
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Public Health , 22 June 2021
Sec. Public Mental Health
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.666753
 Sabuj Kanti Mistry1,2*
Sabuj Kanti Mistry1,2* Ben Harris-Roxas2
Ben Harris-Roxas2 Uday Narayan Yadav2
Uday Narayan Yadav2 Sadia Shabnam3
Sadia Shabnam3 Lal Bahadur Rawal4Mark F. Harris2
Lal Bahadur Rawal4Mark F. Harris2The COVID-19 pandemic has been the most challenging public health issue which not only affected the physical health of the global population but also aggravated the mental health conditions such as stress, anxiety, fear, depression and anger. While mental health services are seriously hampered amid this COVID-19 pandemic, health services, particularly those of Low- and Middle- Income Countries (LMICs) are looking for alternatives to provide psychosocial support to the people amid this COVID-19 and beyond. Community Health Workers (CHWs) are an integral part of the health systems in many LMICs and played significant roles such as health education, contact tracing, isolation and mobilization during past emergencies and amid COVID-19 in many LMICs. However, despite their potentials in providing psychosocial support to the people amid this COVID-19 pandemic, they have been underutilized in most health systems in LMICs. The CHWs can be effectively engaged to provide psychosocial support at the community level. Engaging them can also be cost-saving as they are already in place and may cost less compared to other health professionals. However, they need training and supervision and their safety and security needs to be protected during this COVID-19. While many LMICs have mental health policies but their enactment is limited due to the fragility of health systems and limited health care resources. CHWs can contribute in this regard and help to address the psychosocial vulnerabilities of affected population in LMICs during COVID-19 and beyond.
The COVID-19 pandemic has been the most challenging global public health issue so far in this century. With the notable exception of climate change (1), there have been no events that have affected nearly every person on the planet in the same way COVID has.
The disease continues to spread across the world, with over 85 million confirmed cases with over 1.8 million deaths up to 7th January 2021 (2). The advent of COVID-19 has not only seriously hampered the physical well-being of a vast majority of global people but also aggravated the mental health conditions of many people. The unplanned lockdown and isolation imposed due to COVID-19 and subsequent difficulty in accessing food, health care, medication, and psychological support have exacerbated anxiety, depression, post-traumatic stress disorder among people from all age group (3, 4).
Historically, the mental health and well-being of the population has been disrupted due to the large-scale outbreaks and pandemics. For example, during the H1N1 influenza virus outbreak in 2009, anxiety among the UK's general population increased by 10–30% (5). Similarly, during the severe acute respiratory syndrome (SARS) epidemic in 2002–2004, psychiatric morbidities, depression, and stress disorder increased (6). During the Ebola outbreak, in 2013–2016 in Guinea, Liberia, and Sierra Leone, the psychosocial well-being of the people was seriously hampered (7). It is not surprising that - stress, anxiety, depressive symptoms, insomnia, denial, anger, and fear are associated with the COVID-19, (8, 9) even amongst those who have not been infected.
Mental health services have also been seriously disrupted during the COVID-19 pandemic worldwide. A recent survey carried out in 130 countries reported that mental health services were seriously hampered during the pandemic (10). Several researchers pointed the challenges to mental health services during this pandemic and suggested for alternative ways to provide psychosocial support services (11). Telemedicine or online health services have been used to some extent as an alternative way to provide healthcare services (12). Yet, people from LMICs with limited access to the internet are largely unable to avail themselves of these services (13).
The World Health Organization (WHO) defines “community health worker” as an umbrella term which encompasses a variety of community health aides working in their own community. According to WHO, “community health workers should be members of the communities where they work, should be selected by the communities, should be answerable to the communities for their activities, should be supported by the health system but not necessarily a part of its organization, and have shorter training than professional workers” (14). The American Public Health Association (APHA) defines community health workers more expansively as, “a frontline public health worker who is a trusted member of and/or has an unusually close understanding of the community served. This trusting relationship enables the CHW to serve as a liaison/link/intermediary between health/social services and the community to facilitate access to services and improve the quality and cultural competence of service delivery” (15).
Globally, CHWs are considered as an integral part of the health care system in achieving universal health coverage for all individuals (16, 17). The most recent estimates suggest that there are around five million CHWs currently working worldwide. The WHO have forecasted a global shortage of 18 million trained health professionals by 2030 (18). CHWs have been shown to be a cost-saving way to complement the shortages of health professionals in implementing community-based health care programs, as well as representing a potentially scalable workforce (19). The concept of CHWs primarily evolved in LMICs during the 1970s (20). Further, in the Alma Ata declaration (1978), the WHO explicitly pointed to the importance of CHWs in providing effective primary health care (PHC), by ensuring access to basic health services for the underserved that address local health needs and engage the community (21). Over the last decade many CHW-led programs in LMICs have been restructured to delivering primary health care services for infectious diseases as well as services for prevention and management of non-communicable diseases (22). Some of the most well-known, large-scale and effective CHW programs in LMICs are gentes Comunitários de Saúde in Brazil, Sasthya Sebika and Sasthya Kormis of BRAC, Female Community Health Volunteer (FCHV) in Nepal, Lady Health Worker in Pakistan, and Accredited Social Health Activists (ASHAs) in India (20). There has also been growing attention in recent years regarding the potential contribution of CHWs in high-income countries in reducing health care inequalities as well (23, 24).
