 Heba Saadeh1*
Heba Saadeh1* Reem Q. Al Fayez2
Reem Q. Al Fayez2 Assem Al Refaei3
Assem Al Refaei3 Nour Shewaikani3
Nour Shewaikani3 Hamzah Khawaldah4
Hamzah Khawaldah4 Sobuh Abu-Shanab5
Sobuh Abu-Shanab5 Maysa Al-Hussaini6,7
Maysa Al-Hussaini6,7- 1Department of Computer Science, King Abdullah II School of Information Technology Faculty, The University of Jordan, Amman, Jordan
- 2Department of Computer Information System, King Abdullah II School of Information Technology Faculty, The University of Jordan, Amman, Jordan
- 3School of Medicine, The University of Jordan, Amman, Jordan
- 4Department of Geography, School of Arts, The University of Jordan, Amman, Jordan
- 5Psychosocial Program, King Hussein Cancer Center, Amman, Jordan
- 6Department of Pathology and Laboratory Medicine, King Hussein Cancer Center, Amman, Jordan
- 7Human Research Protection Program Office, King Hussein Cancer Center, Amman, Jordan
To reduce the spread of COVID-19, Jordan enforced 10 weeks of home quarantine in the spring of 2020. A cross-sectional study was designed to assess this extended quarantine's effect on smartphone addiction levels among undergraduates. A random sample of 6,157 undergraduates completed an online questionnaire (mean age 19.79 ± 1.67 years; males 28.7%). The questionnaire contains different sections to collect socio-demographic, socio-economic, academic, quarantine-related information, and smartphone usage. The smartphone addiction scale-short version was used to assess the degree of addiction during the quarantine. The mean addiction score across the whole sample was 35.66 ± 12.08, while the prevalence of addiction among participants was 62.4% (63.5% in males and 61.9% in females). The majority of the participants (85%) reported that their smartphone usage during the quarantine increased or greatly increased (27.6 and 57.2%, respectively), with some 42% using their smartphones for more than 6 h a day. Nevertheless, three-quarters of the students wished to reduce their smartphone usage. Several demographic and quarantine factors have been assessed, and students' gender, the field of study, parental education, household income in addition to the location of quarantine (urban, rural) and the house specifications (apartment, independent house, with/without a garden) showed statistically significant associations with smartphone addiction during the quarantine. Female students, students studying scientific- and medical-related majors compared to those studying humanity majors, those with higher incomes, those who had been quarantined in an apartment without a garden, and those who lived in urban areas showed significantly higher addiction scores.
Introduction
The novel coronavirus 2019 (COVID-19) infected more than 180 million people in 222 countries and killed around 4 million globally (as of 07/07/2021), according to the World Health Organization (1, 2). This disease is a severe acute respiratory syndrome caused by betacoronavirus (SARS-CoV-2), which might disrupt the human body's normal immune response and cause lots of implications (3, 4). Therefore, the vagaries of this pandemic forced many countries to take severe actions to protect their citizens from infection. Jordan applied complete lockdown around mid-March 2020, closing all schools, universities, shops, public and private sectors, borders, and airlines, forbidding any civil movement for several days. A curfew was then applied to restrict all movement, allowing only short walks and for short periods. The majority of the population was under home quarantine for around 10 weeks. These extreme measures helped contain the spread of the virus and controlled the number of casualties and deaths in Jordan in the spring and summer of 2020. Due to the countrywide closure, schools, universities, and companies moved to online platforms for distance learning and remote working. This new lifestyle, enforced by staying at home and under quarantine, has brought new challenges socially, economically, physiologically, and psychologically (5–9).
One significant lifestyle shift is the complete reliance on the internet and smart devices, like tablets, laptops, and mobiles. During the quarantine, with the necessary social/spatial distancing, the usage of these smart devices increased at an increasingly fast pace. Unfortunately, this total dependence has shown to be a form of addiction, i.e., a compulsive physiological need for and use of a habit-forming substance (10). Nowadays, addiction is not only restricted to extensive substance or drug abuse but also extends to the behavioral obsession with a specific activity that disturbs people's healthy daily lives. Recently, internet-based activities, like online gaming, chatting, and communications through the different available applications, have shown similar addiction levels to those of drugs (11–13).
The impact of internet misusage has increased significantly due to its high accessibility through smartphones, especially during the COVID-19 pandemic. Mobile phones are widely used; around 60% of the world's population and 80% of Jordanian households have mobiles (14, 15). In the past year alone, Jordanian mobile phone connections, internet users, and active social media users increased by 1.7, 1.2, and 7.4%, respectively (15). Several studies have identified the prevalence of smartphone addiction risks in different countries, using the smartphone addiction scale-short version (SAS-SV) (16–25). Although a few recent studies have highlighted the different aspects of internet usage related to COVID-19 (26–29), none, to the best of our knowledge, have examined smartphone addiction during the current lockdown and quarantine. This is the first research that presents a large-scale study of thousands of Jordanian undergraduate students to assess the effect of COVID-19 extended home quarantine on smartphone addiction levels. This is assessed by collecting many exposures to cover the demographic, economic, and quarantine-related factors that might worsen the effect of quarantine on smartphone overuse.
Methods
Participants
Responses to the online questionnaire were submitted by 7,146 undergraduates at the University of Jordan (UJ) during the April and May of 2020. After cleaning the data by removing all duplications, 6,157 unique participants who had fully completed the online questionnaire and participated voluntarily remained for analysis. There was no missing data as all the questions were mandatory. Participants could withdraw at any time by failing to answer any of the questions. The study's purpose and procedures had been approved by the Institutional Review Board and the Research Ethics Committee at UJ.
Participants' ages ranged between 17 and 30 years, with a mean of 19.79 ± 1.67. 1,769 students were male (28.7%) and 4,388 female (71.3%). Half were studying humanities-related majors and around one-third scientific majors, with the rest studying medical-related majors. Nearly half of the students were in their first year.
Measurements
This study focuses on the association between the new lifestyle forced by home quarantine and smartphone usage, which might even reach the addiction level. The online questionnaire was distributed in Arabic, the Arabic version of the SAS-SV was validated in 2018 (30), targeting all UJ undergraduates and ensuring that all the participants fully understood the questions and the accompanying choices. The questionnaire contains several sections, collecting an extensive list of exposures, like socio-demographic, socio-economic, and quarantine-related information, in addition to the 10 items of the SAS-SV to measure the primary outcome: smartphone addiction level. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines for observational cross-sectional studies were used to guide the reporting of this study (31).
Socio-Demographic/Socio-Economic Variables
The study examined the participants' different socio-demographic measures: gender, age, place of residence, class (year at university), academic major (Scientific, Medical, or Humanities), academic performance ranging from acceptable to excellent, and their smoking practices. The study also collected a few socio-economic factors, such as parental education levels, parental employment status, and household income level ranging from <200 JD ($282) to more than 1,500 JD ($2,115).
