 Yee Jin Shin1
Yee Jin Shin1 Sun Mi Kim
Sun Mi Kim Ji Sun Hong
Ji Sun Hong Doug Hyun Han
Doug Hyun Han
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 28 April 2021
Sec. Public Mental Health
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.586389
This article is part of the Research Topic Violence and the Young: A Public Health Problem - Etiology, Epidemiology, Intervention, and Prevention View all 6 articles
Introduction: Complex post-traumatic stress disorder (C-PTSD) is characterized by the typical symptoms of PTSD, in addition to affective dysregulation, negative self-concept, and disturbances in interpersonal relationships. Children and adolescents with C-PTSD have been reported to have deficits in emotional and cognitive functions. We hypothesized that the following are associated with the severity of C-PTSD symptoms: (1) adolescents with C-PTSD who show deficits in emotional perception and cognitive functions, including executive function and attention; and (2) deficits in neurocognitive functions.
Methods: Information on 69 adolescents with PTSD, aged 10–19 years, was gathered from seven shelters. All participants were assessed using complete clinical scales, including the C-PTSD Interview and Depression, Anxiety, and Stress Scales, and neurocognitive function tests, including the emotional perception, mental rotation, and modified Tower of London tests.
Results: Adolescents with C-PTSD were more likely to have a history of sexual assault, dissociation, and self-harm than those with PTSD. The total and subscale scores of the C-PTSD Interview Scale in adolescents with C-PTSD were higher than that in adolescents with PTSD. In addition, neurocognitive functions, including emotional perception, attention, and working memory, were correlated with the severity of C-PTSD symptoms.
Discussion: Adolescents with C-PTSD experienced more serious clinical symptoms and showed more deficits in neurocognitive functions than adolescents with PTSD. Clinicians should pay careful attention toward the emotional and neurocognitive functions when assessing and treating patients with C-PTSD.
Complex post-traumatic stress disorder (C-PTSD) was first detailed in 2018, in the International Classification of Diseases, 11th edition. Herman initially reported C-PTSD as a condition with specific deficits in interpersonal relationships, somatization, affective regulation, dissociation, and sense of self (1). The International Statistical Classification of Diseases and Related Health Problems states that C-PTSD consists of PTSD symptoms as well as affective dysregulation, negative self-concept, and disturbances in interpersonal relationships (2).
Developmental trauma can be defined as a type of stressful event that occurs repeatedly and cumulatively over a period of time within specific relationships and contexts (3). Childhood abuse and neglect, including those with sexual, emotional, and physical components, may constitute stressful events (4). These traumatic and stressful events could be associated with several psychiatric diseases, including PTSD (5), borderline personality disorder (6), somatization disorder (7), dissociation disorders (8), self-mutilation (9), and eating disorders (10). Among the different trauma-related psychiatric diseases, C-PTSD is strongly associated with chronic and accumulated trauma from childhood (2, 11), and shows greater functional impairment (12) and poorer prognosis than PTSD (13). C-PTSD is associated with multiple types of childhood developmental and interpersonal trauma (3, 11, 12).
Several large studies support the differentiation of PTSD from C-PTSD (2, 12, 14, 15). Cloitre et al. (12) classified the treatment-seeking United State (US) population with interpersonal and single-incidence traumas into three groups: PTSD, C-PTSD, and low-symptom. In 2014, Cloitre et al. (2) also classified American female participants with a history of childhood abuse into four groups: low-symptoms, PTSD, C-PTSD, and participants with borderline personality. Elklit et al. (14), in a Danish study, classified participants (bereaved parents, rape victims, and victims of physical assault) into three groups: PTSD, C-PTSD, and low-symptoms. Perkonigg et al. (15) classified adolescent and young adult community patients in Germany into four groups: PTSD, C-PTSD, disturbance in self-organization and low PTSD, and low-symptoms.
Several studies have suggested that specific symptoms, such as affective dysregulation, negative self-concept, and disturbance in interpersonal relationships, may be associated with emotional and cognitive dysfunction in patients with C-PTSD (16–19). Adolescents with C-PTSD have a higher prevalence of depressive and anxiety disorders, such as panic disorder and general anxiety disorder (19). Relative to a depressive mood, anxiety is common in both PTSD and C-PTSD (18). In 1346 adults of East Asian origin, aged 18–24 years, Ho et al. (17) reported that anxiety was associated with both C-PTSD and PTSD, but affective dysregulation was significantly associated only with C-PTSD. By merging the findings of the aforementioned studies, it can be concluded that affective dysregulation could be a symptom that differentiates C-PTSD from PTSD.
