 Lissandra Zanovelo Fogaça1
Lissandra Zanovelo Fogaça1 Caio Fabio Schlechta Portella2
Caio Fabio Schlechta Portella2 Ricardo Ghelman2
Ricardo Ghelman2 Carmen Verônica Mendes Abdala3
Carmen Verônica Mendes Abdala3 Mariana Cabral Schveitzer1*
Mariana Cabral Schveitzer1*- 1Department of Preventive Medicine, Universidade Federal de São Paulo, UNIFESP, São Paulo, Brazil
- 2Brazilian Academic Consortium for Integrative Health (CABSIn), São Paulo, Brazil
- 3BIREME (Latin American and Caribbean Center on Health Sciences Information) - Pan American Health Organization/World Health Organization (PAHO/WHO), São Paulo, Brazil
Background: The mind-body therapies of traditional Chinese medicine include several intervention types and combine physical poses with conscious relaxation and breathing techniques. The purpose of this Evidence Map is to describe these different interventions and report related health outcomes.
Methods: This evidence map is based on the 3iE Evidence Gap Map methodology. We searched seven electronic databases (BVS, PUBMED, EMBASE, PEDro, ScienceDirect, Web of Sciences, and PschyInfo) from inception to November 2019 and included systematic reviews only. Systematic reviews were analyzed based on AMSTAR 2. We used Tableau to graphically display quality assessment, the number of reviews, outcomes, and effects.
Results: The map is based on 116 systematic reviews and 44 meta-analyses. Most of the reviews were published in the last 5 years. The most researched interventions were Tai Chi and Qi Gong. The reviews presented the following quality assessment: 80 high, 43 moderate, 23 low, and 14 critically low. Every 680 distinct outcome effect was classified: 421 as potential positive; 237 as positive; 21 as inconclusive/mixed; one potential negative and none no effect. Positive effects were related to chronic diseases; mental indicators and disorders; vitality, well-being, and quality of life. Potential positive effects were related to balance, mobility, Parkinson's disease, hypertension, joint pain, cognitive performance, and sleep quality. Inconclusive/mixed-effects justify further research, especially in the following areas: Acupressure as Shiatsu and Tuiná for nausea and vomiting; Tai Chi and Qi Gong for acute diseases, prevention of stroke, stroke risk factors, and schizophrenia.
Conclusions: The mind-body therapies from traditional Chinese medicine have been applied in different areas and this Evidence Map provides a visualization of valuable information for patients, professionals, and policymakers, to promote evidence-based complementary therapies.
Highlights
- Mind-body therapies affects emotional, social, and health related outcomes.
- Evidence Map provides easy information for patients, professionals, and policy-makers.
- Positive effects include physiological indicators, mental health, and quality of life.
- Positive potential effects include metabolic indicators, pain, vitality, and well-being.
Background
The WHO has been encouraging and strengthening the insertion, recognition, and use of traditional, complementary, and integrative medicines (TCIM), products, and their practitioners in national health systems at all levels of activity: Primary Care, Specialized Care, and Hospital Care, through the recommendations of the WHO Strategy on Traditional Medicine 2014-2023 (1).
Mind-body therapies (MBT) consider the interactions between brain, mind, body, and behavior and understand that emotional, mental, social, and spiritual factors can directly affect health (2). MBT includes Tai Chi, Qigong, Yoga, Meditation, and types of relaxation (e.g., breathing exercises, autogenic training, biofeedback, and neurofeedback) (3). Moreover, these therapies can be offered alone or together with conventional treatments, since self-efficacy by itself may produce physiological benefits (4).
Qi Gong covers several practices and it is important to describe their meaning. The “Qi” means the energy that gives rise to activities of human life and “Gong” concerns the regulation of Qi through practice. Qi Gong practices consist of two forms: Qi Gong dynamic (external) or Qi Gong meditative (internal). Qi Gong external involves movements of the whole body or limbs (e.g., Tai Chi and Baduanjin), while Qigong internal requires the maintenance of posture with subtle body movements when performing exercises involving breathing and the mind (e.g., Meditation and Mindfulness) (5).
Acupressure Shiatsu and Tuiná hold the same principles as Acupuncture, but are non-invasive and do not need sophisticated equipment, as they are technics that use pressure through the body itself, such as through fingers, at the Acupuncture meridians points, to activate the body's internal energy flow (Qi), contributing to the restoration of its internal balance (6). These practices are based on Traditional Chinese Medicine, with Tuiná (7) (Chinese massage therapy) being more developed in China, while Shiatsu is a form of Acupressure more developed in Japan, with reports since the 1920s by Tokujiro Namikoshi (8).
Since 2006, Mind-Body Therapies from Traditional Chinese Medicine (MBTTCM) are some of the 29 complementary therapies included in the Brazilian National Health System. MBTTCM are ancient and consist of skills used in mind-body exercises integrating controlled breathing, body posture, gentle, and synergistic movements with mind adjustments (9, 10).
Therefore, these practices may contribute to the psychological component of quality of life (11), self-care practices (12), hypertension, fall prevention, cognitive performance, osteoarthritis, depression, chronic obstructive pulmonary disease, pain, balance confidence, and muscle strength (13, 14). Because of the recent extension of the complementary therapies policy, the Brazilian Ministry of Health partner up with the Latin American and Caribbean Center on Health Sciences Information (BIREME - PAHO – WHO) and with the Brazilian Academic Consortium of Integrative Health (CABSIn) to develop complementary therapies evidence maps, including this one about Mind-Body Therapies from Traditional Chinese Medicine (MBTTCM). The objective of this Evidence Map is to describe these different interventions and report related health outcomes.
Methods
The methodological steps of the evidence map are parallel to those involved in the initial stages of a systematic review. Although, systematic reviews look to collate a limited subset of the evidence base to answer a specific research question. However, the evidence map does not attempt to answer a specific research question instead guided by broader research objectives (15).
The Campbell Collaboration (16) suggests that any evidence and gap map are a systematic visual presentation of the availability of relevant evidence of effects for a policy domain. The map may be accompanied by a descriptive report to summarize the evidence for stakeholders such as researchers, research commissioners, policymakers, and practitioners.
This Evidence Map summarizes the interventions and health outcomes related to MBTTCM. These evidence maps considered six steps, each with a set of activities: (1) Search, (2) Selection, (3) Categorization, (4) Informetric, (5) Evidence map, and (6) Gaps (17). The method and results were reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (18) and the International Initiative for Impact Evaluation (3iE) Evidence Gap Methodology (19). This Evidence Map was supported by a technical expert panel of librarians, practitioners, policymakers, and researcher content experts.
Data Sources
Our search was conducted in several databases (BVS, PUBMED, EMBASE, PEDro, ScienceDirect, Web of Sciences, and PschyInfo), from each database inception to November 2019, looking for systematic reviews in English, Spanish, and Portuguese. The review question to guide the database search considered the following: (P) general population, (I) MBTTCM as intervention, (C) no comparator, and (O) health-related outcomes. We consulted topic experts and developed the search strategy together with Latin American and Caribbean Center on Health Sciences Information (BIREME), then entered the following expressions as shown in Table 1.
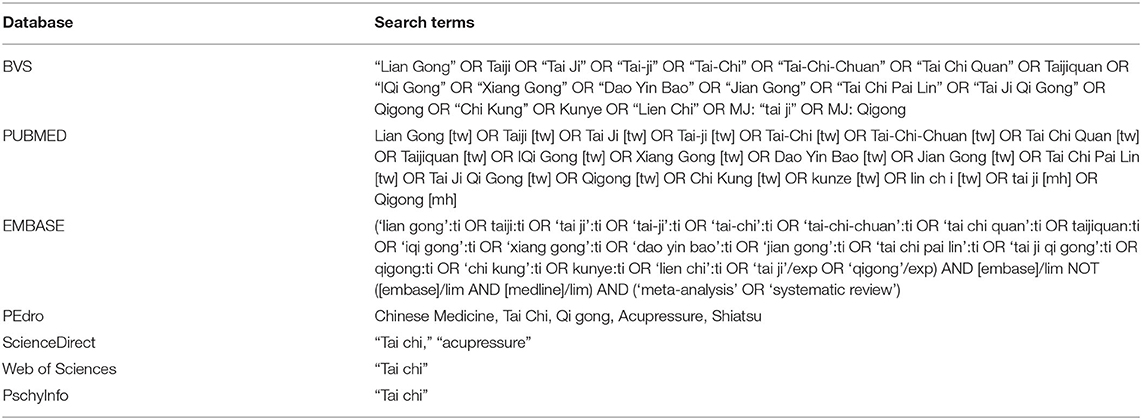
Table 1. Search strategy.
Inclusion Criteria
Systematic reviews about MBTTCM interventions and adequate descriptions of health outcomes were eligible for inclusion. We defined systematic reviews studies that self-identified as such. All participants of all ages, regardless of health status, were eligible for inclusion in the review. We excluded systematic reviews that did not focus on MBTTCM health outcomes. We included interventions on Tai Chi, Qi Gong, Traditional Chinese Exercise, Baduanjin, Acupressure techniques Shiatsu, and Tuiná of any duration and follow up.