Quarantine Variables
To assess the association between smartphone addiction and quarantine, 12 questions were listed. Some questions asked about the place of residence during quarantine, whether in a city or a village and the house specifications, like an apartment or a house with or without a garden. The study also asked about the number of people quarantined with each student, ranging from 0 to >10, how many children are among them, and whether they have specific health issues, including chronic diseases. The students were also asked about communication with the family members who lived with them and those who did not. Furthermore, questions about students' hobbies, including newly practiced ones started during the quarantine, and the household income during quarantine, whether it remained the same, increased, decreased, or stopped altogether, were included.
Smartphone Usage
Smartphone Addiction Scale–Short Version
The original scale consisted of 33 items developed by Kwon et al. (29). The same authors developed the short version (SAS-SV) scale in 2013 (25) to evaluate smartphone addiction's level of risk and its prevalence, based on self-reporting. It has been validated and has greater durable internal consistency than the original version (25). It has 10 items (listed in the results section), each rated on a six-point Likert scale, ranging from strongly disagree (scores 1 point) to strongly agree (scores 6 points). A high score indicates high risk but does not diagnose an addiction. According to Kwon et al. (25), different cut-off values were suggested for each gender: 31 for males and 33 for females. In this study, the short version scale was used to reduce the number of questions the participants needed to answer.
Usage of the Smartphone During Home Quarantine
In addition to the addiction scale, the questionnaire included a few questions regarding the number of hours spent using smartphones per day. Students were also asked about the most frequent smartphone applications (Facebook, YouTube, Twitter, Snapchat, Instagram, and Netflix) used before and during the quarantine, and the level of change in usage was assessed.
Statistical Analysis
Descriptive statistics were performed on the whole sample. Numerical and categorical variables were summarized as mean ± standard deviation and total numbers (percentages), respectively. Binary factors were tested for significance using a two-sample t-test, while factors with more than two values were analyzed using a one-way analysis of variance (ANOVA). Tukey Honestly Significance Difference (TukeyHSD) was used as a post-hoc analysis to follow up on the significant factors that resulted from the ANOVA to identify the pair of values that had a significant mean difference. The significant factors were further investigated using logistic regression to identify the significant predictors of the addiction state, and to control the potential confounding factors and selection bias. A threshold value of p = 0.05 was used to test for significance. All statistical analyses were performed using R version 4.0.0 and RStudio version 1.2.5042.
Results
The original sample consisted of 7,146 submissions, which were then reduced to 6,157 after omitting duplicated responses. Half of the 6,157 undergraduate students were in their first year; the average age was 19.79 ± 1.67. Around 70% (n = 4,388) were female, nearly half (n = 3,092) were studying humanities-related majors, and about 85% (n = 5,151) were non-smokers. The academic performance of the students was categorized into four levels: excellent (10.6%, n = 655), very good (33.5%, n = 2,065), good (33.4%, n = 2,057), and acceptable (22.5%, n = 1,380), as declared by the students themselves. The household income level of the participants ranged from <200 JD (1 JD = ~1.4 USD) to more than 1,500 JD; around 45% (n = 2,807) had very low to low income (<600 JD), around 30% (n = 1,906) had medium-level (600–1,000 JD), and the rest (n = 1,444) had high-level (more than a 1,000 JD) income. The majority of the students (77.2%, n = 4,751) lived in the capital city (Amman). Table 1 summarizes participants' demographics.
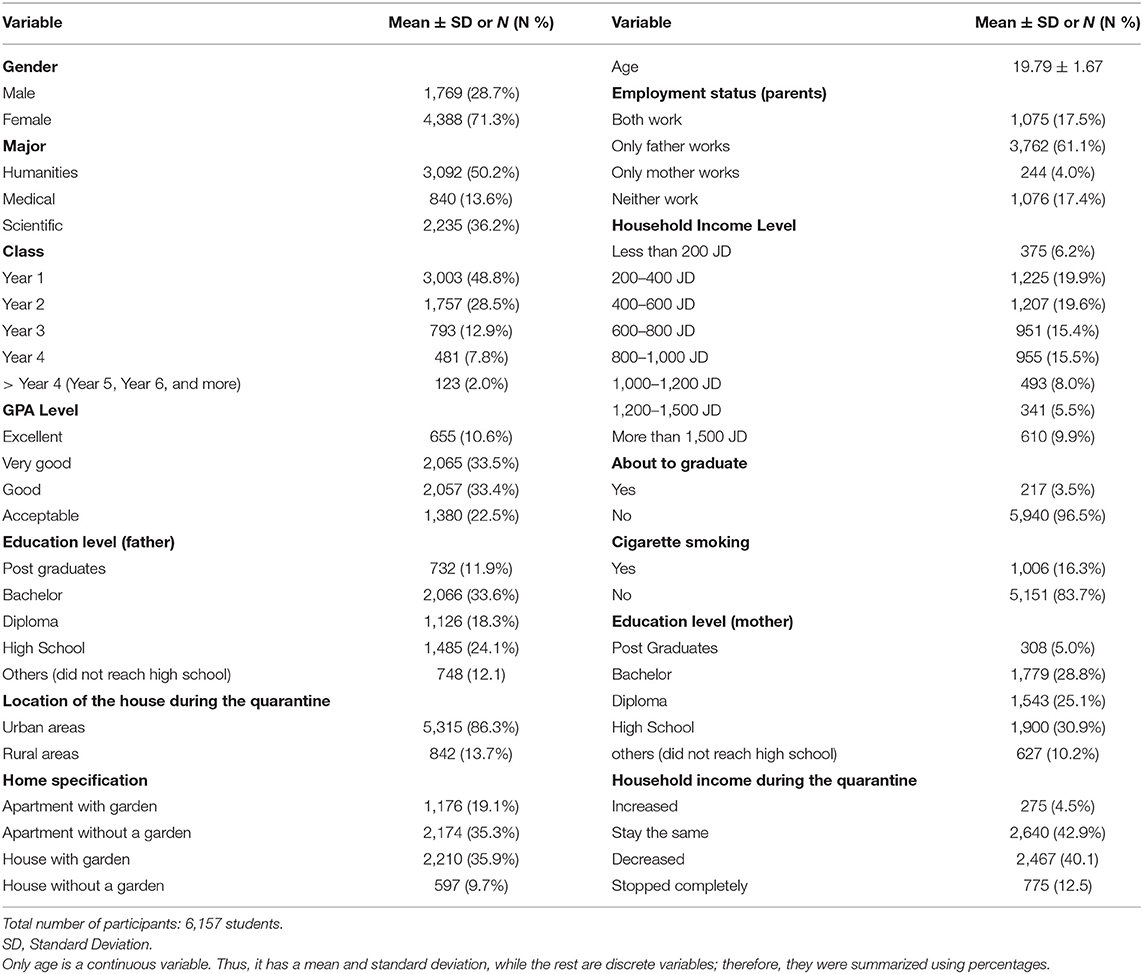
Table 1. Socio-demographic, socio-economic, and quarantine characteristics of study participants.
