 Yongjun Wang
Yongjun Wang Yang Yang
Yang Yang Lina Ren1
Lina Ren1 Xi-jian Dai
Xi-jian Dai
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 09 August 2021
Sec. Public Mental Health
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.684112
Coronavirus disease 2019 (COVID-19), a respiratory disease of unknown origin, has a high rate of morbidity and mortality. Individuals with mental disorders may have a higher risk of infection and worse clinical outcomes because of a variety of factors such as poorer general resilience and lower immune function. However, there have been no studies to date specifically investigating the risk of COVID-19 and associated mortality in these patients. This was addressed in the present study by analyzing the data of 473,958 subjects included in the UK Biobank, 14,877 of whom tested positive for COVID-19 infection. Logistic regression analysis was performed to evaluate the associations between mental disorders and risks of COVID-19 infection and associated mortality. The results showed that subjects who were diagnosed with a mental disorder had a significantly higher risk of developing COVID-19 and a worse outcome as evidenced by higher rates of COVID-19-related mortality, with the strongest effects observed for dementia. Among dementia subtypes, Alzheimer disease patients had the highest risks of COVID-19 infection (7.39-fold increase) and associated mortality (2.13-fold increase). Late-life anxiety only increased the risk of developing COVID-19 while late-life depression not only was associated with a higher risk of infection but also a worse outcome. These findings highlight the need to prioritize patients with mental disorders-especially those who experience these disorders later in life—when implementing preventive strategies such as vaccinations.
Coronavirus disease 2019 (COVID-19), a respiratory disease of unknown origin caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has a high rate of morbidity and mortality, affecting 163 million people and resulting in 3.3 million deaths in over 200 countries (https://www.worldometers.info/coronavirus/, accessed on 16th May 2021). Although neutralizing antibody rapidly develops after infection (1), a second episode of asymptomatic infection occurring 142 days after the first symptomatic episode in an apparently immunocompetent patient has been recently reported (2), suggesting that COVID-19 is a greater public health threat than initially assumed.
According to the World Health Organization, about 20–25% of the adult population is affected by mental disorders (https://www.who.int/). These individuals may have a higher risk of various diseases and have worse physical health and treatment outcomes (3–5) because of a variety of factors such as shorter life expectancy, poorer general resilience, lower immunity (6, 7), and higher susceptibility to infection (8). Recent studies have reported psychological risk factors for infections in general population and among frontline healthcare workers (9, 10). Although several risk factors for COVID-19 infection and associated mortality have been documented [e.g., older age and the presence of complication; (11–13)], the risk for COVID-19 infection and associated mortality left largely unknown.
Recent studies have shown that individuals with a diagnosis of a mental disorder had a higher risk for COVID-19 infection and associated mortality. Li et al. found that patients with a psychiatric diagnosis had a higher risk of mortality compared with those without a psychiatric diagnosis, but the risk of subtypes of psychiatric diagnosis was not studied (14). Nemani et al. found that individuals with a recent psychiatric diagnosis of a schizophrenia spectrum was significantly associated with a higher risk of COVID-19 associated mortality in a small sample-sized cohort study, but those individuals with diagnoses of mood disorders and anxiety disorders were not associated with mortality (15). In a larger sample-sized cohort study by Wang et al. they found that individuals with a recent psychiatric diagnosis of an attention-deficit/hyperactivity disorder, a bipolar disorder, a depression and a schizophrenia had a significantly higher risk for COVID-19 infection (16). However, no such large sample-sized cohort studies concerning on systematically investigated the association of mental disorders (e.g., subtypes of dementia, anxiety, and depression) with COVID-19 infection and associated mortality, especially in a study.
Identifying high-risk populations is important as they can be prioritized in intervention strategies and receive timely and appropriate medical care. In the present larger sample-sized cohort study, we systematically evaluated the impact of middle aged and late-life adults diagnosed with a mental disorder—including psychotic disorders, substance use disorder, bipolar disorder, dementia, anxiety, depression, and depression comorbid with anxiety—on the risk for COVID-19 infection and associated mortality after adjusting for several confounding factors.
After removing the death data (n = 28,547) before 31-November 2019, the remaining data of 473,958 subjects from 22 centers between March 2006 and December 2010 in the UK Biobank were analyzed (Figure 1). Confirmed COVID-19 infection was defined as at least 1 positive test result, 60,446 subjects of whom received COVID-19 test results up to February 24, 2021, with 14,877 subjects confirmed positive for COVID-19 infection (Figure 2). Subjects who did not undergo COVID-19 testing were deemed to have a negative COVID-19 test result. Subjects who received positive COVID-19 test results were classified into two categories: death due to and not due to COVID-19. These data were used to study the risk of COVID-19 associated mortality. Ethical approval was obtained from the North West Multi-Centre Research Ethics Committee (REC reference: 16/NW/0274).