CHWs were trained and deployed throughout the world to address the crisis in healthcare workforce in the 1970s, especially for underserved communities whose healthcare needs were not addressed by the formal healthcare systems (25). The role of CHWs can be varied based on the need of the communities they served (26). CHWs play an important role in addressing health care inequalities by assisting people to access services offered by the formal health care system (22). Several studies have identified different roles of CHWs including health assessment (27) and facilitating treatment (28), health care navigation (29), health education (30), psychosocial support (31) and data collection (32). CHW interventions were previously focused mostly on maternal child health (33, 34), prevention of malnutrition (35) and control of infectious disease such as HIV/AIDS and tuberculosis (35, 36). In recent years, the potential to engage CHWs in the prevention and control of non-communicable diseases in countries of South and South East Asia also has been well-documented (37, 38). Recent research has demonstrated that CHWs are effective in improving the accessibility and acceptability of preventive care and primary health care and providing health education. In these roles they have reduced hospitalization and re-hospitalization particularly for people from disadvantaged communities (39).
Despite strong evidence on the contribution of CHWs at primary health care and community levels, their potential in outbreaks may be under-utilized or overlooked. Several studies (40–42) conducted during previous as well as COVID-19 outbreak pointed out that CHWs were largely underutilized in emergency management and the emergency response failed due largely to not engaging them. While acknowledging the under-utilization of the CHWs at a broader scale in COVID-19 management, Haines et al. also called for training and engaging CHWs to support people in their own homes during this COVID-19 pandemic in UK (43). Peretz et al. also recommended use of CHWs to address the social determinants of health during the COVID-19 pandemic (44).
There is strong evidence supporting the role of CHWs in emergency situations such as humanitarian emergencies and infectious outbreaks when demand for health services increases. BRAC Bangladesh developed the concept of CHWs (Sasthya Sebikas) when there was a diarrhea epidemic in Bangladesh in the 1980s and CHWs played a pivotal role in educating people in terms of prevention and control of diarrhea (45).
It has also been demonstrated during the Ebola outbreak in Guinea, Sierra Leone, and Liberia that CHWs were effective in emergency management through the early identification of cases as well as in pandemic preparedness through proper communication in a culturally appropriate way, community education and mobilization, contribution to surveillance systems, and filling health service gaps (46). Likewise, CHWs enabled Nigeria to quickly treat and isolate cases, thereby helped eradicate the polio from the country (47).
Establishment of a community centric care model of care with CHWs at the center can be effective in managing the COVID-19 pandemic as well as potential future episodes (48, 49). This community centric approach facilitates proactive community-wide services such as rapid testing, contact tracing, promoting isolation and quarantine which are considered crucial in slowing down the spread of COVID-19 (48, 50). CHWs can also be very crucial in providing psychosocial support to the people amid COVID-19 pandemic. In trials carried out in India (51), Uganda (52), Nepal (53) and Pakistan (54), 70% of those cared for by trained CHWs recovered from mental health problems. They have also helped to compensate for critical health workforce shortage during this pandemic, particularly in LMICs (49).
As CHWs are already in touch with the community as their trusted members, they can be engaged to provide psychosocial support to the people who were at increased need due to COVID-19 related stress, anxiety and depression (44, 55). For example, regular home visit is an integral component of the most CHW programs carried out in Bangladesh (56), India (57), Kenya (58), Brazil (59), Pakistan (60) and Nepal (61) (Table 1). Therefore, these CHWs can be trained to provide psychosocial support either face-to- or over telephone (44, 62). Although home visits are limited during this pandemic, CHWs can be the best option who can connect the people to nearby primary health care providers and mental health resources. Moreover, the ethos of CHWs is to empower and engage people in health promotion behaviors, enhance their health literacy in local languages, foster social support, and provide a listening ear (44). Adding to this, CHWs can provide basic mental health support to address stress, anxiety, and depression, which have risen during COVID-19 (63). Figure 1 summarizes potential roles for CHWs in providing psychosocial support.