Parental employment status showed that for more than half of the students (61.1%, n = 3,762) only their father worked and 4%(n = 244) only their mother; 17.5% (n = 1,075) had both parents working, and a similar percentage (n = 1,076) neither. For about one-third (n = 2,066) of the students, their father was educated to bachelor level, and for a similar proportion (n = 1,900) their mother to high school level; only around 12% (n = 732) and 5% (n = 308) of the students had fathers and mothers educated to postgraduate level, respectively (Table 1).
Around one-seventh (n = 842) of the students lived in a village during the quarantine. An equal proportion (n = 2,174 and 2,210, ~35%) lived either in an apartment without a garden or in a house with a garden, with 55% (n = 3,386) living in a household with a garden. For nearly 50% (n = 3,242) of the students, their household income either decreased or completely stopped during the quarantine, indicating financial difficulties (Table 1).
During the quarantine, 77% (n = 4,741) of the students lived with 3–7 family members, and 43% (n = 2,648) were not quarantined with children (Figures 1A,B). More than half (n = 3,386) were quarantined with a smoker, about 20% (n = 1,416) with a diabetic patient, around 8% (n = 493) with a cardiac patient, and 17% (n = 1,047) with an elderly member of the family (>65 years) (Figure 1C). The majority of the students (89.7%, n = 5,523) increased communication with their families, and about 70% (n = 4,310) communicated more with a distant family member during the quarantine. Around 80% (n = 4,926) spent more time with their families than they normally do.
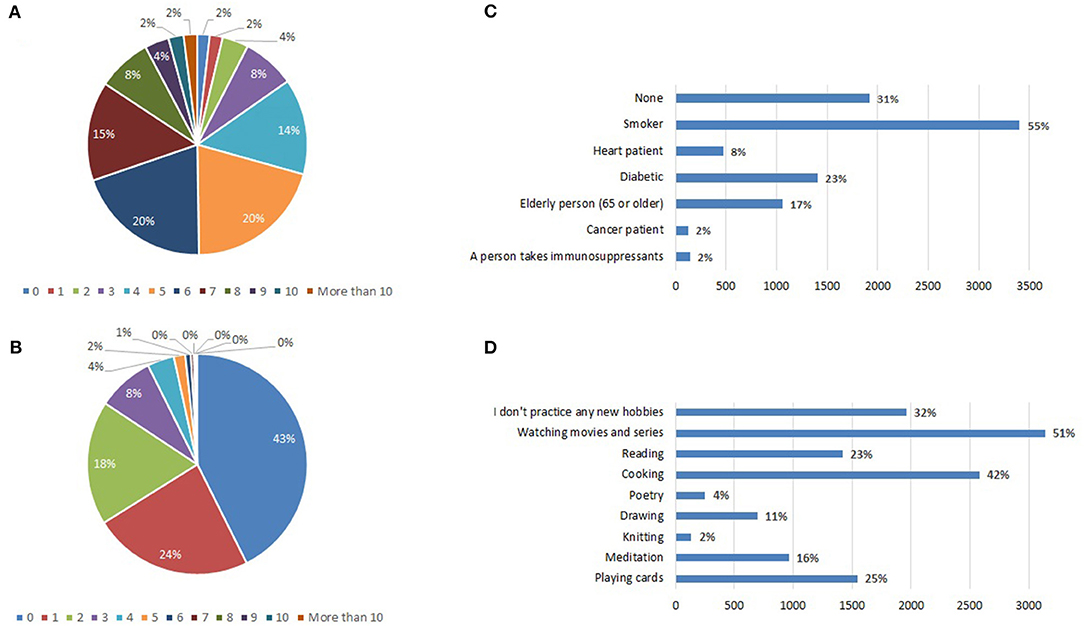
Figure 1. (A) Pie chart for the percentages of people quarantined with each of the study participants ranged from no one (0) to more than 10. (B) Similar to (A) but for the percentage of the children quarantined with each student. (C) Horizontal bar chart for the percentage of the quarantined people (with each student) with specific health issues. (D) Similar to (C) but for the percentages of the new hobbies that the students started to practice during the quarantine. X-axes in (C) and in (D) shows the frequency of the participants.
Nearly 70% (n = 4,310) of the students spent most of their time watching movies/series and/or sleeping and about 50% (n = 3,079) in eating/cooking. Many students (68%, n = 4,187) started new hobbies during quarantine (Figure 1D), including watching movies/series (51%, n = 3,140), cooking (42%, n = 2,586), board games (25%, n = 1,539), reading (23%, n = 1,416), meditation (16%, n = 985) and drawing (11%, n = 677).
The primary outcome (addiction level) was assessed by the SAS-SV. The 10 items in the SAS-SV are included in Table 2. Mean scores ranged from 3.21 (item 6: Table 2) to 4.02 (item 4: Table 2). The 10 items had totals ranging between 10 (all items scored 1) and 60 (all items scored 6) with a mean score of 35.66 ± 12.08. The associations between the different demographic and quarantine variables with smartphone addiction levels, i.e., SAS-SV scores, are presented in Table 3. The lowest SAS-SV score was 33.51 ± 13.25 (house without a garden: Table 3), and the highest 36.83 ± 11.63 (apartment without a garden: Table 3). The prevalence of addiction among participants was 62.4% (n = 3,841), representing potential excessive use, with a mean SAS-SV score of 43.18 and a standard deviation of 7.59. However, based on the suggested SAS-SV score threshold of ≥31 for males and ≥33 for females (25), the prevalence of addiction was 63.5% (n = 1,124, total number of males = 1,769) and 61.9% (n = 2,717, total number of females 4,388) with SAS-SV scores of 42.33 ± 7.85 and 43.53 ± 7.45 for males and females, respectively (Table 4).
