 Simon Marmet
Simon Marmet Matthias Wicki
Matthias Wicki Gerhard Gmel
Gerhard Gmel Céline Gachoud1
Céline Gachoud1 Nicolas Bertholet
Nicolas Bertholet Joseph Studer
Joseph Studer- 1Addiction Medicine, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 2Addiction Switzerland, Lausanne, Switzerland
- 3Centre for Addiction and Mental Health, Toronto, ON, Canada
- 4Faculty of Health and Social Sciences, University of the West of England, Bristol, United Kingdom
Background: The COVID-19 pandemic and its countermeasures may have had a significant impact on the psychological well-being of specific population subgroups. The present study investigated whether sexual minority men (defined here as attracted partly or exclusively to men) from an ongoing cohort study of young Swiss men experienced different psychological impacts, levels of substance use and addictive behaviors, and to which degree pre-existing vulnerabilities and participants experiences during the crisis might explain these differences.
Methods: An ongoing cohort sample based on the general population of young Swiss men (mean age = 29.07 years; SD = 1.27) was assessed before and during the COVID-19 crisis for depression, stress, sleep quality, substance use and addictive behaviors. Additionally, during the crisis, we assessed its impact in form of fear, isolation and traumatic experiences. Potential associations between these outcomes and sexual orientation (sexual minority vs. heterosexual) were tested using linear regression models. It was additionally estimated to which degree these associations were attenuated if adjusted for differences in mental health, personality and socioeconomic status before the crisis, as well as the experience of the COVID-19 crisis (infection with the virus and changes to work situation).
Results: Compared to heterosexual men, sexual minority men showed higher levels of psychological trauma (b = 0.37 [0.25, 0.49]), fear (b = 0.18 [0.06, 0.30]) and isolation (b = 0.32 [0.20, 0.44]) due to the COVID-19 pandemic as well as higher levels of depression (b = 0.31 [0.20, 0.41]) and lower sleep quality (b = −0.13 [−0.24, −0.02]) during the crisis. These differences were to a large degree explained by higher pre-crisis levels of mental health problems and the personality dimension of neuroticism-anxiety. Sexual minority men showed higher overall levels of substance use and addictive behaviors, but these differences were already present before the crisis.
Conclusion: The COVID-19 crisis may have worsened pre-existing vulnerabilities in sexual minority men, leading to its greater psychological impact on them than on heterosexual men. Reducing minority stress due to sexual orientation may help not only to improve mental health among important proportions of the population but also to reduce their vulnerability to crises. Services offering psychological support to sexual minorities may need to be reinforced during crises.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) affected daily life worldwide, including in Switzerland. Although infection and potential infection with the virus had evident impacts on the population's physical health, other consequences could be observed in the form of the psychological stress due to fears for one's health and that of others, the measures taken against the spread of the coronavirus, and even the financial strains of economic uncertainty. Cases of COVID-19 started to increase in Switzerland at the beginning of March 2020, with 3,747 confirmed cases (43.9 cases per 100,000 inhabitants) reported by 16 March (1). The Swiss government took drastic measures to halt the spread of infection (hereafter: COVID measures), including closing schools, restaurants, non-essential shops, tourist attractions and others sites and introducing social/physical distancing (groups of up to 5 people and at least 2 m apart). There were also strong recommendations to work from home and avoid public transport.
Health crises often highlight and amplify pre-existing vulnerabilities (2–4), potentially also in individuals with a non-heterosexual sexual orientation, henceforth called sexual minorities here. The American Psychological Association defines sexual orientation as “…an enduring pattern of emotional, romantic and/or sexual attractions to men, women or both sexes. Sexual orientation also refers to a person's sense of identity based on those attractions, related behaviors and membership in a community of others who share those attractions.” (5) For the purpose of this study, sexual minority is defined as men which are partly or exclusively attracted to men. Being a member of a sexual minority is associated with minority stress (6–10), which Meyer (10) defines as the excess stress social minorities (in this case due to their sexual minority orientation) suffer due to effects such as stigmatization and prejudice. Stress due to sexual minority status can be categorized in four dimensions (10): external/objective stressors (such as stigma, prejudice or violence), expectation of such external stressors, internalization of negative societal attitudes and concealment of sexual orientation. Minority stress has been related to worse mental health (6, 10–15). Studies have also reported associations between personality traits and sexual orientation (16–18), and high scores for some personality traits, notably neuroticism, which have also been correlated with mental health problems (18). Despite the increased prevalence of mental health problems in sexual minorities, compared to heterosexual individuals, it is important to acknowledge that the majority of sexual minority individuals do not suffer from a mental health problem (13).
Consistent with this literature, previous research (14) on our cohort's sample also found that, compared to heterosexual men, sexual minority men reported worse mental health and overall higher levels of substance use disorders and behavioral addictions. Such pre-existing differences in mental health may predispose sexual minorities to worse reactions to a crisis such as COVID-19 (6, 19). Additionally, sexual minority status is often associated with differences in sociodemographic factors that may also contribute to a worse reaction to crises. For example, sexual minorities may have different housing situations, i.e., living less often with children and more often alone. Not having to care for children during such a crisis may be less stressful for some, but may also make them more prone to social isolation. Sexual minorities often have a lower socioeconomic status (20, 21) than heterosexual people, which could also relate to greater psychological impacts in a crisis (22).
Group solidarity and cohesiveness may provide resilience against negative consequences of minority stress (10), however, these resources may be less present due to the breakdown of usual social structures during the COVID-19 crisis. Conversely, the reduced number of social contacts during the COVID-19 crisis may reduce the occurrence of discriminatory experiences due to sexual orientation.
Overall, these factors may predispose sexual minorities to a worse reaction to the crisis (6, 8) and their existing higher addictive behaviors and substance use (14) may also be further exacerbated as a coping mechanism for COVID-19's psychological impact. Recent research has indicated that members of sexual minority groups have suffered a high psychological impact from the crisis (23–31), but these studies were done in samples of sexual minority people only and, therefore, that impact cannot be compared with the psychological impact suffered by the heterosexual people also affected by the crisis (32). Seven studies with online recruited convenience samples from the United States of America (9, 33–38) and one online study conducted in Portugal and Brazil (39) comparing sexual minorities and heterosexual persons found that the psychological impacts among members of sexual minorities were greater. A prospective cohort study in Southern California also found that sexual minorities reported more negative coping strategies with respect to the COVID-19 crisis compared to heterosexual individuals (40). A review of the literature regarding well-being of sexual and gender minorities in the United Kingdoms identified no research published in scientific journals, but several gray literature reports that overall showed poor or worse outcomes in sexual minorities (41).
Earlier publications have reported on the overall psychological impact of the COVID-19 crisis on our sample of young men, including changes in addictive behaviors and substance use (22, 42, 43). Overall, few participants tested positive for COVID-19, but there were considerable changes in work situations (job loss, partial unemployment, and working from home) due to the crisis and substantial psychological impacts (22, 42). Although there was a decrease in alcohol use, there was a marked increase in non-substance related addictive behaviors, such as gaming and watching TV series (43).
The present study focused on associations between sexual orientation and these outcomes. Specifically, the study's primary aim was to investigate whether sexual orientation could be associated with COVID-19's impacts (on mental well-being, substance use and addictive behaviors). A secondary aim was to better understand why sexual orientation was associated with these outcome variables and which parts of these associations could be accounted for by other covariates measured in our study. Therefore, as a first step, we tested whether sexual orientation was associated with: (a) experiences related to COVID-19; (b) sociodemographic factors; (c) indicators of mental health before the crisis; and (d) personality traits before the crisis. In a second step we also tested the degree to which these covariates accounted for the associations between sexual orientation and psychological impacts, substance use and addictive behaviors.
