 Huanhuan Huang
Huanhuan Huang Zhiyu Chen
Zhiyu Chen Songmei Cao1,2
Songmei Cao1,2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 17 September 2021
Sec. Digital Public Health
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.687048
This article is part of the Research Topic Aging and Health in China View all 21 articles
Objective: To explore the Chinese community-dwelling intention of older adults to adopt gerontechnology and its influencing factors.
Design: A mixed-methods sequential explanatory design with an inductive approach was employed. In phase 1, a self-made questionnaire was administered from August 2018 to December 2019. Multifactor logistic regression was used to analyze the adoption intention and factors influencing the use of gerontechnology. In phase 2, participants completed a semistructured interview to explore the adoption intention of a specific form of gerontechnology, Smart Aged Care Platform, from May to July 2020.
Setting: Twelve communities in three districts of Chongqing, China.
Participants: Community-dwelling older adults were included.
Results: A total of 1,180 older adults completed the quantitative study; two-thirds of them (68.7%) showed adoption intention toward gerontechnology. Nineteen participants (10 users and nine nonusers) completed the qualitative study and four themes were explored. Through a summarized understanding of the qualitative and quantitative data, a conceptual model of influencing factors, namely, predictive, enabling, and need factors, was constructed.
Conclusions: This study reveals that most Chinese community-dwelling older adults welcome the emergence of new technologies. However, there was a significant difference in the adoption intention of gerontechnology in Chinese community-dwelling older adults based on their sociodemographic and psychographic characteristics. Our findings extend previous technology acceptance models and theories and contribute to the existing resource base.
In 2019, the number of older people aged over 60 years in China reached 249 million, accounting for 17.9% of the total population (1). It is estimated that by 2050, the total number of older people will exceed 465 million, and 32.3% of them will be over 80 years old (2). As a result, China is not only the country with the highest proportion of elderly people in the world but also one of the countries with the fastest aging rate (3, 4). In addition to the one-child policy (5), population migration to cities (6) and an increase in the “empty nest” elderly population (7) have made it more difficult for Chinese modern families to maintain traditional home-based care (8). Furthermore, with the enhancement of living standards and lifestyles, the demand of older adults for old-age services has become varied; thus, personalized and smart services are being emphasized (9, 10). As a result, there is a growing awareness of the importance of developing and implementing comprehensive health solutions that are affordable, efficient, and of superior quality for older individuals (11).
Gerontechnology, a portmanteau of gerontology and technology and coined in Europe in the early 1990s, refers to techniques, technological products, services, and environments that are aimed at improving the daily life and aging of the elderly with technological advances (12, 13). Conceptually, gerontechnology can be divided into four categories according to its use (14): first, gathering continuous data (e.g., heart rate and motion) to monitor the performance of older adults or detect falls through wearable sensors (15); second, assisting older people cognitively and socially using, for instance, interactive robotic pets (16); third, providing care or monitoring of health from a distance, with the help of telecare or telemedicine (17); and finally, compensating for possible technology deficits in the home environment, which mainly refers to a smart home (18). Some gerontechnological solutions fulfill multiple purposes such as the Smart Aged Care Platform designed by our team (19). In this study, gerontechnology is used as an umbrella term for all the aforementioned technologies.
Gerontechnology helps older adults maintain their health and wellbeing in their homes (20), which is considered to be of positive significance to aging in place (21). Using telecommunications, gerontechnology can now provide health professionals and caregivers with remote access to older patients (22). In addition, gerontechnology has shown great potential in reducing escalating medical costs by eliminating the need for expensive and limited medical facilities (18, 23). In the context of the accelerated aging process, gerontechnology already has a broad market prospect (24), and delivering healthcare services based on gerontechnology has been one of the trends of providing care for older adults in China (25).
Compared to developed countries, the smart health technology of China is still in its infancy. It was only in 2012 that the Chinese Nation Working Commission on Aging first introduced the concept of gerontechnology (26). Thus, although several international studies have explored the perspectives of older adults on emerging technologies across the world (27–31), the data on China are still insufficient. Thus, this study aims to determine:
1. Chinese community-dwelling intention of older adults to adopt gerontechnology.
2. The factors influencing the adoption intention and use of gerontechnology.
A mixed-methods sequential explanatory design with an inductive approach (19) was employed. To explain the quantitative results in more depth, qualitative data comprising the perspectives of participants were collected. Such a sequence of research design had been supported by past studies (32). In phase 1, 1,180 community-dwelling older adults completed a self-made questionnaire from August 2018 to December 2019. Multifactor logistic regression was used to analyze the adoption intention and factors influencing the use of gerontechnology. In phase 2, 19 participants were recruited, who completed a semistructured interview, to explore the adoption intention of a specific form of gerontechnology, Smart Aged Care Platform, from May to July 2020. The flow diagram is shown in Figure 1. This method has previously been used to investigate gerontechnology adoption by using specific forms of gerontechnology such as near-field communication (NFC)-enabled light systems (33) and soft service robots (34).
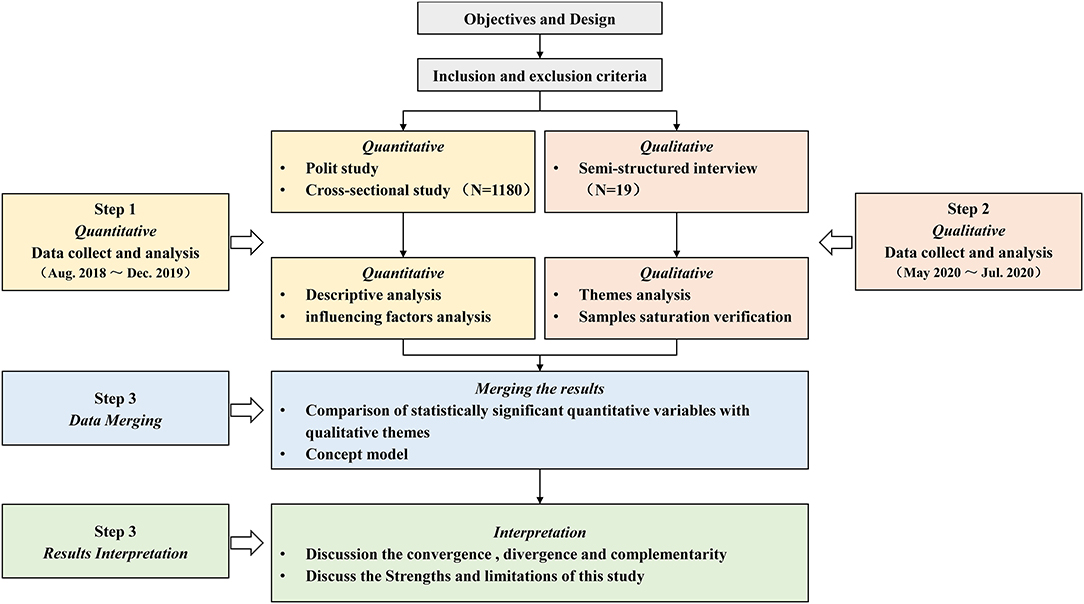
Figure 1. Flow diagram.