Individuals with negative personal experiences report worse psychological well-being and difficulty in autobiographical memory coherence (20). In this context, working memory capacity could affect the concept of self by mediating the association of mood with memory coherence (21). In a systematic review evaluating the cognitive functions of children after natural disasters and/or terrorist attacks, Pfefferbaum et al. (22) reported that experiencing such events in childhood could negatively affect attention, concentration, memory, academic achievement, and executive function. Furthermore, Rivera-Velez et al. (23) reported memory and executive function deficits in 12 women with a history of childhood sexual abuse. Social skill training has been shown to improve social interactions of children with attention problems (24). In this aspect, assessment of working memory and attention could predict the progress and status of patients with C-PTSD.
Based on the clinical characteristics of dysfunction in affective regulation, negative self-concept, and difficulty with interpersonal relationships in patients with C-PTSD, we hypothesized the following: (1) adolescents with C-PTSD have deficits in emotional perception and cognitive functions, including executive function and attention; and (2) deficits in neurocognitive functions are associated with the severity of C-PTSD symptoms.
From 2017 to 2019, the Korean Association against Violence and Abuse, a corporation under the Secretariat of the National Assembly, sent letters to 10 state shelters that host adolescents with a history of parental abuse to offer art therapy for adolescents with C-PTSD. The criteria for participation in the program were as follows: (1) 13–24 years of age, (2) voluntary participation, and (3) PTSD diagnosis (non-complex or complex). Seven shelters accepted to participate. Among the 127 adolescents at these seven shelters, 102 (80.3%) agreed to participate in the program and 25 refused. Before providing art therapy, diagnosis and neurocognitive intervention was provided. Two psychiatrists (Y.J. Shin and J.S. Hong) interviewed all adolescents to assess and diagnose them; 73/102 (71.6%) participants were diagnosed with a form of PTSD by both psychiatrists.
Of the 73 participants with PTSD, 43 had symptoms that checked more than four of the seven C-PTSD-I domains (25); 39 were diagnosed with C-PTSD by both psychiatrists, and four by only one psychiatrist, who were subsequently excluded from the analysis. Eventually, a total of 39 adolescents with C-PTSD and 30 adolescents with PTSD were recruited for the current analyses.
The art therapy program consisted of 16 sessions, described as follows: sessions 1–2: introduction to art therapy and rapport; session 3–6: affecting recognition and regulation, setting goals, and making emotion books using line, color, and face; sessions 7–8: cognition reconstruction; sessions 9–10: interpersonal relationships; sessions 11–13: making a new self-image and wish tree using gypsum; and closing programs: drawing a person in the rain.
After four diagnostic training sessions, the diagnostic concordance rate between the two doctors was 0.80. To differentiate co-occurring psychiatric diseases, the Korean version of the Mini International Neuropsychiatric Interview was used (26). In addition, a psychologist estimated the cognitive and emotional status of all adolescents. We extracted the psychological and emotional assessment results from these data. The ethics committee of Yeonsei University approved this study (IRB number: 4-2019-0156). Written informed consent was provided by participants aged 16 years or older or by the legal guardians of participants aged below 16 years.
The symptoms of C-PTSD were assessed using the Korean version of the C-PTSD Interview Scale (C-PTSD-I) (25, 27). It consists of 37 items, including the following seven domains: regulation of affect and impulse, alterations in attention or consciousness, alteration in self-conception, alteration in perception of the perpetrator, alteration in relationships with others, somatization, and alteration in meaning system. The internal consistency of the C-PTSD-I Korean version was 0.971 (Cronbach's alpha).
The Depression, Anxiety, and Stress Scale (DASS) was developed to measure changes in the emotional state of patients with PTSD (28, 29). The original version of the DASS consists of 42 items, but a short version—the DASS-21—was developed for screening PTSD symptoms at different levels of depression, anxiety, and stress (28, 29). Higher DASS-21 scores reflect higher levels of depression, anxiety, and stress. The correlation between the DASS-21 scores, Beck Depression Inventory, and Beck Anxiety Inventory was 0.79–0.85.
Neurocognitive functions in all adolescents were estimated using the modified Tower of London test, the emotional perception test, and the mental rotation test (CNT-MBI®, Seoul, South Korea). These tests have been used for assessing cognitive and emotional perceptions in professional gamers and pro-baseball players (30).
The emotional perception test consists of 108 questions regarding whether the same or different faces are presented. In each question, 2–8 faces (pleasant, unpleasant, and neutral faces) are presented on the screen in each trial. The subject then pushes the “same” or “different” button in response to the presented faces. During the test, the mean accuracy rate and reaction time from the presentation of the pictures to the pushing of the buttons were recorded. It has a test–retest reliability of 0.81 (Figure 1). Faster reaction times and more correct responses in the emotional perception test represent better emotional perception (31).