Method
Sample
This study was based on data from the Cohort Study on Substance-Use Risk Factors (C-SURF), collected from waves shortly before and during the COVID crisis. Participants were first contacted when they were about 19 years old, during the mandatory recruitment procedures testing their aptitude for military service. They were recruited at three of the six national military recruitment centers (in Lausanne, Windisch and Mels), which together cover 21 of Switzerland's 26 cantons. Subsequent data collection was independent of the army. The Human Research Ethics Committee of the Canton of Vaud approved the research protocols for the parent C-SURF study and the present COVID study (protocol 15/07 (PB_2018-00296). In total, 13,237 participants were invited to participate in the study, of which 7,556 participants gave their written informed consent and 5,987 replied to the first wave (see https://www.c-surf.ch/en/1.html and (44, 45) for more details about the parent study's design). There have been four waves of assessment to date (at roughly the ages of 20, 21, 25, and 28) with excellent follow up participation rates of about 90%. Between April 2019 and 14 February 2020 (1 month before the announcement of the COVID-19 measures, data collection of the 4th wave was still ongoing) 4,407 participants replied to C-SURF's fourth-wave, online questionnaire (hereafter: the pre-COVID wave). On 13 May 2020, these 4,407 participants were sent an e-mail and a short text message by telephone, inviting them to answer the COVID wave assessment. Data was collected online using LimeSurvey software (46), and collection ended on 8 June 2020. A total of 2,548 (57.8%) participants provided their informed consent to participate in the COVID assessment, and 2,415 (54.8% of those invited) filled out at least the first section about their experiences of COVID-19 symptoms and their personal situation. Participants with missing values for predictor variables were excluded from further analysis, and the study's final sample size was 2,345 (53.2% of those invited) participants.
Measurements
Sexual Orientation
One question on sexual orientation in the pre-COVID wave asked about the extent to which participants were attracted to men and women, with five response options ranging from exclusively attracted to women to exclusively attracted to men (47, 48). This was recoded to heterosexual (exclusively attracted to women) vs. sexual minority (at least somewhat attracted to men to exclusively attracted to men). Subgroup sample sizes were too small to meaningfully investigate differences across the spectrum of sexual minority orientations. Nevertheless, results for the five-option spectrum of sexual orientations are presented in the Supplementary Materials.
The Impact of the COVID-19 Pandemic (Outcome Variables)
Psychological Consequences, With No Mention of COVID-19 as Their Cause (Measured Before and During COVID-19)
These variables were investigated in the same format in both the pre-COVID and COVID-19 assessments, with COVID-19 not explicitly mentioned as a potential cause. Symptoms of major depression in the past 2 weeks were measured using the 12-item Major Depression Inventory (WHO–MDI) (49, 50), which was recoded into 10 criteria, resulting in a sum score ranging from 0 to 50. Cronbach's Alpha for the depression scale was 0.906 at the pre-COVID wave and 0.914 during COVID-19. Perceived stress in the last month was measured using the four-item short version of the Perceived Stress Scale (51), with response options from 0 (“never”) to 6 (“very often”), resulting in a sum score ranging from 0 to 24. Cronbach's Alpha for this scale was 0.659 at the pre-COVID and 0.656 during COVID. Sleep quality in the last month was assessed with one question from the Pittsburgh Sleep Quality Index (52), and response options from 0 (“very bad”) to 3 (“very good”).
Psychological Consequences, Explicitly Mentioning COVID-19 as Their Cause (Only Measured During COVID-19)
These variables explicitly mentioned the COVID-19 pandemic and its countermeasures as their cause, using formulations such as “due to the COVID-19 crisis, I experienced….” Psychological trauma due to the COVID-19 crisis in the last seven days was measured using the 22-item Impact of Event Scale (IES) (53). Response options were from 0 (“not at all”) to 4 (“extremely”), resulting in a sum score ranging from 0 to 88. Cronbach's Alpha for this scale was 0.919.
Fear due to the COVID-19 crisis, since the beginning of COVID measures, was asked about using seven items on the degree to which participants were afraid of the negative aspects of the COVID-19 crisis. Questions covered fears for oneself, others and finances, and were adapted from de Quervain et al. (54). Response options were from 0 (“not at all”) to 4 (“extremely”). Cronbach's Alpha for the fear scale was 0.731.
Feelings of isolation since the beginning of COVID-19 measures were asked about using three questions on how often participants felt isolated, adapted from UCLouvain (55). Response options were from 0 (“never”) to 3 (“very often”). Cronbach's Alpha for this scale was 0.773.
Substance Use and Other Addictive Behaviors (Measured Before and During COVID-19)
Weekly drinking volume and number of cigarettes smoked, weekly time spent gaming, watching TV series and watching internet pornography were computed as the product of quantity and frequency of use. One question asked about the frequency of illegal (≥1% THC) cannabis use. The same questions measuring addictive behaviors were used in the pre-COVID and COVID-19 assessments, however, the reference periods were different: i.e., “in the previous 12 months” for the pre-COVID assessment, and “since the start of the COVID-19 measures” for the COVID-19 assessment. All measures were recoded to express weekly use.
Covariates Hypothesized to Account for Associations Between Sexual Orientation and Psychological Impacts
Covariates From the COVID Assessment
Personal experiences of COVID-19 symptoms were assessed using one question (with responses “no symptoms,” “symptoms without having been tested,” “tested negative,” and “tested positive”), and participants were also asked whether other members of their household or entourage had experienced COVID-19 symptoms. Being part of the at-risk group for severe COVID-19 symptoms was assessed using one question asking whether participants suffered from any one of the following diseases: cancer, diabetes, immune system weakness, hypertension, cardiovascular disease or chronic respiratory disease. Changes in work situation due to the COVID-19 crisis were asked about using several questions on participants' employment status (with responses “no change,” “job loss,” “partial unemployment,” “losing money as self-employed”) and increases or decreases in workload. Hours worked from home and in total during the crisis were also assessed. The proportion of time worked from home (“1–49%,” “50–89%,” and “90–100%”) was calculated by dividing hours worked from home by total hours worked. Participants were asked whether they were called up to their military or civil protection unit to assist with the COVID-19 crisis and whether they regularly worked in contact with people potentially infected with the disease, either in medical settings (e.g., as nurses, doctors) or other settings (e.g., supermarkets). Furthermore, participants were asked about their living situation, i.e. whether they lived alone or together with other adults, as children are also people.
Covariates From the Pre-COVID Assessment
One question asked about the highest level of education attained by the participant, and answers were recoded into International Standard Classification of Education (ISCED) codes (56). Socioeconomic status (SES) was measured using two questions about relative financial status and difficulty paying bills. For relative financial status, participants were asked how well-off they considered themselves (adapted from Hibell et al. (57)) with respect to others, and answers were recoded to “below average,” “average,” and “above average.” Difficulty paying bills was measured using one question asking whether participants had sufficient income to pay their usual outgoings and bills at the end of the month, a question adapted from Swiss Federal Statistical Office (58). Answers were recoded to “easy or very easy,” “fairly easy,” and “rather difficult or difficult” to pay bills.
Symptoms of social anxiety disorder in recent weeks were measured using 12 five-point Likert scales for questions from the Clinically Useful Social Anxiety Disorder Outcome Scale (CUSADOS) (59). Cronbach's Alpha for this scale was 0.924. Attention-deficit hyperactivity disorder symptom severity in the last 12 months was measured using five-point Likert scales for six items from the Adult ADHD Self-Report Scale (ASRS–v1.1; (60)). Cronbach's Alpha for the ADHD scale was 0.720. Symptoms of borderline personality disorder (lifetime) were measured using true or false responses to 10 items from the McLean Screening Instrument for Borderline Personality Disorder (61, 62). Cronbach's Alpha for this scale was 0.783. Sensation-seeking was measured using the eight-item Brief Sensation Seeking Scale (63), with response options ranging from 0 (“strongly agree”) to 5 (“strongly disagree”), and the sum score ranging from 0 to 40. Cronbach's Alpha for this scale was 0.769. Aggression–hostility (Cronbach's Alpha = 0.609), neuroticism–anxiety (Cronbach's Alpha = 0.744, and sociability (Cronbach's Alpha = 0.686) were measured using 10 true or false statements from the Zuckermann–Kuhlmann Personality Questionnaire (64), and the response scores were summed.
