavior: evidence from the China Health and Nutrition Survey, 2004-2011. BMC Public Health. (2017) 17:451. doi: 10.1186/s12889-017-4386-5
27. Huang F, Wang H, Wang Z, Zhang J, Du W, Su C, et al. Psychometric properties of the perceived stress scale in a community sample of Chinese. BMC Psychiatry. (2020) 20:130. doi: 10.1186/s12888-020-02520-4
28. Reis RS, Hino AA, Anez CR. Perceived stress scale: reliability and validity study in Brazil. J Health Psychol. (2010) 15:107–14. doi: 10.1177/1359105309346343
29. Wang Z, Chen J, Boyd JE, Zhang H, Jia X, Qiu J, et al. Psychometric properties of the Chinese version of the perceived stress scale in policewomen. PLoS ONE. (2011) 6:e28610. doi: 10.1371/journal.pone.0028610
30. Abhay BM, Krishnakumar MK, Paul CN, Shashidhar GH. Differences in perceived stress and its correlates among students in professional courses. J Clin Diagn Res. (2012) 5:1228–33.
31. Tudor-Locke C, Ainsworth BE, Adair LS, Du S, Popkin BM. Physical activity and inactivity in Chinese school-aged youth: the China Health and Nutrition Survey. Int J Obes Relat Metab Disord. (2003) 27:1093–9. doi: 10.1038/sj.ijo.0802377
32. Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett DR Jr, Tudor-Locke C, et al. Compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. (2011) 43:1575–81. doi: 10.1249/MSS.0b013e31821ece12
33. Fan M, Lyu J, Guo Y, Bian Z, Yu C, Du H, et al. Regional differences on patterns of physical activity and leisure sedentary time: findings from the China Kadoorie Biobank study, including a million people from 10 regions. Zhonghua Liu Xing Bing Xue Za Zhi. (2015) 36:779–85. doi: 10.1002/kin.550250905
34. Pang Y, Kartsonaki C, Turnbull I, Guo Y, Yang L, Bian Z, et al. Metabolic and lifestyle risk factors for acute pancreatitis in Chinese adults: a prospective cohort study of 0.5 million people. PLoS Med. (2018) 15:e1002618. doi: 10.1371/journal.pmed.1002618
35. Lin YY, Lai YF, Lu HI, Lai YL, Lin CC. Physical activity preferences among patients with lung cancer in Taiwan. Cancer Nurs. (2013) 36:155–62. doi: 10.1097/NCC.0b013e31825f4db1
36. Fohr T, Tolvanen A, Myllymaki T, Jarvela-Reijonen E, Peuhkuri K, Rantala S, et al. Physical activity, heart rate variability-based stress and recovery, and subjective stress during a 9-month study period. Scand J Med Sci Sports. (2017) 27:612–21. doi: 10.1111/sms.12683
37. Wood CJ, Clow A, Hucklebridge F, Law R, Smyth N. Physical fitness and prior physical activity are both associated with less cortisol secretion during psychosocial stress. Anxiety Stress Coping. (2018) 31:135–45. doi: 10.1080/10615806.2017.1390083
38. Assadi SN. What are the effects of psychological stress and physical work on blood lipid profiles? Medicine (Baltimore). (2017) 96:e6816. doi: 10.1097/MD.0000000000006816
39. Sinclair I, St-Pierre M, Elgbeili G, Bernard P, Vaillancourt C, Gagnon S, et al. Psychosocial stress, sedentary behavior, and physical activity during pregnancy among canadian women: relationships in a diverse cohort and a nationwide sample. Int J Environ Res Public Health. (2019) 16:5150. doi: 10.3390/ijerph16245150
40. Felez-Nobrega M, Bort-Roig J, Briones L, Sanchez-Niubo A, Koyanagi A, Puigoriol E, et al. Self-reported and activPAL(TM)-monitored physical activity and sedentary behaviour in college students: not all sitting behaviours are linked to perceived stress and anxiety. J Sports Sci. (2020) 38:1566–74. doi: 10.1080/02640414.2020.1748359
41. Liu JC, Verhulst S, Massar SA, Chee MW. Sleep deprived and sweating it out: the effects of total sleep deprivation on skin conductance reactivity to psychosocial stress. Sleep. (2015) 38:155–9. doi: 10.5665/sleep.4346
42. Schwarz J, Gerhardsson A, van Leeuwen W, Lekander M, Ericson M, Fischer H, et al. Does sleep deprivation increase the vulnerability to acute psychosocial stress in young and older adults? Psychoneuroendocrinology. (2018) 96:155–65. doi: 10.1016/j.psyneuen.2018.06.003
43. Gubelmann C, Guessous I, Theler JM, Haba-Rubio J, Gaspoz JM, Marques-Vidal P. Trends and determinants of time in bed in Geneva, Switzerland. J Clin Sleep Med. (2014) 10:1129–35. doi: 10.5664/jcsm.4116
44. Kim JH, Park EC, Lee SG, Yoo KB. Associations between time in bed and suicidal thoughts, plans and attempts in Korean adolescents. BMJ Open. (2015) 5:e008766. doi: 10.1136/bmjopen-2015-008766
45. Sekine M, Tatsuse T, Cable N, Chandola T, Marmot M. U-shaped associations between time in bed and the physical and mental functioning of Japanese civil servants: the roles of work, family, behavioral and sleep quality characteristics. Sleep Med. (2014) 15:1122–31. doi: 10.1016/j.sleep.2014.04.012
Keywords: psychological stress, physical activity, preference, sports, sedentary, resiliency
Citation: Cao B, Zhao Y, Ren Z, McIntyre RS, Teopiz KM, Gao X and Ding L (2021) Are Physical Activities Associated With Perceived Stress? The Evidence From the China Health and Nutrition Survey. Front. Public Health 9:697484. doi: 10.3389/fpubh.2021.697484
Received: 19 April 2021; Accepted: 07 July 2021;
Published: 03 August 2021.
Edited by:
Yuka Kotozaki, Iwate Medical University, JapanReviewed by:
Noemi Tari-Keresztes, Charles Darwin University, AustraliaRicha Tripathi, All India Institute of Medical Sciences Gorakhpur, India
Copyright © 2021 Cao, Zhao, Ren, McIntyre, Teopiz, Gao and Ding. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ling Ding, ZGluZ2xpbmczMjFAeWVhaC5uZXQ=