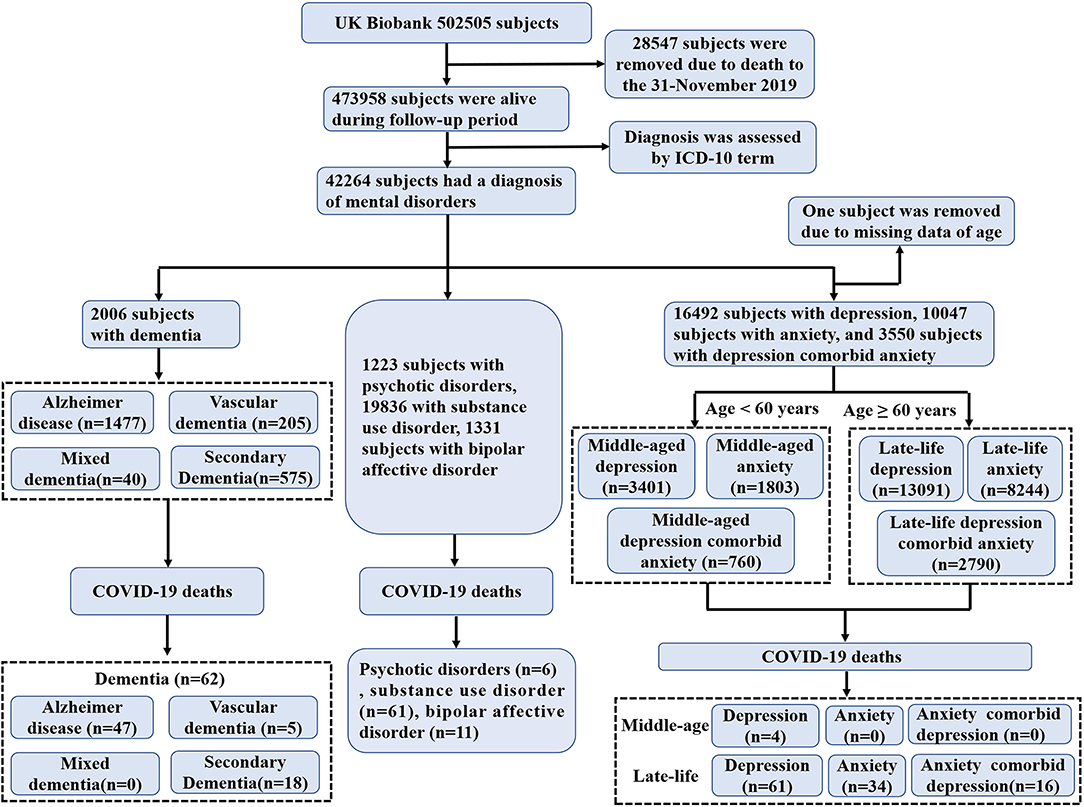
Figure 1. Overview of study sample derivation.
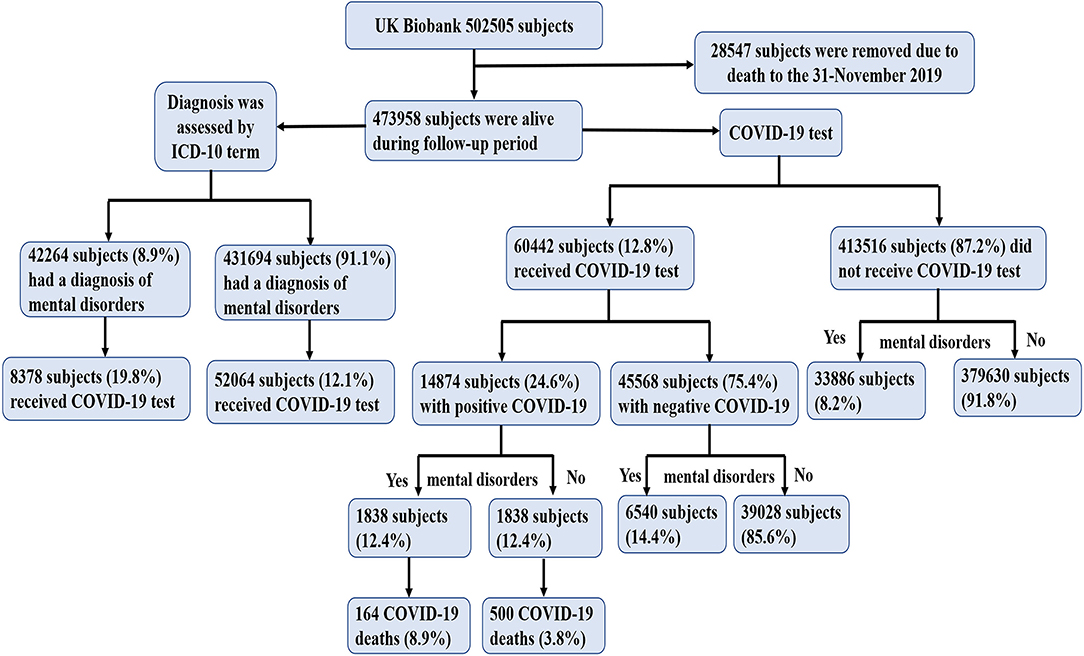
Figure 2. Participant flow diagram with COVID-19.