Statistical Analysis
Descriptive statistics for COVID-related experiences and sociodemographic were calculated for the total sample, and separately for sexual minority and heterosexual men (Table 1). Differences in these COVID-related experiences and sociodemographic factors between sexual minority and heterosexual men were tested using multinomial logistic regression models, with heterosexual men as the reference group. Paired t-tests were used to test for differences in continuous measures for mental health and personality traits before the crisis according to sexual orientation (Supplementary Table S1).
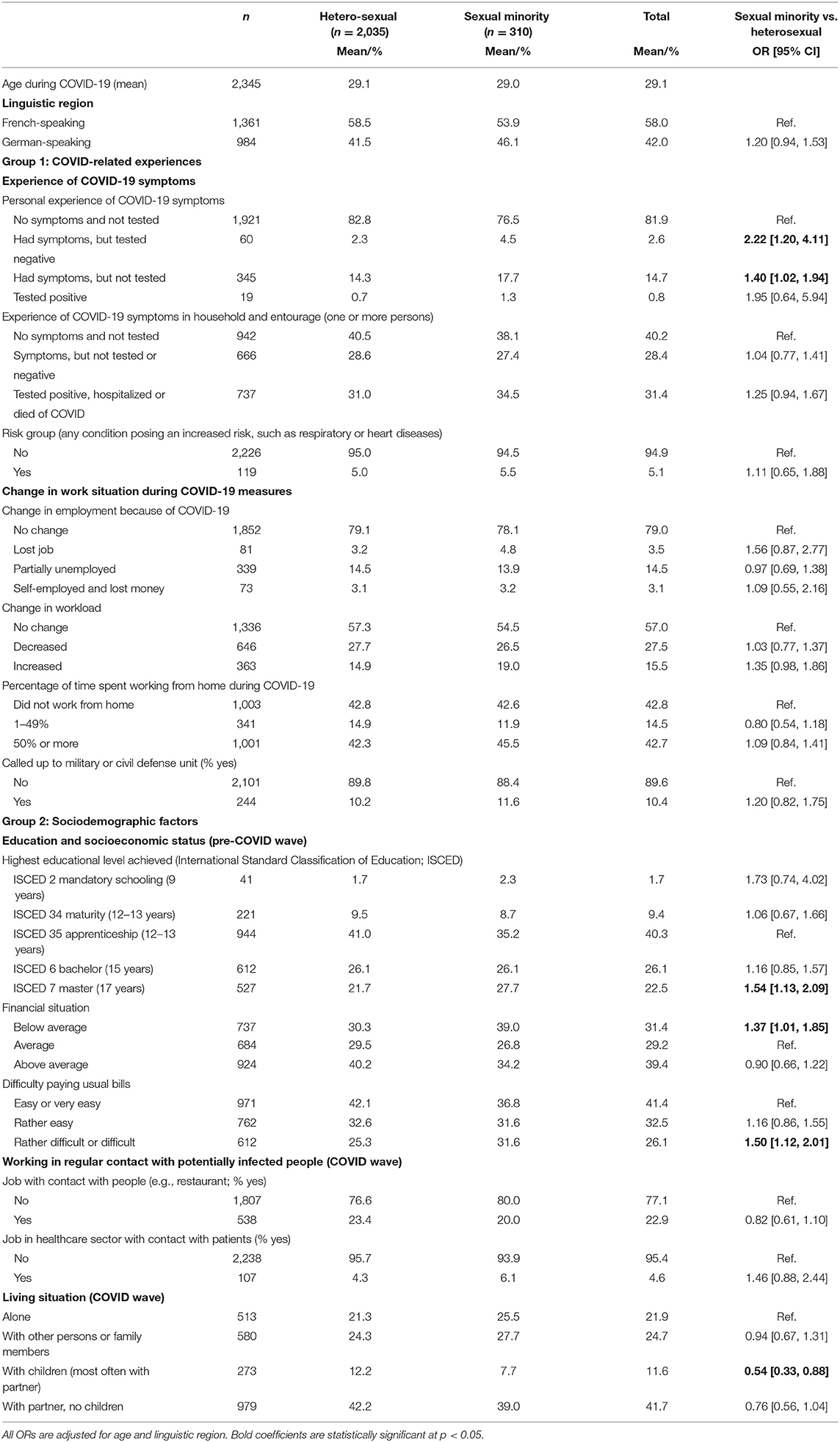
Table 1. Descriptive statistics and results of multinomial regressions testing for differences between sexual minority men and heterosexual men (reference group).
Linear regression models were used to test associations between psychological impacts and sexual orientation [coded as sexual minority (1) vs. heterosexual (0)]. Outcomes were z-standardized (mean = 0, SD = 1) before the analysis to enable better comparability of coefficients across outcomes. The coefficients thus corresponded to the differences in the outcomes, in standard deviations, for a one-unit increase in the predictor. All regressions were adjusted for participants' age and linguistic region (German-speaking vs. French-speaking). Models for depression, perceived stress and sleep quality, as well as for addictive behaviors and substance use, were also adjusted for their baseline levels in the pre-COVID wave in order to estimate to which degree differences by sexual orientation were already present before the crisis. The results present unadjusted and baseline adjusted coefficients.
For the last part of the analysis, covariates were categorized into four groups: (1) COVID-related experiences, (2) sociodemographic factors, (3) mental health problems, and (4) personality. To test the degree to which sexual orientation related differences in psychological impacts, addictive behaviors and substance use between sexual minority men and heterosexual men were reduced after accounting for these covariates, the coefficients for sexual orientation with respect to an outcome (e.g., fear or depression) were divided by their respective coefficient for sexual orientation, adjusted for the respective covariate. This analysis, and tests for the significance of the attenuation, were done using the KHB plugin (65) in Stata 14 software (66). A percentage of attenuation [1–(coefficient adjusted for covariate/unadjusted coefficient)] was then estimated. The higher this percentage, the greater part of sexual orientation's association with the outcome can be explained by differences in the respective covariate. This procedure is very similar to estimating the proportion of the indirect effect of the total effect in mediation analysis. Attenuation was first estimated for each covariate separately, then for the total of each of the four groups, and finally for all four groups combined. For each group, the remaining coefficients for sexual minority orientation after adjustment for the respective group of covariates were also reported. A non-significant coefficient means that there was no significant effect of sexual minority orientation that cannot be explained by the covariates. A remaining significant effect means that there is an independent effect of sexual minority orientation with respect to an outcome that cannot be explained by the covariates in the model.
Results
Overall, 13.2% (n = 310) of our sample of young Swiss men identified as a member of a sexual minority. Further descriptive statistics of the sample are presented in Table 1.
Associations With Psychological Impact and Addictive Behaviors (Aim 1)
Descriptive statistics for psychological impact and addictive behaviors according to sexual orientation are presented in Table 2, while associations of between sexual minority with psychological impact are reported in Table 3. Sexual minority men reported a greater psychological impact in consequences mentioning COVID-19 as a cause (psychological trauma, fear, and isolation). They also felt a greater psychological impact in consequences not mentioning COVID-19 as a cause, however, after adjustment for baseline levels, this was no longer significant for perceived stress, whereas coefficients for depression and sleep quality were lower but remained significant. For depression, there was actually an absolute decrease in scores in sexual minority men and heterosexual men (Table 2), however, sexual minority men had higher scores before and during the crisis, and they decreased less compared to heterosexual men, resulting in a significant positive coefficient before and after baseline adjustment.