Procedure
Two blinded independent literature reviewers screened the systematic review search output through the Rayyan software. Citations deemed potentially relevant by at least one reviewer and unclear citations were obtained as full text. The full-text publications were screened against the specified inclusion criteria by two independent reviewers; disagreements were resolved through discussion. This process is displayed at the PRISMA Flow Diagram (18) (Figure 1).
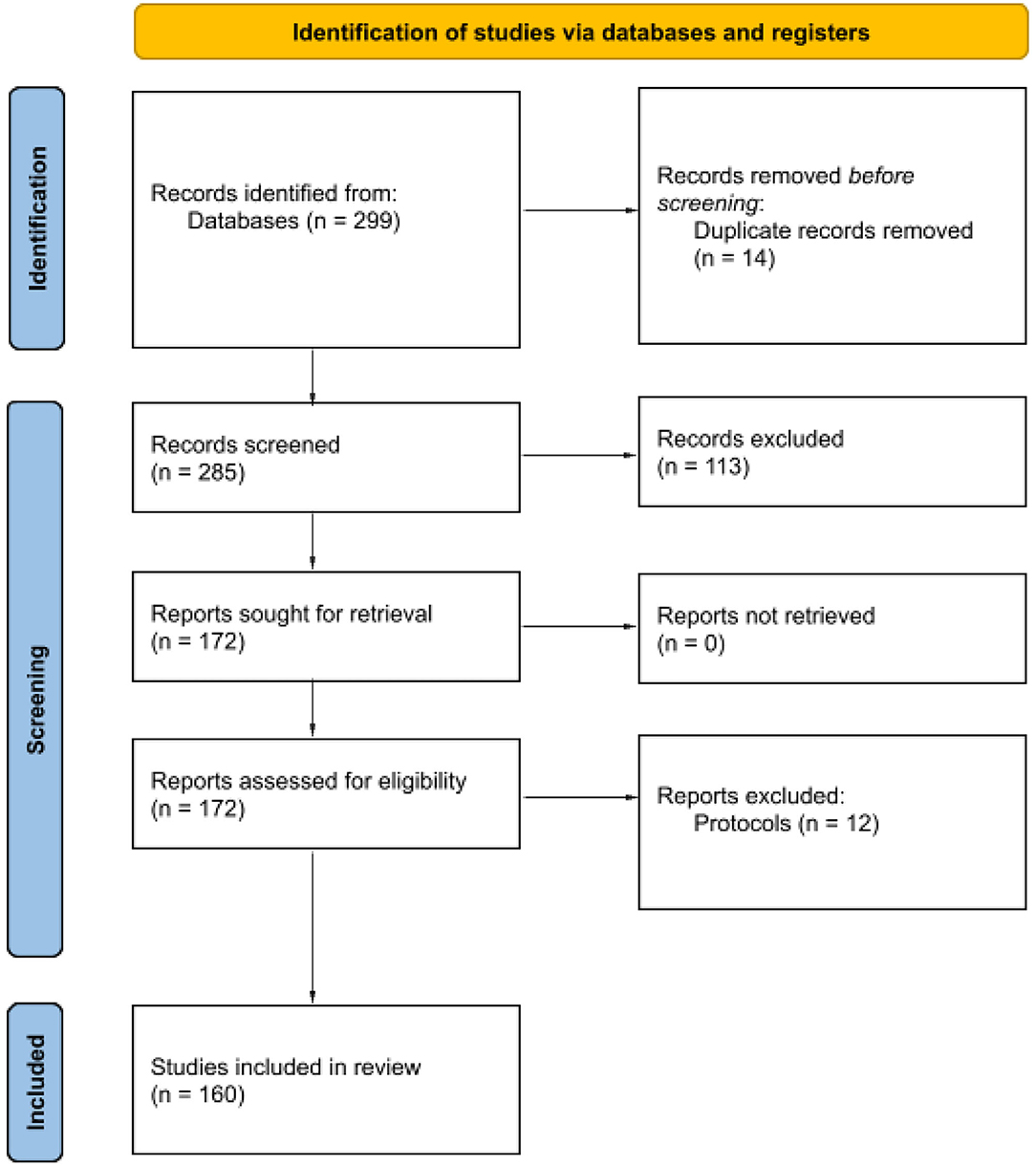
Figure 1. Flow diagram for systematic reviews included in the Mind-Body Therapies from traditional Chinese Medicine Evidence Map. Flow diagram template adopted from the PRISMA approach to systematic reviews (18).
We did not calculate the effect sizes in a meta-analysis nor did we provide the risk of bias assessments, but Assessing the Methodological Quality of Systematic Review (AMSTAR 2) was applied to analyze the quality (high, moderate, low and, critically low) of the included systematic reviews. The AMSTAR 2 by 16 item quality assessment analysis indicates confidence in the results of each review and describes the sources of bias: selection, measurement, and confounding (20). From each included systematic review, the intervention Tai Chi, Qi Gong, Baduanjin, Traditional Chinese Exercise, Shiatsu, and Tuiná was extracted, along with the main health outcomes (e.g., depression, hypertension, balance, physical function, mobility, risk of falls, well-being, pain) that were summarized across the included studies. The data about population, treatment effect (positive, potentially positive, mixed findings, potential negative and negative), estimates for health outcomes, and systematic review characteristics were retrieved.
Data Synthesis
We developed a characterization matrix in Excel to synthesize the findings. This matrix included: Full-Text Citation; Interventions; Outcomes Group; Outcomes; Effect; Population (as described in each study); Database ID; Focus Country; Publication Country; Publication Year; Type of Review; Review Design; Study Design; Quality Assessment. The systematic review outcomes were drafted by one reviewer and discussed by the review team, and the matrix was discussed in two workshops organized by BIREME. We organized the Evidence Map considering the outcomes, effects, and quality assessment of the included systematic reviews. We use the interactive Tableau platform to graphically display all this information.
Results
We identified 299 citations in the database search, 113 studies were excluded for not being systematic reviews, 172 were eligible for eligibility, 12 were excluded for being protocols, and 160 unique systematic reviews met the criteria for inclusion in the Evidence Map. Most of the reviews were published in 2017 and 2019. Tai Chi and Qi Gong were the most researched interventions.
The results found in the 160 systematic reviews were divided into eight major outcomes groups: cancer; acute diseases; chronic diseases; physiological and metabolic indicators and nutritional and metabolic diseases; pain; patient safety; mental indicators and mental disorders; vitality, well-being, and quality of life. This evidence map spanned wide health outcomes, effects, and populations. The outcome group, quality assessment, and effect by interventions are presented in Figure 2.
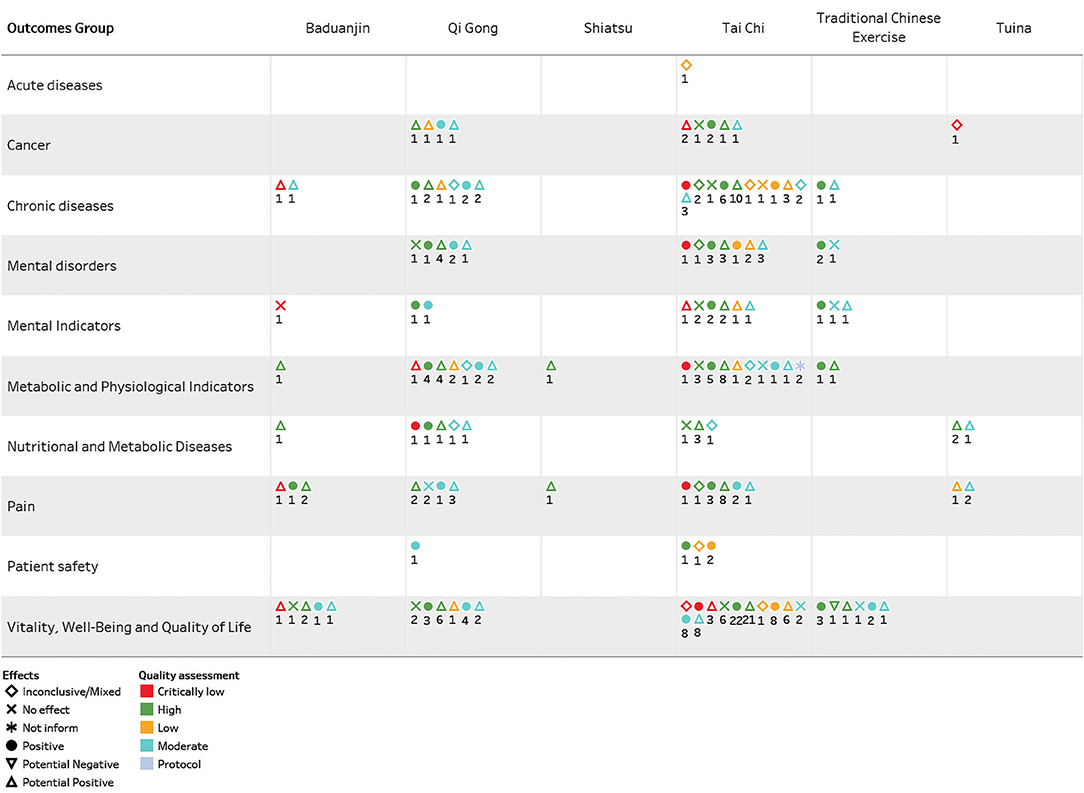
Figure 2. Outcome group, quality assessment, and effect by interventions of systematic reviews included in the Mind-Body Therapies from Traditional Chinese Medicine Evidence Map.
