 Christine Wolter
Christine Wolter Tino Lesener
Tino Lesener Tobias Alexander Thomas
Tobias Alexander Thomas Alicia-Carolin Hentschel1
Alicia-Carolin Hentschel1 Burkhard Gusy
Burkhard Gusy
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 10 June 2021
Sec. Public Health Education and Promotion
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.653435
This article is part of the Research TopicPublic Health Promotion in University StudentsView all 15 articles
Introduction: Heavy alcohol consumption constitutes a major health risk among University students. Social relationships with peers strongly affect University students' perception of the drinking behavior of others, which in turn plays a crucial role in determining their own alcohol intake. University students tend to overestimate their peers' alcohol consumption – a belief that is associated with an increase in an individual's own consumption. Therefore, we implemented a social norms intervention with personalized normative feedback at a major University in Germany to reduce and prevent excessive drinking among University students.
Methods: Our intervention was part of a regular health monitoring survey. We invited all enrolled University students to take part in this survey on two occasions. A total of 862 University students completed the questionnaire, 563 (65.3%) of which received e-mail-based feedback upon request concerning their peers' and their own alcohol consumption. For the intervention group (n = 190) as well as the control group (no feedback requested; n = 101), we included only University students in the evaluation who overestimated their peers' alcohol use and indicated above average consumption of the peers. We applied analyses of variance to assess intervention effects with regard to the correction of overestimated group norms as well as University students' drinking behavior.
Results: Within the intervention group, we observed a significantly larger reduction of the previously overestimated behavioral norms compared to the control group (p < 0.001; = 0.06). With regard to behavioral outcomes the intervention group showed a significantly larger reduction in the AUDIT-C score (p = 0.020; = 0.03).
Discussion: Our study confirms previous research whereupon personalized, gender-specific and selective normative feedback is effective for alcohol prevention among University students. However, University students still overestimated their peers' alcohol intake after the intervention. Furthermore, we did not reach high-risk groups (University students with the highest alcohol intake) since no feedback was requested. Future studies should address factors influencing the impact of the intervention and reachability of selective groups.
Harmful use of alcohol causes about 3 million deaths each year and more than 130 million disability-adjusted life years (1). The mortality caused by alcohol is higher than that caused by diseases such as tuberculosis, HIV/AIDS, or diabetes (1). Constant alcohol use causes social impairments and increases the risk for various serious diseases, like alcoholic cirrhosis, tumors and cancer, as well as premature mortality (2, 3). Especially younger adults are disproportionally affected by alcohol: More than 13% of all deaths between 20 and 39 are attributed to harmful use of alcohol (1). The highest prevalence rates of alcohol use disorders are in high-income countries, especially in Europe and in the US. Heavy alcohol consumption is also highly prevalent among young adults in Germany: 42% of men and 33% of women between 18 and 29 display heavy consumption patterns (4). Research suggests that—within this age group—University students tend to drink even more (5, 6) and also more frequently (5) than their non-University peers. Alcohol consumption is widespread among German University students: On average, two thirds of the University students drink alcohol at least twice a month. Nearly one third of the University students report binge drinking at least once a month, and more than 40% show problematic drinking behavior, i.e., an AUDIT-C sum of at least 3 in women and at least 4 in men (7).
Consequently, and due to these high prevalence rates of heavy alcohol consumption and negative outcomes concerning health, social life and society in general there is a particularly high urgency to address the alcohol consumption of University students with proper interventions in order to prevent early-onsets of heavy drinking behavior. These interventions need to simultaneously reduce the harmful use of alcohol and strengthen responsible and low-risk handling of alcohol.
Heavy drinking behavior is affected by intrapersonal and interpersonal social and normative factors (8). Among University students, social relationships with peers play a crucial role for their drinking behavior (9). Accordingly, University students report drinking motives such as social enhancement, enjoyment, and socialization (10, 11). As a pioneer of social conformity theory, Asch (12) showed the impact of social pressure on individual behavior more than six decades ago. The perception of others' behavior—especially peers—affects University students' alcohol consumption through social norms as social influences (13). Moreover, University students adopt the drinking patterns they perceive in their peers. To prevent heavy alcohol consumption, interventions could therefore address social influences through social norms.
The perception of behavior is biased and therefore often differs from the behavior actually shown (14). This discrepancy is particularly noticeable in alcohol consumption (15, 16). The core of such misperceptions usually lies in an overestimation of others' risk behaviors and an underestimation of health-promoting behaviors (13). Several studies at US (17–19) as well as European universities (20–22) showed that University students systematically overestimate their peers' alcohol consumption. Thus, the fact—and behavioral norm—that the majority of University students use alcohol responsibly is disguised by individual misperceptions (19). Within literature on the causes for this overestimation, there are several explanations: First, it is argued that overestimation is due to the size of the peer group. As there is little/no information about unknown persons within the peer group there is a lack of information on their alcohol use and thus overestimation occurs (23, 24). Second, it was postulated that among the peer group only close peers (e.g., significant others) are used for estimating alcohol use. Thus, overestimation is a product of “underinclusion” as significant others are only a part of the peer group. However, this approach was disproved when being tested empirically (25). Third, it is proposed that this overestimation is due to a cognitive bias resulting in better memory and attention for more extreme behavioral patterns. Furthermore, this more extreme behavior is regarded as transsituationally consistent (26). Finally, overestimation of peers' alcohol use is found to be moderated by time (e.g., “seasonal effects”) as well by own alcohol intake as well as by a loss of self-control (25). This may eventually result in risky drinking behavior since misperceived behavioral norms may encourage individuals to adapt their alcohol intake to what they (mis-)perceive in their peers (13). The social norms intervention and personalized normative feedback approaches promisingly attempt to break this cycle [i.e., “you (unintentionally) drink more because you expect higher intake levels of your own based on peers' evaluation”; (13)].
