 Fabrizio Stasolla
Fabrizio Stasolla Marta Matamala-Gomez
Marta Matamala-Gomez Sara Bernini
Sara Bernini Alessandro O. Caffò
Alessandro O. Caffò Sara Bottiroli
Sara Bottiroli- 1“Giustino Fortunato” University of Benevento, Benevento, Italy
- 2Department of Human Sciences for Education “Riccardo Massa”, Center for Studies in Communication Sciences “Luigi Anolli” (CESCOM), University of Milano-Bicocca, Milan, Italy
- 3Scientific Institute for Research, Hospitalization, and Healthcare (IRCCS), Mondino Foundation, Pavia, Italy
- 4Department of Educational Sciences, Psychology and Communication, University of Bari, Bari, Italy
The COVID-19 poses an ongoing threat to lives around the world and challenges the existing public health and medical service delivery. The lockdown or quarantine measures adopted to prevent the spread of COVID-19 has caused the interruption in ongoing care and access to medical care including to patients with existing neurological conditions. Besides the passivity, isolation, and withdrawal, patients with neurodegenerative diseases experience difficulties in communication due to a limited access to leisure opportunities and interaction with friends and relatives. The communication difficulties may exacerbate the burden on the caregivers. Therefore, assistive-technologies may be a useful strategy in mitigating challenges associated with remote communication. The current paper presents an overview of the use of assistive technologies using virtual reality and virtual body ownership in providing communication opportunities to isolated patients, during COVID-19, with neurological diseases and moderate-to-severe communication difficulties. We postulate that the assistive technologies-based intervention may improve social interactions in patients with neurodegenerative diseases and acquired brain injury-thereby reducing isolation and improving their quality of life and mental well-being.
Introduction
Persons with neurodegenerative diseases and acquired brain injuries may fail while dealing with everyday life environmental requests. Their independence, social interactions, communication skills, and functional activities may be seriously hampered with deleterious effects on their quality of life (1–3). Isolation, passivity, and detachment may be observed with negative outcomes on caregivers and families' burden (4–6). Both intellectual and motor impairments may emerge with a significant reduction of an overall individual's functioning (7, 8). To be effective, a rehabilitative intervention should be implemented early regarding brain damage and should be intensive and assiduously prolonged over the time. Moreover, to be consolidated and generalized, the learning process should be pursued across settings (9, 10). Unfortunately, COVID-19 pandemic relevantly impeded the implementation and the realization of those conditions (11, 12). In fact, by December 24, 2020, over 72 million of cases have been documented worldwide, with almost 1.7 million of deaths (13, 14). Quarantine and social distancing interrupted public health services and regular medical care delivery (15). Public health preventions have centered around social-distancing, masks, and hand-washing strategies. Patients with chronic neurodegenerative diseases (e.g., Alzheimer, Parkinson, amyotrophic lateral sclerosis), demyelinating diseases as multiple sclerosis, and persons with acquired brain injuries (e.g., stroke, post-coma) have been impacted by lockdowns—making them vulnerable during the COVID-19 (16). In order to deal with these issues, one may envisage assistive technology (AT)-based strategies (17, 18).
AT options are broadly recognized as crucial means of support for individuals with neurodegenerative diseases and acquired brain injuries and multiple disabilities (19). Thus, AT-based programs are commonly planned to favorably fill the gap between behavioral/cognitive skills and environmental requests (20). That is, an AT setup is conceived to build functional bridges between users, environment, and technology. Essentially, it ensures that a helpful interaction (i.e., purposeful behavior and goal-oriented) is achieved for persons with extensive motor delays (21). That interaction is critical to enhancing personal fulfillment, social image, active role, satisfaction, and improving quality of life accordingly (22). Among different targeted areas, communication and leisure opportunities have been promoted (23–25). Scopus database emphasizes different empirical contributions which demonstrate the relevance and the beneficial effects on practical daily issues (e.g., communication, leisure, internet access) of technology-based programs in individuals with neurodegenerative diseases and acquired brain injuries (26–32).
At present, striking changes for public health and medical delivery services have been determined by COVID-19, including the need to find alternative solutions to take action against the substantial interruption of the regular medical care assistance and to social distance limitations forced by this pandemic (33–36). The main goal of this article is to propose a perspective on a new AT-based approach in using VR and virtual body ownership illusions to enable the communication of the patients with neurological diseases and severe-to-profound disabilities in case of isolation inside the hospital or in his/her home during this pandemic situation. In this context, current evidence-based recommendations on the use of AT-based strategies, including virtual reality (VR), as technological-aided solutions to support communication and leisure in neurological disorders, will be explored. Table 1 summarizes some relevant examples of AT-based and VR solutions for both targeted populations.
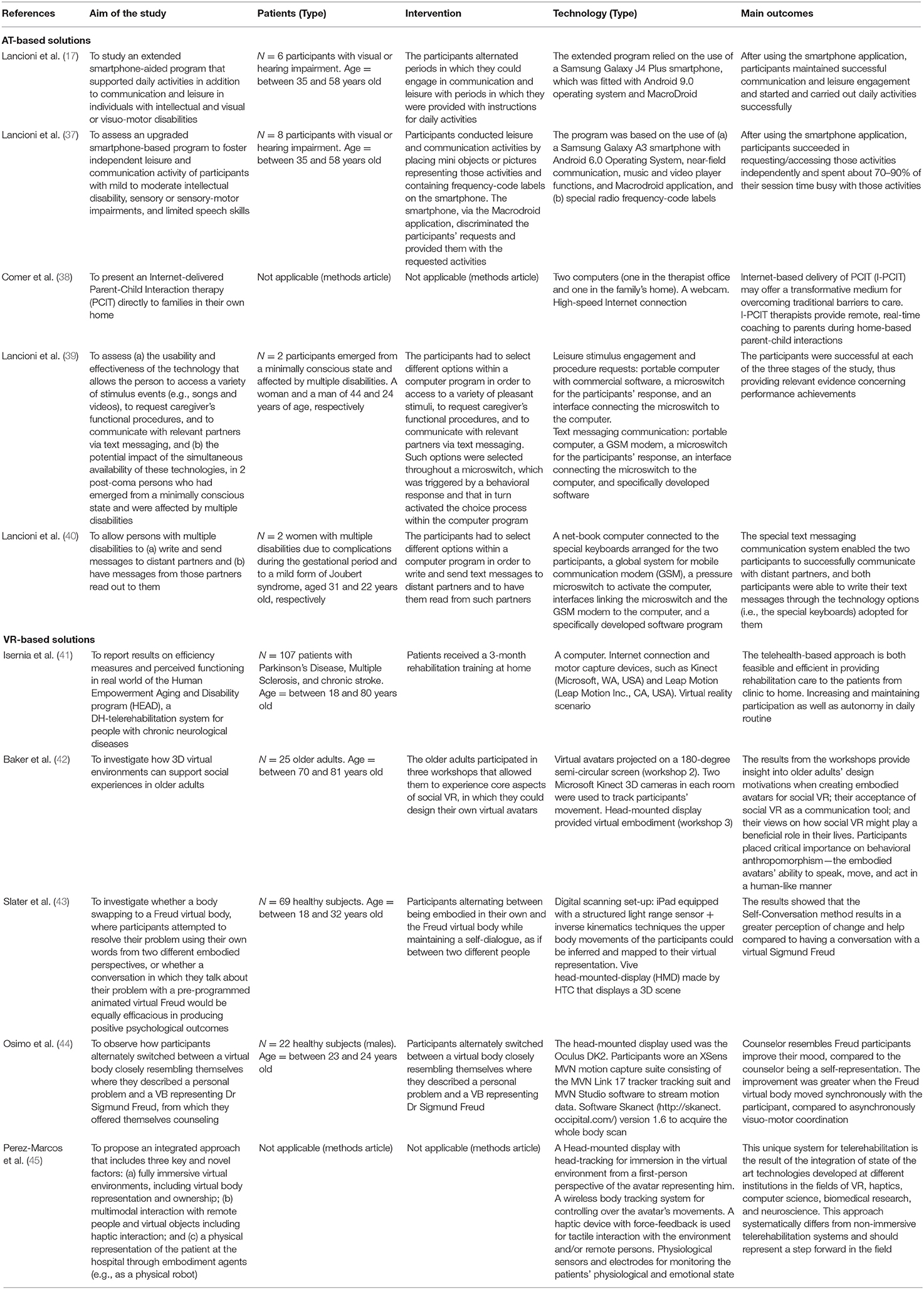
Table 1. Studies integrating AT-based and VR solutions to improve communication in individuals with neurodegenerative diseases and acquired brain injuries.