Interventions
The interventions were divided into two groups: Chinese bodily practices as Tai Chi, Qi Gong, Baduanjin, and Traditional Chinese Exercises; and manual stimulation of Acupuncture points (Acupressure) as Shiatsu and Tuiná. The Chinese bodily practices form was the most found in the reviews, highlighting the 313 Tai Chi and 107 Qi Gong interventions to distinct outcomes.
Population
This evidence map analyzed data from the following populations: people with chronic disease (38), older adults (38), people in general (18), people with heart disease (16), people with cancer (12), women (11). and diabetics (8). In addition, smaller representations with adults (5), people with hypertension (3), patients with stroke (3), and people with osteopenia (2). Patients with schizophrenia, graduation students, children with autism, and women with cancer, each with only one study. Two reviews had mixed populations of adults, women, and older adults.
Countries
The systematic reviews included analyzed data from the following countries: United States of America (50.3%), United Kingdom (23.7%), China (5.9%), Switzerland (5.1%), Singapore (2%), Germany (1.6%), Australia (1.4%), and England (1.25%).
Effects and Outcomes
Mind-Body Therapies from Traditional Chinese Medicine (MBTTCM) was evaluated as an intervention for 109 distinct health outcomes. Every outcome effect was classified as 421 positives; 237 potential positives; 21 inconclusive/mixed; one potentially negative, and none no effect, several reviews had more than one effect. Chronic diseases highlight positive effects for rheumatoid arthritis, hypertension, diabetes mellitus, coronary diseases, osteopenia, and rates of glycemia and high-density lipoprotein (HDL). Mental disorders target depression, anxiety, cognitive performance, humor, well-being, and dementia. Vitality, well-being and, quality of life outcomes emphasize results as balance, physical function, mobility, exercise capacity, quality of life and, risk of falling.
Figure 3 shows all these with more details as distinct ID counts divided by interventions vs. outcome list. Even as the colors show details about quality assessment and, the form shows details about the effects. Finally, the tags are labeled by distinct ID count and, the display is filtered on the effects of each intervention (Figure 3).
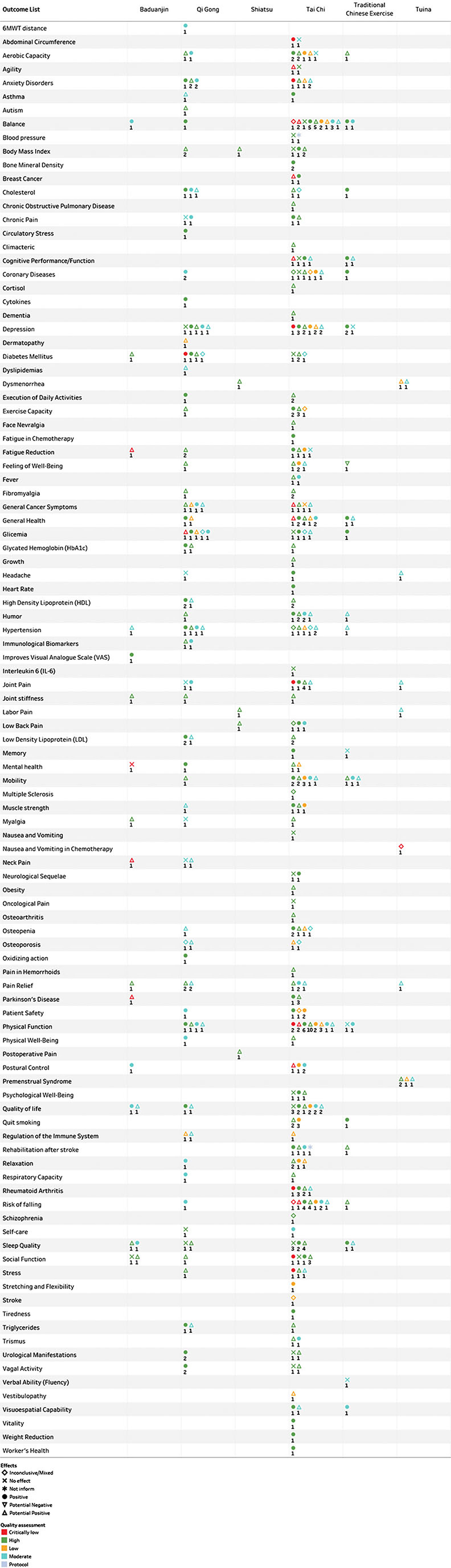
Figure 3. Outcomes, quality assessment, and effects by interventions of systematic interviews included in the Mind-Body Therapies from Traditional Chinese Medicine Evidence Map.
Cancer
The cancer group results in the included systematic reviews were breast cancer, general cancer symptoms, cancer pain, fatigue, nausea, and vomiting. Among these, the MBTTCM showed positive effects for breast cancer, fatigue, and general cancer symptoms (21–23). The systematic reviews showed potential positive effects for general cancer symptoms (24–26), as well as no effects for cancer pain and adjuvant cancer treatment (27–30). One systematic review showed mixed effects for nausea and vomiting (31).
Acute Diseases
The acute disease group results represent Tai Chi and Qi Gong interventions for stroke prevention. However, the effect of the single survey that related the results for stroke were inconclusive and mixed (32).
Chronic Diseases
The chronic diseases group results were rheumatoid arthritis, coronary disease, Parkinson's disease, hypertension, diabetes, osteopenia, osteoporosis, fibromyalgia, osteoarthritis, chronic obstructive pulmonary disease (COPD), asthma, multiple sclerosis, and vestibulopathy. The effects of MBTTCM were positive for osteoarthritis (33–35), coronary diseases (36–39), hypertension (40, 41), cardiovascular disease and risk factors (32, 42), and diabetes (43, 44). The MBTTCM presented a potentially positive effect for Parkinson's disease (45–47), fibromyalgia (48, 49), osteoarthritis (50), premenstrual syndrome (51–53), COPD (27, 54–57), and vestibulopathies (58).
Metabolic and Physiological Indicators and Nutritional and Metabolic Diseases
Mind-Body Therapies from Traditional Chinese Medicine (MBTTCM), as interventions for metabolic and physiological indicators and nutritional and metabolic diseases, showed positive effects for cholesterol, glycemia, and triglycerides (59, 60). Despite positive results, mixed-effects were also found in a study on cholesterol, glycemia, and no effect on blood pressure (36, 61–63).
Pain
Mind-Body Therapies from Traditional Chinese Medicine (MBTTCM), as interventions for pain conditions, showed positive effects for headache, joint pain, chronic pain, and low back pain (64–67) Also, potentially positive effects were related to general pain, dysmenorrhea, neck pain, hemorrhoid pain, labor pain, post-operative pain, myalgia, and facial neuralgia (48, 49, 52, 68–74).
Patient Safety
Mind-Body Therapies from Traditional Chinese Medicine (MBTTCM), as interventions—for patient safety, showed positive effects such as Tai Chi on the quality of life of patients with chronic disease, self-efficacy, psychological health conditions, and to prevent and manage cardiovascular disease (35, 75–79).
Mental Indicators and Mental Disorders
In the mental indicators and mental disorders group, Mind-Body Therapies from Traditional Chinese Medicine (especially Tai Chi and Qi Gong) had positive effects for cognitive performance, memory, physical and psychological well-being, depression, anxiety, dementia, stress (56, 80–83), and mixed effect to schizophrenia (84).
Vitality, Well-Being, and Quality of Life
Mind-Body Therapies from Traditional Chinese Medicine (MBTTCM) (especially Tai Chi and Qi Gong), as interventions in the vitality, well-being, and quality of life group, showed positive effects for balance, physical function, mobility (66, 82, 85–101), quality of life (102–104), and fall prevention (90, 97, 100, 105–107). There were also mixed effects for aerobic exercise, visuospatial capacity, fatigue-reducing, and cardiovascular disease (81, 108–110).
Quality Assessment
The systematic reviews included were analyzed based on AMSTAR 2, resulting in the following quality assessment: 80 High, 43 Moderate, 23 Low, and 14 critically low. The systematic review's authors indicated some methodological flaws, highlighting population heterogeneity in the practice groups, period, and time of intervention.
