 Maha M. AlRasheed1*
Maha M. AlRasheed1* Abdullah M. Alsugair2
Abdullah M. Alsugair2 Hala F. Almarzouqi1
Hala F. Almarzouqi1 Gadah K. Alonazi1
Gadah K. Alonazi1 Fadilah S. Aleanizy3
Fadilah S. Aleanizy3 Fulwah Y. Alqahtani3Gamal A. Shazly3,4Fowad Khurshid1
Fulwah Y. Alqahtani3Gamal A. Shazly3,4Fowad Khurshid1- 1Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia
- 2Department of Civil Engineering, College of Engineering, King Saud University, Riyadh, Saudi Arabia
- 3Department of Pharmaceutics, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia
- 4Department of Industrial Pharmacy, Faculty of Pharmacy, Assiut University, Assiut, Egypt
Aim: This study aimed to assess the knowledge, attitude, and practice (KAP) of security and safety workers toward the COVID-19 pandemic in Saudi Arabia.
Methods: A cross-sectional survey was conducted between April and July 2020 using a self-developed structured questionnaire that was randomly distributed online among security and safety employees in government or private sectors.
Results: Among the 712 participants, 53.9% were female and the respondents' mean age was 39.43 years. Television was chosen as the most reliable source of information by 75.0% of the participants. Most of the respondents had a sufficient knowledge about the COVID-19 pandemic, as the majority of them answered the knowledge questions correctly. The significant predictors for their knowledge were their educational level, age, marital status, parenthood status, and employment sector (private or government). Our study revealed an overall 98.6% positive attitude of safety and security workers toward COVID-19. Majority of the respondents were following good and safe COVID-19 prevention practices.
Conclusion: High level of knowledge was reflected in both the attitude and practice of the participants toward the COVID-19 pandemic.
Introduction
At the end of December 2019, a novel virus, Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2), termed COVID-19, surfaced in Wuhan, China, and has since spread widely across the globe with a substantial clinical impact (1). Based on the currently available information, COVID-19 is a highly contagious disease which can spread through human-to-human transmission. Its primary reported manifestation includes fever, fatigue, dry cough, myalgia anorexia, and sore throat (1, 2). Global concerns about the spread of the virus have risen due to its high transmissibility primarily as respiratory droplet discharge from the mouth or nose through coughing or sneezing (2). It has also been reported that the coronavirus is found in the tongue, mouth floor, and salivary secretions of affected patients, hence, highlighting the potential diagnostic capability of human saliva for the early detection of COVID-19 (3). Early and rapid findings through saliva can help to control the spread of the disease as well as further outbreaks of contagious viruses (3). A systematic review of COVID-19 patients has revealed that individuals with hypertension, diabetes, cardiovascular, and respiratory system diseases belong to the most vulnerable groups (4). Recently, the U.S. Food and Drug administration approved the antiviral drug Remdesivir to be the first and only approved COVID-19 treatment to date (5). At present, a couple of vaccines have been approved to be used in different countries so far. Therefore, to minimize the spread of the virus, preventive measures as recommended by competent authorities are of utmost significance. The ultimate decision on patient management and treatment should be made by the clinician to provide pertinent data in the patients' best interest (6), while adherence to the recommended measures is largely determined by the knowledge, attitude, and practice (KAP) of the community (7).
Saudi Arabia recorded the first confirmed case of COVID-19 on March 2, 2020 (8). With the continuous increase in the devastating numbers of new cases reported globally, on March 11, 2020, the World Health Organization (WHO) declared this outbreak a global pandemic (9). According to the WHO report, as of September 24, 2020, 31,664,104 confirmed cases and 972,221 confirmed deaths had been recorded in the world (10). By then, Saudi Arabia had also been seriously affected by the COVID-19 pandemic, with reports of 331,359 confirmed cases and 4,569 deaths (11). However, early precautionary procedures had been adopted by March 8, before the first case in Saudi Arabia was detected. These included the suspension of entry into KSA for Umrah as well as the closure of all schools and universities in both governmental and private sectors across the country thereby establishing provisions of alternatives to ensure continuity by distance learning. Also, travel to and from specific countries was initially banned on March 9. However, once the cases started to increase in neighboring countries, the government also barred entry to individuals without passports from the Gulf countries to avoid possible transmission emanating within the region in the immediate 2-week period. In particular, precaution was called for at this time requiring any person who has visited Iran recently or during the previous 2 weeks to contact the health authorities for SARS-CoV-2 testing. This was followed by the suspension of all international travel on March 14 for 2 weeks. The closure of malls, restaurants, and coffee shops followed 2 days later, leaving only the supermarkets and pharmacies open, and finally the closure of mosques on March 17. The number of cases continued to rise thereafter, triggering a partial curfew between 7 p.m. and 6 a.m. for 3 weeks starting on March 23. However, the continued culmination in the infection rate triggerred the extension of the curfew initially from 3 p.m. and later to a full day (12).
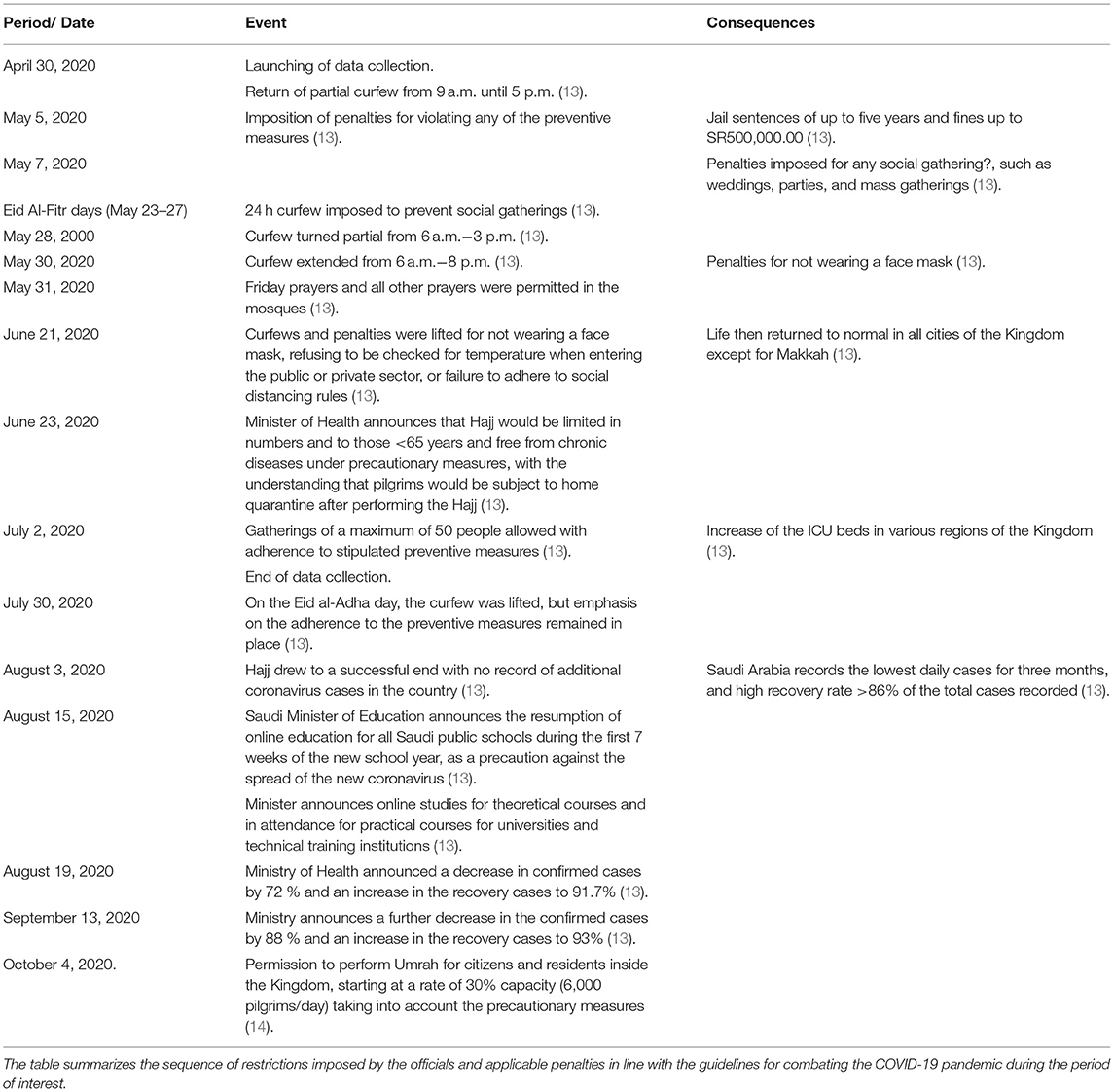
By the time we launched our data collection on April 30, 2020, the partial curfew had returned to 9 a.m. until 5 p.m. The chronological sequence of events during our study is summarized in Table 1.