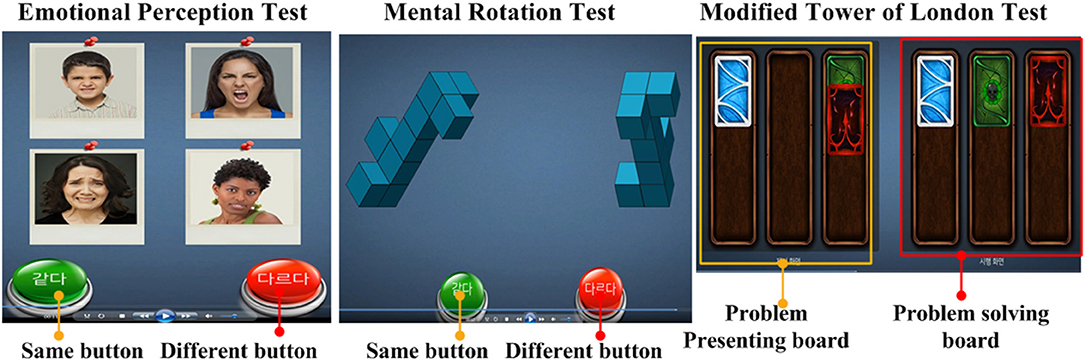
Figure 1. Neurocognitive function test. The images were obtained from the neurocognitive function test manufacturer MBI® (https://www.mbi-clinic.center/).
In the mental rotation test, a pair of three-dimensional (3D) objects is shown on a screen; these objects are rotated along a certain axis by 0, 60, 90, 120, or 180°. In some presentations, the shape of the two objects are the same but rotated, while in some trials, the shapes are different. The subjects are asked to judge whether the two 3D objects are the same. During the test, the mean accuracy rate and reaction time from the presentation of the pictures to a response was recorded. It has a test–retest reliability of 0.79 (Figure 1). Faster reaction times and more correct responses in the mental rotation test represent better spatiotemporal visual attention (32).
In the modified Tower of London test, there are two boards with three lines and cards of different colors. Classically, the Tower of London test was invented to assess working memory for planning (33). The modified Tower of London test shows two boards (problem-presenting board and problem-solving board) on a screen with three lines and several cards of different colors. Using the cards on the boards, the computer presents a problem-solving task to the subject. The subject moves the cards on the problem-solving board to match the order of the cards shown on the problem-presenting board. During the test, the number of cards moved and the time taken to solve the problem were recorded. It has a test–retest reliability of 0.82 (Figure 1). Faster reaction times and a lower number of moves are associated with better working memory (33, 34).
Normality of the data distribution was confirmed with the Shapiro–Wilk-test. Differences in demographic characteristics, history of trauma, and comorbid diseases between the C-PTSD and PTSD groups were analyzed using the independent samples t-test and chi-square-test. Statistical significance was set at p < 0.05. Differences between the two groups in the C-PTSD-I and DASS scores were analyzed using an independent samples t-test. The statistical significance for the total C-PTSD-I score was set at p < 0.05, but significance for subscale scores of C-PTSD-I was set at p < 0.007 (0.05/7). The statistical significance of the DASS score was set at p < 0.017 (0.05/3). Differences in the results of neurocognitive function tests, including the emotional perception test, modified Tower of London test, and mental rotation test, were analyzed using independent samples t-test. To assess the effects of biological sex on C-PTSD, differences in C-PTSD-I scores, DASS scores, and neurocognitive function tests, an analysis was performed using the analysis of covariance and regression (ANCOVA) test, controlling for biological sex. The statistical significance for the neurocognitive function tests was set at p < 0.017 (0.05/3).
Correlations between C-PTSD-I scores and neurocognitive function test results were assessed using partial correlations, controlling for age and years of education. Statistical significance was set at p < 0.017 (0.05/3).
All data, including age, education years, C-PTSD-I Korean subscale scores (including affect and impulse, attention or consciousness, self-perception, perception of perpetrator, relations with others, somatization, and meaning), DASS subscale scores (including depression, anxiety and stress, emotional perception test–reaction time, emotional perception test–accuracy rate, mental rotation–reaction time, and mental rotation–accuracy rate), Tower of London test–reaction time, and Tower of London test–card numbers were slightly skewed and kurtotic for both C-PTSD and PTSD groups. All data was found to be normally distributed for analyses.
Among the 69 adolescents with a history of childhood abuse, 39 (56.5%) were diagnosed with C-PTSD. Compared to the PTSD group, the C-PTSD group showed higher rates of a history of sexual assault (36.7 vs. 71.8%), dissociation (6.7 vs. 28.2%), and self-harm (3.3 vs. 30.8%) (Table 1). The duration of sexual assault in the C-PTSD group was longer than that in the PTSD group (6.64 ± 3.75 years vs. 2.72 ± 1.27 years; Table 1). There were no significant differences in age, sex ratio, or years of education between the C-PTSD and PTSD groups.