Communication and Leisure in Neurological Disorders
Failure to positively engage in communication and leisure activities includes the incapacity to handle social interactions independently and profitably. For instance, individuals with neurodegenerative diseases and acquired brain injuries and multiple disabilities may be unable to undertake and pursue leisure activities autonomously, that is, they remain dependent on both families and caregivers. Additionally, people with neurological impairments may be unable to adequately communicate their needs or favorably make requests and choose desired items. Moreover, people with neurological impairments may face difficulties in communicating with distant partners (37, 46, 47). Technological-aided setups may be viewed as helpful supports focused on filling the existing gap between the actual individual's skills and the skill level necessary to achieve functional objectives. Accordingly, AT-based devices, setups, and tools should be rigorously customized in terms of (a) personal skills and (b) meaningful goals to be useful (48). For instance, whenever the individual has extensive motor disorders and lack of speech but is estimated within a normal range of intellectual functioning (e.g., multiple sclerosis), one may design technological aids aimed at helping the patients perform different adaptive responses. Practically, with the AT-based intervention, persons with neurodegenerative diseases and acquired brain injuries and significant impairments may be helped (a) to make small adaptive responses available in their behavioral repertoire and (b) to use adaptive responses to achieve functional tasks and/or pursue meaningful purposes (49). Communication or leisure opportunities or their combination could be embedded in a rehabilitation program using AT (39, 40, 50). Moreover, communication with distant partners through short text messages, telephone calls, or video-calls may be implemented to promote social interactions (51, 52). For instance, (53) the newly developed high-sensitivity mechanical switch for augmentative and alternative communication access in people with amyotrophic lateral sclerosis, namely the Lever Magnetic-spring Mechanical Switch (i.e., LeMMS). Results of the validation study evidenced that all the participants were capable to operate the LeMMS, which could help these patients to communicate even in an advanced stage of the disease.
Internet-Based Communication in Neurological Disorders
Internet-based communication has revealed a useful transformative medium for overcoming traditional barriers to delivering healthcare services at patients' homes (38). Through internet-based communication services, it is possible to establish direct communication with the patients and their caregivers despite the distance. The increasing availability of internet access has already changed healthcare delivery and communication routines among patients, caregivers, and clinicians (54). Mental health difficulties are commonly documented across neurological disorders. Moreover, meta-analysis reported high anxiety and depression levels among individuals with multiple sclerosis, Parkinson's disease, and acquired brain injuries (55). Across neurological diseases, poor mental health is linked to poor quality of life, greater disability, poor prognosis and disease improvement, poor benefits after intervention (56). Accordingly, some studies have demonstrated that improving social communication in patients presenting neurodegenerative diseases and acquired brain injuries may improve their quality of life (57). Indeed, the relationship between verbal communication ability and quality of life has been shown. In detail, initial speech impairment in patients with neurodegenerative diseases and acquired brain injuries have a strong impact on their quality of life (58).
Internet connections are crucial to ensure people with timely social interactions, general public awareness, enhanced health conditions, specific knowledge on otherwise less-known neurological diseases, and health-related coping (59). Patients with neurological impairments can easily find numerous opportunities for peer social connections, learning, and leisure options (60). Furthermore, neurologists can easily manage user-generated data to satisfactory have an exhaustive representation of patients' needs and carry out epidemiological investigations (61). For example, a recent study (60) explored when and how technology could help interactions among patients with dementia and their caregivers. Three dyads patient-caregiver living in their homes were equipped with tablet computers and web-based applications and researchers analyzed their interactions. The study outlined benefits in terms of dyad interaction derived from the use of technology, suggesting the importance of an adequate provision of technology-based equipment for individuals with dementia.
Telerehabilitation (TR) offers a medium to deliver rehabilitation services and manage patients remotely using technology-based information and communication (61, 62). The adopted technologies may broadly include emails, data transmissions through videos and/or photos sent by the health provider or the user or both (63). Additionally, tablets and computers, internet-based media or programs, video conferencing, smartphones, and webinars are usually embedded (64). Typically, TR may be adopted as synchronous (i.e., the health provider and user are simultaneously connected) or as asynchronous (i.e., the health provider and user are not simultaneously connected but connected through stored data and virtual technologies or electronic communication) (41, 65). Currently, one of the newest technologies used to engage patients and caregivers in the TR training is VR systems (65, 66).