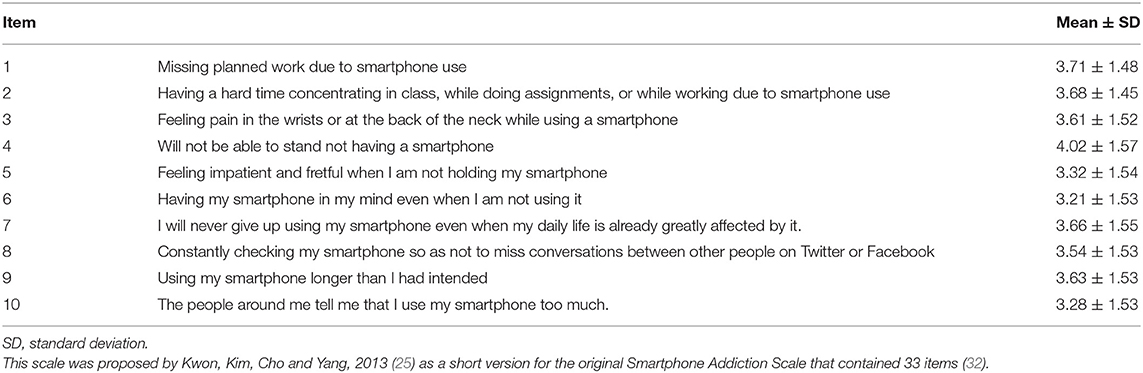
Table 2. Items of smartphone addiction scale–short version.
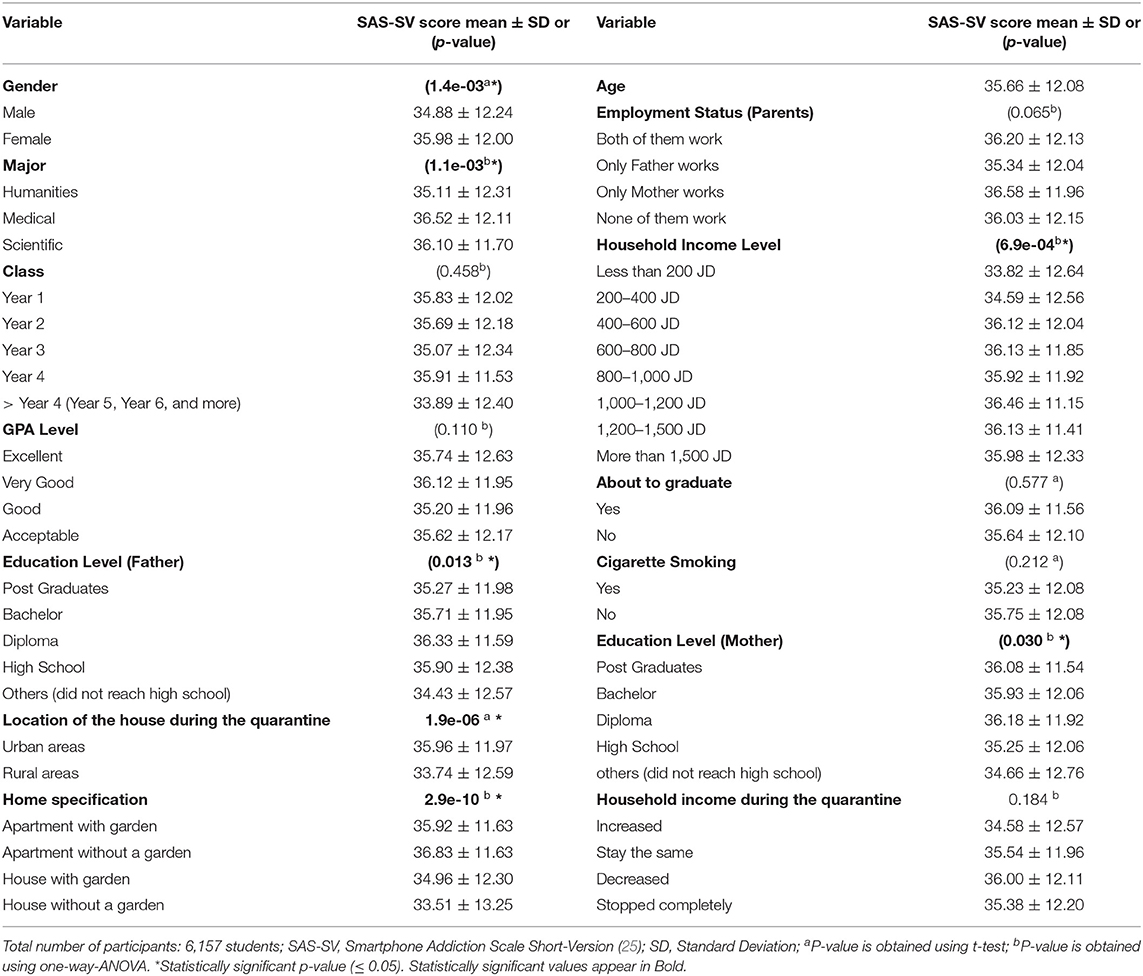
Table 3. Association between smartphone addiction level (SAS-SV score) and the socio-demographic, socio-economic and quarantine characteristics of the participants.
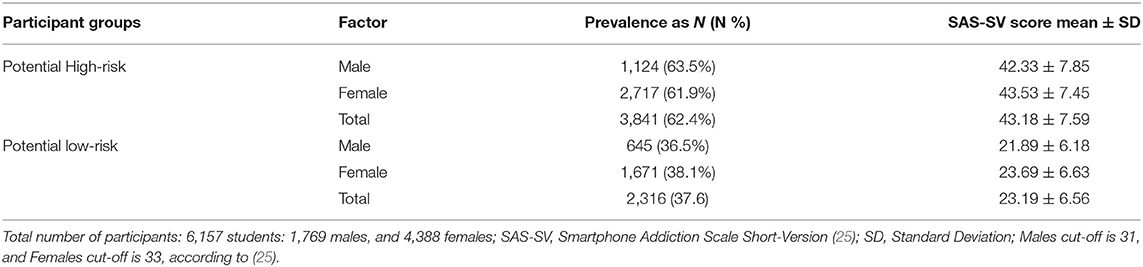
Table 4. Smartphone addiction prevalence among the study participants based on SAS-SV scores.
Among the tested binary variables, including the gender, graduation status, smoking habit, and the house location during the quarantine, both the graduation status and smoking habit variables were not significant (p > 0.05). Females and quarantine in urban areas were significantly associated with smartphone addiction (Table 3). Furthermore, the field of study (major), city, household income, parental education, and the house specifications were found significant (ANOVA p < 0.05). The mean difference between the humanities and each of the scientific and medical majors was significant (TukeyHSD p-values: 0.009 and 0.007, respectively), with the scientific and medical majors having a larger SAS-SV mean score than the humanities-related majors (Table 3). Although the mother's education had a significant association (ANOVA p-value: 0.030), the TukeyHSD analysis did not find any significant pair-wise comparison between its different values (p > 0.05); hence, this factor is not considered significantly associated with smartphone addiction levels. On the other hand, the household income had a significant association (ANOVA p-value: 6.9e-4), and this is mainly due to the difference between <200 JD and higher income levels (TukeyHSD p < 0.05). Likewise, the father's education (ANOVA p-value 0.013); only the comparison between a diploma and below high school was significant (TukeyHSD p-value: 0.007), while other education levels showed no significant associations (Table 3). Finally, house specifications were found to be significantly associated with addiction levels. Living in a house and not in an apartment, as well as having a garden, had lower SAS-SV scores. Quarantine in an apartment without a garden showed a higher significant association with smartphone addiction and the highest SAS-SV score (Table 3).