Limitations and Strengths
Even though Evidence Maps have several limitations, like the fact that we used only published reviews to provide an overview on the research on MBTTCM, more evidence, including qualitative studies, were not included. We did not calculate the effect sizes in a meta-analysis, nor provide the risk of bias assessments, but we tried to overcome these limitations by applying AMSTAR 2 to the quality assessment of the included systematic reviews.
In addition, the grouping of outcomes was review-content driven. Even though individual primary research studies would have more contributions to add to the analysis, this was not the focus of the Map. Besides, we were unable to avoid overlapping the included studies across reviews, but we did not repeat the results from updated reviews. We relied on the review author's skills in conducting systematic reviews, evaluation of primary studies quality, choice of outcomes, analysis of effects, susceptibility to publication, and outcome reporting bias.
Evidence maps are not designed to provide detailed and definitive information on the effectiveness of interventions. The implementation of the reviewed interventions in practice will require additional steps (e.g., identifying the optimal intervention format). Generally, evidence maps are a very broad overview of the evidence base, indicating areas in which research has been conducted, to help stakeholders interpret the state of the evidence to inform policy and clinical decision making.
Therefore, this evidence gap map can only provide a broad research overview, the findings showed more positive effects than potential negative or negative ones, including reviews of high, moderate, low, and critically low-quality assessments. The duration, period, and frequency of MBTTCM have not been analyzed and need more research.
The creation and publication of this evidence map consist in graphically representing the best evidence found, analyzed, and categorized, in addition to linking with the bibliographic records and full texts (when available) of the studies to facilitate access to information for all those interested.
Research Gaps
The systematic reviews included did not clearly report the time of practices, frequency, more details of each practice, and duration of interventions. Therefore, the heterogeneity of the studies regarding the included participants, intervention characteristics, durations, and control groups may also limit the validity of the results. Furthermore, there have been no studies with pregnant women.
This Evidence Map will also not be able to answer more specific questions, such as the most appropriate method of applying Traditional Chinese Medicine Mind-Body Therapies, the difference between health services, adequate training of professionals, patient access, and self-application effects.
Future research, such as qualitative review surveys and evidence maps that only include systematic reviews of randomized clinical trials, are needed to answer refined questions, which are extremely important for the development of Traditional Chinese Medicine Mind-Body Therapies.
Discussion
This evidence map for MBTTCM is based on 160 published systematic reviews and provides an available evidence broad overview of these interventions, related outcomes, and effects. It shows the volume of available research and highlights areas where the interventions showed positive effects.
The characteristics of the MBTTCM (e.g., Tai Chi, Qi Gong, Baduanjin, and Traditional Chinese Exercises) include low cost, moderate intensity, low technology, and low impact, and the possibility of practice by adults and older adults with chronic diseases (111). The movements are slow and rhythmic, linked together in a continuous sequence, and the body weight is shifted from one leg to another, challenging the balance control system to maintain its center within a changing support base (112).
Mind-Body Therapies from Traditional Chinese Medicine (MBTTCM) have been evaluated in different health conditions, including chronic diseases and mental disorders, and in vitality, well-being, and quality of life, assessed in a very broad population, from patients with chronic diseases to older adults.
This evidence map demonstrates that Tai Chi can significantly benefit adults and older adults with chronic diseases related to rheumatoid arthritis, hypertension, diabetes mellitus, coronary diseases, and osteopenia. Furthermore, significant improvements emphasize the results such as balance, physical function, mobility, exercise capacity, quality of life, and risk of falling. Highlighting beneficial effects for reductions in depression, disability falls, pain, and stiffness.
Tai Chi included significant improvements in cancers, chronic obstructive pulmonary disease, coronary heart disease, heart failure, hypertension, low back pain, osteoarthritis, osteoporosis, Parkinson's Disease, and stroke (113) as well as has favorable effects on depressive symptoms and quality of life of older adults (114), psychological well-being among persons with cardiovascular disease (115). Tai Chi can also improve strength, balance, balance confidence, mobility, gait, and executive function among older people (116, 117), reducing outcomes related to the extended frailty phenotype in older age adults (118).
The inconclusive/mixed-effects related to Tai Chi such as schizophrenia, aerobic exercise, visuospatial capacity, fatigue-reducing, and cardiovascular disease need more research.
The evidence map outcomes related Qi Gong to mental disorders scoped depression, anxiety, cognitive performance, mood, and feeling of well-being as well as chronic diseases such as diabetes, hypertension, metabolic syndrome, and cancer. Also, beneficial effects for reductions blood pressure, rates of glycemia, and HDL, pain, and improving risk factors metabolic syndrome were associated with Qi Gong.
Qi Gong may serve as a promising opportunity to improve psychological health domains such as the quality of life, depressive symptoms, fear of falling, and sleep quality in older adults (119), potentially having a beneficial effect on symptoms of anxiety (120), potentially effective to improve gait speed, balance, activities of daily living, and mobility to be a promising complementary therapy in Parkinson's Disease (121, 122), significant improvement in fatigue, and global distress in oncology patients (123).
Although this evidence map found positive effects of Qi Gong for diabetes, further research is suggested to debate these results. Also, Qi Gong applied to children with autism.
This evidence map involves 10 reviews of the Traditional Chinese Exercise (TCE) and only three reviews to present the Baduanjin results. The health outcomes for these interventions report positive and potentially positive effects related to chronic diseases such as diabetes, hypertension, coronary disease, osteoarthritis, and Parkinson's disease and the improvements emphasize results of fatigue, low back pain, neck pain, cognitive performance, psychological well-being and quality of sleep. The Baduanjin to osteoarthritis demonstrated a statistically significant improvement in pain, stiffness, and physical function (124), effective physical exercise intervention in patients with essential hypertension (125), is associated with statistically significant global cognitive function in patients post-stroke and the community of middle-aged and older adults. (126, 127). TCE can be potentially beneficial in alleviating cancer-related sleep disturbance (128), can effectively improve physical performance, balance, and muscle strength in the elderly population (129).
Although these studies include both high and moderate-quality assessments and could be considered for healthcare applications in these areas, further research with TCE and Baduanjin is needed.
Acupressure techniques such as Shiatsu and Tuiná are variants of Acupuncture and use hands and fingers to rub, knead or strike soft tissues and joints of the Acupuncture point regions in the body. They are non-invasive body practices and can be administered by the patients themselves (130).
This evidence map related to acupressure interventions showed potential positive effects involving dysmenorrhea, labor pain, nausea and vomit, low back pain, premenstrual syndrome, and pain relief. These effects appear in only seven reviews with high and moderate-quality assessment highlighting dysmenorrhea, nausea and vomit, and pain relief.
The Cochrane review demonstrates that acupressure probably has efficacy in reducing nausea and vomiting in women in labor, however, the stand-out evidence was generally low warranting further research (131). Acupressure may reduce pain intensity for pain management during labor (132, 133).
This Evidence Map demonstrated that acupressure could be considered for healthcare applications in these areas, nonetheless, further research is required.
Our map showed more positive effects and only one potential negative effect from a moderate quality review related to adverse effects and sense of well-being (134). The mixed effects justify further research and can help to guide different institutions' funding calls.
The outcomes and effects information of MBTTCM showed in these Maps will further advance our evidence-based knowledge of complementary therapies, such as that proposed by the complementary therapies policy in Brazil and promoted by the WHO MTCI 2014-2024 agenda.
Conclusions
Mind-Body Therapies from Traditional Chinese Medicine (MBTTCM) have been applied in different areas and this map indicates 421 positive and promising health outcomes that need further research. Despite the outlined limitations, this evidence map provides a visualization of valuable information for patients, health practitioners, and policymakers, in order to promote evidence-based complementary therapies.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
LF and MS drafted the manuscript. LF, MS, RG, CA, and CP designed the study and were involved in data acquisition and analysis. CA, MS, and LF designed and executed the search strategy. All authors were involved in the interpretation of the data, contributed to the final manuscript, read, and approved the final manuscript.
Funding
The study is part of a project funded by the Brazilian Ministry of Health in partnership with the Latin American and Caribbean Center on Health Sciences Information (BIREME - PAHO - WHO) and the Brazilian Academic Consortium for Integrative Health (CABSIN) to develop complementary therapies Evidence Gap Maps, including Mind-Body Therapies of Traditional Chinese Medicine. The Brazilian Ministry of Health funded the project and BIREME-research partners conducted the study; collection; management; analysis; interpretation of the data; preparation, review, and decision to submit the manuscript for publication. The findings and conclusions in this publication are those of the authors who are responsible for its contents; the findings and conclusions do not necessarily represent the views of the Brazilian Ministry of Health and BIREME-PAHO-WHO.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to express their gratitude to the Ministry of Health, Brazil, and BIREME-PAHO-WHO for the financial support for this research and the technical expert panel advising the project. Any errors of fact or interpretation in this manuscript remain the responsibility of the authors. We would like to do a special knowledge to Gabriela Caires Nunes who helped in data acquisition.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.659075/full#supplementary-material
References
1. World Health Organization. WHO Traditional Medicine Strategy: 2014-2023. (2013). p. 78. Available online at: https://www.who.int/publications/i/item/9789241506096 (accessed November 8, 2020).
