 Yuan Tian
Yuan Tian Bixiao Nian†
Bixiao Nian† Long Rong
Long Rong
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 22 March 2021
Sec. Occupational Health and Safety
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.632608
This article is part of the Research Topic COVID-19 and the Digestive System View all 21 articles
Background: SARS-CoV-2 spreads rapidly around the world, and some patients present gastrointestinal symptoms. The existence of the virus in the gastrointestinal tract makes digestive endoscopy a high-risk operation, which associated with an increased risk of infection rate in healthcare workers. This study aimed at exploring current knowledge, practice and attitudes of healthcare workers in endoscopy units in China regarding the status of occupational protection during COVID-19 pandemic.
Methods: A cross-sectional study of a national online survey involving 717 healthcare workers in endoscopy units from 94 medical structures in 24 provinces and municipalities around China was conducted online via a questionnaire platform called Wenjuanxing (wjx.cn). The data were analyzed using correlation approaches, Kruskal-Wallis test for independent samples, and linear regression models.
Results: Most Chinese healthcare workers in endoscopy units had a good knowledge of COVID-19 (median: 10; range: 7–12), showed a strikingly positive attitude (median: 65; range: 39–65), and carried out good practice (median: 47; range: 14–50) in strengthening the protection, disinfection and management of COVID-19. In terms of attitudes, female staff was more concerned about protection against COVID-19 than male staff (KW = 8.146, P = 0.004). Nurses performed better in both attitude (KW = 2.600, P = 0.009) and practice (KW = 6.358, P < 0.001) than endoscopic physicians when carrying out personal protection, patient care and environmental disinfection against SARS-CoV-2 infection. More positive attitudes in protection were related to better protective behavior in endoscopic daily medical work (r = 0.312; P < 0.001).
Conclusion: The findings of this study suggest that Chinese endoscopy healthcare workers have an excellent mastery of knowledge about COVID-19, which is transformed into positive beliefs and attitudes, contributing to good practice during daily endoscopic procedures. Medical staff may benefit from further education. With the gradual normalization amid the ongoing COVID-19 pandemic, protection and management in endoscopy units may be changed accordingly.
The severe acute respiratory syndrome caused by new coronavirus (SAS-CoV-2) was first cluster in December 2019 and reported from China (1). This disease was spread into global pandemic rapidly, and a total of 93,194,922 confirmed cases and more than 2 million deaths were reported in January 2021 (2). The pandemic of coronavirus disease 2019 (COVID-19) in China at stable status, while a “second wave” of contagion was outbreak outside of China (3). As a highly contagious disease, the risk of infection among healthcare workers is significant. Twenty nine percentage of patients (40 out of 138) were healthcare workers in one of the earliest studies in Wuhan (4). A report of American Center for Disease Control and Prevention (CDC) of US stated that from February 12 to April 9, a total of 9,282 healthcare workers were diagnosed with COVID-19, including 27 deaths. Eleven to nineteen percentage of COVID-19 cases were identified as medical staffs (5). Studies have already illustrated the virus transmission, and found physical distancing of 1 m or more, and use of face masks, respirators, and eye protection could prevent the transmission of COVID-19 (6–13) while the current knowledge, practice and attitudes of healthcare workers in endoscopy units remains unclear.
Digestive symptoms are increasingly recognized among patients with COVID-19, including anorexia, diarrhea, nausea, vomit, and abdominal pain (14). Several studies pointed out that some patients presented only GI symptoms and no typical symptoms throughout the course of the disease (15). Viral RNA was detected in the feces of COVID-19 patients, and active virus particles were isolated (16). Most atypical patients with GI symptoms did not visit the Pulmonary Department, Emergency Department or Fever Clinic, but the Gastroenterology Department, which resulted in healthcare providers being exposed to either respiratory and gastrointestinal droplets or body fluids from patients when performing endoscopy. Aerosols generated from coughing in upper endoscopy and flatus produced in colonoscopy played an important role in endoscopist exposure to the virus (17). Endoscopy therefore was a potential route of infection according to the characteristics and transmission of the virus. These preliminary findings highlight that adequate protection of healthcare workers is critical.