Studies on knowledge, attitude, and practice (KAP) toward infectious diseases can collect information on what is known, believed, and done by a specific population and helps predict the outcomes. Moreover, such studies are important because the readiness to fight communicable diseases like COVID-19 begins with adequate knowledge, a positive attitude, and safe practices (7, 15). In contrast, it is believed that inadequate knowledge, negative attitudes, and unsafe practice toward infectious diseases lead to unnecessary chaos which facilitates the rapid spread of infections, thereby complicating efforts to preclude the spread of the disease (16). There is a paucity of KAP data on COVID-19 prevention among communities. At this critical moment of a rapid rise in cases, it becomes mandatory to conduct such a study to comprehend the community awareness and preparedness to fight against the disease, to facilitate putting in place evidence-based strategies in addressing the identified shortcomings in guiding future management of the disease. Moreover, it is not clear as to whether certain professional groups within a society may respond to the spread of the disease in a particular fashion, as compared to the rest of the community in general. Hence, the present study aimed to explore the KAP of security and safety workers in the prevention of the spread of COVID-19 in Saudi Arabia.
Methodology
Study Design and Setting
A cross-sectional survey was conducted between April and July 2020. All security and safety workers in the government and private sectors (hospitals, universities, ministries) in Saudi Arabia who are able to read and write and willing to participate irrespective of COVID-19 infection status were included in the study. The selection of the security and safety workers as study subjects was facilitated by the fact that the first two authors had an administrative assignment of managing a security and safety administration. Individuals who did not meet the above inclusion criteria were not eligible and were thus excluded from the study.
Sample Size
The required sample size for this study was calculated using the Raosoft sample size calculator employing a margin of error of 5% and a confidence interval of 95% (17). An estimated sample size of 377 individuals was determined as an adequate number for the study. However, to minimize the errors, the sample size taken for this study was 712.
Enrollment
The participants were enrolled between April 30, 2020 and July 2, 2020. Enrollment time was divided into six periods according to the precautionary measures at that time. The first period started from April 30, 2020 until May 6, 2020 observing partial curfew from 9 a.m. to 5 p.m. In the second period (May 7, 2020 until May 5, 2020), the curfew time stayed the same. However, penalties for any social gathering were imposed and a 24-h curfew for Eid Al-Fitr days was applied in the third period running from May 28, 2020 to May 30, 2020. These curfew times were changed to start at 6 a.m. and end at 8 p.m. and penalties were imposed for not wearing a face mask in the fifth period. In the last period covering June 21, 2020 until July 2, 2020, the curfew was lifted, but penalties were enforced for not wearing a face mask, refusal to have temperature checked on entering a public or private sector, as well as failing to adhere to the social distancing rules (12).
Outcome Measures
The present study examined the level of knowledge, attitude, and proper practice toward COVID-19 prevention using gender, age, education level, marital status, and work sector as potential explanatory variables among the security and safety workers in Saudi Arabia.
Study Questionnaire
A standardized (structured, pre-coded, and validated) questionnaire was developed, based on an extensive literature review of previously published literature (7, 15, 18) as well as recent available information from the World Health Organization (WHO) and Saudi Ministry of Health (MOH) official websites. The survey questionnaire was refined from validated questionnaires that had been previously used to address our objectives. The designed questionnaire was validated in two steps. First, the initial draft of the questionnaire was sent to a group of experts in related fields to reflect on the relativity, simplicity, and importance of the questions. Secondly, the structured questionnaire was validated by piloting the survey on a group of 12 participants to make sure that the survey would work properly. Suitable amendments were then made to develop the final questionnaire based on their feedback. The pilot study data were not included in the final analysis. Since it was not feasible to conduct a community-based sampling survey during this critical period, we decided to collect the data online. Hence, the survey was made available on the “Google Forms” online survey platform, which is considered user-friendly and easily accessible on different web browsers (19). Also, the published survey was promoted in social media platforms to reach the target sample size. The self-reported questionnaire was divided into four sections. The first section consisted of 12 questions that determined the respondent's perceived level of knowledge concerning COVID-19. The second section of the survey consisted of eight questions addressing the attitude of the respondents. The third section included seven statements determining their practice toward the disease, while the fourth section included items providing information about the demographic characteristics (age, gender, educational level, marital status, and workplace) of the respondents. The questionnaire was designed in English, subsequently translated into Arabic for the convenience and easy understanding of the participants, and pre-tested to ensure that it maintained its original meaning.
Assessment of Knowledge, Attitude, and Practice
Knowledge was assessed by a three-item scale. A score of one point was given if the correct answer was chosen and zero in the case of a wrong answer or “do not know” response. The total knowledge score was calculated by adding the scores with a maximum obtainable score of 12 for each participant. Total knowledge score was expressed as mean (SD). Total knowledge score was categorized into two levels, poor knowledge (≤ 10), and good knowledge (>10). The attitude score was calculated as a continuous variable by adding the respondent's number of appropriate answers to eight questions. One point was allotted for each appropriate response (agree) that was considered as a positive attitude and zero was given for each “disagree” or uncertain response, which was considered as a negative attitude, with a maximum attainable score of six for each participant. The mean attitude score for each respondent was calculated by dividing the total attitude scores by eight. A score of ≥0.5 was taken as positive and <0.5 as negative attitude. The practice score was calculated as a continuous variable by adding the respondent's number of appropriate responses to seven questions. Two points were given for “Yes,” one point for “Sometimes,” and zero points were given for “No” with a maximum obtainable score of 14 for each participant. Mean practice score for each respondent was calculated by dividing the total practice score by seven. A score of ≥1 was rated as good and <1 as poor practice.
Statistical Analysis
Descriptive analysis was conducted, and data were reported as percentage and frequency. Knowledge scores, attitudes, and practices of the respondents according to their demographic characteristics were compared by independent-samples t-test, one-way analysis of variance (ANOVA), or Chi-square test as appropriate. Binary logistic regression analyses were used to identify the factors associated with attitudes and practices. Spearman's rank correlation coefficient (p < 0.05) was used to evaluate the association between knowledge and attitude or practice. Data were analyzed using the Statistical Package for Social Sciences (IBM SPSS Statistics, version 26). The statistical significance level was accepted at p < 0.05 (two-sided).