The six significant factors (ANOVA and TukeyHSD p < 0.05) of gender, house location, major, household income, father's education, and the house specifications were further investigated using logistic regression. The aim was to identify which of these factors was a significant potential predictor of the students' addiction state [calculated based on the suggested SAS-SV score thresholds of ≥31 for males and ≥33 for females (25)] (Table 5). As expected, quarantine in urban areas and studying health- or science-related majors had a significant positive association with addiction state. Quarantine in a house without a garden showed a significant negative association, indicating a SAS-SV score lower than other values, as listed in Table 3.
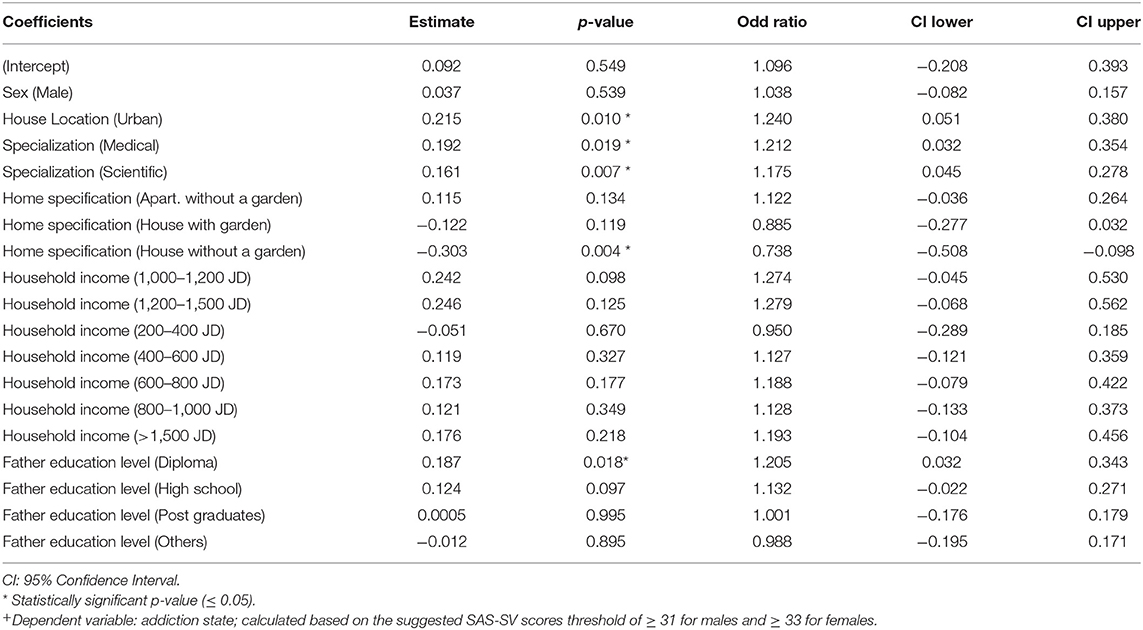
Table 5. Association between addiction state and each of the identified significant factors, as assessed by logistic regression+.
Around 85% (n = 5,234) of the students reported increased smartphone usage during quarantine, and only about 3% (n = 196) reduced their smartphone usage, which correlates well with the SAS-SV scores (Table 6). During this quarantine, around 42% (n = 2,575) of the students, despite their demographics, spent more than 6 h a day on their smartphones with very high SAS-SV scores (38.60 ± 11.18 for 6–8 h and 39.41 ± 13.23 for >8 h: Table 6). Only 3.6% (n = 223) of the students used their smartphones less than an hour per day, and they had relatively small SAS-SV scores (Table 6).
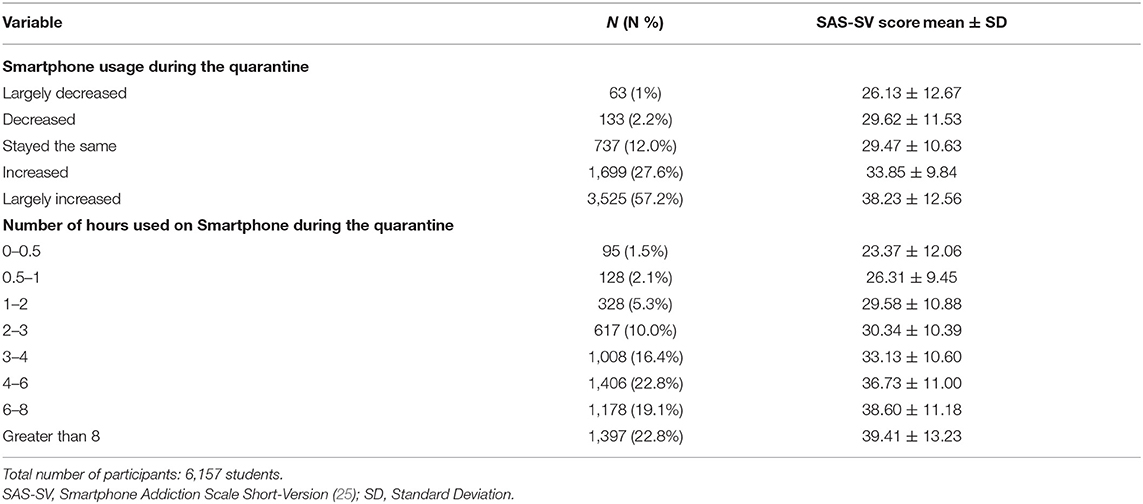
Table 6. Smartphone usage during quarantine and their associations with smartphone addiction level (SAS-SV score).
The top three applications widely used on smartphones before the quarantine were reported to be Facebook and its messenger, Instagram, then YouTube. These applications remained the top three applications used by the students during the quarantine (Table 7). However, the use of Facebook and Instagram was reduced by 5.4 and 9.6%, respectively, and the use of YouTube and Netflix increased by 6.8 and 9.9%, respectively (Figure 2 and Table 7).
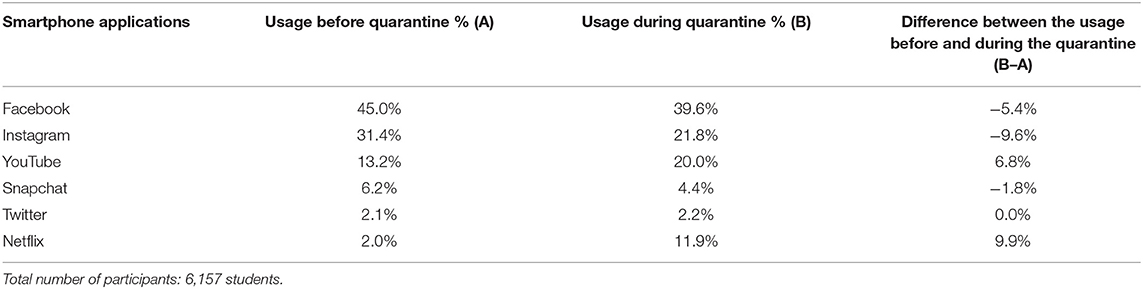
Table 7. Top smartphone applications used by the students before and during the quarantine.