The theory of knowledge, attitude/belief and practice (KAP) model on PHEIC may distinguish from general issues (18, 19). At the early stage of SARS-CoV-2 epidemic in China, National Health Commission of the PRC and Chinese CDC conducted public education and took prevention measures quickly in the whole society as responses to COVID-19 (20). In addition, the Chinese Society of Digestive Endoscopy also made special regulations on endoscopic work (21). With the joint efforts, people's knowledge reserve for epidemic prevention and control reached a high and stable level, which partially accounted for the negative results from knowledge. It is easier for endoscopic healthcare workers who have received medical education for years to master the knowledge of COVID-19. For instance, endoscopy physicians who believe low population density can reduce the transmission of SARS-CoV-2 may limit the daily number of patients examined. Given the adequate protective knowledge, different attitudes lead to different practice. This cross-sectional study was performed using an online questionnaire to evaluate the occupational protection status of healthcare workers in endoscopy units of different hospital scale in different regions in China. The level of knowledge and awareness of healthcare workers about COVID-19 occupational protection during the pandemic, or the behavior of participants with respect to personal protective equipment and disinfection management were assessed in this study, so as to give advice and suggestions to endoscopic units in other regions.
Endoscopic healthcare workers, including endoscopy physicians, nurses, and cleaning workers from general hospitals, specialized hospitals and community medical institutions from 94 medical structures in 24 provinces and municipalities around China were enrolled and invited to complete the questionnaire in this study. Ten times the number of questionnaire entries with extra 10% invalid questionnaires, 389 was regarded as the minimum sample size for this study. This study was approved by the Peking University First Hospital Biomedical Research Ethics Committee (No. 2020-124). All subjects finally enrolled in this study were considered to have signed informed consent agreement prior to answering the questionnaire.
Based on the guidance issued by Chinese Medical Association on the endoscopic diagnosis and treatment during the prevention and control of new coronavirus infection, the questionnaire items were designed and screened by a group of specialists who had experience in the fields of endoscopic diagnosis and treatment, epidemic prevention and control, and public health research. This questionnaire was applied to the evaluation of endoscopic healthcare workers from three aspects, namely, knowledge, attitudes, and behavior toward COVID-19. More details are shown in Table 1 and Appendix 1 (Supplementary Material). The response for each item of knowledge part was scored 0–1. A five-grade scoring method was used to indicate the level for attitude part: 5, strongly agree; 4, agree; 3, neutral; 2, disagree; 1, strongly disagree. Moreover, the five-grade scoring method was applied to indicate the level for practice part: 5. Always; 4. Often; 3. Sometimes; 2. Occasionally; 1. Hardly ever. The scoring system for knowledge ranged from 0 to 12, and the good knowledge score was defined as >7.2 (above 60%), and poor knowledge was defined as below 60%. Similarly, the scoring system for attitude and practice ranged from 13 to 65, and 10 to 50, respectively, and the good attitude and good practice were defined as > 52 (attitude scores above 80% were defined as good attitude) and > 40 (scores >80% were classified as having good practice), respectively (22).
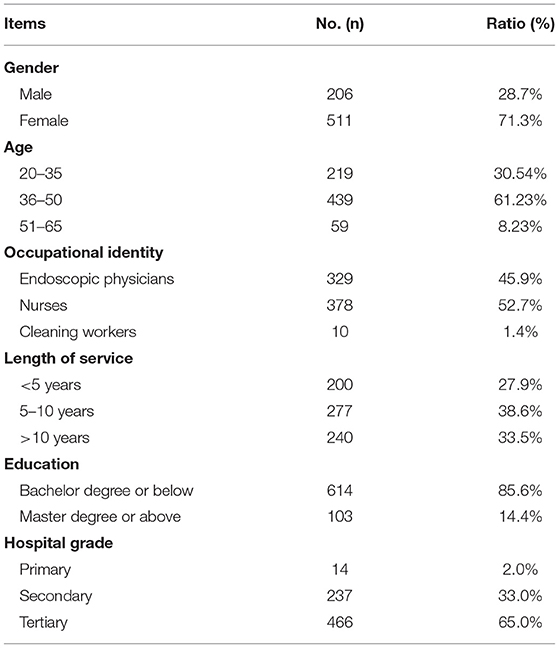
Table 1. Demographic characteristics of subjects.
The quality of the present questionnaire was evaluated from two aspects, namely, validity and reliability. For content validity, the consistency of the contents to be tested with questionnaire items was assessed by five experts from related fields using a four-level scoring method, in which score 1 represented “irrelevant,” 2 “a little bit relevant,” 3 “relevant,” and 4 “very relevant.” Content validity index (CVI) was served as the measurement, and an index value of >0.8 indicated an acceptable content validity. External reliability, also known as test-retest reliability, was also examined in this study.