Telepresence and Virtual Reality
At the end of the last century, VR constitutes the evolution of the old communication interfaces such as telephone, computer, and television toward the emergence of the integration of different data coming from different modalities (67). According to this, Biocca and Levy (68) defined VR as a communication system instead of a piece of technology (69). Then, VR is a communication interface connecting: (1) physical media, (2) codes, (3) information, and (4) sensorimotor channels (69). A main characteristic of VR is that allows the full immersion of the human sensorimotor channels into a vivid and realistic communication experience (68). In fact, VR is a successor of internet-based communication (70). Essentially, VR represents a technology through which it is possible to simulate existing experiences into a fake immersive virtual environment (71). Immersion is related to the extent to which the VR systems can deliver an inclusive, extensive, surrounding, and vivid illusion of reality to the participant's sensory senses. Then, immersion corresponds to the objective and quantifiable description of what the technology can provide (72). For instance, some studies demonstrated the use of VR systems, such as wearable headsets and 3-D smart televisions, to provide enjoyable, leisurely activities, with benefits in terms of quality of life, psychological well-being, and facilitated social interactions in patients with cognitive impairment (73). One example is a VR intervention using a virtual environment displayed on two large screens with head-mounted 3-D glasses and body-tracking sensors to promote engagement in patients with Mild Cognitive Impairment (74).
Another main feature of the VR system is the capability to induce a sense of “presence” into the virtual environment, which corresponds to the psychological perception of being in the virtual environment (72, 75). However, as described by Schroeder in 1996: “The notion of communications technology normally implies two or more people are involved and the emphasis is placed on the messages that pass between them” (p. 146) (76). In this regard, VR allows the possibility to interact with the immersive virtual environment and different virtual characters or avatars (77). Through VR, it is also possible to induce the sense of co-presence, that is the sense of being together in a shared space, combining significant characteristics of being both physically and socially present (78). According to this, it has been argued that the validity of the telepresence depends on the capacity to produce a context in which social actors, or social avatars in the case of VR, may communicate and cooperate between them (79–81). In line with this definition of telepresence, a large number of investigations induced telepresence within a virtual environment by means of virtual body ownership illusions (82–84). In these experimental studies, the researchers induced the illusion, by using synchronous visuo-tactile stimulation of being in the embodied virtual body instead than in the real one, inducing the sense of telepresence among the participants (82–84). Due to the possibility of moving subjects from one place to another when using VR systems, telepresence results as a promising strategy to facilitate communication with patients and their relatives when they are at home (45).
New Communication Technologies: Virtual Reality as a Communication Tool in Clinical Populations
Based on the above-commented VR systems components, a recent study investigated how VR may contribute to older adult well-being by facilitating greater social VR participation (42, 85). In detail, in the study from Baker and colleagues, the authors conducted three workshops in which 25 older adults aged from 70 to 81 used VR as a medium for communicating with other participants (42). Older adults had to create embodied virtual avatars controlled through natural gestures and subsequently successfully and effectively used these avatars in two social VR prototypes from a third- or a first-person perspective. In this line, others used VR as a communication tool allowing medical staff to virtually interact with a virtual avatar assistant to assess and treat a virtual avatar victim presenting clinical complications (86). Additionally, virtual medical interaction with the patients through virtual avatars and telepresence has also been proposed (45, 87–89). In detail, Perez-Marcos and colleagues presented an innovative VR set-up that allows remote interaction and rehabilitation, including both the patient and doctor body projection into virtual bodies in a fully immersive environment and the physical embodiment at the remote place (45).
According to these promising studies, here we propose a VR intervention to foster and facilitate social interactions with both the clinicians and relatives with virtual avatars and telepresence in patients with neurological disorders. Such an intervention could be used when patients are isolated due to their clinical condition or to the social distance limitations forced by the COVID-19 pandemic situation. The proposed intervention aims to improve the patient's well-being avoiding his/her isolation. Specifically, it is a new VR social intervention by means of full-body ownership illusions observed from a first-person perspective and delivered through a head-mounted display and the activation of a social VR application. The effectiveness of the VR social application for enhancing social interactions through virtual avatars has been previously shown in healthy individuals (90). The intervention aims to reproduce the patients' and their relatives' body representation within the same VR environment, that is a virtual living room. In this regard, the virtual avatars' anthropomorphism characteristics are important to further enhance the sense of ownership and increase the sense of presence in interaction with other virtual avatars (42, 43, 91). This intervention is composed of five different phases: (1) the creation of the virtual avatars by scanning patients' and relatives' real bodies as in the study conducted by Osimo and co-authors or in the study by Orts-Escolano and colleagues (44, 92); (2) the integration of such virtual avatars into the VR social application; (3) delivery and teaching to use the VR social application and the head-mounted display; (4) the creation of daily social VR appointments to meet and interact with the patient's relatives during isolation or hospitalization period; and (5) the creation of weekly social VR appointments between relatives and medical staff for an updating about patient's medical condition.
The proposed intervention may represent a solution to the current worldwide situation caused by the COVID-19 pandemic, which requires suitable and effective technology-based approaches. Many recommendations are indeed proliferating about the need of alternative strategies for delivering health care services in this contingency (33, 34, 93). If some months ago the focus was mainly on the treatment of COVID-19 patients (94–99), now a days we are assisting in a growing interest for alternative ways to support the process of care of non-COVID conditions, including patients with neurodegenerative diseases and acquired brain injuries (100–102). For instance, there are many evidences about the use of telemedicine—understood as an interface in a virtual patient-clinician relationship to provide primary and secondary care (62, 99–102)—and virtual reality for remote delivery of cognitive rehabilitation in various settings of neurological care (103–105). In this frame, we propose a VR-based intervention aimed to support another critical aspect of individual's functioning that is communication, in persons with neurodegenerative diseases and acquired brain injury during COVID-19 pandemic. Thus, by using an AT-implemented strategy such as VR interventions, patients with neurodegenerative diseases may be enabled to communicate his/her needs, feelings, and thoughts to their relatives or medical staff during the hospitalization or isolation period. Accordingly, it may be fostered with positive outcomes on his/her health conditions, with a meaningful reduction of the anxiety and/or depression levels, and with beneficial effects in terms of quality of life (106, 107). Therefore, the caregivers, families, and health care systems may find a significant burden reduction (108, 109). In conclusion, through this VR intervention for communication, the patients may (a) communicate their needs, (b) independently access leisure options (e.g., positive stimulation, favorite videos, amusing songs), and (c) be connected with distant relatives. Then, patients will be more engaged in communication, and with a purposeful behavior (110, 111). In this regard, the use of new technologies for fostering engagement in patients with neurodegenerative disorders has been demonstrated (65, 112, 113).