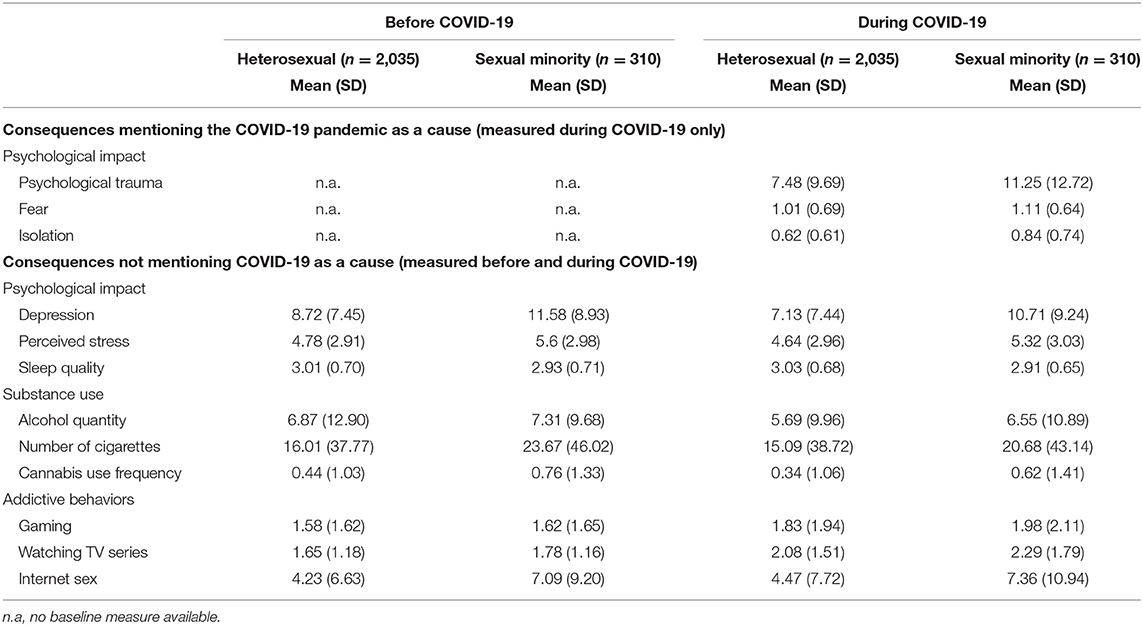
Table 2. Psychological impact, substance use and addictive behaviors according to sexual orientation.
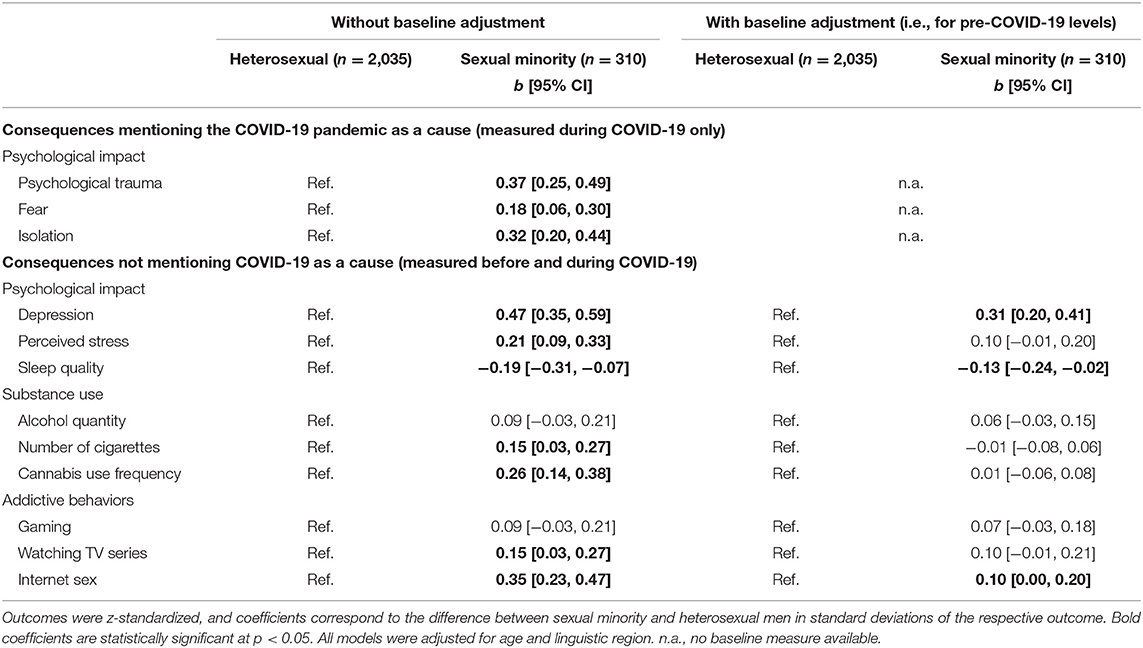
Table 3. Sexual orientation [sexual minority vs. heterosexual (ref.)] as a predictor of the crisis' psychological impact and its impact on substance use and addictive behaviors.
Regarding substance use and addictive behaviors, sexual minority men showed significantly higher levels of cigarette and cannabis use, of watching TV series and of internet sex during the COVID-19 crisis. Alcohol use and gaming were also higher among sexual minority men, but not significantly. After baseline adjustment, only the coefficient for internet sex remained significantly higher (Table 3). The analysis for psychological impact and substance use was repeated for the five-level spectrum of sexual orientation, and results are presented in Supplementary Table S2.
Attenuation of Coefficients by Covariates (Aim 2)
Table 1 reports differences in covariates according to sexual orientation.
For outcomes with a significant association (as presented in Table 3) with sexual orientation, Table 4 shows the degree to which coefficients for sexual orientation were attenuated after adjusting for these covariates (as presented in Table 1) and, thus, the proportion of the total effect of sexual orientation on outcomes explained by the association with the covariate. The covariates from all four groups taken together explained more than half of the association between sexual orientation and sleep quality (66.0%), fear (67.8%) and feelings of isolation (57.5%), about a third of the association with major depression (37.2%) but only 14.4% of the association with internet sex. The greatest attenuations in psychological impacts were observed by mental health problems (group 3) in the pre-COVID wave and personality traits (group 4) in the pre-COVID wave, although the only dimension of personality with a significant attenuation was neuroticism-anxiety. In comparison, attenuation due to sociodemographic factors (group 2) was lower and mostly related to differences in SES (especially for fear and to a lesser degree for psychological trauma) and living situation (especially for internet sex and isolation). COVID-related experiences (group 1) were the group of variables with the lowest potential for explaining associations between sexual orientation and psychological impacts, and only personal experiences of COVID-19 symptoms were associated with a significant attenuation for fear.