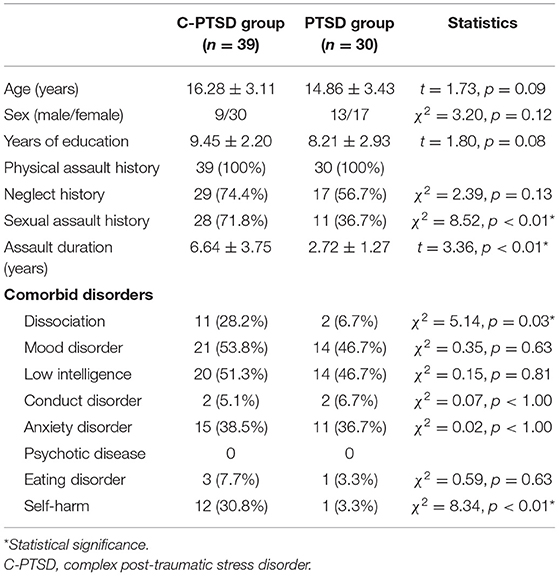
Table 1. Comparison of demographic characteristics and clinical scales between the C-PTSD and PTSD groups.
Adolescents in the C-PTSD group had higher total scores (35.82 ± 26.90 vs. 18.50 ± 17.42) and exhibited significant differences in affect and impulse (9.43 ± 7.07 vs. 4.64 ± 4.57), attention or consciousness (7.43 ± 5.81 vs. 3.33 ± 2.85), self-perception (9.28 ± 7.27 vs. 3.63 ± 5.95), relationships with others (6.51 ± 5.81 vs. 2.83 ± 2.71), and meaning system (2.10 ± 2.08 vs. 0.63 ± 1.21) on the C-PTSD-I than those in the PTSD group (Table 2). Adolescents in the C-PTSD group had higher DASS scores for depression (7.86 ± 6.07 vs. 4.08 ± 4.75) and stress (8.41 ± 5.57 vs. 4.96 ± 4.86) than those in the PTSD group (Table 2). In the ANCOVA test controlling for biological sex, the results of complex PTSD-I scores and DASS scores were the same as those observed in the independent t-test.
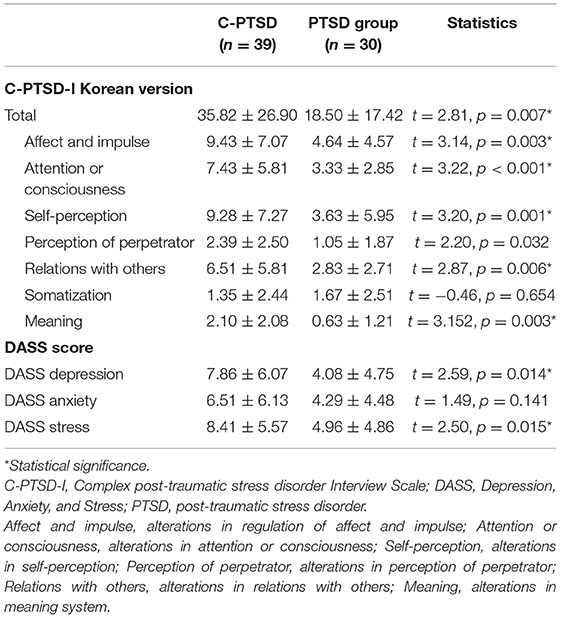
Table 2. Comparison of complex PTSD-I and DASS scores between the complex and non-complex PTSD groups.
Adolescents in the C-PTSD group had a lower accuracy rate in the emotional perception test (0.66 ± 0.15 vs. 0.74 ± 0.11) and the mental rotation test (0.64 ± 0.15 vs. 0.74 ± 0.15) and a higher number of moved cards in the modified Tower of London test (9.16 ± 2.07 vs. 7.81 ± 2.19) than those in the PTSD group (Table 3).

Table 3. Comparison of neurocognitive functions between the complex and non-complex PTSD groups.
In the ANCOVA test controlling for sex, the results of the neurocognitive function tests were the same as those observed in the independent t-test.
The total C-PTSD-I scores of all the participants (C-PTSD and PTSD groups) correlated negatively with the accuracy rate in the emotional perception test (r = −0.414, p = 0.001) and mental rotation test (r = −0.468, p < 0.001), but correlated positively with the number of moved cards in the modified Tower of London test (r = 0.631, p < 0.001; Figure 2).