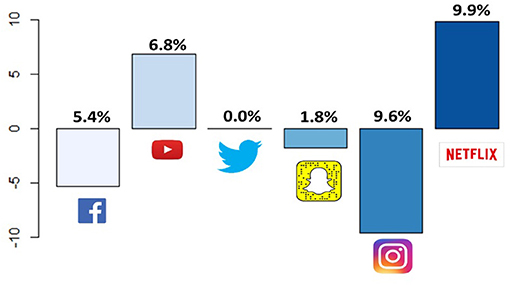
Figure 2. Absolute difference of smartphone applications usage (in percentages) before and during the quarantine.
Finally, around three-quarters (n = 4,690) of the students self-reported that they wished to change their smartphone usage by reducing the number of hours they spent using them. Only 3.4% (n = 208) wished to increase their usage, and around 20% (1,259) reported that they were satisfied with their current smartphone usage.
Discussion
The study was conducted on students at the University of Jordan, the largest public university in the capital, Amman (only 22.8% of the study participants lived outside the capital). UJ hosts around 50,000 students studying undergraduate and postgraduate degrees in humanities, science, and health disciplines. Six thousand one hundred fifty-seven undergraduates voluntarily completed the online questionnaire, comprising around 12.3% of UJ students. This sample of participants is a good representative of the demographics of the university since 76% of the UJ students are female, 50.3% are studying humanities-related majors, 10.5% have excellent GPA, and 22.5% have acceptable GPA; the figures for the study participants are 71.3% females, 50.2% studying humanities, and 10.6 and 22.5% with excellent and acceptable GPAs, respectively. The questionnaire link was uploaded with several obligatory university requirements, usually taken by students in their first 2 years, thus explaining why around 77% of the participants were in years 1 and 2, with a mean age of 20 years; only 3.5% were in their final semester (Table 1).
This sample is also comparable with the Jordanian population, according to the National Council for Family Affairs (NCFA) national survey in 2017 (33). About 78% of the participating families had 3–7 members, consistent with our sample demographics (Figure 1A). Furthermore, 54.4 and 45.6% of the students lived in an apartment or individual house, respectively (Table 1), which is also similar to the corresponding NCFA survey results of 57 and 42%. The NCFA reported that 19% of female adults in Jordanian families work, a similar percentage to the 21.5% of students whose mothers worked. Non-communicable chronic diseases prevail in society as 14.5 and 7.2% suffer from diabetes and cardiovascular diseases, respectively. 23 and 8% of the students in this sample were quarantined with a family member suffering from diabetes or cardiovascular diseases, respectively (Figure 1C). Tobacco smoking in Jordan, as reported by WHO (34), is more prevalent in males, with 70% of males aged more than 14 years being smokers (35); this explains the high proportion, nearly half, of the students quarantined with a smoker (Figure 1C). The preponderance of females in our sample might account for only 16.3% being smokers.
Regrettably, around 50% of parents in our sample had partially or entirely lost their jobs, reducing financial resources since the private sector was primarily affected by the countrywide closure (Table 1). Previous studies disagreed with the effect of household income on smartphone addiction (36, 37), while in this study, lower incomes were negatively associated with addiction scores (Table 3). Similarly, contradictory results were reported regarding parental education and phone usage (36, 38). Nevertheless, this study reported a significant association between parental education and smartphone addiction, precisely the difference between a diploma and below high school (Table 3).
Interestingly, the characteristics of a quarantine site had a significant effect on smartphone usage. Most of the Jordanian population lives in urban areas; hence, a small proportion of the participants were quarantined in rural areas (13.7%: Table 1). Quarantine in an apartment without a garden was significantly associated with addiction scores (Table 3). Additionally, a significant association between quarantine in urban areas and addiction scores is noted (Tables 3, 5). This can be explained by the tight surveillance and strict control the government imposed on the big cities compared to the rural areas, which provided fewer opportunities for practicing outdoor activities and encouraged spending more time on smartphones.
The COVID-19 pandemic home quarantine enforced a sudden and different lifestyle, an extended lockdown with strict rules for remaining indoors. About 70% of the students spent most of their time watching movies/series (Figure 1D). 85% reported an increase in smartphone usage, with about 42% spending more than 6 h a day on their smartphones. Additionally, with the limited available resources within families, many students relied on their mobile phones to attend the university's compulsory online teaching.
Several studies have assessed smartphone addiction among university students; however, none have evaluated its addiction and prevalence during a quarantine. SAS-SV results indicated that smartphone addiction was prevalent in a total of 3,841 (62.4%) participants (63.5% in males and 61.9% in females). The mean SAS-SV score for the potential high-risk group was 43.18 ± 7.59 (42.33 ± 7.85 in males and 43.53 ± 7.45 in females). These alarming results warrant validation and intervention. In comparison, our results are different from those reported in China: 29.8% (17), South Korea: 24.8% (25), Spain: 12.8% (18), Belgium: 21.5% (18), Switzerland: 16.9% (21), but comparable to Lebanon: 44.6% (19), Morocco: 55.8% (30), and Saudi Arabia: 71.9% (20). All previously mentioned studies used the same assessment scale; SAS-SV. Interestingly, another study in Jordan conducted before the COVID-19 pandemic that used a different assessment scale and different cut-offs (39) reported addiction prevalence of 59.8%, compared to 27.2% in Saudi Arabia, 17.3% in Sudan, and 8.6 in Yemen, re-enforcing our findings of mobile phone overuse in Jordan.
The high prevalence of smartphone usage among the students is alarming and raises warning flags on the high risk of excessive use among Jordanians in general and during the quarantine in particular. Depression and anxiety are among the potential contributors to increased addiction to smartphones (40), factors which also increased under quarantine conditions (6, 41). A gender-based effect of mobile phone addiction was reported previously, with the prevalence of females showing more addictive symptoms and reporting more intensive use than males (39, 42–45), agreeing with our findings. Furthermore, a significant association between addiction levels and students' majors was observed in previous research; humanities, but not scientific and medical studies, were more commonly associated with smartphone addiction (39, 46–48). This contradicts our findings. Relying on smartphones for distance learning is more common in scientific/medical majors than humanities, which rely more on hard copy. Finally, although a few studies have demonstrated an association between academic performance and mobile addiction (49–51), no significance was reported in this study (p-value: 0.11).