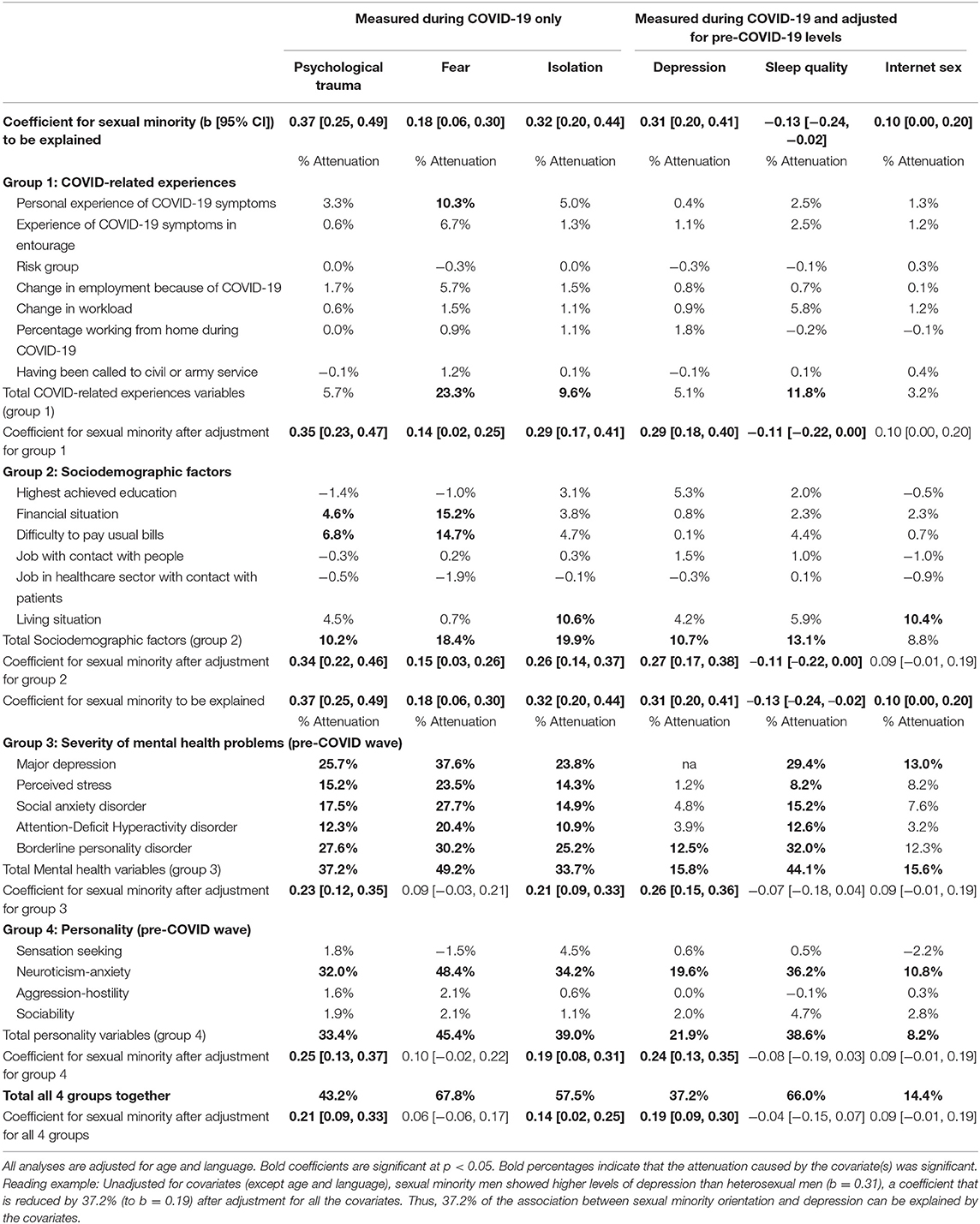
Table 4. Percentage of attenuation/reduction in the coefficients of outcomes with significant associations with sexual minority orientation, after adjustment for COVID-related experiences, sociodemographic factors, mental health and personality.
Discussion
The present study's main objective was to investigate whether sexual minority men (partly or exclusively attracted to men) experienced a higher psychological impact and showed disproportional changes in substance use and addictive behaviors during the COVID-19 crisis compared to heterosexual men. As had been hypothesized early on in the crisis (6, 8), our results show that the COVID-19 crisis had a greater psychological impact on sexual minority men compared to heterosexual men, in form of higher levels of psychological trauma, fear and isolation. Regarding depression, stress and sleep quality measured before and during the crisis, sexual minority men showed higher levels during the crisis compared to heterosexual men, which remained significant after baseline adjustment for depression and sleep quality, meaning that the gap in these measures between sexual minority men and heterosexual men increased during the crisis, even if there was no absolute increase (and even a decrease for depression) in these measures early in the crisis (42). Earlier research had reported the high impact of the COVID-19 crisis on sexual minority men (23–26, 28), but also on the general population (32), it was therefore important to test whether sexual minority men were indeed more affected than heterosexual men. Only relatively few studies mostly based on online convenience samples from the United States of America (9, 33–39), had reported a higher psychological impact of the COVID-19 crisis among sexual minorities compared to heterosexual people. Thus, the present study is certainly among the first to provide evidence that sexual minority men felt a greater impact from the COVID-19 crisis than did heterosexual men, and it was based on a general population sample rather than a convenience sample, and is one of the first published studies outside the United States of America to the best of our knowledge.
Regarding substance use and addictive behaviors, it would appear that the higher levels of substance use and addictive behaviors present among sexual minority men before the crisis compared to heterosexual men (14) remained present during it, and there was no overall indication of any disproportionate change in their substance use and addictive behaviors during the early crisis. Nevertheless, the higher levels of addictive behaviors in sexual minority men remain a reason for concern, before, during and probably after the pandemic. Further research will be needed to investigate whether this situation holds true for the duration of the crisis or whether there will be a disproportional change in addictive behaviors among sexual minorities at some point during it.
Besides the psychological impact they felt, sexual minority men differed from heterosexual men on several factors before and during the crisis. They were significantly more likely to have had symptoms of COVID-19 than heterosexual men, which was consistent with earlier findings from the United States of America (9). They were also slightly more likely to have lost their jobs during the crisis (also consistent with (9)). However, differences in variables measured before the crisis were considerable and consistent with the literature (18, 21, 67): sexual minority men had a lower SES, poorer mental health and a personality profile high in neuroticism-anxiety. These differences before and during the crisis may have contributed to the greater psychological impact of the COVID-19 crisis among sexual minority men, and we tested the degree to which this was the case in our sample. Results showed that when all the covariates were taken together, they explained more than half of the association between sexual orientation and sleep quality (66.0%), fear (67.8%) and feelings of isolation (57.5%), about a third of its association with major depression (37.2%), but only 14.4% of its association with internet sex use during COVID-19. Looking at which variables had the biggest influence on these attenuations, the first key finding was that a substantial part of the association between sexual orientation and the psychological impact of the COVID-19 crisis could be explained by higher levels of mental health problems among sexual minority men before the crisis, which predisposed them to a worse reaction during the crisis (6–8). Second, higher levels of the neuroticism-anxiety personality trait among sexual minority men explained a significant proportion of the association between sexual orientation and the psychological impacts of the crisis, especially for fear. Persons with high levels of neuroticism-anxiety may worry more in general, be more anxious and show a worse reaction to stressors (68), especially during crises like COVID-19 (69). Third, consistent with earlier findings that lower SES was associated with a greater psychological impact from the COVID-19 crisis (22), sexual minority men's lower perceived SES partially explained why they experienced more fear (possible financial worries) and psychological trauma due to COVID-19, but explained relatively little of the differences in the psychological impact for the other outcomes. Fourth, differences in COVID-19-related changes explained relatively little of the association between sexual orientation and the psychological impact of the crisis. Thus, the greater psychological impact of the COVID-19 crisis among sexual minority men was not mainly because they experienced more COVID-19 symptoms or changes in their work situation due to the crisis, but was because of pre-existing differences, primarily in form of lower mental health and higher levels of neuroticism-anxiety, which predisposed them to a worse reaction to the crisis.
Consequently, a large part of the crisis' greater psychological impact on sexual minority men may be explained by the greater vulnerabilities due to minority stress (10, 11), in the form of worse mental health (6, 12, 13) and higher levels of the neuroticism-anxiety personality trait before the COVID-19 crisis (18). Differences in socioeconomic factors (lower SES) (21) and living situation (less often living with children, tendency to live more often alone) also played a role in our sample, but with a comparatively small effect, possibly because not living with children may not only be associated with loneliness, but also be less stressful due to fewer social role obligations. Taken together, our broad range of covariates was able to explain a considerable part (but not all) of why sexual minority men felt a greater psychological impact, and it would appear that these factors surpass any possible beneficial effects of the crisis due to being exposed less to discriminatory experiences as a result of fewer social contacts. Further explanations for the remaining association could be more frequent interfamilial conflicts experienced by sexual minority men and thus less supportive social networks during a crisis (6, 9, 70). They may suffer more from social isolation as a larger part of their social peer network is no longer accessible (8, 21), which may also be an important resource for copying with minority stress (10). However, further research, perhaps using a qualitative approach, would be needed to test such hypotheses. Overall, a combination of factors seems to have created an overall worse reaction to the COVID-19 crisis among the sexual minority men who have less resources for coping with it (15).