Mental disorders were classified according to International Classification of Diseases, Version 10 (ICD-10) terms from UK Biobank data field 41,270, these included dementia (ICD-10 codes F00-F04, and G30), psychotic disorder (codes F20-F29), substance use disorder (codes F10-F19), bipolar disorder (codes F30-F31), anxiety (codes F40-F41), and depression (codes F32-F33). Dementia included Alzheimer disease, vascular dementia, mixed dementia, and secondary dementia. Depression and anxiety were grouped according to diagnosis in middle-age (<60 years) and late-life (≥60 years).
Confounding factors included demographic variables (e.g., age, sex, education level, and ethnicity) and comorbidities (e.g., obesity, cerebrovascular disease, diabetes, hypertension, coronary artery disease, cancers, and respiratory diseases).
Education level (Field ID 6138) was classified into two categories depending on the presence of college or university degree. The definition of obesity was a body mass index (BMI) >30 kg/m2. The definition of diabetes included self-reported type 1 or type 2 diabetes and a primary or secondary hospital diagnosis related to diabetes (ICD-10 codes E10-E14.9). Respiratory disease was defined as pulmonary embolism (code I26), other pulmonary heart diseases (code I27), influenza (codes J09-J11), pneumonia (codes J12-J18), acute bronchitis (code J20), acute bronchiolitis (code J21), unspecified acute lower respiratory infection (code J22), other diseases of the upper respiratory tract (codes J30-J39), chronic lower respiratory diseases (codes J40-J47), lung diseases due to external agents (codes J60-J70), other respiratory diseases principally affecting the interstitium (codes J85-86), and other diseases of the pleura and respiratory system (ICD-10 codes J90-99).
Continuous variables are presented as mean ± SD, and categorical variables are presented as a number (percentage). We used unpaired t-test and χ2-test to compare differences between groups where appropriate.
Logistic regression analysis was used to evaluate associations between mental disorders and risk of COVID-19 infection and associated mortality (among subjects who received positive COVID-19 test results). A univariate model (Model 1) and multivariate models (Model 2–4, adjusted for several confounding factors) were applied to determine the Odd Ratios (ORs) and 95% confidence intervals (95% CIs). Two-tailed p < 0.05 were considered statistically significant.
The demographic characteristics of the study population are presented in Table 1. Total of 8.9% subjects (n = 42,264) had a diagnosis of mental disorders, among whom 19.8% subjects (n = 8,378) had a chance to receive the COVID-19 test (21.9% subjects had a positive COVID-19 test result; n = 1,838). Among the 1,838 subjects, 8.9% (n = 164) deaths due to the COVID-19. However, only 12.1% subjects (n = 52,064) had a chance to receive the COVID-19 test among the remaining subjects who did not have a diagnosis of mental disorders (n = 4,31,694).