2. Morone NE, Greco CM. Mind–body interventions for chronic pain in older adults: a structured review. Pain Med. (2007) 8:359–75. doi: 10.1111/j.1526-4637.2007.00312.x
3. Ramirez-Garcia MP, Gagnon MP, Colson S, Côté J, Flores-Aranda J, Dupont M. Mind-body practices for people living with HIV: a systematic scoping review. BMC Complement Altern Med. (2019) 19:125. doi: 10.1186/s12906-019-2502-z
4. Dossett ML, Fricchione GL, Benson H. A new era for mind-body medicine. N Engl J Med. (2020) 382:1390–1. doi: 10.1056/NEJMp1917461
5. Feng F, Tuchman S, Denninger JW, Fricchione GL, Yeung A. Qigong for the prevention, treatment, and rehabilitation of COVID-19 infection in older adults. Am J Geriatr Psychiatry. (2020) 28:812–9. doi: 10.1016/j.jagp.2020.05.012
6. Jahnke R, Larkey L, Rogers C, Etnier J, Lin F. A comprehensive review of health benefits of Qigong and Tai Chi. Am J Health Promot. (2010) 24:e1–25. doi: 10.4278/ajhp.081013-LIT-248
7. Li D, Wang C, Ruan D, Li J, Ji N, Ma X, et al. Chinese massage, Tui Na, combined with herbs improves clinical symptoms and regulates sex hormones in patients with mammary gland hyperplasia. Medicine. (2020) 99:21. doi: 10.1097/MD.0000000000020300
8. Kobayashia D, Shimbod T, Hayashie H, Takahashi O. Shiatsu for chronic lower back pain: randomized controlled study. Compl Ther Med. (2019) 45:33–7. doi: 10.1016/j.ctim.2019.05.019
9. Lee C, Crawford C, Hickey A. Mind-body therapies for the self-management of chronic pain symptoms. Pain Med. (2014) 15:S21–39. doi: 10.1111/pme.12383
10. Luo C, Wen J, Sun W, Li T, Yu X, Zhang T, et al. Effects of traditional Chinese exercise on cardiac rehabilitation after percutaneous coronary intervention: study protocol for network metanalysis of randomized controlled trials. BMJ Open. (2019) 9:e023096. doi: 10.1136/bmjopen-2018-023096
11. Wang D, Wang P, Lan K, Zhang Y, Pan Y. Effectiveness of Tai chi exercise on overall quality of life and its physical and psychological components among older adults: a systematic review and meta-analysis. Braz J Med Biol Res. (2020) 53:e10196. doi: 10.1590/1414-431x202010196
12. Harvie A, Steel A, Wardle J. Traditional Chinese medicine self-care and lifestyle medicine outside of Asia: a systematic literature review. J Altern Compl Med. (2019) 25:789–808. doi: 10.1089/acm.2018.0520
13. Solloway MR, Taylor SL, Shekelle PG, Miake-Lye IM, Beroes JM, Shanman RM, et al. An evidence map of the effect of Tai Chi on health outcomes. Syst Rev. (2016) 5:126. doi: 10.1186/s13643-016-0300-y
14. Hempel S, Taylor SL, Solloway M, Miake-Lye IM, Beroes JM, Shanman R. Evidence Map of Tai Chi [Internet]. Washington, DC: Department of Veterans Affairs (2014). Available online at: https://www.ncbi.nlm.nih.gov/journals/NBK253200/ (accessed November 24, 2021).
15. Wolffea TAM, Whaleya P, Halsalla C, Rooneyc AA, Walker VR. Systematic evidence maps as a novel tool to support evidence-based decision-making in chemicals policy and risk management. Environ Int. (2019) 130:104871. doi: 10.1016/j.envint.2019.05.065
16. Saran A, White H. Evidence Gap Maps: A Comparison of Different Approaches. Oslo: The Campbell Collaboration. (2018). Available online at: www.campbellcollaboration.org/ (accessed October 23, 2021).
17. Schveitzer MC, Abdala CVM, Portella CFS, Ghelman R. Traditional, complementary, and integrative medicine evidence map: a methodology to an overflowing field of data and noise. Rev Panam Salud Publica. (2021) 45:e48. doi: 10.26633/RPSP.2021.48
18. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ. (2021) 372:n71 doi: 10.1136/bmj.n71
19. Snilstveit B, Vojtkova M, Bhavsar A, Stevenson J, Gaarder M. Evidence & Gap Maps: a tool for promoting evidence informed policy and strategic research agendas. J Clin Epidemiol. (2016) 79:120–9. doi: 10.1016/j.jclinepi.2016.05.015
20. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. (2017) 358:j4008. doi: 10.1136/bmj.j4008
21. Huston P, McFarlane B. Health benefits of Tai Chi. What is the evidence? Can Family Phy. (2016) 62:881–90.
22. Song S, Yu J, Ruan Y, Liu X, Xiu L, Yue X. Ameliorative effects of Tai Chi on cancer-related fatigue: a meta-analysis of randomized controlled trials. Supportive Care Cancer. (2018) 26:2091–102. doi: 10.1007/s00520-018-4136-y
23. Van VuD, Molassiotis A, Ching SS Y, Le TT. Effects of Qigong on symptom management in cancer patients: a systematic review. Compl Ther Clin Pract. (2017) 29:111–21. doi: 10.1016/j.ctcp.2017.09.005
24. Lee MS, Chen KW, Sancier KM, Ernst E. Qigong for cancer treatment: a systematic review of controlled clinical trials. Acta Oncol. (2007) 46:717–22. doi: 10.1080/02841860701261584
25. Klein PJ, Schneider R, Rhoads CJ. Qigong in cancer care: a systematic review and construct analysis of effective Qigong therapy. Support Care Cancer. (2016) 24:3209–22. doi: 10.1007/s00520-016-3201-7
26. Chan CLW, Wang CW, Ho RTH, Ng SM, Chan JSM, Ziea ETC, et al. A systematic review of the effectiveness of qigong exercise in supportive cancer care. Support Care Cancer. (2012) 20:1121–33. doi: 10.1007/s00520-011-1378-3
27. Chen YW, Hunt MA, Campbell KL, Peill K, Reid WD. The effect of Tai Chi on four chronic conditions—cancer, osteoarthritis, heart failure and chronic obstructive pulmonary disease: a systematic review and meta-analyses. Br J Sports Med. (2016) 50:397–407. doi: 10.1136/bjsports-2014-094388
28. Lee MS, Choi TY, Ernst E. Tai Chi for breast cancer patients: a systematic review. Breast Cancer Res Treat. (2010) 120:309–16. doi: 10.1007/s10549-010-0741-2
29. Pan Y, Yang K, Shi X, Liang H, Zhang F, Lv Q. Tai Chi Chuan exercise for patients with breast cancer: a systematic review and meta-analysis. Evid Based Compl Altern Med. (2015) 2015:535237. doi: 10.1155/2015/535237
30. Lee MS, Pittler MH, Ernst E. Is Tai Chi an effective adjunct in cancer care? A systematic review of controlled clinical trials. Supportive Care Cancer. (2017) 15:597–601. doi: 10.1007/s00520-007-0221-3
31. Lee J, Dodd H, Dibble S, Abrams D. Review of acupressure studies for chemotherapy-induced nausea and vomiting control. J Pain Symptom Manag. (2008) 36:529–44. doi: 10.1016/j.jpainsymman.2007.10.019
32. Lauche R, Peng W, Ferguson C, Cramer H, Frawley J, Adams J, et al. (2017). Efficacy of Tai Chi and qigong for the prevention of stroke and stroke risk factors: a systematic review with meta-analysis. Medicine. (2008) 96:e8517. doi: 10.1097/MD.0000000000008517
33. Ye J, Cai S, Zhong W, Cai S, Zheng Q. Effects of Tai Chi for patients with knee osteoarthritis: a systematic review. J Phys Ther Sci. (2014) 26:1133–7. doi: 10.1589/jpts.26.1133
34. Chang WD, Chen S, Lee CL, Lin HY, Lai PT. The effects of Tai Chi Chuan on improving mind-body health for knee osteoarthritis patients: a systematic review and meta-analysis. Evid Based Compl Altern Med. (2016) 2016:1813979. doi: 10.1155/2016/1813979
35. Taylor-Piliae RE. Tai Ji Quan as an exercise modality to prevent and manage cardiovascular disease: a review. J Sport Health Sci. (2014) 3:43–51. doi: 10.1016/j.jshs.2013.09.002
36. Wang XQ, Pi YL, Chen PJ, Liu Y, Wang R, iL X, et al. Traditional Chinese exercise for cardiovascular diseases: systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. (2016) 5:e002562. doi: 10.1161/JAHA.115.002562
37. Chan CL, Wang CW, Ho RT, Ho AH, Ziea ET, Taam Wong VC, et al. A systematic review of the effectiveness of qigong exercise in cardiac rehabilitation. Am J Chin Med. (2012) 40:255–67. doi: 10.1142/S0192415X12500206