Concluding Remarks
The level of independence, social interactions, communication skills, and functional activities may be seriously hampered in patients with neurodegenerative diseases with deleterious effects on their quality of life (1–3). The isolation because of the COVID-19 pandemic situation may enhance such negative aspects with consequences on their quality of life (30, 114). To avoid that, some studies propose VR as a technologically-aided solution for clinical populations (99, 107, 115). However, most of these studies are focused on using VR to continue with the treatments and rehabilitation routines of the patients in case of isolation or social distancing. Depending on their level of functioning, persons with neurodegenerative diseases may be exposed to different aided-technological solutions to enhance communication skills. For example, individuals with extensive motor disabilities and moderate-to-severe intellectual disabilities may be involved in social interactions through vocal output communication aid (VOCA) or speech generating devices (SGD). Else, one may envisage hierarchical computerized systems with adapted software enabling patients with neurodegenerative diseases to request and choice desired items and/or communicate their needs. Otherwise, for individuals estimated with an intellectual normal functioning and extensive motor impairments, the independent access to the literacy through computerized systems and keyboard emulators may be proposed. Moreover, during lockdown or quarantine imposed due to an infectious disease outbreak, one may consider the communication with a distant partner through technology-aided options including a smartphone and a global system for mobile communications (GSM) system (116, 117). Here we proposed a VR-AT solution to enable the communication among patients with neurodegenerative diseases or acquired brain injury, relatives, and medical staff during the COVID-19 pandemic situation. We hypothesized that this intervention may improve the patient's social interactions enhancing their quality of life and mental well-being, avoiding isolation and negative psychological and cognitive effects.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
FS, MM-G, and SBo have conceived the work. All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Funding
This project is funded by the Current Research Fund of the Italian Ministry of Health to the National Neurological Institute C. Mondino Foundation (Ricerca Corrente 2020).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Heinrichs RW. The duality of human cognition: operations and intentionality in mental life and illness. Neurosci Biobehav Rev. (2020) 108:139–48. doi: 10.1016/j.neubiorev.2019.11.002
2. Zhu Y, Gao H, Tong L, Li ZL, Wang L, Zhang C, et al. Emotion regulation of hippocampus using real-time fMRI neurofeedback in healthy human. Front Hum Neurosci. (2019) 13:242. doi: 10.3389/fnhum.2019.00242
3. Kinney KL, Burkhouse KL, Klumpp H. Self-report and neurophysiological indicators of emotion processing and regulation in social anxiety disorder. Biol Psychol. (2019) 142:126–31. doi: 10.1016/j.biopsycho.2019.01.019
4. Rousseau MC, Baumstarck K, Valkov M, Felce A, Brisse C, Khaldi-Cherif S, et al. Impact of severe polyhandicap cared for at home on French informal caregivers' burden: a cross-sectional study. BMJ Open. (2020) 10:e032257. doi: 10.1136/bmjopen-2019-032257
5. Fleisher JE, Klostermann EC, Hess SP, Lee J, Myrick E, Chodosh J. Interdisciplinary palliative care for people with advanced Parkinson's disease: a view from the home. Ann Cardiothorac Surg. (2020) 9:S80–9. doi: 10.21037/apm.2019.09.12
6. Spencer L, Potterton R, Allen K, Musiat P, Schmidt U. Internet-based interventions for carers of individuals with psychiatric disorders, neurological disorders, or brain injuries: systematic review. J Med Internet Res. (2019) 21:e10876. doi: 10.2196/10876
7. Allen J, Molloy E, McDonald D. Severe neurological impairment: a review of the definition. Dev Med Child Neurol. (2020) 62:277–82. doi: 10.1111/dmcn.14294
8. Gardizi E, MacKillop E, Gaind G. Self-injurious behavior in a patient with dementia: a case report and literature review. J Nerv Ment Dis. (2019) 207:6–11. doi: 10.1097/NMD.0000000000000924
9. Zimmern V. Why brain criticality is clinically relevant: a scoping review. Front Neural Circ. (2020) 14:54. doi: 10.3389/fncir.2020.00054
10. Stevenson R, Samokhina E, Rossetti I, Morley JW, Buskila Y. Neuromodulation of glial function during neurodegeneration. Front Cell Neurosci. (2020) 14:278. doi: 10.3389/fncel.2020.00278
11. Szcześniak D, Gładka A, Misiak B, Cyran A, Rymaszewska J. The SARS-CoV-2 and mental health: from biological mechanisms to social consequences. Prog Neuro Psychopharmacol Biol Psychiatry. (2020) 104:110046. doi: 10.1016/j.pnpbp.2020.110046
12. Wilson BA, Betteridge S, Fish J. Neuropsychological consequences of Covid-19. Neuropsychol Rehabil. (2020) 30:1625–8. doi: 10.1080/09602011.2020.1808483
13. Hadi AG, Kadhom M, Hairunisa N, Yousif E, Mohammed SA. A review on COVID-19: origin, spread, symptoms, treatment, and prevention. Biointerface Res Appl Chem. (2020) 10:7234–42. doi: 10.33263/BRIAC106.72347242
14. Director-General W. WHO Remarks at the Media Briefing on 2019-nCoV on 11 February 2020. Geneva: World Heal Orgnatization (2020).