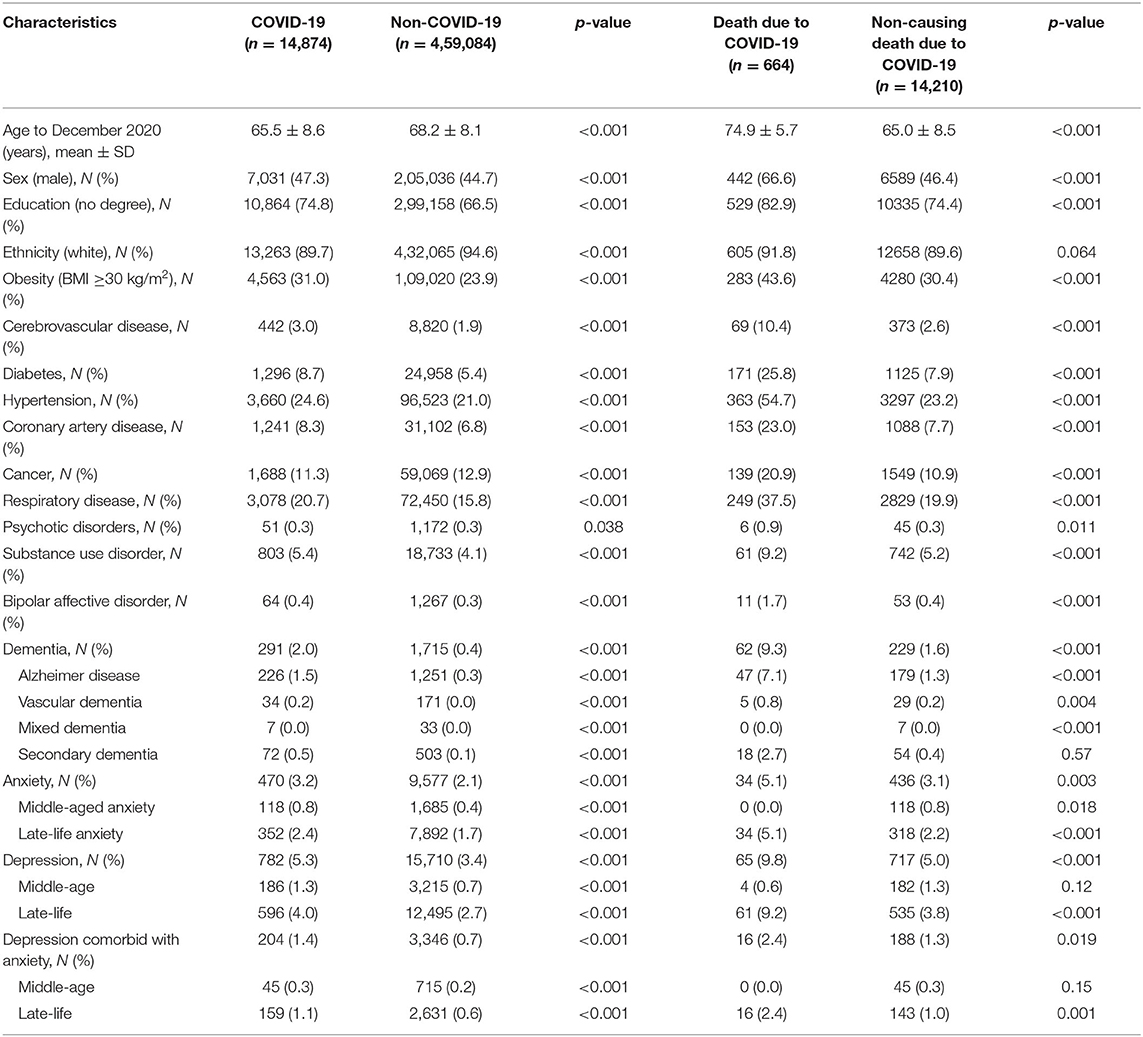
Table 1. Characteristics of UK Biobank cohort.
In general, subjects diagnosed with a mental disorder had higher COVID-19 infection and COVID-19-associated mortality rates than those without a mental disorder; this was not true of COVID-19 morbidity rates in subjects with secondary dementia, middle-aged depression, and middle-aged depression comorbid middle-aged anxiety.
Of the 14,874 subjects in the database who were positive for COVID-19, 664 (4.5%) subjects died due to the COVID-19. Among subjects diagnosed with a mental disorder, the highest rates of COVID-19 infection were among subjects with substance use disorder (5.4%), depression (5.3%), anxiety (3.2%), and dementia (2.0%), whereas subjects with psychotic disorder (0.3%), and bipolar affective disorder (0.4%) had the lowest rates. Among cases of COVID-19-related death, depression (9.8%), dementia (9.3%), substance use disorder (9.2%), and anxiety (5.1%) were the most common mental disorders; there were no deaths from COVID-19 among subjects with mixed dementia, middle-aged anxiety and middle-aged depression comorbid with anxiety.
Subjects with a diagnosis of dementia (OR [95% CI]: 6.43 [5.62, 7.35], p < 0.001), anxiety (1.29 [1.17, 1.42], p < 0.001), or depression (1.22 [1.13, 1.31], p < 0.001) had a significantly higher probability of COVID-19 infection than those without a mental disorder after adjusting for age, sex, education level, ethnicity, BMI, cerebrovascular disease, diabetes, hypertension, coronary artery disease, cancer, and respiratory disease, with the strongest effect observed for Alzheimer disease (7.39 [6.36, 8.60], p < 0.001) among dementia subtypes (Table 2). Furthermore, we also analyzed the COVID-19 risk of these mental disorders among the subjects who received COVID-19 test. Subjects with a diagnosis of dementia (2.89 [2.48, 3.36], p < 0.001) still had a significantly higher probability of COVID-19 infection than those without a mental disorder, and all dementia subtypes showed more than 2-fold risk of COVID-19 infection (Alzheimer disease, 2.94 [2.47, 3.49], p < 0.001; vascular dementia, 3.88 [2.45, 6.14], p < 0.001; mixed dementia, 4.58 [1.68, 12.50], p = 0.011; secondary dementia, 2.40 [1.78, 3.24], p < 0.001).