38. Ng BH, Tsang HW. Psychophysiological outcomes of health qigong for chronic conditions: a systematic review. Psychophysiology. (2009) 46:257–69. doi: 10.1111/j.1469-8986.2008.00763.x
39. Dalusung-Angosta A. The impact of Tai Chi exercise on coronary heart disease: a systematic review. J Am Acad Nurse Pract. (2011) 23:376–81. doi: 10.1111/j.1745-7599.2011.00597.x
40. Lee MS, Pittler MH, Guo R, Ernst E. Qigong for hypertension: a systematic review of randomized clinical trials. J Hypertens. (2007 25:1525–32. doi: 10.1097/HJH.0b013e328092ee18
41. Yeh GY, Wang C, Wayne PM, Phillips R. Tai Chi exercise for patients with cardiovascular conditions and risk factors: a systematic review. J Cardiopulmon Rehabil Prev. (2009) 29:152–60. doi: 10.1097/HCR.0b013e3181a33379
42. Lee MS, Pittler MH, Taylor-Piliae RE, Ernst E. Tai chi for cardiovascular disease and its risk factors: a systematic review. J Hypertens. (2007) 25:1974–5. doi: 10.1097/HJH.0b013e32828cc8cd
43. Lee MS, Choi TY, Lim HJ, Ernst E. Tai chi for management of type 2 diabetes mellitus: a systematic review. Chin J Integr Med. (2011) 17:789–93. doi: 10.1007/s11655-011-0812-1
44. Lee MS, Chen KW, Choi TY, Ernst E. Qigong for type 2 diabetes care: a systematic review. Compl Ther Med. (2009) 17:236–42. doi: 10.1016/j.ctim.2009.05.001
45. Ni X, Liu S, Lu F, Shi X, Guo X. Efficacy and safety of Tai Chi for Parkinson's disease: a systematic review and meta-analysis of randomized controlled trials. PLoS ONE. (2014) 9:e99377. doi: 10.1371/journal.pone.0099377
46. Kedzior KK, Kaplan I. Tai Chi and Parkinson's disease (PD): a systematic overview of the scientific quality of the past systematic reviews. Compl Ther Med. (2019) 46:144–52. doi: 10.1016/j.ctim.2019.08.008
47. Yang Y, Li XY, Gong L, Zhu YL, Hao YL. Tai Chi for improvement of motor function, balance and gait in Parkinson's disease: a systematic review and meta-analysis. PLoS ONE. (2014) 9:e102942. doi: 10.1371/journal.pone.0102942
48. Cheng CA, Chiu YW, Wu D, Kuan YC, Chen SN, Tam KW. Effectiveness of Tai Chi on fibromyalgia patients: a meta-analysis of randomized controlled trials. Compl Ther Med. (2019) 46:1–8. doi: 10.1016/j.ctim.2019.07.007
49. Lauche R, Cramer H, Häuser W, Dobos G, Langhorst J. A systematic review and meta-analysis of qigong for the fibromyalgia syndrome. Evid Based Compl Altern Med. (2013) 2013:635182. doi: 10.1155/2013/635182
50. Lee MS, Pittler MH, Shin BC, Ernst E. Tai chi for osteoporosis: a systematic review. Osteoporosis Int. (2008) 19:139–46. doi: 10.1007/s00198-007-0486-x
51. Chen MN, Chien LW, Liu CF. Acupuncture or acupressure at the sanyinjiao (SP6) acupoint for the treatment of primary dysmenorrhea: a meta-analysis. Evid Based Compl Altern Med. (2013) 2013:493038. doi: 10.1155/2013/493038
52. Jiang HR, Ni S, Li JL, Liu MM, Li J, Cui XJ, et al. Systematic review of randomized clinical trials of acupressure therapy for primary dysmenorrhea. Evid Based Compl Altern Med. (2013) 2013:169692. doi: 10.1155/2013/169692
53. Wang Y, Shan W, Li Q, Yang N, Shan W. Tai Chi exercise for the quality of life in a perimenopausal women organization: a systematic review. Worldviews Evid Based Nursing. (2017) 14:294–305. doi: 10.1111/wvn.12234
54. Wu W, Liu X, Wang L, Wang Z, Hu J, Yan J. Effects of Tai Chi on exercise capacity and health-related quality of life in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Int J Chronic Obstr Pulmo Dis. (2014) 9:1253–63. doi: 10.2147/COPD.S70862
55. Yan JH, Guo YZ, Yao HM, Pan L. Effects of Tai Chi in patients with chronic obstructive pulmonary disease: preliminary evidence. PLoS ONE. (2013) 8:e61806. doi: 10.1371/journal.pone.0061806
56. Wu JJ, Zhang YX, Du WS, Jiang LD, Jin RF, Yu HY, Liu JM, et al. Effect of Qigong on self-rating depression and anxiety scale scores of COPD patients: a meta-analysis. Medicine. (2019) 98:e15776. doi: 10.1097/MD.0000000000015776
57. Tong H, Liu Y, Zhu Y, Zhang B, Hu J. The therapeutic effects of qigong in patients with chronic obstructive pulmonary disease in the stable stage: a meta-analysis. BMC Compl Altern Med. (2019) 19:239. doi: 10.1186/s12906-019-2639-9
58. Wayne PM, Krebs DE, Wolf SL, Gill-Body KM, Scarborough DM, McGibbon CA, et al. Can Tai Chi improve vestibulopathic postural control? Arch Phys Med Rehabil. (2004) 85:142–52. doi: 10.1016/S0003-9993(03)00652-X
59. Song G, Chen C, Zhang J, Chang L, Zhu D, Wang X. Association of traditional Chinese exercises with glycemic responses in people with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. J Sport Health Sci. (2018) 7:442–52. doi: 10.1016/j.jshs.2018.08.004
60. Chao M, Wang C, Dong X, Ding M. The effects of Tai Chi on type 2 diabetes mellitus: a meta-analysis. J Diabetes Res. (2018) 2018:7350567. doi: 10.1155/2018/7350567
61. Zou L, Zhang Y, Sasaki JE, Yeung AS, Yang L, Loprinzi PD, et al. Wuqinxi Qigong as an alternative exercise for improving risk factors associated with metabolic syndrome: a meta-analysis of randomized controlled trials. Int J Environ Res Public Health. (2019) 16:1396. doi: 10.3390/ijerph16081396
62. Zheng G, Huang M, Liu F, Li S, Tao J, Chen L. Tai chi chuan for the primary prevention of stroke in middle-aged and elderly adults: a systematic review. Evid Based Compl Altern Med. (2015) 2015:742152. doi: 10.1155/2015/742152
63. Pan XH, Mahemuti A, Zhang XH, Wang YP, Hu P, Jiang JB, et al. Effect of Tai Chi exercise on blood lipid profiles: a meta-analysis of randomized controlled trials. J Zhejiang Univ Sci B. (2016) 17:640–8. doi: 10.1631/jzus.B1600052
64. Qin J, Zhang Y, Wu L, He Z, Huang J, Tao J, et al. Effect of Tai Chi alone or as additional therapy on low back pain: systematic review and meta-analysis of randomized controlled trials. Medicine. (2019) 98:e17099. doi: 10.1097/MD.0000000000017099
65. Hall A, Copsey B, Richmond H, Thompson J, Ferreira M, Latimer J, et al. Effectiveness of Tai Chi for chronic musculoskeletal pain conditions: updated systematic review and meta-analysis. Phys Ther. (2017) 97:227–38. doi: 10.2522/ptj.20160246
66. Zhang Y, Huang L, Su Y, Zhan Z, Li Y, Lai X. The effects of traditional chinese exercise in treating knee osteoarthritis: a systematic review and meta-analysis. PLoS ONE. (2017). (2017) 12:e0170237. doi: 10.1371/journal.pone.0170237
67. Lee MS, Pittler MH, Ernst E. External qigong for pain conditions: a systematic review of randomized clinical trials. J Pain. (2007) 8:827–31. doi: 10.1016/j.jpain.2007.05.016
68. Kong LJ, Lauche R, Klose P, Bu JH, Yang XC, Guo CQ, et al. Tai Chi for chronic pain conditions: a systematic review and meta-analysis of randomized controlled trials. Sci Rep. (2016) 6:25325. doi: 10.1038/srep25325
69. Zhang Y, Loprinzi PD, Yang L, Liu J, Liu S, Zou L. The beneficial effects of traditional chinese exercises for adults with low back pain: a meta-analysis of randomized controlled trials. Medicina. (2019) 55:118. doi: 10.3390/medicina55050118
70. Robinson N, Lorenc A, Liao X. The evidence for Shiatsu: a systematic review of Shiatsu and acupressure. BMC Complement Altern Med. (2011) 11:88. doi: 10.1186/1472-6882-11-88
71. Cho SH, Hwang EW. Acupressure for primary dysmenorrhoea: a systematic review. Compl Ther Med. (2010) 18:49–56. doi: 10.1016/j.ctim.2009.10.001
72. Zou L, Pan Z, Yeung A, Talwar S, Wang C, Liu Y, et al. A Review Study on the Beneficial Effects of Baduanjin. J Altern Compl Med. (2018) 24:324–35. doi: 10.1089/acm.2017.0241