The Smart Aged Care Platform was designed by our team and empirically tested in Chongqing since January 2020 (35). Up to July 2020, 180 older adults were registered on the platform. The platform was developed to improve the way of life of older adults by helping them live independently. It was designed based on a hybrid aware model (23, 36), which consists of five subsystems: physiological data sensing system, environment data sensing system, location data sensing system, activities data sensing system, and decision support system. Table 1 summarizes the features and functions of each subsystem, and Figure 2 presents the sleep monitoring interface of the Smart Aged Care Platform.
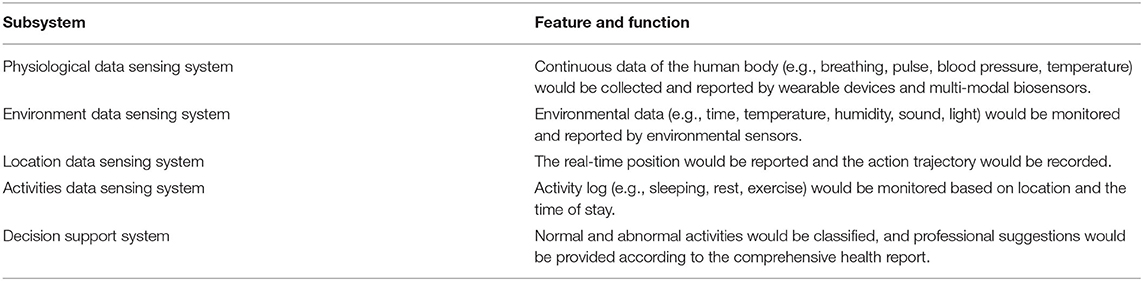
Table 1. User portal (Smart Aged Care Platform) feature summary.
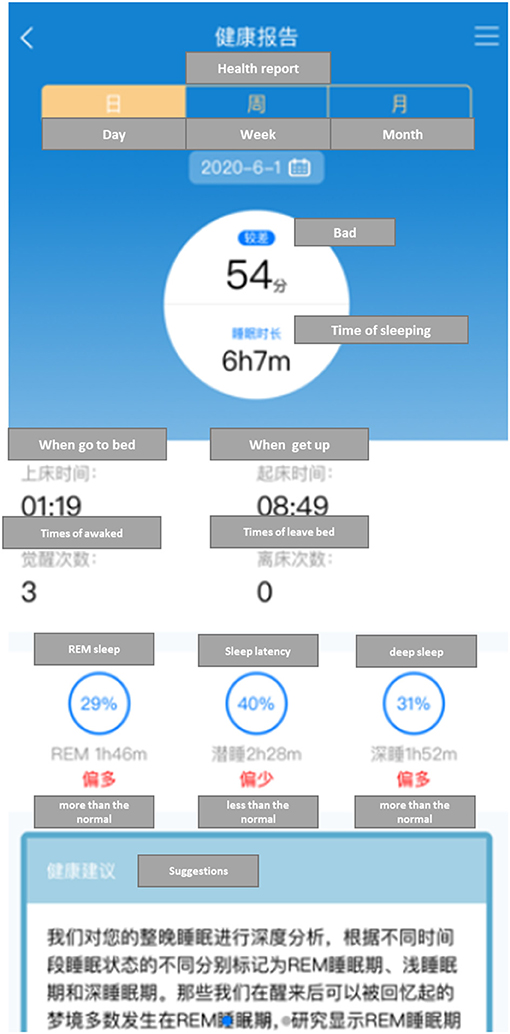
Figure 2. The sleep monitoring and reporting interface of Smart Aged Care Platform.
Chongqing, the largest city in the southwest, is one of the four major municipalities in China, and one of the most rapidly aging modern cities (37). In 2018, the number of older adults over the age of 60 in Chongqing reached 7.195 million, accounting for 21.13% of the total population. Thus, considering the economic level, the number of older people, and other comprehensive factors, 12 communities in three districts of Chongqing were selected as the main site for the study, as it is very probable that the findings would be similar throughout another metropolis of China.
Convenience sampling was carried out in 12 communities in three districts of Chongqing from August 2018 to December 2019. The inclusion criteria were: (1) participants aged over 60 years, (2) those who have been living in the community for more than 6 months, (3) those who could correctly understand the contents of the questionnaire, and (4) those who do not have experience using gerontechnology. Participants who were diagnosed with critical or end-stage diseases, severe psychosis, or cognitive impairment were excluded. Based on the sample size estimation method for multivariate analysis study, the sample size should be 10–20 times the questionnaire variables (38). Hence, a sample size of approximately 260 participants was required. Finally, a total of 1,200 questionnaires were distributed, of which only 1,180 were received, with an effective recovery rate of 98.33%.
Data collection was carried out in the same communities as the first phase from May to July 2020. Due to the differences in e-health literacy and expression ability among different types of older people, the purposive sampling method was used to recruit participants to maximize the variation, in which education level, age, gender, experience using gerontechnology, and other factors were particularly considered. Subsequently, 19 participants were interviewed (n = 10 users; n = 9 nonusers). Users were those who had registered for the Smart Aged Care Platform and had logged in within the last 5–7 months. Nonusers were older adults who had neither registered for the platform nor used other kinds of gerontechnology.
A self-made questionnaire was used, which consisted of three parts: (1) demographic information, namely, gender, age, education level, marital status, monthly income, and type of medical insurance; (2) health status information, namely, self-assessment of health level, chronic disease, and disability; and (3) adoption intention toward gerontechnology, which was assessed by asking participants if they “would intend to use or purchase gerontechnology-related services or products in 6 months” (0 = No; 1 = Yes).
A face-to-face, semistructured interview was conducted to explore and expand the potential factors that affect the adoption intention of gerontechnology by Chinese community-dwelling older adults. Participants were asked to discuss their perceptions about the rise of gerontechnology, any good or bad experiences they have had, the main challenges they face regarding adoption, and optimization advice or anticipation of their wants.
The investigators are uniformly trained medical students, namely, five undergraduate and two graduate students, who were instructed to obtain the consent of the participants and their guardians before the investigation, and to inform all participants of the purpose and content of the study before it began. In the survey, a unified introduction was provided to guide participants through the process of answering questions. The filling of the questionnaire was standardized by the investigators according to the answers of the participants. After the end of the survey, data were collected, and their validity and completeness were checked.
The first and second authors are registered female nurses who have worked in geriatric nursing for a long time and have experience in conducting qualitative studies. They conducted nine and 10 interviews, respectively, and the duration of each interview was about 40–60 min. All the participants were informed of the objective and significance of this study before the interview. All the interviews were conducted as per the outline, and no specific guide was further required. All interview data were recorded and preserved after getting permission from all the interviewees.