Ethics Approvals
Ethical approval for this study was obtained from the King Saud University College of Medicine Institutional Review Board. Since this study was conducted during the lockdown period, a Google survey was prepared with an online informed consent form on the first page carrying a brief explanation of the objectives and benefits of the study emphasizing the confidentiality of personal data and its sole use for the scientific work. Individuals were asked to complete the written consent prior to their contribution in the study.
Results
The demographic descriptions of the respondents are summarized in Table 2. A total of 712 security and safety workers participated in the study. Of these, 53.9% were female. The respondents mean age was 39.4 years [standard deviation (SD): 7.97, range: 20–62]. Around 60.0% of the respondents possessed educational qualifications of a high school certificate or below, while 40.0% of them held a Bachelor's or higher degree. The majority of the participants (87.5%) engaged in field work and 89.4% were on duty during the period from February 2020 to May 2020 (at the time of the onset of COVID-19). Furthermore, the majority of them (71.9%) were Riyadh (the capital city) residents.
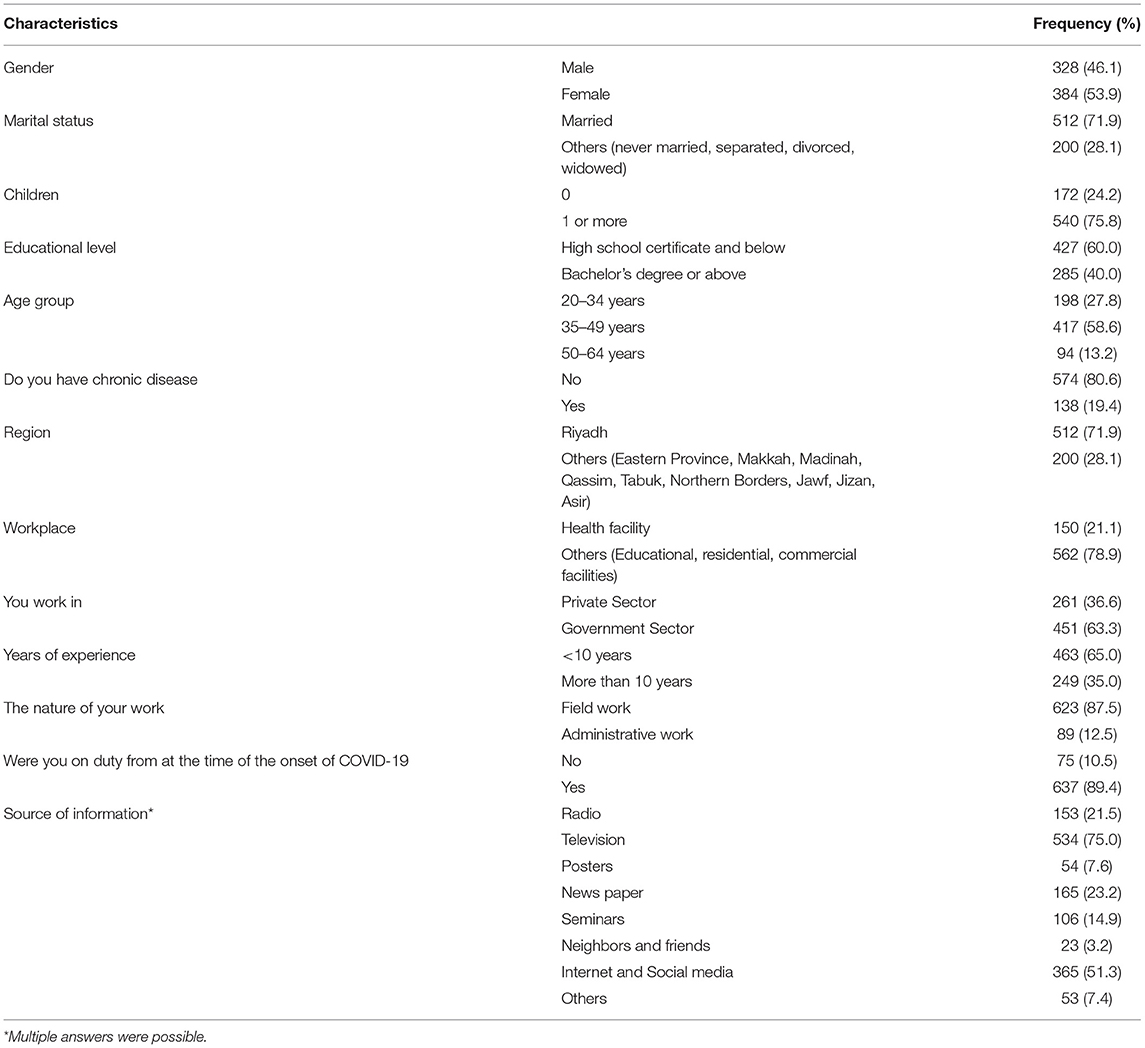
Table 2. Sociodemographic characteristics of participants (N = 712).
The main source of COVID-19 information reported by the participants was television, (75.0%) followed by internet and social media (51.3%), and by newspapers (23.3%). Results are summarized in Table 2.
Respondents' Knowledge Level About COVID-19
Table 3 describes the current status of COVID-19 knowledgeability among security and safety workers in Saudi Arabia. The mean total knowledge score was 10.6 ± 1.4. A total of 435 (61.1%) respondents showed good knowledge, while 277 (38.9%) exhibited the opposite. Poor knowledge was more apparent in response to questions related to the symptoms of the disease, availability of certified treatments and vaccines, transmission, preventive measures, and ways of protection from COVID-19 in which the rates of incorrect responses were 47.1, 20.8, 22.4, 44.7, and 28.5%, respectively.
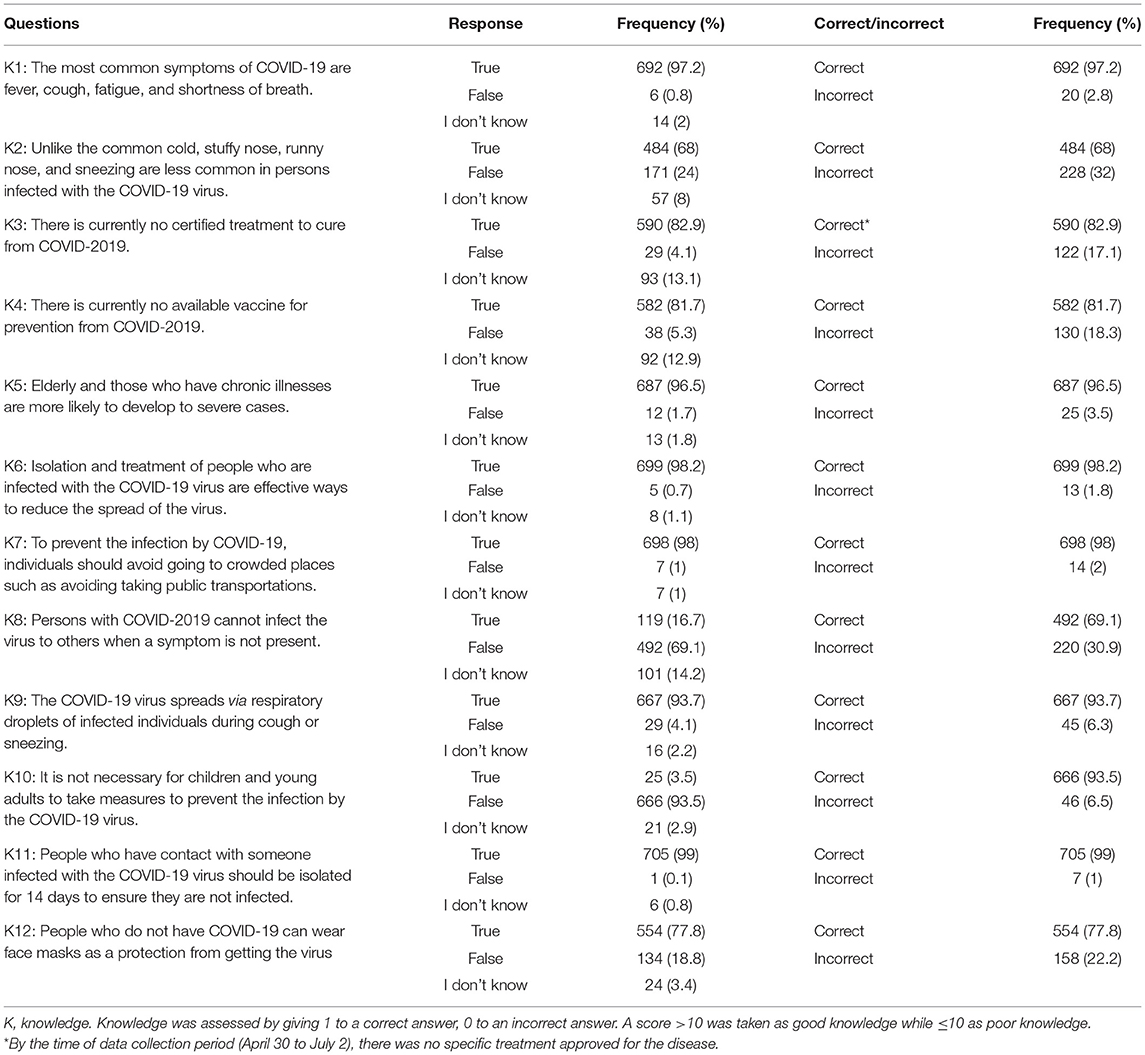
Table 3. Respondents' level of knowledge about COVID-19 (N = 712).