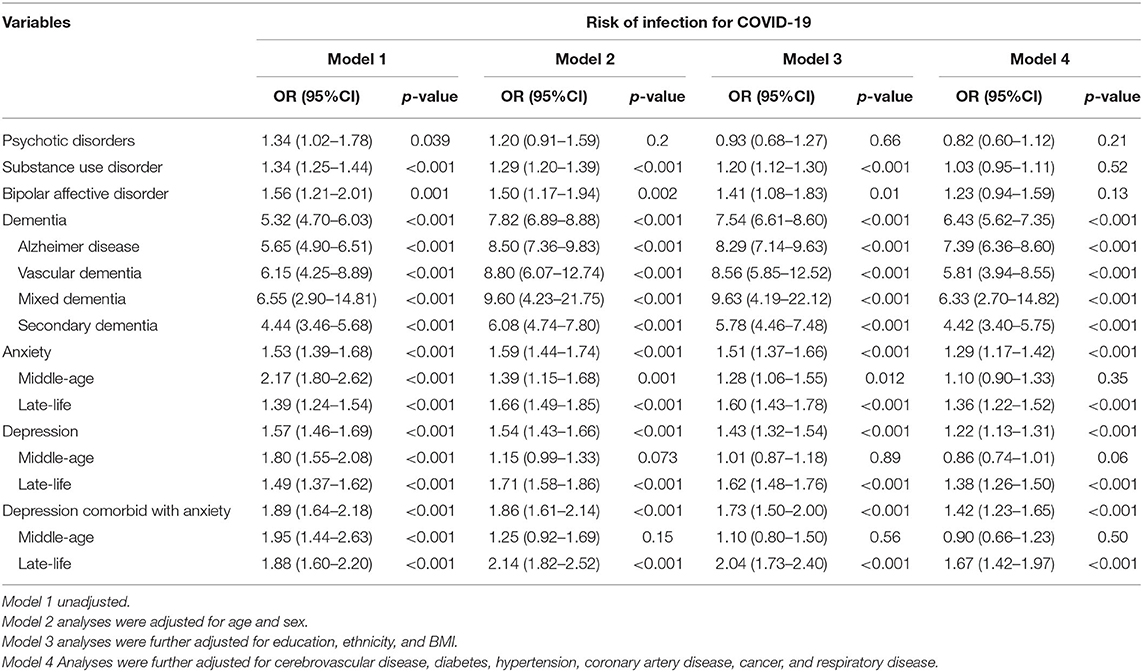
Table 2. Logistic regression analysis of the association between mental disorders and risk of COVID-19.
Subjects with a diagnosis of psychotic disorder did not have a higher risk of COVID-19 infection (p = 0.21) or COVID-19-related death (p = 0.23) than those without a mental disorder (Tables 2, 3). Substance use disorder and bipolar affective disorder were associated with a significantly higher risk of COVID-19 infection compared to absence of a mental disorder after adjusting for age, sex, education level, ethnicity, and BMI in model 3; however, after further adjusting for medical comorbidities (model 4), the higher risk was not significant. In the finally model, subjects with middle-age anxiety, or middle-age depression did not have a higher risk of COVID-19 infection; those with anxiety did not have a higher risk of death from COVID-19; and those with substance use disorder did not have higher risks for COVID-19 infection and associated mortality than subjects without these mental disorders.