All the data were verified and checked by the two authors in phase 1, and then imported into Stata version 14.0 (StataCorp LP, 2015) for statistical analysis. Frequency, constituent ratio, and mean ± standard deviation ( ± S) were used for descriptive analysis; x2 test was used for comparison; and multifactor logistic regression was used to analyze the influencing factors. The test level was bilateral test α = 0.05.
NVivo version 11.0 (QSR Inc., Melbourne, Australia, 2015) was used for data transcription. A qualitative thematic analysis was used for data analysis (39). The following steps were involved: First, at the end of each interview, the third author was mainly responsible for transcription, while the fourth author was responsible for checking its consistency and accuracy. The two did not participate in the interview sessions. Second, the researchers reviewed each transcript line by line to become completely familiar with the content. Then, all the data were initially coded and similar data were classified to form different topics (40). In addition, a list of themes was returned to the participants to reach a consensus on the validity again. Themes were defined and named until the final findings were negotiated among team members. Recruitment stopped when the data reached saturation, that is, when there were no new codes and topics obtained (41). To verify the saturation, five new participants were recruited. The results showed that the resulting topic contained all the important codes and topics put forward by the newly included participants, so it is considered that the samples at this stage are suitable (42).
All the participants were recruited in two parts by the local community health center through recruitment advertisements, and the location of the study was the generally quiet and undisturbed conference room of the agency. Participants and the public were not involved in the design of the quantitative research but were invited to assist in the confirmation process of the qualitative research.
Before the commencement of the study, approval was obtained from the ethics committee of the institution (approval number: 2019-105), and all the participants provided oral consent and willingness to complete the investigation. Transcripts and analysis records were stored on a secure cloud-based server. The anonymity of the respondents was protected in the form of digital codes.
A total of 1,180 participants were included in the quantitative research, whereas in the qualitative research, 19 older adults were invited to be interviewed. Table 2 provides the demographic information of all the participants.
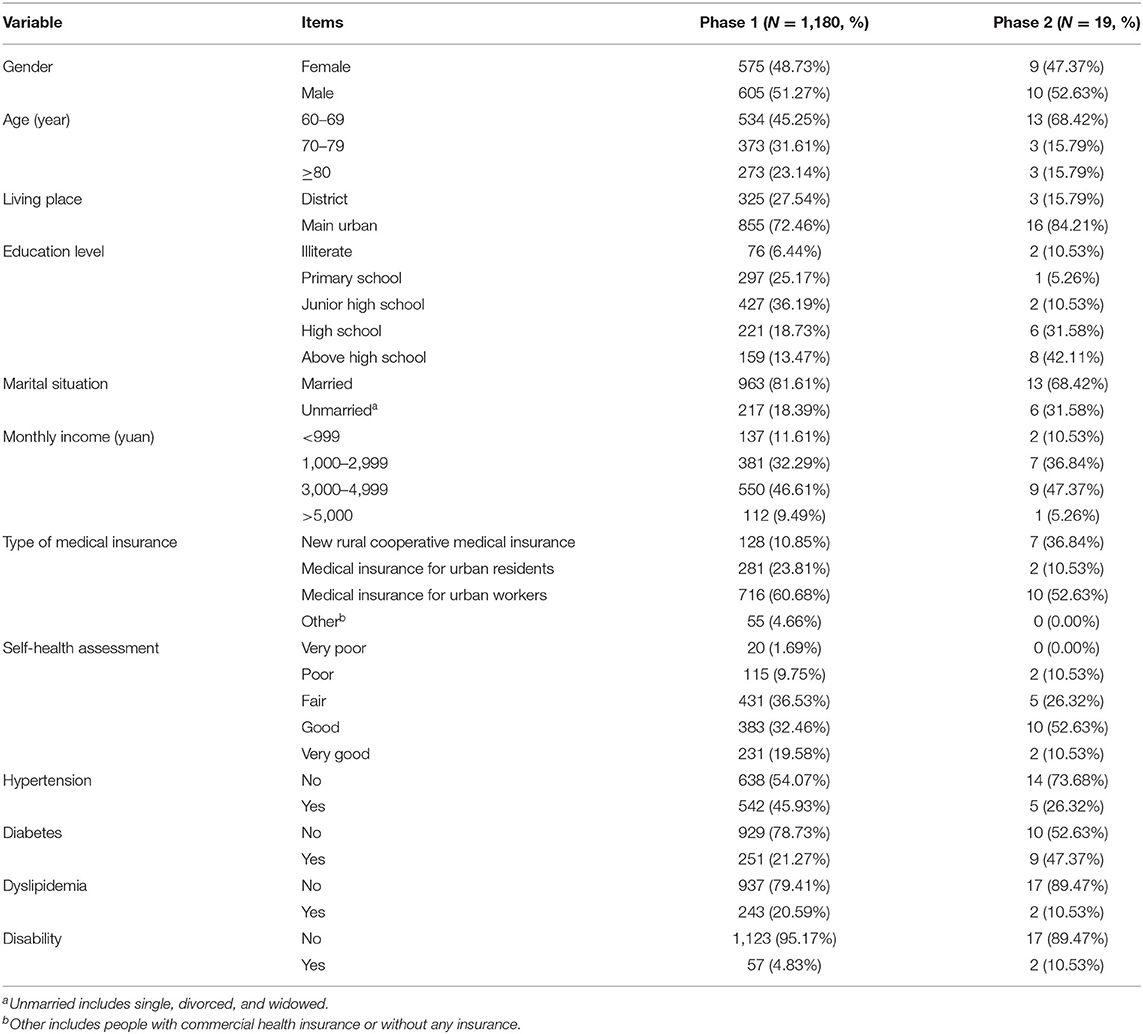
Table 2. Demographic information of all the participants.
A total of 811 (68.7%) older adults showed adoption intention toward gerontechnology. The multiple collinearity test among the variables shows that the variance inflation factor of the model is <10, so there are no multiple collinearities among the variables. Among them, the community older adults with different gender, living places, education levels, monthly income, type of medical insurance, self-health assessment, hypertension, diabetes, dyslipidemia, and disability had different intentions. The difference was statistically significant (P < 0.05), as shown in Table 3.