Electronic questionnaire was adopted in this study to investigate current situations of endoscopic healthcare workers during COVID-19 pandemic. The questionnaire entries were imported to the online platform Wenjuanxing (wjx.cn), and distributed to endoscopic healthcare workers around China via WeChat. All the subjects were invited to finish the survey before April 4th, 2020. The data were subsequently downloaded and sorted by specialists. Investigators were blinded to the identity information of the subjects.
Descriptive statistics was used to summarize demographic data, and internal reliability was measured by Cronbach's α. The questionnaire scores according to demographic data were compared by using independent sample t-test, Mann-Whitney U test, one-way analysis of variance, rank-sum test and Pearson/Spearman correlation analysis separately based on the data distribution. A P < 0.05 was considered to be significant, and the results of all tests noted above were analyzed using SPSS 24.0 software.
A total of 717 valid questionnaires were collected before April 4th. The questionnaire was completed by healthcare workers from 94 medical structures in 24 provinces and municipalities. More demographic details are shown in Table 1. The average rating index of this questionnaire was defined as CVI, which was 0.924, indicating an acceptable content validity.
The distribution of responses to the statements that examined the level of knowledge with respect to COVID-19 is presented below (Table 2). The variable ranged from 0 to 12. Overall, medical staff in endoscopy units had a good knowledge, with the median total score of 10 (total score range: 7–12), and 83.33% of accuracy. The good knowledge rate was 99.4% (713/717). There were no significant differences between other demographic characteristics and the level of knowledge about COVID-19.
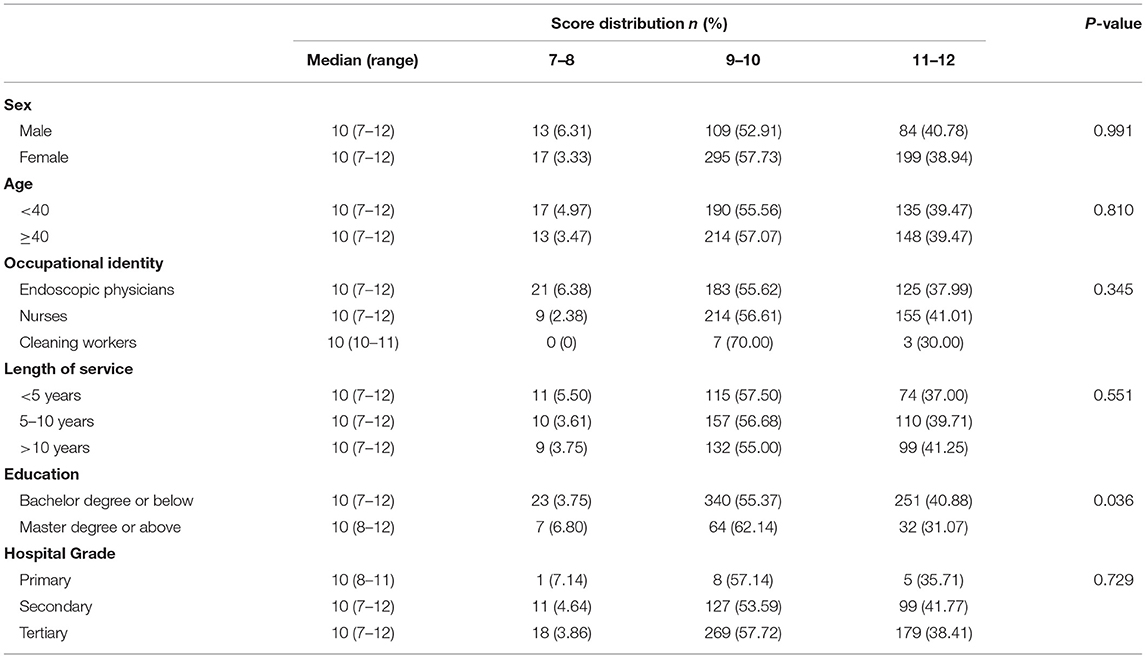
Table 2. Distribution of responses to the knowledge questionnaire.