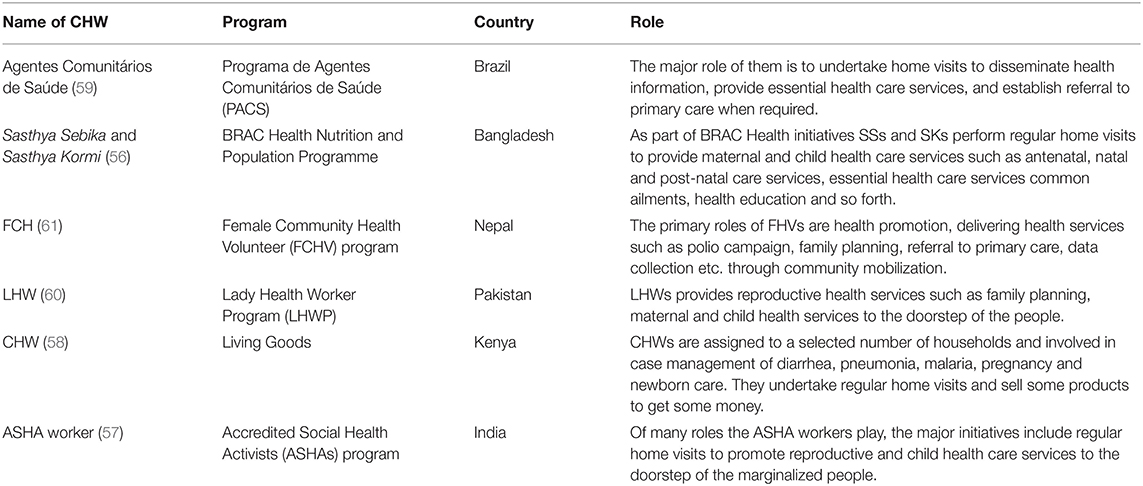
Table 1. Overview of the major global CHW interventions.
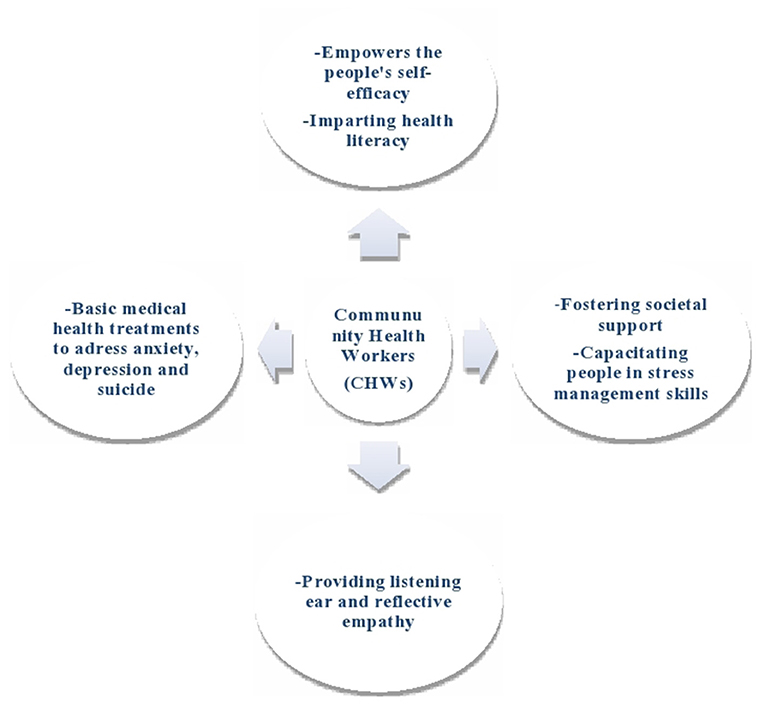
Figure 1. Potential roles of CHWs in providing psychosocial supports.
Incorporating CHWs in providing psychosocial support can be cost saving. They have already been demonstrated to be a less expensive alternative compared to other health professionals (64). On the other hand, little extra effort is needed to recruit or engage them as many of them are already employed casually or part time. For example, a study conducted by Fiedler et al. (65) in Honduras found that CHW programme cost only 11% of the facility-based care. Likewise, Datiko and Lindtjørn (66) found that involving Health Extension Workers (HEWs) in TB treatment was a cost-effective alternative to health facility delivery. Surprisingly, despite their potential to provide psychosocial support to the people at the community level in LMICs, particularly during this overwhelming situation, CHWs have been underutilized in this role (67, 68).
Cultural factors may stop people presenting with psychological conditions or mask them as somatised physical symptoms. CHWs are well-placed to address this because they understand the cultural belief and practices of their communities. However, they need specific training in how to address possible conflicts between cultural beliefs and western health care (69).
CHWs need to be equipped with adequate training before they are engaged in providing psychosocial support. They need to be trained in assessment, communication skills, problem solving, professional responsibilities and boundaries, as well as stress and emotion management strategies. Previous research has demonstrated that short duration training for up to 2 weeks produced good results (56, 70, 71). For example, Barnett et al. (71) found that a 5-day training resulted in improved ability of the CHWs in identification and management of mental health issues among the patients. Alternative models of delivery such as e-learning may be of value in the context of COVID-19 (72). Digital technologies can be effectively employed to conduct training and provide supervision remotely (49, 73). Also, digital technology can be one of the less expensive ways to disseminate the mental health information as the number of people using phones and internet is increasing with an estimate of 84% in LMICs (74).