Respondents' Attitude Toward COVID-19
Of the 712 respondents, 702 (98.6%) showed a positive attitude (0.84 ± 0.09), while 10 (1.4%) displayed a negative attitude (0.27 ± 0.16) toward COVID-19. The mean score of the group's attitude toward the disease was 0.83 ± 0.11. The majority of the respondents (n = 670, 94.1%) agreed that COVID-19 is preventable, will eventually be successfully controlled (n = 587, 82.4%), and that the Kingdom of Saudi Arabia will be able to eradicate the new epidemic (n = 685, 96.2%) (Table 4).
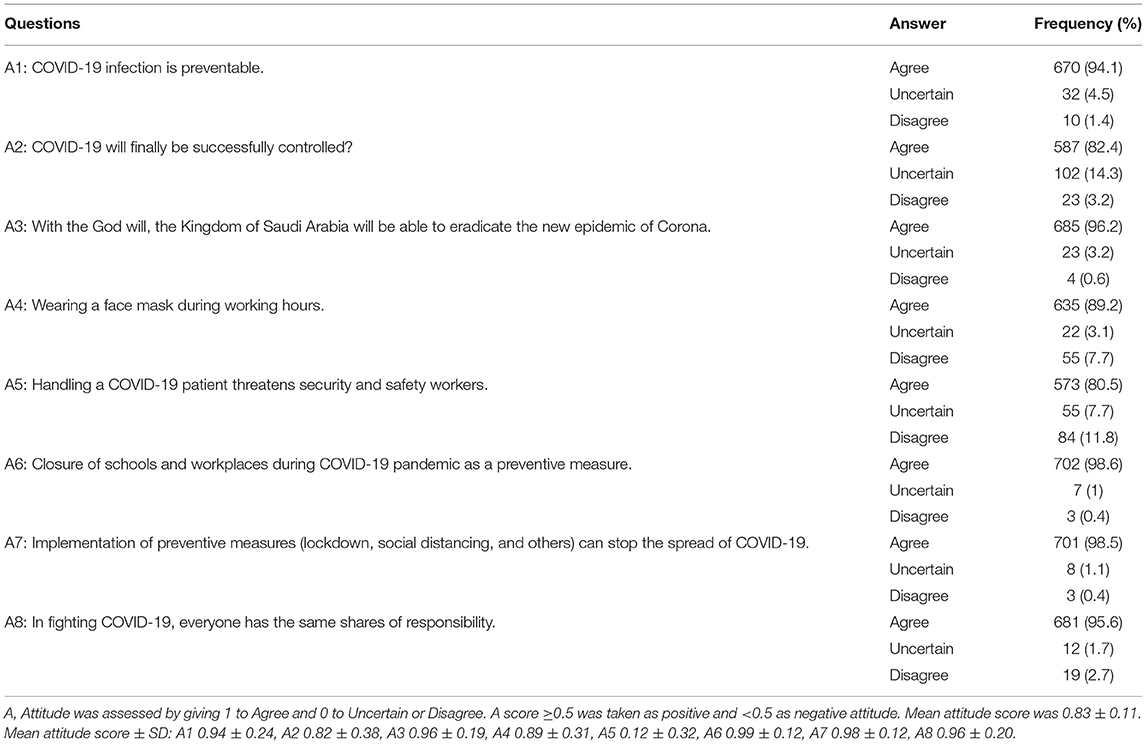
Table 4. Distribution of participant response to attitude related questions on COVID-19 (N = 712).
Multiple logistic regression analysis revealed a significant association between the respondents and chronic disease (vs. others, OR: 0.354, P = 0.001) with the disagreement that COVID-19 infection is preventable. Female gender (OR: 0.693; P = 0.029) and age group of 35–49 years vs. 50+ years were significantly linked (OR: 0.694; P = 0.004) to the disagreement that COVID-19 will eventually be successfully controlled (Table 5). The attitude toward the ability of Saudi Arabia to eradicate the new epidemic differed across the categories of marital status (married vs. others, OR 0.421; P = 0.027). Accordingly, childless respondents were 2.5 times (OR: 2.512; P = 0.020) more likely to display a negative attitude (A3) as compared to those with children (Table 5). Furthermore, while the majority of the respondents agreed to wearing face masks during working hours (n = 635, 89.2%), the 35–49 year age group (vs. 50+ years) were inclined to disagree (OR: 0.549; P = 0.041) with doing so. The most noticeable negative attitude was expressed on the question of whether or not the handling of COVID-19 patients threatened them (0.12 ± 0.32). This differed significantly between genders (female vs. male, OR: 0.916, P = 0.002) (Table 5).