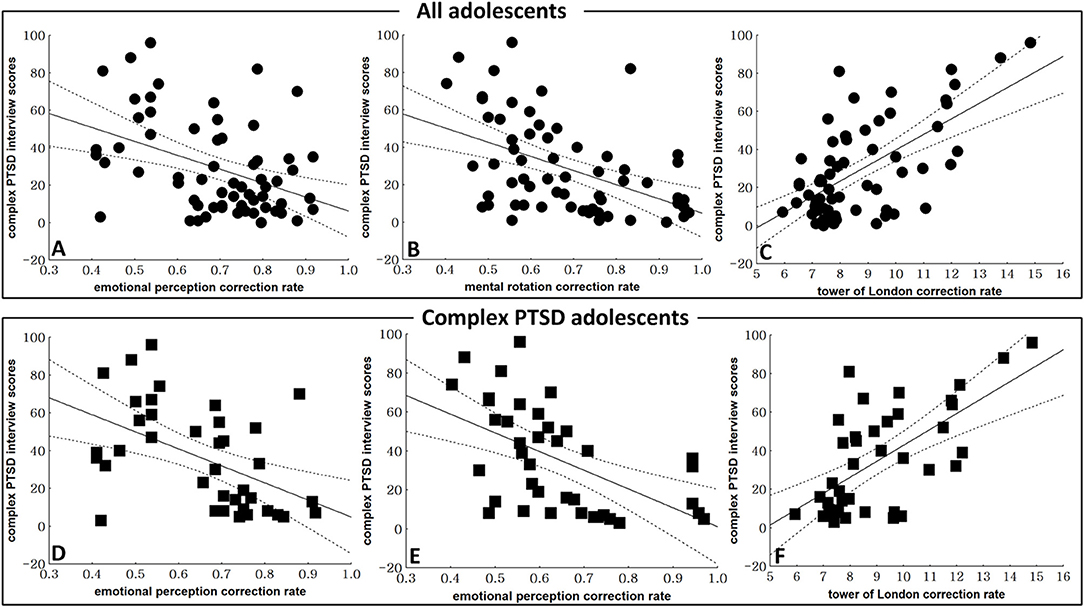
Figure 2. Correlations between C-PTSD symptoms and neurocognitive function test results. (A) The correlation between total complex post-traumatic stress disorder (C-PTSD) Interview Scale scores and the accuracy rate in the emotional test (r = −0.414, p = 0.001) in all adolescents (C-PTSD and PTSD groups). (B) The correlation between the total C-PTSD Interview Scale and the accuracy rate in the mental rotation test (r = −0.468, p < 0.001) in all adolescents. (C) The correlation between the total C-PTSD Interview Scale and the number of moved cards in the modified Tower of London test (r = 0.631, p < 0.001) in all adolescents. (D) The correlation between the total C-PTSD Interview Scale scores and the accuracy rate in the emotional test (r = −0.497, p = 0.001) in the C-PTSD group. (E) The correlation between total C-PTSD Interview Scale scores and the accuracy rate in the mental rotation test (r = −0.542, p < 0.001) in the C-PTSD group. (F) The correlation between the total C-PTSD Interview Scale scores and the number of moved cards in the modified Tower of London test (r = 0.636, p < 0.001) in the C-PTSD group.
In the C-PTSD group, the total C-PTSD-I scores correlated negatively with the accuracy rate in the emotional perception test (r = −0.497, p = 0.001) and the mental rotation test (r = −0.542, p < 0.001), and positively with the number of moved cards in the modified Tower of London test (r = 0.636, p < 0.001; Figure 2). In the PTSD group, there were no significant correlations between the total C-PTSD-I scores and the neurocognitive function test results.
The results of this study show that adolescents with C-PTSD have a higher rate of a history of sexual assault, dissociation, and self-harm than those with PTSD. The total and subscale scores of the C-PTSD-I, including affect and impulse, attention, self-perception, perception of perpetrator, relationship with others, and meaning in adolescents with C-PTSD, were higher than those in adolescents with PTSD. In addition, neurocognitive functions, including emotional perception, attention, and working memory, correlated with the severity of C-PTSD symptoms.
In this study, adolescents with C-PTSD had a higher rate of history of sexual assault, dissociation, and self-harm than those with PTSD. As a core symptom of C-PTSD, affective dysregulation can differentiate C-PTSD from PTSD. Among the different trauma stressors, sexual assault is thought to be the most likely cause of psychopathology and emotional dysregulation in patients with PTSD (4, 5). Hyland et al. (35) reported that patients with C-PTSD have higher levels of dissociative experiences than those with PTSD and healthy individuals. Classically, a history of childhood sexual and physical assault is thought to be a predictive factor for self-destructive behaviors in adults (9). Villalta et al. (36) reported that self-organization disturbance in adolescents with C-PTSD is strongly associated with sexual assault.
In the current study, adolescents with C-PTSD had higher total C-PTSD-I scores as well as differences in the affect and impulse, attention or consciousness, self-perception, relationship with others, and meaning system subscales than those with PTSD. In addition, adolescents in the C-PTSD group had higher DASS depression and DASS stress scores than those in the PTSD group. As the definition of C-PTSD includes affective dysregulation, negative self-concept, and disturbances in relationships (2), the functional deficits due to clinical symptoms were represented in the total and five subscale scores of C-PTSD-I in our sample. In a study on North Korean defectors with a history of trauma, Kim (37) reported the symptoms of C-PTSD using the total and seven subscale scores of the C-PTSD-I. Interestingly, there were no significant differences in the DASS anxiety scores between C-PTSD and PTSD in the current study. Prominent affective dysregulation and the similarity in anxiety scores between C-PTSD and PTSD were consistent with the findings of previous studies (17, 18).