Management of CHWs requires sustainable support by and integration into local and national health systems, plans and policies. It also requires supportive supervision that solves problems and improves skills. To address most of the mental health problems at the community level, CHWs need to be trained on providing psychosocial support for basic mental illnesses such as anxiety, fear, and depression. One study (75) also reported that poor supervision led to compromised CHW performance. Also, they need to be well-trained in navigation for the people with moderate or severe mental health illness to the nearest health service.
While the importance of CHWs' engagement in effective COVID-19 management has been well-documented, it is also essential that several precautions are taken before scaling up CHWs roles in COVID 19 management. CHWs should be provided with appropriate and adequate personal protective equipment (PPE) (76, 77) and needs to be equipped with sufficient and appropriate training and supervision for community sensitization activities as well as their own protection for effective service delivery (78, 79). Availability of PPE and adequate training can make the CHWs more confident of delivering the services (80, 81). However, it should be noted that there is scarce of PPE resources in some communities and they need to be appropriately used (82). Of course, the psychosocial support provided by CHWs needs to be monitored by debriefing with supervisors (71). It is also important that CHWs are offered psychosocial support, non-performance-based allowances, additional transport allowances, childcare support and so forth to ensure their active participation and reduced stigmatization and isolation (83). Safety from any potential violence in the community also need to be ensured when home visits are being done by CHWs.
Despite the high prevalence of mental health disorders in LMICs, compared to high-income countries, it has received fairly little attention in many LMICs (84). Recognizing the high burden of mental health disorders, various LMICs have passed policies and laws, but the implementation of these seems challenging because of fragility of the health systems, inadequate human resources for mental health, and ineffective decision making by health leaders (85). As the COVID-19 has aggravated mental health conditions, it is very important that decision makers and implementors consider the importance of engaging CHWs into the policy discourse. More importantly, integrating mental health services into primary health care through involving and engaging CHWs can help extend the capacity of the workforce to address mental health issues in LMICs. A mixed funding strategy may be required to achieve this, including recognition that some activities may not be funded (86). It is also important to consider CHW roles in relation to other health workforce and integrate CHW intervention into the general health and community system (87).
The COVID-19 pandemic has made a negative impact on the mental health in LMICs. As a result, health services are looking for alternative ways to tackle the issue. Employing CHWs, training and support them on mental health issues can be a cost saving and effective approach to provide psychosocial support to the people at the local level in LMICs within their fragile health systems.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
SM conceived and designed the study. SM, BH-R, UY, SS, and LR contributed to the first draft of the manuscript. MH commented extensively on the first draft and edited the entire paper. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. IPCC. Global Warming of 1.5°C: An IPCC Special Report on the impacts of global warming of 1.5°C above Pre-industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty. Geneva: Intergovernmental Panel on Climate Change (2015).
3. Singh S, Roy MD, Sinha CPTMK, Parveen CPTMS, Sharma CPTG, Joshi CPTG. Impact of COVID-19 and lockdown on mental health of children and adolescents: a narrative review with recommendations. Psychiatry Res. (2020) 293:113429. doi: 10.1016/j.psychres.2020.113429
4. Das S. Mental health and psychosocial aspects of COVID-19 in India: the challenges and responses. J Health Manag. (2020) 22:197–205. doi: 10.1177/0972063420935544
5. Rubin GJ, Potts HWW, Michie S. The impact of communications about swine flu (influenza A H1N1v) on public responses to the outbreak: results from 36 national telephone surveys in the UK. Health Technol Assess. (2010) 14:183–266. doi: 10.3310/hta14340-03
6. Sim K, Chan YH, Chong PN, Chua HC, Soon SW. Psychosocial and coping responses within the community health care setting towards a national outbreak of an infectious disease. J Psychosomat Res. (2010) 68:195–202. doi: 10.1016/j.jpsychores.2009.04.004
7. Van Bortel T, Basnayake A, Wurie F, Jambai M, Koroma AS, Muana AT, et al. Psychosocial effects of an Ebola outbreak at individual, community and international levels. Bull World Health Org. (2016) 94:210. doi: 10.2471/BLT.15.158543
8. Torales J, O'Higgins M, Castaldelli-Maia JM, Ventriglio A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int J Soc Psychiatry. (2020) 66:317–20. doi: 10.1177/0020764020915212
9. Holmes EA, O'Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. The Lancet Psychiatry. (2020) 7:547–60. doi: 10.1016/S2215-0366(20)30168-1
11. Li W, Yang Y, Liu Z-H, Zhao Y-J, Zhang Q, Zhang L, et al. Progression of mental health services during the COVID-19 Outbreak in China. Int J Biol Sci. (2020) 16:1732–8. doi: 10.7150/ijbs.45120
12. Hasan M, Hassan MN, Khan MSI, Al Banna MH. Prevalence and determinants of early initiation of breastfeeding among mothers in Dhaka City, Bangladesh: a Cross-sectional Study. SN Compr Clin Med. (2020) 14:1–7. doi: 10.1371/journal.pone.0220224
13. World Economic Forum. Coronavirus has Exposed the Digital Divide Like Never Before. Geneva (2020).
14. World Health Organization. Strengthening the Performance of Community Health Workers in Primary Health Care: Report of a WHO Study Group [meeting held in Geneva from 2 to 9 December 1987]. Geneva (1989).