The distribution of responses to statements that examined attitudes is shown in Table 3. The variable in attitudes ranged from 13 to 65, and medical staff had a strikingly positive attitude toward strengthening the protection, disinfection and management of COVID-19, with the median score of 65 (score range: 39–65). 99.3% (712/717) of participants supported limited daily endoscopy services or service suspension, and 92.9% (666/717) had a positive attitude toward risk-based screening before the endoscopy procedure and appropriate occupational protection during the outbreak. The good attitude rate was 99.3% (712/717). Female staff were more concerned about COVID-19 than male staff (KW = 8.146, P = 0.004), and the same phenomenon was observed between nurses and physicians. Nurses had a more positive attitude than physicians (KW = 2.600, P = 0.009, Adj. P = 0.028).
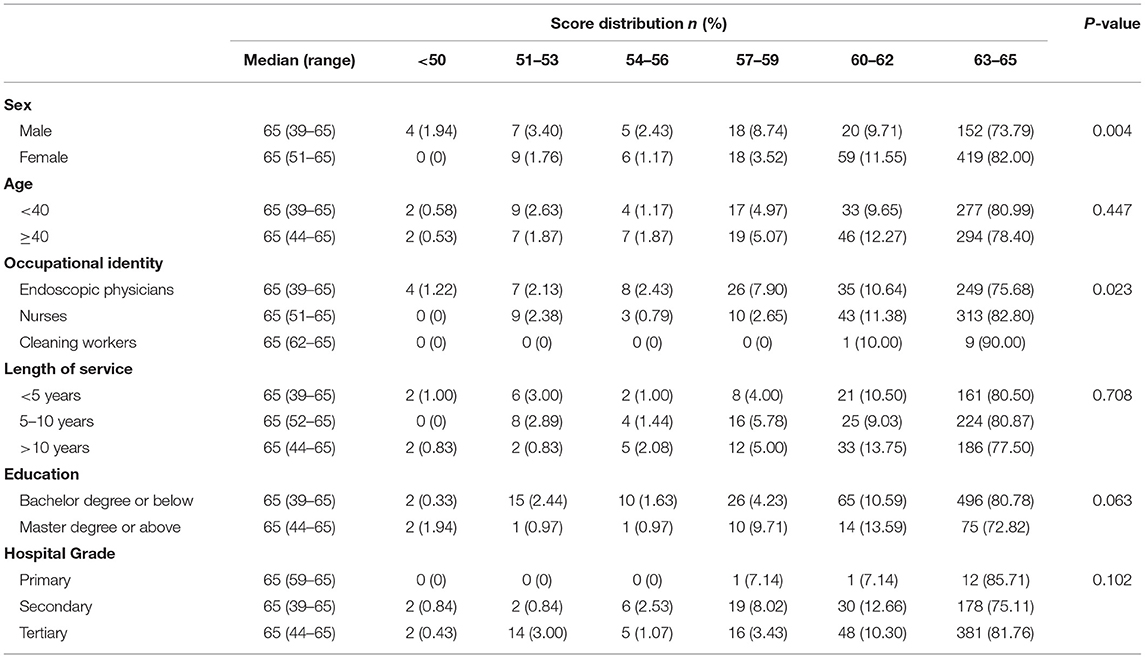
Table 3. Distribution of responses to the attitude questionnaire.
Table 4 shows the distribution of responses to statements that examined personal protection, patient care and disinfection management practice or behavior. The variable in behavior ranged from 10 to 50. The median score of the survey was 47 (score range: 14–50), which showed that medical staff had good practice in COVID-19. The good practice rate was 87.2% (625/717). The comparison of attitudes showed that 93.8% (673/717) of the subjects provided limited daily endoscopy services, the risk-based visit process was implemented in the endoscopy units of 88.1% (632/717) of the subjects, and 1.4% (10/717) believed that their hospitals needed to increase the supply of personal protective equipment.