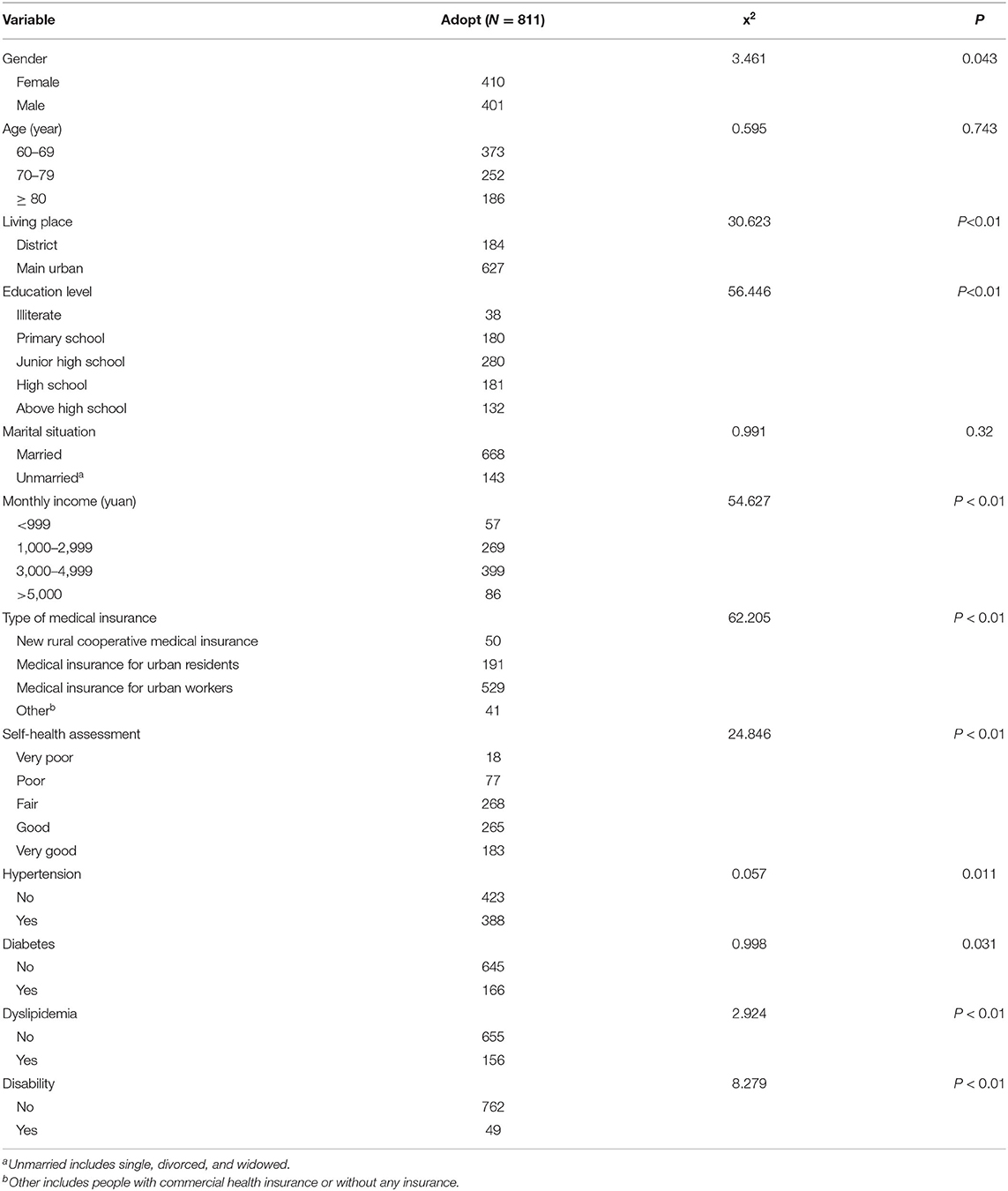
Table 3. Univariate analysis.
The adoption of gerontechnology was set as a dependent variable, and the variables with statistical differences in univariate analysis were taken as independent variables. Multivariate logistic regression analysis was carried out to test the goodness of fit of the model, as shown in Table 4. Omnibus tests of model coefficients showed that x2 = 153.721 (P < 0.01), and the Hausman and Lemeshow test showed that x2 = 157.266 (P = 0.303 > 0.1). The results showed that the most significant factors for the community-dwelling older adults to adopt gerontechnology (P < 0.05) included above high school education (OR = 3.595, 95% CI = 1.707–7.571), monthly income between 1,000 and 2,999 yuan (OR=2.126, 95% CI=1.326–3.407), other type of health insurance (OR=3.336, 95% CI=1.573–7.072), poor self-health assessment (OR= 0.291, 95% CI= 1.061–1.376), hypertension (OR = 1.643, 95% CI = 1.216–2.221), diabetes (OR = 0.691, 95% CI = 0.497–0.96), dyslipidemia (OR = 0.567, 95% CI = 0.397–0.809), and disability (OR = 2.515, 95% CI = 1.118–5.658).
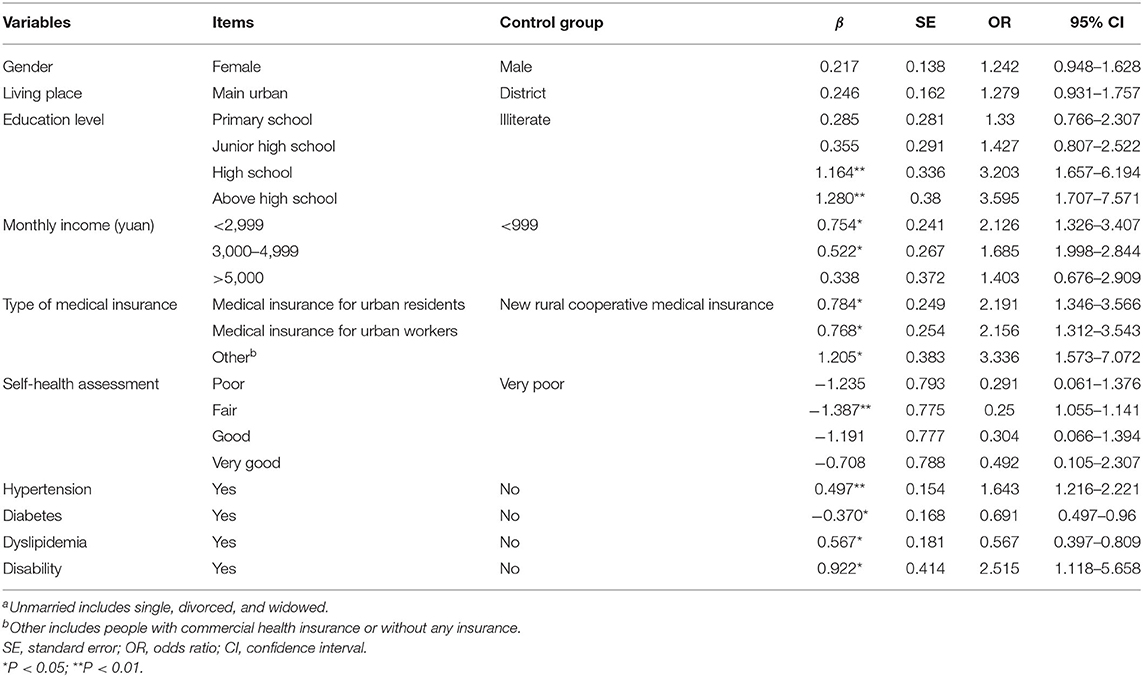
Table 4. Multivariate logistic regression analysis.
Four themes and six subthemes were defined after thematic analysis.
The study found that most participants showed a positive attitude toward gerontechnology, believed that with the development of science and technology, it will be helpful to use emerging technologies to maintain and improve the quality of life in twilight years, and thought that this is a kind of care and well-being. “The standard of living is getting higher and higher…. Even the elderly can enjoy the fruits of science and technology.”, Q4.