Whether this can be classified as an addiction or overuse is still debatable (52). Panova et al. argue that the strict definition of addiction is not fulfilled in smartphone overuse. Smartphone soveruse is not associated with significant functional, financial or physical impairment. Besides, an increase in smartphone use is not equivalent to tolerance; nowadays, smartphone use is a normalized part of everyday life in many societies, even when engaged with very frequently (52). This is precisely what the students encountered during the quarantine. The dependence on distance learning, the substitution of hardcopy books and journal references with softcopies, affluence, and affordable free applications all helped direct the students toward smartphone overuse.
The study's limitations include the dependence on self-reporting of the use of smartphones, which might be associated with recall bias, thus under- or over-estimation. In addition, all students were from the same university, which might be associated with selection bias. However, the large number of participants (6,157), spread over various economic sectors, is an accurate reflection of Jordanian society, rendering the results generalizable. Another limitation is the potential selection bias resulted from having around 70% of female participants. More balanced selection criteria would be better to apply. However, this factor was controlled in the logistic regression model. Furthermore, increasing the reliance on remote learning during the imposed quarantine might be associated with the overuse of smartphones. The study should be repeated outside the quarantine period to give a better insight into the magnitude and the socio-cultural factors related to smartphone overuse.
Conclusions and Recommendations
Quarantine is a stressful situation with several challenges, casting its shadow over routine life. No previous study has assessed the relationship between quarantine and smartphone addiction levels during the quarantine period. Female gender, urban areas, apartment quarantine, higher income, and scientific and medical majors had higher and significant overuse scores. The SAS-SV scores are higher than previously reported scores for other countries, although they are comparable to other countries in the region (39). Whether an addiction or overuse, the high scores and prevalence reported are alarming and indicate the severity of smartphone dependence among Jordanian university students during the quarantine. A repeat questionnaire on a comparable study population with follow-up interventions is warranted.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Institutional Review Board and the Research Ethics Committee at the University of Jordan. The ethics committee waived the requirement of written informed consent for participation.
Author Contributions
HS conceived the idea, performed the analysis, and wrote the manuscript. RA performed the pre-processing and part of the statistical analysis and figures. HK performed part of the statistical analysis. AA, NS, and SA-S contributed to the literature search. MA-H co-wrote the manuscript and helped in designing the study. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Coronavirus disease (COVID-19) (2019). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019
2. Coronavirus Update (Live)0,.134,980,610 Cases 2,921,163 Deaths from COVID-19 Virus Pandemic-Worldometer [Internet]. (2021). Available online at: https://www.worldometers.info/coronavirus/
3. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
4. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
5. Sahu P. Closure of universities due to coronavirus disease 2019 (COVID-19): Impact on Education and Mental Health of Students and Academic Staff. Cureus. (2020). 12:e7541. doi: 10.7759/cureus.7541
6. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
7. Mattioli AV, Ballerini Puviani M, Nasi M, Farinetti A. COVID-19 pandemic: the effects of quarantine on cardiovascular risk. Eur J Clin Nutr. (2020) 852–5. doi: 10.1038/s41430-020-0646-z
8. Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg. (2020) 8:185–93. doi: 10.1016/j.ijsu.2020.04.018
9. Gilat R, Cole BJ. COVID-19, medicine, and sports. Arthrosc Sports Med Rehabil. (2020). 2:e175–6. doi: 10.1016/j.asmr.2020.04.003
10. Maddux JF, Desmond DP. Addiction or dependence? Addiction. (2000) 95:661–5. doi: 10.1046/j.1360-0443.2000.9556611.x
11. Lee Y-S. Biological model and pharmacotherapy in internet addiction. J Korean Med Assoc. (2006) 49:209. doi: 10.5124/jkma.2006.49.3.209
12. Kuss DJ, Griffiths MD. Online social networking and addiction-A review of the psychological literature. In J Environ Res Public Health. (2011) 8:3528–52. doi: 10.3390/ijerph8093528
13. Griffiths MD, Kuss DJ, Billieux J, Pontes HM. The evolution of internet addiction: a global perspective. Addict Behav. (2016) 53:193–5. doi: 10.1016/j.addbeh.2015.11.001
14. Global Digital Overview. DataReportal – Global Digital Insights [Internet]. (2020). Available online at: https://datareportal.com/global-digital-overview
15. Digital 2020. Jordan—DataReportal–Global Digital Insights [Internet]. (2020). Available online at: https://datareportal.com/reports/digital-2020-jordan
16. Sohn S, Rees P, Wildridge B, Kalk NJ, Carter B. Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: a systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry. (2019) 19:356. doi: 10.1186/s12888-019-2350-x
17. Chen B, Liu F, Ding S, Ying X, Wang L, Wen Y. Gender differences in factors associated with smartphone addiction: a cross-sectional study among medical college students. BMC Psychiatry. (2017) 17:341. doi: 10.1186/s12888-017-1503-z
18. Lopez-Fernandez O. Short version of the smartphone addiction scale adapted to spanish and french: towards a cross-cultural research in problematic mobile phone use. Addict Behav. (2017) 64:275–80. doi: 10.1016/j.addbeh.2015.11.013
19. Hawi NS, Samaha M. To excel or not to excel: strong evidence on the adverse effect of smartphone addiction on academic performance. Comput Educ. (2016) 98:81–9. doi: 10.1016/j.compedu.2016.03.007
20. Venkatesh E, Al Jemal MY, Al Samani AS. Smart phone usage and addiction among dental students in saudi arabia: a cross sectional study. Int J Adolesc Med Health. (2019) 31(1). doi: 10.1515/ijamh-2016-0133
21. Haug S, Paz Castro R, Kwon M, Filler A, Kowatsch T, Schaub MP. Smartphone use and smartphone addiction among young people in Switzerland. J Behav Addict. (2015) 4:299–307. doi: 10.1556/2006.4.2015.037
22. Lee EB. Too much information: heavy smartphone and facebook utilization by african american young adults. J Black Stud. (2015) 46:44–61. doi: 10.1177/0021934714557034
23. Lee H, Ahn H, Nguyen TG, Choi SW, Kim DJ. Comparing the self-report and measured smartphone usage of college students: a pilot study. Psychiatry Investig. (2017) 14:198–204. doi: 10.4306/pi.2017.14.2.198
24. Yuchang J, Cuicui S, Junxiu A, Junyi L. Attachment styles and smartphone addiction in chinese college students: the mediating roles of dysfunctional attitudes and self-esteem. Int J Ment Health Addict. (2017) 15:1122–34. doi: 10.1007/s11469-017-9772-9
25. Kwon M, Kim DJ, Cho H, Yang S. The smartphone addiction scale: development and validation of a short version for adolescents. PLoS ONE. (2013) 8:e83558. doi: 10.1371/journal.pone.0083558
26. Pontes HM, Stavropoulos V, Griffiths MD. Emerging insights on internet gaming disorder: conceptual and measurement issues. Addict Behav Rep. (2020) 11:100242. doi: 10.1016/j.abrep.2019.100242
27. King DL, Delfabbro PH, Billieux J, Potenza MN. Problematic online gaming and the COVID-19 pandemic. J Behav Addict. (2020) 9:184–6. doi: 10.1556/2006.2020.00016
28. Király O, Potenza MN, Stein DJ, King DL, Hodgins DC, Saunders JB, et al. Preventing problematic internet use during the COVID-19 pandemic: consensus guidance. Compr Psychiatry. (2020) 100:152180. doi: 10.1016/j.comppsych.2020.152180
29. Dubey MJ, Ghosh R, Chatterjee S, Biswas P, Chatterjee S, Dubey S. COVID-19 and addiction. Diabet Metab Syndr Clin Res Rev. (2020) 14:817–23. doi: 10.1016/j.dsx.2020.06.008
30. Sfendla A, Laita M, Nejjar B, Souirti Z, Touhami AAO, Senhaji M. Reliability of the arabic smartphone addiction scale and smartphone addiction scale-short version in two different moroccan samples. Cyberpsychol Behav Soc Netw. (2018) 21:325–32. doi: 10.1089/cyber.2017.0411
31. Elm E, von Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. (2007) 335:806–8. doi: 10.1136/bmj.39335.541782.AD
32. Kwon M, Lee J-Y, Won W-Y, Park J-W, Min J-A, Hahn C, et al. Development and validation of a smartphone addiction scale (SAS). PLoS ONE. (2013) 8:e56936. doi: 10.1371/journal.pone.0056936