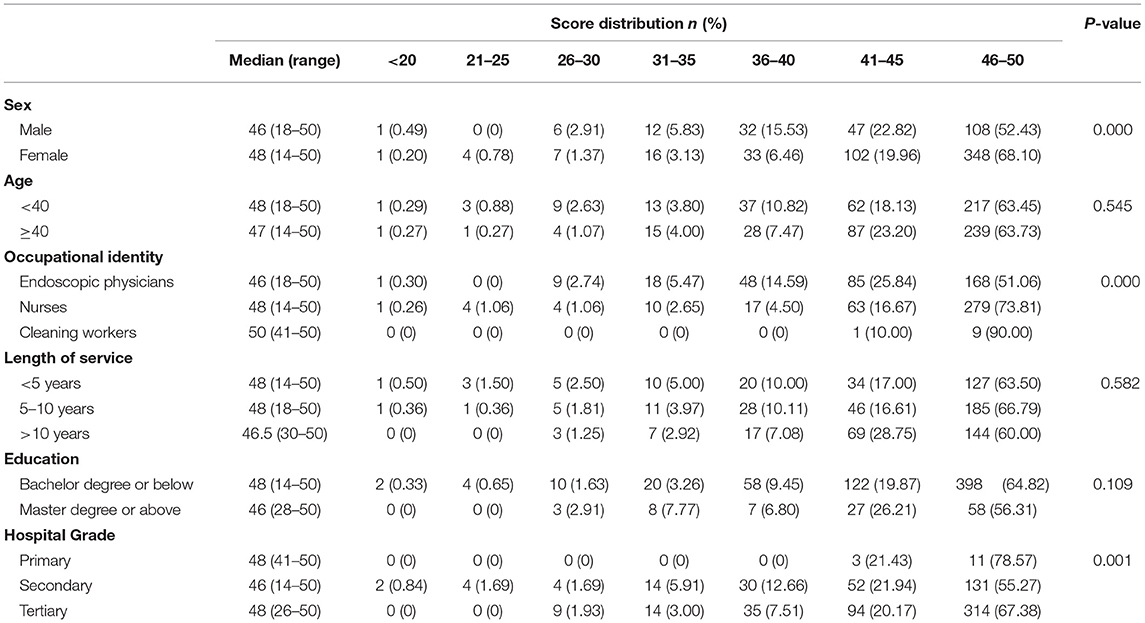
Table 4. Distribution of responses to the practice questionnaire.
Similar to the above findings about healthcare workers' attitudes, female staff were more active than male staff in carrying out personal protection, patient care, and environmental disinfection practice against SARS-CoV-2 infection (KW = 18.564, P < 0.001). Nurses (KW = 6.358, P < 0.001, Adj. P < 0.001) and cleaning workers (KW = −2.585, P = 0.010, Adj. P = 0.029) had a higher score than physicians. Medical staff in tertiary hospitals performed better in practice than those in secondary hospitals (KW = −3.591, P < 0.001, Adj. P = 0.001).
The relationships among three dimensions were explored via Spearman's rank correlation analysis. As a result, there was no significant correlation either between knowledge and practice (r = 0.014; P = 0.710) or between knowledge and attitudes (r = 0.038; P = 0.314). However, a positive correlation between the level of attitudes and practice was found in the subjects (r = 0.312; P < 0.001). More positive attitudes in protection were related to better protective behavior in endoscopic daily medical work (Figure 1).

Figure 1. The relationships among knowledge, attitudes, and practice. ***P < 0.001.
The KAP proposed in the last century has been applied to explaining how personal knowledge and attitudes affected practice in various fields (23–25). In general, knowledge is the basis of behavior formation, and only when knowledge rises to the level of belief can an individual be possible to adopt a positive attitude to change practice. During the COVID-19 pandemic, Chinese health departments have organized various forms of learning activities about SARS-CoV-2, including the virus characteristics, transmission routes, personal protection, quarantine policies, and so on. All the Chinese citizens had access to the knowledge, which was transformed into beliefs. Positive beliefs and attitudes were the motivation for the protective behavior. The medical staff have close contact with patients, and the risks was high, and the KAP theory was more important for medical staff. Therefore, we designed the present questionnaire and enrolled staffs from different institutions to investigate the application of KAP theory by endoscopic healthcare workers in COVID-19 pandemic in China (26–29).
It was found that a high proportion of participants had a good knowledge of COVID-19, which could be possibly attributed to the effective continuing medical education and training going on across the country. Endoscopy-related continuing medical education has an important part to play in preparing for and responding to this situation. Li et al. (30) underscored the importance of continuous medical education and training in this pandemic. Chinese National Health Commission has held online lectures, requiring all medical staff to learn the characteristics and protection requirements of COVID-19.