In ANCOVA analysis controlling for biological sex, the results of C-PTSD-I scores, DASS scores, and neurocognitive functions were the same as those observed in the independent t-test. Other study has not reported the effects of biological sex on C-PTSD (11). However, the respective numbers of participants in those studies were small. Future studies should consider the biological sex effects on C-PTSD using a balanced number of male and female participants in a larger cohort.
The results of neurocognitive functional assessments showed that the emotional perception, mental rotation, and Tower of London tests in the C-PTSD group were worse than those in the PTSD group. In addition, all neurocognitive functions correlated with the severity of C-PTSD symptoms. Emotional dysregulation and deficits in emotional perception are well-known C-PTSD symptoms (16, 19). The lower accuracy scores of the emotional perception test already represented the dysfunction of emotional perception in previous studies (38). Affective dysregulation assessed using the neurocognitive function test in C-PTSD would also be more prominent than that in PTSD.
Inattention and intrusive visual memory dysfunction are well-known symptoms of PTSD (34, 35). Intrusive visual memories are core PTSD symptoms (39). Inattention induced by intrusive visual memories is a key target for early intervention in patients with a history of trauma (40). However, inattention is also thought to be a crucial factor in interpersonal relationships. Difficulty in interpersonal relationships is another key factor in C-PTSD (19). In the current study, we found more deficits in spatiotemporal visual attention, which were assessed using the mental rotation test, in adolescents with C-PTSD than in those with PTSD.
PTSD symptoms, including re-experiencing the traumatic event, avoidance, and hyperarousal in maltreated youth, are associated with a deficit in working memory (41). In the current study, we found more deficits in working memory, which was assessed using the modified Tower of London test, in adolescents with C-PTSD than in those with PTSD. Working memory is thought to mediate the association between mood and negative self-concept (21). Working memory training is considered effective for emotional regulation in the treatment of patients with PTSD (42). Affective dysregulation and negative self-concept are the main symptoms of C-PTSD. For these reasons, the deficit of working memory in C-PTSD might be more serious than that observed in PTSD.
This study has a few limitations. First, the number of subjects was limited to confidently generalize the study results. Moreover, we could not link the effect of sexual assault on C-PTSD symptoms because of the small number of subjects. Second, the diagnosis of participant was established by psychiatrists only using clinical ratings, without psychometric diagnostic interview. Therefore, readers should be cautious with interpreting the results. Finally, the family environment of adolescents with C-PTSD could not be investigated in the current study. Future studies should consider the family environment and a large number of participants.
Because adolescents with C-PTSD showed more deficits in clinical symptoms and cognitive functions than those with PTSD, psychiatrists should pay careful attention toward neurocognitive function when assessing patients with C-PTSD. In addition, regulation of emotion and improving working memory could be crucial factors for treating C-PTSD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by The Ethics Committee of Yeonsei University. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
YS and DH: conceptualization. DH and SK: methodology. SK: formal analysis. JH: investigation. DH: writing—original draft preparation. YS: writing—review, editing, and supervision. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
This work was supported by the Korean Creative Content Agency (KOCCA-2017-2019).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Special thanks to the Korean Association against Violence and Abuse.