The social norms intervention (SNI) is a health-promoting intervention that aims to correct misperceptions by providing information about the behavioral norm in a population in order to support more health-conscious decision-making processes (27). This intervention approach assumes that correcting the misperceived behavioral norm by replacing it with the actual norm reduces the individual's pressure with regard to the mistakenly overestimated peer consumption (27). The SNI is based on two basic assumptions: (1) accurate information about the beliefs and behaviors of relevant others is not always known and salient, (2) providing the behavioral norm may change the understanding of group norms and one's own position within the group (28). The SNI differs from traditional behavioral change approaches. It focuses on indirect methods of persuasion by presenting information about (health-conscious) behavioral norms that already exist within a group (29). SNIs do not aim to change the behavioral norms but to correct misperceptions of that behavioral norm (13). The given information is a positive statement showing that responsible and moderate behavior is the behavioral norm, and that the group majority acts and thinks health-consciously (30).
With personalized normative feedback (PNF), each person receives individual, personal feedback, e.g., on their own as well as their peers' alcohol consumption (28). For this purpose, a mode of communication is chosen that allows for this kind of feedback, like face-to-face conversations in counseling (31), e-mails (32) or web-based messages via a personal link to a website (33).
Intervention studies (34–38) and systematic reviews (27, 39, 40) demonstrate small to medium effects of SNIs on various alcohol-related outcomes such as drinking quantity, frequency and risky drinking. However, these results often do not persist in the long term. Neighbors et al. (37) showed significant short-term effects of their intervention (PNF, specifically) but no long-term effects on the individual estimation of the behavioral norms, alcohol frequency and quantity. Foxcroft et al. (41) reported inconsistent results in their meta-analytical review: While some studies found significant short- and long-term effects of SNIs and PNFs on alcohol quantity and binge drinking, other studies did not [see also (42)]. Additionally, the overall effect size was very small. However, Dotson et al. (43) declared even small effects as clinically relevant from a public health perspective. Referring to the “prevention paradox” even small improvements at the individual level might achieve large health gains at the population level. In their review, PNF was proven an effective stand-alone approach for reducing college student drinking (43). Moreover, some recent studies were able to obtain medium- and long-term effects of PNFs on drinking frequency after 3 months (44) and drinking prevalence after 6 months (45).
PNF has proven to be effective in correcting misperceived drinking behavioral norms (37, 46, 47). This modification of misperceived behavioral norms has been found to mediate the relationship between PNF and behavioral outcomes with regard to reduced drinking levels (38, 47–49).
Several aspects might improve the efficacy of SNIs, such as the frequency, the reference group, or the selection of the intervention group. Samson and Tanner-Smith (50) meta-analytically showed that even one single session of PNF might have the same positive impact on alcohol consumption in the short- and medium-term as motivational enhancement therapy, motivational interviewing, or even more elaborated techniques. Most PNF interventions refer to “typical University students” as the normative peer group (43, 51). However, recent research highlights the importance of personal significance of the reference group to the individual. Close reference persons such as friends or peers, as well as factors like specificity (e.g., gender specificity) seem to have a greater impact on individual alcohol consumption than less close or specific reference groups such as “typical University students” (35, 52–54). Furthermore, Haug et al. (55) argue for selective SNI for persons who consume more alcohol than the average, as the intervention was more effective in studies that pre-selected persons with problematic alcohol use [see also (48)].
In summary, research shows that email-based PNF for alcohol prevention and reduction of alcohol consumption is effective among University students. Interventions seem to be most effective when they are personalized, gender-specific, and targeted at University students who drink more alcohol than the average of their peers.
While interventions based on social norms are popular and widely applied at US universities, interventions that address University students in Europe and especially Germany are rare (41). SNIs have established themselves in the US as a meaningful way to reduce alcohol consumption. In order to popularize this type of intervention in Germany, the effects of an SNI were tested in this study.
Based on the existing evidence, we expect the effects of our PNF to be two-fold: First, we expect a correction of University students' misperceived behavioral norms with regard to their peers' alcohol consumption. Second, we expect a reduction of alcohol intake on the behavioral level.
The intervention aims to specifically address students who overestimate their peers' alcohol consumption and consume more than the average of their peers. Consequently, our hypotheses are:
Hypothesis 1: The intervention (personalized normative feedback) corrects misperceived behavioral norms in University students who overestimate the alcohol intake of their peers and consume more alcohol than the average of their peers at 12 weeks after the intervention.
Hypothesis 2: The intervention (personalized normative feedback) reduces levels of alcohol intake on the behavioral level in University students who overestimate the alcohol intake of their peers and consume more alcohol than the average of their peers at 12 weeks after the intervention.
Our intervention was part of a general health monitoring survey at a major University in Germany. The survey covered University students' perception of study characteristics, health outcomes as well as their health behavior. All University students enrolled at the University were invited to take part in the survey. The survey was conducted twice (January/February and June/July 2019), with a total of 862 University students (mean age: 24 years; see Figure 1) participating. Two months (6–10 weeks) after the first survey, 563 (65.3%) University students received feedback upon request concerning their own and their peers' alcohol consumption. In the second survey, 432 (76.7%) University students of those who had received feedback indicated that they had actually read the feedback. University Students who had not taken part in the intervention (no feedback requested or not read the feedback) were assigned to the control group. The gender ratio (♀:♂) was 3:1 in each group. All subjects answered the questions on alcohol consumption on both occasions.