Moreover, the Endoscopic Society delivered a course of recommended operating procedures in endoscopy units, especially about personal protection and endoscope decontamination, to related healthcare workers, and related questions were required to answer after the course. SARS-CoV-2 is a newly emerged virus, whose virological and disease characteristics are gradually explored and may change at any time. Therefore, continuing education courses for medical staff are also regularly updated in order to enable them to better cope with COVID-19.
Healthcare workers had an extremely positive attitude and carried out favorable practice overall in COVID-19 pandemic. We found that women tended to be more concerned about strengthening the occupational protection, disinfection and management than men, and they did better than men in protective behavior as well. There was a similar phenomenon between nurses and doctors. However, ~87% of men were endoscopy physicians, whereas over 70% of women were nurses in endoscopy units. The results above couldn't distinguish whether the differences in attitudes and behavior were due to gender, occupation, or both of them. We further analyzed the differences between male/female endoscopy physicians and male/female nurses, and noticed that there was a statistical difference between male doctors and female nurses in attitudes. The distinctions in behavior were mainly caused by occupation, not gender. The causes might be as follows. Firstly, nurses spend more time with patients than endoscopy physicians. Endoscopy nurses need to not only assess patients, answer patients' questions and address their concerns before the procedure but also assist doctors throughout the procedure, help patients recover, and complete all necessary documentation including patient notes and discharge documents after the procedure. Secondly, nurses may be more aware of the disinfection because they are responsible for preparing the instruments, equipment and supplies for the procedure as well as cleaning and sterilizing equipment before and after use.
Additionally, medical staff in tertiary hospitals had better protective behavior than those in secondary hospitals. Tertiary hospitals are comprehensive or general hospitals at the city, provincial or national level with a bed capacity exceeding 500. One possible explanation of the phenomenon above is as follows. During the outbreak of COVID-19, it was recommended to defer the elective endoscopies and only perform the urgent endoscopies by strategically assigned staff to minimize concomitant exposure. Endoscopic examinations on patients who were suspected or confirmed with COVID-19 should be performed in a negative pressure room with strict isolation precautions when available (31). Therefore, it was more in line with the protection requirements to complete the urgent endoscopies in a tertiary hospital setting, where the medical staff was more experienced in protective measures and environmental treatment.
The present study investigated the relationships among knowledge, attitudes, and practice of healthcare workers during the prevention and control of new coronavirus infection. The attitudes of endoscopic healthcare workers were positively related to their actual behaviors. In addition, according to theories of mediation effects and KAP, people acquire protection-related knowledge through learning, when their beliefs and attitudes gradually form, which contribute to the emergence of corresponding behavior (32, 33). In this study, we attempted to explore this pattern through mediation effect analysis, but failed to reach a statistical result.
The present study also has some limitations. We only received 10 questionnaires from the cleaning workers, which might be too small to present the real world accurately, thus affecting the comparison among different occupational identities. A larger sample of research is required to be conducted in the future. In addition, our study has geographical bias, to some extent. Most of the questionnaires collected came from non-epidemic areas, while there were fewer questionnaires from areas with severe epidemics. There were particularities in the questionnaire during the epidemic. In the early stage of the epidemic, the country issued corresponding policies that required all organizations to learn the knowledge of the COVID-19, which led to the skewed results of the questionnaire and a narrow gap of knowledge among different occupational identities, thereby concealing some statistical differences.
In conclusion, most Chinese healthcare workers in endoscopy units are well-trained for protection against COVID-19 infection. Given the adequate protective knowledge, more positive attitudes lead to more effective practice. Female staff has a more positive attitude than male staff, and nurses perform better in both attitudes and practice than endoscopic physicians. Medical staff in tertiary hospitals is more experienced in practice than those in secondary hospitals.
The outbreak of COVID-19 has exposed human vulnerability to unknown diseases, and new viruses have caught us off guard. Future campaigns on medical education should emphasize medical staff's knowledge about the virus and the corresponding protective measures they should take to respond to such sudden public health incidents, especially the protective practice for medical operations, such as endoscopy and endotracheal intubation, which have a high risk of exposing the staff to respiratory infectious diseases.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Peking University First Hospital Biomedical Research Ethics Committee (No. 2020-124). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
LR had the idea for and took responsibility for the integrity of the data and the accuracy of the data analysis. XG, YT, and YM designed the questionnaire. XG and BN collected the questionnaire and provided the analysis. YT, YM, BN, and XG contributed to the statistical analysis. YT, YM, and BN drafted the manuscript. LR revised the manuscript. FW participated in the literature search and discussion. All authors read and approved the final manuscript.