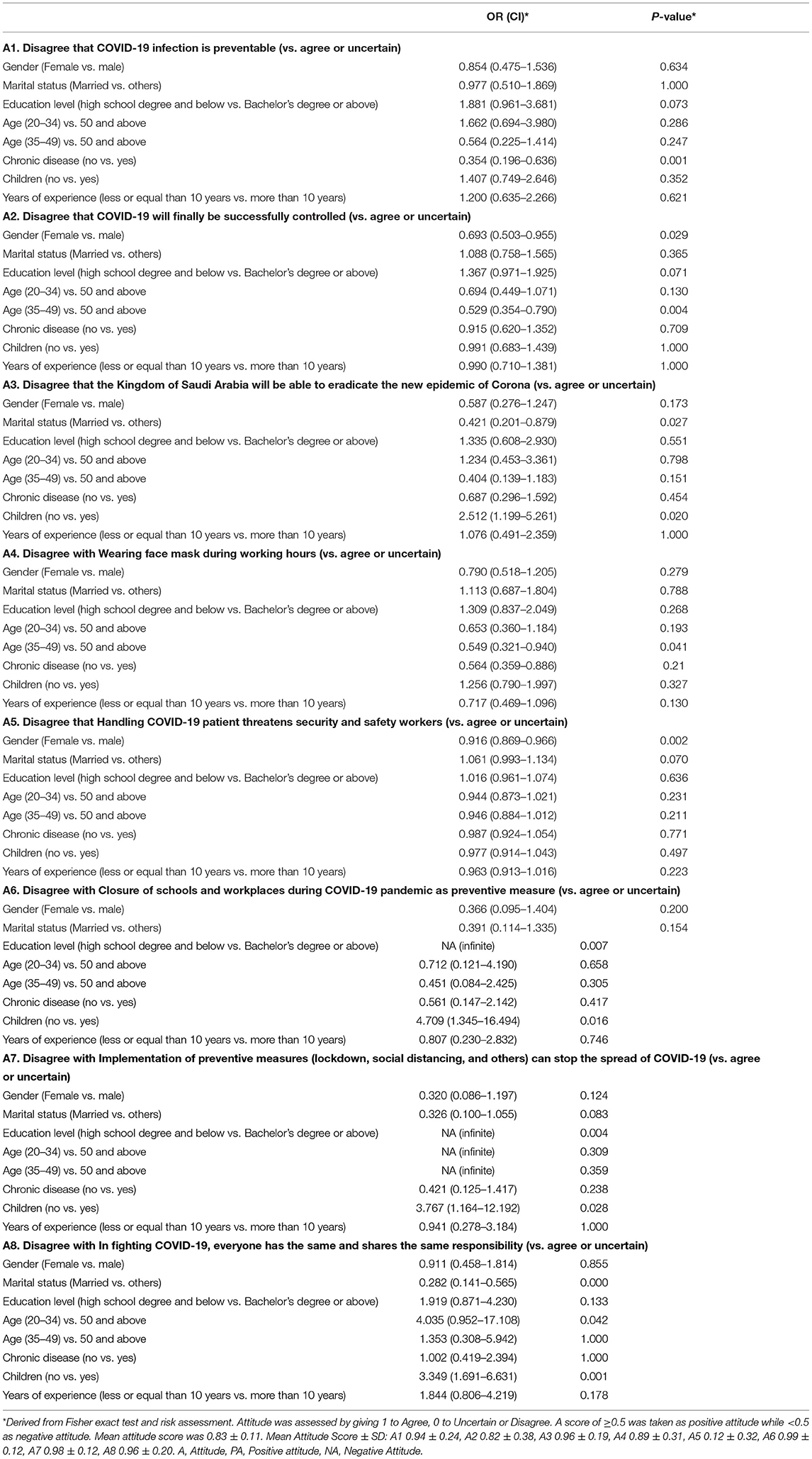
Table 5. Factors affecting good attitude among the participants toward COVID-19.
Nearly all of the respondents agreed on the closure of schools and workplaces during the COVID-19 pandemic as a preventive measure and that the implementation of such measures could stop the spread of the disease (n = 702; 98.6%, n = 701; 98.5%, respectively). These attitudes differed significantly across the educational levels and parenthood status. Childless respondents were 4.7 times (OR: 4.709; P = 0.016) more likely to express a negative attitude toward school closure (A6) and 3.8 times (OR: 3.767; P = 0.028) more likely to disagree with the implementation of preventative measures (A7) as compared to those with children (Table 5).
In total, 681 of the participants (95.6%) agreed with the notion of everyone bearing the same responsibility in fighting COVID-19. However, this notion varied significantly across the marital categories, age, and family status. Respondents aged 20–34 years were four times (OR = 4.035; P = 0.042) more likely to have a negative attitude than those aged 50 and above, while respondents with no children were 3.3 times (OR = 3.349; P = 0.001) more likely to show a negative attitude compared to those with children (Table 5).
Respondents' Level of Practice Toward COVID-19
The vast majority of the participants used soap and water to wash their hands continuously (696, 97.8%), covered their nose and mouth in sneezing or coughing (701, 98.5%), disposed of used tissues (703, 98.7%), and avoided crowded places (697, 97.9%). Also, most of the participants used face masks upon leaving their home (594, 83.4%) and maintained healthy eating (601, 84.4%) and lifestyles (602, 84.6%) (Table 6).
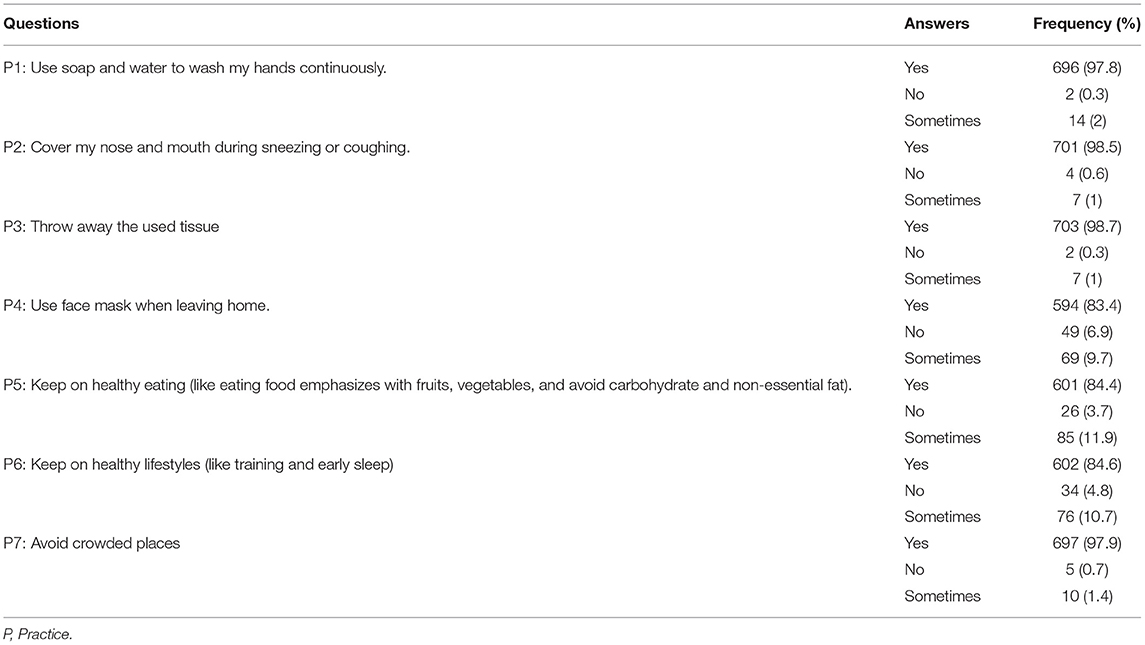
Table 6. Frequency distribution of participant's response on practice related questions on COVID-19 (N = 712).