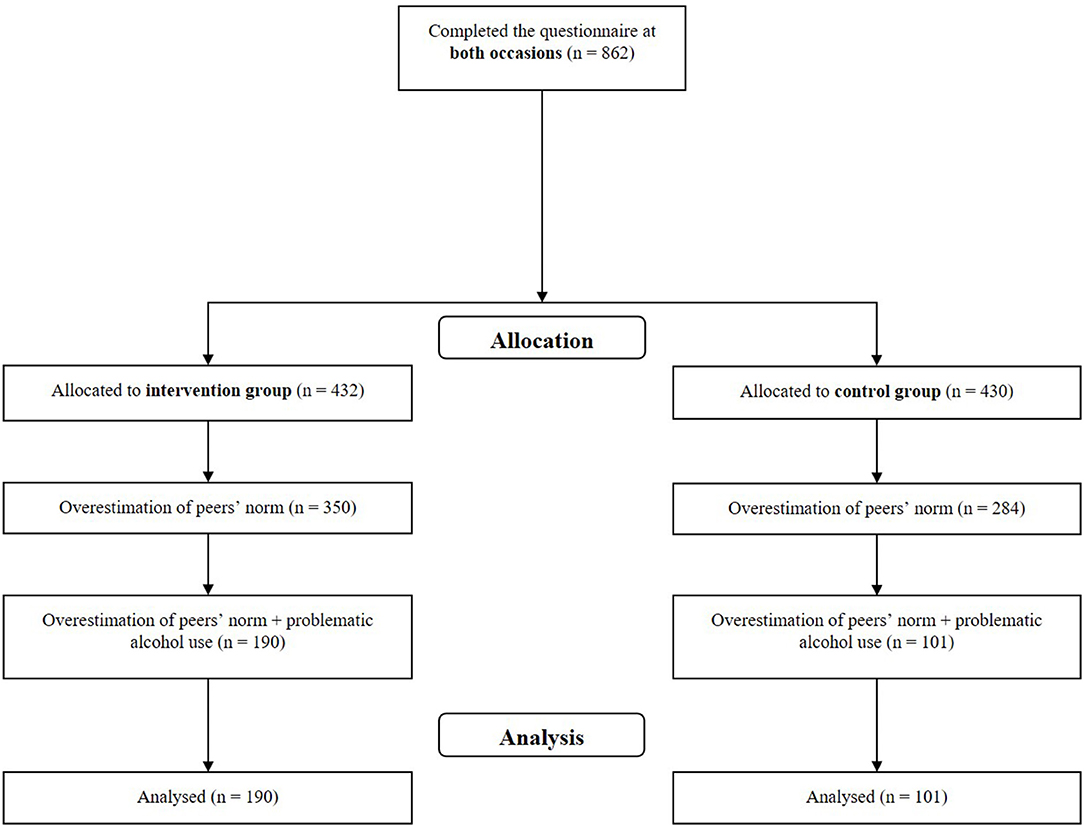
Figure 1. Flowchart of our study.
Within our a-priori defined subgroup analysis, we included only University students who overestimated their peers' alcohol consumption and who had indicated above average own consumption compared to the median of the peers' consumption. We refer to above average alcohol consumption as “heavy drinking.” No randomized assignment to the groups was possible. Consequently, 190 students fulfilling these criteria and were assigned to the intervention group and 101 students that also met these criteria to the control group. Those who did not fulfill inclusion criteria but wanted feedback were also given feedback. Thus, every University student requesting feedback received one.
To assess University students' individual alcohol intake, we used the Alcohol Use Disorders Identification Test Consumption [AUDIT-C; (56)]. The AUDIT-C consists of three items of the original 10-item AUDIT. Each question (e.g., “How often do you drink an alcoholic beverage e.g., one glass of wine, beer, cocktail, schnapps or liqueur?”) is scored from 0 (e.g., “never”) to 4 (e.g., “6 or more times a week”) points, resulting in a score from 0 to 12. An AUDIT-C score of 0 means that participants never drink alcohol.
We utilized frequency-quantity-indices, combined values containing information about both frequency and quantity of alcohol use, within our analyses. These indices were also applied to assess the department- and gender-specific individually estimated group norm. We first asked University students to evaluate their peers' alcohol intake with regard to frequency (“How often does the majority of all female students in your department drink an alcoholic beverage e.g., one glass of wine, beer, cocktail, schnapps or liqueur?”) and quantity [“How many alcoholic beverages does the majority of all female students in your department usually drink per drinking occasion? One alcoholic beverage (standard drink) is a small bottle of beer (0,33l), a small glass of wine or sparkling wine (0,125l) or a double schnapps (4cl)”]. The items were adopted from AUDIT-C for estimation of peers' alcohol frequency and quantity. We then multiplied frequency and quantity and thus obtained the frequency-quantity index for the individually estimated group norm.
We computed another frequency-quantity index indicating the behavioral norm (i.e., median of peers' alcohol frequency multiplied with median of peers' alcohol quantity) and compared them by using a difference value (individually estimated group norm – behavioral norm) for the two frequency-quantity indices. By using the term overestimation, we refer to any difference value > 0 (meaning the individually estimated group norm is larger than the behavioral norm). We utilized frequency-quantity-indices, combined values containing information about both frequency and quantity of alcohol use, within our analyses. These indices were also applied to assess the department- and gender-specific individually estimated group norm. We first asked University students to evaluate their peers' alcohol intake with regard to frequency (“How often does the majority of all female students in your department drink an alcoholic beverage e.g., one glass of wine, beer, cocktail, schnapps or liqueur?”) and quantity [“How many alcoholic beverages does the majority of all female students in your department usually drink per drinking occasion? One alcoholic beverage (standard drink) is a small bottle of beer (0,33l), a small glass of wine or sparkling wine (0,125l) or a double schnapps (4cl)”]. The items were adopted from AUDIT-C for estimation of peers' alcohol frequency and quantity. We then multiplied frequency and quantity and thus obtained the frequency-quantity index for the individually estimated group norm.
In 2016, we started the project ISPI (“Internet, Studierende, Peers & Intervention”) in cooperation with the Leibniz-Institut für Präventionsforschung und Epidemiologie in Bremen and implemented a first intervention. This 2016 intervention resulted in a change of difference to norms but not a change of behavior regarding the alcohol consumption of University students (57).