15. Bhaskar S, Rastogi A, Chattu VK, Adisesh A, Thomas P, Alvarado N, et al. Key strategies for clinical management and improvement of healthcare services for cardiovascular disease and diabetes patients in the coronavirus (COVID-19) settings: recommendations from the REPROGRAM consortium. Front Cardiovasc Med. (2020) 7:112. doi: 10.3389/fcvm.2020.00112
16. Bhaskar S, Rastogi A, Menon KV, Kunheri B, Balakrishnan S, Howick J. Call for action to address equity and justice divide during COVID-19. Front Psychiatry. (2020) 11:1411. doi: 10.3389/fpsyt.2020.559905
17. Lancioni GE, Singh NN, O'Reilly MF, Sigafoos J, D'Amico F, Buonocunto F, et al. Mainstream technology to support basic communication and leisure in people with neurological disorders, motor impairment and lack of speech. Brain Inj. (2020) 34:921–7. doi: 10.1080/02699052.2020.1763462
18. Chandrakala S. Machine learning based assistive speech technology for people with neurological disorders. In: Costin H, Schuller B, Florea A, editors. Recent Advances in Intelligent Assistive Technologies: Paradigms and Applications. Cham, New York, NY: Springer (2020). p. 143–63. doi: 10.1007/978-3-030-30817-9_6
19. Mishra R, Banerjea AC. Neurological damage by coronaviruses: a catastrophe in the queue! Front Immunol. (2020) 11:2204. doi: 10.3389/fimmu.2020.565521
20. Bertelli MO, Rossi M, Varrucciu N, Bianco A, Scuticchio D, Del Furia C, et al. Relationship between psychiatric disorders and adaptive functioning in adults with intellectual disabilities. Adv Ment Heal Intellect Disabil. (2016) 10:92–101. doi: 10.1108/AMHID-08-2015-0038
21. Papais Alvarenga RM, de Araújo e Araújo ACR, Nascimento ACB, de Araujo NEC, Meneguette NS, Neri VC, et al. Is Asian type MS an MS phenotype, an NMO spectrum disorder, or a MOG-IgG related disease? Mult Scler Relat Disord. (2020) 42:102082. doi: 10.1016/j.msard.2020.102082
22. Troncoso-Escudero P, Sepulveda D, Pérez-Arancibia R, Parra AV, Arcos J, Grunenwald F, et al. On the right track to treat movement disorders: promising therapeutic approaches for Parkinson's and Huntington's disease. Front Aging Neurosci. (2020) 12:284. doi: 10.3389/fnagi.2020.571185
23. Caldwell DJ, Ojemann JG, Rao RPN. Direct electrical stimulation in electrocorticographic brain-computer interfaces: enabling technologies for input to cortex. Front Neurosci. (2019) 13:804. doi: 10.3389/fnins.2019.00804
24. Mayo CD, Miksche K, Attwell-Pope K, Gawryluk JR. The relationship between physical activity and symptoms of fatigue, mood, and perceived cognitive impairment in adults with multiple sclerosis. J Clin Exp Neuropsychol. (2019) 41:715–22. doi: 10.1080/13803395.2019.1614535
25. Dekhtyar S, Marseglia A, Xu W, Darin-Mattsson A, Wang HX, Fratiglioni L. Genetic risk of dementia mitigated by cognitive reserve: a cohort study. Ann Neurol. (2019) 86:68–78. doi: 10.1002/ana.25501
26. Koumakis L, Chatzaki C, Kazantzaki E, Maniadi E, Tsiknakis M. Dementia care frameworks and assistive technologies for their implementation: a review. IEEE Rev Biomed Eng. (2019) 12:4–18. doi: 10.1109/RBME.2019.2892614
27. Stamford JA, Schmidt PN, Friedl KE. What engineering technology could do for quality of life in Parkinson's disease: a review of current needs and opportunities. IEEE J Biomed Heal Informat. (2015) 19:1862–72. doi: 10.1109/JBHI.2015.2464354
28. Jamieson M, Cullen B, McGee-Lennon M, Brewster S, Evans JJ. The efficacy of cognitive prosthetic technology for people with memory impairments: a systematic review and meta-analysis. Neuropsychol Rehabil. (2014) 24:419–44. doi: 10.1080/09602011.2013.825632
29. Brandt Å, Jensen MP, Søberg MS, Andersen SD, Sund T. Information and communication technology-based assistive technology to compensate for impaired cognition in everyday life: a systematic review. Disabil Rehabil Assist Technol. (2020) 15:810–24. doi: 10.1080/17483107.2020.1765032
30. Clasby B, Hughes N, Catroppa C, Morrison E. Community-based interventions for adolescents following traumatic brain injury: a systematic review. NeuroRehabilitation. (2018) 42:345–63. doi: 10.3233/NRE-172385
31. Charters E, Gillett L, Simpson GK. Efficacy of electronic portable assistive devices for people with acquired brain injury: a systematic review. Neuropsychol Rehabil. (2015) 25:82–121. doi: 10.1080/09602011.2014.942672
32. Des Roches CA, Kiran S. Technology-based rehabilitation to improve communication after acquired brain injury. Front Neurosci. (2017) 11:382. doi: 10.3389/fnins.2017.00382
33. Bhaskar S, Bradley S, Israeli-Korn S, Menon B, Chattu VK, Thomas P, et al. Chronic neurology in COVID-19 era: clinical considerations and recommendations from the REPROGRAM Consortium. Front Neurol. (2020) 11:664. doi: 10.3389/fneur.2020.00664
34. Bloem BR, Dorsey ER, Okun MS. The coronavirus disease 2019 crisis as catalyst for telemedicine for chronic neurological disorders. JAMA Neurol. (2020) 77:927–8. doi: 10.1001/jamaneurol.2020.1452
35. Chen PM, Hemmen TM. Evolving healthcare delivery in neurology during the coronavirus disease 2019 (COVID-19) pandemic. Front Neurol. (2020) 11:578. doi: 10.3389/fneur.2020.00578
36. Platz T, Sandrini G. Specialty grand challenge for neurorehabilitation research. Front Neurol. (2020) 11:349. doi: 10.3389/fneur.2020.00349
37. Lancioni GE, Singh NN, O'Reilly MF, Sigafoos J, Alberti G, Perilli V, et al. An upgraded smartphone-based program for leisure and communication of people with intellectual and other disabilities. Front Public Health. (2018) 6:234. doi: 10.3389/fpubh.2018.00234
38. Comer JS, Furr JM, Cooper-Vince C, Madigan RJ, Chow C, Chan PT, et al. Rationale and considerations for the internet-based delivery of parent–child interaction therapy. Cogn Behav Pract. (2015) 22:302–16. doi: 10.1016/j.cbpra.2014.07.003
39. Lancioni GE, O'Reilly MF, Singh NN, Sigafoos J, Buonocunto F, Sacco V, et al. Technology-aided leisure and communication opportunities for two post-coma persons emerged from a minimally conscious state and affected by multiple disabilities. Res Dev Disabil. (2013) 34:809–16. doi: 10.1016/j.ridd.2012.10.008
40. Lancioni GE, O'Reilly MF, Singh NN, Sigafoos J, Green VA, Oliva D, et al. Two women with multiple disabilities communicate with distant partners via a special text messaging system. Res Dev Disabil. (2013) 34:397–403. doi: 10.1016/j.ridd.2012.08.024
41. Isernia S, Pagliari C, Jonsdottir J, Castiglioni C, Gindri P, Gramigna C, et al. Efficiency and patient-reported outcome measures from clinic to home: the human empowerment aging and disability program for digital-health rehabilitation. Front Neurol. (2019) 10:1206. doi: 10.3389/fneur.2019.01206
42. Baker S, Kelly RM, Waycott J, Carrasco R, Hoang T, Batchelor F, et al. Interrogating social virtual reality as a communication medium for older adults. Proc ACM Hum Comput Interact. (2019) 3:1–24. doi: 10.1145/3359251
43. Slater M, Neyret S, Johnston T, Iruretagoyena G, de la Campa Crespo MÁ, Alabèrnia-Segura M, et al. An experimental study of a virtual reality counselling paradigm using embodied self-dialogue. Sci Rep. (2019) 9:10903 doi: 10.1038/s41598-019-46877-3
44. Osimo SA, Pizarro R, Spanlang B, Slater M. Conversations between self and self as Sigmund Freud—A virtual body ownership paradigm for self counselling. Sci Rep. (2015) 5:13899. doi: 10.1038/srep13899
45. Perez-Marcos D, Solazzi M, Steptoe W, Oyekoya O, Frisoli A, Weyrich T, et al. A fully immersive set-up for remote interaction and neurorehabilitation based on virtual body ownership. Front Neurol. (2012) 3:110. doi: 10.3389/fneur.2012.00110
46. Lancioni GE, Singh NN, O'Reilly MF, Sigafoos J, Alberti G, Chiariello V, et al. Extended smartphone-aided program to sustain daily activities, communication and leisure in individuals with intellectual and sensory-motor disabilities. Res Dev Disabil. (2020) 105:103722. doi: 10.1016/j.ridd.2020.103722
47. Lancioni GE, Singh NN, O'Reilly MF, Sigafoos J, Alberti G, Perilli V, et al. A tablet-based program to enable people with intellectual and other disabilities to access leisure activities and video calls. Disabil Rehabil Assist Technol. (2020) 15:14–20. doi: 10.1080/17483107.2018.1508515
48. Lancioni GE, Singh NN, O'Reilly MF, Sigafoos J, Boccasini A, Perilli V, et al. Persons with multiple disabilities manage positive leisure and communication engagement through a technology-aided program. Int J Dev Disabil. (2017) 63:148–57. doi: 10.1080/20473869.2016.1187462
49. Lancioni GE, Singh NN, O'Reilly MF, Sigafoos J, Alberti G, Perilli V, et al. Technology-aided options for helping persons with multiple disabilities engage in communication behavior. Life Span Disabil. (2017) 20:7–26.