73. Girard J, Girard A. The effects of qigong on neck pain: a systematic review. Compl Ther Clin Pract. (2019) 34:23–29. doi: 10.1016/j.ctcp.2018.10.013
74. Zou L, Yeung A, Quan X, Boyden SD, Wang H. A systematic review and meta-analysis of mindfulness-based (Baduanjin) exercise for alleviating musculoskeletal pain and improving sleep quality in people with chronic diseases. Int J Environ Res Public Health. (2018) 15:206. doi: 10.3390/ijerph15020206
75. Chen YW, Wang HH. The effectiveness of acupressure on relieving pain: a systematic review. Pain Manag Nurs. (2014) 15:539–50. doi: 10.1016/j.pmn.2012.12.005
76. Li G, Yuan H, Zhang W. Effects of Tai Chi on health-related quality of life in patients with chronic conditions: a systematic review of randomized controlled trials. Compl Ther Med. (2014) 22:743–55. doi: 10.1016/j.ctim.2014.06.003
77. Dechamps A, Lafont L, Borudel-Marchasson I. Effects of Tai Chi exercises on self-efficacy and psychological health. Eur Rev Aging Phys Activity. (2007) 4:25–32. doi: 10.1007/s11556-007-0015-0
78. Taylor E, Taylor-Piliae RE. The effects of Tai Chi on physical and psychosocial function among persons with multiple sclerosis: a systematic review. Compl Ther Med. (2017) 31:100–8. doi: 10.1016/j.ctim.2017.03.001
79. Chang PS, Knobf T, Oh B, Funk M. Physical and psychological health outcomes of qigong exercise in older adults: a systematic review and meta-analysis. Am J Chin Med. (2019) 47:301–22. doi: 10.1142/S0192415X19500149
80. Wang X, Pi Y, Chen B, Chen P, Liu Y, Wang R, et al. Effect of traditional Chinese exercise on the quality of life and depression for chronic diseases: a meta-analysis of randomised trials. Sci Rep. (2015) 5:15913. doi: 10.1038/srep15913
81. Lim KH, Pysklywec A, Plante M, Demers L. The effectiveness of Tai Chi for short-term cognitive function improvement in the early stages of dementia in the elderly: a systematic literature review. Clin Interv Aging. (2019) 14:827–39. doi: 10.2147/CIA.S202055
82. Song R, Grabowska W, Park M, Osypiuk K, Vergara-Diaz GP, Bonato P, et al. The impact of Tai Chi and Qigong mind-body exercises on motor and non-motor function and quality of life in Parkinson's disease: a systematic review and meta-analysis. Parkinsonism Relat Disord. (2017) 41:3–13. doi: 10.1016/j.parkreldis.2017.05.019
83. Webster CS, Luo AY, Krägeloh C, Moir F, Henning M. A systematic review of the health benefits of Tai Chi for students in higher education. Prev Med Rep. (2015) 3:103–12. doi: 10.1016/j.pmedr.2015.12.006
84. Zheng W, Li Q, Xiang Y, Guo T, Chen Q, Cai D, et al. Tai Chi for schizophrenia: a systematic review. Shanghai Arch Psychiatry. (2016) 28:185–94. doi: 10.11919/j.issn.1002-0829.216051
85. Rand D, Miller WC, Yiu J, Eng JJ. Interventions for addressing low balance confidence in older adults: a systematic review and meta-analysis. Age Ageing. (2011) 40:297–306. doi: 10.1093/ageing/afr037
86. Cwiekala-Lewis KJ, Gallek M, Taylor-Piliae RE. The effects of Tai Chi on physical function and well-being among persons with Parkinson's Disease: a systematic review. J Bodywork Mov Ther. (2017) 21:414–21. doi: 10.1016/j.jbmt.2016.06.007
87. Che BL, Guo JB, Liu MS, Li X, Zou J, Chen X, et al. Effect of traditional chinese exercise on gait and balance for stroke: a systematic review and meta-analysis. PLoS ONE. (2015) 10:e0135932. doi: 10.1371/journal.pone.0135932
88. Ge L, Zheng QX, Liao YT, Tan JY, Xie QL Rask M. Effects of traditional Chinese exercises on the rehabilitation of limb function among stroke patients: a systematic review and meta-analysis. Complement Ther Clin Pract. (2017) 29:35–47. doi: 10.1016/j.ctcp.2017.08.005
89. Hao L, Adam F. Tai chi as a balance improvement exercise for older adults: a systematic review. J Geriatr Phys Ther. (2001) 33:103–9.
90. Huang Y, Liu X. Improvement of balance control ability and flexibility in the elderly Tai Chi Chuan (TCC) practitioners: a systematic review and meta-analysis. Arch Gerontol Geriatr. (2015) 60:233–8. doi: 10.1016/j.archger.2014.10.016
91. Ren X, Li Y, Yang X, Li J, Li H, Yuan Z, et al. The effects of Tai Chi training in patients with heart failure: a systematic review and meta-analysis. Front Physiol. (2017) 8:989. doi: 10.3389/fphys.2017.00989
92. Gu Q, Wu S-J, Zheng Y, Zhang Y, Liu C, Hou J-C, et al. Tai Chi exercise for patients with chronic heart failure: a meta-analysis of randomized controlled trials. Am J Phys Med Rehabil. (2017) 96:706–16. doi: 10.1097/PHM.0000000000000723
93. Gouw VXH, Jiang Y, Seah B, He H, Hong J, Wang W. Effectiveness of internal Qigong on quality of life, depressive symptoms and self-efficacy among community-dwelling older adults with chronic disease: a systematic review and meta-analysis. Int J Nurs Stud. (2019) 99:103378. doi: 10.1016/j.ijnurstu.2019.06.009
94. Harling A, Simpson JP. A systematic review to determine the effectiveness of Tai Chi in reducing falls and fear of falling in older adults. In: Database of Abstracts of Reviews of Effects (DARE): Quality-assessed Reviews. York: Centre for Reviews and Dissemination (2008). doi: 10.1179/174328808X309241
95. Park M, Song R. Effects of Tai Chi on fall risk factors: a meta-analysis. J Korean Acad Nurs. (2013) 43:341–51. doi: 10.4040/jkan.2013.43.3.341
96. Huang ZG, Feng YH, Li YH, Lv CS. Systematic review and meta-analysis: tai Chi for preventing falls in older adults. BMJ Open. (2017) 7:e013661. doi: 10.1136/bmjopen-2016-013661
97. Lomas-Veja R, Obrero-Gaitán E, Molina-Ortega FJ, Del-Pino-Casado R. Tai, Chi for Risk of Falls. A Meta-analysis. J Am Geriatr Soc. (2017) 65:2037–43. doi: 10.1111/jgs.15008
98. Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson LM, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. (2012) 2012:CD007146. doi: 10.1002/14651858.CD007146.pub3
99. Wua Y, Wangab Y, Burgessa EO, Wu J. The effects of Tai Chi exercise on cognitive function in older adults: a meta-analysis. J Sport Health Sci. (2013) 2:193–203. doi: 10.1016/j.jshs.2013.09.001
100. Zhang Q, Hu J, Wei L, Cao R, Ma R, Song H, et al. Effects of traditional Chinese exercise on cognitive and psychological outcomes in older adults with mild cognitive impairment. A systematic review and meta-analysis. Medicine. (2019) 98:e14581. doi: 10.1097/MD.0000000000014581
101. Wayne PM, Walsh JN, Taylor-Piliae RE, Wells RE, Papp KV, Donovan NJ, et al. The Impact of Tai Chi on cognitive performance in older adults: a systematic review and meta-analysis. J Am Geriatr Soc. (2014) 62:25–39. doi: 10.1111/jgs.12611
102. Du S, Dong J, Zhang H, Jin S, Xu G, Liu Z, et al. Tai chi exercise for self-rated sleep quality in older people: a systematic review and meta-analysis. Int J Nurs Stud. (2015) 52:368–79. doi: 10.1016/j.ijnurstu.2014.05.009
103. Wang C, Collet JP, Lau J. The effect of Tai Chi on health outcomes in patients with chronic conditions: a systematic review. Arch Intern Med. (2004) 164:493–501. doi: 10.1001/archinte.164.5.493
104. Guo Y, Shi H, Yu D, Qiu P. Health benefits of traditional Chinese sports and physical activity for older adults: a systematic review of evidence. J Sport Health Sci. (2016) 5:270–80. doi: 10.1016/j.jshs.2016.07.002
105. Li F, Harmer P, Fitzgerald K, Eckstrom E, Stock R, Galver J, S. Tai chi and postural stability in patients with Parkinson's disease, et al. N Engl J Med. (2012) 366:511–9. doi: 10.1056/NEJMoa1107911
106. Yeh GY, McCarthy EP, Wayne PM, Stevenson LW, Wood MJ, Forman D, et al. Tai chi exercise in patients with chronic heart failure: a randomized clinical trial. Arch Intern Med. (2011) 171:750–7. doi: 10.1001/archinternmed.2011.150