Limitations
Our sample consisted exclusively of young Swiss men, but they may very well generalize (although with the required caution) to sexual minorities of other age groups and women, who are similarly affected by minority stress. All the measurement data were self-reported, and measures of mental health cannot reach the accuracy of a clinical assessment by this means. The pre-COVID-19 assessment was spread across 9 months, whereas the COVID-19 assessment was spread across 4 weeks, so there were significant differences in the periods covered by the assessments. In addition, the crisis situation was constantly and rapidly evolving: participants who completed the questionnaire at the end of the evaluation period may have experienced the pandemic very differently to those who completed the questionnaire early on. However, this should not have systematically affected our results. Only one aspect of sexual orientation (sexual attraction) was measured which yields rather higher estimates for non-heterosexual orientation compared to measures of sexual identity (identifying as homosexual or bisexual) (48, 71). Nevertheless, the subgroup sample sizes for non-heterosexual orientations (homosexual and bisexual) were too small to test for differences between them, we were unable to consider the entire spectrum of sexual orientations. However, supplementary analyses showed that there were some differences across the spectrum of sexual minority orientations (e.g., between “mostly heterosexual,” and “mostly homosexual” men), albeit not systematically in one direction. This may deserve further attention in future studies with larger sample sizes. Finally, our COVID study was conducted relatively early on in the pandemic; thus, its long-term psychological consequences could not be assessed.
Conclusion
Sexual minority men reported experiencing a greater psychological impact due to the COVID-19 crisis than did heterosexual men. The crisis revealed or amplified pre-existing vulnerabilities in sexual minority men. A substantial proportion of these greater psychological impacts was due to sexual minority men's lower overall mental health status before the crisis, thus, preventing and treating mental health problems, especially in sexual minority men, may improve resilience to the psychological impacts of the current COVID-19 crisis and future crises. Psychological interventions may need to be adapted to personality profiles high in neuroticism-anxiety (72). Services offering psychological support or counseling to sexual minorities may need to be reinforced during crises such as the COVID-19 pandemic. Mitigating minority stress by reducing social or internalized stressors, for example improved sex education in school, abolishing discriminating laws (e.g., by recognizing same-sex unions), and by bolstering sexual minorities' stress coping resources (23, 73–78) may help to improve mental health among important proportions of the population and also to reduce their vulnerability to crises. The present study analyzed differences in the short-term consequences of the COVID-19 crisis. The significant unanswered question remains whether the greater psychological impact of the crisis among sexual minority men will persist for a longer time, or even whether it will be further amplified as the COVID-19 crisis runs its yet unknown course.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Human Research Ethics Committee of the Canton of Vaud. The participants provided their written informed consent to participate in this study.
Author Contributions
SM contributed to the questionnaire design, conducted the data analysis and wrote the initial draft of the manuscript. MW, GG, CG, JS, and NB contributed to the questionnaire design, interpretation of the results and the writing of the manuscript. JS and GG were responsible for the development of the questionnaire and the data collection. All authors approved the final version of the manuscript.
Funding
The C-SURF study was funded by the Swiss National Science Foundation (FN 33CSC0-122679, FN 33CS30_139467, FN 33CS30_148493, and FN 33CS30_177519).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.692884/full#supplementary-material
References
1. Federal Office of Public Health. COVID-19 in der Schweiz [COVID-19 in Switzerland]. (2020). Available online at: https://covid-19-schweiz.bagapps.ch/de-2.html
2. Kantamneni N. The impact of the COVID-19 pandemic on marginalized populations in the United States: a research agenda. J Vocat Behav. (2020) 119:103439. doi: 10.1016/j.jvb.2020.103439
3. Bambra C, Riordan R, Ford J, Matthews F. The COVID-19 pandemic and health inequalities. J Epidemiol Community Health. (2020) 74:964–8. doi: 10.1136/jech-2020-214401
4. Anderson G, Frank JW, Naylor CD, Wodchis W, Feng P. Using socioeconomics to counter health disparities arising from the covid-19 pandemic. BMJ. (2020) 369:m2149. doi: 10.1136/bmj.m2149
5. American Psychological Association. Sexual Orientation & Homosexuality. (2008). Available online at: https://www.apa.org/topics/lgbtq/orientation
6. Salerno JP, Williams ND, Gattamorta KA. LGBTQ populations: psychologically vulnerable communities in the COVID-19 pandemic. Psychol Trauma: Theor Res Pract Policy. (2020) 12:S239. doi: 10.1037/tra0000837
7. Banerjee D, Nair VS. “The Untold Side of COVID-19”: struggle and perspectives of the sexual minorities. J Psychosexual Health. (2020) 2:113–20. doi: 10.1177/2631831820939017
8. Brennan DJ, Card KG, Collict D, Jollimore J, Lachowsky NJ. How might social distancing impact gay, bisexual, queer, trans and two-spirit men in Canada? AIDS Behav. (2020) 24:2480–2. doi: 10.1007/s10461-020-02891-5
9. Moore SE, Wierenga KL, Prince DM, Gillani B, Mintz LJ. Disproportionate impact of the COVID-19 pandemic on perceived social support, mental health and somatic symptoms in sexual and gender minority populations. J Homosex. (2021) 86:1–15. doi: 10.1080/00918369.2020.1868184
10. Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. (2003) 129:674. doi: 10.1037/0033-2909.129.5.674
12. Bromberg DJ, Paltiel AD, Busch SH, Pachankis JE. Has depression surpassed HIV as a burden to gay and bisexual men's health in the United States? A comparative modeling study. Social Psychiatry Psychiatric Epidemiol. (2020) 56:1–10. doi: 10.2139/ssrn.3439575
13. Plöderl M, Tremblay P. Mental health of sexual minorities. Syst Rev Int Rev Psychiatry. (2015) 27:367–85. doi: 10.3109/09540261.2015.1083949
14. Wicki M, Marmet S, Studer J, Epaulard O, Gmel G. Curvilinear associations between sexual orientation and problematic substance use, behavioural addictions and mental health among young Swiss men. Addictive Behav. (2020) 112:106609. doi: 10.1016/j.addbeh.2020.106609
15. Slimowicz J, Siev J, Brochu PM. Impact of status-based rejection sensitivity on depression and anxiety symptoms in gay men. Int J Environ Res Public Health. (2020) 17:1546. doi: 10.3390/ijerph17051546
16. Wang J, Dey M, Soldati L, Weiss M, Gmel G, Mohler-Kuo M. Psychiatric disorders, suicidality, and personality among young men by sexual orientation. European Psychiatry. (2014) 29:514–22. doi: 10.1016/j.eurpsy.2014.05.001
17. Allen MS, Robson DA. Personality and sexual orientation: new data and meta-analysis. J Sex Res. (2020) 57:953–65.
18. Zietsch BP, Verweij KJ, Bailey JM, Wright MJ, Martin NG. Sexual orientation and psychiatric vulnerability: A twin study of neuroticism and psychoticism. Arch Sex Behav. (2011) 40:133–42. doi: 10.1007/s10508-009-9508-4
19. Asmundson GJ, Paluszek MM, Landry CA, Rachor GS, McKay D, Taylor S. Do pre-existing anxiety-related and mood disorders differentially impact COVID-19 stress responses and coping? J Anxiety Disord. (2020) 74:102271. doi: 10.1016/j.janxdis.2020.102271
20. Konnoth C. Supporting LGBT communities in the COVID-19 Pandemic. In: Assessing Legal Responses to COVID-19. (2020). Boston: Public Health Law Watch. doi: 10.2139/ssrn.3675915
21. OutRight Action International. Vulnerability Amplified: The Impact of the COVID-19 Pandemic on LGBTIQ People. New York: OutRight Action International (2020).