Some participants reported that they had begun to use a variety of digital technologies at home, such as WeChat, Internet devices, and home sensors, to establish contact with their families and medical staff, and had had a pleasant experience. “It's great that the machine can record the data directly and upload it to the cloud, then the doctor can track the changes. That's good.”, Q9.
Some participants reported their confidence in the use of new technologies and products, and showed great curiosity; while others were relatively cautious, believing that the use of new technologies is time and energy consuming under the idea that traditional services can meet the demand. “I am old in age, but young in mind. Although I am more than 70 years old, I always live with the mentality of learning.”, Q1. “I feel that my life is very comfortable now, and I don't want to put an extra burden on myself.”, Q13.
Generally, most participants were worried about adverse events or complications of diseases. Those who had experienced such events before were more aware of the importance of health management in their daily life. “Thirty percent depends on the doctor, and the rest depends on maintenance in your daily life.”, Q16. One participant who once fell recalled that using home smart technology increased her sense of security and self-confidence to live alone at home. “I fell and couldn't take care of myself for months. I'm afraid of falling again.…, technologies gave me a sense of security because I knew someone would come to help me in case of any emergency.”, Q7.
The sense of control over technology and products was the biggest concern of the participants. The older adults had observed the effects of aging on their daily life, which might have limited their ability to adopt new technology. “I am worried that I cannot use it correctly…, after all, this is a high-tech creation.”, Q2. The suitability of the technical features of the products affected the adoption intention of participants. “If the screen is too small, it will make it more difficult for me to read…,” “if this product is a behemoth, I don't think most old people will like it.”, Q11.
Reliability concerns whether the efficacy of the product or service felt by the user is stable and reliable. For example, some participants reported doubts about the accuracy of home technology measurement. “I'm not sure if the data measured by these kinds of products are accurate, just like those in hospitals.”, Q5.
Participants also expressed concerns about the resources needed to use the product. The cost of technology was the biggest concern. “Although there are many benefits, you know, there is very little money for the older adults.”, Q17. Some participants suggested that national policies need to help and support older adults. “If this is the future trend of our country, then the government should consider how to help the low-income elderly to bear these expenses.”, Q9.
Some older people mentioned community and family resources and remarked that access to the Internet was a problem. “If I live in the city, everything is fine, but if I go back to the countryside and I don't have Internet, then I have to abandon it.”, Q18. Other participants had some doubts about the ability of the community to provide timely services. “I mean, if we are far away, the healthcare workers in the ‘cloud’ will not be able to arrive at home to deal with the crisis as soon as possible.”, Q2.
Assessed need refers to the actual poor physical condition of an individual. Many participants pointed out that if such technologies possess only conventional functions, such as measuring vital signs and environmental sensing, they would not be particularly attractive, but if the functions of these technologies and products are targeted to meet individual needs and can solve real problems in life, then they can be promoted for the well-being of the older adults. “This is one of the doctor's suggestions, which allows me to avoid frequent hospitalization and reduce medical expenses.”, Q3.
Perceived needs mean that the older population were not satisfied with their current health level or were willing to have a healthier experience; therefore, they were willing to try a helpful technology in achieving the same. Some participants pointed out that walking is a common leisure activity, and smart bracelets can help them understand and visualize their heart rate and evaluate their exercise intensity. Participants also pointed out that sleep quality is another important indicator of physical health. “I often suffer from insomnia, and smart mattresses can be linked to my phone's application to help me understand how I sleep every night.”, Q1.
We found that the results of the two phases complemented each other. For example, income, health insurance policy, self-health assessment, and actual health status were considered as influencing factors in both quantitative and qualitative results. In addition, some other factors such as personal characteristics, resource accessibility, and product characteristics were supplemented and found in interviews.
Therefore, we created a loose conceptual model based on the technology acceptance model (43) and health behavioral model of Anderson (44) to classify and visualize the factors found. As adoption intention is the main concern of this study, it is selected as the central action, which links the main results (Figure 3).
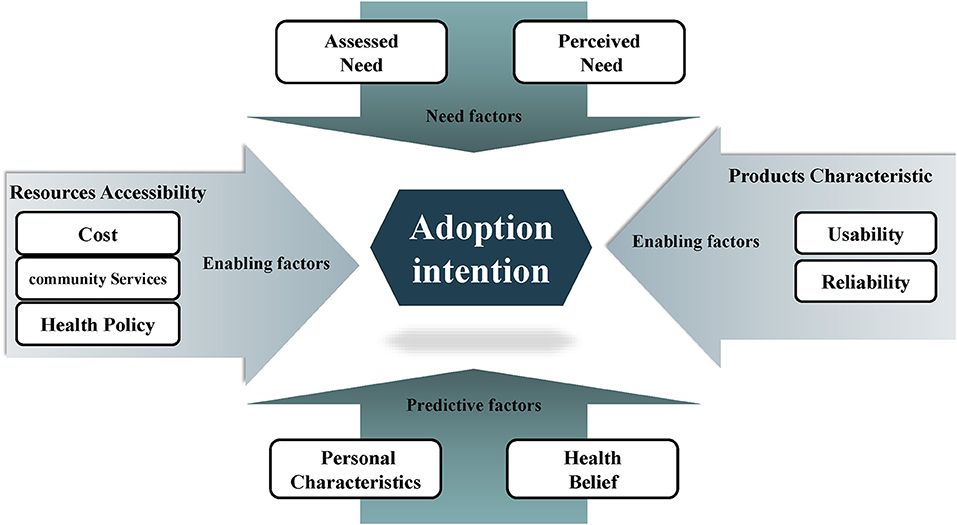
Figure 3. Conceptual model of influencing factors.
The definitions are determined as: (1) predictive factors, namely, personality traits and health beliefs, refer to the social-demographic characteristics that affect the adoption intention of older adults and use of gerontechnology. (2) Enabling factors, namely, product characteristics and resource accessibility, refer to the requirements of realizing technology utilization. (3) Need factors, namely, assessed and perceived needs, refer to the needs of community-dwelling older adults regarding the use of gerontechnology.
The results show that about two-thirds (68.7%) of the older population in this study shows adoption intention of gerontechnology, and welcomes the emergence of these technologies, which is consistent with the findings of many previous studies (45, 46).
However, we found a significant difference in the adoption intention of gerontechnology in Chinese community-dwelling older adults based on their sociodemographic characteristics. This result differs from the findings of a study conducted by Lim et al. (47), in which the subsequent impacts of usefulness evaluations on the intentions of older adults to use the NFC light system were explored. It was consequently found that older adults do not differ in their intentions to use gerontechnology when demographics and psychographics are considered. We feel that the results of our study differed because, in phase 1, the investigation was conducted with community-dwelling older adults, who do not have experience of using gerotechnology. Hence, their perceptions were based partly on their imagination and expectations regarding gerotechnology. According to existing literature, the evidence of the impact of demographic variables on the adoption of gerontechnology is inconsistent and weak (46, 48). Vroman et al. (31) proposed that age, education, and attitude are related to the adoption of technology. In addition to the above factors, de Veer et al. (46) found that men are more likely to adopt e-healthcare than women. Therefore, in the future, it is necessary to focus on the quantitative investigation of the impact of social-demographic characteristics on the adoption of technology.