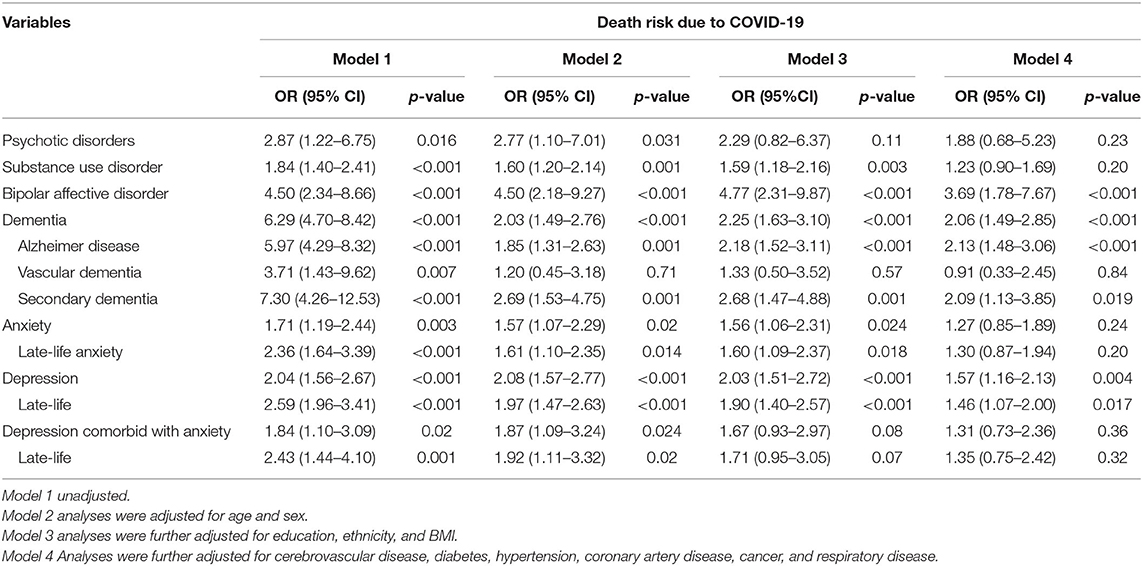
Table 3. Logistic regression analysis of the association between mental disorders and risk of death due to COVID-19.
Subjects with a diagnosis of a dementia (2.06 [1.49, 2.85], p < 0.001) or a depression (1.57 [1.16, 2.13], p = 0.004) had a significantly higher risk of death from COVID-19 than those without a mental disorder. A diagnosis of depression comorbid with anxiety increased probability of COVID-19 infection (depression comorbid with anxiety, 1.42 [1.23, 1.65], p < 0.001; depression, 1.22 [1.13, 1.31], p < 0.001; anxiety, 1.29 [1.17, 1.42], p < 0.001) but not COVID-19–related death of depression comorbid with anxiety (1.31 [0.73, 2.36], p = 0.36) compared to depression (1.57 [1.16, 2.13], p = 0.004) or anxiety (1.27 [0.85, 1.89], p = 0.24) alone.
This study of a large sized UK Biobank cohort yielded three novel findings. First, we document that subject diagnosed with a mental disorder had a significantly higher risk of COVID-19 infection and worse outcome (COVID-19-related death) than those without a mental disorder. Second, among dementia subtypes, Alzheimer disease exhibited the highest risk of COVID-19 infection (7.39-fold risk) and COVID-19–related death (2.13-fold risk). Mixed dementia and vascular dementia did not increase the risk of COVID-19-related death. Third, late-life anxiety increased the risk of COVID-19 infection, and subjects with late-life depression had a higher risk of COVID-19 infection and a worse outcome from COVID-19 than those without late-life depression. Moreover, late-life depression comorbid with anxiety significantly increased the risk of COVID-19 infection compared to either disorder alone. However, middle-aged anxiety, middle-aged depression, and depression comorbid with anxiety were not associated with elevated risks of COVID-19 infection and COVID-19-related death.
The most striking and strongest risk factors for COVID-19 infection and associated death was dementia. In particular, subjects with Alzheimer disease had the highest risks of COVID-19 infection and associated mortality among all dementia subtypes. This finding was confirmed by a previous study (17). There are a few possible explanations for this finding. Firstly, SARS-CoV-2 has been detected in the central nervous system of patients with dementia (18) and may cause brain damage and dysfunction (19). Patients with severe neurological dysfunction and injury are more likely to develop pulmonary diseases that further worsen clinical outcomes, in what is known as the brain-lung-brain axis theory (20). Secondly, the risk genotype for dementia was shown to predict the severity of COVID-19 (21) and risk of COVID-19–related death (22). Thirdly, patients with dementia often require the support of others to communicate their needs; however, the COVID-19 pandemic has reduced the availability of social support services for these patients (23).
Our results also suggest that anxiety and depression were only risk factors in subjects diagnosed with these disorders in late-life but not in middle age. The negative effects of anxiety and depression on immunity are not fully understood. Age is a known risk factor for COVID-19 infection (24). The immune system undergoes numerous age-related changes in a process known as immune senescence (25); we speculated that this is the reason for the higher risks of COVID-19 infection and associated mortality in late-life anxiety and late-life depression relative to middle-aged anxiety and middle-aged depression. Late-life depression has been linked to an elevated risk of respiratory conditions (26) and is a risk factor for or early symptom of dementia (27), but not at younger ages (28). These findings may also explain why anxiety and depression were found to be risk factors for COVID-19 infection and associated mortality only in subjects diagnosed at older ages.