33. The Hashemite Kingdom of Jordan. The National Council for Family Affairs 2017 Survey Results. Jordan: Amman (2018).
34. WHO. World Health Organization [Internet] (2020). Available online at: https://www.who.int/
35. WHO. World Health Organization [Internet]. (2020). Available online at: http://gamapserver.who.int/gho/interactive_charts/tobacco/use/atlas.html
36. Zulkefly SN, Baharudin R. Mobile phone use amongst students in a university in Malaysia: Its correlates and relationship to psychological health. Eur J Sci Res. (2009) 37:206–18.
37. Brown K, Campbell SW, Ling R. Mobile phones bridging the digital divide for teens in the US? Futur Internet. (2011) 3:144–58. doi: 10.3390/fi3020144
38. Ahn J. Digital divides and social network sites: which students participate in social media? J Educ Comput Res. (2011) 45:147–63. doi: 10.2190/EC.45.2.b
39. Albursan IS Al Qudah MF Dutton E Hassan EMAH Bakhiet SFA Alfnan AA . National, sex and academic discipline difference in smartphone addiction: a study of students in jordan, saudi arabia, yemen and sudan. Community Ment Health J. (2019) 55:825–30. doi: 10.1007/s10597-019-00368-x
40. Matar Boumosleh J, Jaalouk D. Depression, anxiety, and smartphone addiction in university students- a cross sectional study. (2017) PLoS ONE. 12:e0182239. doi: 10.1371/journal.pone.0182239
41. Saadeh H, Saadeh M, Almobaideen W, Al Refaei A, Shewaikani N, Al Fayez RQ, et al. Effect of COVID-19 quarantine on the sleep quality and the depressive symptom levels of university students in Jordan during the spring of 2020. Front Psychiatry. (2021) 12:605676. doi: 10.3389/fpsyt.2021.605676
42. Kawasaki N, Tanei S, Ogata F, Burapadaja S, Loetkham C, Nakamura T, et al. Survey on cellular phone usage on students in Thailand. J Physiol Anthropol. (2006) 25:377–82. doi: 10.2114/jpa2.25.377
43. Billieux J, Van Der Linden M, Rochat L. The role of impulsivity in actual and problematic use of the mobile phone. Appl Cogn Psychol. (2008) 22:1195–210. doi: 10.1002/acp.1429
44. Sánchez-Martínez M, Otero A. Factors associated with cell phone use in adolescents in the community of Madrid (Spain). Cyberpsychol Behav. (2009) 12:131–7. doi: 10.1089/cpb.2008.0164
45. Leung L. Linking psychological attributes to addiction and improper use of the mobile phone among adolescents in hong kong. J Child Media. (2008) 2:93–113. doi: 10.1080/17482790802078565
46. Long J, Liu TQ, Liao YH, Qi C, He HY, Chen SB, et al. Prevalence and correlates of problematic smartphone use in a large random sample of Chinese undergraduates. BMC Psychiatry. (2016) 16:408. doi: 10.1186/s12888-016-1083-3
47. Al-Barashdi H, Bouazza A, Jabur N. Smartphone addiction among university undergraduates: a literature review. J Sci Res Reports. (2015) 4:210–25. doi: 10.9734/JSRR/2015/12245
48. Abu-Jedy A. Mobile phone addiction and its relationship with self-discloser among sample of students from University Of Jordan And Amman Al-Ahliyya University. Jordan J Educ Sci. (2008) 4:137–50.
49. Kubey RW, Lavin MJ, Barrows JR. Internet use and collegiate academic performance decrements: early findings. J Commun. (2001) 51:366–82. doi: 10.1111/j.1460-2466.2001.tb02885.x
50. Rodrigues A. The perceived impacts of smartphone use on the performance of senior managers in South African firms (Unpublished Master's thesis). University of Cape Town, Cape Town, South Africa (2011).
51. Pierce TA, Vaca R. Distracted: academic performance differences between teen users and non-users of MySpace and other communication technology. J Syst Cybern Inform. (2008) 6:67–71.
Keywords: COVID-19, Jordan, quarantine, short version addiction scale, smartphone addiction, university students
Citation: Saadeh H, Al Fayez RQ, Al Refaei A, Shewaikani N, Khawaldah H, Abu-Shanab S and Al-Hussaini M (2021) Smartphone Use Among University Students During COVID-19 Quarantine: An Ethical Trigger. Front. Public Health 9:600134. doi: 10.3389/fpubh.2021.600134
Received: 28 August 2020; Accepted: 30 June 2021;
Published: 26 July 2021.
Edited by:
Morteza Arab-Zozani, Birjand University of Medical Sciences, IranReviewed by:
Jian-ye Zhang, Guangzhou Medical University, ChinaDomenico Criscuolo, Italian Society of Pharmaceutical Medicine, Italy
Copyright © 2021 Saadeh, Al Fayez, Al Refaei, Shewaikani, Khawaldah, Abu-Shanab and Al-Hussaini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Heba Saadeh, aGViYS5zYWFkZWhAanUuZWR1Lmpv