With the current intervention, we tried to strengthen and expand the effects of 2016. We further personalized the reference group for the University students by not only specifying it to their gender but also to their study department. With an even smaller comparison group we wanted to reach a higher degree of identification and a stronger effect of the intervention on both group norms and behavior. Additionally, we revised and clarified the normative feedback. We used PNF in the form of e-mails to reach as many University students as possible. One crucial advantage of e-mail-based interventions is that participants can access the information at any time or place whilst also protecting their anonymity (58). SNI with PNF represents a stand-alone, e-mail-based, personalized, normative feedback intervention.
The University students received feedback concerning their own as well as their peers' alcohol intake with regard to frequency and quantity as well as binge drinking behavior (defined as six or more alcoholic drinks per drinking occasion). The feedback consisted of three parts. In the first part, the University students received feedback of what they had indicated with regard to their own alcohol consumption (e.g., “You stated that you consume alcohol 3 to 4 times per week, usually 1 alcoholic drink per drinking occasion.” / “You stated that you drink more than 6 alcoholic drinks per drinking occasion once a month.”). In the second part, the University students received feedback with regard to their estimated alcohol intake of their peers i.e., the (mis-)perceived group norm (e.g., “You suppose, that the majority of the female students in your department consume alcohol 3–4 times per week, usually 2 alcoholic drinks per drinking occasion.”). In the third part, the students received feedback about their peers' alcohol intake (behavioral norm e.g., “In fact, the majority of the female students in your department consume alcohol 1–2 times per week, usually 2 alcoholic drinks per drinking occasion.”). Lastly, the University students received a statement indicating whether their alcohol intake was similar or above that of their peers.
We applied analyses of covariance (ANCOVA) to assess intervention effects with regard to the correction of overestimated group norms as well as University students' drinking behavior. We considered age, sex, self-efficacy and depressive symptoms as covariates. To evaluate the correction of overestimated group norms, we first calculated a frequency-quantity-index for the estimated as well as behavioral norms. Subsequently, we calculated a difference value between the individually estimated group norm (perceived alcohol intake of peers) and the behavioral norm (median, department- and gender-specific). With these indicators, we analyzed the difference values of both occasions for the intervention and control group. Finally, we assessed the changes in intervention and control group drinking behavior by comparing the AUDIT-C scores prior to and after the intervention. We used a 0.05 significance level.
We first identified the gender- and subject-specific behavioral norms for drinking frequency and drinking quantity that were also part of the intervention (feedback). Due to the high number of different behavioral norms that we computed for every gender and subject combination we only constitute the range of behavioral norms for the several combinations: Behavioral norms for quantity varied from 2 drinks to 4.5 drinks and behavioral norms for frequency varied from 1 time per month to 1–2 times per week.
With regard to hypothesis 1—the correction of overestimated individually estimated drinking norms—we observed a significantly larger reduction in the difference value (between the individually estimated group norm and the behavioral norm) in the intervention group compared to the control group [F(2) = 8.46, p < 0.001, = 0.06]. This confirms hypothesis 1, namely that the intervention would correct misperceived individually estimated group norms in the intervention group.
With regard to hypothesis 2—the reduction of alcohol intake—we observed a significant reduction in their AUDIT-C scores [F(2) = 3.96, p = 0.020; = 0.03]. Hence, the behavioral outcomes were in line with our hypothesis 2. Corrected means, standard deviations and test statistics of the outcome measures are depicted in Table 1.
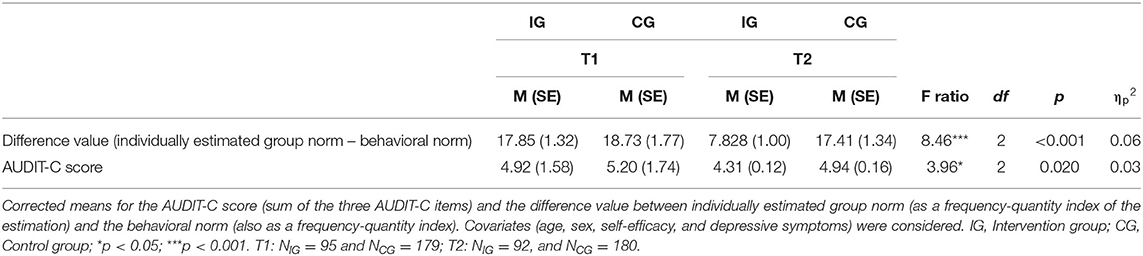
Table 1. Corrected Means and test statistics of the ANCOVA outcome measures.
We investigated whether a personalized, gender-specific social norms intervention for University students would affect their perception of their peers' alcohol intake as well as their own drinking behavior. Specifically, we compared the effects in the intervention group with a control group. Since most studies on SNI in University students were conducted in the USA, Australia, Brazil, New Zealand, Sweden, or the United Kingdom (41), our intervention constitutes one of the first studies evaluating SNI in German University students.
Our results are in line with our hypotheses. In contrast to the control group, participants in the intervention group ended up with a more realistic perception of their peers' alcohol intake. However, their perception was still above the group norm. Furthermore, participants of the intervention group reported a significantly larger reduction in the AUDIT-C score, which means that—compared to the control group—they drank less and less often after the intervention. However, their drinking level was still high yet lowered.
Our results confirm prior SNI research that found that University students reported significant decreases of their alcohol intake [e.g., (59, 60)]. There has, however, been serious criticism concerning SNI use with European populations. John and Alwyn (61) argue that there are important differences in campus life and in the definitions of alcohol misuse or heavy drinking between the UK and the US. They consider SNIs to be an ineffective tool in tackling heavy drinking behavior in European populations. Contrastingly, our study was able to validate SNI's efficacy in a European population and thus makes a valuable contribution to the knowledge about SNI.
We decided to use PNF in the form of e-mails to reach as many University students as possible. Since we integrated the intervention into our regular health monitoring survey, we showed that it is possible to implement both, health assessment and intervention simultaneously. This is a very effective and cost-efficient method. Still, there are several other feedback delivery options, in particular web/computer feedback, individual face-to-face feedback, group face-to-face feedback and general social norms marketing campaigns. In some cases, like when the intervention targets specific and small courses, it may be more appropriate to choose another delivery method, e.g., face-to-face feedback. Overall though, (e-)mailed feedback has been identified as one of the best delivery options for SNI (41).