The strengths of this study are concerning the COVID-19 risk and associated mortality for dementia subtypes and age stratification for depression and anxiety with a large sized cohort. However, there are several limitations that should be addressed. First, subjects in the UK Biobank have a restricted age range, and therefore our data could not represent the whole population. Second, individuals identified with positive COVID-19 tests from the UK Biobank cohort may represent the hospitalized and severe cases, which might limit the generalization. Third, subjects who did not undergo COVID-19 testing were deemed to have a negative COVID-19 test result, and we did not know if some subjects were tested but not captured in our dataset. Fourth, some medical co-morbidities may not be listed in the hospital diagnosis, and therefore the number of reported medical comorbidities may be lower than the actual number.
In conclusion, our findings indicate that public health measures for COVID-19 such as vaccinations should prioritize individuals with mental disorders, especially those with both COVID-19 infection and dementia or depression. Future studies should explore the risk factors for COVID-19 in individuals with late-life-related diseases (e.g., dementia), given the increasing prevalence of these disorders in the global population.
Publicly available datasets were analyzed in this study. This data can be found here: UKBIOBANK.
The studies involving human participants were reviewed and approved by ethical approval was obtained from the North West Multi-Centre Research Ethics Committee (REC reference: 16/NW/0274). The patients/participants provided their written informed consent to participate in this study.
X-jD and YW had the idea for and designed this study, had full access to all the data in this study, take responsibility for the integrity of the data and the accuracy of the data analysis, critically revised the manuscript for important intellectual content and gave final approval for the version to be published, drafted the paper, and did the analysis. YW, YY, LR, YS, and WT takes responsibility for double check of the data analysis. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately resolved.
This work was supported by National Natural Science Foundation of China (Grant No. 81701678), China Postdoctoral Science Foundation (Grant No. 2020M670052), Guangdong Basic and Applied Basic Research Foundation (Grant No. 2020A1515011469), and Sanming Project of Medicine in Shenzhen (Grant No. SZSM201812052).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. To KK, Tsang OT, Leung WS, Tam AR, Wu TC, Lung DC, et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis. (2020) 20:565–74. doi: 10.1016/S1473-3099(20)30196-1
2. To KK, Hung IF, Ip JD, Chu AW, Chan WM, Tam AR, et al. COVID-19 re-infection by a phylogenetically distinct SARS-coronavirus-2 strain confirmed by whole genome sequencing. Clin Infect Dis. (2020). doi: 10.1093/cid/ciaa1275. [Epub ahead of print].
3. Rodgers M, Dalton J, Harden M, Street A, Parker G, Eastwood A. Integrated care to address the physical health needs of people with severe mental illness: a mapping review of the recent evidence on barriers, facilitators and evaluations. Int J Integr Care. (2018) 18:9. doi: 10.5334/ijic.2605
4. Yao H, Chen JH, Xu YF. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry. (2020) 7:e21. doi: 10.1016/S2215-0366(20)30090-0
5. Sartorious N. Comorbidity of mental and physical diseases: a main challenge for medicine of the 21st century. Shanghai Arch Psychiatry. (2013) 25:68–9. doi: 10.3969/j.issn.1002-0829.2013.02.002
6. Minihan E, Gavin B, Kelly BD, McNicholas F. Covid-19, mental health and psychological first aid. Ir J Psychol Med. (2020) 37:259–63. doi: 10.1017/ipm.2020.41
7. Glaser R, Kiecolt-Glaser JK. Stress-induced immune dysfunction: implications for health. Nat Rev Immunol. (2005) 5:243–51. doi: 10.1038/nri1571
8. Kelly BD. Coronavirus disease: challenges for psychiatry. Br J Psychiatry. (2020) 217:352–3. doi: 10.1192/bjp.2020.86
9. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
10. Lu W, Wang H, Lin Y, Li L. Psychological status of medical workforce during the COVID-19 pandemic: a cross-sectional study. Psychiatry Res. (2020) 288:112936. doi: 10.1016/j.psychres.2020.112936