16. Mishra SR, Neupane D, Preen D, Kallestrup P, Perry HB. Mitigation of non-communicable diseases in developing countries with community health workers. Glob Health. (2015) 11:43. doi: 10.1186/s12992-015-0129-5
17. Schaaf M, Fox J, Topp SM, Warthin C, Freedman LP, Robinson RS. Community health workers and accountability: reflections from an international “think-in.” Int J Equity Health. (2018) 17:66. doi: 10.1186/s12939-018-0781-5
18. O'Donovan J, O'Donovan C, Kuhn I, Sachs SE, Winters N. Ongoing training of community health workers in low-income and middle-income countries: a systematic scoping review of the literature. BMJ Open. (2018) 8:e021467. doi: 10.1136/bmjopen-2017-021467
19. Long H, Huang W, Zheng P, Li J, Tao S, Tang S. Barriers and facilitators of engaging community health workers in non-communicable disease (NCD) prevention and control in china: a systematic review (2006–2016). Int J Environ Res Public Health. (2018) 15:2378. doi: 10.3390/ijerph15112378
20. Perry HB, Zulliger R, Rogers MM. Community health workers in low-, middle-, and high-income countries: an overview of their history, recent evolution, current effectiveness. Ann Rev Public Health. (2014) 35:399–21. doi: 10.1146/annurev-publhealth-032013-182354
21. World Health Organization. Primary Health Care: report of the International Conference on Primary Health Care Alma-Ata, USSR. Geneva: World Health Organization (1978).
22. Scott K, Beckham SW, Gross M, Pariyo G, Rao KD, Cometto G, et al. What do we know about community-based health worker programs? A systematic review of existing reviews on community health workers. Hum Resour Health. (2018) 16:39. doi: 10.1186/s12960-018-0304-x
23. Najafizada SA, Bourgeault IL, Labonte R, Packer C, Torres S. Community health workers in Canada and other high-income countries: a scoping review and research gaps. Can J Public Health. (2015) 106:e157–64. doi: 10.17269/CJPH.106.4747
24. Necochea E, Badlani M, Bossemeyer D. Systematic Management of Human Resources for Health: An Introduction for Health Managers. Baltimore, MD: The Johns Hopkins University (2013).
25. Alam K, Oliveras E. Retention of female volunteer community health workers in Dhaka urban slums: a prospective cohort study. Human Resour Health. (2014) 12:29. doi: 10.1186/1478-4491-12-29
26. Cherrington A, Ayala GX, Elder JP, Arredondo EM, Fouad M, Scarinci I. Recognizing the diverse roles of community health workers in the elimination of health disparities: from paid staff to volunteers. Ethnicity Dis. (2010) 20:189. doi: 10.13016/odom-fok7
27. Bemelmans M, Baert S, Negussie E, Bygrave H, Biot M, Jamet C, et al. Sustaining the future of HIV counselling to reach 90-90-90: a regional country analysis. J Int AIDS Soc. (2016) 19:20751. doi: 10.7448/IAS.19.1.20751
28. Kredo T, Adeniyi FB, Bateganya M, Pienaar ED. Task shifting from doctors to non-doctors for initiation and maintenance of antiretroviral therapy. Cochrane Database Syst Rev. (2014) 1:1–51. doi: 10.1002/14651858.CD007331.pub3
29. Percac-Lima S, Ashburner JM, Zai AH, Chang Y, Oo SA, Guimaraes E. Patient navigation for comprehensive cancer screening in high-risk patients using a population-based health information technology system: a randomized clinical trial. JAMA Int Med. (2016) 176:930–7. doi: 10.1001/jamainternmed.2016.0841
30. Kangovi S, Mitra N, Grande D, White ML, McCollum S, Sellman J. Patient-centered community health worker intervention to improve posthospital outcomes: a randomized clinical trial. JAMA Int Med. (2014) 174:535–43. doi: 10.1001/jamainternmed.2013.14327
31. Lassi ZS, Bhutta ZA. Community-based intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. Cochrane Database Syst Rev. (2015). doi: 10.1002/14651858.CD007754.pub3
32. Agarwal S, Perry HB, Long LA, Labrique AB. Evidence on feasibility and effective use of mH ealth strategies by frontline health workers in developing countries: systematic review. Trop Med Int Health. (2015) 20:1003–14. doi: 10.1111/tmi.12525
33. Haines A, Sanders D, Lehmann U, Rowe AK, Lawn JE, Jan S. Achieving child survival goals: potential contribution of community health workers. Lancet. (2007) 369:2121–31. doi: 10.1016/S0140-6736(07)60325-0
34. Gilmore B, McAuliffe E. Effectiveness of community health workers delivering preventive interventions for maternal and child health in low-and middle-income countries: a systematic review. BMC Public Health. (2013) 13:847. doi: 10.1186/1471-2458-13-847
35. Hall JJM. Effective community-based interventions to improve exclusive breast feeding at four to six months in low-and low–middle-income countries: a systematic review of randomised controlled trials. Midwifery. (2011) 27:497–502. doi: 10.1016/j.midw.2010.03.011
36. Boyce MR, O'Meara W. Use of malaria RDTs in various health contexts across sub-Saharan Africa: a systematic review. BMC Public Health. (2017) 17:470. doi: 10.1186/s12889-017-4398-1
37. Abdullah AS, Rawal LB, Choudhury SR, Baral S, Jiang L, Sha T, et al. Use of Community Health Workers to Manage and Prevent Noncommunicable Diseases: Policy Options Based on the Findings of the Coach Study. New Delhi: World Health Organization Regional Office for South-East Asia (2019). 1–68 p.