107. Del-Pino-Casado R, Obrero-Gaitán E, Lomas-Veja R. The effect of Tai Chi on reducing the risk of falling: a systematic review and meta-analysis. Am J Chin Med. (2016) 44:895–906. doi: 10.1142/S0192415X1650049X
108. Hu YN, Chung YJ, Yu HK, Chen YC, Tsai CT, Hu GC. Effect of Tai Chi exercise on fall prevention in older adults: systematic review and meta-analysis of randomized controlled trials. Int J Gerontol. (2016) 10:131–6. doi: 10.1016/j.ijge.2016.06.002
109. Lee MS, Lee E, Ernst E. Is tai chi beneficial for improving aerobic capacity? A systematic review. J Britânico Med Esportiva. (2009) 43:569–73. doi: 10.1136/bjsm.2008.053272
110. Zou L, Wang H, Xiao Z, Fang Q, Zhang M, Li T, et al. Tai chi for health benefits in patients with multiple sclerosis: a systematic review. PLoS ONE. (2017) 12:e0170212. doi: 10.1371/journal.pone.0170212
111. Hartley L, Flores N, Lee MS, Ernst E, Rees K. Tai chi for primary prevention of cardiovascular disease. Cochrane Database Syst Rev. (2014) CD010366. doi: 10.1002/14651858.CD010366.pub2
112. Li SYH, Bressington D. The effect of mindfulness-based stress reduction on depression, anxiety, and stress in older adults: a systematic review and meta-analysis. Int J Ment Health Nurs. (2019) 28:635–56. doi: 10.1111/inm.12568
113. Easwaran K, Gopalasingam Y, Green DD, Lach V, Melnyk JA, Wan C, et al. Effectiveness of Tai Chi for health promotion for adults with health conditions: a scoping review of Meta-analyses. Disabil Rehabil. (2021) 43:2978–89. doi: 10.1080/09638288.2020.1725916
114. Choo YT, Jiang Y, Hong J, Wang W. Effectiveness of Tai Chi on quality of life, depressive symptoms and physical function among community-dwelling older adults with chronic disease: a systematic review and meta-analysis. Int J Nurs Stud. (2020) 111:103737. doi: 10.1016/j.ijnurstu.2020.103737
115. Taylor-Piliae RE, Finley BA. Tai Chi exercise for psychological well-being among adults with cardiovascular disease: a systematic review and meta-analysis. Eur J Cardiovasc Nurs. (2020) 19:580–91. doi: 10.1177/1474515120926068
116. Chewning B, Hallisy KM, Mahoney JE, Wilson D, Sangasubana N, Gangnon R. Disseminating Tai Chi in the community: promoting home practice and improving balance. Gerontologist. (2020) 60:765–75. doi: 10.1093/geront/gnz006
117. Zhu R, Wang W, Zhao L, Mao S. Comparisons of tai chi and Iyengar yoga intervention effects on muscle strength, balance, and confidence in balance. J Sports Med Phys Fitness. (2021) 61:1333–8. doi: 10.23736/S0022-4707.20.11752-3
118. Kasim NF, Veldhuijzen van Zanten J, Aldred S. Tai Chi is an effective form of exercise to reduce markers of frailty in older age. Exp Gerontol. (2020) 135:110925. doi: 10.1016/j.exger.2020.110925
119. Weber M, Schnorr T, Morat M, Morat T, Donath L. Effects of mind-body interventions involving meditative movements on quality of life, depressive symptoms, fear of falling and sleep quality in older adults: a systematic review with meta-analysis. Int J Environ Res Public Health. (2020) 17:6556. doi: 10.3390/ijerph17186556
120. Liu F, Cui J, Liu X, Chen KW, Chen X, Li R. The effect of tai chi and Qigong exercise on depression and anxiety of individuals with substance use disorders: a systematic review and meta-analysis. BMC Compl Med Ther. (2020) 20:161. doi: 10.1186/s12906-020-02967-8
121. Kamieniarz A, Milert A, Grzybowska-Ganszczyk D, Opara J, Juras G. Tai Chi and Qi Gong therapies as a complementary treatment in Parkinson's disease – a systematic review. Compl Ther Med. (2021) 56:102589. doi: 10.1016/j.ctim.2020.102589
122. Carvalho LP, Décary S, Beaulieu-Boire I, Dostie R, Lalonde I, Texier É, et al. Baduanjin Qigong Intervention by Telerehabilitation (TeleParkinson): a proof-of-concept study in Parkinson's disease. Int J Environ Res Public Health. (2021) 18:6990. doi: 10.3390/ijerph18136990
123. Lopez G, Narayanan S, Christie A, Powers-James C, Liu W, Garcia MK, et al. Effects of center-based delivery of Tai Chi and Qi Gong group classes on self-reported symptoms in cancer patients and caregivers. Integr Cancer Ther. (2020) 19:1534735420941605. doi: 10.1177/1534735420941605
124. Zeng ZP, Liu YB, Fang J, Liu Y, Luo J, Yang M. Effects of Baduanjin exercise for knee osteoarthritis: a systematic review and meta-analysis. Compl Ther Med. (2020) 48:102279. doi: 10.1016/j.ctim.2019.102279
125. Guan Y, Hao Y, Guan Y, Wang H. Effects of Baduanjin exercise on essential hypertension: a meta-analysis of randomized controlled trials. Medicine. (2020) 99:e21577. doi: 10.1097/MD.0000000000021577
126. Zheng G, Zheng Y, Xiong Z, Ye B. Effect of Baduanjin exercise on cognitive function in patients with post-stroke cognitive impairment: a randomized controlled trial. Clin Rehabil. (2020) 34:1028–39. doi: 10.1177/0269215520930256
127. Ye M, Xiong J, Zhao F, Sun S, Wang L, Zheng G. Comparison of traditional Chinese exercises and nontraditional chinese exercise modalities on cognitive and executive function in community middle-aged and older adults: a cross-sectional study. Evid Based Compl Altern Med. (2020) 2020:4380805. doi: 10.1155/2020/4380805
128. Yao LQ, Tan JY, Turner C, Wang T, Liu XL. Traditional Chinese exercise for cancer-related sleep disturbance: a systematic review and descriptive analysis of randomized controlled trials. Compl Ther Clin Pract. (2020) 40:101197. doi: 10.1016/j.ctcp.2020.101197
129. Wang C, Liang J, Si Y, Li Z, Lu A. The effectiveness of traditional Chinese medicine-based exercise on physical performance, balance and muscle strength among older adults: a systematic review with meta-analysis. Aging Clin Exp Res. (2021). doi: 10.1007/s40520-021-01964-2. [Epub ahead of print].
130. Godley E, Smith MA. Efficacy of acupressure for chronic low back pain: a systematic review. Compl Ther Clin Pract. (2020) 39:01146. doi: 10.1016/j.ctcp.2020.101146
131. Griffiths JD, Gyte GML, Popham PA, Williams K, Paranjothy S, Broughton HK, et al. Interventions for preventing nausea and vomiting in women undergoing regional anaesthesia for caesarean section . Cochrane Database Syst Rev. (2021) 2021:CD007579. doi: 10.1002/14651858.CD007579.pub3
132. Smith CA, Collins CT, Levett KM, Armour M, Dahlen HG, Tan AL, et al. Acupuncture or acupressure for pain management during labour. Cochrane Database Syst Rev. (2020) 2:CD009232. doi: 10.1002/14651858.CD009232.pub2
133. Alimoradia Z, Kazemi F, Gorjic M, Valiani M. Effects of ear and body acupressure on labor pain and duration of labor active phase: a randomized controlled trial. Compl Ther Med. (2020) 51:102413. doi: 10.1016/j.ctim.2020.102413
Keywords: mind-body therapies, traditional Chinese medicine, Tai Chi, Qi Gong, evidence map, public health
Citation: Fogaça LZ, Portella CFS, Ghelman R, Abdala CVM and Schveitzer MC (2021) Mind-Body Therapies From Traditional Chinese Medicine: Evidence Map. Front. Public Health 9:659075. doi: 10.3389/fpubh.2021.659075
Received: 26 January 2021; Accepted: 08 November 2021;
Published: 10 December 2021.
Edited by:
Hélio José Coelho Júnior, Catholic University of the Sacred Heart, ItalyReviewed by:
Li-Fan Liu, National Cheng Kung University, TaiwanRhayun Song, Chungnam National University, South Korea
Copyright © 2021 Fogaça, Portella, Ghelman, Abdala and Schveitzer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariana Cabral Schveitzer, bWFyaWFuYS5jYWJyYWxAdW5pZmVzcC5icg==