1. Herman JL. Complex PTSD: a syndrome in survivors of prolonged and repeated trauma. J Trauma Stress. (1992) 5:377–91. doi: 10.1002/jts.2490050305
2. Cloitre M, Garvert DW, Weiss B, Carlson EB, Bryant RA. Distinguishing PTSD, complex PTSD, and borderline personality disorder: a latent class analysis. Eur J Psychotraumatol. (2014) 5:25097. doi: 10.3402/ejpt.v5.25097
3. Courtois CA. Complex trauma, complex reactions: assessment and treatment. Psychother Theor Res Pract Train. (2004) 41:412–25. doi: 10.1037/0033-3204.41.4.412
4. Ozturk E, Sar V. Apparently normal family: a contemporary agent of transgenerational trauma and dissociation. J Trauma Pract. (2005) 4:287–303. doi: 10.1300/J189v04n03_06
5. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. (1995) 52:1048–60. doi: 10.1001/archpsyc.1995.03950240066012
6. Herman JL, Perry JC, van der Kolk BA. Childhood trauma in borderline personality disorder. Am J Psychiatry. (1989) 146:490–5. doi: 10.1176/ajp.146.4.490
7. Saxe GN, Chinman G, Berkowit R, Hall K, Lieberg G, Schwartz J, et al. Somatization in patients with dissociative disorders. Am J Psychiatry. (1994) 151:1329–34. doi: 10.1176/ajp.151.8.1251
8. Ross CA, Miller SD, Reagor P, Bjornson L, Fraser GA, Anderson G. Structured interview data on 102 cases of multiple personality disorder from four centers. Am J Psychiatry. (1990) 147:596–601. doi: 10.1176/ajp.147.5.596
9. van der Kolk BA, Perry JC, Herman JL. Childhood origins of self-destructive behavior. Am J Psychiatry. (1991) 148:1665–71. doi: 10.1176/ajp.148.12.1665
10. Herzog DB, Staley JE, Carmody S, Robbins WM, van der Kolk BA. Childhood sexual abuse in anorexia nervosa and bulimia nervosa: a pilot study. J Am Acad Child Adolesc Psychiatry. (1993) 32:962–6. doi: 10.1097/00004583-199309000-00011
11. Karatzias T, Shevlin M, Fyvie C, Hyland P, Efthymiadou E, Wilson D, et al. Evidence of distinct profiles of posttraumatic stress disorder (PTSD) and complex posttraumatic stress disorder (CPTSD) based on the new ICD-11 trauma questionnaire (ICD-TQ). J Affect Disord. (2017) 207:181–7. doi: 10.1016/j.jad.2016.09.032
12. Cloitre M, Garvert DW, Brewin CR, Bryant RA, Maercker A. Evidence for proposed ICD-11 PTSD and complex PTSD: a latent profile analysis. Eur J Psychotraumatol. (2013) 4:20706. doi: 10.3402/ejpt.v4i0.20706
13. Brewi CR, Cloitre M, Hyland P, Shevlin M, Maercker A, Bryant RA, et al. A review of current evidence regarding the ICD-11 proposals for diagnosing PTSD and complex PTSD. Clin Psychol Rev. (2017) 58:1–15. doi: 10.1016/j.cpr.2017.09.001
14. Elklit A, Hyland P, Shevlin M. Evidence of symptom profiles consistent with posttraumatic stress disorder and complex posttraumatic stress disorder in different trauma samples. Eur J Psychotraumatol. (2014) 5:24221. doi: 10.3402/ejpt.v5.24221
15. Perkonigg A, Hofler M, Cloitre M, Wittchen HU, Trautmann S, Maercker A. Evidence for two different ICD-11 posttraumatic stress disorders in a community sample of adolescents and young adults. Eur Arch Psychiatry Clin Neurosci. (2016) 266:317–28. doi: 10.1007/s00406-015-0639-4
16. Gilbar O, Hyland P, Cloitre M, Dekel R. ICD-11 complex PTSD among Israeli male perpetrators of intimate partner violence: construct validity and risk factors. J Anxiety Disord. (2018) 54:49–56. doi: 10.1016/j.janxdis.2018.01.004
17. Ho GWK, Hyland P, Shevlin M, Chien WT, Inoue S, Yang PJ, et al. The validity of ICD-11 PTSD and complex PTSD in East Asian cultures: findings with young adults from China, Hong Kong, Japan, and Taiwan. Eur J Psychotraumatol. (2020) 11:1717826. doi: 10.1080/20008198.2020.1717826
18. Hyland P, Shevlin M, McNally S, Murphy J, Hansen M, Elklit A. Exploring differences between the ICD-11 and DSM-5 models of PTSD: Does it matter which model is used? J Anxiety Disord. (2016) 37:48–53. doi: 10.1016/j.janxdis.2015.11.002
19. Rytwinski NK, Scur MD, Feeny NC, Youngstrom EA. The co-occurrence of major depressive disorder among individuals with posttraumatic stress disorder: a meta-analysis. J Trauma Stress. (2013) 26:299–309. doi: 10.1002/jts.21814
20. Vanderveren E, Bijttebier P, Hermans D. Autobiographical memory coherence and specificity: examining their reciprocal relation and their associations with internalizing symptoms and rumination. Behav Res Ther. (2019) 116:30–5. doi: 10.1016/j.brat.2019.02.003
21. Christopher G, MacDonald J. The impact of clinical depression on working memory. Cogn Neuropsychiatry. (2005) 10:379–99. doi: 10.1080/13546800444000128
22. Pfefferbaum B, Noffsinger MA, Jacobs AK, Varma V. Children's cognitive functioning in disasters and terrorism. Curr Psychiatry Rep. (2016) 18:48. doi: 10.1007/s11920-016-0685-2
23. Rivera-Velez GM, Gonzalez-Viruet M, Martinez-Taboas A, Perez-Mojica D. Post-traumatic stress disorder, dissociation, and neuropsychological performance in Latina victims of childhood sexual abuse. J Child Sex Abus. (2014) 23:55–73. doi: 10.1080/10538712.2014.864746
24. Fox A, Dishman S, Valicek M, Ratcliff K, Hilton C. Effectiveness of social skills interventions incorporating peer interactions for childrenwith attention deficit hyperactivity disorder: a systematic review. Am J Occup Ther. (2020) 74:7402180070-1. doi: 10.5014/ajot.2020.040212
25. Ouimette P, Saxe G, van der Kolk BA. The complex PTSD Interview. In: Measurement of Stress, Trauma, and Adaptation. Lutherville, MD: Sicran Press (1996).