The feedback in our study was department- and gender-specific. We do not know whether the overestimation of the group norms was affected by this choice of reference group. Galesic et al. (23) propose that the overestimation of people's behavior results from judging the behavior of a rather unfamiliar sample. Consequently, assessing the behavior of acquainted others might yield more realistic estimations. However, Giese et al. (25) have disproven this hypothesis. They showed that overestimation still occurs even when the reference group comprises only familiar people.
Not much research exists concerning the content and precise wording of the feedback. When studying the efficacy of a campaign to correct social group norm, Thombs et al. (62) found that only 38.5% of their sample understood the intended purpose of the campaign and its intervention. Therefore, we decided to not only include the participant's own and their peers' alcohol intake in the feedback but to also explicitly state whether the participant's alcohol intake was similar or above that of their peers. We also added whether or not their consumption would be categorized as problematic. We hoped that this information would made the feedback's intention easier to understand.
Furthermore, it is still rather unclear why SNI are more effective for some University students than for others. Giese et al. (25) have shown that University students with high self-control make more realistic estimations of their peers' alcohol consumption. There may be several other individual characteristics that impact the efficacy of SNI. We need much more knowledge on why University students overestimate peers' alcohol intake, and which University students are most vulnerable to such an overestimation, in order to target SNI most effectively. Other SNI studies suggest that several other contextual factors may influence its efficacy, e.g., social and environmental factors [availability of alcohol, acceptance of alcohol consumption in public; (63)]. Future research could also operationalize and control these social and environmental factors.
Our intervention is not free of shortcomings.
First, we used the AUDIT-C as an efficient, reliable and valid measure to assess the alcohol intake of the participants as well as the alcohol intake of their peers. The AUDIT-C has been successfully applied in previous SNIs (41). However, more direct behavioral measures such as the Alcohol Timeline Followback [TLFB; (64)] might be better suited to examining alcohol consumption and thus the effects of the intervention.
Second, a larger sample size might have improved and expanded our results. Since we included the intervention in our regular health monitoring survey, only 190 University students met our inclusion criteria for the intervention that we formulated a-priori (University students who overestimated their peers' alcohol use and indicated above average own consumption compared to peers' median alcohol use). Most of the studies on SNI targeted University students with increased risk (41), however, it may also be important to consider the intervention as a prevention tool for those who are not (yet) at increased risk or even at low-risk University students [e.g., (65)]. Furthermore, almost 75% of the participants were female, which also limits the generalizability of our results.
Third, we promised all interested University students who participated in our health monitoring survey a detailed feedback on their and their peers' alcohol intake, regardless of whether their intake was above the group norm. Hence, we did not randomly assign survey participants to either intervention or control group. A randomized assignment did not seem ethically justifiable as this would mean withholding the intervention from the control group or at least postponing their intervention. However, this selection procedure involves several shortcomings, especially the limited comparability between intervention and control group. Thus, we cannot rule out potential selection biases as would be possible with randomized control trials (RCT). RCTs randomly assign participants to either intervention or control group. Thus, RCTs are more comparative, minimize several biases (e.g., allocation or selection bias) and also minimize confounding factors. Since RCTs are the gold standard in interventional research, future studies should preferably use this design. Nevertheless, our design allowed us to control for known confounders and we therefore used sex, age, self-efficacy, and depressive symptoms as covariates within the ANCOVAs.
Fourth, although we asked participants if they received the intervention, we cannot be sure whether all of them read their feedback carefully and attentively. As described above, feedback of earlier studies was sometimes not clear enough, so we tried to keep the feedback as easy and understandable as possible. We are certain that the majority of University students was able to interpret it correctly.
Fifth, we used the second survey of our health monitoring to capture the effects of the intervention. This second survey was 12–16 weeks after the intervention. Unfortunately, we were not able to evaluate any long-term effects (e.g., after 1 year).
Sixth, we were able to observe significant differences in difference to norm (individually estimated group norm – group norm), AUDIT-C score. These effects were rather small in terms of effect sizes. However, in line with the prevention paradox, even small effect sizes can make a difference in such interventions.
Our study proves SNI's overall efficacy in both norm and behavioral outcome variables. It is one of the first studies applying SNI in a German student sample. Since we focused on University students with overestimation of the group norm and an above average alcohol intake, we examined SNI's effect not only on University students with harmful alcohol consumption. Our intervention successfully addressed alcohol intake in University students with above average alcohol use. Therefore, SNI can also be used as a primary preventive instrument reducing alcohol use not only in those with problematic alcohol use.
Our study furthermore shows that it is possible to integrate SNI into regular health monitoring. This is an effective, cost-efficient, and pragmatic way to combine both, screening and intervention of alcohol misuse in University students. Along with environmental interventions and possible restrictions of alcohol promotion, SNI may be one important piece in the prevention of health problems due to alcohol misuse (59).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics committee Freie Universität Berlin; FB Erziehungswissenschaft & Psychologie. The patients/participants provided their written informed consent to participate in this study.
CW, TL, and BG: conceptualization, investigation, validation, data curation, and project administration. CW, TL, BG, and TT: methodology. CW: formal analysis. CW, TL, BG, and A-CH: writing—original draft preparation. TL, CW, BG, A-CH, and TT: writing—review and editing. TL and CW: visualization. BG: supervision. All authors contributed to the article and approved the submitted version.
We acknowledge support by the Open Access Publication Initiative of Freie Universität Berlin.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. World Health Organization. Global Status Report on Alcohol and Health 2018. World Health Organization. (2018). Available online at: https://apps.who.int/iris/bitstream/handle/10665/274603/9789241565639-eng.pdf (accessed May 28, 2021).