More importantly, this study focused on the reasons, thoughts, and factors influencing the adoption intention of a specific gerontechnology from the perspective of community-dwelling older persons. The findings revealed that the factors influencing adoption intention are complex and systematic (49, 50), which involve predictive, enabling, and need factors. This knowledge can be applied to the design, improvement, optimization, and promotion of the technology industry, products, and services in the future.
This study found that personality traits and health beliefs are important influencing factors and are deemed as predictive factors.
This study supports the evidence of the influence of personality traits on the adoption of technology. Qualitative research found that older users with optimistic characteristics and curiosity were more willing to try new products and technologies, which suggests that product developers should consider the psychological characteristics of the target consumers (49).
In addition, it was found that health beliefs were related to the behavior and willingness of older adults, which is consistent with previous research results (51–53). It is suggested that while formulating marketing strategies for geriatric technology, seminars must be designed simultaneously to raise awareness of its possible significant health benefits.
Product characteristics are a significant part of enabling factors. One is usability, which mainly refers to the external features of technology, whose importance has been demonstrated in previous studies (51, 54, 55). Another is reliability, which emphasizes more on the inherent quality of technology, however, there are different views on this factor (45). Kaium et al. (56) found that system quality, expected performance, convenience, and social influence are of great significance to the continuous adoption intention of older adults in developing countries; however, service and information quality are not. While Hsieh et al. (57) found that system quality has the greatest impact on use intention and service quality has the strongest overall impact on user satisfaction (57). Overall, our study suggested that usability is as important as reliability; usability allows the participants to use the product correctly and reliability ensures that they can achieve the desired results. At present, more and more engineers and gerontologists are beginning to collaborate on issues at the intersection of technology, and listen extensively to the views of older users to find innovative solutions that are acceptable to older users (58).
In addition, we found that resource accessibility is also an important enabling factor, which consists of community services, cost, and health policy.
Our research results imply that the ability to obtain community services, such as medical care and the Internet, would influence the adoption intention of gerontechnology, which is consistent with related studies. Kohnke et al. (59) found that the support and assistance available during difficult times encourage the intention to use healthcare telemedicine equipment. This suggests that the design of health technologies for older persons should consider the obstacles that they may encounter in using the tool and carefully assess their current level of understanding.
This study suggests additional, potentially fruitful areas of inquiry. For example, our qualitative results found that older adults hope to ease economic pressure with the help of policies. A possible explanation is that since the long-term insurance system of China has not yet been established, most older people who lack a reliable and sustainable income are not willing to take the huge risk of losing money for owning these emerging technologies. Thus, this study suggests that bringing some gerontechnology into the reimbursement category of long-term care insurance in the future could be considered, to encourage older adults to stay at home longer and improve their quality of life with the help of technology.
Cost is examined in the research on almost all types of technologies and appears in various adoption models (51, 54, 55). According to Alsulami et al. (60), the cost of technology poses a great challenge to the behavioral intentions of older adults, in which the costs of installation, maintenance, and running are considered to be the main obstacles (61).
This study shows that the technology adoption intention of the older population is mainly driven by demand, which can be the assessed need for real health situations and the perceived need for health promotion, which is similar to the results of a large number of previous studies (49). However, some studies believe that, compared with the two kinds of demand, the impact of perceived demand is less than that of assessed demand (51). Lee et al. (62) found that the adoption intention of information technology has nothing to do with self-assessed health. Therefore, it is necessary to further study the relationship between the adoption of communication technology and the physical and mental health of older adults in the future.
This study used a mixed-methods approach to explore the complex factors that affect the adoption intention of older adults and constructed a conceptual model, comprising predictive, enabling, and need factors. This study provides theoretical insights on the adoption willingness of the older population in China and is expected to expand the previous technology acceptance models and theories, and to contribute to the existing knowledge database.
This study has four main limitations that could pave the way for further research. First, the relationships between the influencing factors in the conceptual model need to be verified statistically. Second, questionnaires measuring the intention to use gerontechnology have been developed by other scholars (63, 64) recently, and thus, it is suggested that these tools be translated into Mandarin to quantify and verify the intention to gerontechnology. Third, in phase 2, the data or description of the frequency, depth, and types of use of specific gerotechnology could be added to increase analytical depth. Finally, considering the close interaction among stakeholders, perspectives of informal caregivers toward gerontechnology are worth exploring.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the hospital research ethics committee (approval number: 2019-105) and all the participants provided oral consent and willingness to complete the investigation.
QHZ, MZX, and LLX: conceptualization, validation, and supervision. HHH, SMC, and ZYC: methodology. HHH: software and writing original draft preparation. ZYC: formal analysis and visualization. HHH and SMC: investigation. SMC and ZYC: writing, reviewing, and editing. QHZ and MZX: funding acquisition. All authors have read and agreed to the published version of the manuscript.
This research was funded by the Ministry of Science and Technology of China, Grant number 2020YFC2005900, Municipal Education Commission of Chongqing, China, Grant number KJCX2020018&yjg211006, and Science and Technology Committee of Chongqing, China, Grant number cstc2018jscx-maszdX00113. However, the funders had no role in the study design, data collection, management, analysis, or interpretation, manuscript writing, or the decision to submit the report for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would thank all the participants who contributed their time to the study. The authors also acknowledge Qi Huang, Taoyi Li, Yaxin Guan, Xuan Che, Jia He, and Hong Dong for their support in the recruitment of study participants.
1. State Statistics Bureau. National data. (2019). Available at: http://data.stats.gov.cn/search.htm?s=%E6%80%BB%E4%BA%BA%E5%8F%A3 (accessed February 25, 2020).