38. Long H, Ma Z, Hanh TTD, Minh HV, Rawal LB, Urmi DS, et al. Engaging village health workers in non-communicable disease (NCD) prevention and control in Vietnam: a qualitative study. Global Public Health. (2020) 15:611–25. doi: 10.1080/17441692.2019.1678660
39. Sharma N, Harris E, Lloyd J, Mistry SK, Harris M. Community health workers involvement in preventative care in primary healthcare: a systematic scoping review. BMJ Open. (2019) 9:1–23. doi: 10.1136/bmjopen-2019-031666
40. Miller NP, Milsom P, Johnson G, Bedford J, Kapeu AS, Diallo AO, et al. Community health workers during the Ebola outbreak in Guinea, Liberia, Sierra Leone. J Global Health. (2018) 8:1–17. doi: 10.7189/jogh-08-020601
41. Think Global Health. Without Community Health Workers, the Global COVID-19 Response Could Fail (2021).
42. Palafox B, Renedo A, Lasco G, Palileo-Villanueva L, Balabanova D, McKee M. Maintaining population health in low-and middle-income countries during the Covid-19 pandemic: why we should be investing in Community Health Workers. Trop Med Int Health. (2021) 26:20–2. doi: 10.1111/tmi.13498
43. Haines A, de Barros EF, Berlin A, Heymann DL, Harris MJ. National UK programme of community health workers for COVID-19 response. Lancet. (2020) 395:1173–5. doi: 10.1016/S0140-6736(20)30735-2
44. Peretz PJ, Islam N, Matiz LA. Community health workers and Covid-19—addressing social determinants of health in times of crisis and beyond. New Engl J Med. (2020) 383:e108. doi: 10.1056/NEJMp2022641
45. Chowdhury AMR, Karim F, Sarkar SK, Cash RA, Bhuiya A. The status of ORT in Bangladesh: how widely is it used? Health Policy Plann. (1997) 12:58–66. doi: 10.1093/heapol/12.1.58
46. Perry HB, Dhillon RS, Liu A, Chitnis K, Panjabi R, Palazuelos D, et al. Community health worker programmes after the 2013–2016 Ebola outbreak. Bull World Health Org. (2016) 94:551. doi: 10.2471/BLT.15.164020
47. Lewis J, LeBan K, Solomon R, Bisrat F, Usman S, Arale A. The critical role and evaluation of community mobilizers in polio eradication in remote settings in Africa and Asia. Global Health: Sci Pract. (2020) 8:396–412. doi: 10.9745/GHSP-D-20-00024
48. Goldfield NI, Crittenden R, Fox D, McDonough J, Nichols L, Rosenthal EL. COVID-19 crisis creates opportunities for community-centered population health: community health workers: at the center. J Ambul Care Manag. (2020) 43:184–90. doi: 10.1097/JAC.0000000000000337
49. Ballard M, Bancroft E, Nesbit J, Johnson A, Holeman I, Foth J, et al. Prioritising the role of community health workers in the COVID-19 response. BMJ Global Health. (2020) 5:e002550. doi: 10.1136/bmjgh-2020-002550
50. Nacoti M, Ciocca A, Giupponi A, Brambillasca P, Lussana F, Pisano M, et al. At the epicenter of the Covid-19 pandemic and humanitarian crises in Italy: changing perspectives on preparation and mitigation. NEJM Catal Innovat Care Deliv. (2020) 1:1–5. doi: 10.1056/CAT.20.0080
51. Patel V, Weiss HA, Chowdhary N, Naik S, Pednekar S, Chatterjee S, et al. Lay health worker led intervention for depressive and anxiety disorders in India: impact on clinical and disability outcomes over 12 months. Br J Psychiatry. (2011) 199:459–66. doi: 10.1192/bjp.bp.111.092155
52. Bolton P, Bass J, Neugebauer R, Verdeli H, Clougherty KF, Wickramaratne P, et al. Group interpersonal psychotherapy for depression in rural Uganda: a randomized controlled trial. JAMA. (2003) 289:3117–24. doi: 10.1001/jama.289.23.3117
53. Markkula N, Lehti V, Adhikari P, Peña S, Heliste J, Mikkonen E, et al. Effectiveness of non-medical health worker-led counselling on psychological distress: a randomized controlled trial in rural Nepal. Global Mental Health. (2019) 6:1–11. doi: 10.1017/gmh.2019.15
54. Rahman A, Malik A, Sikander S, Roberts C, Creed F. Cognitive behaviour therapy-based intervention by community health workers for mothers with depression and their infants in rural Pakistan: a cluster-randomised controlled trial. Lancet. (2008) 372:902–9. doi: 10.1016/S0140-6736(08)61400-2
55. Rahman MS, Rahman MA, Afroze L, Islam SMS. Unmet needs for mental care services for older people in Bangladesh during the COVID-19 pandemic. General Psychiatry. (2020) 33:e100294. doi: 10.1136/gpsych-2020-100294