11. Petrilli CM, Jones SA, Yang J, Rajagopalan H, O'Donnell LF, Chernyak Y, et al. Factors associated with hospitalization and critical illness among 4,103 patients with COVID-19 disease in New York City. medRxiv [preprint]. (2020). doi: 10.1101/2020.04.08.20057794
12. Kuo CL, Pilling LC, Atkins JC, Masoli J, Delgado J, Tignanelli C, et al. COVID-19 severity is predicted by earlier evidence of accelerated aging. medRxiv [preprint]. (2020). doi: 10.1101/2020.07.10.20147777
13. Team CCR, Bialek SR, Boundy EO, Bowen VB, Chow NA, Cohn AC, et al. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) — United States, February 12–March 16, 2020. Morb Mort Weekly Rep. (2020). 69: 343–6. doi: 10.15585/mmwr.mm6912e2
14. Li L, Li F, Fortunati F, Krystal JH. Association of a prior psychiatric diagnosis with mortality among hospitalized patients with coronavirus disease 2019. (COVID-19) infection. JAMA Netw Open. (2020). 3:e2023282. doi: 10.1001/jamanetworkopen.2020.23282
15. Nemani K, Li C, Olfson M, Blessing EM, Razavian N, Chen J, et al. Association of psychiatric disorders with mortality among patients with COVID-19. JAMA Psychiatry. (2021) 78:380–6. doi: 10.1001/jamapsychiatry.2020.4442
16. Wang Q, Xu R, Volkow ND. Increased risk of COVID-19 infection and mortality in people with mental disorders: analysis from electronic health records in the United States. World Psychiatry. (2021) 20:124–30. doi: 10.1002/wps.20806
17. Yu Y, Travaglio M, Popovic R, Leal NS, Martins LM. Alzheimer's and Parkinson's diseases predict different COVID-19 outcomes: a UK Biobank study. Geriatrics. (2021) 6:10. doi: 10.3390/geriatrics6010010
18. Matías-Guiu J, Gomez-Pinedo U, Montero-Escribano P, Gomez-Iglesias P, Porta-Etessam J, Matias-Guiu JA. Should we expect neurological symptoms in the SARS-CoV-2 epidemic? Neurología. (2020) 35:170–5. doi: 10.1016/j.nrleng.2020.03.002
19. Li YC, Bai WZ, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol. (2020) 92:552–5. doi: 10.1002/jmv.25728
20. Stevens R, Puybasset L. The brain-lung-brain axis. Intens Care Med. (2011) 37:1054–6. doi: 10.1007/s00134-011-2233-1
21. Kuo CL, Pilling LC, Atkins JL, Masoli JAH, Delgado J, Kuchel GA, et al. APOE e4 genotype predicts severe COVID-19 in the UK Biobank community cohort. J Gerontol A Biol Sci Med Sci. (2020) 75:2231–2. doi: 10.1093/gerona/glaa131
22. Kuo CL, Pilling LC, Atkins JL, Masoli JAH, Delgado J, Kuchel GA, et al. ApoE e4e4 genotype and mortality with COVID-19 in UK Biobank. J Gerontol A Biol Sci Med Sci. (2020) 75:1801–3. doi: 10.1093/gerona/glaa169
23. Giebel C, Cannon J, Hanna K, Butchard S, Eley R, Gaughan A, et al. Impact of COVID-19 related social support service closures on people with dementia and unpaid carers: a qualitative study. Aging Mental Health. (2020) 25:1281–8. doi: 10.1080/13607863.2020.1822292
24. Pan A, Liu L, Wang C, Guo H, Hao X, Wang Q, et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA. (2020) 323:1915–23. doi: 10.1001/jama.2020.6130
25. Nikolich-Zugich J. The twilight of immunity: emerging concepts in aging of the immune system. Nat Immunol. (2018) 19:10–9. doi: 10.1038/s41590-017-0006-x
26. Agustini B, Lotfaliany M, Woods RL, McNeil JJ, Nelson MR, Shah RC, et al. Patterns of association between depressive symptoms and chronic medical morbidities in older adults. J Am Geriatr Soc. (2020) 68:1834–41. doi: 10.1111/jgs.16468
27. Osorio R, Gumb T, Pomara N. Soluble amyloid-β levels and late-life depression. Cur Pharmaceut Des. (2014) 20:2547–54. doi: 10.2174/13816128113199990502
Keywords: COVID-19, mental disorders, SARS-CoV-2, dementia, Parkinson's disease, late-life
Citation: Wang Y, Yang Y, Ren L, Shao Y, Tao W and Dai X-j (2021) Preexisting Mental Disorders Increase the Risk of COVID-19 Infection and Associated Mortality. Front. Public Health 9:684112. doi: 10.3389/fpubh.2021.684112
Received: 29 March 2021; Accepted: 12 July 2021;
Published: 09 August 2021.
Edited by:
Giorgio Di Lorenzo, University of Rome Tor Vergata, ItalyReviewed by:
Yizhou Yu, University of Cambridge, United KingdomCopyright © 2021 Wang, Yang, Ren, Shao, Tao and Dai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xi-jian Dai, ZGFpeGpkb2N0b3JAMTI2LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.