This research was funded by Youth Clinical Research Project of Peking University First Hospital (2018CR28).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We acknowledge all healthcare workers participate in the survey; we thank Prof. Weidong Nian, Prof. Jianxiang Liu, Ass. Prof. Nan Li, Ass. Prof. Liping Liu, and Ass. Prof. Xi Yao for their professional questionnaire evaluation.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.632608/full#supplementary-material
1. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
2. World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Geneva (2020). Available online at: https://covid19.who.int/ (accessed January 18, 2021).
3. World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. (2021). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/?gclid=CjwKCAjwq_D7BRADEiwAVMDdHvneRLIPC03U3FJa-UNKxxjMd7TP28noIrDy_k9iqdH6_ns_ns6_ns_k9iqdH6_ns (accessed January 18, 2021).
4. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. (2020) 323:1061–9. doi: 10.1001/jama.2020.1585
5. CDC COVID-19 Response Team. Characteristics of Health Care Personnel with COVID-19 - United States, February 12-April 9, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:477–81. doi: 10.15585/mmwr.mm6915e6
6. Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. (2020) 395:1973–87. doi: 10.1016/S0140-6736(20)31142-9
7. Morawska L, Tang JW, Bahnfleth W, Bluyssen PM, Boerstra A, Buonanno G, et al. How can airborne transmission of COVID-19 indoors be minimised? Environ Int. (2020) 142:105832. doi: 10.1016/j.envint.2020.105832
8. Buonanno G, Stabile L, Morawska L. Estimation of airborne viral emission: Quanta emission rate of SARS-CoV-2 for infection risk assessment. Environ Int. (2020) 141:105794. doi: 10.1016/j.envint.2020.105794
9. Morawska L, Milton DK. It is time to address airborne transmission of coronavirus disease 2019 (COVID-19). Clin Infect Dis. (2020) 71:2311–13. doi: 10.1093/cid/ciaa939
10. Liang M, Gao L, Cheng C, Zhou Q, Uy JP, Heiner K, et al. Efficacy of face mask in preventing respiratory virus transmission: a systematic review and meta-analysis. Travel Med Infect Dis. (2020) 36:101751. doi: 10.1016/j.tmaid.2020.101751
11. Buonanno G, Morawska L, Stabile L. Quantitative assessment of the risk of airborne transmission of SARS-CoV-2 infection: prospective and retrospective applications. Environ Int. (2020) 145:106112. doi: 10.1016/j.envint.2020.106112
12. Spinazzè A, Cattaneo A, Cavallo DM. COVID-19 outbreak in Italy: protecting worker health and the response of the Italian Industrial Hygienists Association. Ann Work Expo Health. (2020) 64:559–64. doi: 10.1093/annweh/wxaa044
13. Cherrie JW, Loh M, Aitken RJ. Protecting healthcare workers from inhaled SARS-CoV-2 virus. Occup Med. (2020) 70:335–7. doi: 10.1093/occmed/kqaa077
14. Tian Y, Rong L, Nian W, He Y. Review article: gastrointestinal features in COVID-19 and the possibility of faecal transmission. Aliment Pharmacol Ther. (2020) 51:843–51. doi: 10.1111/apt.15731
15. An P, Chen H, Jiang X, Su J, Xiao Y, Ding Y, et al. Clinical features of 2019 novel coronavirus pneumonia presented gastrointestinal symptoms but without fever onset. SSRN Electronic J. (2020) doi: 10.2139/ssrn.3532530
16. Xiao F, Tang M, Zheng X, Liu Y, Li X, Shan H. Evidence for gastrointestinal infection of SARS-CoV-2. Gastroenterology. (2020) 158:1831–3.e3. doi: 10.1053/j.gastro.2020.02.055
17. Zhang Y, Zhang X, Liu L, Wang H, Zhao Q. Suggestions for infection prevention and control in digestive endoscopy during current 2019-nCoV pneumonia outbreak in Wuhan, Hubei province, China. Endoscopy. (2020) 52:312–14. doi: 10.1055/a-1128-4313
18. Sakr S, Ghaddar A, Hamam B, Sheet I. Antibiotic use and resistance: an unprecedented assessment of university students' knowledge, attitude and practices (KAP) in Lebanon. BMC Public Health. (2020) 20:535. doi: 10.1186/s12889-020-08676-8