56. Rahman M, Jhohura FT, Mistry SK, Chowdhury TR, Ishaque T, Shah R, et al. Assessing community based improved maternal neonatal child survival (IMNCS) program in rural Bangladesh. PLoS ONE. (2015) 10:e0136898. doi: 10.1371/journal.pone.0136898
57. Kohli C, Kishore J, Sharma S, Nayak H. Knowledge and practice of Accredited Social Health Activists for maternal healthcare delivery in Delhi. J Fam Med Prim Care. (2015) 4:359. doi: 10.4103/2249-4863.161317
58. Taylor CA, Lilford RJ, Wroe E, Griffiths F, Ngechu R. The predictive validity of the Living Goods selection tools for community health workers in Kenya: cohort study. BMC Health Serv Res. (2018) 18:803. doi: 10.1186/s12913-018-3620-x
59. Melo TE, Maia PF, Valente EP, Vezzini F, Tamburlini G. Effectiveness of an action-oriented educational intervention in ensuring long term improvement of knowledge, attitudes and practices of community health workers in maternal and infant health: a randomized controlled study. BMC Med Educ. (2018) 18:224. doi: 10.1186/s12909-018-1332-x
60. Mumtaz Z, Salway S, Nykiforuk C, Bhatti A, Ataullahjan A, Ayyalasomayajula B. The role of social geography on Lady Health Workers' mobility and effectiveness in Pakistan. Soc Sci Med. (2013) 91:48–57. doi: 10.1016/j.socscimed.2013.05.007
61. Kandel N, Lamichhane J. Correspondence female health volunteers of Nepal: the backbone of health care. Lancet. (2019) 393:e19–20. doi: 10.1016/S0140-6736(19)30207-7
62. Rahman A, Naslund JA, Betancourt TS, Black CJ, Bhan A, Byansi W, et al. The NIMH global mental health research community and COVID-19. Lancet Psychiatry. (2020) 7:834–6. doi: 10.1016/S2215-0366(20)30347-3
63. Waters R. Community Workers Lend Human Connection To COVID-19 Response. Health Aff. (2020) 39:1–6. doi: 10.1377/hlthaff.2020.00836
64. Vaughan K, Kok MC, Witter S, Dieleman M. Costs and cost-effectiveness of community health workers: evidence from a literature review. Human Resour Health. (2015) 13:71. doi: 10.1186/s12960-015-0070-y
65. Fiedler JL, Villalobos CA, De Mattos AC. An activity-based cost analysis of the Honduras community-based, integrated child care (AIN-C) programme. Health Policy Plann. (2008) 23:408–27. doi: 10.1093/heapol/czn018
66. Datiko DG, Lindtjørn B. Cost and cost-effectiveness of smear-positive tuberculosis treatment by Health Extension Workers in Southern Ethiopia: a community randomized trial. PLoS ONE. (2010) 5:1–7. doi: 10.1371/journal.pone.0009158
67. Jack HE, Myers B, Regenauer KS, Magidson JF. Mutual Capacity Building to Reduce the Behavioral Health Treatment Gap Globally. Administr Policy Mental Health Mental Health Serv Res. (2020) 47:497–500. doi: 10.1007/s10488-019-00999-y
68. Mutamba BB, van Ginneken N, Paintain LS, Wandiembe S, Schellenberg D. Roles and effectiveness of lay community health workers in the prevention of mental, neurological and substance use disorders in low and middle income countries: a systematic review. BMC Health Serv Res. (2013) 13:1–11. doi: 10.1186/1472-6963-13-412
69. Armstrong G, Kermode M, Raja S, Suja S, Chandra P, Jorm AF. A mental health training program for community health workers in India: impact on knowledge and attitudes. Int J Mental Health Syst. (2011) 5:1–11. doi: 10.1186/1752-4458-5-17
70. Miller PC, Rashida G, Tasneem Z, ul Haque M. The effect of traditional birth attendant training on maternal and neonatal care. Int J Gynecol Obstetr. (2012) 117:148–52. doi: 10.1016/j.ijgo.2011.12.020
71. Barnett ML, Gonzalez A, Miranda J, Chavira DA, Lau AS. Mobilizing community health workers to address mental health disparities for underserved populations: a systematic review. Administr Policy Mental Health Mental Health Serv Res. (2018) 45:195–211. doi: 10.1007/s10488-017-0815-0
73. Vaughan EM, Naik AD, Lewis CM, Foreyt JP, Samson SL, Hyman DJ. Telemedicine training and support for community health workers: improving knowledge of diabetes. Telemed e-Health. (2020) 26:244–50. doi: 10.1089/tmj.2018.0313
74. Pew Research Centre. Internet Seen as Positive Influence on Education but Negative On Morality in Emerging and Developing Nations. Washington, DC (2015).