2. Orth B. Die Drogenaffinität Jugendlicher in der Bundesrepublik Deutschland 2015: Rauchen, Alkoholkonsum und Konsum illegaler Drogen: aktuelle Verbreitung und Trends (BZgA-Forschungsbericht). Köln: Bundeszentrale für gesundheitliche Aufklärung (2016). Available online at: https://www.drogenbeauftragte.de/fileadmin/dateien-dba/Drogenbeauftragte/2_Themen/1_Drogenpolitik/2_Initiativen/DAS_2015_Basis-Bericht_fin.pdf (accessed November 3, 2017).
3. Robert Koch-Institut. Gesundheit in Deutschland – die wichtigsten Entwicklungen (Gesundheitsberichterstattung des Bundes. Gemeinsam getragen von RKI und Destatis). Berlin. (2016). Available online at: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsGiD/2015/kurzfassung_gesundheit_in_deutschland.pdf?__blob=publicationFile (accessed February 2, 2018).
4. Robert Koch-Insitut. Alkoholkonsum: Faktenblatt zu GEDA 2012: Ergebnisse der Studie Gesundheit in Deutschland aktuell 2012. (2014). Available online at: http://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsF/Geda2012/Alkoholkonsum.pdf?__blob=publicationFile
5. Carter AC, Obremski Brandon K, Goldman MS. The college and noncollege experience: a review of the factors that influence drinking behavior in young adulthood. J Stud Alcohol Drugs. (2010) 71:742–50. doi: 10.15288/jsad.2010.71.742
6. Kypri K, Cronin M, Wright CS. Do University students drink more hazardously than their non-student peers? Addiction. (2005) 100:713–4. doi: 10.1111/j.1360-0443.2005.01116.x
7. Grützmacher J, Gusy B, Lesener T, Sudheimer S, Willige J. Gesundheit Studierender in Deutschland 2017 [Health of Students in Germany 2017]: Ein Kooperationsprojekt zwischen dem Deutschen Zentrum für Hochschul- und Wissenschaftsforschung, der Freien Universität Berlin und der Techniker Krankenkasse. (2018). Available online at: https://www.ewi-psy.fu-berlin.de/einrichtungen/arbeitsbereiche/ppg/forschung/BwB/bwb-2017/index.html (accessed May 28, 2021).
8. Lorant V, Nicaise P, Soto VE, d'Hoore W. Alcohol drinking among college students: college responsibility for personal troubles. BMC Public Health. (2013) 13:615. doi: 10.1186/1471-2458-13-615
9. Helmer S. Substanzkonsum von Studierenden und Einflüsse der Peergroup. Über die Bedeutung von sozialen Normen für den legalen und illegalen Substanzkonsum von europäischen Studierenden (Dissertation). Fakultät für Gesundheitswissenschaften der Universität Bielefeld, Bielefeld (2015). Available online at: https://d-nb.info/1073642348/34 (accessed May 28, 2021).
10. Kuntsche E, Knibbe R, Gmel G, Engels R. Why do young people drink? A review of drinking motives. Clin Psychol Rev. (2005) 25:841–61. doi: 10.1016/j.cpr.2005.06.002
11. Park CL. Positive and negative consequences of alcohol consumption in college students. Addictive Behav. (2004) 29:311–21. doi: 10.1016/j.addbeh.2003.08.006
12. Asch SE. Opinions and social pressure. Sci Am. (1955) 193:31–5. doi: 10.1038/scientificamerican1155-31
13. Berkowitz AD. An overview of the social norms approach. In: Lederman LC, Stewart LP, editors. Changing the Culture of College Drinking: A Socially Situated Health Communication Campaign. Hampton Press (2005). p. 193–214. Available online at: https://pdfs.semanticscholar.org/6ef6/20971cfda65d43ec3cac2c2a0cd7bf7c02f0.pdf (accessed August 18, 2017).
14. Cooter RD, Feldman M, Feldman Y. The misperception of norms: the psychology of bias and the economics of equilibrium. Rev. Law Econ. (2006) 4:899–911. doi: 10.2202/1555-5879.1222
15. Haug S, Ulbricht S, Hanke M, Meyer C, John U. Overestimation of drinking norms and its association with alcohol consumption in apprentices. Alcohol Alcoholism. (2011) 46:204–9. doi: 10.1093/alcalc/agq103
16. Kypri K, Langley JD. Perceived social norms and their relation to University student drinking. J Stud Alcohol. (2003) 64:829–34. doi: 10.15288/jsa.2003.64.829
17. Perkins HW, Haines MP, Rice R. Misperceiving the college drinking norm and related problems: a nationwide study of exposure to prevention information, perceived norms and student alcohol misuse. J Stud Alcohol. (2005) 66:470–8. doi: 10.15288/jsa.2005.66.470
18. Perkins HW. Misperceptions of peer drinking norms in Canada: another look at the “reign of error” and its consequences among college students. Addictive Behav. (2007) 32:2645–56. doi: 10.1016/j.addbeh.2007.07.007
19. Perkins HW, Berkowitz AD. Perceiving the community norms of alcohol use among students: some research implications for campus alcohol education programming. Int J Addict. (1986) 21:961–76. doi: 10.3109/10826088609077249
20. Boot CR, Dahlin M, Lintonen T, Stock C, van Hal G, Rasmussen S, et al. A survey study on the associations between misperceptions on substance use by peers and health and academic outcomes in University students in North-West Europe. Int J Disabil Hum Dev. (2012) 11:273–9. doi: 10.1515/ijdhd-2012-0027
21. McAlaney J, Boot CR, Dahlin M, Lintonen T, Stock C, Rasmussen S, et al. A comparison of substance use behaviours and normative beliefs in North-West European University and college students. Int J Disabil Hum Dev. (2012) 11:281–7. doi: 10.1515/ijdhd-2012-0032
22. Riou França L, Dautzenberg B, Reynaud M. Heavy episodic drinking and alcohol consumption in French colleges: the role of perceived social norms. Alcoholism Clin Exp Res. (2010) 34:164–74. doi: 10.1111/j.1530-0277.2009.01078.x
23. Galesic M, Olsson H, Rieskamp J. Social sampling explains apparent biases in judgments of social environments. Psychol Sci. (2012) 23:1515–23. doi: 10.1177/0956797612445313
24. Pape H. Young people's overestimation of peer substance use: an exaggerated phenomenon? Addiction. (2012) 107:878–84. doi: 10.1111/j.1360-0443.2011.03680.x
25. Giese H, Stok FM, Renner B. Perceiving college peers' alcohol consumption: temporal patterns and individual differences in overestimation. Psychol Health. (2019) 34:147–61. doi: 10.1080/08870446.2018.1514118
26. Perkins HW. College student misperceptions of alcohol and other drug norms among peers: exploring causes, consequences, and implications for prevention programs. In: Designing Alcohol and Other Drug Prevention Programs in Higher Education: Bringing Theory Into Practice. (1997). p. 177–206. Available online at: http://alcohol.hws.edu/perkinstheorychapter.pdf (accessed May 28, 2021).