50. Lancioni GE, O'Reilly MF, Singh NN, Sigafoos J, Buonocunto F, Sacco V, et al. Communication opportunities via special messaging technology for two post-coma persons with multiple disabilities. Res Dev Disabil. (2011) 32:1703–8. doi: 10.1016/j.ridd.2011.02.025
51. Lancioni G, O'Reilly M, Singh N, Buonocunto F, Sacco V, Colonna F, et al. Technology-assisted messaging opportunities for two persons emerged from a minimally conscious state and showing extensive motor disabilities. Dev Neurorehabil. (2011) 14:8–14. doi: 10.3109/17518423.2010.519760
52. Orsini A, Corsi M, Santangelo A, Riva A, Peroni D, Foiadelli T, et al. Challenges and management of neurological and psychiatric manifestations in SARS-CoV-2 (COVID-19) patients. Neurol Sci. (2020) 41:2353–66. doi: 10.1007/s10072-020-04544-w
53. Caligari M, Godi M, Giardini M, Colombo R. Development of a new high sensitivity mechanical switch for augmentative and alternative communication access in people with amyotrophic lateral sclerosis. J Neuroeng Rehabil. (2019) 16:1–3. doi: 10.1186/s12984-019-0626-5
54. Field MJ, Grigsby J. Telemedicine and remote patient monitoring. J Am Med Assoc. (2002) 288:423–5. doi: 10.1001/jama.288.4.423
55. Hampson N, King L, Eriksson LM, Smee H. The effects of relaxation training on depression and anxiety in people living with long-term neurological conditions. Disabil Rehabil. (2020) 42:2100–5. doi: 10.1080/09638288.2018.1554009
56. Amanzio M, Bartoli M, Cipriani GE, Palermo S. Executive dysfunction and reduced self-awareness in patients with neurological disorders. A mini-review. Front Psychol. (2020) 11:1697. doi: 10.3389/fpsyg.2020.01697
57. Szemere E, Jokeit H. Quality of life is social-towards an improvement of social abilities in patients with epilepsy. Seizure. (2015) 26:12–21. doi: 10.1016/j.seizure.2014.12.008
58. Felgoise SH, Zaccheo V, Duff J, Simmons Z. Verbal communication impacts quality of life in patients with amyotrophic lateral sclerosis. Amyotroph Lateral Scler Front Degener. (2016) 17:179–83. doi: 10.3109/21678421.2015.1125499
59. Reverté-Villarroya S, Dávalos A, Font-Mayolas S, Berenguer-Poblet M, Sauras-Colón E, López-Pablo C, et al. Coping strategies, quality of life, and neurological outcome in patients treated with mechanical thrombectomy after an acute ischemic stroke. Int J Environ Res Public Health. (2020) 17:6014. doi: 10.3390/ijerph17176014
60. Oleen-Burkey MK, Castelli-Haley J, Lage MJ, Johnson KP. Burden of a multiple sclerosis relapse: the patients perspective. Patient. (2012) 5:57–69. doi: 10.2165/11592160-000000000-00000
61. Ellul MA, Benjamin L, Singh B, Lant S, Michael BD, Easton A, et al. Neurological associations of COVID-19. Lancet Neurol. (2020) 19:767–83. doi: 10.1016/S1474-4422(20)30221-0
62. Srivastav AK, Samuel AJ. E-rehabilitation: one solution for patients with Parkinson's disease in COVID-19 era. Parkinsonism Relat Disord. (2020) 75:128–9. doi: 10.1016/j.parkreldis.2020.05.021
63. Bhaskar S, Bradley S, Chattu VK, Adisesh A, Nurtazina A, Kyrykbayeva S, et al. Telemedicine as the new outpatient clinic gone digital: position paper from the pandemic health system REsilience PROGRAM (REPROGRAM) international consortium (part 2). Front Public Health. (2020) 8:410. doi: 10.3389/fpubh.2020.00410
64. Hosseiniravandi M, Kahlaee AH, Karim H, Ghamkhar L, Safdari R. Home-based telerehabilitation software systems for remote supervising: a systematic review. Int J Technol Assess Health Care. (2020) 36:113–25. doi: 10.1017/S0266462320000021
65. Matamala-Gomez M, Maisto M, Montana JI, Mavrodiev PA, Baglio F, Rossetto F, et al. The role of engagement in teleneurorehabilitation: a systematic review. Front Neurol. (2020) 11:354. doi: 10.3389/fneur.2020.00354
66. Matamala-Gomez M, De Icco R, Avenali M, Balsamo F. Multisensory integration techniques in neurorehabilitation: the use of virtual reality as a rehabilitation tool. Confin Cephalalgica. (2018) 28:81–5.
68. Biocca F, Delaney B. Immersive virtual reality technology. Commun Age virtual Real. (1995) 15:1–68.
69. Biocca F, Levy M, editors. Virtual reality as a communication system. In: Communication in the Age of Virtual Reality. New York, NY: Routledge (1995). p. 416.