22. Marmet S, Wicki M, Gmel G, Gachoud C, Daeppen J-B, Bertholet N, et al. The psychological impact of the COVID-19 crisis is higher among young Swiss men with a lower socioeconomic status: evidence from a cohort study. Plos one. (2021) 16:e0255050. doi: 10.1371/journal.pone.0255050
23. Millar BM, Adebayo T, Dellucci TV, Behar E, Starks TJ. Keeps me awake at night: the potential of the COVID-19 pandemic to affect sleep quality among sexual minority men in the USA. Psychol Sex Orientation Gender Diversity. (2021) 8:213–219. doi: 10.1037/sgd0000441
24. Gonzales G, de Mola EL, Gavulic KA, McKay T, Purcell C. Mental health needs among lesbian, gay, bisexual, and transgender college students during the COVID-19 pandemic. J Adolescent Health. (2020) 67:645–8. doi: 10.1016/j.jadohealth.2020.08.006
25. Kneale D, Becares L. Discrimination as a predictor of poor mental health among LGBTQ+ people during the COVID-19 pandemic: cross-sectional analysis of the online Queerantine study. BMJ Open. (2021) 11:e049405. doi: 10.1136/bmjopen-2021-049405
26. Santos G-M, Ackerman B, Rao A, Wallach S, Ayala G, Lamontage E, et al. Economic, mental health, HIV prevention and HIV treatment impacts of COVID-19 and the COVID-19 response on a global sample of cisgender gay men and other men who have sex with men. AIDS Behav. (2021) 25:311–21. doi: 10.21203/rs.3.rs-33958/v1
27. Gato J, Barrientos J, Tasker F, Miscioscia M, Cerqueira-Santos E, Malmquist A, et al. Psychosocial effects of the COVID-19 pandemic and mental health among LGBTQ+ young adults: a cross-cultural comparison across six nations. J Homosex. (2021) 68:612–30. doi: 10.1080/00918369.2020.1868186
28. Suen YT, Chan RC. Wong EMYJPr. Effects of general and sexual minority-specific COVID-19-related stressors on the mental health of lesbian, gay, and bisexual people in Hong Kong. Psychiatry Res. (2020) 292:113365. doi: 10.1016/j.psychres.2020.113365
29. Chang CJ, Feinstein BA, Chu BC. Selby EAJPoSO, Diversity G. The negative impact of COVID-19 on sexual minority young adults: demographic differences and prospective associations with depression. Psychol Sex Orientation Gender Divers. (2021) 8:220. doi: 10.1037/sgd0000494
30. Nelson KM, Gordon AR, John SA, Stout CD. Macapagal KJJoAH. “Physical Sex Is Over for Now”: impact of COVID-19 on the well-being and sexual health of adolescent sexual minority males in the US. J Adolescent Health. (2020) 67:756–62. doi: 10.1016/j.jadohealth.2020.08.027
31. MacCarthy S, Izenberg M, Barreras JL, Brooks RA, Gonzalez A. Linnemayr SJPO. Rapid mixed-methods assessment of COVID-19 impact on Latinx sexual minority men and Latinx transgender women. PLoS ONE. (2020) 15:e0244421. doi: 10.1371/journal.pone.0244421
32. Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. (2020) 16:1–11. doi: 10.1186/s12992-020-00589-w
33. Peterson ZD, Vaughan EL, Carver DN. Sexual identity and psychological reactions to COVID-19. Traumatology. (2021) 27:6–13. doi: 10.1037/trm0000283
34. Hoyt LT, Cohen AK, Dull B, Castro EM, Yazdani N. “Constant stress has become the new normal”: stress and anxiety inequalities among US college students in the time of COVID-19. J Adolesc Health. (2021) 68:270–276. doi: 10.1016/j.jadohealth.2020.10.030
35. Kamal K, Li JJ, Hahm HC. Liu CH. Psychiatric impacts of the COVID-19 global pandemic on US sexual and gender minority young adults. Psychiatry Res. (2021) 299:113855. doi: 10.1016/j.psychres.2021.113855
36. Fish JN, Salerno J, Williams ND, Rinderknecht RG, Drotning KJ, Sayer L, et al. Sexual minority disparities in health and well-being as a consequence of the COVID-19 pandemic differ by sexual identity. LGBT Health. (2021) 8. doi: 10.1089/lgbt.2020.0489
37. Rodriguez-Seijas C, Fields EC, Bottary R, Kark SM, Goldstein MR, Kensinger EA. et al. Comparing the impact of CoViD-19-related social distancing on mood and psychiatric indicators in sexual and gender minority (SGM) and non-SGM individuals. Front Psychiatry. (2020) 11:1448. doi: 10.3389/fpsyt.2020.590318
38. Solomon DT, Morey KE, Williams CJ, Grist CL, Malesky LA. COVID-19 health behaviors in a sexual minority sample: the impact of internalized stigma. Psychol Sexual Orientation Gender Div. (2021) 8:159–171. doi: 10.1037/sgd0000466
39. Duarte M. Pereira HJBS. The impact of COVID-19 on depressive symptoms through the lens of sexual orientation. Brain Sci. (2021) 11:523. doi: 10.3390/brainsci11040523
40. Krueger EA, Barrington-Trimis JL, Unger JB, Leventhal AM. Sexual and gender minority young adult coping disparities during the COVID-19 pandemic. (2021). J Adolescent Health. doi: 10.1016/j.jadohealth.2021.07.021
41. McGowan VJ, Lowther HJ. Meads C. Life under COVID-19 for LGBT+ people in the UK: systematic review of UK research on the impact of COVID-19 on sexual and gender minority populations. BMJ Open. (2021) 11:e050092. doi: 10.1136/bmjopen-2021-050092
42. Marmet S, Wicki M, Gmel G, Gachoud C, Daeppen J-B, Bertholet N, et al. The psychological impact of the COVID-19 crisis on young Swiss men participating in a cohort study. Swiss Med Wkly. (2021) 151:w30028. doi: 10.31234/osf.io/kwxhd
43. Studer J, Marmet S, Gmel G, Wicki M, Labhart F, Gachoud C, et al. Changes in substance use and other reinforcing behaviours during the COVID-19 crisis in a general population cohort study of young Swiss men. J. Behav. Addict. (accepted). doi: 10.1556/2006.2021.00073
44. Studer J, Baggio S, Mohler-Kuo M, Dermota P, Gaume J, Bertholet N, et al. Examining non-response bias in substance use research—are late respondents proxies for non-respondents? Drug Alcohol Depend. (2013) 132:316–23. doi: 10.1016/j.drugalcdep.2013.02.029
45. Gmel G, Akre C, Astudillo M, Bähler C, Baggio S, Bertholet N, et al. The swiss cohort study on substance use risk factors—findings of two waves. SUCHT. (2015) 61:251–62. doi: 10.1024/0939-5911.a000380
46. Limesurvey GmbH. LimeSurvey: An Open Source Survey Tool. (2020). Available online at: http://www.limesurvey.org. (retrieved March 18, 2020).