2. Fang EF, Scheibye-Knudsen M, Jahn HJ, Li J, Ling L, Guo H, Zhu X, et al. A research agenda for aging in China in the 21st century. Ageing Res Rev. (2015) 24:197–205. doi: 10.1016/j.arr.2015.08.003
3. Chen R, Xu P, Song P, Wang M, He J. China has faster pace than Japan in population aging in next 25 years. Biosci Trends. (2019) 13:287–91. doi: 10.5582/bst.2019.01213
4. Yang G, Wang Y, Zeng Y, Gao GF, Liang X, Zhou M, et al. Rapid health transition in China, 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet. (2013) 381:1987–2015. doi: 10.1016/S0140-6736(13)61097-1
5. Muramatsu N, Mitzen PB, Burton JR, Djangi AR, Dong X, Flowers N, et al. China's one-child policy and US long-term care. J Am Geriatr Soc. (2016) 64:e61–62. doi: 10.1111/jgs.14292
6. Dou X, Liu Y. Elderly migration in China: types, patterns, and determinants. J Appl Gerontol. (2017) 36:751–71. doi: 10.1177/0733464815587966
7. Qian Y, Qin W, Zhou C, Ge D, Zhang L, Sun L. Utilisation willingness for institutional care by the elderly: a comparative study of empty nesters and non-empty nesters in Shandong, China. BMJ Open. (2018) 8:e022324. doi: 10.1136/bmjopen-2018-022324
8. Phillips DR, Feng Z. Challenges for the aging family in the People's Republic of China. Can J Aging. (2015) 34:290–304. doi: 10.1017/S0714980815000203
9. Xiao M, Lei X, Zhang F, Sun Z, Harris VC, Tang X, Yan L. Home blood pressure monitoring by a mobile-based model in Chongqing, China: a feasibility study. Int J Environ Res Public Health. (2019) 16:3325. doi: 10.3390/ijerph16183325
10. Bao Y, Hoque R, Wang S. Investigating the determinants of Chinese adult children's intention to use online health information for their aged parents. Int J Med Inform. (2017) 102:12–20. doi: 10.1016/j.ijmedinf.2017.01.003
11. Lv Q, Jiang Y, Qi J, Zhang Y, Zhang X, Fang L, et al. Using mobile apps for health management: a new health care mode in China. JMIR mHealth and uHealth. (2019) 7:e10299. doi: 10.2196/10299
12. Graafmans JA, Taipale V, Charness N. Gerontechnology: a sustainable investment in the future. Stud Health Technol Inform. (1998) 48:3–6. doi: 10.3233/978-1-60750-892-2-3
13. Miskelly F. Gerontechnology: growing old in a technological society. Age Ageing. (2007) 36:706. doi: 10.1093/ageing/afm125
14. Sundgren S, Stolt M, Suhonen R. Ethical issues related to the use of gerontechnology in older people care: A scoping review. Nurs Ethics. (2020) 27:88–103. doi: 10.1177/0969733019845132
15. Piau A, Mattek N, Crissey R, Beattie Z, Dodge H, Kaye J. When will my patient fall? Sensor-based in-home walking speed identifies future falls in older adults. J Gerontol A Biol Sci Med Sci. (2020) 75:968–73. doi: 10.1093/gerona/glz128
16. Hudson J, Ungar R, Albright L, Tkatch R, Schaeffer J, Wicker ER. Robotic pet use among community-dwelling older adults. J Gerontol B Psychol Sci Soc Sci. (2020) 75:2018–28. doi: 10.1093/geronb/gbaa119
17. Evans J, Papadopoulos A, Silvers CT, Charness N, Boot WR, Schlachta-Fairchild L, et al. Remote health monitoring for older adults and those with heart failure: adherence and system usability. Telemed J E Health. (2016) 22:480–8. doi: 10.1089/tmj.2015.0140
18. Arthanat S, Wilcox J, Macuch M. Profiles and predictors of smart home technology adoption by older adults. OTJR (Thorofare N J). (2019) 39:247–56. doi: 10.1177/1539449218813906
19. Creswell JW, Clark P. Research design: Qualitative, quantitative and mixed methods approaches. Third London: SAGE. (2009).
20. Liu L, Stroulia E, Nikolaidis I, Miguel-Cruz A, Rios Rincon A. Smart homes and home health monitoring technologies for older adults: A systematic review. Int J Med Inform. (2016) 91:44–59. doi: 10.1016/j.ijmedinf.2016.04.007
21. Özsungur F. A research on the effects of successful aging on the acceptance and use of technology of the elderly. Assist Technol. (2019) 1–14. doi: 10.1080/10400435.2019.1691085
22. Correa G, Domènech M. Care networking: a study of technical mediations in a home telecare service. Int J Environ Res Public Health. (2013) 10:3072–88. doi: 10.3390/ijerph10073072
23. Loreti D, Chesani F, Mello P, Roffia L, Antoniazzi F, Cinotti TS, et al. Complex reactive event processing for assisted living: The Habitat project case study. Expert Syst Appl. (2019) 126:200–17. doi: 10.1016/j.eswa.2019.02.025
24. Kao Y-S, Nawata K, Huang C-Y. An exploration and confirmation of the factors influencing adoption of iot-based wearable fitness trackers. Int J Environ Res Public Health. (2019) 16:3227. doi: 10.3390/ijerph16183227
25. The State Council of China. Guidelines on actively promoting the “Internet Plus” initiative.(2015). Available online at: http://www.gov.cn/zhengce/content/2015-07/04/content_10002.htm (accessed August 19, 2020).
26. Zuo M. The connotation, mode and opportunity of smart aged care. China Public Security. (2014) 48–50. doi: 10.3969/j.issn.1672-2396.2014.10.003
27. Ahn M, Beamish JO, Goss RC. Understanding older adults' attitudes and adoption of residential technologies. Fam Consum Sci Res J. (2008) 36:243–60. doi: 10.1177/1077727X07311504
28. Demiris G, Rantz MJ, Aud MA, Marek KD, Tyrer HW, Skubic M, et al. Older adults' attitudes towards and perceptions of ‘smart home’ technologies: a pilot study. Med Inform Internet Med. (2004) 29:87–94. doi: 10.1080/14639230410001684387
29. Mitzner TL, Boron JB, Fausset CB, Adams AE, Charness N, Czaja SJ, et al. Older adults talk technology: Technology usage and attitudes. Comput Human Behav. (2010) 26:1710–21. doi: 10.1016/j.chb.2010.06.020
30. Peek STM, Luijkx KG, Rijnaard MD, Nieboer ME, Voort CS, van der, Aarts S, et al. Older Adults' Reasons for Using Technology while Aging in Place. Gerontology. (2016) 62:226–37. doi: 10.1159/000430949
31. Vroman KG, Arthanat S. Lysack C. “Who over 65 is online?” Older adults' dispositions toward information communication technology. Computers in Human Behavior. (2015) 43:156–66. doi: 10.1016/j.chb.2014.10.018
32. Park Y-H, Chang HK, Lee MH, Lee SH. Community-dwelling older adults' needs and acceptance regarding the use of robot technology to assist with daily living performance. BMC Geriatr. (2019) 19:208. doi: 10.1186/s12877-019-1227-7
33. Teh P-L, Lim WM, Ahmed PK, Chan AHS, Loo JMY, Cheong S-N, et al. Does power posing affect gerontechnology adoption among older adults? Behav Inf Technol. (2017) 36:33–42. doi: 10.1080/0144929X.2016.1175508
34. Lee L, Lim W, Teh P-L, Malik O, Nurzaman S. Understanding the interaction between older adults and soft service robots: insights from robotics and the technology acceptance model. AIS Transactions on Human-Computer Interaction. (2020) 12:125–45. doi: 10.17705/1thci.00132
35. Huanhuan H, Kejia Z, Songmei C, Xuejun C, Mingzhao X, Rongrong W, et al. Establishment and practice of smart aged care platform based on hybrid aware model. Chin J Nurs. (2021) 56:421–6. doi: 10.3761/j.issn.0254-1769.2021.03.018
36. Jung Y. Hybrid-aware model for senior wellness service in smart home. Sensors (Basel). (2017) 17:1182. doi: 10.3390/s17051182
37. Giri M, Chen T, Yu W, Lü Y. Prevalence and correlates of cognitive impairment and depression among elderly people in the world's fastest growing city, Chongqing, People's Republic of China. Clin Interv Aging. (2016) 11:1091–8. doi: 10.2147/CIA.S113668
39. Braun V, Clarke V, Braun V, Clarke V. Using thematic analysis in psychology. (2006) 3:77–101. Available at: http://www.mendeley.com/catalog/braun-v-clarke-v-using-thematic-analysis-psychology-32-2006-77101/ (accessed May 18, 2020).