70. Riva G. Virtual reality as communication tool: a sociocognitive analysis. Presence Teleoper Virtual Environ. (1999) 8:462–8. doi: 10.1162/105474699566341
71. Brooks FP. What's real about virtual reality? IEEE Comput Graph Appl. (1999) 19:16–27. doi: 10.1109/38.799723
72. Slater M, Wilbur S. A framework for immersive virtual environments (FIVE): speculations on the role of presence in virtual environments. Presence Teleoper Virtual Environ. (1997) 6:603–16. doi: 10.1162/pres.1997.6.6.603
73. D'Cunha NM, Nguyen D, Naumovski N, McKune AJ, Kellett J, Georgousopoulou EN, et al. A mini-review of virtual reality-based interventions to promote well-being for people living with dementia and mild cognitive impairment. Gerontology. (2019) 65:430–40. doi: 10.1159/000500040
74. Bourrelier J, Ryard J, Dion M, Merienne F, Manckoundia P, Mourey F. Use of a virtual environment to engage motor and postural abilities in elderly subjects with and without mild cognitive impairment (MAAMI Project). Irbm. (2016) 37:75–80. doi: 10.1016/j.irbm.2016.02.007
75. Riva G, Mantovani F. Being there: understanding the feeling of presence in a synthetic environment and its potential for clinical change. In: Eichenberg C, editor. Virtual Reality in Psychological, Medical and Pedagogical Applications. London: Intechopen (2012). p. 3–34. doi: 10.5772/46411
76. Schroeder R. Possible Worlds: The Social Dynamic of Virtual Reality Technology. Boulden: Westview Press, Inc (1996).
77. Bhaskar S, Bradley S, Sakhamuri S, Moguilner S, Chattu VK, Pandya S, et al. Designing futuristic telemedicine using artificial intelligence and robotics in the COVID-19 era. Front Public Health. (2020) 8:708. doi: 10.3389/fpubh.2020.556789
78. Riva G, Davide F, IJsselsteijn WA (editors). Being there: the experience of presence in mediated environments. In: Being There: Concepts, Effects and Measurement of User Presence in Synthetic Environments. Amsterdam: IOS Press (2003). p. 5.
79. Mantovani G, Riva G. “Real” presence: how different ontologies generate different criteria for presence, telepresence, and virtual presence. Presence Teleoper Virtual Environ. (1999) 8:540–50. doi: 10.1162/105474699566459
80. Riva G. Design of clinically oriented virtual environments: a communicational approach. Cyberpsychol Behav. (2000) 3:351–7. doi: 10.1089/10949310050078797
81. Riva G. Virtual reality and telepresence. Science. (2007) 318:1240–2. doi: 10.1126/science.318.5854.1240d
82. Lenggenhager B, Tadi T, Metzinger T, Blanke O. Video ergo sum: manipulating bodily self-consciousness. Science. (2007) 317:1096–9. doi: 10.1126/science.1143439
83. Petkova VI, Ehrsson HH. If i were you: perceptual illusion of body swapping. PLoS ONE. (2008) 3:e3832. doi: 10.1371/journal.pone.0003832
84. Slater M, Perez-Marcos D, Ehrsson HH, Sanchez-Vives M V. Inducing illusory ownership of a virtual body. Front Neurosci. (2009) 3:29. doi: 10.3389/neuro.01.029.2009
85. Tuena C, Pedroli E, Trimarchi PD, Gallucci A, Chiappini M, Goulene K, et al. Usability issues of clinical and research applications of virtual reality in older people: a systematic review. Front Hum Neurosci. (2020) 14:93. doi: 10.3389/fnhum.2020.00093
86. Badler NI, Erignac CA, Liu Y. Virtual humans for validating maintenance procedures. Commun ACM. (2002) 45:56–63. doi: 10.1145/514236.514264
87. Matamala-Gomez M, Malighetti C, Cipresso P, Pedroli E, Realdon O, Mantovani F, et al. Changing body representation through full body ownership illusions might foster motor rehabilitation outcome in patients with stroke. Front Psychol. (2020) 11:1962. doi: 10.3389/fpsyg.2020.01962
88. Matamala Gómez M. The Use of Immersive Virtual Reality in Neurorehabilitation and its Impact in Neuroplasticity. (Doctoral dissertation), Barcelona: Universitat de Barcelona (2017).
89. Matamala-Gomez M, Donegan T, Bottiroli S, Sandrini G, Sanchez-Vives MV., Tassorelli C. Immersive virtual reality and virtual embodiment for pain relief. Front Hum Neurosci. (2019) 13:279. doi: 10.3389/fnhum.2019.00279
90. Moustafa F. Social VR-an Investigation into the Affective Triggers of Virtual Reality. UCL Interaction Center, University College London, HCI-E MSc Final Project Report (2017).
91. Lugrin JL, Latt J, Latoschik ME. Avatar anthropomorphism and illusion of body ownership in VR. In: 2015 IEEE Virtual Reality (VR). Arles: IEEE (2015). p. 229–30. doi: 10.1109/VR.2015.7223379
92. Orts-Escolano S, Rhemann C, Fanello S, Chang W, Kowdle A, Degtyarev Y, et al. Holoportation: virtual 3d teleportation in real-time. In: Proceedings of the 29th Annual Symposium on User Interface Software and Technology. New York, NY (2016). p. 741–54. doi: 10.1145/2984511.2984517
93. Scuteri D, Matamala-Gomez M, Bottiroli S, Corasaniti MT, De Icco R, Bagetta G, et al. Pain assessment and treatment in dementia at the time of coronavirus disease covid-19. Front Neurol. (2020) 11:890. doi: 10.3389/fneur.2020.00890
94. Salawu A, Green A, Crooks MG, Brixey N, Ross DH, Sivan M. A proposal for multidisciplinary tele-rehabilitation in the assessment and rehabilitation of COVID-19 survivors. Int J Environ Res Public Health. (2020) 17:4890. doi: 10.3390/ijerph17134890
95. Simpson R, Robinson L. Rehabilitation after critical illness in people with COVID-19 infection. Am J Phys Med Rehabil. (2020) 99:470–4. doi: 10.1097/PHM.0000000000001480
96. Lopez M, Bell K, Annaswamy T, Juengst S, Ifejika N. COVID-19 guide for the rehabilitation clinician: a review of nonpulmonary manifestations and complications. Am J Phys Med Rehabil. (2020) 99:669–76. doi: 10.1097/PHM.0000000000001479
97. Curci C, Pisano F, Bonacci E, Camozzi DM, Ceravolo C, Bergonzi R, et al. Early rehabilitation in post-acute COVID-19 patients: data from an Italian COVID-19 rehabilitation unit and proposal of a treatment protocol. Eur J Phys Rehabil Med. (2020) 56:633–41. doi: 10.23736/S1973-9087.20.06339-X
98. Sivan M, Halpin S, Hollingworth L, Snook N, Hickman K, Clifton IJ. Development of an integrated rehabilitation pathway for individuals recovering from COVID-19 in the community. J Rehabil Med. (2020) 52:jrm00089. doi: 10.2340/16501977-2727
99. Matamala-Gomez M, De Icco R, Sandrini G. Telemedicina e realtà virtuale ai tempi della pandemia da Covid-19. Confinia Cephalalg Neurol. (2020) 30:79–83.