19. Alzghoul BI, Abdullah NA. Pain management practices by nurses: an application of the Knowledge, Attitude and Practices (KAP) model. Glob J Health Sci. (2015) 8:154–60. doi: 10.5539/gjhs.v8n6p154
20. National Health Commission of the PRC (2020). Available online at: http://en.nhc.gov.cn/
21. Chinese Society of Digestive Endoscopology. Guideline of Digestive Endoscopy Diagnosis and Treatment of Chinese Medical Association During COVID-19 Pandemic. (2020). Available online at: http://www.csde.org.cn/
22. Dauda Goni M, Hasan H, Naing NN, Wan-Arfah N, Zeiny Deris Z, Nor Arifin W, et al. Assessment of knowledge, attitude and practice towards prevention of respiratory tract infections among Hajj and Umrah Pilgrims from Malaysia in 2018. Int J Environ Res Public Health. (2019) 16:4569. doi: 10.3390/ijerph16224569
23. Haq IU, Liu Y, Liu M, Xu H, Wang H, Liu C, et al. Association of smoking-related Knowledge, Attitude, and Practices (KAP) with nutritional status and diet quality: a cross-sectional study in China. Biomed Res Int. (2019) 2019:5897478. doi: 10.1155/2019/5897478
24. Odeyemi OA, Sani NA, Obadina AO, Saba CKS, Bamidele FA, Abughoush M, et al. Food safety knowledge, attitudes and practices among consumers in developing countries: an international survey. Food Res Int. (2019) 116:1386–90. doi: 10.1016/j.foodres.2018.10.030
25. Assefa EM. Knowledge, Attitude and Practice (KAP) of health providers towards safe abortion provision in Addis Ababa health centers. BMC Womens Health. (2019) 19:138. doi: 10.1186/s12905-019-0835-x
26. Jones RM. Relative contributions of transmission routes for COVID-19 among healthcare personnel providing patient care. J Occup Environ Hyg. (2020) 17:408–15. doi: 10.1080/15459624.2020.1784427
27. Phan LT, Sweeney D, Maita D, Moritz DC, Bleasdale SC, Jones RM, et al. Respiratory viruses on personal protective equipment and bodies of healthcare workers. Infect Control Hosp Epidemiol. (2019) 40:1356–60. doi: 10.1017/ice.2019.298
28. Zietsman M, Phan LT, Jones RM. Potential for occupational exposures to pathogens during bronchoscopy procedures. J Occup Environ Hyg. (2019) 16:707–16. doi: 10.1080/15459624.2019.1649414
29. Phan LT, Sweeney DM, Maita D, Moritz DC, Bleasdale SC, Jones RM, et al. Respiratory viruses in the patient environment. Infect Control Hosp Epidemiol. (2020) 41:259–66. doi: 10.1017/ice.2019.299
30. Li L, Xv Q, Yan J. COVID-19: the need for continuous medical education and training. Lancet Respir Med. (2020) 8:e23. doi: 10.1016/S2213-2600(20)30125-9
31. Chiu PWY, Ng SC, Inoue H, Reddy DN, Ling Hu E, Cho JY, et al. Practice of endoscopy during COVID-19 pandemic: position statements of the Asian Pacific Society for Digestive Endoscopy (APSDE-COVID statements). Gut. (2020) 69:991–6. doi: 10.1136/gutjnl-2020-321185
32. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. (1986) 51:1173–82. doi: 10.1037/0022-3514.51.6.1173
Keywords: occupational protection, COVID-19, endoscopy, knowledge, attitudes, practice
Citation: Tian Y, Nian B, Ma Y, Guo X, Wang F and Rong L (2021) The Status of Occupational Protection During COVID-19 Pandemic: Knowledge, Attitudes, and Practice of Healthcare Workers in Endoscopy Units, China. Front. Public Health 9:632608. doi: 10.3389/fpubh.2021.632608
Received: 24 November 2020; Accepted: 22 February 2021;
Published: 22 March 2021.
Edited by:
Omur Cinar Elci, Asian University for Women, BangladeshReviewed by:
Andrea Spinazzè, University of Insubria, ItalyCopyright © 2021 Tian, Nian, Ma, Guo, Wang and Rong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Long Rong, ZHJyb25nbG9uZ0Bmb3htYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.