40. Marshall CD, Rossman GB. Designing qualitative research. Modern Language Journal. (1999) 80:224. doi: 10.2307/329453
41. Sandelowski M. Sample size in qualitative research. Res Nurs Health. (1995) 18:179–83. doi: 10.1002/nur.4770180211
42. Moser A, Korstjens I. Series: Practical guidance to qualitative research. Part 3: Sampling, data collection and analysis. Eur J Gen Pract. (2018) 24:9–18. doi: 10.1080/13814788.2017.1375091
43. Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS quarterly. (1989) 319–40. doi: 10.2307/249008
44. Kehrer BH, Andersen R, Glaser WA. A. Behavioral Model of families' use of health services. J Human Resources. (1972) 7:125. doi: 10.2307/145064
45. Kavandi H, Jaana M. Factors that affect health information technology adoption by seniors: A systematic review. Health Soc Care Community. (2020) 28:1827–42. doi: 10.1111/hsc.13011
46. de Veer AJE, Peeters JM, Brabers AE, Schellevis FG, Rademakers JJJ, Francke AL. Determinants of the intention to use e-Health by community dwelling older people. BMC Health Serv Res. (2015) 15:103. doi: 10.1186/s12913-015-0765-8
47. Lim WM, Teh P-L, Ahmed PK, Chan AHS, Cheong S-N, Yap W-J. Are older adults really that different? Some insights from gerontechnology. In: 2015 IEEE International Conference on Industrial Engineering and Engineering Management (IEEM). Singapore: IEEE. (2015) 1561–1565. doi: 10.1109/IEEM.2015.7385909
48. Khosravi P, Ghapanchi AH. Investigating the effectiveness of technologies applied to assist seniors: A systematic literature review. Int J Med Inform. (2016) 85:17–26. doi: 10.1016/j.ijmedinf.2015.05.014
49. Chen K, Chan AH. Use or non-use of gerontechnology—a qualitative study. Int J Environ Res Public Health. (2013) 10:4645–66. doi: 10.3390/ijerph10104645
50. Zhou J, Zhang B, Tan R, Tseng M-L, Zhang Y. Exploring the systematic attributes influencing gerontechnology adoption for elderly users using a meta-analysis. Sustainability. (2020) 12:2864. doi: 10.3390/su12072864
51. Kim J, Park H-A. Development of a health information technology acceptance model using consumers' health behavior intention. J Med Internet Res. (2012) 14:e133. doi: 10.2196/jmir.2143
52. Chau KY, Lam MHS, Cheung ML, Tso EKH, Flint SW, Broom DR, Tse G, Lee KY. Smart technology for healthcare: Exploring the antecedents of adoption intention of healthcare wearable technology. Health Psychol Res. (2019) 7:8099. doi: 10.4081/hpr.2019.8099
53. Zhang M, Luo M, Nie R, Zhang Y. Technical attributes, health attribute, consumer attributes and their roles in adoption intention of healthcare wearable technology. Int J Med Inform. (2017) 108:97–109. doi: 10.1016/j.ijmedinf.2017.09.016
54. Bagozzi RP. The legacy of the technology acceptance model and a proposal for a paradigm shift. J Associat Informat Systems. (2007) 8:3. doi: 10.17705/1jais.00122
55. Cimperman M, Makovec Brenčič M, Trkman P. Analyzing older users' home telehealth services acceptance behavior—applying an Extended UTAUT model. Int J Med Inform. (2016) 90:22–31. doi: 10.1016/j.ijmedinf.2016.03.002
56. Kaium MA, Bao Y, Alam MZ. Hoque MdR. Understanding continuance usage intention of mHealth in a developing country: An empirical investigation. Int J Pharm Healthc. (2020) 14:251–72. doi: 10.1108/IJPHM-06-2019-0041
57. Hsieh H, Tsai C, Chih W, Lin H. Factors affecting success of an integrated community-based telehealth system. Technology and Health Care. (2015) 23:S189–96. doi: 10.3233/THC-150953
58. Tremblay M, Latulippe K, Giguere AM, Provencher V, Poulin V, Dubé V, et al. Requirements for an electronic health tool to support the process of help seeking by caregivers of functionally impaired older adults: co-design approach. JMIR Aging. (2019) 2: e12327. doi: 10.2196/12327
59. Kohnke A, Cole ML, Bush R. Incorporating UTAUT predictors for understanding home care patients' and clinician's acceptance of healthcare telemedicine equipment. J Technol Management Innovation. (2014) 9:29–41. doi: 10.4067/S0718-27242014000200003
60. Alsulami MH, Atkins AS. Factors influencing ageing population for adopting ambient assisted living technologies in the Kingdom of Saudi Arabia. Ageing Int. (2016) 41:227–39.
61. Peek STM, Wouters EJM, van Hoof J, Luijkx KG, Boeije HR, Vrijhoef HJM. Factors influencing acceptance of technology for aging in place: a systematic review. Int J Med Inform. (2014) 83:235–48. doi: 10.1016/j.ijmedinf.2014.01.004
62. Lee HY, Kim J, Sharratt M. Technology use and its association with health and depressive symptoms in older cancer survivors. Qual Life Res. (2018) 27:467–77. doi: 10.1007/s11136-017-1734-y
63. Anderberg P, Eivazzadeh S, Berglund JS. A novel instrument for measuring older people's attitudes toward technology (TechPH): development and validation. J Med Internet Res. (2019) 21:e13951. doi: 10.2196/13951
Keywords: antioxidants, crop water productivity, irrigation regimes, Mediterranean region, nano-SiO2, principal components analysis, yield contributing traits
Citation: Huang H, Chen Z, Cao S, Xiao M, Xie L and Zhao Q (2021) Adoption Intention and Factors Influencing the Use of Gerontechnology in Chinese Community-Dwelling Older Adults: A Mixed-Methods Study. Front. Public Health 9:687048. doi: 10.3389/fpubh.2021.687048
Received: 29 March 2021; Accepted: 11 August 2021;
Published: 17 September 2021.
Edited by:
Stuart Gietel-Basten, Hong Kong University of Science and Technology, Hong Kong, SAR ChinaReviewed by:
Naubahar Sharif, Hong Kong University of Science and Technology, Hong Kong, SAR ChinaCopyright © 2021 Huang, Chen, Cao, Xiao, Xie and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huanhuan Huang, aHh1ZWhhb0AxMjYuY29t; Qinghua Zhao, cWgyMDA2M0AxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.