100. Negrini S, Kiekens C, Bernetti A, Capecci M, Ceravolo MG, Lavezzi S, et al. Telemedicine from research to practice during the pandemic “instant paper from the field” on rehabilitation answers to the COVID-19 emergency. Eur J Phys Rehabil Med. (2020) 56:327–30. doi: 10.23736/S1973-9087.20.06331-5
101. Leocani L, Diserens K, Moccia M, Caltagirone C, Neurorehabilitation scientific panel of the european academy of neurology-EAN. Disability through COVID-19 pandemic: neurorehabilitation cannot wait. Eur J Neurol. (2020) 27:e50–1. doi: 10.1111/ene.14320
102. De Biase S, Cook L, Skelton DA, Witham M, Ten Hove R. The COVID-19 rehabilitation pandemic. Age Ageing. (2020) 49:696–700. doi: 10.1093/ageing/afaa118
103. Chirra M, Marsili L, Wattley L, Sokol LL, Keeling E, Maule S, et al. Telemedicine in neurological disorders: opportunities and challenges. Telemed e-Health. (2019) 25:541–50. doi: 10.1089/tmj.2018.0101
104. Montana JI, Gomez MM, Maisto M, Mavrodiev PA, Cavalera CM, Diana B, et al. The benefits of emotion regulation interventions in virtual reality for the improvement of wellbeing in adults and older adults: a systematic review. J Clin Med. (2020) 9:500. doi: 10.3390/jcm9020500
105. Tuena C, Semonella M, Fernández-Álvarez J, Colombo D, Cipresso P. Predictive precision medicine: towards the computational challenge. In: Pravettoni G, Triberti S, editors. P5 eHealth: An Agenda for the Health Technologies of the Future. Cham: Springer (2020). p. 71–86. doi: 10.1007/978-3-030-27994-3_5
106. Soares WB, Silvestre IT, Lima AM de O, de Almondes KM. The influence of telemedicine care on the management of behavioral and psychological symptoms in dementia (BPSD) risk factors induced or exacerbated during the COVID-19 pandemic. Front Psychiatry. (2020) 11:965. doi: 10.3389/fpsyt.2020.577629
107. Mantovani E, Zucchella C, Bottiroli S, Federico A, Giugno R, Sandrini G, et al. Telemedicine and virtual reality for cognitive rehabilitation: a roadmap for the COVID-19 pandemic. Front Neurol. (2020) 11:926. doi: 10.3389/fneur.2020.00926
108. Maggio MG, De Luca R, Manuli A, Calabrò RS. The five ‘W’ of cognitive telerehabilitation in the Covid-19 era. Expert Rev Med Devices. (2020) 17:473–5. doi: 10.1080/17434440.2020.1776607
109. Rajavenkatanarayanan A, Kanal V, Tsiakas K, Calderon D, Papakostas M, Abujelala M, et al. A survey of assistive technologies for assessment and rehabilitation of motor impairments in multiple sclerosis. Multimodal Technol Interact. (2019) 3:6. doi: 10.3390/mti3010006
110. Connors K, Mahony L, Morgan P. Variation in assistive technology use in motor neuron disease according to clinical phenotypes and ALS functional rating scale-revised score: a prospective observational study. NeuroRehabilitation. (2019) 44:303–13. doi: 10.3233/NRE-182511
111. Stasolla F, Damiani R, Perilli V, D'Amico F, Caffò AO, Stella A, et al. Computer and microswitch-based programs to improve academic activities by six children with cerebral palsy. Res Dev Disabil. (2015) 45–6:1–13. doi: 10.1016/j.ridd.2015.07.005
112. Pinto S, Quintarelli S, Silani V. New technologies and amyotrophic lateral sclerosis–which step forward rushed by the COVID-19 pandemic? J Neurol Sci. (2020) 418:117081. doi: 10.1016/j.jns.2020.117081
113. Fried-Oken M, Mooney A, Peters B. Supporting communication for patients with neurodegenerative disease. NeuroRehabilitation. (2015) 37:69–87. doi: 10.3233/NRE-151241
114. Stasolla F, Caffò AO, Perilli V, Boccasini A, Damiani R, D'Amico F. Assistive technology for promoting adaptive skills of children with cerebral palsy: ten cases evaluation. Disabil Rehabil Assist Technol. (2019) 14:489–502. doi: 10.1080/17483107.2018.1467972
115. Di Carlo F, Sociali A, Picutti E, Pettorruso M, Vellante F, Verrastro V, et al. Telepsychiatry and other cutting-edge technologies in COVID-19 pandemic: bridging the distance in mental health assistance. Int J Clin Pract. (2020) 75:e13716. doi: 10.1111/ijcp.13716
116. Bernini S, Panzarasa S, Barbieri M, Sinforiani E, Quaglini S, Tassorelli C, et al. A double-blind randomized controlled trial of the efficacy of cognitive training delivered using two different methods in mild cognitive impairment in Parkinson's disease: preliminary report of benefits associated with the use of a computerized tool. Aging Clin Exp Res. (2020) 8:1–9. doi: 10.1007/s40520-020-01665-2
Keywords: assistive technology, neurodegenerative diseases, healthcare, COVID19, quality of life, caregivers burden
Citation: Stasolla F, Matamala-Gomez M, Bernini S, Caffò AO and Bottiroli S (2021) Virtual Reality as a Technological-Aided Solution to Support Communication in Persons With Neurodegenerative Diseases and Acquired Brain Injury During COVID-19 Pandemic. Front. Public Health 8:635426. doi: 10.3389/fpubh.2020.635426
Received: 30 November 2020; Accepted: 24 December 2020;
Published: 16 February 2021.
Edited by:
Sonu Bhaskar, Liverpool Hospital & South West Sydney Local Health District (SWSLHD), AustraliaReviewed by:
Robert Weissert, University of Regensburg, GermanyNegman Walmore Alvarado Rivera, Universidad Nacional Tecnológica, Argentina
Copyright © 2021 Stasolla, Matamala-Gomez, Bernini, Caffò and Bottiroli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabrizio Stasolla, Zi5zdGFzb2xsYUB1bmlmb3J0dW5hdG8uZXU=