Factors Influencing the Knowledge, Attitude, and Practice Scores
The association of the participants' demographic characteristics with the knowledge, attitude, and practice scores is displayed in Table 7. Accordingly, age and educational levels were significantly associated with a higher knowledge and attitude scores. Thus, Bachelor's degree holders or above showed a greater knowledge (10.76 ± 1.34 vs. 10.42 ± 1.47; p = 0.002) and positive attitude (0.85 ± 0.10 vs. 0.82 ± 0.12; p = 0.001) toward COVID-19 than high school certificate holders and below. In addition, the 50–64-year-old age group exhibited a greater knowledge (10.69 ± 1.57 vs. 10.32 ± 0.62 and 10.63 ± 1.28; p = 0.023), while the 35–49-year-old age group showed a more positive attitude (0.85 ± 0.09 vs. 0.82 ± 0.15 and 0.81 ± 0.12, p = 0.001) compared to others. It was also revealed that females (0.85 ± 0.10 vs. 0.82 ± 0.13; P = 0.001), individuals free from chronic disease (0.84 ± 0.11 vs. 0.81 ± 0.12, P = 0.018), those residing outside Riyadh (0.85 ± 0.10 vs. 0.83 ± 0.12; p = 0.009), or those who were not employed in a health facility (0.84 ± 0.12 vs. 0.81 ± 0.11; p = 0.014) showed a more positive attitude than their counterparts. Similarly, females (1.92 ± 0.16 vs. 1.87 ± 0.23; p = 0.000), those living outside Riyadh (1.93 ± 0.14 vs. 1.88 ± 0.22; p = 0.000), or those working in the private sector (1.92 ± 0.17 vs. 1.89 ± 0.21; p = 0.035) had better practices than their counterparts. Additionally, total knowledge scores varied significantly across age groups, categories of marital and parenthood status, and workplace (private vs. government sectors). Married individuals (10.63 ± 1.28 vs. 10.36 ± 1.74, p = 0.040), parents (10.63 ± 1.34 vs. 10.33 ± 1.65; p = 0.029), and government employees (10.66 ± 1.30 vs. 10.38 ± 1.62; p = 0.018) were better informed than their counterparts. Thus, the Spearman correlation test revealed a significant positive relationship between knowledge and both attitude (r = 0.182, p = 0.000) and practice (r = 0.186; p = 0.022) of security and safety workers toward COVID-19.
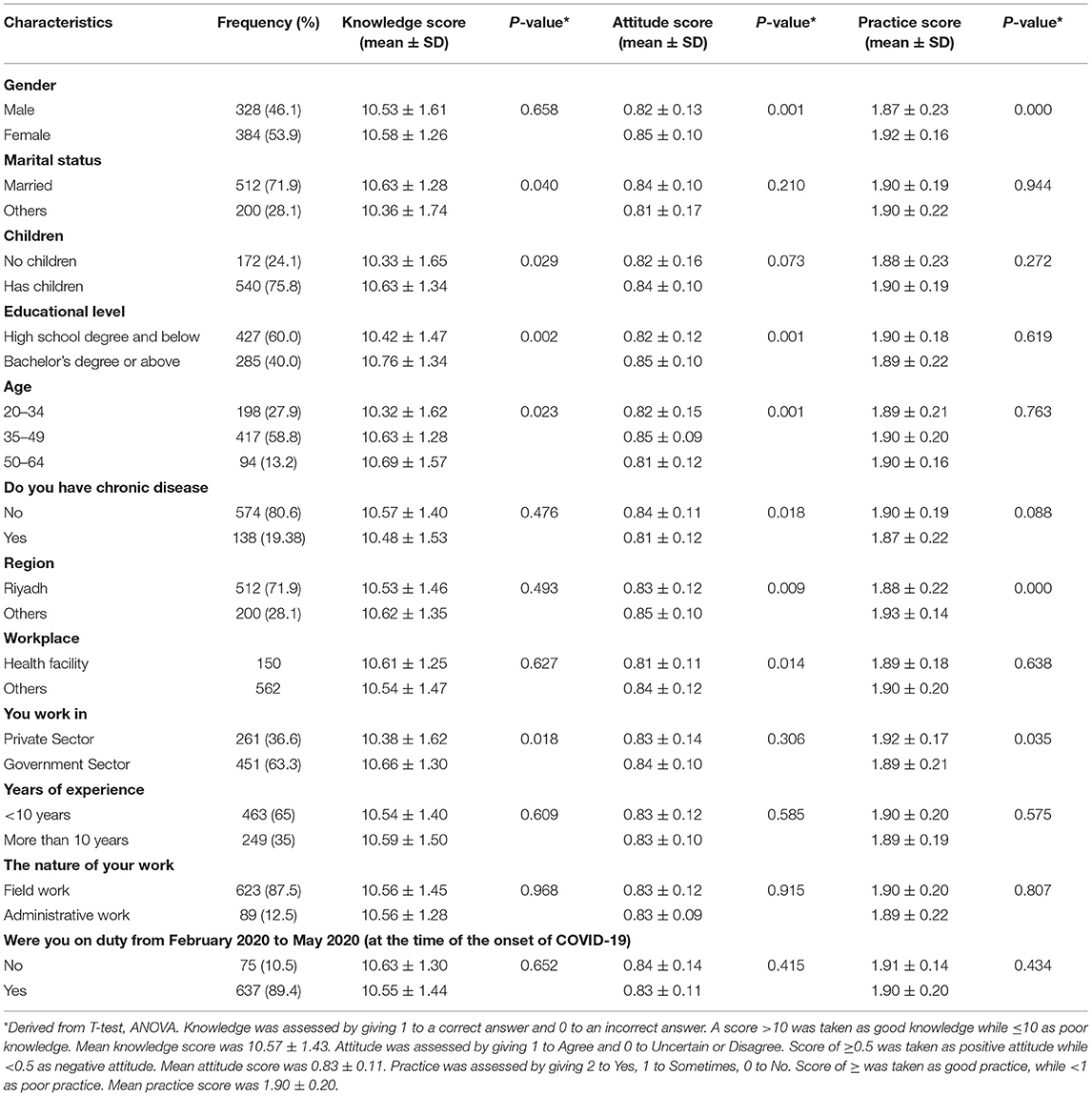
Table 7. Influence of respondent characteristics on their level of knowledge, attitude, and practice toward COVID-19 (n = 712).
Discussion
In the course of the rapidly rising COVID-19 cases, security and safety workers carrying out unusual tasks are continually engaged in combating the disease without any specific preparation. Indeed, they are performing an enormous task in supporting both healthy and infected citizens, possibly impacting their own health during and after the accomplishment of their responsibilities. Effective prevention and control of COVID-19 is attainable through enhancing the KAP of the population toward the disease. Appropriate knowledge is crucial in order to embrace better attitudes and in adopting precautionary practices to prevent and control the spread of the disease (20, 21). Hence, this study aimed to assess the KAP of security and safety workers toward COVID-19 in Saudi Arabia. Our findings indicate that most respondents were sufficiently knowledgeable about the disease, as the majority of them answered the knowledge questions correctly providing an overall 88.0% correct rate on these questions. To the best of our knowledge, this study is the first of its kind not only in Saudi Arabia, but also in the Gulf Cooperation Council (GCC) countries as a whole.
Studies in various parts of the world have arrived at partly different conclusions on the same or similar subject, possibly due to a couple of reasons. For example, the knowledge score attained in our study is slightly lower than the 90% reported in the Chinese general population (7), but somewhat higher than the KAP reported toward COVID-19 in several local and other international studies (15, 18, 22–25). Besides, a cross-sectional study recently reported a greater knowledgeability about COVID-19 in Saudi Arabia (22), while another pointed to a moderate general awareness level (58%) toward this emerging disease among Saudi communities in Riyadh (23). Yet another investigation demonstrated a moderate knowledge level (55.0%) on COVID-19 transmission and preventive measures in the general population in Saudi Arabia (24). In contrast, a cross-sectional study in Uganda described a lack of knowledge among certain population groups (drivers and security agents) on the prevention of the spread of the disease (26). Also, Sarfaraz et al. (27) assessed the knowledge and attitude of dental health practitioners from 23 different countries across the world, indicating a lack of knowledge (4.19 ± 1.88 out of 12) in dentists about the fundamental aspects of disinfection protocols. Moreover, a multinational cross-sectional study conducted in three Middle Eastern countries (Jordan, Saudi Arabia, and Kuwait) to explore the knowledge and practices of this population toward the disease reported a relatively low level of knowledge, particularly on its transmission routes (25). These variations might be ascribed to differences in the socioeconomic status of the study participants. However, inconsistences in the measurement and scoring systems may also hamper accurate comparisons of knowledge levels among different studies. Significant predictors for knowledgeability included educational level, age, marital, and parenthood status, as well as the employment sector (private or government) of the participants. Thereby, in concordance with observations by several other studies (7, 15, 18, 22), Bachelor's degree holders or higher appeared to be better informed. Furthermore, older and married individuals, as well as those with children or working in a government institution attained higher knowledge scores when compared to their counterparts. Conversely, lack of knowledge contributed to the emergence and spread of the outbreak potentially increasing the burden of the disease on the community. Establishment of factors associated with knowledge gaps among participants should be valuable for policymakers to recognize target populations for health educational activities in the outbreak.