47. Bailey JM, Vasey PL, Diamond LM, Breedlove SM, Vilain E, Epprecht M. Sexual orientation, controversy, and science. Psychol Sci Publ Interest. (2016) 17:45–101. doi: 10.1177/1529100616637616
48. Patterson JG, Jabson JM, Bowen DJ. Measuring sexual and gender minority populations in health surveillance. LGBT health. (2017) 4:82–105. doi: 10.1089/lgbt.2016.0026
49. Bech P, Rasmussen NA, Olsen LR, Noerholm V, Abildgaard W. The sensitivity and specificity of the major depression inventory, using the present state examination as the index of diagnostic validity. J Affect Disord. (2001) 66:159–64. doi: 10.1016/S0165-0327(00)00309-8
50. Bech P, Timmerby N, Martiny K, Lunde M, Soendergaard S. Psychometric evaluation of the Major Depression Inventory (MDI) as depression severity scale using the LEAD (Longitudinal Expert Assessment of All Data) as index of validity. BMC Psychiatry. (2015) 15:190. doi: 10.1186/s12888-015-0529-3
51. Cohen S, Williamson GM. Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S, editors. The Social Psychology of Health Newbury Park. CA: Sage. (1988) pp. 31–67.
52. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
53. Weiss DS. The impact of event scale: revised. In: Cross-Cultural Assessment of Psychological Trauma and PTSD. (2007). New York: Springer. p. 219–38. doi: 10.1007/978-0-387-70990-1_10
54. de Quervain D, Aerni A, Amini E, Bentz D, Coynel D, Gerhards C, et al. The Swiss corona stress study. (2020). doi: 10.31219/osf.io/jqw6a. [Epub ahead of print].
55. UCLouvain. COVID-19 Research in IPSY. (2020). Available online at: https://uclouvain.be/fr/instituts-recherche/ipsy/recherches-covid-19-en-ipsy.html
56. Swiss Federal Statistical Office. Bildungsstatistik 2019. (2020). Neuchatel, Switzerland: Bundesamt für Statistik.
57. Hibell B, Guttormsson U, Ahlström S, Balakireva O, Bjarnason T, Kokkevi A, et al. The 2011 ESPAD Report. Substance Use Among Students in 36 European Countries. Tukholma: The Swedish Council for Information on Alcohol and other Drugs (2012).
58. Federal Statistical Office. Statistics on Income and Living Conditions: household questionnaire 2019. Available online at: https://www.bfs.admin.ch/bfs/en/home/statistics/economic-social-situation-population/surveys/silc.html.
59. Dalrymple K, Martinez J, Tepe E, Young D, Chelminski I, Morgan T, et al. A clinically useful social anxiety disorder outcome scale. Compr Psychiatry. (2013) 54:758–65. doi: 10.1016/j.comppsych.2013.02.006
60. Kessler RC, Adler L, Ames M, Demler O, Faraone S, Hiripi E, et al. The World Health Organization adult ADHD self-report scale (ASRS): a short screening scale for use in the general population. Psychol Med. (2005) 35:245–56. doi: 10.1017/S0033291704002892
61. Melartin T, Häkkinen M, Koivisto M, Suominen K, Isometsä E. Screening of psychiatric outpatients for borderline personality disorder with the McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD). Nord J Psychiatry. (2009) 63:475–9. doi: 10.3109/08039480903062968
62. Zanarini MC, Vujanovic AA, Parachini EA, Boulanger JL, Frankenburg FR, Hennen J, et al. Screening measure for BPD: the mclean screening instrument for borderline personality disorder (MSI-BPD). J Pers Disord. (2003) 17:568–73. doi: 10.1521/pedi.17.6.568.25355
63. Hoyle RH, Stephenson MT, Palmgreen P, Lorch EP, Donohew RL. Reliability and validity of a brief measure of sensation seeking. Pers Individ Dif. (2002) 32:401–14. doi: 10.1016/S0191-8869(01)00032-0
64. Aluja A, Garcia Ó, Garcia LF. A comparative study of Zuckerman's three structural models for personality through the NEO-PI-R, ZKPQ-III-R, EPQ-RS and Goldberg's 50-bipolar adjectives. Pers Individ Dif. (2002) 33:713–25. doi: 10.1016/S0191-8869(01)00186-6
65. Karlson KB, Holm A. Decomposing primary and secondary effects: a new decomposition method. Res Soc Stratif Mobil. (2011) 29:221–37. doi: 10.1016/j.rssm.2010.12.005
67. Herek GM, Garnets LD. Sexual orientation and mental health. Annu Rev Clin Psychol. (2007) 3:353–75. doi: 10.1146/annurev.clinpsy.3.022806.091510
68. Schneider TR, Rench TA, Lyons JB, Riffle RR. The influence of neuroticism, extraversion and openness on stress responses. Stress Health. (2012) 28:102–10. doi: 10.1002/smi.1409
69. Modersitzki N, Phan LV, Kuper N, Rauthmann JF. Who is impacted? Personality predicts individual differences in psychological consequences of the COVID-19 pandemic in Germany. Social Psychol Pers Sci. (2021) 12:1110–1130. doi: 10.1177/1948550620952576
70. Rosa WE, Shook A, Acquaviva KD. LGBTQ+ inclusive palliative care in the context of COVID-19: pragmatic recommendations for clinicians. J Pain Symptom Manage. (2020) 60:e44–47. doi: 10.1016/j.jpainsymman.2020.04.155
71. Copen CE, Chandra A, Febo-Vazquez I. Sexual Behavior, Sexual Attraction, and Sexual Orientation Among Adults Aged 18-44 in the United States: Data from the 2011-2003 National Survey of Family Growth. Natl Health Stat Report. (2016) 7:1–14.
72. Miller TR. The psychotherapeutic utility of the five-factor model of personality: a clinician's experience. J Pers Assess. (1991) 57:415–33. doi: 10.1207/s15327752jpa5703_3
73. Chaudoir SR, Wang K, Pachankis JE. What reduces sexual minority stress? A review of the intervention “toolkit”. J Social Issues. (2017) 73:586–617. doi: 10.1111/josi.12233
74. Gesundheitsförderung Schweiz. Geschlechtliche und sexuelle Minderheiten in Gesundheitsförderung und Prävention. Faktenblatt. Gesundheitsförderung Schweiz. (2017). 19.
75. Williams SL, Mann AK. Sexual and gender minority health disparities as a social issue: how stigma and intergroup relations can explain and reduce health disparities. J Social Issues. (2017) 73:450–61. doi: 10.1111/josi.12225
76. Coulter RW, Egan JE, Kinsky S, Friedman MR, Eckstrand KL, Frankeberger J, et al. Mental health, drug, and violence interventions for sexual/gender minorities: a systematic review. Pediatrics. (2019) 144:e20183367. doi: 10.1542/peds.2018-3367
77. Drabble LA, Wootton AR, Veldhuis CB, Riggle ED, Rostosky SS, Lannutti PJ, et al. Perceived psychosocial impacts of legalized same-sex marriage: a scoping review of sexual minority adults' experiences. PLoS ONE. (2021) 16:e0249125. doi: 10.1371/journal.pone.0249125
Keywords: COVID-19, Switzerland, mental health, sexual orientation, sexual minorities
Citation: Marmet S, Wicki M, Gmel G, Gachoud C, Bertholet N and Studer J (2021) Sexual Minority Orientation Is Associated With Greater Psychological Impact Due to the COVID-19 Crisis—Evidence From a Longitudinal Cohort Study of Young Swiss Men. Front. Public Health 9:692884. doi: 10.3389/fpubh.2021.692884
Received: 09 April 2021; Accepted: 24 September 2021;
Published: 22 October 2021.
Edited by:
Susan Garthus-Niegel, Medical School Hamburg, GermanyReviewed by:
Andreas Staudt, Technische Universität Dresden, GermanyMaria Manuela Peixoto, Lusíada University of Porto, Portugal
Copyright © 2021 Marmet, Wicki, Gmel, Gachoud, Bertholet and Studer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Simon Marmet, c2ltb24ubWFybWV0QGNodXYuY2g=