27. Berkowitz AD. The Social Norms Approach: Theory, Research, Annotated Bibliography. Trumansburg, NY (2004). Available online at: http://www.alanberkowitz.com/articles/social_norms.pdf (accessed May 28, 2021).
28. Miller DT, Prentice DA. Changing norms to change behavior. Ann Rev Psychol. (2016) 67:339–61. doi: 10.1146/annurev-psych-010814-015013
29. McAlaney J, Bewick B, Hughes C. The international development of the ‘social norms' approach to drug education and prevention. Drugs Educ Prevent Policy. (2010) 18:81–9. doi: 10.3109/09687631003610977
30. Perkins HW. Social norms and the prevention of alcohol misuse in collegiate contexts. J Stud Alcohol Suppl. (2002) 14:164–72. doi: 10.15288/jsas.2002.s14.164
31. Neighbors C, Lewis MA, Bergstrom RL, Larimer ME. Being controlled by normative influences: self-determination as a moderator of a normative feedback alcohol intervention. Health Psychol. (2006) 25:571–9. doi: 10.1037/0278-6133.25.5.571
32. Larimer ME, Lee CM, Kilmer JR, Fabiano PM, Stark CB, Geisner IM, et al. Personalized mailed feedback for college drinking prevention: a randomized clinical trial. J Consult Clin Psychol. (2007) 75:285–93. doi: 10.1037/0022-006X.75.2.285
33. Neighbors C, Lee CM, Lewis MA, Fossos N, Walter T. Internet-based personalized feedback to reduce 21st-birthday drinking: a randomized controlled trial of an event-specific prevention intervention. J Consult Clin Psychol. (2009) 77:51–63. doi: 10.1037/a0014386
34. Bryant ZE, Henslee AM, Correia CJ. Testing the effects of e-mailed personalized feedback on risky alcohol use among college students. Addict Behav. (2013) 38:2563–7. doi: 10.1016/j.addbeh.2013.06.007
35. Collins SE, Spelman PJ. Associations of descriptive and reflective injunctive norms with risky college drinking. Psychol Addict Behav. (2013) 27:1175–81. doi: 10.1037/a0032828
36. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters E. Lifetime prevalances and age-of-onset distributions of DSM-IV disoders in the national comorbidity survey replication. Arch Gen Psychiatry. (2005) 62:593–602. doi: 10.1001/archpsyc.62.6.593
37. Neighbors C, Lewis MA, LaBrie J, DiBello AM, Young CM, Rinker DV, et al. A multisite randomized trial of normative feedback for heavy drinking: social comparison versus social comparison plus correction of normative misperceptions. J Consult Clin Psychol. (2016) 84:238–47. doi: 10.1037/ccp0000067
38. Walters ST, Vader AM, Harris TR. A controlled trial of web-based feedback for heavy drinking college students. Prevent Sci. (2007) 8:83–8. doi: 10.1007/s11121-006-0059-9
39. Carey KB, Scott-Sheldon LAJ, Elliott JC, Garey L, Carey MP. Face-to-face versus computer-delivered alcohol interventions for college drinkers: a meta-analytic review, 1998 to 2010. Clin Psychol Rev. (2012) 32:690–703. doi: 10.1016/j.cpr.2012.08.001
40. Sundström C, Blankers M, Khadjesari Z. Computer-based interventions for problematic alcohol use: a review of systematic reviews. Int J Behav Med. (2017) 24:646–58. doi: 10.1007/s12529-016-9601-8
41. Foxcroft DR, Moreira MT, Almeida Santimano NML, Smith LA. Social norms information for alcohol misuse in University and college students. Cochrane Database Syst Rev. (2015) 1 CD006748. doi: 10.1002/14651858.CD006748.pub3
42. Cronce JM, Larimer ME. Individual-focused approaches to the prevention of college student drinking. Alcohol Res Health. (2011) 34:210–21.