Our study revealed an overall positive attitude by safety and security workers toward COVID-19 as a preventable disease as indicated by the fact that the majority of them agreed on this notion and were convinced of it being eventually successfully controlled. The confidence of the participants on the ability of Saudi Arabia to eradicate this new epidemic was consistent with the findings from other studies conducted in Saudi Arabia (22), China (7), and Malaysia (18), supporting the confidence on its curability and their respective countries succeeding in the battle against the pandemic. In our study, the positive attitude and high confidence level of the participants were probably built on the previous experience of the Saudi government in response to the Middle East Respiratory Syndrome (MERS) epidemic in 2012 (28), which helped the country reinstate the improved public health alerting system and infection control policies. Thus, the experience gathered from combating MERS placed Saudi Arabia on a high sense of alert and readiness to take instant action and drastic measures to curb the spread of COVID-19 (29). In line with this, the country imposed a number of extreme measures such as enforced lockdown, implementing curfews, stopping all flights (domestic and international), suspending Umrah, interdiction of social and religious gatherings, restricting outdoor activities, closure of mosques, and suspension of schools and universities eventual shifting to remote learning and virtual classrooms.
In the current study, the majority of the safety and security workers were following good and safe COVID-19 prevention practices. Most participants reported taking precautions such as avoiding crowded places, practicing proper hand hygiene, covering their nose and mouth when sneezing or coughing, and wearing face masks on leaving their homes. These are very vital practices to prevent the person to person transfer of the disease. In addition, females and respondents residing outside Riyadh or employed in private sectors had better practices as compared to their male counterparts. The findings related to prevention practices are consistent with those from other studies such as that of Alahdal et al. (23) in Saudi Arabia, Azlan et al. (18) in Malaysia, Olum et al. (15) in Uganda, Zhong et al. (7) in China, Abdel Wahed et al. (30) in Egypt, and Almofada et al. (31) and Al-Hanawi et al. (22) in Saudi Arabia. These preventive practices are attributable to the educational materials provided by the MOH and WHO through multiple media platforms for the detection, prevention, and control of COVID-19. It is important to focus on providing precise knowledge to individuals as this has a significant influence on the attitudes and practices in a pandemic. In this study, a higher knowledge level was displayed in both the attitude and practice of the participants as demonstrated by the Spearman correlation test showing a significant positive relationship between knowledge as well as both the attitude and practices of security and safety workers toward COVID-19.
Lastly, the information on COVID-19 used by most of the participants in our study was acquired primarily through television, followed by internet and social media. This is concordant with previous studies pointing similarly to TV and/or radio (32) and social media (33) as the primary sources of information, therefore highlighting the important roles for these platforms in spreading knowledge. However, while social media and internet platforms provide an easy accessibility to information, they can also be a source of misinformation. Currently, a vast diversity of information is readily available through the internet, including unverified malicious information that can spread quickly and misguide individuals, hence causing fear and anxiety among the population. People with anxiety may become panicked and are more likely to make mistakes leading to irrational behavior. Likewise, a cross-sectional study among dental professionals in 30 different countries across the globe reported that dentists were in a state of anxiety of getting infected and fear of carrying infections from their practices to their families while working during the current viral outbreak (34). On the other hand, it can be assumed that a clear communication and an updated educational content provided by the MOH about COVID-19 through multiple media platforms probably contributed to improving public knowledge and preparedness during the current pandemic (31).
This study has some limitations. These include the convenient sampling and self-reported questionnaires which partly depended on participant honesty and recall ability which may therefore be subject to a recall bias. Moreover, our study was designed as a cross-sectional survey, thereby limiting our ability to identify causality between study variables. In addition, there is yet a lack of studies assessing the KAP of safety and security workers during the COVID-19 pandemic worldwide, which limited our ability to compare our findings with similar groups. Accordingly, we suggest cohort studies in future to validate our findings.
Conclusion
Our study suggests that most of the safety and security workers possessed sufficient knowledge and positive attitude as well as exercised appropriate practices toward COVID-19. The significant predictors for the positive attitude were gender, educational level, age, and workplace similar to those found in previous studies. Also, in this study, a better knowledge level was reflected in both the attitude and practices of the participants. This finding demonstrates that virtuous knowledge is important in empowering individuals to demonstrate better attitudes and practices for current pandemic risk reduction as well as for future epidemics.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by King Saud University College of Medicine Institutional Review Board. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MA, AA, HA, and GA conceptualized the study. HA and GA collected data. MA analyzed and interpreted the data. MA and FK wrote the first draft. AA, FSA, FYA, and GS edited the draft. MA and FK reviewed and edited the final manuscript. All authors approved the final version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors extend their appreciation to the Deputyship for Research & Innovation, “Ministry of Education” in Saudi Arabia for funding this research work through the project number IFKSURG-2020-107.
References
1. Chen NS, Zhou M, Dong X, Qu JM, Gong FY, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
2. Huang CL, Wang YM, Li XW, Ren LL, Zhao JP, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
3. Khurshid Z, Asiri FYI, Al Wadaani H. Human saliva: non-invasive fluid for detecting novel coronavirus (2019-nCoV). Int J Environ Res Public Health. (2020) 17:e1–4. doi: 10.3390/ijerph17072225
4. Baradaran A, Ebrahimzadeh MH, Baradaran A, Kachooei AR. Prevalence of comorbidities in COVID-19 patients: a systematic review and meta-Analysis. Arch Bone Jt Surg. (2020) 8(Suppl. 1):247–55. doi: 10.22038/abjs.2020.47754.2346
5. US Food and Drug Administration. FDA's Approval of Veklury (remdesivir) for the Treatment of COVID-19—The Science of Safety and Effectiveness. Available online at: https://www.fda.gov/drugs/drug-safety-and-availability/fdas-approval-veklury-remdesivir-treatment-covid-19-science-safety-and-effectiveness (assessed November 08, 2020).
6. Azim AA, Shabbir J, Khurshid Z, Zafar MS, Ghabbani HM, Dummer PMH. Clinical endodontic management during the COVID-19 pandemic: a literature review and clinical recommendations. Int Endod J. (2020) 53:1461–71. doi: 10.1111/iej.13406
7. Zhong BL, Luo W, Li HM, Zhang QQ, Liu XG, Li WT, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. (2020) 16:1745–52. doi: 10.7150/ijbs.45221
8. Alsofayan YM, Althunayyan SM, Khan AA, Hakawi AM, Assiri AM. Clinical characteristics of COVID-19 in Saudi Arabia: a national retrospective study. J Infect Public Health. (2020) 13:920–5. doi: 10.1016/j.jiph.2020.05.026
9. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. (2020) 91:157–60. doi: 10.23750/abm.v91i1.9397
10. WHO Coronavirus Disease (COVID-19) Dashboard. Global Situation. Available online at: https://covid19.who.int/. (assessed September 24, 2020).