75. Kok MC, Dieleman M, Taegtmeyer M, Broerse JEW, Kane SS, Ormel H, et al. Which intervention design factors influence performance of community health workers in low-and middle-income countries? A systematic review. Health Policy Plann. (2015) 30:1207–27. doi: 10.1093/heapol/czu126
76. Mahase E. Covid-19: retired doctors could be asked to return to work, says Hancock. Br Med J Publ Group. (2020) 368:1. doi: 10.1136/bmj.m831
77. McMahon SA, Ho LS, Brown H, Miller L, Ansumana R, Kennedy CE. Healthcare providers on the frontlines: a qualitative investigation of the social and emotional impact of delivering health services during Sierra Leone's Ebola epidemic. Health Policy Plann. (2016) 31:1232–9. doi: 10.1093/heapol/czw055
78. Englert EG, Kiwanuka R, Neubauer LC. ‘When I die, let me be the last.'Community health worker perspectives on past Ebola and Marburg outbreaks in Uganda. Global Public Health. (2019) 14:1182–92. doi: 10.1080/17441692.2018.1552306
79. Wurie HR, Samai M, Witter S. Retention of health workers in rural Sierra Leone: findings from life histories. Human Resour Health. (2016) 14:3. doi: 10.1186/s12960-016-0099-6
80. Witter S, Wurie H, Chandiwana P, Namakula J, So S, Alonso-Garbayo A, et al. How do health workers experience and cope with shocks? Learning from four fragile and conflict-affected health systems in Uganda, Sierra Leone, Zimbabwe and Cambodia. Health Policy Plann. (2017) 32:iii3–13. doi: 10.1093/heapol/czx112
81. Bower H, Grass JE, Veltus E, Brault A, Campbell S, Basile AJ, et al. Delivery of an Ebola virus-positive stillborn infant in a rural community health center, Sierra Leone, 2015. Am J Trop Med Hyg. (2016) 94:417–9. doi: 10.4269/ajtmh.15-0619
82. Mahase E. Covid-19: hoarding and misuse of protective gear is jeopardising the response, WHO warns. Br Med J Publ Group. (2020) 368:1. doi: 10.1136/bmj.m869
83. Bhaumik S, Moola S, Tyagi J, Nambiar D, Kakoti M. Community health workers for pandemic response: a rapid evidence synthesis. BMJ Global Health. (2020) 5:e002769. doi: 10.1136/bmjgh-2020-002769
84. Patel V. Mental health in low-and middle-income countries. Br Med Bull. (2007) 81:81–96. doi: 10.1093/bmb/ldm010
85. Hossain MM, Hasan MT, Sultana A, Faizah F. New mental health act in Bangladesh: unfinished agendas. Lancet Psychiatry. (2019) 6:e1. doi: 10.1016/S2215-0366(18)30472-3
86. Singh D, Negin J, Otim M, Orach CG, Cumming R. The effect of payment and incentives on motivation and focus of community health workers: five case studies from low-and middle-income countries. Hum Resour Health. (2015) 13:1–12. doi: 10.1186/s12960-015-0051-1
Keywords: community health workers, psychosocial support, low- and middle- income countries, COVID-19, mental health
Citation: Mistry SK, Harris-Roxas B, Yadav UN, Shabnam S, Rawal LB and Harris MF (2021) Community Health Workers Can Provide Psychosocial Support to the People During COVID-19 and Beyond in Low- and Middle- Income Countries. Front. Public Health 9:666753. doi: 10.3389/fpubh.2021.666753
Received: 15 April 2021; Accepted: 24 May 2021;
Published: 22 June 2021.
Edited by:
Elisa Harumi Kozasa, Hospital Israelita Albert Einstein, BrazilReviewed by:
Renata Lima, Albert Einstein Israelite Hospital, BrazilCopyright © 2021 Mistry, Harris-Roxas, Yadav, Shabnam, Rawal and Harris. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabuj Kanti Mistry, c21pdHJhNDExQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.