26. Yoo SW, Kim YS, Noh JS, Oh KS, Kim CH, Nam K, et al. Validity of Korean version of the mini-international neuropsychiatric interview. Anxiety Mood. (2006) 1:50–5.
27. Lee JM, Hong CH. The complex post-traumatci stress disorder of prostituted women. Korean J Counsel Psychother. (2008) 20:553–80.
28. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther. (1995) 33:335–43. doi: 10.1016/0005-7967(94)00075-U
29. Lovibond SH, Lovibond PF. Manual for the depression anxiety stress scales (DASS). New South Wales: Psychology Foundation Monograph (1995).
30. Kang JO, Kang KD, Lee JW, Nam JJ, Han DH. Comparison of psychological and cognitive characteristics between professional internet game players and professional baseball players. Int J Environ Res Public Health. (2020) 17:4797. doi: 10.3390/ijerph17134797
31. Lewis GJ, Lefevre CE, Young AW. Functional architecture of visual emotion recognition ability: a latent variable approach. J Exp Psychol Gen. (2016) 145:589–602. doi: 10.1037/xge0000160
32. Habacha H, Lejeune-Poutrain L, Margas N, Molinaro C. Effects of the axis of rotation and primordially solicited limb of high level athletes in a mental rotation task. Hum Mov Sci. (2014) 37:58–68. doi: 10.1016/j.humov.2014.06.002
33. Kaller CP, Debelak R, Köstering L, Egle J, Rahm B, Wild PS, et al. Assessing planning ability across the adult life span: population-representative and age-adjusted reliability estimates for the Tower of London (TOL-F). Arch Clin Neuropsychol. (2016) 31:148–64. doi: 10.1093/arclin/acv088
34. Kostering L, Nitschke K, Schumacher FK, Weiller C, Kaller CP. Test-retest reliability of the Tower of London Planning Task (TOL-F). Psychol Assess. (2015) 27:925–31. doi: 10.1037/pas0000097
35. Hyland P, Shevlin M, Fyvie C, Cloitre M, Karatzias T. The relationship between ICD-11 PTSD, complex PTSD and dissociative experiences. J Trauma Dissociation. (2020) 21:62–72. doi: 10.1080/15299732.2019.1675113
36. Villalta L, Khadr S, Chua KC, Kramer T, Clarke V, Viner RM, et al. Complex post-traumatic stress symptoms in female adolescents: the role of emotion dysregulation in impairment and trauma exposure after an acute sexual assault. Eur J Psychotraumatol. (2020) 11:1710400. doi: 10.1080/20008198.2019.1710400
37. Kim HK. Differences in the symptoms of complex PTSD and PTSD in North Korean defectors by trauma type. Korean Soc Sci Rev. (2014) 4:65–92.
38. Bae S, Kang KD, Kim SW, Shin YJ, Nam JJ, Han DH. Investigation of an emotional perception test using functional magnetic resonance imaging. Comput Methods Programs Biomed. (2019) 179:104994. doi: 10.1016/j.cmpb.2019.104994
39. Rademaker AR, van Minnen A, Ebberink F, van Zuiden M, Hagenaars MA, Geuze E. Symptom structure of PTSD: support for a hierarchical model separating core PTSD symptoms from dysphoria. Eur J Psychotraumatol. (2012) 3:17580. doi: 10.3402/ejpt.v3i0.17580
40. Brewin CR. Episodic memory, perceptual memory, and their interaction: foundations for a theory of posttraumatic stress disorder. Psychol Bull. (2014) 140:69–97. doi: 10.1037/a0033722
41. Ross EH, Kearney CA. Posttraumatic symptoms among maltreated youth using classification and regression tree analysis. Child Abuse Negl. (2017) 69:177–87. doi: 10.1016/j.chiabu.2017.04.028
Keywords: complex post-traumatic stress disorder, adolescents, emotional perception, spatiotemporal attention, working memory
Citation: Shin YJ, Kim SM, Hong JS and Han DH (2021) Correlations Between Cognitive Functions and Clinical Symptoms in Adolescents With Complex Post-traumatic Stress Disorder. Front. Public Health 9:586389. doi: 10.3389/fpubh.2021.586389
Received: 23 July 2020; Accepted: 31 March 2021;
Published: 28 April 2021.
Edited by:
Elisabetta Miglietta, University of Verona, ItalyReviewed by:
Sebastian Trautmann, Medical School Hamburg, GermanyCopyright © 2021 Shin, Kim, Hong and Han. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Doug Hyun Han, aGR1azcwQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.