11. WHO Coronavirus Disease (COVID-19) Dashboard. Saudi Arabia Situation. Available online at: https://covid19.who.int/region/emro/country/sa (assessed September 24, 2020).
12. Alshammari TM, Altebainawi AF, Alenzi KA. Importance of early precautionary actions in avoiding the spread of COVID-19: Saudi Arabia as an example. Saudi Pharm J. (2020) 28:898–902. doi: 10.1016/j.jsps.2020.05.005
13. Wikipedia.  2020. Available online at: https://ar.wikipedia.org/wiki/%D8%AC%D8%A7%D8%A6%D8%AD%D8%A9_%D9%81%D9%8A%D8%B1%D9%88%D8%B3_%D9%83%D9%88%D8%B1%D9%88%D9%86%D8%A7_%D9%81%D9%8A_%D8%A7%D9%84%D8%B3%D8%B9%D9%88%D8%AF%D9%8A%D8%A9_2020 (assessed November 12, 2020).
2020. Available online at: https://ar.wikipedia.org/wiki/%D8%AC%D8%A7%D8%A6%D8%AD%D8%A9_%D9%81%D9%8A%D8%B1%D9%88%D8%B3_%D9%83%D9%88%D8%B1%D9%88%D9%86%D8%A7_%D9%81%D9%8A_%D8%A7%D9%84%D8%B3%D8%B9%D9%88%D8%AF%D9%8A%D8%A9_2020 (assessed November 12, 2020).
14. Alarabiya News.  . Available online at: https://ara.tv/ckvcj (assessed October 06, 2020).
. Available online at: https://ara.tv/ckvcj (assessed October 06, 2020).
15. Olum R, Chekwech G, Wekha G, Nassozi DR, Bongomin F. Coronavirus disease-2019: knowledge, attitude, and practices of health care workers at Makerere University Teaching Hospitals, Uganda. Front Public Health. (2020) 8:181. doi: 10.3389/fpubh.2020.00181
16. Person B, Sy F, Holton K, Govert B, Liang A, National Center for Inectious Diseases SCOT. Fear and stigma: the epidemic within the SARS outbreak. Emerg Infect Dis. (2004) 10:358–63. doi: 10.3201/eid1002.030750
17. Raosoft Sample Size Calculator. Available online at: http://www.raosoft.com/samplesize.html (accessed March 20, 2020).
18. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS ONE. (2020) 15:e0233668. doi: 10.1371/journal.pone.0233668
19. Rayhan RU, Zheng Y, Uddin E, Timbol C, Adewuyi O, Baraniuk JN. Administer and collect medical questionnaires with Google documents: a simple, safe, and free system. Appl Med Inform. (2013) 33:12–21.
20. Leung GM, Quah S, Ho LM, Ho SY, Hedley AJ, Lee HP, et al. A tale of two cities: community psychobehavioral surveillance and related impact on outbreak control in Hong Kong and Singapore during the severe acute respiratory syndrome epidemic. Infect Control Hosp Epidemiol. (2004) 25:1033–41. doi: 10.1086/502340
21. Yap J, Lee VJ, Yau TY, Ng TP, Tor PC. Knowledge, attitudes and practices towards pandemic influenza among cases, close contacts, and healthcare workers in tropical Singapore: a cross-sectional survey. BMC Public Health. (2010) 10:442. doi: 10.1186/1471-2458-10-442
22. Al-Hanawi MK, Angawi K, Alshareef N, Qattan AMN, Helmy HZ, Abudawood Y, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front Public Health. (2020) 8:217. doi: 10.3389/fpubh.2020.00217
23. Alahdal H, Basingab F, Alotaibi R. An analytical study on the awareness, attitude and practice during the COVID-19 pandemic in Riyadh, Saudi Arabia. J Infect Public Health. (2020) 13:1446–52. doi: 10.1016/j.jiph.2020.06.015
24. Alyami HS, Orabi MAA, Aldhabbah FM, Alturki HN, Aburas WI, Alfayez AI, et al. Knowledge about COVID-19 and beliefs about and use of herbal products during the COVID-19 pandemic: a cross-sectional study in Saudi Arabia. Saudi Pharm J. (2020) 28:1326–32. doi: 10.1016/j.jsps.2020.08.023
25. Naser AY, Dahmash EZ, Alwafi H, Alsairafi ZH, Al Rajeh AM, Alhartani YJ, et al. Knowledge and practices towards COVID-19 during its outbreak: a multinational cross-sectional study. medRxiv-Infect Dis(except HIV/AIDS). (2020). doi: 10.1101/2020.04.13.20063560
26. Ssebuufu R, Sikakulya FK, Mambo SB, Wasingya L, Nganza SK, Ibrahim B, et al. Knowledge, attitude, and self-reported practice toward measures for prevention of the spread of covid-19 among Ugandans: a nationwide online cross-sectional survey. Front Public Health. (2020) 8:618731. doi: 10.3389/fpubh.2020.618731
27. Sarfaraz S, Shabbir J, Mudasser MA, Khurshid Z, Al-Quraini AAA, Abbasi MS, et al. Knowledge and attitude of dental practitioners related to disinfection during the COVID-19 pandemic. Healthcare. (2020) 8:e1–9. doi: 10.3390/healthcare8030232
28. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. (2012) 367:1814–20. doi: 10.1056/NEJMoa1211721
29. Algaissi AA, Alharbi NK, Hassanain M, Hashem AM. Preparedness and response to COVID-19 in Saudi Arabia: building on MERS experience. J Infect Public Health. (2020) 13:834–8. doi: 10.1016/j.jiph.2020.04.016
30. Abdel Wahed WY, Hefzy EM, Ahmed MI, Hamed NS. Assessment of knowledge, attitudes, and perception of health care workers regarding COVID-19, a cross-sectional study from Egypt. J Community Health. (2020) 45:1242–51. doi: 10.1007/s10900-020-00882-0
31. Almofada SK, Alherbisch RJ, Almuhraj NA, Almeshary BN, Alrabiah B, Al Saffan A, et al. Knowledge, attitudes, and practices toward COVID-19 in a Saudi Arabian population: a cross-sectional study. Cureus. (2020) 12:e8905. doi: 10.7759/cureus.8905
32. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. (2020) 13:1949–60. doi: 10.2147/IDR.S258736
33. Bhagavathula AS, Aldhaleei WA, Rahmani J, Mahabadi MA, Bandari DK. Knowledge and perceptions of COVID-19 among health care workers: cross-sectional study. JMIR Public Health Surveill. (2020) 6:e19160. doi: 10.2196/19160
Keywords: COVID-19, pandemic, attitudes, practices, worker
Citation: AlRasheed MM, Alsugair AM, Almarzouqi HF, Alonazi GK, Aleanizy FS, Alqahtani FY, Shazly GA and Khurshid F (2021) Assessment of Knowledge, Attitude, and Practice of Security and Safety Workers Toward the COVID-19 Pandemic: A Cross-Sectional Study. Front. Public Health 9:631717. doi: 10.3389/fpubh.2021.631717
Received: 20 November 2020; Accepted: 01 March 2021;
Published: 28 April 2021.
Edited by:
Zohaib Khurshid, King Faisal University, Saudi ArabiaReviewed by:
Juzer Shabbir, Dow University of Health Sciences, PakistanMuhammad Adeel Ahmed, King Faisal University, Saudi Arabia
Copyright © 2021 AlRasheed, Alsugair, Almarzouqi, Alonazi, Aleanizy, Alqahtani, Shazly and Khurshid. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maha M. AlRasheed, bWFoYWxyYXNoZWVkQGtzdS5lZHUuc2E=