43. Dotson KB, Dunn ME, Bowers CA. Stand-alone personalized normative feedback for college student drinkers: a meta-analytic review, 2004 to 2014. PLoS ONE. (2015) 10:e0139518. doi: 10.1371/journal.pone.0139518
44. Lewis MA, Litt DM, Tomkins M, Neighbors C. Prototype Willingness model drinking cognitions mediate personalized normative feedback efficacy. Prevent Sci. (2017) 18:373–81. doi: 10.1007/s11121-016-0742-4
45. Ganz T, Braun M, Laging M, Schermelleh-Engel K, Michalak J, Heidenreich T. Effects of a stand-alone web-based electronic screening and brief intervention targeting alcohol use in University students of legal drinking age: a randomized controlled trial. Addict Behav. (2018) 77:81–8. doi: 10.1016/j.addbeh.2017.09.017
46. Rodriguez LM, Neighbors C, Rinker DV, Lewis MA, Lazorwitz B, Gonzales RG, et al. Remote versus in-lab computer-delivered personalized normative feedback interventions for college student drinking. J Consult Clin Psychol. (2015) 83:455–63. doi: 10.1037/a0039030
47. Young CM, Neighbors C. Incorporating writing into a personalized normative feedback intervention to reduce problem drinking among college students. Alcoholism Clin Exp Res. (2019) 43:916–26. doi: 10.1111/acer.13995
48. Elliott JC, Carey KB, Bolles JR. Computer-based interventions for college drinking: a qualitative review. Addict Behav. (2008) 33:994–1005. doi: 10.1016/j.addbeh.2008.03.006
49. Thompson K, Burgess J, MacNevin PD. An evaluation of e-CHECKUP TO GO in Canada: the mediating role of changes in social norm misperceptions. Substance Use Misuse. (2018) 53:1849–58. doi: 10.1080/10826084.2018.1441306
50. Samson JE, Tanner-Smith EE. Single-session alcohol interventions for heavy drinking college students:a systematic review and meta-analysis. J Stud Alcohol Drugs. (2015) 76:530–43. doi: 10.15288/jsad.2015.76.530
51. Labrie JW, Lewis MA, Atkins DC, Neighbors C, Zheng C, Kenney SR, et al. Rct of web-based personalized normative feedback for college drinking prevention: are typical student norms good enough? J Consult Clin Psychol. (2013) 81:1074–86. doi: 10.1037/a0034087
52. Larimer ME, Kaysen DL, Lee CM, Kilmer JR, Lewis MA, Dillworth T, et al. Evaluating level of specificity of normative referents in relation to personal drinking behavior. J Stud Alcohol Drugs Suppl. (2009) 16:115–21. doi: 10.15288/jsads.2009.s16.115
53. Larimer ME, Neighbors C, Labrie JW, Atkins DC, Lewis MA, Lee CM, et al. Descriptive drinking norms: for whom does reference group matter? J Stud Alcohol Drugs. (2011) 72:833–43. doi: 10.15288/jsad.2011.72.833
54. Neighbors C, Labrie JW, Hummer JF, Lewis MA, Lee CM, Desai S, et al. Group identification as a moderator of the relationship between perceived social norms and alcohol consumption. Psychol Addict Behav. (2010) 24:522–8. doi: 10.1037/a0019944
55. Haug S, Sannemann J, Meyer C, John U. Reduktion des Alkoholkonsums und Förderung der Rauchabstinenz bei Jugendlichen und jungen Erwachsenen mittels Internet und Mobiltelefon: Ein Literaturüberblick [Internet and mobile phone interventions to decrease alcohol consumption and to support smoking cessation in adolescents: a review]. Gesundheitswesen. (2012) 74:160–77. doi: 10.1055/s-0030-1268446
56. Bush KR, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Arch Intern Med. (1998) 158:1789–95. doi: 10.1001/archinte.158.16.1789
57. Farnir E, Gräfe C, Wolter C, Gusy B. Eine Intervention zur Reduktion des Alkoholkonsums bei Studierenden der Freien Universität Berlin. Evaluationsbericht (Schriftenreihe des AB Public Health: Prävention und psychosoziale Gesundheitsforschung 01/P18). Berlin: Freie Universität Berlin (2018). Available online at: https://www.ewi-psy.fu-berlin.de/einrichtungen/arbeitsbereiche/ppg/publikationen/forschung/Schriftenreihe/ISPI_Gesamtbericht_V09.pdf (accessed May 28, 2021).
58. Jo SJ Lee HK Kang K Joe KH Lee SB Efficacy of a Web-based screening and brief intervention to prevent problematic alcohol use in Korea: results of a randomized controlled trial. Alcoholism Clin Exp Res. (2019) 43:2196–202. doi: 10.1111/acer.14169
59. Kypri K, Vater T, Bowe SJ, Saunders JB, Cunningham JA, Horton NJ, et al. (2014). Web-based alcohol screening and brief intervention for University students: a randomized trial. JAMA. 311:1218–24. doi: 10.1001/jama.2014.2138
60. Martens MP, Smith AE, Murphy JG. The efficacy of single-component brief motivational interventions among at-risk college drinkers. J Consult Clin Psychol. (2013) 81:691–701. doi: 10.1037/a0032235
61. John B, Alwyn T. Revisiting the rationale for social normative interventions in student drinking in a UK population. Addict Behav. (2014) 39:1823–6. doi: 10.1016/j.addbeh.2014.07.022
62. Thombs DL, Dotterer S, Olds RS, Sharp KE, Raub CG. A close look at why one social norms campaign did not reduce student drinking. J Am Coll Health. (2004) 53:61–8. doi: 10.3200/JACH.53.2.61-70
63. Dowdall GW, Wechsler H. Studying college alcohol use: widening the lens, sharpening the focus. J Stud Alcohol Suppl. (2002) 14:14–22. doi: 10.15288/jsas.2002.s14.14
64. Sobell LC, Maisto SA, Sobell MB, Cooper A. Reliability of alcohol abusers' self-reports of drinking behavior. Behav Res Ther. (1979) 17:157–60. doi: 10.1016/0005-7967(79)90025-1
Keywords: social norms intervention, prevention of alcohol misuse, University students, alcohol intervention, heavy drinking
Citation: Wolter C, Lesener T, Thomas TA, Hentschel A-C and Gusy B (2021) Finding the Right Balance: A Social Norms Intervention to Reduce Heavy Drinking in University Students. Front. Public Health 9:653435. doi: 10.3389/fpubh.2021.653435
Received: 14 January 2021; Accepted: 18 May 2021;
Published: 10 June 2021.
Edited by:
Pavel Dietz, Johannes Gutenberg University Mainz, GermanyReviewed by:
Matteo Sattler, University of Graz, AustriaCopyright © 2021 Wolter, Lesener, Thomas, Hentschel and Gusy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tino Lesener, dC5sZXNlbmVyQGZ1LWJlcmxpbi5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.